Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Optimising Complex Surgical Trays Based on PDSA Cycles
Authors Duan HX, Wang XM, Guo Y, Wei L, Hao RX, Guo ZS
Received 14 August 2023
Accepted for publication 16 November 2023
Published 24 November 2023 Volume 2023:16 Pages 3619—3628
DOI https://doi.org/10.2147/JMDH.S435427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hong-Xia Duan, Xiu-Mei Wang, Yue Guo, Ling Wei, Rui-Xia Hao, Zhen-Shan Guo
Department of Surgery, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences), Taiyuan, Shanxi, People’s Republic of China
Correspondence: Hong-Xia Duan, Department of Surgery, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences), No. 99 Longcheng Street, Taiyuan, Shanxi, People’s Republic of China, Tel +86-3518379228, Email [email protected]
Objective: To investigate the application of a multidisciplinary collaboration model to optimise the configuration management of orthopaedic external device sets in general hospitals.
Methods: A pretest–post-test study design was used. Sixty patients who underwent unilateral total knee arthroplasty and 60 patients who underwent posterior lumbar interbody fusion between March and May 2022 were recruited as the control stage. Additionally, a total of 120 patients, 60 of each, who underwent the two procedures between September and November 2022, were recruited as the experimental stage. For the control stage, conventional external equipment management was used, and for the experimental stage, an external device management programme was implemented based on multidisciplinary collaboration with the control stage. Based on the PDSA cycle, the configuration management of orthopaedic external device sets was optimised, and the differences in collating and counting external devices, nurses’ overtime in the external device stage and orthopaedic surgeon satisfaction were compared between the two stages.
Results: Compared with the control stage, the collation count took less time (8.65 ± 0.25 min vs 5.37 ± 0.13 min; 13.55 ± 1.10 min vs 7.85 ± 0.82 min), the number of overtime hours was shorter (175.80 ± 12.19 min vs 96.68 ± 13.66 min) and orthopaedic surgeon satisfaction was improved (4.58 ± 0.62 vs 4.10 ± 0.68; 4.33 ± 0.73 vs 3.87 ± 0.77; 4.20 ± 0.71 vs 3.82 ± 0.71; 4.12 ± 0.69 vs 3.87 ± 0.72; 4.05 ± 0.68 vs 3.79 ± 0.68) in the experimental stage (all P < 0.05).
Conclusion: Multidisciplinary collaboration offers various benefits for optimising the configuration of external device sets, such as reducing the time taken for the preoperative sorting and counting of external devices, enhancing nurses’ work efficiency and improving surgeons’ job satisfaction; therefore, it is worthy of reference in clinical practice.
Keywords: operating theatre, optimisation configuration, external instruments, item counting, scientific management, work efficiency
External surgical devices are reusable devices leased to hospitals by suppliers for use primarily in implant-related procedures.1 External devices used in surgery are difficult to manage for two reasons: one is the increased risk of infection owing to the frequent movement between hospitals,2 and the other is the burdensome task of counting surgical items3 brought about by the large number of external devices.4 According to research, only 13% of all surgical items on an operating table are utilised during surgery.5 To this end, surgeons actively participate in optimising the configuration of surgical items to reduce the disposal time of those items at each stage.6,7 Domestically, surgical items are mostly configured by nurses in operating theatres according to the preferences of surgeons, whereas external devices are configured by the manufacturer’s personnel, requiring almost no participation by surgeons or nurses in the operating theatre. One study revealed poor communication between clinical departments, operating theatres and disinfection supply centres in the management of external surgical devices.8 Frequently, external surgical devices are not delivered to disinfection supply centres on time, causing surgical delays and even affecting the efficiency of the entire operating theatre.9 Orthopaedic external surgical devices are generally used as implants. They are supplied with power tools and instrument boxes, which constitute an important part of hospital instrument management.10 No studies have been found to optimise the management of orthopaedic kits based on the PDSA cycle; however, such problems often exist in reality, and improving and optimising the management process can greatly improve work efficiency and reduce the risk of infection.
Our hospital is a grade-A tertiary comprehensive hospital that performs approximately 6000 orthopaedic surgeries requiring external devices (implants) every year. Surgical devices from eight foreign medical device companies have been approved for use in our hospital, mainly for spinal, joint and bone trauma surgeries. As demonstrated by the results of the pre-investigation above, external device kits are over-configured, and many are not used routinely, resulting in the inconvenience of counting items in the operating theatre. Despite the existence of some external devices with a high frequency of use, they are not managed in a targeted manner, which leads to a high risk of infection due to frequent movements between companies and hospitals. Moreover, repeated receiving and counting increase the workload of nurses in supply rooms. In this study, based on the management of external surgical devices in our hospital’s department of orthopaedics, the application of a multidisciplinary cooperation model (such as between the operating theatre, orthopaedic department and supply rooms) in the management of external device sets in the department of orthopaedics in general hospitals is discussed, providing a reference for clinical practice. The details are reported as follows.
Materials and Methods
General Data
This study used a pretest–post-test design. Using the historical control study method, 60 patients who underwent unilateral total knee arthroplasty and 60 patients who underwent posterior lumbar interbody fusion (PLIF), which were common surgeries in the department of orthopaedics in our hospital between March and May 2022, were recruited as the control stage (10 were excluded). An additional 120 patients, of whom 60 underwent the first procedure and 60 underwent the second between September and November 2022, were recruited as the experimental stage (8 were excluded).
The inclusion criteria were as follows: (1) patients who underwent unilateral total knee arthroplasty or PLIF; (2) patients with complete relevant data related to this study; (3) patients without infection before surgery; (4) patients and their families were aware of the specific content of this study and gave the relevant signed informed consent. The exclusion criteria were as follows: (1) patients with abnormal immune function; (2) patients with organic diseases, such as coronary heart disease and diabetic nephropathy; (3) patients with poor control of basic diseases; (4) patients with mental disorders resulting in an inability to communicate normally; (5) patients transferred from other hospitals.
The same circulating nurses and instrument nurses participated in the cooperation between the two stages. Among the four orthopaedic nurses, the instrument nurses had “3 years” work experience each, and the two circulating nurses had 10 years’ work experience each. The nurses in the external device stage in the supply room were fixed in their posts.
Intervention Methods
Implementation Scheme of the Control Stage
The control stage was managed using routine external devices.
Before surgery, the surgeon applied to the equipment department to use implants and informed the personnel of the external device manufacturer, who notified the warehouse management personnel of the company to prepare the implants and supporting external devices and print a device counting list. Subsequently, the manufacturer’s personnel delivered the prepared implants to the equipment department for inspection and then sent them together with the external devices to the supply room, where these devices and implants were received according to the counting list. After cleaning and sterilising, the external devices and implants were sent to the operating theatre for later use. Devices that were not included in the counting list were rejected, and the counting list was reprinted after modification.
On the day of surgery, the instrument nurses opened all the prepared external device kits at the same time, selected the necessary items and arranged the instrument table. After the external devices had been used, they were transferred from the operating theatre to the supply room, where they were cleaned and disinfected; they were then handed over to the manufacturer’s personnel and returned to the company’s warehouse for storage.
Implementation Scheme of the Experimental Stage
Implementation for the experimental stage was based on a multidisciplinary collaborative external device management programme based on that of the control stage, which was determined by the project expert group’s reference to previous data collection and interview results and clinical discussion. The PDSA cycle mode was applied in the experimental stage.11 See Figure 1 for specific optimization process.
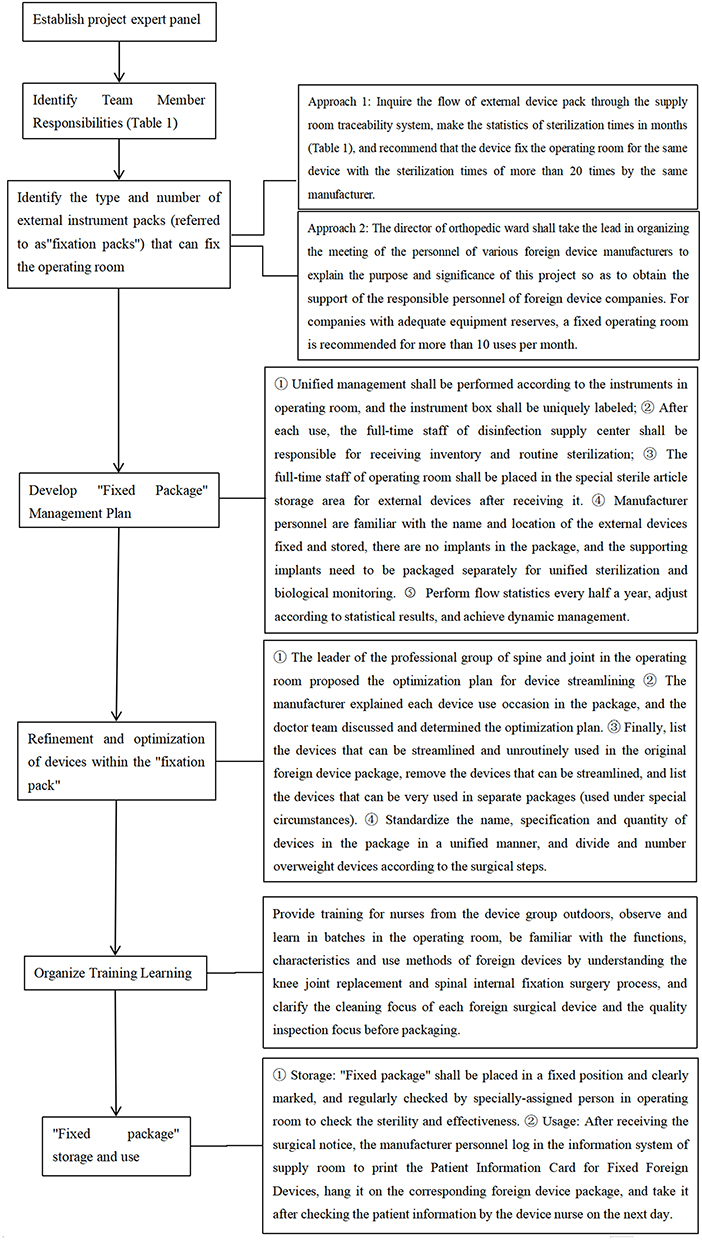 |
Figure 1 Optimization Flow Chart. |
Plan (P)
According to previous data collection and interview results, the existing problems were analysed, and the research topics for optimising the configuration of external device sets and formulating fixed external device management programmes were established.
Implementation (D)
A multidisciplinary expert group (comprising the chief physician of the orthopaedic joint ward, chief physician of the spinal ward, head nurse of the operating theatre, head nurse of the operating theatre orthopaedic professional group, head nurse of the operating theatre device management group, head nurse of the supply room and head nurse of the external device group) was formed to establish specific implementation plans through meetings and discussions (See Table 1).
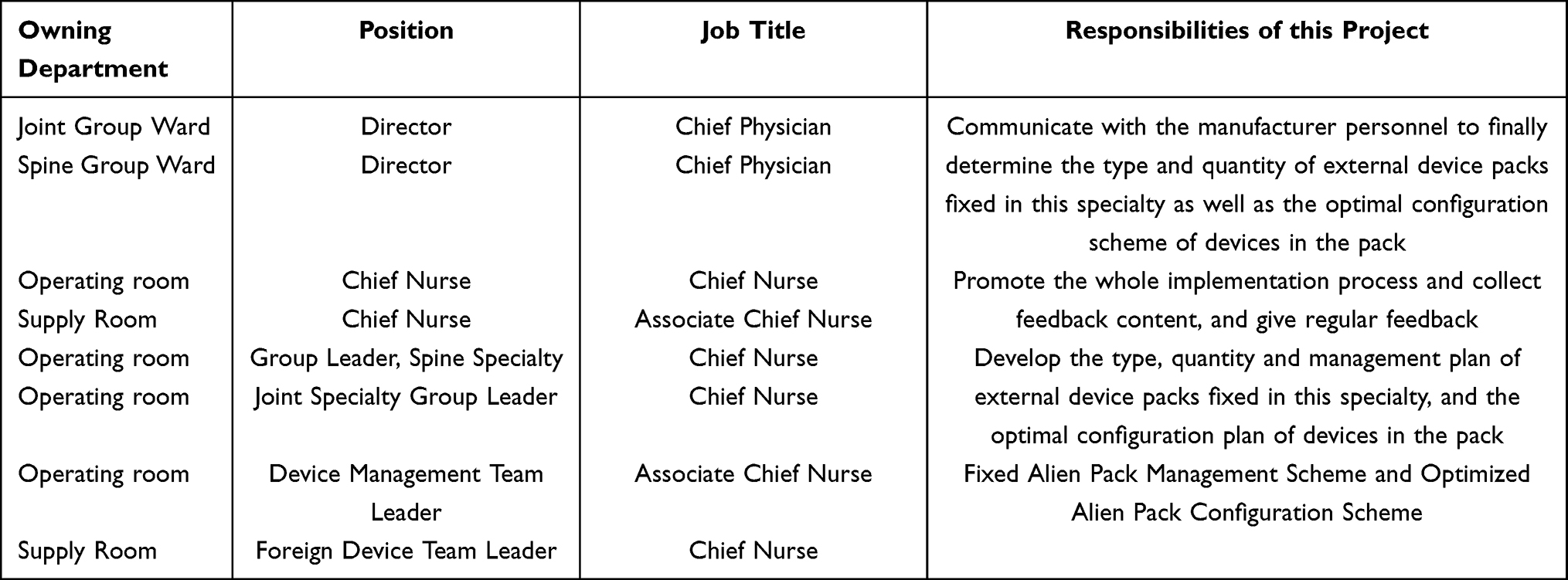 |
Table 1 Project Expert Group Members and Responsibilities |
(1) Optimisation of type and quantity of fixed external device kits: The first task was to investigate the flow of external device kits via the traceability system in the supply room and count the number of sterilisations in months. If the sterilisation times of the same set of devices from the same manufacturer exceeded 20 times, it was suggested that the device be fixed in the operating theatre and the head nurse in the operating theatre should communicate with the person in charge at the manufacturer. The second task, which was led by the chief physician of the orthopaedic joint ward, was to organise a meeting with staff from the external device manufacturers. For companies with sufficient external device reserves, it was recommended that the device be used more than 10 times a month to fix it in the operating theatre, and the final result was determined by the person in charge of the company. The management scheme for fixed external device kits mainly includes the following: ① Unified management is performed for the devices in the operating theatre, with unique labels attached to the device boxes; ② after each use, the external devices are received, counted and routinely sterilised by the full-time staff at the disinfection supply centre; ③ after being received by the specialised personnel in the operating theatre, external devices are placed in a dedicated sterile article storage area; ④ manufacturer’s personnel should be familiar with the names and locations of external devices, which are stored in their respective places, and there should be no implants in the instrument packs. The supporting implants should be packaged separately, sterilised and biologically monitored; ⑤ flow statistics should be gathered every 6 months, and adjustments should be made according to the statistical results to achieve dynamic management.
(2) Optimisation of the fixation of outsourcing devices in the operating theatre: ① Based on the use of and need for various outsourced devices, the team leader of the operating theatre spinal group listed the backup devices for spinal internal fixation, and the team leader of the operating theatre joint group listed the backup devices for arthroplasty. Following this, project team meetings were held to discuss the finalised protocol, which listed the streamlined instruments and non-traditional instruments in the original external device set. As streamlined instruments were removed, infrequently used instruments were listed and individually packaged (for special use). ② The leader of the orthopaedic professional group in the operating theatre, the leader of the instrument management group, the leader of the external instrument group in the supply room and the personnel from the instrument manufacturers configured the instruments according to the streamlined scheme; standardised the name, specification and quantity of the items in the sets; framed and numbered overweight devices according to the surgical steps and marked unconventional devices as “additional”. If a whole set of knee arthroplasty devices was divided into four frames, they were named “Haotuo Total Knee Item 4-1#”, “Haotuo Total Knee Item 4-2#”, “Haotuo Total Knee Item 4-3#” and “Haotuo Total Knee Item 4-Additional”; “Haotuo” indicated the manufacturer an device belonged to, and “4” indicated there were four complete sets, which served as a reminder for the instrument nurses when preparing items. A detailed card was attached to each device kit, and the counting list of external devices corresponded to each individual item. The counting list details and plan were uploaded to the traceability system of the supply room to synchronise the surgical anaesthesia system.
(3) Optimisation of external device storage management: The sterile article storage area in the operating theatre was set up with a special area for external devices, and each company was assigned individual shelves. The fixed external devices were placed in a specific position and marked clearly. There were several sets of devices packaged in frames that should be marked on the label, and the specialised personnel in the operating theatre regularly counted them and checked for sterility. After receiving a notice of surgery, the manufacturer’s personnel went to the equipment department to check the implants and pass them to the supply room. They logged in to the supply room’s information system and printed a Patient Information Card for Fixed External Devices, which included the patient’s name, hospital number, the name of the scheduled surgery, name of the external device and surgeon. The supporting implant qualification certificate and information card were submitted to the supply room, and after completing biological monitoring, the implants were sterilised and sent from the supply room to the operating theatre. The operating theatre arranged for specific management personnel to receive the implants and classify them by manufacturer. The patient information card was hung on the corresponding external device set and retrieved the next day after being checked by the instrument nurses.
Learning (S)
The nurses in the experimental stage were trained in spinal surgical devices and joint replacement surgical devices from different perspectives, such as surgical procedures and device use, by the leaders of the orthopaedic professional group in the operating theatre and the external device manufacturers. The nurses were organised into groups to observe and learn in the operating theatre. The learning was assessed and supervised, timely guidance was provided, and any problems found were addressed to continuously improve familiarity with the management process.
Treatment (A)
In the process of implementing the intervention measures, the head nurse recorded the practical problems arising from clinical practice, held regular departmental meetings to guide and educate the nurses in the device group, summarised the previous cycle’s effect, re-educated (conducted meetings, learning and improvement every 2 weeks), summarised the clinical experience and expanded the scale of clinical application.
Evaluation Indicators
Time Taken for Preoperative Sorting and Counting of External Devices
The counting time of the external devices was recorded by a professional researcher. The counting began with the opening of the first external device set on the operating table and ended with the instrument nurses setting the parts of the kit out in order. After sorting, the counting began until all external devices on the operating table had been counted. In the case of an interval between the use of two sets of external instruments in an operation, they were counted independently and then added.
Overtime Hours of Nurses in the External Device Group in the Supply Room
Statistics were gathered on the overtime hours of the nurses in the external device group in the supply room via the attendance system. The overtime hours of the four nurses in the external device group for 66 working days were summed and then averaged for each nurse per day to obtain the daily overtime hours.
Satisfaction of Orthopaedic Surgeons
A self-made satisfaction questionnaire for orthopaedic surgeons was developed, which consisted of 15 items in five dimensions: preparation of surgical items, delivery of devices, cooperation in surgery, use of special instruments and management of external devices. Each item was scored using the 5-point Likert scoring method, with 1–5 points scored for very dissatisfied, “dissatisfied”, “generally satisfied”, “satisfied” or “very satisfied”, respectively. The higher the score was, the higher the surgeons’ satisfaction. The satisfaction evaluation was performed after each surgery. The pre-investigation assessment revealed that the Cronbach’s α coefficient of the scale was 0.947.
Statistical Analysis
A statistical analysis was performed using SPSS 26.0 software. Data were tested for normality using the Shapiro–Wilk test with measurements conforming to a normal distribution expressed as  , and comparisons between stages were performed using a t-test. Count data were expressed by frequency and percentage, and comparisons between stages were made using the χ2 test, with P < 0.05 indicating a statistically significant difference.
, and comparisons between stages were performed using a t-test. Count data were expressed by frequency and percentage, and comparisons between stages were made using the χ2 test, with P < 0.05 indicating a statistically significant difference.
Results
Statistics on External Device Sets Fixed in the Operating Theatre After Project Implementation
Before implementation, the external devices were not fixed regardless of the frequency of use. Subsequently, 13 external devices were fixed in the spine group and 15 in the joint group, making a total of 28 external devices fixed in the operating theatre.
2.2 Statistics on the number of surgical instruments in the orthopaedic external device sets before and after the optimised configuration
The use of the DK spinal internal fixation devices from CMIC were optimised from 58 to 47, of which 9 were additional devices. Haotuo knee arthroplasty devices were optimised from 142 to 85 items, including 4 sets, of which 12 items were additional devices, and 73 items were sub-packaged into 4-1#, 4-2# and 4-3# according to the order of use. Furthermore, the additional devices were reserved under special circumstances and not routinely used on the operating table; furthermore, they were not used during data collection.
Comparison of Time Taken for Preoperative Sorting and Counting of External Devices Between the Two Stages
Compared with the control stage, the sorting count before PLIF and spinal instrumentation was shorter in the experimental stage (8.65 ± 0.25 min vs 5.37 ± 0.13 min; 13.55 ± 1.10 min vs 7.85 ± 0.82 min) by almost two-thirds, and the difference was statistically significant (P < 0.001) (Table 2).
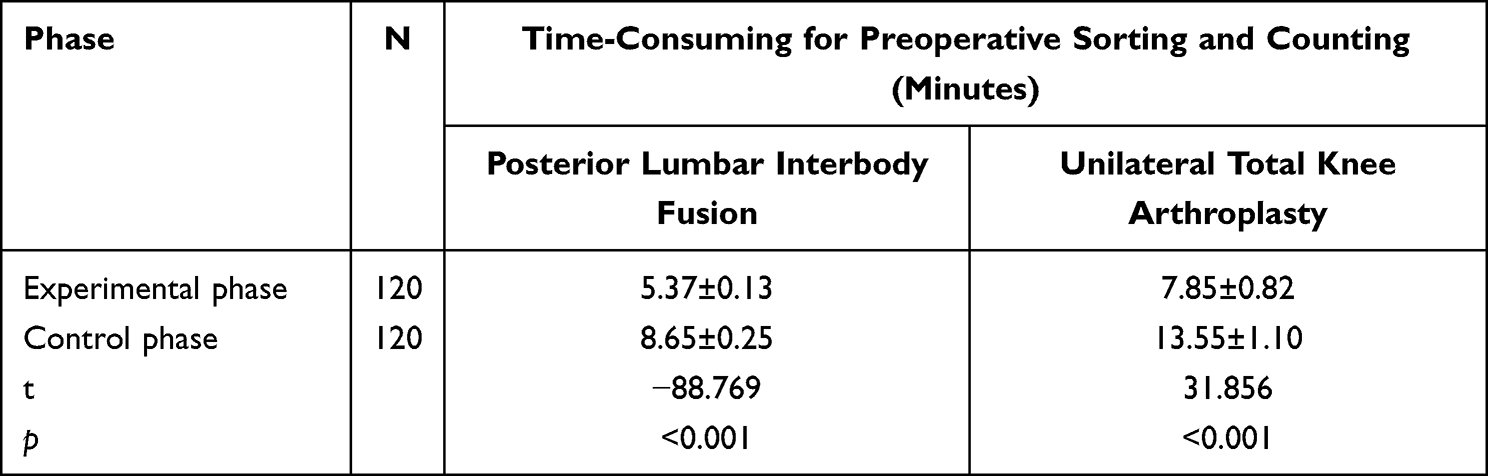 |
Table 2 Comparison of Time-Consuming for Preoperative Sorting and Counting of External Instruments Between the Two Phases (Minutes) |
Average Daily Overtime Hours of Nurses in the External Device Group in the Supply Room
The mean daily overtime hours were significantly shorter in the experimental stage than in the control stage (96.68 ± 13.66 min vs 175.80 ± 12.19 min) by 79.12 min (P < 0.001) (Table 3).
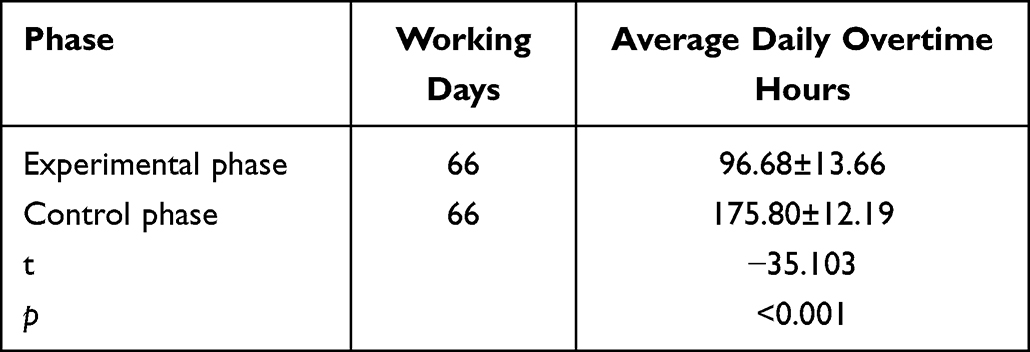 |
Table 3 Average Daily Overtime Hours of Nurses of the External Instrument Group in the Supply Room (Minutes) |
Comparison of Orthopaedic Surgeons’ Satisfaction with the Two Stages
Orthopaedic surgeons’ satisfaction with surgical instrument preparation, device delivery, cooperation during surgery, use of special devices and management of external devices was higher in the experimental stage than in the control stage (4.58 ± 0.62 vs 4.10 ± 0.68; 4.33 ± 0.73 vs 3.87 ± 0.77; 4.20 ± 0.71 vs 3.82 ± 0.71; 4.12 ± 0.69 vs 3.87 ± 0.72; 4.05 ± 0.68 vs 3.79 ± 0.68, respectively). The degree of satisfaction mostly changed from “satisfied” to “very satisfied”, and the difference was statistically significant (P < 0.05) (Table 4).
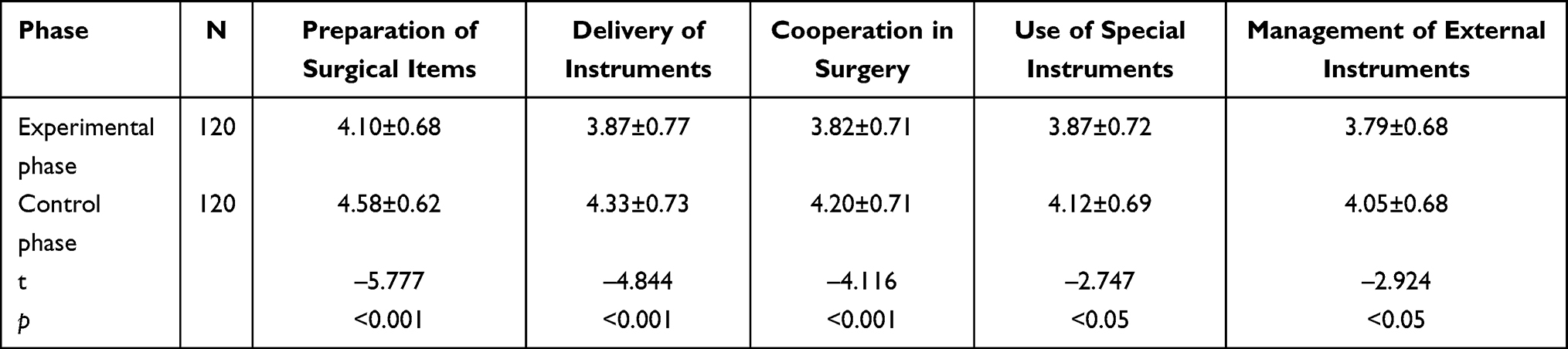 |
Table 4 Comparison of Orthopedic Surgeons’ Satisfaction with the Two Phases |
Discussion
Orthopaedic external devices are mostly configured independently by the manufacturer’s personnel, with little involvement from orthopaedic surgeons. To cope with various unexpected situations, the manufacturer’s personnel often over prepare the devices, resulting in as many as 200 devices and three or four inventories for a single operation.12 As a result, instrument nurses are required to spend a long time sorting and counting external devices, which affects the cooperation process in surgery.13 One study14 revealed that the number of surgical instruments in a surgical tray can be reduced by 70% without harming the safety of patients, shortening the surgical time and facilitate the arrangement of more surgical procedures. In this study, the number and configuration of external devices were streamlined and optimised by orthopaedic surgeons under the initiative of the operating theatre through multidisciplinary cooperation. The results showed that the classification and counting time of external devices in PLIF decreased from 8.65 ± 0.25 minutes to 5.37 ± 0.13 minutes, and unilateral total knee arthroplasty decreased from 13.55 ± 1.10 minutes to 7.85 ± 0.82 minutes after the optimised configuration of external devices. The time was almost two-thirds shorter, which shows improved optimisation. Compared with the study results of Martyn et al14 the time was further reduced, saving about 3.5 and 5.5 min, indicating the effectiveness of this experimental scheme. Moreover, the time taken by instrument nurses to sort the instrument table and count the devices was clearly reduced. The reason for this may be as follows. First, by removing unused items, single-packing spare items and streamlining external devices, instrument nurses no longer need to determine which instruments should be used, which are spare and which will not be used before sorting the external devices; they can directly place the devices on the operating table according to the surgical steps, saving time by not having to sort instrument tables, especially if instrument nurses are not familiar with surgery.15,16 Second, after the devices are divided into frames according to the surgical steps, when the surgical time is tight, the time for each external device to be placed on the operating table can be reasonably arranged according to the surgical steps to avoid interruptions from counting and ensure the quality of counting, effectively resolving the time-consuming issue of sorting and counting external instruments.17
The results of this study showed that the average daily overtime hours of the nurses in the group supplying external devices decreased from 175.80 ± 12.19 minutes to 96.68 ± 13.66 minutes as a result of implementing the management programme for fixed external device kits, with overtime hours significantly reduced. The number of hours of overtime was reduced by half (79.12 min) and changed significantly before and after the experiment; this greatly reduced the workload of instrument nurses and improved work efficiency, and the study showed improved optimisation. External medical devices are not the fixed assets of hospitals but are circulated and used by suppliers in multiple hospitals to maximise their benefits.18 Regrettably, such a complex circulatory connection poses many difficulties for management.19 In the present study, some external device kits were stored in a fixed manner through the flow statistics of external device kits and active communication with the manufacturer’s personnel. Fixed external device kits were not returned to the company’s warehouse after use; therefore, the counting, receiving and cleaning processes before removal and the same ones for delivery were integrated, greatly reducing the workload of the nurses in the external device group in the supply room. By optimising the configuration of external devices in the fixed operating theatre, each instrument was simplified to reduce the cleaning and counting workload. Furthermore, the nurses in the external device group in the supply room understood and mastered the function of the devices after targeted training so that they could count easily, find the key points when cleaning and greatly improve their work efficiency. For a long time, the handover of external devices has been the focus of many researchers.20 It is specified in the Health Industry Standards of the People’s Republic of China that external devices must arrive in the supply room before 15:00 the day before surgery. For various reasons, the personnel of external device companies often deliver all external devices at the specified time, resulting in the clustered handover of external devices. Since the implementation of the scheme, fixed external device sets have been managed in the same way as operating theatre instruments and are cleaned and sterilised immediately after use. This is performed on a staggered basis with the receipt and counting of temporary external equipment, solving the problem of unnecessary overtime caused by the clustered handover of external devices and the difficulty in coordinating the working hours and intensity of the nurses of the external device group in the supply room; consequently, the overall work efficiency of the nurses of the external device group is improved.
The results of this study show that the orthopaedic surgeons in the experimental stage were more satisfied with the preparation of surgical items, the delivery of devices, cooperation during surgery, the use of special instruments and the management of external devices than those in the control stage. Most changed from “satisfied” to “very satisfied”, which greatly improved the satisfaction of surgeons and increased the cooperation between doctors and nurses,21 thereby improving the accuracy and efficiency of surgery. Multidisciplinary cooperation, as a trend in modern hospital management,21–23 allows surgeons to truly participate in the optimal configuration of external instruments. In this study, the number of knee arthroplasty devices was optimised from 142 to 85, and the additional devices used for special situations were not routinely used on the operating table. The preoperative and postoperative times for sorting and counting instruments were clearly shortened, cooperation during surgery became smoother and shortened the surgical process, and the satisfaction of surgeons with nurses improved, which was consistent with the results of Liu et al.24 The management scheme for fixed external device sets further regulates the name, fixed quantity, storage, use and recovery of external devices. The set is labelled “total number–serial number”, making it easy for instrument nurses to see the reference total number when preparing instruments. In case of tight operating times, external devices are placed on the operating table in frames and stages according to the surgical steps so that instrument nurses can work methodically and pass the instruments accurately.
Due to the limitations of study conditions, only a small number of external device sets were fixed in this study. The full implementation of a volume-based procurement policy will enable distributors to reserve commonly used orthopaedic products in hospitals. In subsequent research, our research team will further establish a complete external device management system in conjunction with relevant departments to make the management of external devices safer and more standardised. This project is a small step to improving the operational efficiency of operating theatres by optimising the management of surgical instruments to reduce surgery time. However, many constraints affect the duration of surgery; thus, more comprehensive and detailed research is needed to analyse strategies to improve the operational efficiency of operating theatres.
Conclusion
In this study, external devices were fixed in the operating theatre using a multidisciplinary cooperation model, and a corresponding management scheme was formulated to reduce the frequent flow and handover of external devices. Optimising the configuration of fixed external device sets can reduce the time needed for the preoperative and postoperative sorting and counting of external devices, which is worthy of clinical reference.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Shanxi Bethune Hospital.
Funding
The project was supported by Research project of Shanxi Provincial Health Commission: Establishment and application of standardized node control platform in perioperative patient safety management (2023137).Funding agencies did not play a role in study design, data collection, analysis and interpretation, and manuscript writing.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Wu S, Cerceo E. Sustainability initiatives in the operating room. Jt Comm J Qual Patient Saf. 2021;47(10):663–672. doi:10.1016/j.jcjq.2021.06.010
2. Qing Z, Haiyan G, Tianyu Z, Kanwen J, Liming Q. Survey of loaner instrument and implants processing status in 764 hospitals in China. Chn Nur Mgmt. 2019;19(01):119–122.
3. Helmkamp JK, Le E, Hill I, et al. Addressing surgical instrument oversupply: a focused literature review and case-study in orthopedic hand surgery. Hand NY. 2022;17(6):1250–1256. doi:10.1177/15589447211017233
4. Qin X, Weiming Q, Tiyu Z, Jianwen Y. Investigation on the current management situation of foreign surgical instruments in 1166 public hospitals in China. Chn Nur Mgmt. 2022;22(10):1477–1481.
5. Crosby L, Lortie E, Rotenberg B, Sowerby L. Surgical instrument optimization to reduce instrument processing and operating room setup time. Otolaryngol Head Neck Surg. 2020;162(2):215–219. doi:10.1177/0194599819885635
6. Dos Santos BM, Fogliatto FS, Zani CM, et al. Approaches to the rationalization of surgical instrument trays: scoping review and research agenda. BMC Health Serv Res. 2021;21(1):163. doi:10.1186/s12913-021-06142-8
7. Olivere LA, Hill IT, Thomas SM, et al. Radiofrequency identifification track for tray optimization: an instrument utilization pilot study in surgical oncology. J Surg Res. 2021;264:490–498. doi:10.1016/j.jss.2021.02.049
8. Yuhong S, Yujian Q, Wei W, Weiming Q. Analysis on the present situation of surgical instruments management in hospitals of level II and above. Chn Nur Mgmt. 2019;19(05):729–734.
9. Tipple AFV, Costa DM, Lopes LKO, et al. Reprocessing of loaned surgical instruments/implants in Australia and Brazil: a survey of those at the coalface. Infect Dis Health. 2022;27(1):23–30. doi:10.1016/j.idh.2021.09.003
10. Costa DM, Lopes LKO, Vickery K, et al. Reprocessing safety issues associated with complex-design orthopaedic loaned surgical instruments and implants. Injury. 2018;49(11):2005–2012. doi:10.1016/j.injury.2018.09.006
11. Taylor MJ, McNicholas C, Nicolay C, Darzi A, Bell D, Reed JE. Systematic review of the application of the plan-do-study-act method to improve quality in healthcare. BMJ Qual Saf. 2014;23(4):290–298. doi:10.1136/bmjqs-2013-001862
12. Zhou Q, Xinglian G, Juanjuan H, Jing L, Tian X, Yesong X. Practice of optimizing the inventory method of orthopedic external instruments based on Pad inventory system. J Nur. 2022;29(12):25–27. doi:10.16460/j.ISSN1008-9969.2022.
13. Xinyu Z, Changxia X. Application of standardized management mode of orthopedic external instruments in orthopedic surgery. Elec J Pract Clin Nurs Sci. 2020;5(21):179–180.
14. Martyn K, Gay Samuel S, Konchan Sarah K, et al. Data analysis of vascular surgery instrument trays yielded large cost and efficiency savings. J Vasc Surg. 2021;73(6):2144–2153. doi:10.1016/j.jvs.2020.09.043
15. Zhu X, Yuan L, Li T, Cheng P. Errors in packaging surgical instruments based on a surgical instrument tracking system: an observational study. BMC Health Serv Res. 2019;19(1):176. doi:10.1186/s12913-019-4007-3
16. Neumann J, Angrick C, Höhn C, et al. Surgical workflow simulation for the design and assessment of operating room setups in orthopedic surgery. BMC Med Inform Decis Mak. 2020;20(1):145. doi:10.1186/s12911-020-1086-3
17. Cichos KH, Hyde ZB, Mabry SE, et al. Optimization of orthopedic surgical instrument trays: lean principles to reduce fixed operating room expenses. J Arthropl. 2019;34(12):2834–2840. doi:10.1016/j.arth.2019.07.040
18. Minzhi J, Fenglian C, Kanwen J, et al. Application of the whole-process quality traceability information management for rental medical devices. Chn Nur Mgmt. 2021;21(10):1457–1459.
19. Yanyan W, Tingting X, Lijuan X, et al. Management of loaner medical instruments and implants in hospitals in Hubei province. Chn J Infect Control. 2022;21(05):420–429.
20. Chang N, Miao Z, Yanan L, Li X. Application of PDCA cycle combined with failure mode and effect analysis in the management of implants and foreign devices. J Zhengzhou Uni (Med Sci). 2023;58(01):113–116.
21. Chobin N. Surgical instrument decontamination: a multistep process. AORN J. 2019;110(3):253–262. doi:10.1002/aorn.12784
22. Loesche AH. Using huddles to improve communication and teamwork in an instrument-processing department. Nurs Mgmt (Harrow). 2020;27(6):34–42. doi:10.7748/nm.2020.e1958
23. Jianhong C, Mingmin C, Wenjun Y. Application of multidisciplinary cooperation in the construction of process management system for external instruments and implants. J Trad Chn Med Mmtg. 2020;28(11):220–223. doi:10.16690/j.cnki.1007-9203.2020.11
24. Liu L, Guo L, Jianmei J, Chunyang Z, Yuquan P. Practice and the effect of optimizing the allocation of surgical instrument kits for open surgery in a cancer hospital in Beijing. Chn Nur Mgmt. 2022;22(01):5–8.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.