Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Optimisation and Effect Analysis of the Blood Collection Method in Pre-Deposit Autotransfusion Patients Undergoing Thoracotomy Surgery
Authors Jia L, Wang Y, Zhang W, Lin Y, Chen F, Wan Y, Fu X
Received 5 June 2023
Accepted for publication 11 September 2023
Published 20 September 2023 Volume 2023:16 Pages 2793—2798
DOI https://doi.org/10.2147/JMDH.S424470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Limin Jia,1 Yanfeng Wang,2 Wenyuan Zhang,3 Yulian Lin,1 Fang Chen,1 Yixiao Wan,1 Xin Fu4,5
1Department of Cardiothoracic Surgery, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, Zhejiang, 317000, People’s Republic of China; 2Department of Geriatrics, Taizhou Central Hospital (Taizhou University Hospital) of Zhejiang, Taizhou, Zhejiang, 318000, People’s Republic of China; 3Department of ICU, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, Zhejiang, 317000, People’s Republic of China; 4Department of Radiology, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, Zhejiang, 317000, People’s Republic of China; 5Department of Radiology, Enze Hospital, Taizhou Enze Medical Center (Group), Taizhou, Zhejiang, 318000, People’s Republic of China
Correspondence: Xin Fu, Department of Radiology, Taizhou Hospital of Zhejiang Province affiliated to Wenzhou Medical University, No. 150 Ximen Street, Linhai City, Taizhou, Zhejiang, 317000, People’s Republic of China, Tel + 86-0576-85120120, Email [email protected]
Background and Purpose: To explore the feasibility of the modified blood collection method in pre-deposit autotransfusion in patients undergoing thoracotomy surgery.
Methods: This double-blinded randomised controlled trial enrolled 92 patients from the cardiothoracic surgery department from February 2019 to October 2020.
Results: Compared with the conventional blood collection method, the modified blood collection method avoided blood overflow from the oblique plane of the needle (χ2 = 61.986, P < 0.01) and reduced the diameter of the bruising area after 24 hours (χ2 = 24.611, P < 0.01). Furthermore, due to optimising the blood collection method, diastolic blood pressure reduced slightly before and after blood collection (t = 2.036, P < 0.05), and patients in the test group had less pain (based on the numerical rating score) (t = 5.556, P < 0.01). Meanwhile, the time required to collect 400 mL of blood was shortened (t = 17.744, p < 0.01).
Conclusion: An improved blood collection method can enhance the blood donation experience, avoid blood spillage, lessen pain and reduce adverse reactions. This may be of great significance in ensuring blood quality and the safety of subsequent transfusions.
Clinical Trials Registration: ClinicalTrials.gov Identifier: NCT05539846.
Keywords: pre-deposit autotransfusion, extracorporeal circulation, open heart surgery
Introduction
Autologous blood transfusion has the advantages of saving blood resources, decreasing allogeneic blood consumption,1 avoiding immunosuppression caused by allogeneic blood transfusion,2 reducing the risk of blood transfusion and blocking blood-borne diseases.3 However, perioperative blood transfusion during cardiac surgery may cause postoperative complications.4 Pre-deposit autotransfusion (also called pre-deposit autologous blood transfusion) has no age limitations and is safe if the cardiovascular condition is stable, even for elderly patients undergoing cardiovascular surgery.5,6 It is especially suitable for patients with rare blood types undergoing heart surgery.7 Therefore, pre-deposit autologous blood transfusion has been promoted and used earlier in clinical practice.8 Due to different blood collection subjects, there are still many problems with the blood collection method at the same in the blood station. Although there are many benefits to pre-deposit autologous blood transfusions, safe, effective and individualised blood collection methods have not yet been reported.
The front of the blood sampling needle is wedge-shaped and the middle is an empty core. When the blood sampling needle tip enters the blood vessel, but the wedge-shaped inclined plane of that needle does not fully enter that blood vessel, there is a short moment when the venous vascular cavity is connected with the outside, resulting in blood overflow. Second, the diameter of the bruised area after 24 hours is greater than 5 mm. Third, blood clotting occurs after an autologous blood transfusion. Thus, whether the bevel direction influences the safety and comfort of patients in the pre-deposit autotransfusion remains unknown.
The study aims to investigate the effect of improved blood collection methods on patients having pre-deposit autotransfusion while undergoing open heart surgery.
Materials and Methods
Participants
A total of 92 patients admitted to the cardiothoracic surgery department from February 2019 to October 2020 who had planned mitral valve surgery were included in this study. The study was in accordance with the Declaration of Helsinki and was reviewed and approved by the Taizhou Hospital of Zhejiang Province affiliated to Wenzhou Medical University’s ethics committee (Approval No. K20200618). Written informed consent was obtained from all participants.
The inclusion criteria were as follows:9 ① weight: ≥50 kg; ② haemoglobin ≥110 g/L; ③ heart function: I–II; ④ patients who were expected to have a large amount of surgical bleeding and may require blood transfusion; and ⑤ with surgical indications and surgical conditions. The exclusion criteria included ① having a history of hematophobia; ② having communication difficulties and being unable to cooperate; and ③ having blood collection interruption caused by various accidents.
Study Design
All participants were randomly divided into two groups by SPSS software, which generated random numbers and groups. Control group: According to the conventional blood collection method, the bevel of the blood collection needle head was upward, and the needle was inserted at a 30–45 degrees angle to the patient’s blood vessel. Test group: The bevel of the blood collection needle head was downward, and the needle was inserted into the skin with the bevel of the needle parallel to the skin. The other blood collection operations of the two groups were the same: The blood collection volume was 400 mL, and the routine treatment was performed after the blood collection. In total, there were 45 cases in the test group, including 21 males and 24 females, and 47 cases in the control group, with 24 males and 22 females. The blood collection process is presented in Supplementary Table 1.
Data collection and evaluation indicators were as follows: ① blood spilling from the bevel of the needle when the needle was inserted;10 ② the diameter of the bruised area being greater than 5 mm after 24 hours;11 ③ a blood clot during the autologous blood transfusion when checked;12 ④ changes of heart rate and blood pressure before and after blood collection;13 ⑤ the patient pain score (numerical rating scale score);11 ⑥ the time required to collect 400 mL of blood;14 and ⑦ adverse reactions, such as dizziness, palpitations, pale complexion and low volume shock.15
Statistical Analysis
SPSS 25.0 statistical software was used for statistical analysis of the data. The measurement data were normally distributed and expressed as mean ± standard deviation ( ). The independent samples t-test was used for inter-group comparison. The paired sample t-test was used for comparison before and after treatment. The counting data were expressed by rate or constituent ratio (%), and the chi-squared test was used for inter-group comparison (χ2), with the inspection level being α = 0.05. The statistical power was calculated using the PASS 15 software (NCSS, LLC., Kaysville, Utah, USA, ncss.com/software/pass). Group sample sizes of 47 in control group 1 and 45 in test group achieved a 99.995% power, detecting a difference between the group proportions of 0.5050. The proportion in the control group) was assumed to be 0.1330 under the null hypothesis and 0.6380 under the alternative hypothesis. The proportion in the test group was 0.1330. The test statistic used was the two-sided z-test with unpooled variance. The significance level of the test was 0.0500.
). The independent samples t-test was used for inter-group comparison. The paired sample t-test was used for comparison before and after treatment. The counting data were expressed by rate or constituent ratio (%), and the chi-squared test was used for inter-group comparison (χ2), with the inspection level being α = 0.05. The statistical power was calculated using the PASS 15 software (NCSS, LLC., Kaysville, Utah, USA, ncss.com/software/pass). Group sample sizes of 47 in control group 1 and 45 in test group achieved a 99.995% power, detecting a difference between the group proportions of 0.5050. The proportion in the control group) was assumed to be 0.1330 under the null hypothesis and 0.6380 under the alternative hypothesis. The proportion in the test group was 0.1330. The test statistic used was the two-sided z-test with unpooled variance. The significance level of the test was 0.0500.
Results
A total of 92 participants were enrolled. There was no difference in age, height, weight, atrial fibrillation, oral warfarin, coagulation function and haemoglobin between the test and control groups (Table 1). Figure 1 shows the wound by bevel up (left) and bevel down (right).
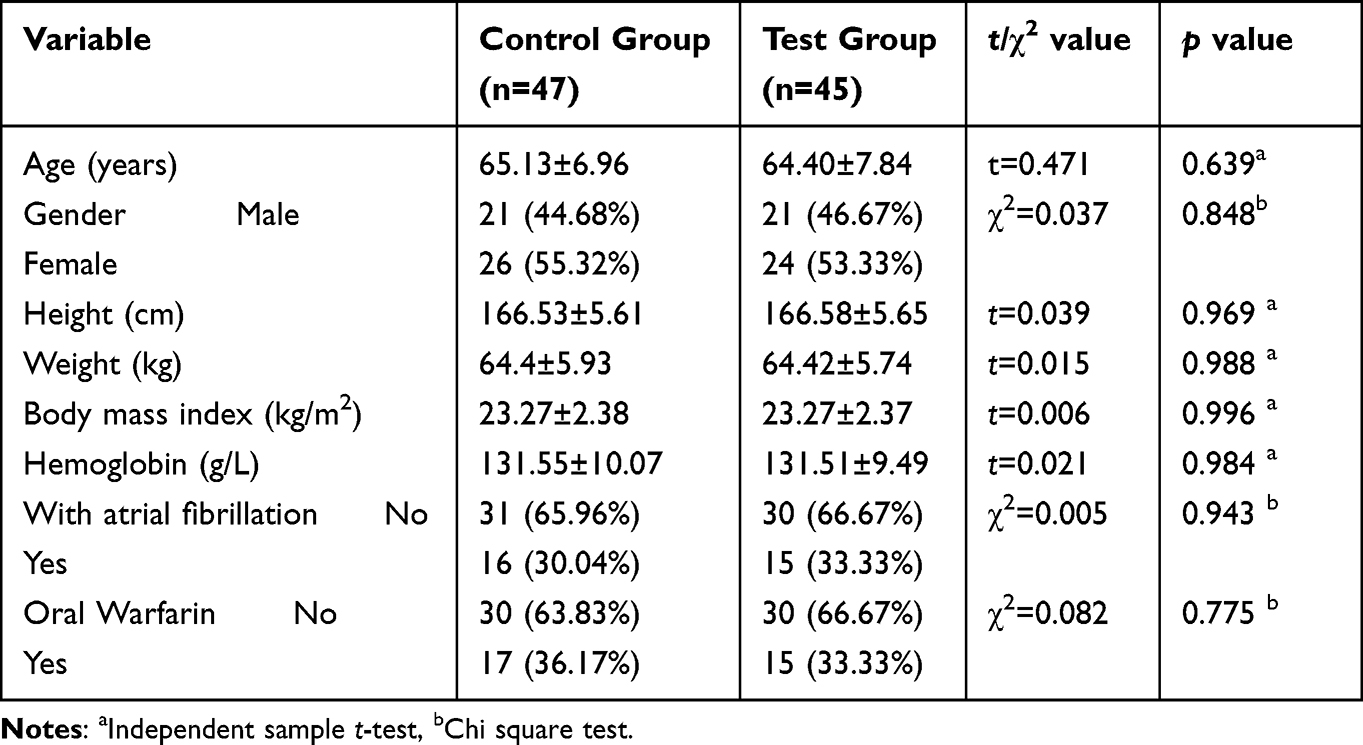 |
Table 1 Comparison of General Baseline Data Between the Two Groups |
 |
Figure 1 Routine blood collection method (bevel up) and optimized needle insertion method (bevel down). (A) Routine blood collection method; (B) Optimized needle insertion method. |
The incidence of blood overflow and the diameter of the bruised area in the control group were higher than in the experimental group (P < 0.001). The incidence of a blood clot was higher than that in the experimental group (P = 0.073), and the incidence of dizziness was similar to that in the experimental group (P = 0.975) (Table 2).
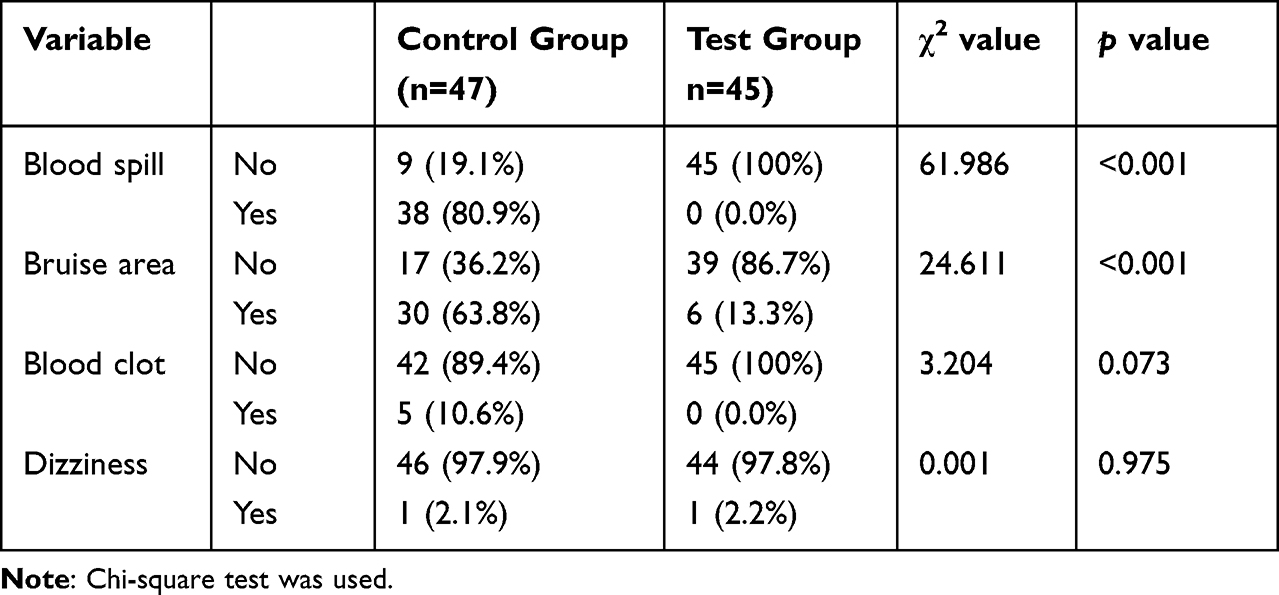 |
Table 2 Comparison of Blood Spill (Cases), Bruise Area (Cases), Blood Clot (Cases), and Dizziness (Cases) Between the Two Groups |
Table 3 shows a comparison of the heart rates and blood pressures of the two groups of patients before and after blood collection. There was no difference in the heart rates and blood pressures between the two groups before and after blood collection (P > 0.05). Intra-group comparison: There was no difference in the heart rates and blood pressures before blood collection in the control group compared with that after blood collection (P > 0.05). There was no difference in heart rate and systolic blood pressure before blood collection (P > 0.05), and the diastolic blood pressure before blood collection was higher than that after blood collection (P > 0.05) (Table 3). The two groups had significant differences in pain scores and blood collection time (Table 4).
 |
Table 3 Comparison of Heart Rate (Times/Min) and Blood Pressure (mmHg) Between the Two Groups Before and After Blood Collection |
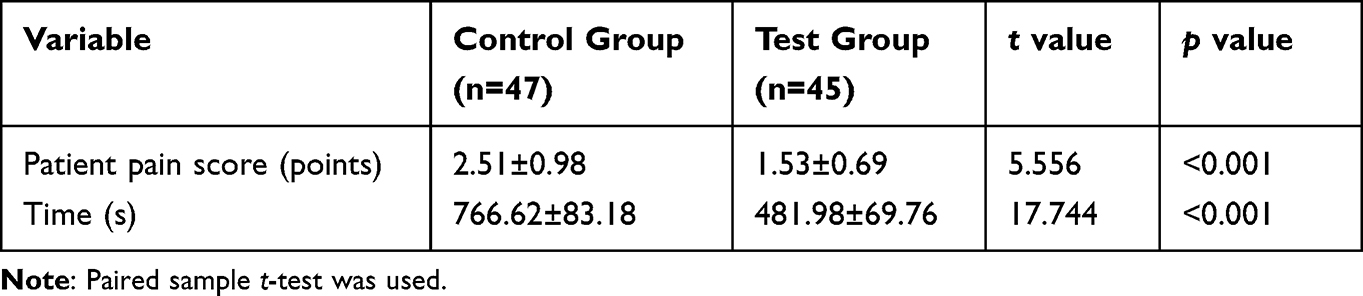 |
Table 4 Comparison of Patient Pain Score (NRS Score: Minutes) and Blood Collection Time (Seconds) Between the Two Groups |
Discussion
The results showed that compared with the control group (bevel up), the test group (bevel down) had lower pain scores, blood collection times and blood spills with similar safety according to the vital signs.
The modified method may be expected to overcome these problems. First, the test group let the wedge-shaped inclined plane of the blood collection needle into the needle parallel to the skin to avoid the possibility of connecting the vascular cavity with the outside world so there would be no blood in the blood collection process. Second, an in vitro simulation test shows that in the conventional blood collection scheme, the skin damage is oval-shaped, while in the improved method, the skin damage appears as a clear arc, which is also confirmed in practice, as Figure 1 shows. Third, in the conventional blood collection method, the wedge-shaped inclined plane of the blood collection needle enters the blood vessel. Then, the pinhole of the blood collection needle into the blood vessel is covered with a sterile dressing. The tail end of the blood collection needle is fixed on the forearm with an adhesive tape with the blood collection needle parallel to the direction of the corresponding blood vessel, resulting in the wedge-shaped inclined plane of the blood collection needle.
The authors’ hospital has carried out pre-deposited autotransfusion for patients undergoing open heart surgery from early stage. In recent years, the use of the optimised needle insertion method during blood collection can ensure that: ① no blood overflows in the process of blood collection; ② there is almost no bruising at the needle entry point after blood collection; ③ the patient complains of only mild pain; ④ the blood collection process is smooth without any blood clots; ⑤ the vital signs are stable; and ⑥ there are no obvious adverse reactions. This method may be of great significance in improving the patient’s blood collection experience, avoiding extravasation of the blood, lessening pain and reducing the incidence of adverse reactions, ensuring blood quality and subsequent blood transfusion safety.
This study’s results showed no blood spill during the needle insertion process in the test group, mainly because the bevel of the blood collection needle was downward and parallel to the skin to avoid the possibility of the vascular cavity communicating with the outside world.10 Twenty-four hours after blood collection in the control group: The enlarged image of the puncture point shows an oval shape with blood clots in the middle. The incidence of bruises was 63.8%. Twenty-four hours after blood collection in the test group: The enlarged image of the puncture point showed a clear arc shape, and the incidence of bruises was 13.3%. Since there was no significant difference in coagulation function between the two groups of patients using the same pressing method, the bruises may be related to blood extravasation caused by the different levels of local tissue damage.11 Also, the severity of the pain patients complained about was consistent with the size of the bruises. The incidence of blood clots in the control group was 10.6%, significantly higher than 0.086% in the normal blood donors.16,17 In the blood collection method of the test group, there was no bevel of the needle head sticking to the blood vessel wall, the blood flow was smooth and there were no blood clots in this group. Before and after blood collection, the diastolic blood pressure in the test group decreased slightly, likely related to the rapid change of blood volume,15,18,19 and other vital signs were stable, with the patients experiencing no discomfort.
There are still some limitations: The sample size is limited. In addition, although the optimised blood collection method has advantages in open heart surgery patients, it is still uncertain whether people who donate blood at blood stations can benefit.
Conclusion
An improved blood collection method (bevel down) can enhance the blood donation experience, avoid blood spillage, lessen pain and reduce adverse reactions. This may be of great significance in ensuring blood quality and the safety of subsequent transfusions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tawfick WA, O’Connor M, Hynes N, Sultan S. Implementation of the Continuous AutoTransfusion System (C.A.T.S) in Open Abdominal Aortic Aneurysm Repair: an Observational Comparative Cohort Study. VASC ENDOVASCULAR SURG. 2008;42(1):32–39. doi:10.1177/1538574407309316
2. Opelz G, Sengar DP, Mickey MR, et al. Effect of blood transfusions on subsequent kidney transplants. Transplant Proc. 1973;5(1):253–259.
3. Li C, Jiang XQ. Research and progress on clinical application of autologous blood transfusion. J Taishan Med College. 2017;4:475–477.
4. Moskowitz DM, McCullough JN, Shander A, et al. The impact of blood conservation on outcomes in cardiac surgery: is it safe and effective? Ann Thoracic Surg. 2010;90(2):451–458. doi:10.1016/j.athoracsur.2010.04.089
5. Ping D, Rongzhi W, Wang JP, Wu R. Application of predeposit autologous blood transfusion in cardiac surgery. Chine J Blood Transfusion. 2007;4:315–316.
6. Huang JF, Zhang XL, Chen BT, Wu YJ. Application of predeposit autologous blood in elderly patients. J Clin Transfusion Lab Med. 2019;5:477–480.
7. Yu SY, Che DQ. Clinical observation of autotransfusion in patients undergoing Rh (d) negative cardiac surgery. J Clin Hematol. 2010;1:114–115.
8. Lin Y. Nursing care of 60 cases of autotransfusion in open heart surgery. J Practical Nursing. 2003;19(6):18.
9. McQuilten ZK, Schembri N, Polizzotto MN, et al. Hospital blood bank information systems accurately reflect patient transfusion: results of a validation study. Transfusion. 2011;51(5):943–948. doi:10.1111/j.1537-2995.2010.02931.x
10. Zheng XP, Huang JH, Huang JJ. Techniques of preventing blood overflow from catheterization of superficial vein. PLA J Nursing. 2010;4:261.
11. Li Y. Nursing research progress of subcutaneous bruising rate caused by intravenous infusion in elderly patients. Med Information. 2018;31:40–41.
12. Liu L, Wang L, Liu YZ. Analysis of blood scrapping of unpaid blood donors. Chine J Blood Transfusion. 2019;32(1):49–52.
13. Ye G, Ren ZF, Wen HR, Jiang ZM. Research progress of perioperative blood pressure target control in adults. Int J Anesthesiology Resuscitation. 2021;42(1):83–87.
14. Fu QH, Zhang XX, Zhang JY. Discussion on the pain reducing skills of venipuncture. Nurs Res. 2009;23(29):2682.
15. Zhang T, Luo JZ, Lin QW, Huang JH, Zhu XM. Investigation on Influencing Factors of unpaid blood donation and blood collection time of mobile blood collection vehicle. Med Information. 2011;9:5729–5730.
16. Fu MW, Wu Y, Li JL. Application of storage autotransfusion in 170 patients undergoing elective surgery. Chine J Blood Transfusion. 2018;31(2):172–175.
17. Virchow R. Gesammalte abhandlungen zur wissenschaftlichen medtzin. Frankfurt: Medinger Sohn&Company; 1856.
18. Ma LJ. A case of severe blood donation reaction caused by fasting blood donation. J Practical Med Technol. 2016;23(2):223–224.
19. Leypoldt JK, Cheung AK, Delmez JA, et al. Relationship between volume status and blood pressure during chronic hemodialysis. Kidney Int. 2002;61(1):266–275. doi:10.1046/j.1523-1755.2002.00099.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.