Back to Journals » Drug Design, Development and Therapy » Volume 18
Optimal Programmed Intermittent Epidural Bolus Interval Timing When Using 10 mL of 0.1% Ropivacaine and 0.5 mcg/mL Sufentanil for Labor Analgesia in Patients Without Breakthrough Pain: A Prospective, Randomized Study
Authors Xu DC, Ying J, Zhao J, Chen XD, Deng GP, Zhao YP, Xiao F ![]()
Received 11 August 2024
Accepted for publication 26 November 2024
Published 3 December 2024 Volume 2024:18 Pages 5563—5571
DOI https://doi.org/10.2147/DDDT.S491054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Ding-Chao Xu,1,* Jun Ying,2,* Jing Zhao,1 Xin-De Chen,1 Guo-Ping Deng,1 Yan-Ping Zhao,3 Fei Xiao3
1Department of Anesthesia, Jiashan First People’s Hospital, Jiaxing City, People’s Republic of China; 2Department of Anesthesia, Jiashan Maternity and Child Care Hospital, Jiaxing City, People’s Republic of China; 3Department of Anesthesia, Jiaxing University Affiliated Women and Children Hospital, Jiaxing City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fei Xiao; Yan-Ping Zhao, Department of Anesthesia, Jiaxing University Affiliated Women and Children Hospital, East Zhonghuang Road, Jiaxing City, People’s Republic of China, Tel +86 573 83963131, Email [email protected]; [email protected]
Background: Interval time, defined as the period of time that effective analgesia can be achieved without the need for patient-controlled epidural analgesia (PCEA), has been investigated as an important parameter for the design of programmed intermittent epidural bolus (PIEB) approaches to labor analgesia. PCEA approaches offer flexibility in the management of labor-related pain while minimizing the risk of patient overdose. Here, the optimal interval between PIEB boluses of 0.1% ropivacaine and 0.5 μg/mL sufentanil was evaluated while using revised criteria to define effective analgesia that allowed for the administration of a rescue PCEA bolus during these intervals.
Methods: Participants were assigned at random to five different groups with PIEB intervals that ranged from 35 to 55 minutes. Labor epidural analgesia was initiated by administering 15mL of 0.1% ropivacaine with 0.5 μg/mL sufentanil over a 2-minute period. Analgesia was considered effective if there was no additional requirement for manual analgesia or an additional PCEA bolus beyond a maximum of one PCEA bolus between intervals during the first stage of labor. Probit regression analyses were used to estimate the effective PIEB intervals that achieved 50% (EI50) and 90% (EI90) success rates in patients.
Results: The final analysis included 142 patients who underwent PIEB for maintaining analgesia during labor. Intervals of 55, 50, 45, 40, and 35 minutes were associated with analgesia efficacy odds of 82.8% (24/29), 86.2% (25/29), 96.3% (26/27), 100% (29/29), and 100% (28/28), respectively. The respective EI50 and EI90 intervals associated with patients not suffering from breakthrough pain were 62.9 (95% CI 57.2– 91.8) and 50.4 (95% CI 45.3– 54.9) minutes.
Conclusion: Under the condition of this study, the optimal PIEB interval for the administration of 10 mL boluses of 0.1% ropivacaine and 0.5 μg/mL sufentanil is approximately 50 minutes.
Keywords: ropivacaine, sufentanil, labor analgesia, epidural
Introduction
As an advanced neuraxial analgesia approach to analgesia during labor, the programmed intermittent epidural bolus (PIEB) technique can achieve prolonged periods of analgesia while reducing the need for epidural medication delivery, reducing the potential for breakthrough pain and motor block, and increasing overall patient satisfaction relative to traditional continuous epidural infusion (CEI).1–6 The quality of analgesia achieved via the PIEB technique is closely tied to parameters including bolus volume, injection speed, and bolus interval timing. In several recent studies, researchers have explored the optimal interval timing for the implementation of the PIEB technique7–10 In all of these studies, the authors defined analgesia as being effective if there was no need for patient-controlled epidural analgesia (PCEA) during the first 6 hours of the initial stage of labor. Using these criteria, the optimal interval time across these studies was consistently found to be approximately 40 minutes. However, PCEA strategies can enable flexible epidural medication delivery and may thus be able to extend this PIEB interval times while improving maternal satisfaction and decreasing the potential for adverse outcomes attributable to shorter PIEB intervals when used for labor analgesia.11
Here, the optimal PIEB interval between 10 mL boluses of 0.1% ropivacaine and 0.5 μg/mL sufentanil was investigated. In contrast with past reports, effective analgesia in this study was defined as allowing for the administration of a single PCEA bolus administration within the defined PIEB interval during the first stage of labor. The study was based on the hypothesis that the use of this alternative definition of effective analgesia would allow for the extension of optimal interval timing relative to prior studies.
Methods
Ethical Oversight
This study was approved by the Ethical Committee of the Jiashan First People’s Hospital (IRB 2023–007, 30 August 2023) and was registered on the Chinese Clinical Trial Register (ChiCTR2400080270) on 25 January 2024 before patient enrollment. All participants provided written informed consent. Patient enrollment was initiated on 1 February 2024. This study was performed according to the principles of the Declaration of Helsinki.
Subjects and Setting
In total, an effort was made to recruit 150 nulliparous parturients undergoing spontaneous labor with regular uterine contractions at intervals of at least 5 minutes requesting neuraxial analgesia who were 18–45 years of age, had singleton pregnancies, had a gestational age of 36–42 weeks, and had an American Society of Anesthesiologists (ASA) Physical Status of grade II. Parturients were excluded if they declined to participate, had any contraindications to epidural analgesia, exhibited hypertension or preeclampsia, were affected by comorbidities including diabetes or gestational diabetes, had a BMI exceeding 40, were unable to tolerate sufentanil or ropivacaine, experienced failed epidural puncture, or underwent intrapartum cesarean delivery.
Study Protocol
A randomized spreadsheet generated in Microsoft Excel (Microsoft, WA, USA) was used to allocate parturients requesting neuraxial analgesia into five different groups in which PIEB administration was performed at intervals of 35, 40, 45, 50, or 55 min, respectively. Random numbers were concealed in opaque numbers envelopes that were opened for each participant who was enrolled in the study. An anesthesia assistant aware of patient group assignments was responsible for setting up the infusion machine (Apon MC ZZB-IV, Jiangsu Apon Medical Technology Co., Ltd., Nantong, China) and preparing the epidural solution (0.1% ropivacaine, 0.5 μg/mL sufentanil). All investigators responsible for managing patient pain and collecting data were blinded to interval timing.
When arriving in the labor room, non-invasive blood pressure, pulse oximetry, electrocardiography, fetal heart rate, and tocodynamometer measurements were performed. Three baseline heart rate and systolic blood pressure (SBP) readings were averaged during uterine contractions. A peripheral venous channel was established in an upper limb, and lactated Ringer’s solution (250 mL, pre-warmed) was infused prior to initiating neuraxial analgesia. Patients were provided with instructions regarding visual analog scale (VAS) use (0: no pain, 100: worst pain imaginable) and the use of the PCEA button.
Three fixed anesthesiologists were responsible for ascertaining the epidural space while patients were in the left lateral position. This used a 17-gauge epidural Tuohy needle, assessing the L3-4 intervertebral space based on the reduction in resistance to saline (< 2 mL), before the cephalad insertion of a 19-gauge flexible wire-reinforced multi-orifice epidural catheter 4–5 cm within the epidural space, using transparent tape to fix the catheter in place. Following the confirmation of the absence of blood or cerebrospinal fluid with gentle aspiration, 3 mL of lidocaine (1.5%) containing epinephrine (15 μg) was administered through the catheter as a test dose.
Labor Epidural Analgesia Initiation
Five minutes after a negative observation for the test dose, an epidural loading dose of 15 mL of 0.1% ropivacaine with 0.5 μg/mL sufentanil was given over a 2-minute period. Patients were asked to report their VAS scores at 30 minutes following the delivery of the loading dose, with a VAS score > 30 prompting the administration of a rescue bolus (10 mL of 1% lidocaine). If pain continued to persist 15 minutes after the rescue bolus, the epidural catheterization was deemed unsuccessful and the case was not included in subsequent analyses. The epidural catheter was then replaced by the observer, with subsequent reformulation of the analgesia strategy at the discretion of the observer.
Labor Epidural Analgesia Maintenance
At 1 hour following the administration of the initial loading dose, a fixed bolus of 10 mL of 0.1% ropivacaine and 0.5 μg/mL sufentanil was given to maintain analgesia. Per the established study protocol, patients were assigned to receive subsequent PIEB boluses at five different intervals: 35, 40, 45, 50, and 55 minutes. If patients felt pain within these PIEB intervals, they were permitted to press the PCEA button for the delivery of a further rescue dose. At 20 minutes following a PCEA dose, a VAS score < 30 was considered indicative of effective labor analgesia, whereas VAS scores above this value prompted the administration of a manual rescue bolus of 10 mL of 0.25% ropivacaine with 100 μg fentanyl, and the analgesia was considered ineffective. If this rescue dose failed, this was deemed a catheter problem and the case was not included in subsequent analyses. The PCEA button was adjusted to administer a 5 mL bolus with a 20-minute lockout interval and a maximum dose of 35 mL/h.
Outcome Assessment
The primary outcome was the number of patients achieving effective labor analgesia, defined as the absence of any need for additional manual analgesia other than a PCEA bolus in the first labor stage within the defined PIEB intervals. A research assistant who was blinded to group assignments was responsible for checking the infusion machine on an hourly basis. Patients who required additional PCEA or a manual bolus were regarded as having ineffective epidural analgesia. In these cases, the study was concluded and all subsequent medical decision-making was at the discretion of attending medical professionals. Secondary study outcomes included the characteristics of epidural block, both motor and sensory, maternal side effects, neonatal outcomes, and patient satisfaction. A cotton ball soaked with alcohol was used to assess the sensory block level, while Bromage scores were used for motor block assessments12 (0 = no motor block; 1 = ability to flex knees; 2 = ability to flex ankles; 3 = complete motor block). Block characteristics were assessed at 30 and 60 min following administration of the loading dose and at 1 h intervals thereafter until completion of the assessment. All patient side effects were recorded, including hypotension (SBP < 90 mmHg or < 80% of baseline; treated with phenylephrine 50 μg), maternal bradycardia (heart rate < 60 beats/min; treated with atropine 0.5 mg), fetal bradycardia (fetal heart rate < 110 bpm), and depression of respiration (oxygen saturation < 90%). Analyzed neonatal outcomes included weight, Apgar scores (1 and 5 min), and umbilical arterial blood gas levels. A verbal numerical rating scale was used for the postpartum assessment of patient satisfaction from 1 (completely unsatisfied) to 5 (completely satisfied).
Power Calculations and Statistical Analyses
The Cochran-Armitage Test was used to conduct sample size calculations in PASS (v 11.0.7; NCSS, LLC, UT, USA). In preliminary analyses of groups of patients with 35, 40, 45, 50, and 55 min PIEB intervals in whom analgesia was effective were 95%, 95%, 90%, 80%, and 60%, respectively. For a power of 90% in detecting a linear trend in the numbers of patients achieving effective analgesia using a continuity-corrected Z-test with a 0.05 significance threshold, 21 patients were determined to be necessary in each group (105 total patients). Given the potential for patient dropout, a total target sample size of 30 was established for each of these groups.
Data distributions were assessed using Kolmogorov–Smirnov tests. Descriptive statistics were used to present demographic data (age, weight, height, gestational age). When normally distributed, data are reported as mean (SD) and analyzed with one-way ANOVAs with post-hoc Bonferroni testing for pairwise comparisons, whereas skewed data were reported as median [range] and compared with the Kruskal–Wallis test with post-hoc Dunn’s testing for pairwise comparisons. For categorical data (ie side effect incidence), the Cochran–Armitage χ2 test for trend was applied. When significant differences were evident in overall tests, χ2 tests were applied for pairwise comparisons. Probit regression was applied for calculation of the median effective time intervals for 50% and 90% effective analgesia (EI50 and EI90, respectively). A two-sided P < 0.05 was considered significant. SPSS 22.0 and GraphPad Prism 5.0 were used for statistical analyses.
Results
In total, 179 parturients were initially recruited and assessed for eligibility, of whom 15 declined to participate and 14 failed to meet the criteria for inclusion due to their classification as ASA Physical Status grade III, twin pregnancy, or being outside the inclusive age range. The remaining 150 parturients who provided written informed consent were separated into five groups, with 8 of these subjects ultimately being excluded from analysis as they were transferred for cesarean delivery. Data from 142 patients were ultimately analyzed. A CONSORT (Consolidated Standards of Reporting Trials) flowchart is presented in Figure 1. The details of the participant demographic information are provided in Table 1.
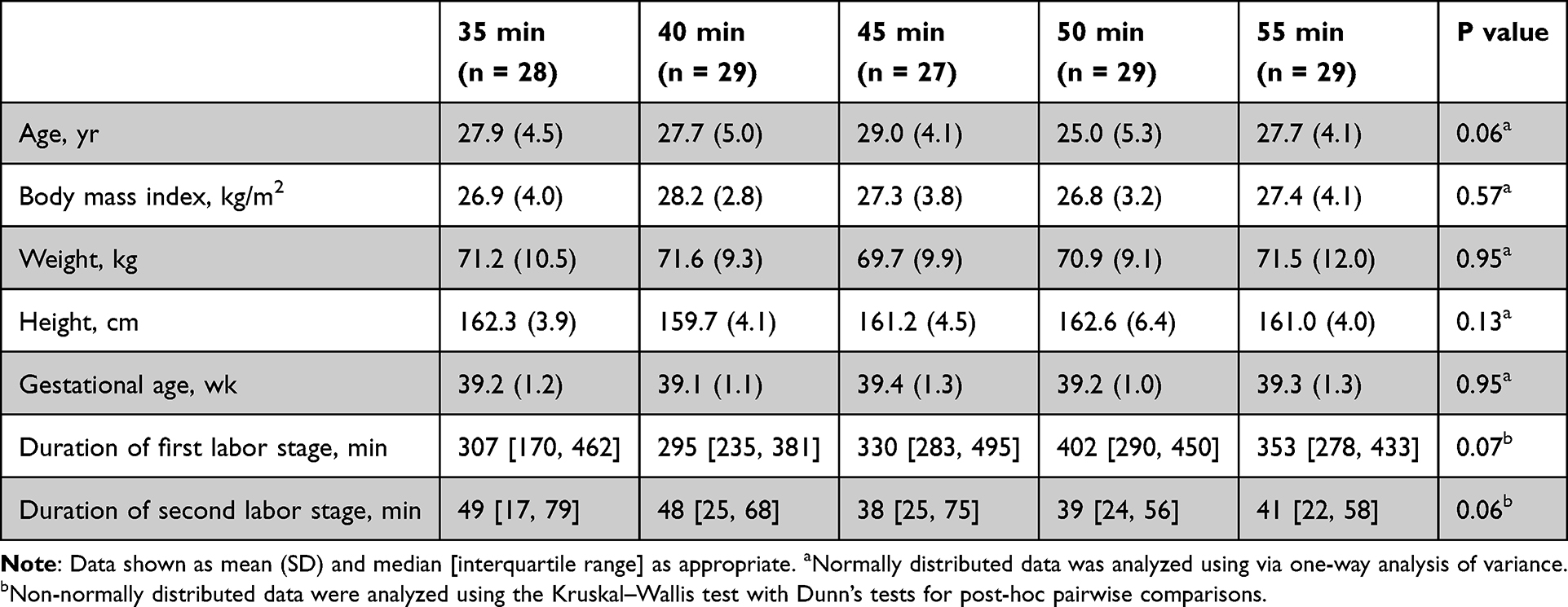 |
Table 1 Demographics and Labor Characteristics |
 |
Figure 1 CONSORT flow diagram. CONSORT, Consolidated Standards of Reporting Trials. |
Of the patients in the 35, 40, 45, 50, and 55 min interval groups, 3 (10.7%), 4 (13.8%), 7 (25.9%), 12 (41.4%), and 15 (51.7%) respectively required at least one PCEA bolus during labor, with a significant linear trend among these groups (P < 0.001). Of patients in the 35, 40, 45, 50, and 55 min interval groups, 0, 0, 1, 4, and 5 patients respectively received a manual bolus within the established interval while in the first labor stage.
The respective odds of effective analgesia in the 55, 50, 45, 40, and 35 min groups were 82.8% (24/29), 86.2% (25/29), 96.3% (26/27), 100% (29/29), and 100% (28/28). The interval response curve for 0.1% ropivacaine and 0.5 μg/mL sufentanil administration using PIEB is shown in Figure 2. The respective EI50 and EI90 intervals associated with 50% and 90% of patients not experiencing breakthrough pain based on established criteria were 62.9 (95% CI 57.2–91.8) and 50.4 (95% CI 45.3–54.9) min. The probit model exhibited good fit using the Pearson goodness-of-fit χ2 test (χ2 = 1.272, P = 0.736).
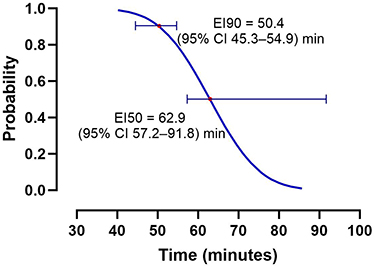 |
Figure 2 Interval time-response curves determined by probit regression. The respective EI50 and EI90 intervals for the absence of breakthrough pain were 62.9 (95% CI 57.2–91.8) and 50.4 (95% CI 45.3–54.9) min. Abbreviations: CI, confidence interval; EI50, effective interval of PIEB in 50% of patients; EI90, effective interval of PIEB in 90% of patients; PIEB, programmed intermittent epidural bolus. |
At 30 min following the initial bolus, sensory block >T10 was achieved in all patients, with significant differences in the sensory block level among groups (P < 0.001). The 35 and 40 min interval groups exhibited a higher dermatome sensory block level relative to the 45, 50, and 55 min interval groups (Figure 3). Of these, three participants in the 35-min group and one in the 40-min group exhibited Bromage scores of 1, with no significant differences among groups. One patient each in the 35 and 45 min groups experienced hypotension and was intravenously administered 50 μg of phenylephrine. The incidence of other side effects was comparable across groups (Table 2). However, patient satisfaction did differ significantly among groups (P = 0.004), with post-hoc testing revealing higher satisfaction in the 35 min group relative to the 55 min group (adjusted P = 0.0025 (Table 2).
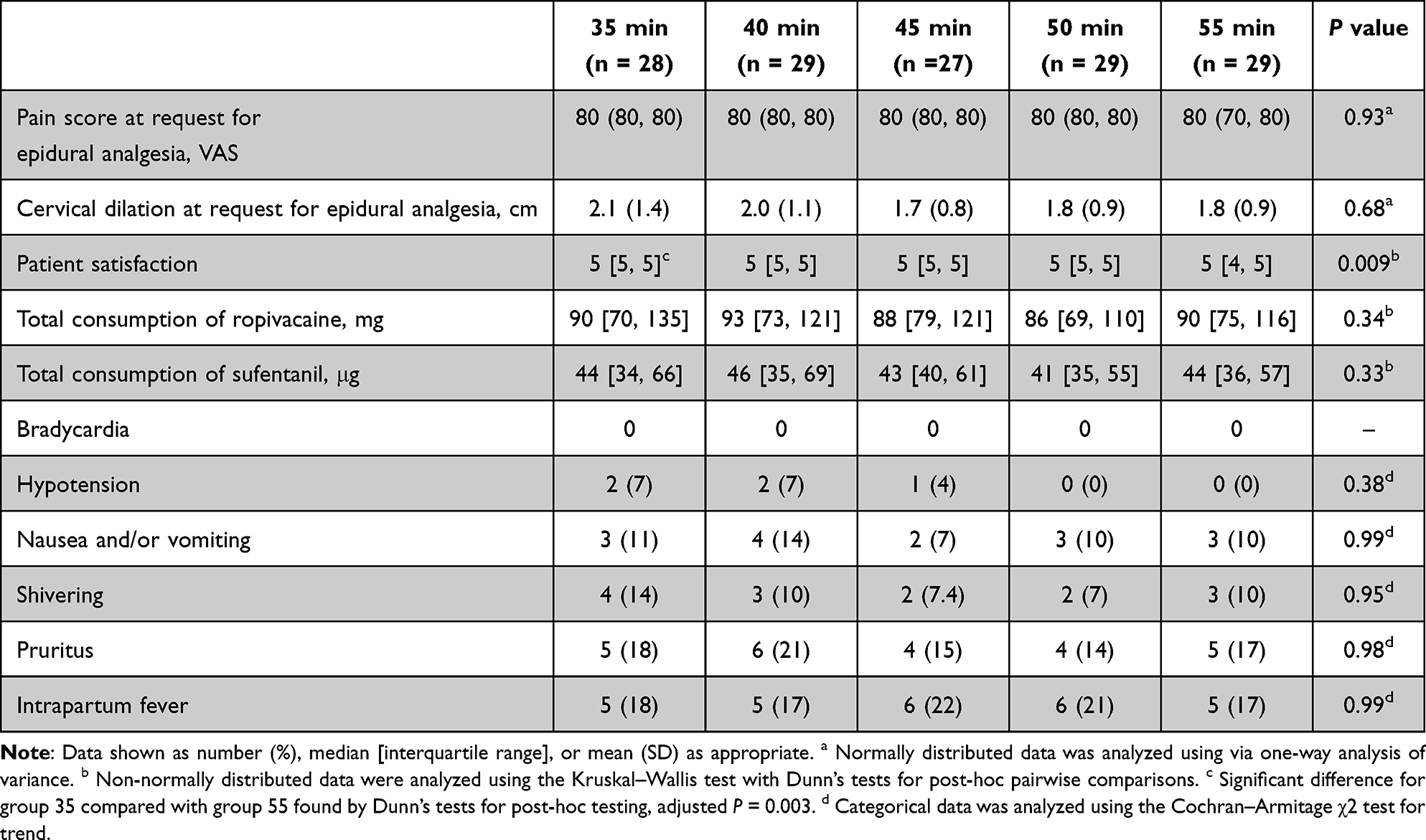 |
Table 2 Characteristics of Analgesia, and Maternal Side Effects |
 |
Figure 3 Maximum levels of sensory block in the different groups. Boxplots represent the median with the 25th and 75th percentiles. The groups were found to differ significantly, as shown by Kruskal Wallis tests (P < 0.0001), with markedly higher sensory blocks in the 35- and 40-min groups relative to the 45-, 50-, and 55-min groups (adjusted P < 0.0001). Abbreviations: PIEB, programmed intermittent epidural bolus. |
The groups did not differ significantly in terms of neonatal weight, 1 min or 5 min Apgar scores, pH levels, or lactic acid levels in umbilical artery blood (Table 3).
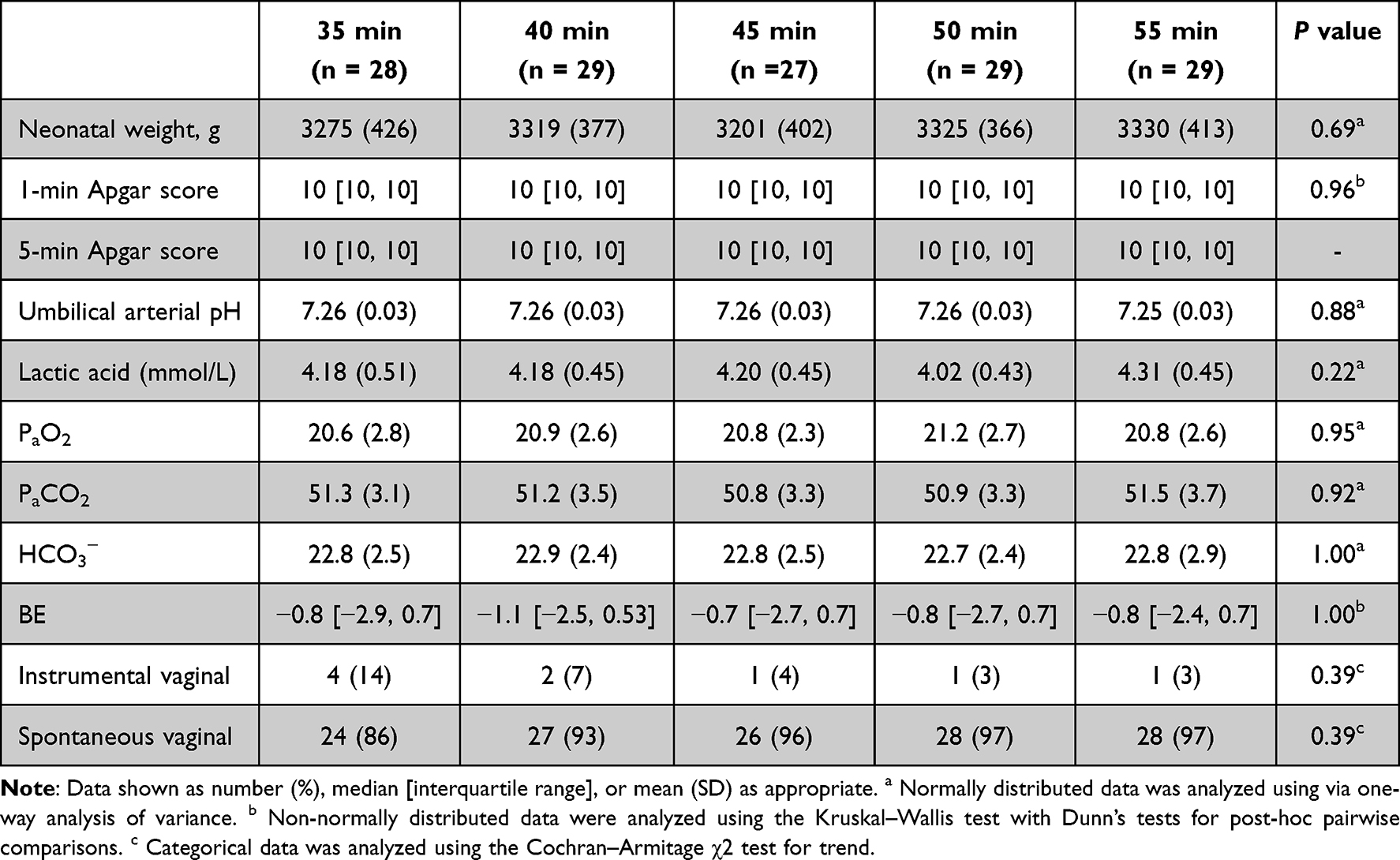 |
Table 3 Neonatal Outcomes and Delivery Model |
Discussion
Here, five different PIEB intervals were compared to determine the optimal timing to maintain epidural analgesia during labor, yielding respective EI50 and EI90 intervals of 62.9 (95% CI 57.2–91.8) and 50.4 (95% CI 45.3–54.9) min. A positive correlation was also detected between shorter PIEB intervals and higher epidural block level. The groups did not differ significantly in terms of either maternal side effects or neonatal outcomes.
In past reports focused on establishing the optimal PIEB interval when maintaining epidural analgesia during labor, the authors universally defined effective analgesia as the absence of any need for additional patient-controlled or manual bolus administration within the first labor stage or within the first 6 hours thereof. Kanczuk et al utilized a biased-coin up-down design and ultimately calculated an optimal interval of 40 min for PIEB administration (10 mL of 0.0625% bupivacaine 0.0625% and 2 μg/mL fentanyl).8 Song et al utilized this same approach with fixed 8 mL boluses of 0.1% ropivacaine and 0.3 μg/mL sufentanil initiated via dural puncture epidural (DPE), leading to the determination of a ~41 minute optimal PIEB interval for labor analgesia.7 Yao et al found that, when using DPE for initiation, the optimal interval for PIEB administration (10 mL of 0.1% ropivacaine and 0.5 μg/mL sufentanil) was approximately 37 minutes.9
Unlike past reports,7–10 the definition of effective analgesia in this study was based on the absence of any requirement for additional manual analgesia with the exception of a PCEA bolus in the first labor stage within the defined PIEB intervals. Based on this definition, the infusion interval estimated to prevent breakthrough pain in 90% of cases was ~50 minutes, which is nearly 10 minutes longer than the optimal intervals reported previously. A key strength of this protocol for labor pain management is that it allows for PCEA treatment, enabling flexible self-adjustment of analgesia. This strategy can help minimize excessive drug administration resulting from a higher frequency of PIEB dosing, as a shorter dosing interval may unnecessarily result in overdose in some cases.
Based on the results of this study, shorter PIEB intervals in the 35–40 minute range are more likely to elicit higher levels of sensory block using the selected testing procedure relative to longer intervals (45–55 minutes). Hypotension was only observed in two patients in the 35 and 40 minute groups, and these patients were treated using phenylephrine (50 μg) without any hypotension-related side effects. Motor blocks were experienced by four patients in the 35 and 40 minute groups, with Bromage scores of 1. Providers monitoring analgesia should be aware that maternal motor block is linked to higher rates of instrumental vaginal delivery and a decrease in overall maternal satisfaction. Striking an appropriate balance between analgesia and the potential for adverse analgesia-related labor outcomes is thus essential. To that end, a random allocation-based dose-finding approach was herein used to clarify the correlative relationship between dosing interval, effective analgesia, and adverse event incidence. The present results suggest that a dosing interval of 50 minutes is the optimal timing for PIEB administration for labor epidural analgesia.
Specific clinical conditions have the potential to shape the PIEB intervals calculated through these optimization strategies, including differences in infusion rates, PIEB volume, and local anesthetic concentrations. Future research will thus be necessary to fully explore the effects of these different parameters in order to provide patients with the best analgesia possible. However, the use of 10 mL boluses of 0.1% ropivacaine mixed with 0.5 μg/mL sufentanil is common in our clinical practice.
Based on the protocol employed in this study, efforts were made to keep parturients and anesthesiologists blinded to the selected intervals. Analgesic device operation, however, may have led to the inadvertent unblinding of group assignments. To maximize the degree of double-blinding, the differences in intervals between neighboring groups were just 5 minutes. Individual patients are also a relatively objective indicator for pain perception such that these results are unlikely to be impacted by awareness of group assignments.
Lastly, this study only focused on women in the first stage of labor after loading dose administration. These findings may not be applicable to the second stage of labor, which may coincide with an increased minimal local analgesic concentration. Additional, caution should be exercised when interpreting the data analysis for the secondary outcomes due to potential limitations in sample size, which may have introduced reporting bias and impeded the detection of statistically significant differences, such as side effects, in this study.
In summary, the optimal PIEB dosing interval for the administration of 10 mL of 0.1% ropivacaine and 0.5 μg/mL sufentanil is roughly 50 minutes under the established experimental conditions. This labor analgesic regimen may help mitigate pain while also minimizing the potential for patient overdose. Future studies employing various drug combinations and PIEB parameters are warranted to build on these results.
Abbreviations
PIEB, programmed intermittent epidural bolus; CEI, continuous epidural infusion; PCEA, patient-controlled epidural analgesia; ASA, American Society of Anesthesiologists; BMI, body mass index; SBP, systolic blood pressure; EI50, median effective time intervals; EI90, 90% effective time intervals.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the privacy policy but are available from the corresponding authors on reasonable requests.
Acknowledgments
The authors thank all the staff at the Department of Laboring Room of Jiashan First People’s Hospital, Jiaxing, China, for their help in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Sia ATH, Lim Y, Ocampo C. Automated regular boluses for epidural analgesia: a comparison with continuous infusion. Int J Obstet Anesth. 2005;14:305–309. doi:10.1016/j.ijoa.2005.05.004
2. Fettes PD, Moore CS, Whiteside JB, McLeod GA, Wildsmith JA. Intermittent vs continuous administration of epidural ropivacaine with fentanyl for analgesia during labour. Br J Anaesth. 2006;97:359–364. doi:10.1093/bja/ael157
3. Wong CA, Ratliff JT, Sullivan JT, Scavone BM, Toledo P, McCarthy RJ. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth Analg. 2006;102:904–909. doi:10.1213/01.ane.0000197778.57615.1a
4. Lim Y, Ocampo C, Sia AT. A comparison of a basal infusion with automated mandatory boluses in parturient controlled epidural analgesia during labor. Anesth Analg. 2007;104:673–678. doi:10.1213/01.ane.0000253236.89376.60
5. Wong CA, McCarthy RJ, Hewlett B. The effect of manipulation of the programmed intermittent bolus time interval and injection volume on total drug use for labor epidural analgesia: a randomized controlled trial. Anesth Analg. 2011;112:904–911. doi:10.1213/ANE.0b013e31820e7c2f
6. Capogna G, Camorcia M, Stirparo S, Farcomeni A, Programmed intermittent epidural bolus versus continuous epidural infusion for labor analgesia: the effects on maternal motor function and labor outcome. A randomized double-blind study in nulliparous women. Anesth Analg. 2011;(113):826–831. doi:10.1213/ANE.0b013e31822827b8
7. Song Y, Du W, Tao Y, et al. Optimum programmed intermittent epidural bolus interval time between 8 mL boluses of Ropivacaine 0.1% with sufentanil 0.3 μg/mL with dural puncture epidural technique for labor analgesia: a biased-coin up-and-down sequential allocation trial. J Clin Anesth. 2022;79:110698. doi:10.1016/j.jclinane.2022.110698
8. Epsztein Kanczuk M, Barrett NM, Arzola C, Downey K, Ye XY, Carvalho JC. Programmed Intermittent Epidural Bolus for Labor Analgesia During First Stage of Labor: a Biased-Coin Up-and-Down Sequential Allocation Trial to Determine the Optimum Interval Time Between Boluses of a Fixed Volume of 10 mL of Bupivacaine 0.0625% With Fentanyl 2 μg/mL. Anesth Analg. 2017;124:537–541. doi:10.1213/ANE.0000000000001655
9. Yao HQ, Huang JY, Deng JL, et al. Randomized Assessment of the Optimal Time Interval Between Programmed Intermittent Epidural Boluses When Combined With the Dural Puncture Epidural Technique for Labor Analgesia. Anesth Analg. 2023;136:532–539. doi:10.1213/ANE.0000000000006201
10. Zhou SQ, Wang J, Du WJ, Song YJ, Xu ZD, Liu ZQ. Optimum interval time of programmed intermittent epidural bolus of ropivacaine 0.08% with sufentanyl 0.3 μg/mL for labor analgesia: a biased-coin up-and-down sequential allocation trial. Chin Med J. 2020;133:517–522. doi:10.1097/CM9.0000000000000669
11. Merrer J, Bonnet MP, Blondel B, et al. Predictors of incomplete maternal satisfaction with neuraxial labor analgesia: a nationwide study. Anaesth Crit Care Pain Med. 2021;40:100939. doi:10.1016/j.accpm.2021.100939
12. Bromage PR. A comparison of the hydrochloride and carbon dioxide salts of lidocaine and prilocaine in epidural analgesia. Acta Anaesthesiol Scand Suppl. 1965;16:55–69. doi:10.1111/j.1399-6576.1965.tb00523.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dural Puncture Epidural with 25-G Spinal Needles versus Conventional Epidural Technique in Conjunction with PIEB for Labor Analgesia: A Randomized Trial
Lin W, Yang Y, Lin J, Chen J, Lin Q
Journal of Pain Research 2023, 16:3797-3805
Published Date: 8 November 2023
Circadian Variation in Ropivacaine Requirement for Initiation of Epidural Labour Analgesia: A Random-Allocation Graded Dose-Response Study
Huang XD, Xiao F, Hu B, Dong XY, Chen XZ
Drug Design, Development and Therapy 2026, 20:573078
Published Date: 10 March 2026