Back to Journals » Infection and Drug Resistance » Volume 16
Optimal Perioperative Antimicrobial Management Strategies of Kidney Transplant Recipients Guided by Metagenomic Next-Generation Sequencing of Deceased Donors’ Microbiology Samples
Authors Rao Z, Wang Z, Tang M, Zhang K
Received 26 June 2023
Accepted for publication 20 September 2023
Published 29 September 2023 Volume 2023:16 Pages 6473—6486
DOI https://doi.org/10.2147/IDR.S427656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Zhengsheng Rao, Zhiling Wang, Ming Tang, Keqin Zhang
Urinary Nephropathy Center, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Keqin Zhang, Email [email protected]
Background: There is no consensus on the optimal use of perioperative antibiotics prophylaxis after kidney transplantation, but there is a common trend to limit the duration of antibiotic use worldwide. Metagenomic next-generation sequencing (mNGS) has emerged as a novel technology for pathogen detection in clinical practice due to its noninvasive, rapid, precise and high susceptibility to detect infectious pathogens. However, data are lacking on whether mNGS analyses could be used to detect pathogens and guide anti-infection regimens in kidney transplant donors and recipients.
Methods: We conducted a retrospective study to review all clinic data of mNGS and traditional laboratory methods (TMs) for pathogen detection in kidney transplant recipients and their corresponding deceased donors from August 1, 2021 to October 30, 2022 in our center.
Results: A total of 57 donors and 112 of their corresponding recipients were included. The antimicrobial strategy mainly depended on mNGS results combined with traditional pathogen culture and clinical conditions. The percentages of positive pathogen detected by mNGS in blood, urine, bronchoalveolar lavage fluid (BALF) and preservation fluids (PFs) were 50.9% (29/57), 35.1% (20/57), 84.2% (48/57) and 54.4% (31/57) respectively, and were 24.6% (14/57), 15.8% (9/57), 57.9% (33/57) and 14.1% (8/57) respectively when using TMs. mNGS could detected all of pathogens which were detected by TMs. However, samples with negative TMs testing can be additionally detected as positive by mNGS (15/43 in blood, 11/48 in urine, 15/24 in BALF and 23/49 in PFs). Drug resistance genes were detected in 9 donors by mNGS,which were consistent with 6 donors by TMs. There was only one case of donor-derived infection in this study.
Conclusion: This study showed that it is effective to combine mNGS with traditional pathogen detection methods and clinical features to develop optimal perioperative antimicrobial management strategies for deceased donor kidney transplantation.
Keywords: kidney transplantation, metagenomic next-generation sequencing, donor-derived infection, perioperative infection, antimicrobial strategy
Introduction
Kidney transplantation is the most effective treatment for individuals with end-stage renal disease.1 Deceased donors in China have increased rapidly since January 2015 because civilian organ donation has been the sole source of organ transplant.2 Marginal donors have increasingly been accepted for transplantation due to the significant disparity between the supply and demand of organs.3 However, most donors experience multiple invasive procedures, use of high-intensity antibiotics and long stays in the intensive care unit (ICU) that increase the risk of donor-derived infections (DDI), including multidrug-resistant (MDR) bacterial infections.4,5 Additionally, the use of high-dose immunosuppressive agents increase the risk of infections for kidney transplant recipients in the early post-transplant period.6,7 Donors with bacteremia or organ infection are often considered contraindications for transplantation in most transplant centers. However, some of the infections can be controlled, which requires us to quickly identify pathogens and actively treat them, thereby we can expand the donor pool.
In general, donors are systematically screened for infectious diseases.8,9 However, the use of organs from infected donors and antimicrobial therapy in recipients remains controversial.10,11 The prophylactic antibiotic treatment for recipients during the perioperative period varies worldwide, and at least a seven-day course of antimicrobial therapy is recommended if the culture of biological specimen from donor is positive.12,13 Nevertheless, high-intensity and prolonged antibiotic use will promote the emergence of MDR bacteria and cause side effects on the other organ systems.14 Thus, the optimal management of antibiotic therapy requires early and precise detection of infectious pathogens in donors.
Conventional laboratory methods, including nucleic acid testing, serology detection and culture of different body fluids and tissues, are time-consuming and may produce false negative results. Metagenomic next-generation sequencing (mNGS) has become an effective approach to detecting infectious diseases.15,16 mNGS can overcome many shortcomings of traditional detection technology and directly detect different microbes from clinical specimens regardless of prior antibiotic exposure and culture.17,18 To date, few studies have reported on the early detection of infectious diseases in kidney transplant recipients, and reports on the use of mNGS to identify potential pathogens in deceased donors to guide perioperative antimicrobial treatment in their corresponding recipients are lacking.19,20
In this study, we proposed a new strategy for optimal perioperative antibiotic use after kidney transplantation. We aim to validate the efficacy of perioperative antibiotic strategy by combining mNGS with traditional laboratory methods (TMs) to detect donor body fluids and preservation fluid (PF).
Materials and Methods
Patients, Perioperative Management
We retrospectively reviewed all first adult HLA and ABO compatible kidney transplant recipients and their corresponding deceased donors between August 1, 2021 and October 30, 2022 in our Hospital. A total of 57 donors and 112 of their corresponding recipients were included. All kidneys were donated voluntarily with written informed consent, and that this was conducted in accordance with the Declaration of Istanbul. All the clinical data of donors and recipients during the hospitalization period were collected.
All the recipients received induction therapy of basiliximab or anti-thymocyte globulin. We used 500 mg intravenous methylprednisolone for three days from the day of the operation. Then, oral prednisone was taken and tapered off to 20 mg once a day in the first month after transplantation. Maintenance immunosuppressive treatment consisted of a triple-drug regimen of mycophenolic acid (MPA), calcineurin inhibitors (CNI) and corticosteroids. After transplantation, all recipients received prophylaxis with trimethoprim-sulfamethoxazole for 6–12 months and valganciclovir or ganciclovir for three months in case of a cytomegalovirus IgG-negative recipient of a cytomegalovirus IgG-positive organ.
The strategy for antibiotic optimization after kidney transplantation during the perioperative period was developed according to the results of mNGS of donors as follows:
“Negative donor” was defined as negative culture results and mNGS of blood, urine, bronchoalveolar lavage fluid (BALF) and preservation fluids (PFs). Then, third-generation cephalosporin was used for 3 days.
“Possible infectious donor” was defined as at least a positive result of culture or mNGS of blood, urine or BALF but with a negative culture or mNGS of PF. Then, the antibiotic targeted to the organism was used for 5–7 days.
“Infectious donor” was defined as the a positive culture or mNGS of PF, and the same organism was isolated from the donors in ICU. Then the targeted antibiotic was used for at least 7–10 days. However, if only the mNGS of PF was positive when previous results of mNGS or culture were negative, we defined it as contamination or colonization. Then the antibiotic strategy was the same as the “Possible infectious donor”, but the antibacterial spectrum can cover the possible organism.
Samples Collection and Processing
The donor’s samples, including blood, urine and BALF, were obtained immediately after hospitalized in our center, and PF was obtained preoperatively. We would conduct the first evaluation after 3–5 days, if the donor’s infection related indicators and symptoms continued to worsen after anti infection based on the mNGS results, or none-infected donors showed signs of infection. In this case, we would repeat the mNGS evaluation for infection and adjust the antibiotics. All the samples were used for culture and mNGS. Microbiological monitoring of the kidney recipients involved the routine sampling of blood, drainage fluid and urine on postoperative days (POD) 1, 4, and 7. The recipient’s samples were just for routine laboratory tests and cultures. When a postoperative infection was suspected, the samples from the blood, drainage fluid, and urine were collected for mNGS. Traditional laboratory testing pathogen detection included: the culture of bacterial and fungal for all specimens; PCR-based assay of Epstein-Barr virus (EBV), Cytomegalovirus (CMV),BK virus,Hepatitis B virus (HBV),and Hepatitis C virus (HCV) in blood; serological assay including 1.3-Beta-D-glucan, Galactomannan antigen,Cryptococcus antigen,Cryptococcus antigen, HBV antigen,HCV and Human immunodeficiency virus (HIV)antibody,CMV and EBV immunoglobulin G/M (IgG/M),Syphilis antibody; and Interferon-gamma release assays for tuberculosis; Smear microscopy for parasitic in stool, blood or BALF.
All samples were stored at 4◦C in sterile containers and immediately sent to Hugo Biotech Co., Ltd., (Beijing, China) to perform mNGS detection. For blood samples, at least five mL of whole blood was centrifuged at 1600g for 10 min, and the supernatant was centrifuged at 16,000g for 10 min to obtain plasma. Other samples, including PF, BALF, urine and drainage fluid, were collected using aseptic techniques. The 1.5-mL microcentrifuge tube with the 0.6-mL sample and 1.0g of 0.5-mm glass beads was attached to a horizontal platform on a vortex mixer and agitated vigorously at 2800–3200 rpm for 30 min.
mNGS and Data Analysis
The DNA in samples was extracted and purified using QIAamp DNA Micro Kit (QIAGEN, Hilden, Germany) according to the manufacturer’s instructions. DNA concentration and quality were checked using Qubit 3.0 Fluorometer (Invitrogen, Q33216) and agarose gel electrophoresis (Major Science, UVC1-1100) according to the manufacturer’s instruction. Then, DNA libraries were constructed through DNA fragmentation, end-repair, adapter ligation and PCR amplification. Qubit 3.0 Fluorometer (Invitrogen, Q33216) and Agilent 2100 Bioanalyzer (Agilent Technologies, Palo Alto, USA) were used for quality control of the DNA libraries. Finally, quality-qualified DNA libraries were sequenced on the Illumina NextSeq 550 sequencing platform (Illumina, San Diego, USA) and a SE75bp sequencing strategy according to the manufacturer’s instructions.
High-quality effective sequencing data were obtained by filtering out connectors, low-quality, low-complexity and shorter sequences. Then, human-derived sequences were removed by mapping to the human reference genome (GRCh38. p13) using BWA (Burrows Wheeler alignment). The remaining sequencing data were classified by simultaneous alignment to the reference database [NCBI database and GenBank], which covers more than 30,000 microorganisms, including 17,748 species of bacteria, 11,058 species of viruses, 1134 species of fungi and 308 species of parasites. The positive criteria for the mNGS result were determined as follows: (1) For bacteria other than TB, fungi other than Cryptococcus and parasites, sequencing coverage in the top 10 of all pathogens were detected and not detected in the negative control (NTC), or the RPM (reads per million mapped reads) ratio of the sample/NTC greater than 10; (2) For viruses, tuberculosis and cryptococci, at least one specific sequence was detected and not detected in the NTC, or the RPM ratio of the sample/NTC was greater than five.
Statistical Analysis
Descriptive statistics were computed for the overall sample and stratified by the presence of positive pathogen detected by mNGS or positive bacterial culture on samples. Mean ± standard deviation (SD) or median was used for describing the continuous variables. The performance of mNGS and TMs for diagnostic assessments was compared using the X2 test. A two-tailed value of 0.05 was considered statistically significant. Data were analyzed using SPSS, version 26.0 (SPSS, Chicago, IL, USA).
Results
Clinical Characteristics of Recipient
A total of 112 recipients were consecutively included in this study, and their demographic characteristics are presented in Table 1. The median age of patients was 39.5 years (range: 18–71), and most recipients were male (73/112, 65.2%). Hemodialysis was the choice for most patients before transplantation (82/112, 73.2%). The average duration of dialysis was 846 days (range: 20–3659). Most patients with end-stage renal disease had an unknown cause (56/112, 50%). Basiliximab was used as induction therapy in immunologically low-risk patients (101/112, 90.2%). The mean length of hospital stay was 11.1 days (range: 8–35). Delayed graft function (DGF) occurred in 12 recipients and biopsy-proven acute rejection in five patients in the first month. The average cold ischemia and operation times were 3.2 h and 185 minutes, respectively. The mean indwelling times for urinary catheters, double-J ureteral stents and central venous catheters were 8.5, 19.8 and 4.7 days, respectively. Hypothermic machine perfusion was used in 54 kidneys, and the mean perfusion time was 2.5 h (range: 1.3–15).
 |
Table 1 Recipient Characteristics (N=112) |
Donor Characteristics
Demographic features of the donors in the study are provided in Table 2. The average age of donors was 45.7 years (range: 4–67), and most were male (48/57, 84.2%). The median length of stay in the ICU was 10.9 days (range: 2–127). The main causes of death were cerebral hemorrhage and trauma (47/57, 82.5%), and brain death was the most common type of death (37/57, 64.9%). Combined abdominal organ procurement was applied to all donors, and digestive wounds during procurement occurred in two cases.
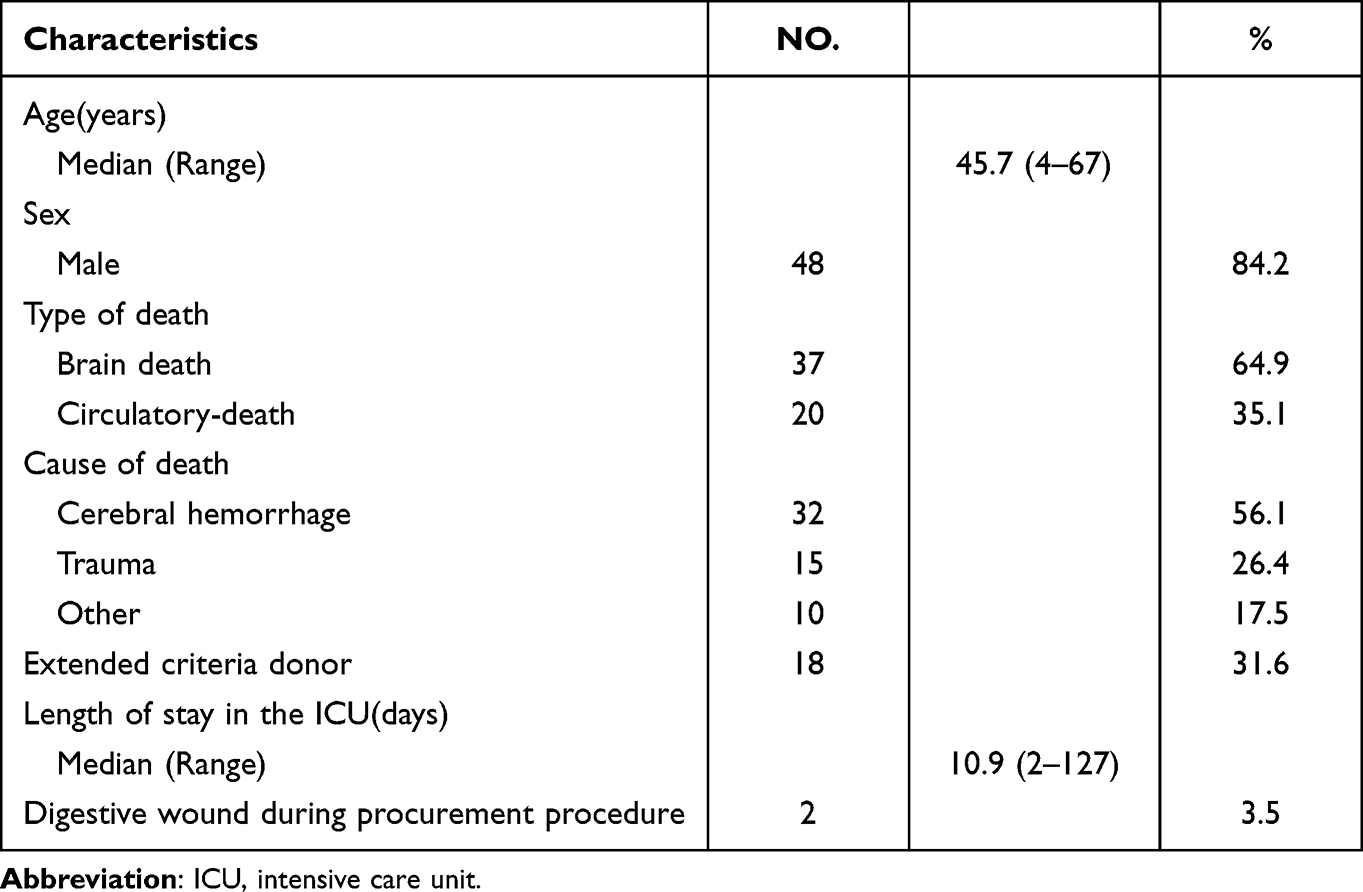 |
Table 2 Characteristics of Donors (N=57) and Procurement |
The Spectrum of Pathogens in Donors
The pathogen-positive percentage detected separately by mNGS and TMs in donors is shown in Figure 1. The percentage of donors with mNGS-positive pathogen results was significantly higher than when using TMs in different samples. The percentages of positive pathogens detected by mNGS in blood, urine, BALF and PFs were 50.9% (29/57), 35.1% (20/57), 84.2% (48/57) and 54.4% (31/57), respectively, and which were 24.6% (14/57), 15.8% (9/57), 57.9% (33/57) and 14.1% (8/57) respectively when using TMs (Figure 1A). The percentage of co-infection of several pathogens, detected by mNGS in blood, urine, BALF and PFs were 17.5% (10/57), 22.8% (13/57), 66.7% (38/57), 17.5% (10/57),and which were 3.5% (2/57), 5.3% (3/57), 8.8% (5/57), 0.0% (0/57) respectively when using TMs (Figure 1B). For samples that were positive by TMs, the mNGS results were consistent and additional pathogens could be detected. mNGS could detected all of pathogens which were detected by TMs. However, samples with negative TMs testing can be additionally detected as positive by mNGS (15/43 in blood, 11/48 in urine, 15/24 in BALF and 23/49 in PFs). mNGS detected 21 pathogens in the blood of 29 donors (bacteria: 61.9%, 13/21; viruses: 28.6%, 6/21; fungi: 9.5%, 2/21), whereas only 10 pathogens were identified using TMs (bacteria: 80.0%%, 8/10; fungi: 20.0%, 2/10),and the frequency of each pathogen is shown in Figure 2A. No parasites were identified in different samples. Other pathogens detected by mNGS or TMs and their frequency are shown in Figures 2B–D. About 22 categories of pathogens were detected in different samples. Candida and aspergillus were the most frequent fungi found by mNGS. The rate of positive fungi was high in urine (7/57), PFs (8/57) and BALF (8/57) and low in blood (3/57). Different types of human herpes virus were detected in different specimens, and human polyomavirus and torque teno virus were the other two common viruses. Meanwhile, over ten types of bacteria were detected by mNGS in various specimen, and common bacteria such as Klebsiella pneumoniae, Acinetobacter baumannii, Escherichia coli and staphylococcus were the main cause of infection of donors in the ICU (Figure 2). In general, the pathogen detection rate of the traditional methods is significantly lower than that of mNGS, regardless of the samples. In our study, the virus was difficult to detect by traditional methods.
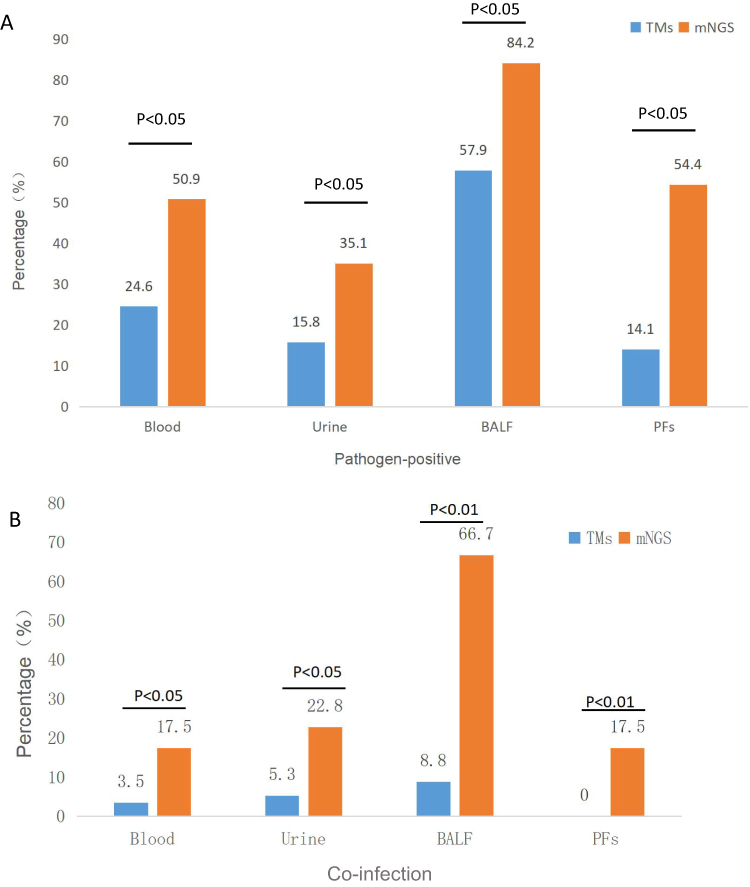 |
Figure 1 The comparison of pathogen-positive percentage (A) and co-infection rate (B) of different specimens detected by mNGS and TMs in donors. mNGS for metagenomic next-generation sequencing, TMs for traditional laboratory methods, BALF for bronchoalveolar lavage fluid and PFs for preservation fluids. |
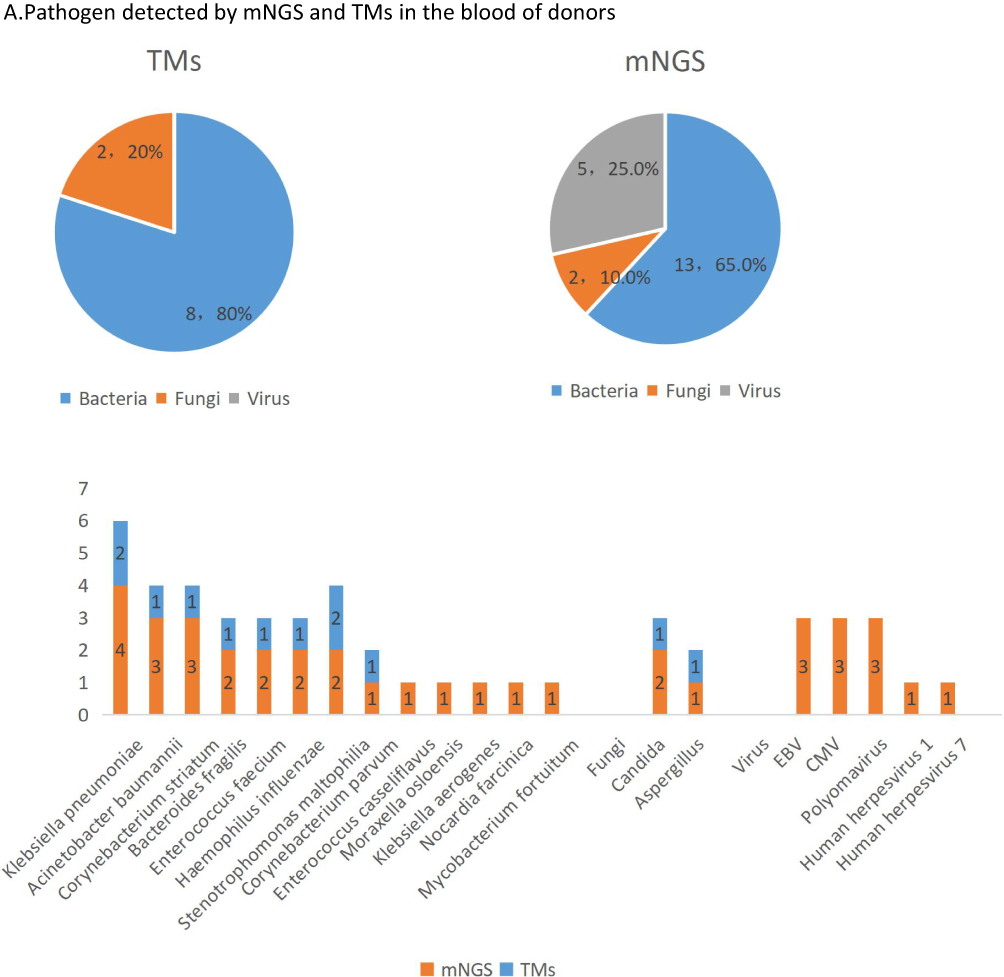 |
Figure 2 Continued. |
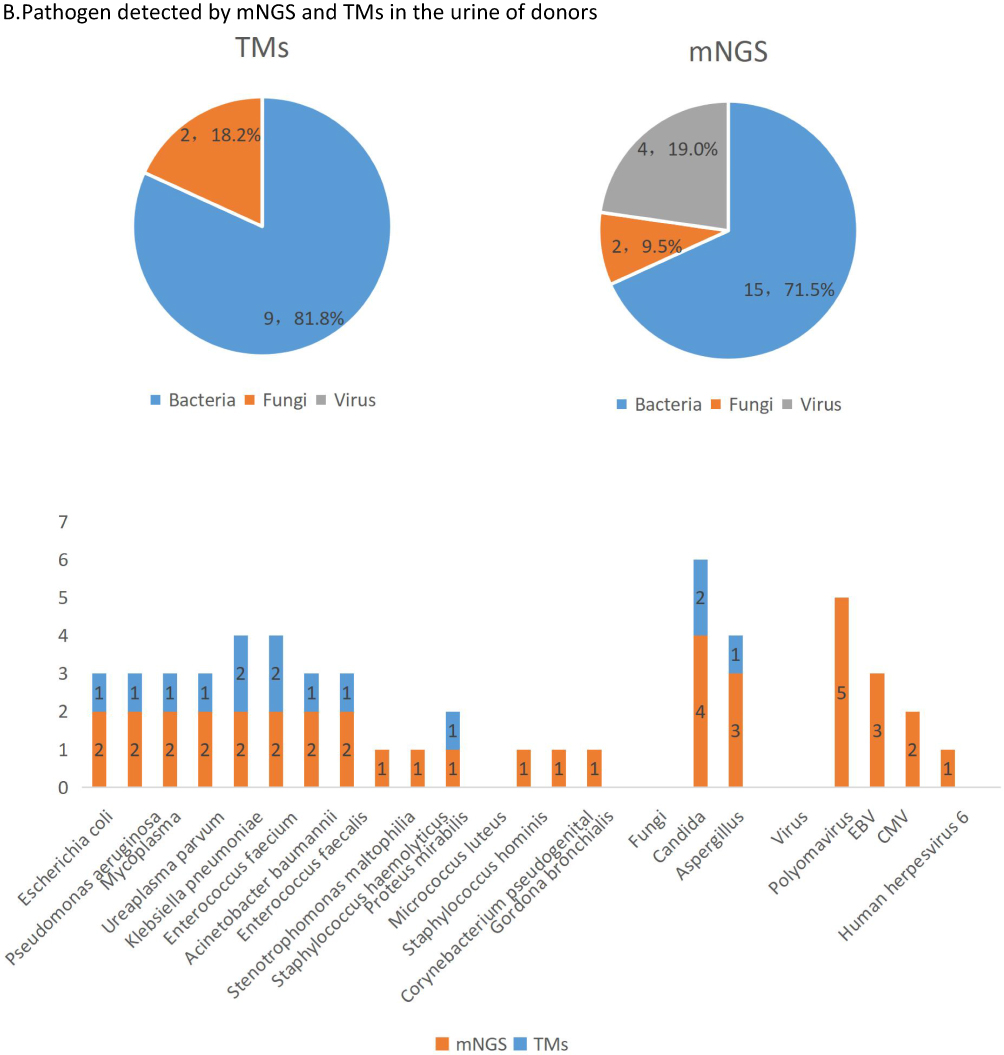 |
Figure 2 Continued. |
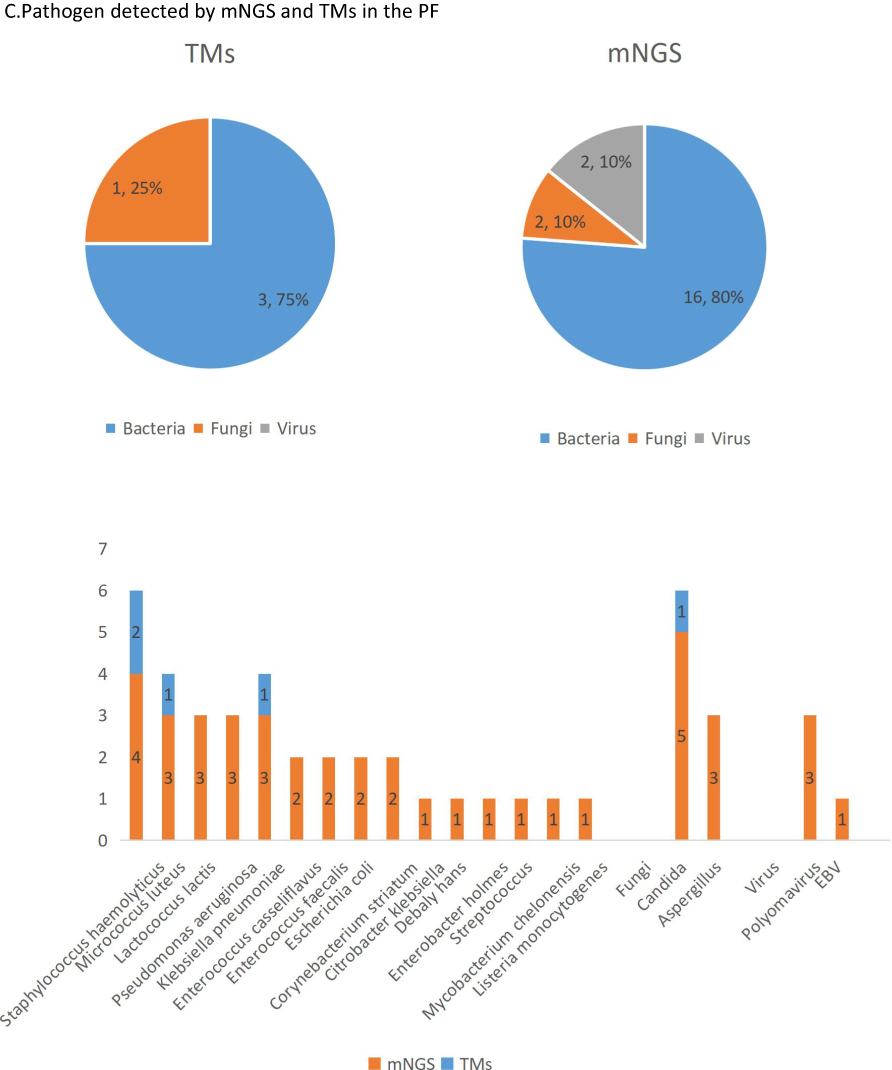 |
Figure 2 Continued. |
 |
Figure 2 The pathogen spectrum in donors detected by mNGS and TMs. (A) Pie chart demonstrating the distribution of different types of pathogens detected by mNGS and TMs in blood of donors, and a total of 20 species of pathogens were detected in blood samples with their corresponding frequencies plotted in histograms. (B) Pie chart demonstrating the distribution of different types of pathogens detected by mNGS and TMs in urine of donors, and a total of 21 species of pathogens were detected in urine samples with their corresponding frequencies plotted in histograms. (C) Pie chart demonstrating the distribution of different types of pathogens detected by mNGS and TMs in PFs of donors, and a total of 20 species of pathogens were detected in PF samples with their corresponding frequencies plotted in histograms. (D) Pie chart demonstrating the distribution of different types of pathogens detected by mNGS and TMs in BALF of donors, and a total of 21 species of pathogens were detected in BALF samples with their corresponding frequencies plotted in histograms. |
The Drug Resistance Gene Detected by mNGS
Another advantage of mNGS is that it can detect drug resistance genes while detecting pathogens, which can guide the possible drug resistance information of pathogens in advance and use appropriate antibiotics in a timely manner compared with traditional methods. However, whether the detection results of drug resistance genes are consistent with clinical practice needs more verification. In our study, resistance genes were detected in 9 donors by mNGS (Table 3). These pathogenic bacteria carrying drug-resistant genes were mainly detected in BALF and urine, and no drug-resistant gene-related pathogens were detected in blood and preservation fluid. Several common drug-resistant pathogens are still Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterococcus faecium. Tet and Erm are the two most common resistance genes among these pathogens. However, these drug resistance speculations based on mNGS results are not completely consistent with the results of drug susceptibility tests after actual bacterial culture. The drug resistance results data by mNGS are consistent with TMs in 6 out of 9 donors.
 |
Table 3 The Drug Resistance Gene Detected by mNGS |
The Antibiotic Strategies in the Donors and Recipients and Donor-Derived Infections
We usually choose one antibiotic for treating the infection of donors according to the spectrum of bacteria in the ICU of our Hospital. The antibiotic may be changed according to the results of mNGS and drug susceptibility analysis. Of the donors in our study, 43.9% (25/57) used β-lactamase inhibitor (for example, cefoperazone and piperacillin) as the only antibiotic, 35.1% (20/57) received combined carbapenems (Imipenem or meropenem) and some other anti-fungal drugs like caspofungin and voriconazole. Additional antibiotics, such as linezolid, vancomycin, tigecycline and ceftazidime/avibactam, were added to the therapy for gram-positive or drug-resistant bacteria in the other 21.1% (12/57) of donors.
The initial antibiotic regimen was made according to the results of pathogens detected by mNGS and drug susceptibility analysis. The drainage fluid and urine of recipients were sent to pathogen culture for three consecutive postoperative days. If no pathogen was detected in the donor, third-generation cephalosporin was used as the basic antibiotic regimen for 3–5 days, according to the patient’s clinical indications. Among the recipients in this study, 27.7% (31/112) used cefoperazone/sulbactam as the only antibiotic. Anti-fungal drugs were used in accordance with pathogen detection reports from pathogen culture and mNGS of donors. A total of 53.6% (60/112) of the recipients used caspofungin or posaconazole for prophylaxis of donor-derived fungal infection. Carbapenem antibiotics such as imipenem/cilastatin were used in 43.8% (49/112). More than two kinds of antibiotics were taken in 21.4% (24/112) of patients, and the additional antibiotics such as tigecycline, linezolid or ceftazidime/avibactam were mainly targeted at gram-positive bacteria and drug-resistant bacteria.
Surgical site infection occurred in one patient caused by MDR mycoplasma(ureaplasma) derived from the donor, although prophylactic minocycline was used. Readmission occurred in three patients due to urosepsis caused by Escherichia coli, detected by mNGS in the blood and urine culture during the first month post-transplantation. No other donor-derived infection occurred among recipients.
Discussion
Infectious complications have become the leading cause of morbidity and mortality in the early post-transplant period for kidney transplant recipients, and it is reported that 40–80% of kidney recipients experience infectious complications after kidney transplantation.21 The use of antibiotics combinations to prevent infections in kidney transplant patients is controversial. Infections from MDR bacteria due to the use of high-intensity antibiotics have continued to increase globally, especially carbapenem-resistant Klebsiella pneumoniae (CRKP).22 In this study, we proposed a new perioperative antimicrobial strategy in the early stage after renal transplantation depending on the pathogenic results of different clinical samples of deceased donors detected by mNGS. We reduced the risk of infection of recipients by early and accurate identification of pathogens from donors so that the targeted antibiotic in recipients could be more effective. Our study confirmed that this strategy may be effectively to reduce DDIs.
The selection and treatment of organs from infected donors are controversial, despite the widening gap between the supply of organs and the number of recipients awaiting transplant.10,23 In this study, we screened all the possible pathogens from multiple clinical samples of donors using mNGS, and targeted antimicrobial therapy was administered promptly. The results of pathogen cultures of donors using TMs could guide the adjustment of antibiotics. Thus, no organ was discarded due to the infectious donors. Due to differences in donor selection criteria among different centers, the reported incidence of DDI varies, ranging from 1–3%.24,25 Only one (1/112, 0.9%) DDI incident occurred in this study.
Due to the critical condition of the donors, we usually do not have enough time for anti-infective treatment. The average feedback time of traditional pathogen culture is ≥3 days for bacteria and seven days for fungi, and some atypical pathogens cannot be detected.17 mNGS can detect more than one pathogen in a single test within 24 h, and the results are less affected by prior antibiotic exposure.26 As positive results of mNGS analyses are comprehensive, including bacteria, fungi and viruses, the presence of co-infection should be excluded. A previous study suggested that common bacterium-associated co-infection should combine mNGS with traditional pathogen culture to distinguish the causative pathogens.27 According to our data, positive results of common bacterium-associated infection using mNGS were consistent with those from TMs 100% of the time. However, we found that candida, which was the most common fungal infection, was detected by mNGS in 14% (8/57) and 7% (4/57) by TMs, respectively. Thus, the results of mNGS could help clinicians hasten clinical decision-making to reduce the risk of DDIs.
The results of pathogen detection in PFs are important evidence for prophylactic use of antibiotics in kidney transplant recipients. A nationwide retrospective observational study reported that the positive rates of PF culture were 24% and 1.8% in deceased and living donors, respectively.28 We found that 14.1% of deceased-donor PFs cultures were positive using TMs, which can increase to 54.4% when using mNGS. Aspergillus was always detected using mNGS when continuous hypothermic machine perfusion (Lifeport and Kidney Preservation Solution-1, Organ Recovery Systems, US) was used to preserve renal grafts, which was confirmed to be due to aspergillus fermentation in the perfusate production process. Thus, prophylactic anti-fungal agents were used in 53.6% of recipients until the results of traditional pathogen culture in this situation were negative. PFs contamination during procurement seemed to be the major cause of the high positive rate and multiple pathogens identified by mNGS. Another nationwide survey of prescription practices in case of positive cultures of kidney transplant preservation fluid suggested that the duration of treatment for bacteria (such as Pseudomonas aeruginosa and Klebsiella pneumoniae) and fungus was seven and 21 days, respectively.29 In this study, the primary antibiotic strategy was based on the results of mNGS in donors, and adjustment was made according to the results of traditional pathogen culture in PF and drainage of recipients. A study of a brief survey among the Eurotransplant renal transplantation centers revealed that a single shot of perioperative antibiotic prophylaxis after kidney transplantation was effective in 44.6% (29/65) of centers.30 However, one-shot antibiotic prophylaxis was not enough to prevent DDIs in the case of an infectious donor from our experience.
In addition to detecting multiple pathogens at the same time, mNGS can also detect drug resistance genes. In our study, drug resistance genes were detected in the BALF and urine of 9 donors. Our choice of antibiotics for initial treatment also takes into account this result. However, this is not consistent with the results of traditionally cultured. It is traditionally believed that drug resistance genes and drug resistance phenotypes are not completely consistent. The results of drug resistance gene detection still need to be combined with traditional culture and drug sensitivity test to formulate an anti-infection plan more accurately. These detected drug-resistant bacteria were not completely consistent with the routine detection of drug-resistant bacteria in our hospital’s ICU, as the hospitalization time and course of these donors were shorter than that of ordinary patients in our hospital’s ICU, and these donors were managed in independent isolation units in the ICU. In addition, mNGS test results do not fully distinguish between active infection, colonization and contamination. Therefore, it is still necessary to combine TMs to further identify. However, the high detection cost of mNGS may be an obstacle to its further promotion. The cost of each detection is as high as 3000 yuan in our center, while the TMs only needs about 300 yuan.
There were some limitations to our study. First, the number of cases in this study is small (only including 57 donors and 112 recipients). Larger prospective studies are needed to confirm the validity of such perioperative antibiotic strategy. Second, mNGS analysis of recipients’ samples was not enough to verify the morbidity of DDIs. Additionally, RNA-Seq data was not concomitantly tested with DNA sequencing in our study, which might give meaningful complementary information such as RNA virus. Finally, due to a lack of a standardized protocol and potential nucleic acid contamination during mNGS, mNGS results directly from clinical samples should be interpreted with care.
Our study showed that it may be effective to combine mNGS with traditional pathogen detection methods and clinical features to develop optimal perioperative antimicrobial management strategies for deceased donor kidney transplantation. The positive results of PF using mNGS should be carefully interpreted based on traditional pathogen culture. Large-scale multicenter randomized controlled studies are warranted to confirm the value of mNGS in routine clinical practice of donors and patients undergoing kidney transplants.
Data Sharing Statement
The raw data supporting the conclusions of this article will be available from the corresponding author on reasonable request.
Ethics Statements
This study was conducted in accordance with the Declaration of Helsinki. All organs were donated voluntarily with written informed consent, and that this was conducted in accordance with the Declaration of Istanbul. The study received ethical approval from The Ethical Review Committee of The Second Affiliated Hospital of Chongqing Medical University. The requirement of informed consent from patients including the review of their medical records was waived by the Committee, the reasons consisted of (1) any identifying information of human participants were anonymous and had no commercial interests, (2) the patients may suffer almost no risk from this study, (3) the study had no negative influence on rights and interests of the patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–1730. doi:10.1056/NEJM199912023412303
2. Huang J, Millis JM, Mao Y, et al. Voluntary organ donation system adapted to Chinese cultural values and social reality. Liver Transpl. 2015;21(4):419–422. doi:10.1002/lt.24069
3. Matas AJ, Payne WD. Transplantation: increasing the use of available deceased donor kidneys. Nat Rev Urol. 2016;13(9):500–501. doi:10.1038/nrurol.2016.135
4. Bonten M, Johnson JR, van den Biggelaar A, et al. Epidemiology of Escherichia coli bacteremia: a systematic literature review. Clin Infect Dis. 2021;72(7):1211–1219. doi:10.1093/cid/ciaa210
5. Wang Y, Tian GB, Zhang R, et al. Prevalence, risk factors, outcomes, and molecular epidemiology of mcr-1-positive Enterobacteriaceae in patients and healthy adults from China: an epidemiological and clinical study. Lancet Infect Dis. 2017;17(4):390–399. doi:10.1016/S1473-3099(16)30527-8
6. Kinnunen S, Karhapää P, Juutilainen A, et al. Secular trends in infection-related mortality after kidney transplantation. Clin J Am Soc Nephro. 2018;13(5):755–762. doi:10.2215/CJN.11511017
7. Fishman JA. Infection in organ transplantation. Am J Transplant. 2017;17(4):856–879. doi:10.1111/ajt.14208
8. Fishman JA, Grossi PA. Donor-derived infection—the challenge for transplant safety. Nat Rev Nephrol. 2014;10(11):663–672. doi:10.1038/nrneph
9. Fischer SA, Lu K. Screening of donor and recipient in solid organ transplantation. Am J Transplant. 2013;13(Suppl 4):9–21. doi:10.1111/ajt.12094
10. Anesi JA, Han JH, Lautenbach E, et al. Impact of deceased donor multidrug-resistant bacterial organisms on organ utilization. Am J Transplant. 2020;20(9):2559–2566. doi:10.1111/ajt.15830
11. Mularoni A, Bertani A, Vizzini G, et al. Outcome of transplantation using organs from donors infected or colonized with carbapenem-resistant gram-negative bacteria. Am J Transplant. 2015;15(10):2674–2682. doi:10.1111/ajt.13317
12. Wolfe CR, Ison MG. Donor-derived infections: guidelines from the American society of transplantation infectious diseases community of practice. Clin Transplant. 2019;33(9):e13547. doi:10.1111/ctr.13547
13. Len O, Garzoni C, Lumbreras C, et al. Recommendations for screening of donor and recipient prior to solid organ transplantation and to minimize transmission of donor-derived infections. Clin Microbiol Infec. 2014;20(7):10–18. doi:10.1111/1469-0691.12557
14. Anesi JA, Blumberg EA, Han JH, et al. Risk factors for multidrug-resistant organisms among deceased organ donors. Am J Transplant. 2019;19(9):2468–2478. doi:10.1111/ajt.15488
15. Duan H, Li X, Mei A, et al. The diagnostic value of metagenomic next-generation sequencing in infectious diseases. BMC Infect Dis. 2021;21(1):62. doi:10.1186/s12879-020-05746-5
16. Li Y, Sun B, Tang X, et al. Application of metagenomic next-generation sequencing for bronchoalveolar lavage diagnostics in critically ill patients. Eur J Clin Microbiol Infect Dis. 2020;39(2):369–374. doi:10.1007/s10096-019-03734-5
17. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788. doi:10.1093/cid/cix881
18. Huang ZD, Zhang ZJ, Yang B, et al. Pathogenic detection by metagenomic next-generation sequencing in osteoarticular infections. Front Cell Infect Microbiol. 2020;10:471. doi:10.3389/fcimb.2020.00471
19. Duan W, Yang Y, Zhao J, et al. Application of metagenomic next-generation sequencing in the diagnosis and treatment of recurrent urinary tract infection in kidney transplant recipients. Front Public Health. 2022;22(10):901549. doi:10.3389/fpubh.2022.901549
20. Al-Heeti O, En Ling W, Ison MG, et al. Transfusion-transmitted Cache Valley virus infection in a kidney transplant recipient with meningoencephalitis. Clin Infect Dis. 2022;76(3):e1320–e1327. doi:10.1093/cid/ciac566
21. Graversen ME, Dalgaard LS, Jensen-Fangel S, et al. Risk and outcome of pyelonephritis among renal transplant recipients. BMC Infect Dis. 2016;16:264. doi:10.1186/s12879-016-1608-x
22. Errico G, Gagliotti C, Monaco M, et al. Colonization and infection due to carbapenemase-producing Enterobacteriaceae in liver and lung transplant recipients and donor-derived transmission: a prospective cohort study conducted in Italy. Clin Microbiol Infec. 2019;25(2):203–209. doi:10.1016/j.cmi.2018.05.003
23. Tong LI, Hu XG, Huang FA, et al. Clinical impacts and outcomes with possible donor-derived infection in infected donor liver transplantation: a single-center retrospective study in China. J Infect Dis. 2020;221(Suppl 2):S164–S173. doi:10.1093/infdis/jiz591
24. Ison MG, Hager J, Blumberg E, et al. Donor-derived disease transmission events in the United States: data reviewed by the OPTN/UNOS disease transmission advisory committee. Am J Transplant. 2009;9(8):1929–1935. doi:10.1111/j.1600-6143.2009.02700.x
25. Ison MG, Nalesnik MA. An update on donor-derived disease transmission in organ transplantation. Am J Transplant. 2011;11(6):1123–1130. doi:10.1111/j.1600-6143.2011.03493.x
26. Tarabichi M, Shohat N, Goswami K, et al. Diagnosis of Periprosthetic Joint Infection: the potential of next-generation sequencing. J Bone Joint Surg Am. 2018;100(2):147–154. doi:10.2106/JBJS.17.00434
27. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240. doi:10.1093/cid/ciy693
28. Corbel A, Ladrière M, Le Berre N, et al. Microbiological epidemiology of preservation fluids in transplanted kidney: a nationwide retrospective observational study. Clin Microbiol Infect. 2020;26(4):475–484. doi:10.1016/j.cmi.2019.07.018
29. Le Berre N, Ladrière M, Corbel A, et al. Antibiotic therapy in case of positive cultures of kidney transplant preservation fluid: a nationwide survey of prescribing practices. Eur J Clin Microbiol Infect Dis. 2020;39(5):915–921. doi:10.1007/s10096-019-03808-4
30. Bachmann F, Adam T, Friedersdorff F, et al. Perioperative antibiotic prophylaxis in renal transplantation: a single-center comparison between two regimens and a brief survey among the Eurotransplant renal transplantation centers. World J Urol. 2019;37(5):957–967. doi:10.1007/s00345-018-2440-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Positive Metagenomic Next-Generation Sequencing of Renal Lavage Fluid Associates with Delayed Graft Function in Kidney Transplants from Donors After Circulatory Death: A Retrospective Study
Li D, Pan J, Yang M, Zhong J, Ding H, Chen W, Zhang J, Liao G
Infection and Drug Resistance 2025, 18:4579-4592
Published Date: 30 August 2025