Back to Journals » Journal of Pain Research » Volume 18
Optimal Information for Chronic Pain (OICP): Delphi Consensus on Patient Assessment and Interventional Techniques
Authors Frutos V ![]() , Delgado D
, Delgado D ![]() , Cuñat T
, Cuñat T ![]() , Aguilar JL, Recasens-Urbez J, Homs M
, Aguilar JL, Recasens-Urbez J, Homs M ![]() , Fernandez-Bravo A
, Fernandez-Bravo A ![]() , Izquierdo RM, Munoz-Ortego J, Sánchez M
, Izquierdo RM, Munoz-Ortego J, Sánchez M ![]() , Cordero-García C
, Cordero-García C ![]() , Abejón D, Cayuela M
, Abejón D, Cayuela M
Received 19 June 2025
Accepted for publication 21 October 2025
Published 31 October 2025 Volume 2025:18 Pages 5661—5671
DOI https://doi.org/10.2147/JPR.S548388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Video abstract of “Minimum Information for Chronic Pain” [548388]
Views: 31
Victor Frutos,1 Diego Delgado,2 Tomas Cuñat,3 José Luis Aguilar,1 Jordi Recasens-Urbez,4 Marta Homs,4 Almudena Fernandez-Bravo,5 Rosa María Izquierdo,6 Juan Munoz-Ortego,7 Mikel Sánchez,2,8 Carlos Cordero-García,9 David Abejón,10 María Cayuela11
1Pain Management Unit, Hospital Quironsalud Palmaplanas, Palma, Spain; 2Advanced Biological Therapy Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain; 3Pain Management Unit, Hospital Clínic de Barcelona, Barcelona, Spain; 4Pain Management Unit, Hospital Universitari Dexeus, Barcelona, Spain; 5Department of Physical Medicine and Rehabilitation, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain; 6Pain Management Unit, Hospital La Fe, Valencia, Spain; 7Centro Médico Teknon & CEO Regenera Medical Center, Barcelona, Spain; 8Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain; 9Department of Physical Medicine and Rehabilitation, Hospital Universitario Juan Ramón Jiménez, Huelva, Spain; 10Pain Management Unit, Hospital Universitario Quirónsalud Madrid, Madrid, Spain; 11BioSmartData SL, Marratxí, Spain
Correspondence: Victor Frutos, Pain Management Unit, Hospital Quironsalud Palmaplanas, Camí dels Reis, 308, Nord, Palma, Illes Balears, 07010, Spain, Email [email protected] María Cayuela, BioSmartData SL, C/ Xesc Forteza (Actor), 5 – Local – 07141, Marratxí, Illes Balears, Spain, Email [email protected]
Purpose: Chronic pain is characterized by a persistence beyond the healing time of the injury. However, clinical documentation in this field remains highly variable, limiting the quality of patient care and research. Due to its multifactorial nature, a comprehensive evaluation of the methods used is essential. The objective of this work was to develop a consensus to define the optimal requirements for the evaluation of patients with chronic pain, with implications for real-world data analysis, predictive modeling, and standardized care pathways.
Patients and Methods: A Delphi method was employed to gather expert opinions and to establish optimal criteria for evaluating chronic pain patients. After composition of the steering group and selection of the expert panel, based on clinical experience and multidisciplinary background, three surveys were conducted related to patient/pathology, treatment and follow-up. Survey items were derived from literature review and clinical guidelines and rated on a 5-point Likert scale. Three rounds per survey were conducted and the variables were categorized as essential if more than 70%/70%/75% of the experts agreed and less than 20%/10%/5% disagreed in each of the 3 rounds. The variables on which there was most consensus cover the whole pain management, including demographics, pain treatments, and follow-up assessing pain and medication consumption.
Results: The number of variables considered essential to be collected were 38/60 in patient/pathology survey, 103/150 in treatment survey and 13/34 in follow-up survey, reaching an overall percentage of 63.1%. The variables on which there was most consensus cover all pain management, including demographics, pain treatments, and follow-up assessing pain and medication use.
Conclusion: This work identifies several variables considered essential in the management of chronic pain patients, covering aspects related to the patient, pathology, treatment and follow-up, pointing out the importance of consensus within this field of medicine.
Plain Language Summary: Chronic pain can have a serious impact on people’s lives, often lasting for months or years and affecting their ability to work, sleep, and enjoy daily activities. Doctors and healthcare teams need reliable and consistent information to properly assess and treat people living with chronic pain. However, there is no widely agreed list of the most important information that should be collected when seeing these patients.
To help solve this, a group of pain specialists from across Spain worked together using a method called Delphi. This approach allows experts to anonymously share their opinions over several rounds of surveys until they reach agreement. The goal was to identify an optimal set of essential information that should be recorded for every person with chronic pain.
The researchers developed three surveys focused on the patient’s condition, the treatments received, and the follow-up care. After three rounds, the group agreed on a list of 154 key data points. These include details such as pain location, treatments used, medication response, and how pain affects the person’s daily life.
This agreed set of information – called the Optimal Information for Chronic Pain (OICP) – can help improve communication between healthcare professionals, support better decision-making, and make it easier to compare results between clinics and research studies. It also sets a foundation for using real-world data and digital tools in chronic pain care.
By standardizing how chronic pain is evaluated, this work aims to improve the quality and consistency of care for people living with this challenging condition.
Keywords: consensus methodology, real-world data, health information standardization, clinical data collection, pain medicine, multidisciplinary evaluation
Introduction
Chronic pain affects between 11% and 40% of the world´s population,1 with an estimated prevalence of 20.4% in the United States alone.2 At the same time in the United Kingdom, chronic pain was estimated to have a combined prevalence of 43.5%,3 with an annual incidence rate of 8.3%,4 while in Europe, studies report a percentage of the population with chronic pain of around 20%.5
This high prevalence also implies a major socioeconomic challenge for healthcare services. The significant limitations of these patients in their ability to work and participate in daily activities further increases the demand for healthcare resources. Thus, chronic pain also represents a significant economic burden in both the United States and Europe.1 In the United States, for instance, the annual economic cost of chronic pain is estimated to be between 560 billion and 635 billion dollars.6
One of the main characteristics that could define chronic pain is its persistence beyond the healing time of the lesion that initially caused it, without a clearly identifiable cause.7 It affects the quality of life of those who suffer from it, with serious physical and emotional consequences.8 According to the World Health Organization (WHO) and the International Association for the Study of Pain (IASP), chronic pain is not simply a symptom, but a disease in itself.9 In contrast to acute pain, which is a resolving response to tissue damage, chronic pain no longer has evolutionary benefits. It cannot be easily eradicated, and its management focuses on controlling it to restore the patient’s function and emotional well-being.10,11
The subjective and multifactorial nature of chronic pain makes its accurate diagnosis difficult. Biological, psychological and social factors influence the perception of pain, complicating its proper assessment.1 This makes the approach and treatment of this pathology a challenge for healthcare professionals. Thus, pain management involves the application of different treatments, alone or in combination, including pharmacological therapy, interventional procedures, physical therapy and/or behavioral therapy,12,13 with a gaining popularity in most recent therapies such as biological therapies within the framework of regenerative medicine.14
Given the complexity and multidisciplinary nature of chronic pain, a comprehensive evaluation of the current methods used in its diagnosis and management is essential. This approach encompasses not only the diversity of pathologies associated with chronic pain, but also the need to guide the future use of treatments and establish standardized working protocols for patients.
Clinicians face multiple challenges when evaluating patients with chronic pain. Patient history is often incomplete due to limited recall or fragmented documentation, and access to prior records is frequently insufficient. Structured documentation is further hindered by system-level barriers such as time constraints, complexity of electronic health records, and limited staffing. These issues are compounded by long wait times and shortages of pain specialists. As a result, data capture is often inconsistent, reducing the quality of care and limiting the value of clinical data for research. These challenges highlight the need for a standardized documentation framework to improve consistency and support clinical and scientific progress.
Several national and international guidelines exist for the diagnosis and management of chronic pain (eg, IASP criteria, NICE guidelines, and pain society protocols).11–15 However, these documents typically focus on clinical criteria and treatment recommendations rather than providing a standardized set of variables to be collected in real-world clinical settings.16,17
Therefore, the objective of the present work was to develop a consensus to define the optimal requirements for the evaluation of patients with chronic pain, using the Delphi consensus method. This widely used method helps structure expert consensus when empirical evidence is limited. However, its reliability depends on the quality of expert selection and the available evidence base.18,19
Materials and Methods
Study Design
This was a Delphi consensus study designed to define a minimum dataset of essential variables for chronic pain patient assessment and interventional management following the recommendations of the guidelines for Delphi studies.20,21 Although the study was not prospectively developed following the CREDES guidelines, we have referred to them retrospectively to improve transparency in reporting.19
The process included three iterative rounds for each of the three domains explored: patient/pathology, treatment, and follow-up. Surveys were distributed electronically using a secure online platform, and all data were anonymized prior to analysis. Participants rated items using a 5-point Likert scale and could provide free-text suggestions at each round.
Steering Group Composition
The steering group consisted of 11 multidisciplinary members with clinical and academic expertise in chronic pain, research, and consensus methodologies. All had prior experience with Delphi studies. The group was responsible for selecting items to be assessed, designing the survey structure, analyzing intermediate results, and preparing subsequent rounds.
Selection of the Expert Panel
Experts were required to be clinically active physicians with recognized expertise in chronic pain, demonstrated by leadership positions, scientific publications, or national/international recognition. Eleven principal investigators were purposively selected from four specialties: anesthesiology/pain medicine, rehabilitation, rheumatology, and traumatology. Each investigator then nominated at least five additional experts meeting the same eligibility criteria (snowball sampling), resulting in a diverse and experienced panel.
A total of 52 experts were included: 26 anesthesiologists, 13 rehabilitation physicians, 9 orthopedic surgeons, and 4 rheumatologists. Experts received Email invitations with personalized links to the surveys. Non-responders received up to two electronic reminders per round. Only completed responses were included in each round’s analysis, though participants remained eligible for subsequent rounds.
Delphi Process and Item Generation
The study was prospectively designed to include three rounds per survey. Items were derived from targeted literature review, national and international clinical guidelines, routinely collected variables in electronic health records, and the clinical experience of the steering group. Surveys were organized into three thematic areas: (1) Patient and pathology characteristics, (2) Treatment variables and (3) Follow-up assessment (Supplementary Material). In Round 1, participants rated all initial items and could suggest new ones via free-text responses. The steering group reviewed free-text comments using thematic analysis. Suggestions deemed relevant were added as new items or used to reword existing items for subsequent rounds.
All items were rated on a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree). Consensus rules remained constant across rounds; only the thresholds became more stringent:
- Round 1: Items were retained if ≥70% of participants rated them as “agree” (scores 4–5), and ≤20% rated them as “disagree” (scores 1–2).
- Round 2: Thresholds tightened to ≥70% agreement and ≤10% disagreement.
- Round 3: Final consensus required ≥75% agreement and ≤5% disagreement.
Items that did not meet these criteria were either discarded or classified as “no consensus.” Items that met inverse thresholds (eg, high disagreement) were classified as “negative consensus.” No changes were made to the definition of consensus during the study; only the strictness of the thresholds increased with each round. The first round of the first survey was conducted in September 2024, and the third round of the fourth and final survey in January 2025.
Data Analysis
Survey data were exported to Microsoft Excel for descriptive statistical analysis. For each round, percentages of agreement/disagreement were calculated. In Round 3, weighted means were also calculated by computing agreement scores within each specialty and averaging across them, to ensure equal representation regardless of panel size.
Results
The number of variables considered essential to be collected were 38/60 in patient/pathology survey, 103/150 in treatment survey and 13/34 in follow-up survey, reaching an overall percentage of 63.1%. The variables on which there was most consensus cover all pain management, including demographics, pain treatments, and follow-up assessing pain and medication use.
The results of the preliminary survey of the most frequent pathologies and treatments in medical practices are shown in Table 1. Concerning the three main blocks of the study, the first survey consisted of 60 variables related to the patient and pathology, the second of 150 variables related to treatment and the third of 34 variables related to follow-up. The number of variables on which a consensus was reached to be considered optimal to be collected were 38, 103 and 13, respectively, reaching an overall percentage of 63.1%.
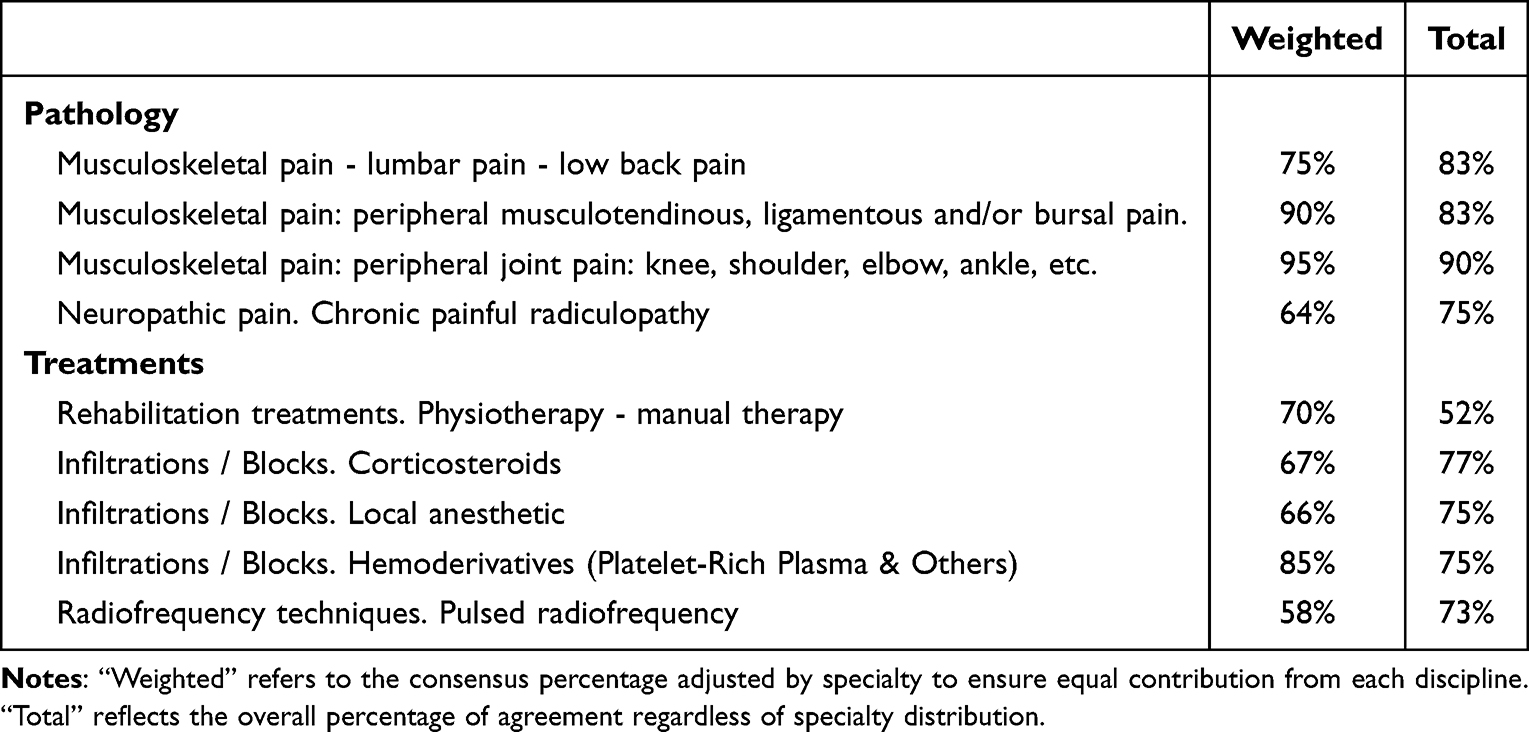 |
Table 1 Most Common Pathologies and Treatments |
Patient and Pathology Variables
Table 2 lists the variables considered as optimal in the collection of data on the patients and the pathology they suffer from. Regarding patient characteristics, most of them are related to demographic aspects, medication or medical history, as well as employment status. Thus, the variables that reached the greatest consensus (over 95%) were medical history (100%), current pain medication (100%), current psychiatric medication (99%), current anticoagulant medication (97%) and drug allergies (96%). Regarding the subset related to the pathology, 88.8% (16/18) of the proposed variables were agreed upon with a high level of consensus, highlighting diagnosis (100%), night’s rest (100%), main treatment (100%) and factors that improve pain (100%).
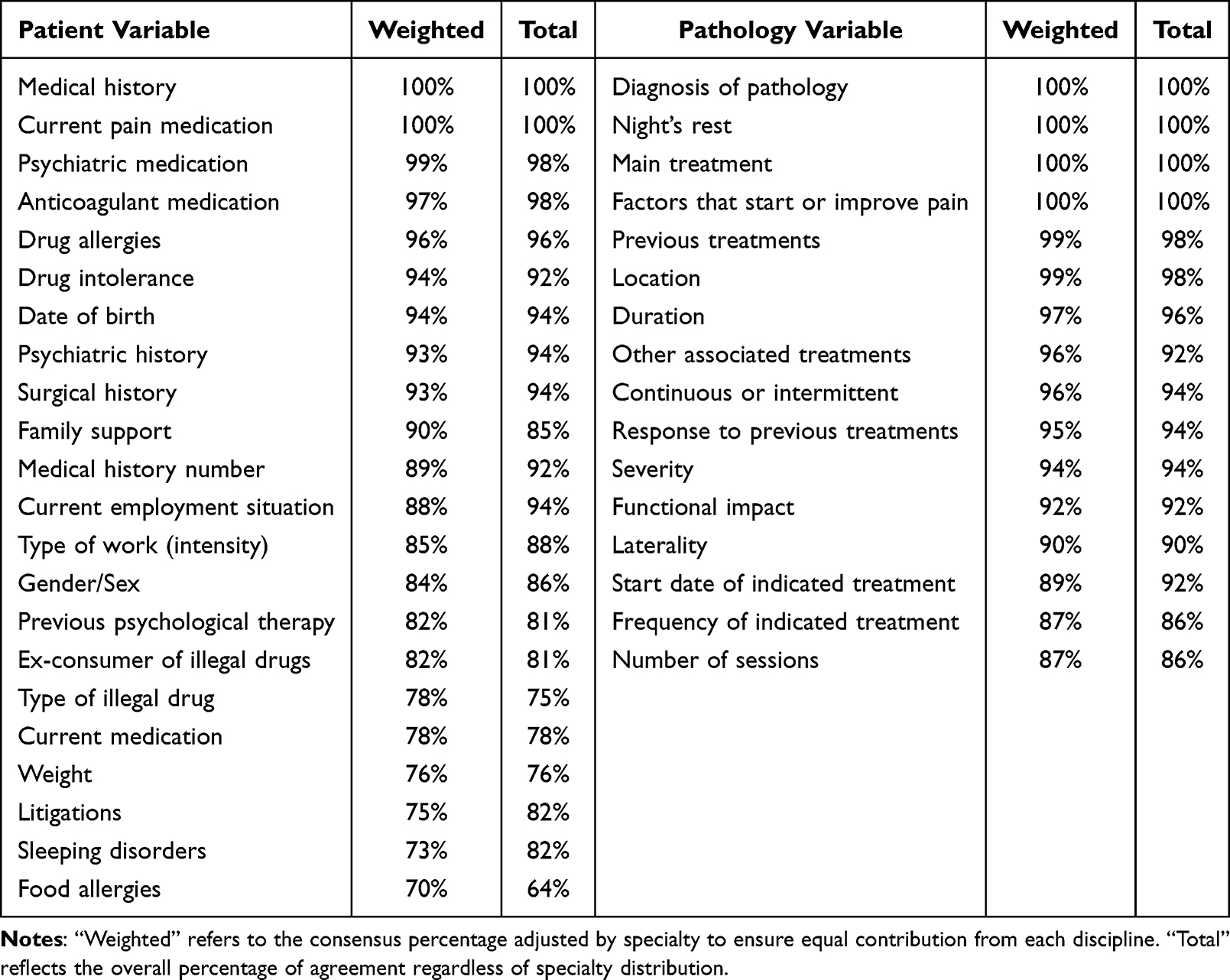 |
Table 2 Optimal Patient- and Pathology-Related Variables to Be Collected |
Treatment Variables
The survey on the variables to be collected related to the treatment was divided into 11 different blocks depending on each treatment and with a great variety in the percentage of variables agreed upon per treatment: magnetotherapy (50%), shock waves (64.3%), cryotherapy (55.6%), manual therapy (100%), dry needling (33.3%), rest (83.3%), infiltrations and blocks (80%), blood-derived products (57.7%), neuromodulation (60%), medullary neurostimulation (94.4%) and radiofrequency (80%).
The agreed variables are shown in Table 3. The variables with the highest degree of agreement were common to the different treatments, especially the area of localization, the number of sessions and the mode of application.
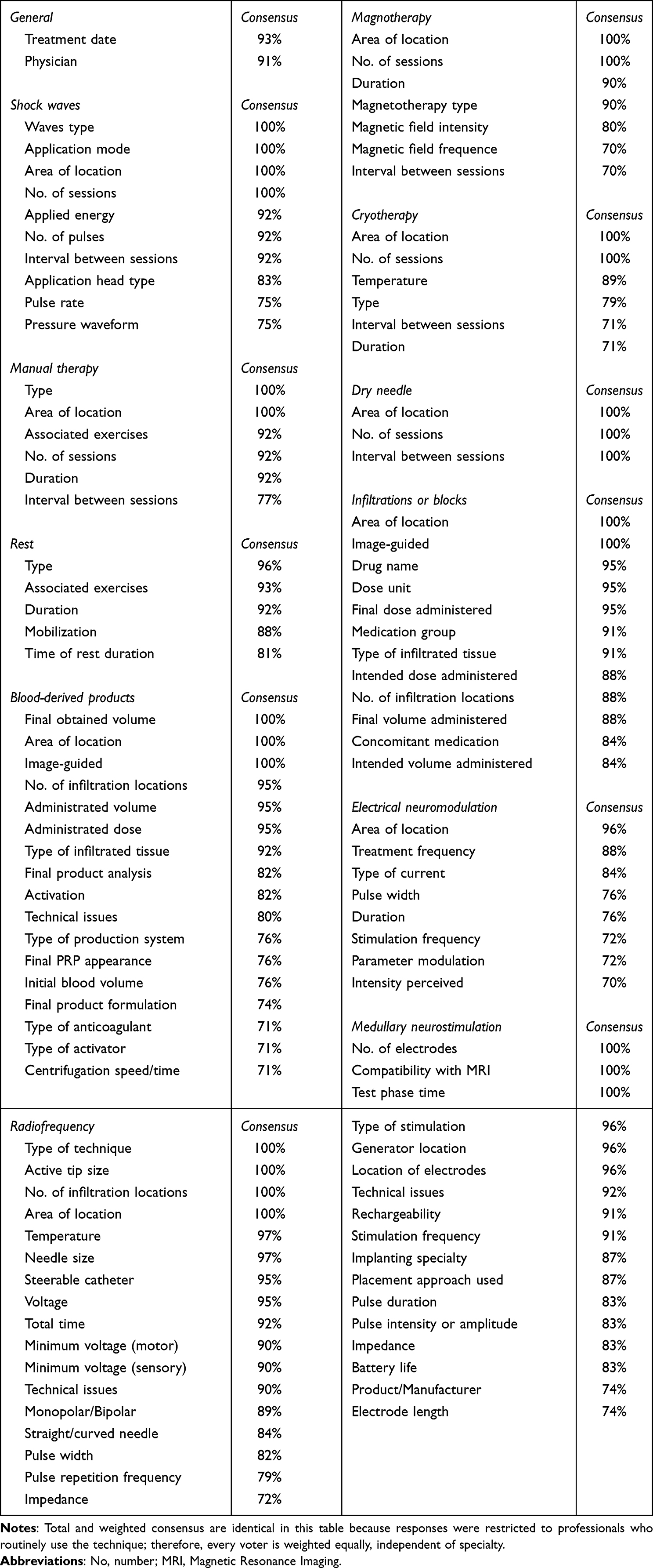 |
Table 3 Optimal Treatment-Related Variables to Be Collected |
Follow-up Variables
Table 4 shows the optimal variables to be collected during patient follow-up. Thirteen of the 34 variables proposed (38.2%) were accepted by consensus. The variables that reached the highest degree of consensus were related to the effectiveness and safety of the treatment, such as the evolution of pain intensity (97%) and the appearance of adverse effects and complications (97%). The full set of results, including agreement and disagreement percentages for each item across all three Delphi rounds, is available in the Supplementary Material.
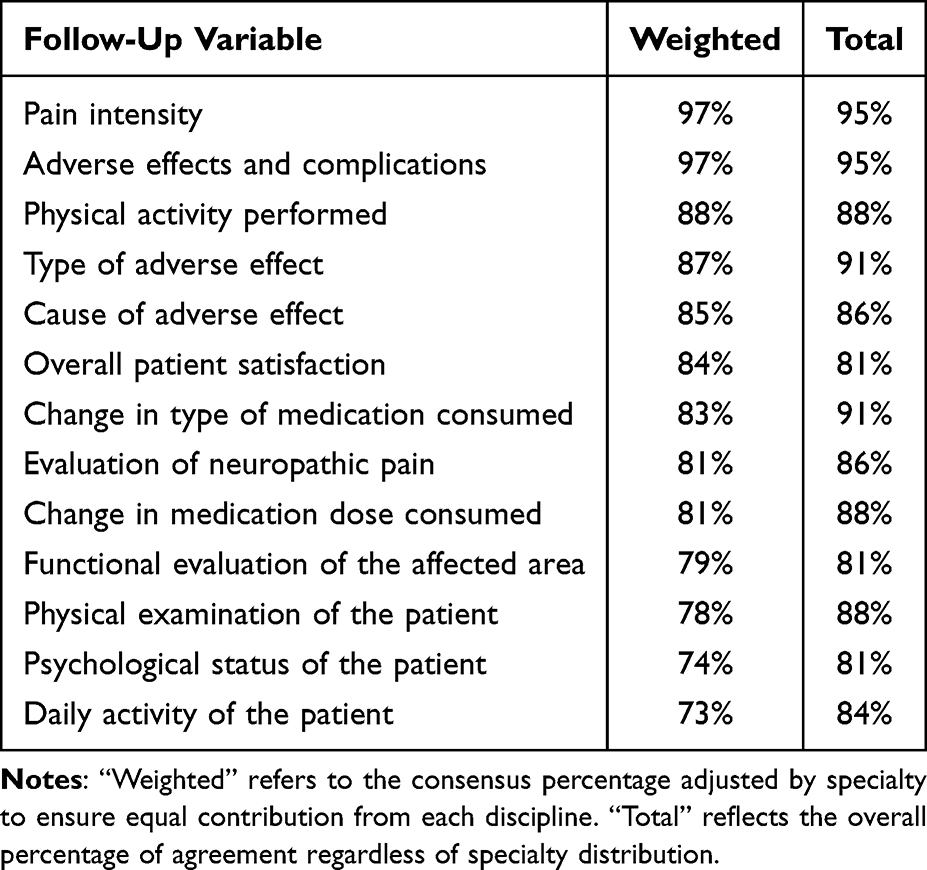 |
Table 4 Optimal Essential Follow-Up Related Variables to Be Collected |
Discussion
In the present work, a number of variables were identified using the Delphi method, which were agreed upon by the panel of experts as optimal to be collected during the management of a patient suffering from chronic pain. Of all the variables consulted, 63.1% were selected by consensus, divided into variables related to the pathology and the patient, as well as to the treatment and follow-up.
The identification of the variables described in this work are considered to be collected in daily medical practice, facilitating healthcare professionals to collect in a standardized way all the necessary information for a correct diagnosis, treatment and follow-up of patients with chronic pain. In addition, this standardization will allow clinical research to be conducted through Real-World Evidence (RWE) studies. The rise of these kind of studies is significantly transforming the landscape of clinical research and healthcare decision making. Unlike traditional controlled clinical trials, these studies are based on real-world data, such as electronic medical records and patient registries. This makes it possible to evaluate the effectiveness and safety of treatments in everyday settings, more representative of routine medical practice.22 This is of particular importance in the field of pain, where interest in RWE for benefit-risk assessments of pain treatments and procedures is increasing, given the paucity of drugs showing efficacy in randomized controlled trials.23 This approach has been successfully used by Venkatraman et al to collect variables in patients with chronic pain treated by spinal cord stimulation, improving patient satisfaction compared to registries to date.24 Moreover, RWE studies are being used in many other pathologies and treatments related to chronic pain such as migraine,25 neck pain,26 peripheral nerve stimulation27 or pulsed radiofrequency targeting on dorsal root ganglion.28 A comprehensive and systematic data collection combined with next-generation data analysis and implementing artificial intelligence would allow the development of algorithms that would optimize decision making in the management of these patients.
Regarding patient- and treatment-related factors, the variables selected cover typical medical history data such as demographic characteristics, medical and medication history, previous treatments, and concomitant pathologies. It is worth noting the high consensus reached by the experts on including variables such as psychological and psychiatric history, family support or history related to drug use. This is in line with previous studies demonstrating the importance of these factors in this type of pathology.29,30 Paradoxically, variables also included in the psychosocial sphere such as drug and tobacco abuse, financial situation, marital status or sexual abuse in childhood were among those that reached the least consensus, possibly due to excessive intrusion into the patient’s privacy.31
The collected variables related to treatment point out the most used treatments for chronic pain. It is worth mentioning that biological treatments framed in regenerative medicine are amongst these treatments. More specifically, the use of blood-derived products such as Platelet Rich Plasma, is shown to be emerging strongly in pain medicine, thanks to their anti-inflammatory and tissue repair-stimulating properties.32 However, one of the main problems with this type of treatment is its great heterogeneity, which often leads to contradictory results and confusing conclusions.33 Therefore, an exhaustive data collection that includes aspects on the type of product and protocol applied is necessary for the optimization of biological therapies.34 The variables agreed upon in this work coincide with the recommendations of the MIBO guidelines (Minimum Information for Studies Evaluating Biologics in Orthopaedics) in which the characterization of the final product is essential.35 Finally, it is necessary to point out the absence of variables on treatments based on cell therapies, which could indicate the initial state of these products.
Finally, the follow-up variables selected in this study are consistent with previous similar studies where aspects such as pain, medication consumption and adverse events were the most relevant.7,36 Thus, in the present study the expert panel reached a broad consensus in identifying as essential variables the assessment of pain intensity, complications and adverse effects, and changes in medication type or dosage, as well as functional assessments and patient satisfaction. Interestingly, a presumably objective indicator in patient assessment such as the number of days of sick leave, was the variable that reached the least consensus among the experts, probably due to the influence of other aspects unrelated to the pathology such as economic, social, work space conditions or moral considerations.37–39 Of note, no consensus was reached for certain clinical conditions such as headache, complex regional pain syndrome (CRPS), and polyneuropathy. This may reflect the inherent heterogeneity in their clinical presentation, variability in diagnostic and therapeutic approaches, or the possibility that some of these conditions were less familiar to a subset of panelists depending on their subspecialty focus. These results highlight the need for further consensus development in specific pain syndromes.
Our findings must also be interpreted considering existing guidelines. For example, the IMMPACT initiative recommends the use of validated core outcome domains to evaluate treatment effectiveness in clinical trials.40 Similarly, the IASP and the European Pain Federation (EFIC) have published guidance on the assessment of chronic pain.41,42 The OICP framework does not aim to replace these efforts, but rather to complement them by providing a standardized optimal dataset applicable in real-world clinical practice and multicenter registries. This approach may bridge the gap between guideline-based outcome measurement and the variability observed in routine care.43
The main limitations of this study are inherent to the Delphi process. Firstly, although the questions and variables provided by the steering group to the expert panel were considered broadly extensive, it is possible that factors that could have been considered essential by the expert panel were missing. Secondly, although chronic pain is a cross-cutting condition across the specialties to which the members of the expert panel belong, the imbalance between the number of specialists in the different types of specialties could be a bias in the final selection of the variables. Another limitation is that the initial selection of candidate variables was not based on a formal systematic literature review. Instead, the steering group developed the list using targeted literature searches, routinely collected data in electronic health records, and expert clinical experience. While this pragmatic approach aimed to reflect real-world practice, future studies could benefit from a more structured evidence synthesis in the item development phase.
Additionally, no patients or patient representatives were included in the Delphi panel. While the aim of this first phase was to establish consensus among clinicians on core clinical data elements, we acknowledge that this limits the framework’s ability to reflect patient-centered outcomes.40 Future developments of the MICP framework should incorporate the perspectives of people living with chronic pain, especially regarding outcome domains that matter most to them in treatment evaluation and daily life. While the OICP framework provides a comprehensive reference for chronic pain data collection, its implementation may be limited by variability in clinical documentation, resource constraints, and healthcare system differences. It should be interpreted as a flexible guidance tool — a “North Star” — rather than a rigid standard. Adoption can be gradual and tailored to local capacity, prioritizing the most feasible and impactful variables. Also, the external validity of the OICP recommendations may be limited by geographical factors. The expert panel was composed exclusively of clinicians practicing in Spain, which may influence prioritization of certain data elements. Moreover, some interventional techniques or therapies included in the consensus may not be available or widely used outside of European healthcare systems. As such, future adaptations of the OICP framework should consider regional practices, resource availability, and regulatory environments.
Implementing the OICP framework into electronic health systems could help standardize data collection and enhance the understanding of chronic pain conditions and their management. This, in turn, may facilitate the generation of high-quality real-world data to develop predictive models that support more effective and personalized treatment strategies.
Conclusion
This work identifies several variables considered optimal in the management of chronic pain patients, covering aspects related to the patient, the pathology, the treatment and the follow-up, pointing out the importance of consensus within this field of medicine. The collection and analysis of these variables during medical practice could help to improve and optimize future decision-making in the management of such a heterogeneous and complex pathology, which chronic pain is considered to be.
Acknowledgments
The authors wish to thank the BioSmartData coordination team—Amrei Ewers, María Sánchez, and Juan Cifre—for their unfailing logistical support throughout every stage of the project.
Our sincere appreciation also goes to the members of the voting panel whose expertise and commitment made this consensus possible: Juan Fernando, Alejandro San Martín, Rosario Armand, Álvaro García, Guilherme Ferreira, María del Mar Monerris, Jesús de Santiago, Alfredo Rodríguez, Antonio Ojeda, Antonio Montero, Antonio Montes, Alejandro Ortega, Blanca Cabaleiro, Blanca B. Martínez, Gisela Roca, Diego Benítez, Lucía Fernández-Mellado, Ana Belén Puentes, Carles Espinós, Hermann Ribera, Daniel Samper, Dores Sánchez, Antonia P. Soriano, Juan Casar, Luis Moltó, María del Ara Bermejo, Ruth M. Robledo, Beatriz Castel, David Bande, Juan Azofra, Beatriz Aizpurua, Nicolás Fiz, Jaime Oraa, Leonor López de Dicastillo, Sergio González, Alexis Fernández, Ana López de Pariza, Lucía B. Guidali, María Cano, Alberto Sánchez, Aitziber Ereniozaga, and Deiene Lasuen. Their collective insights and disciplined engagement across successive Delphi rounds ensured a robust, multidisciplinary consensus for the Optimal Information for Chronic Pain (OICP) framework.
This study did not involve human participants, identifiable human data, or clinical interventions. It was based on expert consensus using the Delphi method. According to national regulations and institutional policies, this type of non-interventional research is exempt from ethical committee approval. All participating experts provided informed consent to participate in the study and for the use of anonymized responses in publication. BioSmartData supported the technical deployment of the Delphi platform and coordination of survey dissemination. The company had no role in the study design, data analysis, interpretation of findings, or manuscript writing.
Funding
This study is part of the project “Real-World Evidence in Chronic Pain: MICP consensus for patient evaluation and efficiency models” (ref. PINEM23_019), co-financed by the European Regional Development Fund (ERDF/FEDER) within the Balearic Islands ERDF 2021-2027 program (60%), and the Impost de Turisme Sostenible de les Illes Balears (ITS) - Sustainable Tourism Tax of the Balearic Islands Government.
Disclosure
Dr Carlos Cordero-García reports personal fees from Merz Therapeutics, Ipsen, Viatris, Fidia Pharma, IBSA Iberia, and Cardiva, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
2. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults—United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
3. Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364. doi:10.1136/bmjopen-2015-010364
4. Elliott AM, Smith BH, Hannaford PC, Smith WC, Chambers WA. The course of chronic pain in the community: results of a 4-year follow-up study. Pain. 2002;99(1–2):299–307. doi:10.1016/S0304-3959(02)00138-0
5. Reid KJ, Harker J, Bala MM, et al. Epidemiology of chronic non-cancer pain in Europe: narrative review of prevalence, pain treatments and pain impact. Curr Med Res Opin. 2011;27(2):449–462. doi:10.1185/03007995.2010.545813
6. Steglitz J, Buscemi J, Ferguson MJ. The future of pain research, education, and treatment: a summary of the IOM report “Relieving pain in America. Transl Behav Med. 2012;2(1):6–8. doi:10.1007/s13142-012-0110-2
7. De la Calle JL, Abejón D, Canós-Verdecho Á, et al. Recommendations to standardize patients’ follow-up after interventional procedures in chronic pain treatment: a Delphi study. Pain Pract. 2023;23(6):618–625. doi:10.1111/papr.13228
8. Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain. 2019;160(1):28–37. doi:10.1097/j.pain.0000000000001390
9. Breivik H, Eisenberg E, O’Brien T. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health. 2013;13(1):1229. doi:10.1186/1471-2458-13-1229
10. Clauw DJ, Essex MN, Pitman V, Jones KD. Reframing chronic pain as a disease, not a symptom: rationale and implications for pain management. Postgrad Med. 2019;131(3):185–198. doi:10.1080/00325481.2019.1574403
11. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
12. Ashcraft LE, Hamm ME, Omowale SS, et al. The perpetual evidence-practice gap: addressing ongoing barriers to chronic pain management in primary care in three steps. Front Pain Res. 2024;5:1376462. doi:10.3389/fpain.2024.1376462
13. Wang J, Doan LV. Clinical pain management: current practice and recent innovations in research. Cell Rep Med. 2024;5(10):101786. doi:10.1016/j.xcrm.2024.101786
14. D’Souza RS, Her YF, Hussain N, et al. Evidence-based clinical practice guidelines on regenerative medicine treatment for chronic pain: a consensus report from a multispecialty working group. J Pain Res. 2024;17:2951–3001. doi:10.2147/JPR.S480559
15. National Institute for Health and Care Excellence (NICE). Chronic Pain (Primary and Secondary) in Over 16s: Assessment of All Chronic Pain and Management of Chronic Primary Pain. NICE guideline [NG193]; 2021.
16. Eccleston C, Fisher E, Cooper TE, et al. Interventions for the reduction of prescribed opioid use in chronic non-cancer pain. Cochrane Database Syst Rev. 2023;5(5):CD010323.
17. Nijs J, Leysen L, Vanlauwe J, et al. Treatment of central sensitization in patients with chronic pain: an update on current evidence and future directions. Expert Opin Pharmacother. 2021;22(9):1119–1134. doi:10.1080/14656566.2021.1901885
18. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
19. Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on conducting and reporting Delphi studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med. 2017;31(8):684–706. doi:10.1177/0269216317690685
20. Hsu CC, Sandford BA. The Delphi technique: making sense of consensus. Pract Assess Res Eval. 2007;12(1):10.
21. Von der Gracht HA. Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc Change. 2012;79(8):1525–1536. doi:10.1016/j.techfore.2012.04.013
22. Bakker E, Plueschke K, Jonker CJ, et al. Contribution of real-world evidence in European medicines agency’s regulatory decision making. Clin Pharmacol Ther. 2023;113(1):135–151. doi:10.1002/cpt.2766
23. Baron R, Mick G, Serpell M. The relevance of real-world data for the evaluation of neuropathic pain treatments. Pain Manag. 2022;12(7):845–857. doi:10.2217/pmt-2022-0057
24. Venkatraman V, Bharmi R, Coletti F, et al. Real-world characterization of chronic pain, success rates and implant rates: evidence from a digital health platform of patients undergoing spinal cord stimulation evaluations. J Pain. 2023;24(12):2228–2239. doi:10.1016/j.jpain.2023.07.008
25. Oliveira R, Gil-Gouveia R, Puledda F. CGRP-targeted medication in chronic migraine: systematic review. J Headache Pain. 2024;25(1):51. doi:10.1186/s10194-024-01753-y
26. Huang JF, Meng Z, Zheng XQ, et al. Real-world evidence in prescription medication use among U.S. adults with neck pain. Pain Ther. 2020;9(2):637–655. doi:10.1007/s40122-020-00193-1
27. Pingree MJ, Hurdle MF, Spinner DA, et al. Real-world evidence of sustained improvement following 60-day peripheral nerve stimulation treatment for pain: a cross-sectional follow-up survey. Pain Manag. 2022;12(5):611–621. doi:10.2217/pmt-2022-0005
28. Hong LW, Chen KT. A real-world evidence of a consecutive treatment of 42 spine-related pain using dorsal root ganglion–pulsed radiofrequency (DRG-PRF). Clin Neurol Neurosurg. 2020;197:106186. doi:10.1016/j.clineuro.2020.106186
29. Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168–182. doi:10.1016/j.pnpbp.2018.01.017
30. Van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013;111(1):13–18. doi:10.1093/bja/aet123
31. Lacasse A, Gagnon V, Nguena Nguefack HL, et al. Chronic pain patients’ willingness to share personal identifiers on the web for the linkage of medico-administrative claims and patient-reported data: the chronic pain treatment cohort. Pharmacoepidemiol Drug Saf. 2021;30(8):1012–1026. doi:10.1002/pds.5255
32. Ferreira-Dos-Santos G, Hurdle MFB, Clendenen SR, et al. Autologous platelet-rich plasma applications in chronic pain medicine: establishing a framework for future research—a narrative review. Pain Physician. 2022;25(1):15–27.
33. Chahla J, Cinque ME, Piuzzi NS, et al. A call for standardization in platelet-rich plasma preparation protocols and composition reporting: a systematic review of the clinical orthopaedic literature. J Bone Joint Surg Am. 2017;99(20):1769–1779. doi:10.2106/JBJS.16.01374
34. Kon E, Di Matteo B, Delgado D, et al. Platelet-rich plasma for the treatment of knee osteoarthritis: an expert opinion and proposal for a novel classification and coding system. Expert Opin Biol Ther. 2020;20(1):1–14. doi:10.1080/14712598.2020.1691994
35. Murray IR, Geeslin AG, Goudie EB, et al. Minimum information for studies evaluating biologics in orthopaedics (MIBO): platelet-rich plasma and mesenchymal stem cells. J Bone Joint Surg Am. 2017;99(10):809–819. doi:10.2106/JBJS.16.00793
36. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
37. Arocena P, García-Carrizosa LM. Determinants of the duration of sick leave due to occupational injuries: evidence from Spanish manufacturing. J Safety Res. 2023;86:311–317. doi:10.1016/j.jsr.2023.07.009
38. Corbett K, Gran JM, Kristensen P, Mehlum IS. Adult social position and sick leave: the mediating effect of physical workload. Scand J Work Environ Health. 2015;41(6):542–553. doi:10.5271/sjweh.3525
39. Pollak C. The impact of a sick pay waiting period on sick leave patterns. Eur J Health Econ. 2017;18(1):13–31. doi:10.1007/s10198-015-0755-0
40. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337–345. doi:10.1016/j.pain.2003.08.001
41. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
42. Pickering G, O’Keeffe M, Bannister K, et al. A pain research strategy for Europe: a European survey and position paper of the European Pain Federation EFIC. Eur J Pain. 2025;29(1):e4767. doi:10.1002/ejp.4767
43. Dworkin RH, Turk DC, Peirce-Sandner S, et al. Considerations for improving assay sensitivity in chronic pain clinical trials: IMMPACT recommendations. Pain. 2012;153(6):1148–1158. doi:10.1016/j.pain.2012.03.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.