Back to Journals » Journal of Pain Research » Volume 14
Optimal Cut-Off Points of Sagittal Spinopelvic Parameters as a Morphological Parameter to Predict Efficiency in Nerve Block and Pulsed Radiofrequency for Lumbar Facet Joint Pain: A Retrospective Study
Authors Liang CL, Wang SW, Chen HJ, Tsai YD, Chen JS, Wang HK ![]() , Wang KW
, Wang KW
Received 3 February 2021
Accepted for publication 16 June 2021
Published 28 June 2021 Volume 2021:14 Pages 1949—1957
DOI https://doi.org/10.2147/JPR.S303979
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Cheng-Loong Liang,1,2 Shih-Wei Wang,1,3 Han-Jung Chen,1,2 Yu-Duan Tsai,1,2 Jui-Sheng Chen,1,2 Hao-Kuang Wang,1,2 Kuo-Wei Wang2,4
1Department of Neurosurgery, E-DA Hospital, Kaohsiung, Taiwan; 2School of Medicine, I-Shou University, Kaohsiung, Taiwan; 3Department of Rheumatology, E-DA Hospital, Kaohsiung, Taiwan; 4Department of Neurosurgery, E-Da Cancer Hospital, Kaohsiung, Taiwan
Correspondence: Kuo-Wei Wang Email [email protected]
Background: After proper patient selection, anatomically correct pulsed radiofrequency of the lumbar facet joints provide long-term pain relief in a routine clinical setting. In the study, we performed an analysis of clinical and radiological predictive factors and provide the scientific basis for this promising modality.
Methods: The study included 198 patients with lower back pain due to lumbar facet joint disease who underwent medial branch block and pulsed radiofrequency during the period 2015– 2019. According to the improvement in pain score, the patients were divided into good and poor outcome groups. Clinical and radiological data were collected and analyzed.
Results: The multivariable analysis revealed the predictive factors, including lumbar lordosis, lower lumbar lordosis, pelvic tilt, the number of facet joints, old compression fracture with/without vertebroplasty, and post lumbar fusion procedures.
Conclusion: With the results of this study, we demonstrated that the improved outcome after the surgery was related to lumbar lordosis, lower lumbar lordosis, pelvic tilt, the number of facet joints, old compression fracture with/without vertebroplasty, and the lumbar fusion procedures. Old compression fractures and lumbar fusion would change the radiological factors and cause refractory lumbar facet joint pain.
Keywords: lumbar facet joint pain, pulsed radiofrequency, lumbar lordosis, lower lumbar lordosis, pelvic tilt angle, lumbar fusion
Introduction
Chronic lower back pain (CLBP) is a cause of disability and mainly caused by abnormalities in the lumbar intervertebral disc, facet joints, and sacroiliac joints.1,2 The clinical characteristics of lumbar facet pain are that it eases with light flexion in the lower back and worsens with weight on the facet and extension of the lower back, accompanied by paraspinal tenderness, and is exacerbated by extension/rotation (facet loading) but not with flexed leg lifting or coughing.3,4 Lumbar facet joint disease is diagnosed on the basis of a combination of patient history, physical activity, and diagnostic imaging, frequently including computed tomography (CT) and magnetic resonance imaging (MRI).5,6
The only way to confirm facet pain is pain relief by diagnostic block.7 The prevalence of lumbar facet joint pain in CLBP ranges from 15% to 45%.8,9 Repetitive mechanical stress on the lumbar facet joints may cause osteoarthritis and can cause inflammation and narrowing of the capsule, resulting in axial CLBP.10
Several treatment procedures are used in the management of lumbar facet joint-related CLBP. Intra-articular injections, facet joint nerve blocks, and pulsed radiofrequency (PRF) have been shown to be effective. However, RF treatment has been shown to be superior to injection therapy in well-designed studies.11–13 Proper patient selection and correct anatomical placement of the electrodes for PRF have been described as important outcomes.14 In the patient selection, the main focus was on diagnostic medial branch block before performing PRF.14,15 Clinical and radiological factors are rarely discussed with the prognosis after PRF for lumbar facet joint pain. In the present study, we performed nerve block and PRF in patients with lumbar facet joint pain and investigated the predictive factors.
Methods and Materials
Patient Selection
Our institutional review board approved this retrospective study (EMRP-109-073, Institutional Review Boards of E-Da Hospital), and the source populations for the study were all consecutive patients who underwent lumbar facet medial branch block and PRF in the lumbar facet joint for lower back pain between January 2015 and December 2019. Written informed consent was obtained from all patients in E-Da cancer hospital and this study was ongoing in accordance with the ethical standards set out in the Declaration of Helsinki. The inclusion criteria were age ≥ 18 years, predominantly axial low back pain for ≥3 months, mean back pain score ≥ 3 of 10 over the past week on a numerical rating scale, failure to respond to more-conservative therapies (eg, physical therapy, integrative therapy, and pharmacotherapy), and presence of paraspinal tenderness. All the patients accepted conventional lying down X-rays, and MRI examinations before the procedures. Excluded from participation were patients with a known, specific etiology of low back pain (eg, significant spinal stenosis, grade II or III spondylolisthesis, cancer, or spinal scoliosis according to the findings on MRI); focal neurological signs or symptoms; pain related to sacroiliac joint degeneration; previous facet interventions; unilateral facet joint pain; pain associated with disc degeneration, the paraspinal muscles, and repeated lumbar spinal surgery; long-term medication with opioid drugs; and concomitant medical (eg, unstable angina) or psychiatric conditions that were likely to undermine the diagnostic workup or treatment response. The manuscript adheses to the applicable CONSORT guidelines.
Medial Branch Block
Medial branch blocks were performed in accordance with the previously published standards and techniques.16 Lumbar 5 dorsal rami blocks were performed by placing a 22-gauge needle in the groove between the sacral ala and articular process, while higher-level lumbar medial branch blocks were performed by inserting 22-gauge needles in an oblique trajectory at a point several millimeters below the junction of the upper transverse and superior articular processes. After confirmation of the needle placement in the anteroposterior and lateral views, a contrast medium was injected to ascertain the appropriate spread and absence of intravascular uptake. When needle placement was deemed appropriate, 0.5 mL of a solution containing 0.25 mL of 0.5% bupivacaine mixed with 0.25 mL of 40 mg/mL depomethylprednisolone was administered.
PRF Procedure
The radiofrequency procedures were performed whenever possible after 2 weeks of the first follow-up visit. At that time, better pain control was observed after the medial branch block. The radiofrequency procedures were performed in accordance with the previously published standards and techniques, at the spinal levels targeted for the diagnostic injections.15,16 To alleviate the procedure-related pain, superficial anesthesia was administered, along with light sedation as needed. With the image intensifier positioned in an ipsilateral oblique and sharp caudad-cephalad direction to maximize the lesion size in an orientation parallel to the course of the target nerve, 18-gauge curved radiofrequency needles with 10-mm active tips (RF Straight Cannula, Abbott, USA) were inserted in coaxial views until bone was contacted between the superomedial border of the transverse and superior articular processes, and with the inferior portion of the lateral neck of the superior articular process, with the convex surface apposed to the bone. For Lumbar 5 dorsal rami lesioning, the cannula was positioned in the crevice between the lateral aspect of the Sacral 1 articular process and the sacral ala. For each nerve, needles were adjusted to optimize the sensory and motor stimulations. For each nerve lesion, electrodes were inserted and adjusted until correct placement was confirmed by electrostimulation at 50 Hz, with the goal being concordant sensation at ≤0.5 V. Before denervation, multifidus stimulation and the absence of leg contractions were verified with electrostimulation at 2 Hz. After the optimal electrode placement was ascertained, 1 mL of 2% lidocaine was injected to reduce the procedure-related pain and enhance the lesion size. Ablation was then commenced at 42°C for 120 s with a radiofrequency generator (NT 1100TM Radiofrequency Generator Abbott Medical USA). At the completion of the lesioning, 10 mg of depomethylprednisolone mixed with saline (total, 0.5 mL) was administered at each site to reduce the risk of neuritis.17
Treatment Course and Follow-Up
For this study, 198 patients were selected. After medical branch block, the first follow-up was conducted 2 weeks later. Fifty patients received only a medial branch block, and 148 patients received a medial branch block and PRF according to the pain improvement. A positive block was defined as ≥50% pain relief sustained for at least 12 h. A good outcome was predesignated as a decrease of at least 50% in average back pain.15 The patients who did not have a good outcome after nerve block were not arranged for further PRF. The follow-up period was 1 year. The follow-up time points were 2 weeks after medial branch block, 1 month after PRF, 3 months after PRF, and 12 months after PRF. In the study, only 50 patients received a nerve block. In this group, a good outcome was defined as a decrease of at least 80% in back pain, and the patients were satisfied with the nerve block and continuously observed for further follow-up. During the follow-up, PRF was not needed. In the other patients in this group, nerve block showed no effect. The visual analog scale (VAS) score for pain was used in this study during the follow-ups. Health-related quality of life was assessed using Short form 36 (SF-36) before treatment and 1 year after treatment.
Clinical and Radiological Predictive Factors
The clinical and radiological predictive factors included age, sex, upper lumbar lordosis(ULL)(the angle between Thoracic 12 lower end plate and lumbar 2 lower end plate), middle lumbar lordosis(MLL)(the angle between Lumbar 2 lower end plate and Lumbar 4 upper end plate), lower lumbar lordosis(LLL)(the angle between Lumbar 4 upper end plate and Sacral 1 upper end plate), lumbar lordosis(LL)(the angle between Thoracic 12 lower end plate and Sacral 1 upper end plate), pelvic tilt(PT)(the angle subtended by a vertical line through the femoral heads axis and a line drawn from the midpoint of the sacral endplate to the femoral heads axis), pelvic incidence(PI)(an angle subtended by a line drawn from the femoral heads axis to the midpoint of the sacral endplate and a line perpendicular to the sacral endplate), sacral slope(SS)(the angle subtended by a horizontal reference line and the sacral endplate), number of involved facet joints, old compression fracture with/without vertebroplasty, lumbar laminectomy, lumbar discectomy, lumbar fusion, and adjacent facet joint pain after lumbar fusion.16
Statistical Analyses
The clinical characteristics of the patients with a good outcome and those with a poor outcome were compared using the independent sample t-test for continuous variable or the Fisher’s exact test for categorical variables. The variables whose significance was <0.2 were introduced into a multivariable logistic regression model with a backward elimination procedure. As the lumbar fusion and adjacent facet joint pain due to the lumbar fusion had high multicollinearity, we used two multivariable models that included the two variables separately. The aforementioned analyses were repeated with stratification of the receiving block only or both blocks and RF surgery. Further, the optimal degree to discriminate a poor outcome was assessed using the receiver-operating characteristic curve analysis. At last, the improvement of visual analog scale (VAS) and quality of life (SF-36) from baseline to follow ups between the good outcome and poor outcome groups was compared using the generalized estimating equation (GEE). A significant interaction term of “time by group” (good outcome and poor outcome) indicated a significant difference of the change value between the good outcome and poor outcome groups. All the tests were two-tailed, and a P value < 0.05 was considered statistically significant. Data analyses were conducted using SPSS 25 (IBM SPSS Inc, Chicago, Illinois).
Results
A total of 198 patients were included in the study, of whom 50 received nerve block only and 148 received a subsequent PRF. Of the patients, the men were less predominant (30%), and the mean age was 55.9 years (standard deviation: 15.7 years). The patients were divided into two groups as follows: those with good outcomes and those with poor outcomes. The patients with poor outcomes were older; had less lower lumbar lordosis, less lumbar lordosis, and sacral slope (SS); had more pelvic tilt and more involved facet joints; were more likely to have an old compression fracture with/without vertebroplasty; and had lumbar fusion and adjacent facet joint pain due to lumbar fusion. The patients with poor outcomes were more likely to receive nerve block only (36.9% vs 19.5%, P = 0.014; Table 1). The multivariable logistic model showed that a less lower lumbar lordosis, a higher number of involved facet joints, and both lumbar fusion and adjacent facet joint pain due to lumbar fusion were associated with the risk of poor outcome (Table 2).
 |
Table 1 The Clinical Characteristic of Patient with Good Outcome versus with Poor Outcome |
 |
Table 2 Univariate and Multivariable Analysis for Factor Associated with the Risk of Poor Outcome |
Of the patients with nerve block only, 52% (26/50) had good outcomes and 48% (24/50) had poor outcomes. The patients with poor outcomes tended to have less lower lumbar lordosis and less lumbar lordosis, more pelvic tilt, and more involved facet joints (Table 3). The multivariable logistic model demonstrated that a less lumbar lordosis and more pelvic tilt were associated with the risk of poor outcomes (Table 4).
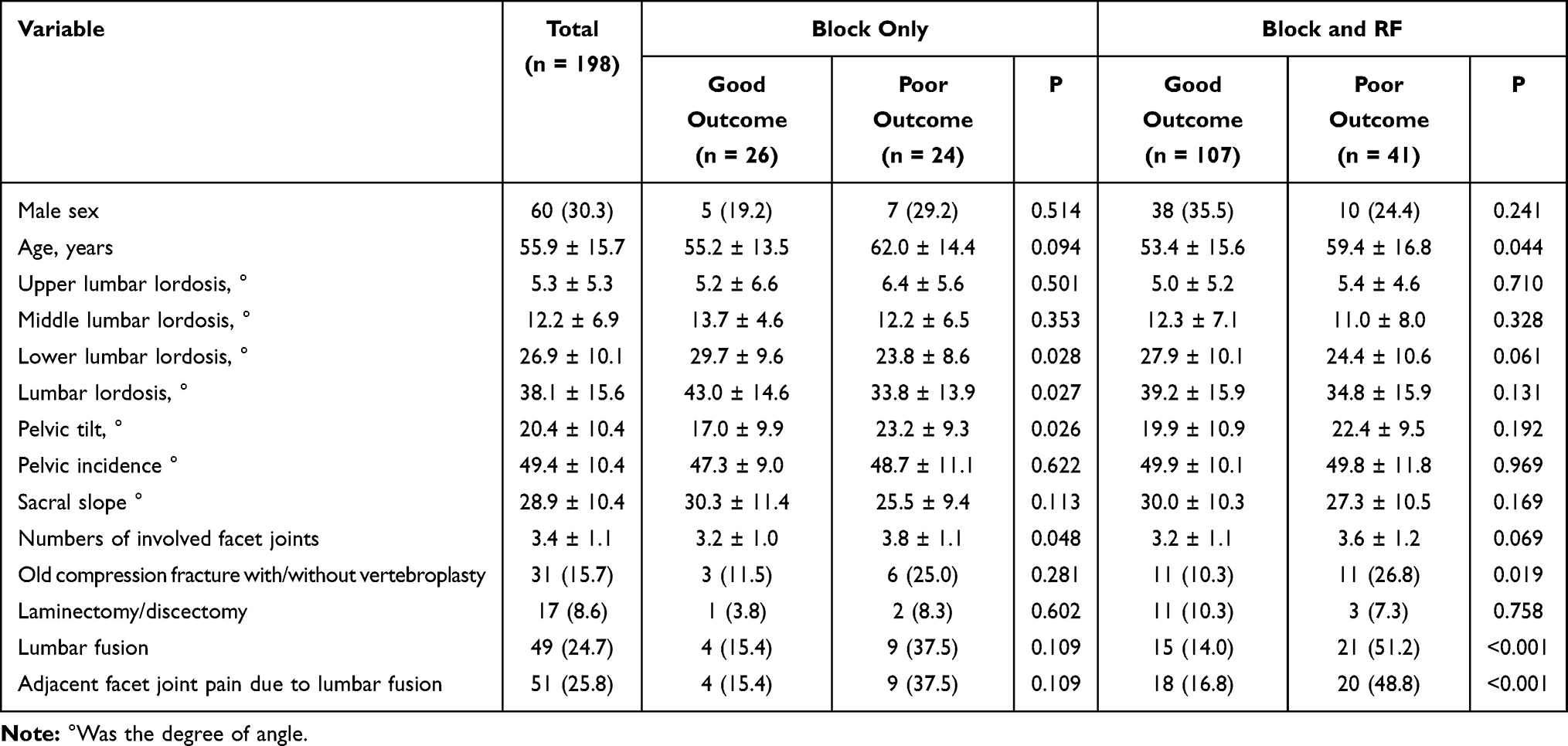 |
Table 3 The Clinical Characteristic of Patient with Good Outcome versus with Poor Outcome Stratified by Receiving Block Only or Both Block and PRF |
 |
Table 4 Univariate and Multivariable Analysis for Factor Associated with the Risk of Poor Outcome Stratified by Receiving Block Only or Both Block and PRF |
In the patients who received a subsequent PRF, 72% (107/148) had good outcomes and 28% (41/148) had poor outcomes. The patients with poor outcomes tended to be older, were more likely to have an old compression fracture with/without vertebroplasty, and had lumbar fusion and adjacent facet joint pain due to lumbar fusion (Table 3). The multivariable logistic model suggested that a higher number of involved facet joints and both lumbar fusion and adjacent facet joint pain due to lumbar fusion were associated with the risk of poor outcome (Table 4).
For the patients with nerve block only, the discrimination ability of lumbar lordosis was 68.2% (95% confidence interval [CI], 53.2%–83.2%), with ≤ 45° as the optimal cutoff. By contrast, the discrimination ability of pelvic tilt was 70.4% (95% CI, 55.3–85.4), with >23.5° as the optimal cutoff. For the patients who received a subsequent RF surgery, the discrimination ability of lower lumbar lordosis was 61.0% (95% CI, 52.7%–69.3%), with ≤29° as the optimal cutoff (Table 5).
 |
Table 5 Discrimination Property of the Degrees in Patients Who Receiving Block Only and Both Block and PRF |
We collected the VAS during the 1st, 3rd, 6th and 12th month. The result showed that patients who had a poor outcome did not have an improvement across the follow ups in either the nerve block only group or both surgery group (Figure 1A and B). We also collected the quality of life scale (SF-36) before the surgery and the 12th month after surgery. The result demonstrated that patients who had a poor outcome had few improvement at the 12th month after surgery in either groups (Figure 1C and D).
 |
Figure 1 The mean and 95% confidence interval of VAS of the good outcome and poor outcome groups across the measurements in patients who received block only (A) or both block and PRF (B). The asterisk “*” indicates a significant interaction between the two outcome groups. The mean and 95% confidence interval of SF-36 of the good outcome and poor outcome groups across the measurements in patients who received block only (C) or both block and PRF (D). The asterisk “*” indicates a significant interaction between the two outcome groups. |
Discussion
Minimally invasive techniques have proven their effectiveness and safety in the relief of lower back pain caused by lumbar facet joint diseases. Pulsed radiofrequency in the medial branches is currently the best treatment option for managing the pain of facet joint origin, and excellent improvements in pain control and functional outcomes have been reported.13,17–20 Appropriate patient selection and the correct anatomical placement of electrodes for PRF have been described as important outcomes. In recent years, there have been several studies on the sagittal balance and clinical outcomes in the treatment of degenerative lumbar diseases.21–23 However, no study has investigated the predictive factors for performing such a treatment from the perspective of the clinical and radiological conditions.
From our results, we found that lower lumbar lordosis, lumbar lordosis, and pelvic tilt were predictive factors. Other studies showed that increased pelvic incidence may lead to facet joint arthritis at the lower lumbar spine, and the pelvic incidence (PI) may increase to compensate for a decrease in the lumbar lordosis.24–26 Facet joint pain may arise due to several misbalanced forces such as increased lumbar lordosis, which leads to higher forces on the facet joints, and lumbar lordosis showed a significant linear association with facet joint arthritis.27–29 Hence, both decreased and increased lumbar lordosis could cause facet joint pain. The normal average lordosis was reported to be approximately 55° (range, 35°–80°) from the T12 up to the S1 spine levels in the “Essentials of spinal deformities”.30 Several studies showed no significant correlation between the degree of lumbar lordosis and facet joint degeneration.31–33 Only one study has been conducted to investigate lower back pain and spinopelvic radiological parameters, and it showed that increased pelvic tilt and decreased lumbar lordosis were associated with lower back pain.34 However, the good outcome group in our study had greater lumbar lordosis with a cut-off point of 45°, and this could be explained by the clinical conditions. The clinical predictive factors were old compression fracture and lumbar fusion with adjacent facet joint pain. The presence of an old compression fracture and lumbar fusion decreased the degree of lumbar lordosis. Of the patients with poor outcomes, > 50% had an old compression fracture and lumbar fusion.
Zhu et al reported an average pelvic tilt of 11.2° in asymptomatic individuals. Compared with this value, the average pelvic tilt was relatively high in our patients with facet joint pain.30,35 The result was similar to those reported in other studies.36,37 In our study, the cut-off point was 23.5°.
Our results showed that lower lumbar lordosis was a predictor, and it has not yet been discussed. From our data, 177 of the 198 patients had facet joint pain below the L3 level, and facet joint pain in the lower lumbar spine comprised the majority of cases. The lower lumbar spine, defined as the spine from the upper endplate of the fourth lumbar vertebra to the sacrum, is the most important part for determining lumbar lordosis.38,39 In addition, it is the most common surgical site in degenerative spinal diseases.40 The good outcome group had more lower lumbar lordosis with a cut-off point of 29°.
Percutaneous vertebroplasty (PV) has proven to be an effective treatment for back pain caused by vertebral compression fractures. However, some patients continue to experience substantial back pain even after PV. Subsequent or persistent back pain may be due to a failed procedure, a new compression fracture other than the one at the treated vertebral level, or another new or old pain generator such as the sacroiliac or facet joints;38–41 in our study, we excluded persistent back pain after a compression fracture and the sacroiliac joint, disc degeneration, and muscles as pain sources. We investigated the predictive factors for subsequent facet joint pain after a compression fracture, and the pain is associated with recurrent pain after a compression fracture and PV.39–42 A literature review revealed different results in pain relief after facet joint injection. In our study, 16 of 31 patients underwent vertebroplasty, and only three patients had facet joint pain at the compression sites. This could be explained by the fact that anatomical changes associated with the fracture deformity may adversely affect the facet joints. Radiological analysis of the anatomical changes and sagittal alignment of the spine revealed that these caused less severe lower lumbar lordosis, lumbar lordosis, and increased pelvic tilt.
Facet joints may be associated with pain after spinal surgery in several ways. These joints may continue to degenerate after a surgical procedure for the treatment of a herniated disc or spondylolisthesis at the same spinal level. Surgery may change the loading or movement patterns of these joints, leading to degeneration and pain. Our results showed that only the lumbar fusion procedure was associated with the outcome. After spinal fusion at one spinal level, the motion of the adjacent level(s) may be altered to compensate for the changes caused by the fusion. This change in motion pattern may cause facets at the adjacent segment(s) to degenerate and become painful.43 From our results, 30 of 65 patients with a poor outcome received lumbar fusion, and the radiological data showed less severe lumbar lordosis and lower lumbar lordosis in the poor outcome group. Hence, the radiological analysis revealed that the fusion procedures caused less severe lumbar lordosis, lower lumbar lordosis, and increased pelvic tilt. In our study, we also recorded the adjacent joint pain, and all patients who underwent fusion had adjacent facet joint pain. Adjacent degeneration was a possible complication of fusion procedures.
However, the results showed that discectomy and laminectomy were not risk factors. These procedures may not have changed the sagittal alignment of the spine. We evaluated the quality of life of patients after treatment using the SF-36 questionnaire (functional capacity, physical aspects, pain, general health status, vitality, social aspects, emotional aspects, and mental health). The SF-36 data were essentially identical, meaning that poor outcomes would cause extensive effects on these aspects, including the functional capacity, physical aspects, general health status, vitality, social aspects, emotional aspects, and mental health, in addition to pain.44
Conclusion
This study provides a scientific basis for the use of PRF in the treatment of lumbar facet joint pain. Our study results, particularly those of the analysis, showed that the clinical predictive factors were the number of facet joints, compression fractures, and lumbar fusion, and the radiological factors were more lower lumbar lordosis (> 29°), more lumbar lordosis (> 45°), and less pelvic tilt (< 23.5°).
Abbreviations
CLBP, chronic lower back pain; CT, computed tomography; MRI, magnetic resonance imaging; PRF, pulsed radiofrequency; VAS, visual analog scale; SF-36, Short form 36; ULL, upper lumbar lordosis; MLL, middle lumbar lordosis; LLL, lower lumbar lordosis; LL, lumbar lordosis; PT, pelvic tilt; PI, pelvic incidence; SS, sacral slope; PV, Percutaneous vertebroplasty.
Acknowledgments
This study was supported by the Research Program of E-DA cancer hospital (EDCHP-106006).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Support was provided solely from institutional and/or departmental sources.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Prevalence of disabilities and associated health conditions among adults: United States. From the Centers for Disease Control and Prevention. Prevalence of disabilities and associated health conditions among adults--United States, 1999. JAMA. 2001;285(12):1571–1572.
2. Hancock MJ, Maher CG, Latimer J, et al. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eruv Spine J. 2007;16(10):1539–1550.
3. Abdurrahman Çetin A, Yektas A. Evaluation of the short- and long-term effectiveness of pulsed radiofrequency and conventional radiofrequency performed for medial branch block in patients with lumbar facet joint pain. Pain Res Manag. 2018;2018:7492753.
4. Revel M, Poiraudeau S, Auleley GR, et al. Capacity of the clinical picture to characterize low back pain relieved by facet joint anesthesia. Proposed criteria to identify patients with painful facet joints. Spine. 1998;23(18):1972–1976.
5. Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The false-positive rate of uncontrolled diagnostic blocks of the lumbar zygapophysial joints. Pain. 1994;58(2):195–200.
6. Hammer M, Meneese W. Principles and practice of radiofrequency neurolysis. Curr Rev Pain. 1998;2(4):267–278.
7. Sluijter ME, van Kleef M. Pulsed radiofrequency. Pain Med. 2007;8(4):388–389.
8. Manchikanti L, Pampati V, Fellows B, Baha AG. The inability of the clinical picture to characterize pain from facet joints. Pain Phys. 2000;3(2):158–166.
9. Manchikanti L, Pampati V, Fellows B, Bakhit CE. Prevalence of lumbar facet joint pain in chronic low back pain. Pain Phys. 1999;2(3):59–64.
10. van Kleef M, Vanelderen P, Cohen SP, Lataster A, Van Zundert J, Mekhail N. Pain originating from the lumbar facet joints. Pain Pract. 2010;10:459–469.
11. Cohen SP, Raja SN. Pathogenesis, diagnosis, and treatment of lumbar zygapophysial (facet) joint pain. Anesthesiology. 2007;106:591–614.
12. Manchikanti L, Datta S, Gupta S, et al. A critical review of the American Pain Society clinical practice guidelines for interventional techniques: part 2. Therapeutic interventions. Pain Phys. 2010;13:E215–E264.
13. Falco FJ, Manchikanti L, Datta S, et al. An update of the effectiveness of therapeutic lumbar facet joint interventions. Pain Phys. 2012;15:E909–E953.
14. Gofeld M, Jitendra J, Faclier G. Radiofrequency denervation of the lumbar zygapophysial joints: 10-year prospective clinical audit. Pain Phys. 2007;10:291–300.
15. Cohen SP, Doshi TL, Constantinescu OC, et al. Effectiveness of lumbar facet joint blocks and predictive value before radiofrequency denervation anesthesiology: the Facet Treatment Study (FACTS), a randomized, controlled clinical trial. Pain Med. 2018;129(3):517–535.
16. Cohen SP, Williams KA, Kurihara C, et al. Multicenter, randomized, comparative cost-effectiveness study comparing 0, 1, and 2 diagnostic medial branch (facet joint nerve) block treatment paradigms before lumbar facet radiofrequency denervation. Anesthesiology. 2010;113:395–405.
17. Martinez-Suarez JE, Camblor L, Salva S, De Jongh WA. Termocoagulación facetaria lumbar. Experiencia en 252 pacientes. Revista de la Sociedad Española del Dolor. 2005;12:425–428.
18. McCormick ZL, Marshall B, Walker J, McCarthy R, Walega DR. Long-term function, pain and medication use outcomes of radiofrequency ablation for lumbar facet syndrome. Int J Anesth. 2015;2:028.
19. Civelek E, Cansever T, Kabatas S, et al. Comparison of effectiveness of facet joint injection and radiofrequency denervation in chronic low back pain. Turk Neurosurg. 2012;22:200–206.
20. Tomé-Bermejo F, Barriga-Martín A, Martín JLR. Identifying patients with chronic low back pain likely to benefit from lumbar facet radiofrequency denervation: a prospective study. J Spinal Disord Tech. 2011;24:69–75.
21. Le Huec JC, Faundez A, Dominguez D, Hoffmeyer P, Aunoble S. Evidence showing the relationship between sagittal balance and clinical outcomes in surgical treatment of degenerative spinal diseases: a literature review. Int Orthop. 2015;39(1):87–95.
22. Lv X, Liu Y, Zhou S, et al. Correlations between the feature of sagittal spinopelvic alignment and facet joint degeneration: a retrospective study. BMC Musculoskelet Disord. 2016;17(1):341.
23. Bassani T, Casaroli G, Galbusera F. Dependence of lumbar loads on spinopelvic sagittal alignment: an evaluation based on musculoskeletal modeling. PLoS One. 2019;14(3):e0207997.
24. Jentzsch T, Geiger J, Bouaicha S, Slankamenac K, Tdl N-K, Werner CML. Increased pelvic incidence may lead to arthritis and sagittal orientation of the facet joints at the lower lumbar spine. BMC Med Imaging. 2013;13:34.
25. Hanson DS, Bridwell KH, Rhee JM, Lenke LG. Correlation of pelvic incidence with low- and high-grade isthmic spondylolisthesis. Spine (Phila Pa 1976). 2002;27(18):2026–2029.
26. Mendoza-Lattes S, Ries Z, Gao Y, Weinstein SL. Natural history of spinopelvic alignment differs from symptomatic deformity of the spine. Spine (Phila Pa 1976). 2010;35(16):792–798.
27. Kirkaldy-Willis WH, Paine KW, Cauchoix J, McIvor G. Lumbar spinal stenosis. Clin Orthop Relat Res. 1974;99:30–50.
28. Adams MA. Hutton WC The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J Bone Joint Surg Br. 1980;62(3):358–362.
29. Jentzsch T, Geiger J, König MA, Werner CML. Hyperlordosis is associated with facet joint pathology at the lower lumbar spine. Clin Spine Surg. 2017;30(3):129–135.
30. Heary RF, Albert TJ. Spinal Deformities: The Essentials. New York: Thieme Medical Publishers; 2007.
31. Ashraf A, Farahangiz S, Jahromi BP, Setayeshpour N, Naseri M, Nasseri A. Correlation between radiologic sign of lumbar lordosis and functional status in patients with chronic mechanical low back pain. Asian Spine J. 2014;8(5):565–570.
32. Chaleat-Valayer E, Mac-Thiong JM, Paquet J, Berthonnaud E, Siani F, Roussouly P. Sagittal spinopelvic alignment in chronic low back pain. Eur Spine J. 2011;20(Suppl 5):634–640.
33. Kang KB, Kim YJ, Muzaffar N, Yang JH, Kim YB, Yeo ED. Changes of sagittal spinopelvic parameters in normal Koreans with age over 50. Asian Spine J. 2010;4:96–101.
34. Patil S, Jayakumar T. Spino-pelvic radiological parameters in patients presenting with low back pain in a tertiary care centre in India. Int J Orthop Sci. 2019;5(2):172–176.
35. Zhu Z, Xu L, Zhu F, et al. Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations. Spine. 2014;39(1):E1–E6.
36. Lv X, Liu Y, Zhou S, et al. Correlations between the feature of sagittal spinopelvic alignment and facet joint degeneration: a retrospective study. BMC Musculoskelet Disord. 2016;17:341.
37. Barrey C, Jund J, Noseda O, Roussouly P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about 85 cases. Eur Spine J. 2007;16(9):1459–1467.
38. Liliang P-C, Lu K, Shen S-H. Persistent back pain after percutaneous vertebroplasty. Pain Med. 2015;16:554–557.
39. Kamalian PS, Bordia R, Ortiz AO. Post-vertebral augmentation back pain: evaluation and management. Am J Neuroradiol. 2012;33(2):370–375.
40. Manchikanti L, Singh V, Falco FJ, et al. Evaluation of lumbar facet joint nerve blocks in managing chronic low back pain: a randomized, double-blind, controlled trial with a 2-year follow-up. Int J Med Sci. 2010;7:124–135.
41. Boswell MV, Colson JD, Sehgal N, et al. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Phys. 2007;10:229–253.
42. Staal JB, de Bie RA, de Vet HC, et al. Injection therapy for subacute and chronic low back pain: an updated Cochrane review. Spine (Phila Pa. 1976;2009(34):49–59.
43. Hochschuler S. Facet Joint Pain After Spine Surgery. Texas Back Institute.
44. Adorno ML, Brasil-Neto JP. Assessment of the quality of life through the SF-36 questionnaire in patients with chronic nonspecific low back pain. Acta Ortop Bras. 2013;21(4):202–207.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.