Back to Journals » Cancer Management and Research » Volume 13
Opportunistic Detection for Pancreatic Cystic Lesions During Chest Multidetector CT Scans for Lung Cancer Screening
Authors Chen X ![]() , Yu Z, Wang J, Cui W
, Yu Z, Wang J, Cui W ![]() , Cui C, Wang Y, Liu Y, Zhou H
, Cui C, Wang Y, Liu Y, Zhou H ![]() , Wang C, Wang Z, Chen X
, Wang C, Wang Z, Chen X
Received 9 July 2021
Accepted for publication 14 September 2021
Published 2 October 2021 Volume 2021:13 Pages 7559—7568
DOI https://doi.org/10.2147/CMAR.S327022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Xin Chen,1,2,* Zhicheng Yu,1,3,* Jianhua Wang,1 Wenjing Cui,1 Can Cui,1 Yajie Wang,1 Yongkang Liu,1 Hao Zhou,1 Cheng Wang,4 Zhongqiu Wang,1 Xiao Chen1
1Department of Radiology, The Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 2Department of Radiology, Shanghai Jiaotong University Affiliated Sixth People’s Hospital, Shanghai, 200233, People’s Republic of China; 3Department of Radiology, Jiading Central Hospital, Shanghai University of Medicine & Health Sciences, Shanghai, 201800, People’s Republic of China; 4Department of Radiology, Nanjing Drum Tower Hospital the Affiliated Hospital of Nanjing University Medical School, Nanjing, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhongqiu Wang; Xiao Chen
Department of Radiology, The Affiliated Hospital of Nanjing University of Chinese Medicine, 155 Hanzhong Road, Nanjing, 210029, People’s Republic of China
Tel +86-025-86619843
Email [email protected]; [email protected]
Purpose: The purpose of this study was to analyze the prevalence of and risk factors for incidental pancreatic cystic lesions (PCLs) in the Chinese general population. Furthermore, the association between baseline imaging findings and PCL progression was also investigated.
Patients and Methods: A total of 9826 individuals who underwent computed tomography (CT) examinations for lung cancer screening between January 1, 2018 and January 1, 2019 were included in this study. The participants’ CT imaging findings and biochemical biomarker levels were reviewed and analyzed. PCLs detected during the screening were followed up for 12 months. Associations between imaging findings and clinical factors with PCL progression were explored.
Results: PCLs were observed in 172 of the 9826 participants. The crude prevalence of PCLs in total population was 1.75%. In subjects aged > 60 years, the prevalence of PCLs was 3.2% (102/3151). The occurrence of PCLs was significantly increased with an increase of age in both men and women (p < 0.001). High-risk PCLsL commonly located in pancreatic head showed extrapancreatic growth, and had high urea levels (p = 0.005, p = 0.015, p = 0.002, respectively) compared with low-risk PCLs. Location in the pancreatic head (odds ratio (OR) = 6.286, 95% confidence interval (CI): 1.842– 21.452) and extrapancreatic growth (OR = 4.049, 95% CI: 1.235– 13.333) were risk factors for PCL progression.
Conclusion: PCLs are not uncommon in the Chinese general population. Location in the pancreatic head and extrapancreatic growth are the independent predictors of high-risk of PCLs and PCL progression.
Keywords: pancreatic cystic lesion, computed tomography, prevalence, progression, Chinese population
Introduction
Pancreatic cystic lesions (PCLs) comprise several different entities and each of them exhibits peculiar biological behaviors ranging from benign to premalignant or frankly malignant neoplasms.1 Most encountered cysts are neoplastic lesions.2 and the mucinous form of PCLs has malignant potential.3 Intraductal papillary mucinous neoplasm (IPMN) is the most common PCLs.4 The prevalence of malignant IPMNs (high-grade dysplasia and invasive carcinoma) was 11–30% in side-branch IPMNs and 62% in main duct involving IPMNs.4 PCLs were also considered one of the precursors for pancreatic cancer. The risk of pancreatic malignancies is higher in patients with PCLs than in those without them.2 Early detection of those precursors would be valuable because the low 5-year survival rate of pancreatic cancer.
Interestingly, the detection rate of PCLs is increasing due to the wide use of ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) in physical or medical examinations.1,3 The reported prevalence of PCLs ranged from 1.5% to 44.7% across different population and using different imaging modalities.5–8 However, most of the studies on PCLs were performed on inpatients and outpatients. The prevalence of PCLs in the general population, particularly in China, has not been clarified. In 2013, the International Cancer of the Pancreas Screening (ICAPS) consortium recommended performing pancreatic cancer screening in high-risk populations.9 Recently, US Preventive Services Task Force (USPSTF) reported a recommendation “Screening for Pancreatic Cancer US Preventive Services Task Force Reaffirmation Recommendation Statement” in JAMA.10 They recommend against the screening for pancreatic cancer in asymptomatic adults after reviewing the benefits and harms of the screening. Therefore, an alternative approach for PCL detection must be identified.
CT screening for lung cancer is available in several parts of the world which may present an opportunity to use CT data to identify or monitor progression of PCLs with no additional radiation exposure or cost. Age and cigarette smoking exposure are the two critical risk factors for lung cancer screening. Expanding screening eligibility criteria may be applicable in China because of air pollution and huge number of non-smoking female population.11 CT is also recommended in patients with PCLs by European expert pancreatologists.12 In the present study, we showed the prevalence of PCLs in subjects who underwent CT screening for lung cancer. The progression of PCLs is associated with risk of malignancy and health management. Furthermore, we preliminarily explored the predictive factors for lesion progression during a 12-month follow-up.
Materials and Methods
Patients and Data Collection
This study was approved by the Ethics Committee of Jiangsu Province Hospital of Chinese Medicine. The informed consent was waived by the Ethics Committee because this was a retrospective study. A total of 10,130 individuals who underwent chest CT for lung cancer screening between January 1, 2018 and January 1, 2019 were found in our institution. Those subjects were excluded: (1) imaging data or clinical data were incomplete, (2) the pancreas and duodenum area were not scanned, (3) who had a known or suspected history of pancreatic solid tumor, (4) who had history of surgical treatment for pancreatic diseases, (5) image quality was poor that did not meet the requirements for clinical diagnosis.
In order to reduce the interference of pancreatitis-related pseudocysts, subjects with any conditions as follows were also excluded:
- Subjects who had medical history of pancreatitis.
- Subjects showed both significant pancreatic atrophy, fibrosis or had multiple classifications on CT.
Finally, a total of 9826 individuals were enrolled in this study. Declaration of Helsinki was followed during the study.
Imaging Technique
The CT scans were performed using the following multi-slice spiral CT machines: 16-channel CT scanner (Sensation 16, Siemens Healthcare, Erlangen, Germany; Brilliance 16, Philips Healthcare, Cleveland, OH), 64-channel CT scanner (Brilliance 64, Philips Healthcare, DA Best, the Netherlands; Optima CT660, GE Healthcare, Milwaukee, WI, USA; Optima CT680, GE Health-care, Milwaukee, WI, USA), and 128-channel CT scanner (Brilliance ICT, Philips Healthcare, Cleveland, OH, USA).
Detector collimations of 0.75, 0.625, and 0.625 mm were used for 16-, 64- and 128-detector CT scanner, respectively. Other imaging parameters were shown as follows: Pitch of 0.9–1.5, 2.5–3 mm section thickness, matrix of 512 × 512, gantry rotation time of 0.5–0.75 s, tube voltage of 120 kV, and automated tube current modulation (200–400 mA) with a noise index.
For contrast-enhanced examinations, a total of 1.5 mL/kg of non-ionic contrast agent with different iodine concentrations (300–350 mg/mL) was injected using a power injector at a rate of 3–4 mL/s via an intravenous catheter, followed by a 20-mL flush of sterile saline. Then, arterial phase, portal venous phase, delayed-phase images were acquired at approximately 30–35 s, 55–60 s, 120–180 s after contrast agent injection, respectively. Images were reconstructed at 2-mm intervals with a 2-mm section thickness.
Imaging Analysis
Every abdominal image was reviewed to identify the presence of PCLs. The following criteria were used to define PCLs based on a previous study:13 round or oval shape and with a relatively clear boundary, short diameter ≥5mm, and average CT value between −10HU and 20HU. The maximum cyst diameter, cyst location, number of lesions, pancreatic duct dilatation, lesion calcification and cyst growth pattern were obtained. For multiple cysts, the characteristics of the largest cyst were recorded for further analysis. Pancreatic duct dilatation was considered if diameter was greater than 3 mm.14 The pancreatic head was defined as the part of pancreatic gland located on the right side of the superior mesenteric vein, and the body of the pancreas was defined as a part located on the left side of the superior mesenteric vessels. The tail was defined as the distal aspect of the pancreas that extended into the splenic hilum. If the lesion was too large, the location of the lesion was judged by the location of the cyst center. Endogenous growth of PCLs was defined when the center of the lesion was within the contour of pancreas, otherwise extrapancreatic growth was considered. We also calculated the liver/pancreas and pancreas/spleen CT value ratio and spleen. The research flow diagram is presented in Figure 1.
 |
Figure 1 The flow diagram of this study. 9826 subjects were included. 172 PCLs were observed and 107 of them was followed up for 12 months. |
Definition of High-Risk PCLs
In addition, PCLs with different characteristics have different management strategies. In order to estimate the associated factors of high-risk PCLs, we divided the individuals into high-risk and low-risk according to the ACG Clinical Guidelines15 released in 2017 and the system review that focused on the management of neoplastic pancreatic cysts.16 Those lesions were considered high-risk group: cyst size was greater than 3 cm; the diameter of main pancreatic (MPD) was greater than 5 mm.
Follow-Up
We also performed a 12-month follow-up on those subjects with PCLs. Individuals who lost to follow-up on radiology or underwent pancreatic surgery after baseline examination were excluded from the follow-up study. The cysts were categorized into two groups according to their longest diameter at initial scans: 5 mm ≤ cysts <15 mm and ≥15 mm. The progression was defined based on the recommendations of the latest White Paper of the American College of Radiology incidental Findings Committee:17 for baseline PCLs with a size of 5–15 mm, an increased size of 50% or more; for baseline PCLs with a size more than 15 mm, an increased size of 20% or more. An increase in PCLs number was also considered as progression. To explore the predictors of PCL progression, participants were categorized into two groups: progression group and stable group (Figure 1).
 |
Figure 2 The association between prevalence of pancreatic cystic lesions (PCLs) and age and location. (A) in total population; (B) in female and male population; (C) prevalence of PCLs in different parts of the pancreas. |
Statistical Analysis
To explore the association between prevalence of PCLs and age, individuals were categorized according to gender and age (18–29, 30–39, 40–49, 50–59, 60–69, 70–79 and over 80 years). Qualitative data were expressed as counts and percentage, and were analyzed using the Chi-square test or Fisher’s exact test. Quantitative data were analyzed for normality using the Kolmogorov–Smirnov test. Those parameters showing a normal distribution were expressed as mean ± standard deviation and analyzed using Student’s t test, and the other data showing non-normal distribution were expressed as median with the interquartile range (IQR) and analyzed using Mann–Whitney U-test. Continuous variables were converted into categorical variables using optimal cut-off values and logistic regression analysis was performed to determine independent risk factors or predictors. Based on the associated factors, predictive models were established. In addition, receiver operating characteristic curve (ROC) was used to evaluate the diagnostic performance for the predictive model. A p value <0.05 was used to indicate a statistical significance. All statistical analyses were performed using commercially available software (SPSS 24.0 for Windows; Chicago, USA).
Results
Characteristics of Subjects
There were 5949 men and 3877 women. The age distribution showed similar trends in men and women. The median age was 53 years in men and 51 years in women. Patients with incidental PCLs seemed older than those without PCLs (median age 63 vs 52 years, p < 0.05)(Table 1). Patients with PCLs tended to have higher liver/spleen CT value ratio and lower pancreas/spleen CT value ratio than those without PCLs (p < 0.05). Statistical differences in alkaline phosphatase (AKP), alanine aminotransferase (ALT), serum creatinine (Scr) and blood glucose (Glu) were observed between the patients with and without PCLs (p = 0.013, 0.003, 0.007 and 0.001, respectively).
Prevalence and Associated Factors of PCLs
PCLs were identified in 172 cases among 9826 individuals. The prevalence of PCLs in the study population was 1.75%. The prevalence was significantly increased with age (p < 0.001) (Table 1). The age-specific prevalence of incidental PCLs in 18–29, 30–39, 40–49, 50–59, 60–69, 70–79 and 80- age groups was 0.7%, 0.6%, 0.6%, 1.9%, 1.9%, 4.3% and 6.6%, respectively (Figure 2A). No gender predominance was observed in the total prevalence and age-specific prevalence (Figure 2B). 60% of PCLs occurred in pancreatic body-tail. The tumor location-specific prevalence of incidental PCLs was 0.31% in head, 0.38% in neck, 0.69% in body and 0.39% in tail, respectively (Figure 2C). The characteristics of the pancreatic cystic neoplasms at baseline examination are presented in Table 2. The median tumor size was 10.66 mm (IQR: 8.32, 15.93). One hundred and forty-four (83.7%) cases showed endogenous growth and 23 (13.4%) cases had pancreatic duct dilatation and 5 (2.9%) lesions had calcification. In multivariate logistic analysis, patient’s age and ratio of CT value between liver and spleen were independent risk factor for PCLs (p < 0.01).
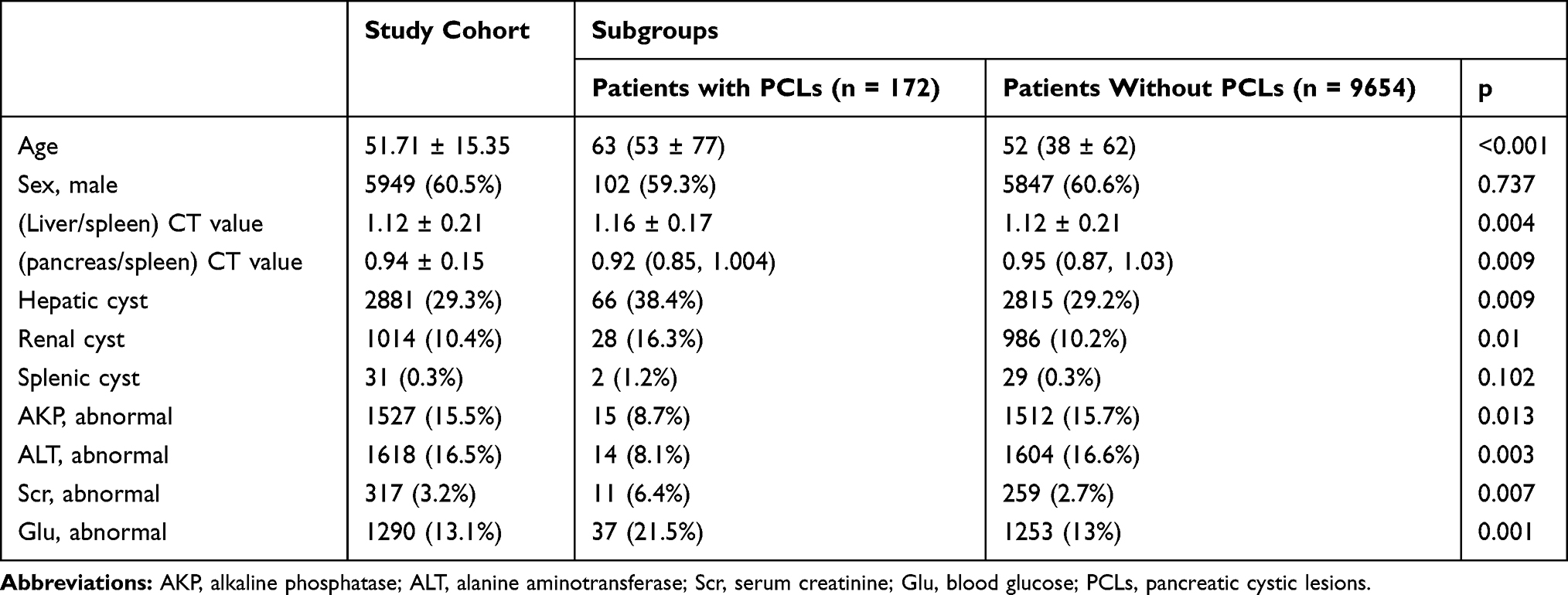 |
Table 1 Characteristics of Study Population |
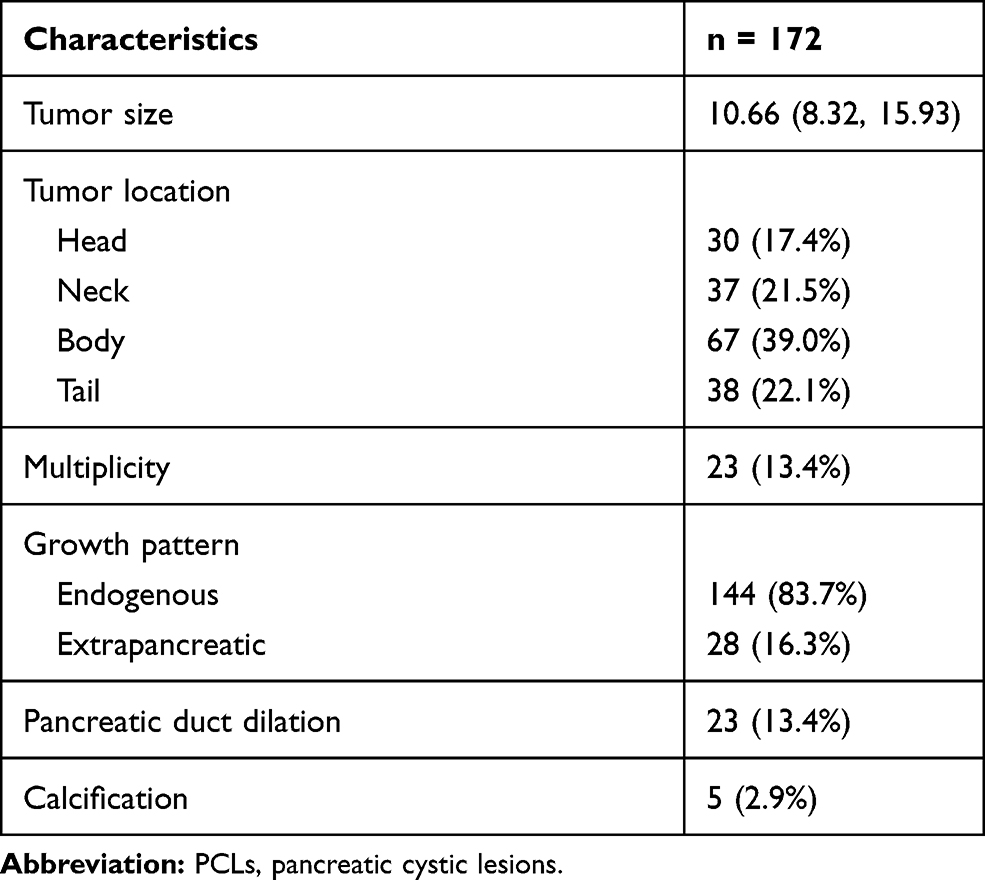 |
Table 2 CT Imaging Characteristics of PCLs |
 |
Figure 3 The operating receiver curves for identifying high-risk pancreatic cystic lesions (PCLs) (A) and PCL progression (B) based on potential associated factors. The area under the curve was 0.799 (95% CI:0.681–0.918) and 0.862 (95% CI:0.758–0.939). |
Associated Factors of High-Risk PCLs
For subjects with high-risk PCLs, 12 cases had pancreatic duct dilatation (>3.mm) and 3 cases had cyst size > 3cm, and 1 patient had both above risk factors. We further analyzed the differences between patients with high-risk PCLs (n = 14) and low-risk PCLs (n = 158) (Table 3). High-risk PCLs tended to have lower pancreas/spleen CT value ratio and were more likely to be located in the pancreatic head (71.4%) than low-risk PCLs (p = 0.036 and p = 0.005, respectively). In addition, high-risk PCLs usually exhibited extrapancreatic growth pattern (42.9%), and the low-risk PCLs usually showed endogenous growth pattern (86.1%) (p = 0.015). Biochemical data showed that abnormal serum creatinine and urea were more common in high-risk group (p = 0.048 and p = 0.002, respectively) than in the low-risk group. Multivariate regression analysis showed that urea, tumor location, and growth pattern were independent associated factors for the high risk of PCLs (all p < 0.01) after adjusting with modifiers, such as liver function and diabetes. ROC curve analysis showed that the above factors had potential to identify high-risk PCLs [area under the curve (AUC) = 0.799, 95% confidence interval (CI): 0.681–0.918, with a sensitivity of 92.9% and a specificity of 53.2%] (Figure 3A). Cases of high-risk PCLs are shown in Figure 4A–C).
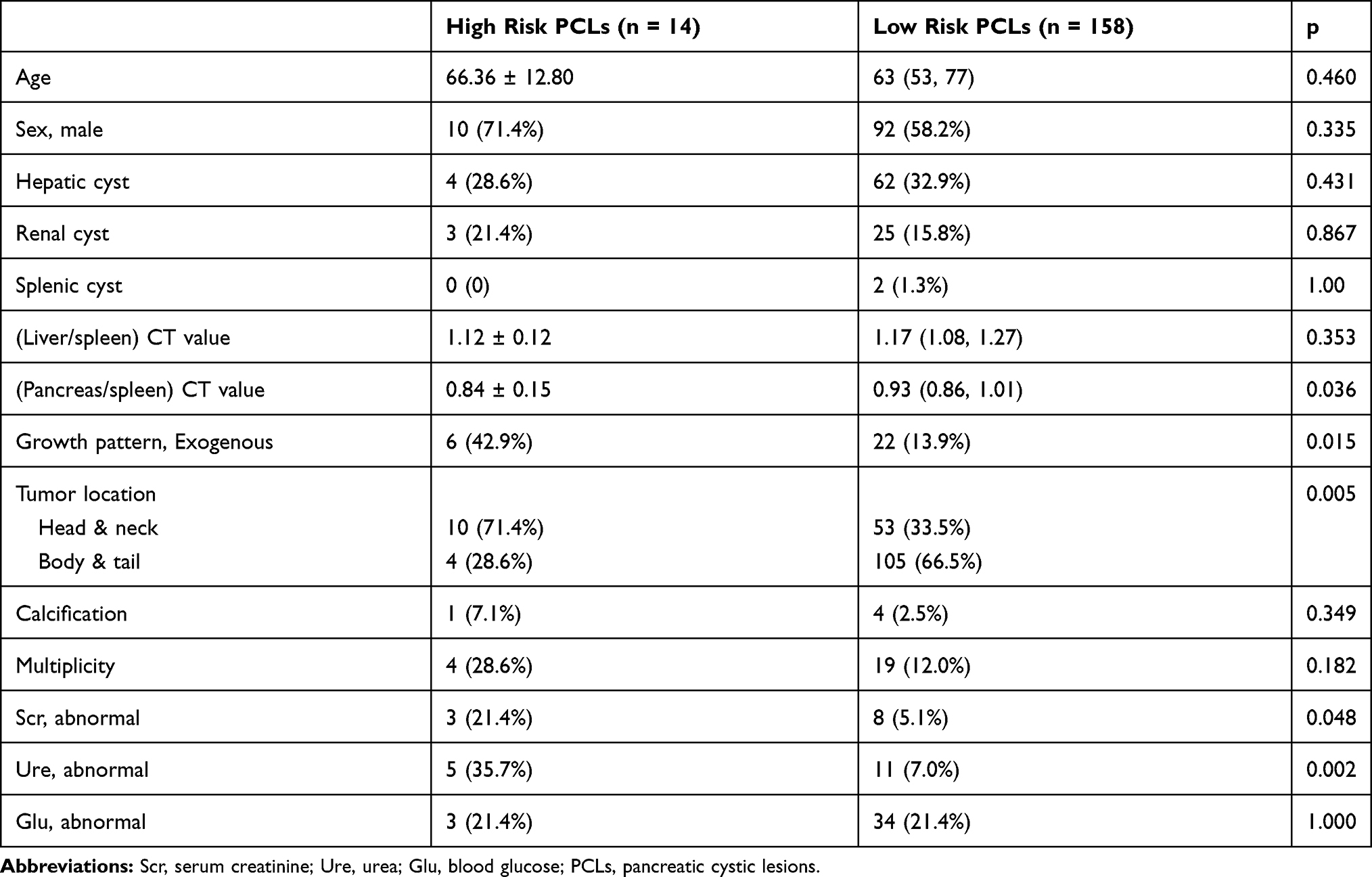 |
Table 3 Characteristics of Study Population with High-Risk and Low-Risk PCLs |
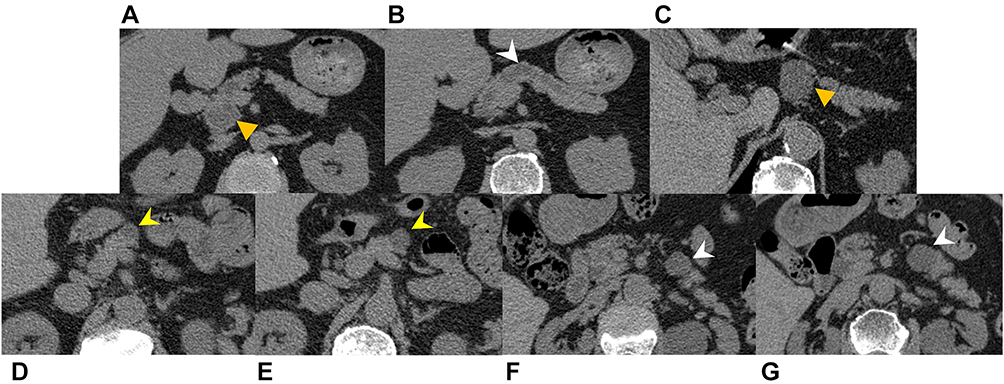 |
Figure 4 Two Cases of high-risk pancreatic cystic lesions (PCLs): case 1 had a 2.67 cm lesion located in the pancreatic head (yellow arrow triangle) (A) and a 0.95 cm of main pancreatic duct (white arrow head) (B). Case 2 only had a 3.10 cm lesion located in the pancreatic body (yellow arrow triangle) (C). And two cases of PCL progression: The size of lesion in case 1 increased to 1.78 cm (yellow arrow head) (E) from 1.42 cm (yellow arrow head) (D) during 12 months. In case 2, the size increased to 2.51 cm (white arrow head) (G) from 1.93 cm (white arrow head) (F) during 12 months. |
Associated Factors of PCL Progression
One hundred and seven cases were followed up for 12 months. Significant progression was observed in 14.0% (15/107) of them. The characteristics of PCLs in progression group and stable group are displayed in Table 4. Patients in the progression group appeared to be older than those in the stable group (median age 71.87 years vs 63.39 years, p = 0.028). Cysts located in the pancreatic head and neck were more likely to progress than those located in the pancreatic body and tail (p = 0.011). Pancreatic duct dilatation, extrapancreatic growth and abnormal urea were more common in the progression group (p = 0.027, p = 0.039 and p = 0.007, respectively) than in the stable group. Abnormal serum creatinine was also related with PCL progression (p = 0.056).
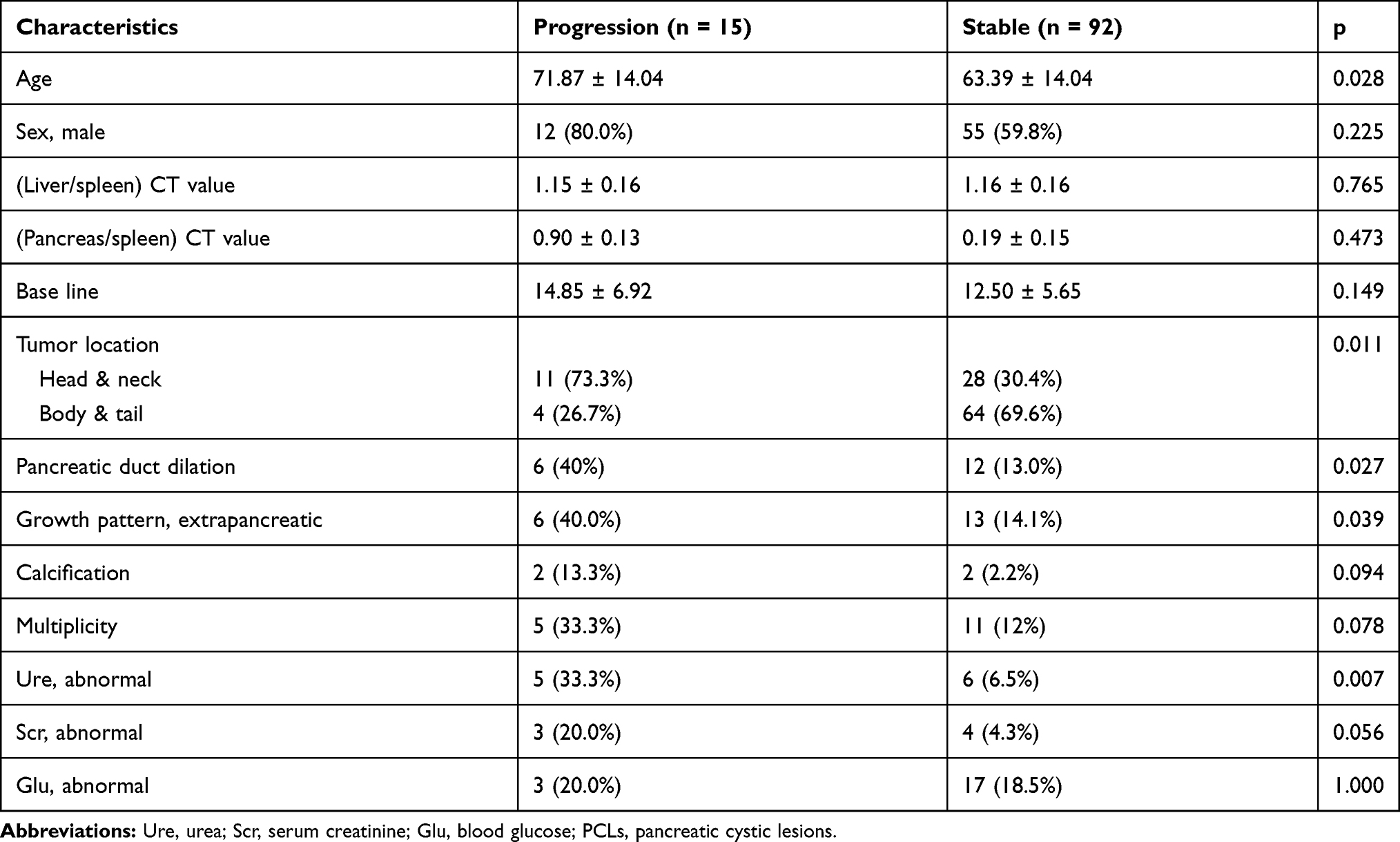 |
Table 4 Baseline Characteristics of Population with Progressive and Stable PCLs |
Multivariate regression analysis showed that the tumor location (odds ratio (OR): 9.283 (95% CI: 1.554–35.118), p = 0.002), growth pattern (OR: 6.135 (95% CI: 1.445–26.315), p = 0.014) and serum creatinine level (OR: 8.0 (95% CI: 1.647–38.462), p = 0.01) were the risk factors for the progression of PCLs after adjusting with modifiers, such as liver function and diabetes. We developed a clinical model to predict PCL progression based on the associated factors, the AUC was 0.862 (95% CI: 0.758–0.939) with a sensitivity of 93.3% and specificity of 66.3% (Figure 3B). Cases of PCLs with progression are shown in Figure 4D–G.
Discussion
With the widespread application of high-quality cross-sectional imaging, there is a dramatic increase in detection of PCLs in the past two decades.18 Although many studies have focused on PCLs based on different nations or populations,1 the prevalence and characteristics of incidental PCLs in Chinese population have not been well-studied,19 especially for the general population. Our data showed that the crude prevalence of incidental PCLs in Chinese healthy examination population was 1.75%. The prevalence of incidental PCLs increased with increasing of age. Tumor location and growth pattern are independent risk factors for the high risk of PCLs and PCL progression.
Extensive screening for PCLs is not recommended in the general population. Some studies have reported the incidental detection of PCLs on CT or MRI.20 One report showed that the incidental borderline and malignant lesions were observed in 29 of 92,309 cases during the pancreatic scanning in CT and MRI.7 Considering the huge number of abdominal CT or MRI examinations in each year, those incidental findings act as one of indirect screening approaches for pancreatic diseases. In addition, there is another indirect screening approach for pancreatic diseases. Low-dose CT for lung cancer screening has been used in certain parts of the world, such as in United States and China. Pancreas is usually scanned during the lung screening. Our study assessed the prevalence of incidental PCLs detected during lung cancer screening in a Chinese general population. To the best of our knowledge, this may be the first report to show prevalence of PCLs using data of lung cancer screening. The prevalence of incidental PCLs in our study population was similar to that reported in other Chinese studies (1.93% and 1.91%).19,21 Prevalence of 2.6–3.0% was also reported in several studies.4,22 These previous studies included all outpatients and inpatients. Many inpatients may suffer from other diseases such as extra-pancreatic tumors, which is positively correlated to PCLs.23 The association between age and PCLs has been widely observed.6,8,24,25 Our data also showed a similar trend. If incidental PCLs were detected during the routine low-dose CT scan for lung cancer screening, those patients would undergo MRI examinations for further evaluation. For those patients with IPMN or MCN or lesions with malignant tendency, further evaluations for surgery should be performed.
We also primarily observed possible associated factors of PCLs. In univariate analysis, decreased pancreas/spleen and increased liver/spleen CT value ratio were the associated factors for PCLs. The decreased CT ratio of the pancreas/spleen may be related to obesity. Mizuno et al25 proposed that obesity is a risk factor for PCLs. The increase in liver density in the general population is mainly related to liver cirrhosis caused by various factors, such as hepatocyte necrosis, fibrosis and iron deposition. Girometti et al24 found that alcoholic liver cirrhosis is closely related to the prevalence of PCLs. Moreover, our study showed that abnormal of AKP, ALT and serum creatinine were more common in patients with PCLs than those without PCLs, which suggests that PCls may be related to abnormal liver and kidney function. However, the mechanisms of PCLs development are complex. Our study is just an exploration, and further studies are strongly needed to identify possible risk factors.
Not all PCLs are IPMNs and mucinous cystic neoplasms which have malignant potential. We have summarized a lot of studies and clinical guidelines4,17,26 before defining the high-risk PCLs. At present, there is still controversy about the “worrisome feature” of pancreatic duct dilatation.12,27 Hacker et al reported that main-duct IPMNs with a MPD between 5 and 9 mm already bear a significant risk of malignancy and surgical treatment should be clearly indicated in these patients.28 Therefore, we considered pancreatic duct dilation >5 mm as one of the features of high-risk PCLs.15 Our data demonstrated that urea, tumor location, and growth pattern are independent risk factors for the high-risk PCLs. Walters et al29 studied the relationship between pancreatic exocrine function and renal injury and reported that increased blood urea concentration was detected when the pancreatic duct was dilated. We suspected that pancreatic duct dilatation may cause pancreatic inflammation or directly affect the exocrine state of the pancreas, and lead to an increase in blood urea. However, further research is needed to clarify this link. Our data further showed that PCLs in head-neck tend to have high potential for high-risk PCLs. IPMN which has a high malignant potential is commonly occurred in head region of the pancreas.27
We further assessed associated factors of PCL progression in 107 subjects. Our study showed that 14% PCLs progressed during 12-month follow up which was consistent with previous reports.30,31 Cyst size may be an indicator of PCLs progression.31–33 However, no such association was found in our study. This may be due to the entry criteria of our study which did not include lesions less than 5 mm in length, and short-term period of follow-up. Similar to a previous study,19 we found that PCLs located in the pancreatic head and neck were more likely to progress than others located in the body-tail. Those cystic lesions with malignant potential, such as IPMNs, usually occur in the pancreatic head. Age is another factor that was associated with the progression of PCLs, which is also concordant with previous reports.25,31 In addition, the growth pattern of cystic lesion was an independent predictor of progression. Our data may provide valuable contribution to PCLs management.
Our study has several advantages. This is the first study to explore the prevalence and characteristic of PCLs in the Chinese general population. In addition, PCLs were detected based on lung cancer screening. Therefore, the subjects neither received additional radiation exposure and nor incurred additional cost. Moreover, we also performed a follow-up for 107 PCLs. This study has many limitations. First, most of our individuals did not undergo contrast-enhanced imaging examinations and the lesions that were less than 5 mm cannot be clearly displayed. Therefore, the prevalence of PCLs may be underestimated. However, previous data showed that pancreatic cancer risk in cysts >5.0 mm was increased by 6.2 folds.14 Those lesions >5.0 mm may deserve more attention. Second, the treatment of PCLs is mainly based on follow-up observations. Our research lacks the support for pathological diagnosis. Third, we only conducted a primary study to identify the possible associated factors. Many factors were not included, such as alcohol drinking, and smoking. Finally, our follow-up period is too short and a longer observation is needed.
In summary, our data indicate that the indirect findings from CT lung cancer screening is helpful for PCL detection. The crude prevalence of incidental PCLs in the Chinese general population is 1.75%. The prevalence significantly increases with increasing of age. PCLs located in the pancreatic head-neck and with an extrapancreatic growth pattern tends to be high-risk PCLs and tends to progress. These findings are helpful in the management of patients with PCLs.
Acknowledgments
Xiao Chen and Zhongqiu Wang are co-correspondence authors for this study. This study was funded by National Natural Science Foundation of China (81771899), the Key Program of Research and Development of Jiangsu Province (BE2017772) and Foundaton of Administration of Traditional Chinese Medicine of Jiangsu Province (ZD201907).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zerboni G, Signoretti M, Crippa S, Falconi M, Arcidiacono PG, Capurso G. Systematic review and meta-analysis: prevalence of incidentally detected pancreatic cystic lesions in asymptomatic individuals. Pancreatology. 2019;19(1):2–9. doi:10.1016/j.pan.2018.11.014
2. Munigala S, Javia SB, Agarwal B. Etiologic distribution of pancreatic cystic lesions identified on computed tomography/magnetic resonance imaging. Pancreas. 2019;48(8):1092–1097. doi:10.1097/MPA.0000000000001372
3. Wu BU, Sampath K, Berberian CE, et al. Prediction of malignancy in cystic neoplasms of the pancreas: a population-based cohort study. Am J Gastroenterol. 2014;109(1):
4. van Huijgevoort NCM, Del Chiaro M, Wolfgang CL, van Hooft JE, Besselink MG. Diagnosis and management of pancreatic cystic neoplasms: current evidence and guidelines. Nat Rev Gastroenterol Hepatol. 2019;16(11):676–689. doi:10.1038/s41575-019-0195-x
5. Martinez B, Martinez JF, Aparicio JR. Prevalence of incidental pancreatic cyst on upper endoscopic ultrasound. Ann Gastroenterol. 2018;31(1):90–95.
6. Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol. 2010;105(9):2079–2084. doi:10.1038/ajg.2010.122
7. Matsubara S, Tada M, Akahane M, et al. Incidental pancreatic cysts found by magnetic resonance imaging and their relationship with pancreatic cancer. Pancreas. 2012;41(8):1241–1246. doi:10.1097/MPA.0b013e31824f5970
8. de Oliveira PB, Puchnick A, Szejnfeld J, Goldman SM. Prevalence of incidental pancreatic cysts on 3 tesla magnetic resonance. PLoS One. 2015;10(3):e0121317. doi:10.1371/journal.pone.0121317
9. Canto MI, Harinck F, Hruban RH, et al. International Cancer of the Pancreas Screening (CAPS) consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut. 2013;62(3):339–347. doi:10.1136/gutjnl-2012-303108
10. Owens DK, Davidson KW, Krist AH, et al. Screening for pancreatic cancer: us preventive services task force reaffirmation recommendation statement. JAMA. 2019;322(5):438–444.
11. Yang D, Liu Y, Bai C, Wang X, Powell CA. Epidemiology of lung cancer and lung cancer screening programs in China and the United States. Cancer Lett. 2020;468:82–87. doi:10.1016/j.canlet.2019.10.009
12. Del Chiaro M, Verbeke C, Salvia R, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis. 2013;45(9):703–711. doi:10.1016/j.dld.2013.01.010
13. Chalian H, Tore HG, Miller FH, Yaghmai V. CT attenuation of unilocular pancreatic cystic lesions to differentiate pseudocysts from mucin-containing cysts. JOP. 2011;12(4):384–388.
14. Tanaka S, Nakao M, Ioka T, et al. Slight dilatation of the main pancreatic duct and presence of pancreatic cysts as predictive signs of pancreatic cancer: a prospective study. Radiology. 2010;254(3):965–972. doi:10.1148/radiol.09090992
15. Elta GH, Enestvedt BK, Sauer BG, Lennon AM. ACG clinical guideline: diagnosis and management of pancreatic cysts. Am J Gastroenterol. 2018;113(4):464–479. doi:10.1038/ajg.2018.14
16. Scheiman JM, Hwang JH, Moayyedi P. American Gastroenterological Association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology. 2015;148(4):824–848 e822.
17. Megibow AJ, Baker ME, Morgan DE, et al. Management of incidental pancreatic cysts: a white paper of the ACR incidental findings committee. J Am Coll Radiol. 2017;14(7):911–923. doi:10.1016/j.jacr.2017.03.010
18. Gardner TB, Glass LM, Smith KD, et al. Pancreatic cyst prevalence and the risk of mucin-producing adenocarcinoma in US adults. Am J Gastroenterol. 2013;108(10):1546–1550. doi:10.1038/ajg.2013.103
19. Sun L, Wang Y, Jiang F, Qian W, Shao C, Jin Z. Prevalence of pancreatic cystic lesions detected by magnetic resonance imaging in the Chinese population. J Gastroenterol Hepatol. 2019;34(9):1656–1662. doi:10.1111/jgh.14658
20. Kromrey M-L, Bülow R, Hübner J, et al. Prospective study on the incidence, prevalence and 5-year pancreatic-related mortality of pancreatic cysts in a population-based study. Gut. 2018;67(1):138–145. doi:10.1136/gutjnl-2016-313127
21. Zhu S, Wang WT, Shang XS, et al. Difference analysis in prevalence of incidental pancreatic cystic lesions between computed tomography and magnetic resonance imaging. BMC Med Imaging. 2019;19(1):43. doi:10.1186/s12880-019-0341-5
22. Pereira SP, Oldfield L, Ney A, et al. Early detection of pancreatic cancer. Lancet Gastroenterol Hepatol. 2020;5(7):698–710. doi:10.1016/S2468-1253(19)30416-9
23. Zanini N, Giordano M, Smerieri E, et al. Estimation of the prevalence of asymptomatic pancreatic cysts in the population of San Marino. Pancreatology. 2015;15(4):417–422. doi:10.1016/j.pan.2015.05.461
24. Girometti R, Intini S, Brondani G, et al. Incidental pancreatic cysts on 3D turbo spin echo magnetic resonance cholangiopancreatography: prevalence and relation with clinical and imaging features. Abdom Imaging. 2011;36(2):196–205. doi:10.1007/s00261-010-9618-4
25. Mizuno S, Isayama H, Nakai Y, et al. Prevalence of pancreatic cystic lesions is associated with diabetes mellitus and obesity: an analysis of 5296 individuals who underwent a preventive medical examination. Pancreas. 2017;46(6):801–805. doi:10.1097/MPA.0000000000000833
26. Harrison JM, Castillo CF. To resect or not to resect: a review of pancreatic cyst disease management. Curr Opin Gastroenterol. 2018;34(5):343–348. doi:10.1097/MOG.0000000000000463
27. Tanaka M, Fernandez-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology. 2012;12(3):183–197. doi:10.1016/j.pan.2012.04.004
28. Hackert T, Fritz S, Klauss M, et al. Main-duct intraductal papillary mucinous neoplasm: high cancer risk in duct diameter of 5 to 9 mm. Ann Surg. 2015;262(5):
29. Walters MN. Studies on the exocrine pancreas. I. Nonspecific pancreatic ductular ectasia. Am J Pathol. 1964;44:973–981.
30. Morris-Stiff G, Falk GA, Chalikonda S, Walsh RM. Natural history of asymptomatic pancreatic cystic neoplasms. HPB. 2013;15(3):175–181. doi:10.1111/j.1477-2574.2012.00522.x
31. Nougaret S, Reinhold C, Chong J, et al. Incidental pancreatic cysts: natural history and diagnostic accuracy of a limited serial pancreatic cyst MRI protocol. Eur Radiol. 2014;24(5):1020–1029. doi:10.1007/s00330-014-3112-2
32. Park HW, Lee JS, Park SY, et al. Progression of pancreatic cystic lesions without any risk features is associated with initial cyst size and obesity. J Gastroenterol Hepatol. 2019;35:874–884.
33. Pandey P, Pandey A, Luo Y, et al. Follow-up of incidentally detected pancreatic cystic neoplasms: do baseline MRI and CT features predict cyst growth? Radiology. 2019;292(3):647–654. doi:10.1148/radiol.2019181686
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.