")
Back to Journals » Journal of Pain Research » Volume 16
Opioids Prescribing Among Patients with Zoster-Related Pain in Real-Life: A Retrospective, Cohort Study Based on the Clinical Database
Authors Su W, Liu D, Yang P, Ye L
Received 4 August 2023
Accepted for publication 23 October 2023
Published 8 November 2023 Volume 2023:16 Pages 3785—3796
DOI https://doi.org/10.2147/JPR.S430439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Wei Su,1,2 Dong Liu,2 Pingliang Yang,3 Ling Ye1
1Department of Pain Management, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China; 2Department of Pain Management, Chengdu Second People’s Hospital, Chengdu, Sichuan, 610011, People’s Republic of China; 3Department of Anesthesiology, the First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, 610500, People’s Republic of China
Correspondence: Ling Ye, Department of Pain Management, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China, Tel +86-28-85423593, Email [email protected]
Purpose: The aim of this study was to analysis of the opioid use of opioid native zoster-related pain (ZRP) patients to evaluate the impact of opioid use on pain control and quality of life improvement based on the clinical database.
Patients and Methods: We conducted a retrospective cohort study to identify opioid native patients who were hospitalized in the pain department between May 1, 2020, and May 1, 2021. The primary outcomes were persistent opioid use after discharge, visual analogue scale (VAS) at the admission, VAS remission rate during hospitalization, VAS score and quality of life at follow-up. Then, we assessed patient-level risk factors for persistent opioid use after the discharge.
Results: A total of 350 patients met the inclusion criteria. Of those patients, 255 (72.9%) were administered with opioid during hospitalization, and 95 (27.1%) patients were not. Opioid prescription during hospitalization was independently associated with increased odds of persistent use after the discharge (adjusted odds ratio, 20.74; 95% CI, 4.504– 95.474; P < 0.01). In the two groups, the VAS score at admission and the VAS score at follow-up were different. In the group with opioids during hospitalization, the persistent opioid use after discharge was more common (38% vs 2.1%) compared to patients without opioids, and VAS remission rate during hospitalization was less, restrictions on daily life, work or housework, and social activities were more common, and mood, diet and sleep were worse, respectively.
Conclusion: Opioids prescription during hospitalization might increase the risk of chronic opioid use in opioid native ZRP patients, and it has limited benefits in pain control and quality of life improvement. Even though PHN was painful and intractable, the use of opioids should also be more cautious, and strict follow-up, management in this population.
Keywords: opioids, persistent opioid use after discharge, real-life, zoster-related pain, postherpetic neuralgia
Introduction
Zoster-related pain (ZRP) occurs after herpes zoster (HZ) infection, which is characterized by moderate-to-severe pain.1 The most frequent and debilitating complication of zoster is postherpetic neuralgia (PHN).2 A cross-sectional survey in 2019 showed that the incidence of HZ and PHN in the Chinese population was 7.7% and 2.3%, and 29.8% of HZ patients developed into PHN, which was more than 3 million, especially the elderly over 70 years old.3 At present, in addition to common drug therapy, there are various interventional pain management to help relieve the pain, but the treatment effect varies greatly from individual to individual, and there is lack of very effective specific treatments.4–6 Stubborn and severe pain seriously affects the mental and physical health of these patients.7,8 Therefore, to better meet the analgesic needs of these patients, opioids are considered (including traditional opioids and compound opioid analgesics) as an important auxiliary treatment method for more complex and serious patients while constantly exploring and optimizing the treatment methods of ZRP, and it has received more and more attention.9
Since opioid crisis, with the deepening understanding of opioids, although a recent meta-analysis of randomized controlled trials ranging between 4 and 12 weeks concluded that some opioids could provide a short-term substantial pain relief in patients who suffer from postherpetic neuralgia and peripheral neuropathies of different aetiologies.10 But in recent years, several studies had demonstrated that the new opioid exposure after surgery was a significant and independent risk factor for chronic opioid use,11–13 and the long-term use might develop an opioid use disorder.14 To date, opioid use had largely been used as a secondary outcome in most studies on ZRP, and few had evaluated both the improvement of pain degree and general quality of life in ZRP patients after opioid use. Therefore, given the huge risks and social costs of chronic opioid use, it is worth to evaluate the use of opioids among ZRP patients in real-life, quantify the risks of chronic opioid use in such patients after discharge, and explore whether the risks outweigh the benefits. This study tried to determine the incidence and associated factors of persistent opioid use after discharge in patients with ZRP, and to evaluate the benefits of opioid use on pain control and quality of life improvement.
Materials and Methods
Study Design and Participants
This was a retrospective cohort study, which analyze the use of opioids in ZRP patients during hospitalization, and to follow up the persistent use of opioids, pain degree and quality of life after discharge.
Study participants were selected from patients enrolled in the ZRP database, which collected hospitalized patients with ZRP in the Department of Pain Management of our hospital, and pooled each patient’s hospitalization medical records, prescription, imaging, and related laboratory data. This study was registered at ChiCTR.org.cn (ChiCTR2200059672, date of registration: May 2022) and was approved by the Information Center and the Biomedical Ethics Committee of West China Hospital, Sichuan University (No. 2019[1121], date of approval: May 2020). Our ethics committee specifically waived the requirement for informed consent due to the retrospective nature of this study, which complies with the Declaration of Helsinki. The data was maintained with confidentiality.
The study included patients in the database who were admitted between May 1, 2020, and May 1, 2021. The exclusion criteria were: (1) patients who had used opioids (including traditional opioids and compound opioid analgesics) before illness according to the past medical history recorded in the database, (2) patients treated with morphine pump, and (3) patients with incomplete clinical data collection or death.
According to the opioids prescription during hospitalization, the enrolled patients were divided into opioid fill group and non-opioid fill group during hospitalization. Opioid prescription during hospitalization was obtained from the database of prescriptions recorded during hospitalization.
Data Collection and Follow-Up
According to the content of the database, we included patient sociodemographic characteristics, pre-hospital, in-hospital information (mainly comorbidities, pharmacological and nonpharmacological therapies), and post-discharge information. Since this study was based on an established database, there was no follow-up at a fixed interval for every patient after discharge. However, all participants completed a telephone follow-up at least 120 days after the discharge to included relevant data after discharge (all patients were followed up from the end of September to the beginning of October 2021).
The primary outcome variable was persistent opioid use after discharge defined as persistent opioid use for at least 120 days after discharge, which was established based on previous study15 and the sample size before data extraction. The second was the visual analogue scale (VAS) score at admission, VAS remission rate during hospitalization, VAS score and quality of life at follow-up. The quality of life at follow-up included six dimensions: daily life, work or housework, social activities, daily mood, diet, and sleep. The first three dimensions were divided into three levels: without restriction, generally restriction and very restriction, and the last three dimensions were divided into three levels: bad, general, and good.
Sociodemographic characteristics included age, gender, body mass index (BMI), major comorbidity, Charlson Comorbidity Index (CCI), tobacco use, alcohol use, social security type, and marital status. According to the Chinese standard,16,17 BMI was categorized into 4 categories: low weight < 18.5, normal: 18.5–23.9, overweight: 24–27.9, obesity: ≥28, and the levels were expressed as 1, 2, 3, 4. The main types of comorbidities included diabetes, connective tissue disease, kidney disease, liver disease, malignant tumor, HIV, gastrointestinal ulcer, chronic lung disease, other chronic physical pain, and mental and psychological diseases. Pre-hospital treatment information included interventional pain management procedure (nerve pulse radiofrequency, thermocoagulation, spinal cord stimulation, doxorubicin injection, and absolute ethanol injection), nerve blocks, and antineuropathic drugs use (gabapentin, pregabalin, carbamazepine, oxcarbazepine, duloxetine). In-hospital information including herpes position (left or right), the affected spinal nerve segment, symptoms associated with pain (hyperalgesia, numbness, pruritus, formication, weakness), disease duration, antineuropathic drug use, nonsteroidal anti-inflammatory drug (NSAIDS) use, nerve block, interventional pain management and lidocaine intravenous infusion, adverse events during hospitalization, and hospitalization days. Post-discharge information mainly included adverse events.
Statistical Analysis
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS, 26.0 version). Descriptive statistics were calculated for covariates such as sociodemographic variables, comorbidities, and zoster-related conditions (before, during, and after hospitalization). Ordinal variables and continuous variables were expressed as medians and interquartile range, categorical variables were expressed as numbers and associated percentages. “Opioid fill” and “no opioid fill” characteristics were compared using t-tests for continuous variables, Pearson chi-squared tests for categorical variables, and Mann–Whitney U-tests for ordinal variables. A multivariable logistic regression model was used to examine differences in persistent opioid use by opioid exposure during hospitalization while controlling for patient characteristics. These patient characteristics were included in the logistic regression model due to their clinical relevance. The P values were two-tailed, and the significance was set at P < 0.05.
One sensitivity analysis was performed. Although opioids were used in some patients during hospitalization, they were only used temporarily to control the breakthrough pain. Therefore, to test the robustness of the effect of opioid fill during hospitalization on the persistence of use after discharge, these patients were redivided into the group of patients who did not use opioids during hospitalization and analyzed again. The logistic regression model used in this analysis also included the relevant variables mentioned above.
Results
In this database, 428 ZRP patients from May 1, 2020, to May 1, 2021, were included. Twenty patients lost follow-up (telephone follow-up failed), 5 patients died, 52 patients used opioids before illness, and 1 patient used morphine pump. Finally, 350 (82.0%) patients met the inclusion criteria of this study. Among them, 255 patients (72.9%) used opioids during hospitalization, and 95 patients (27.1%) did not. The procedure for cohort inclusion and exclusion was shown in Figure 1.
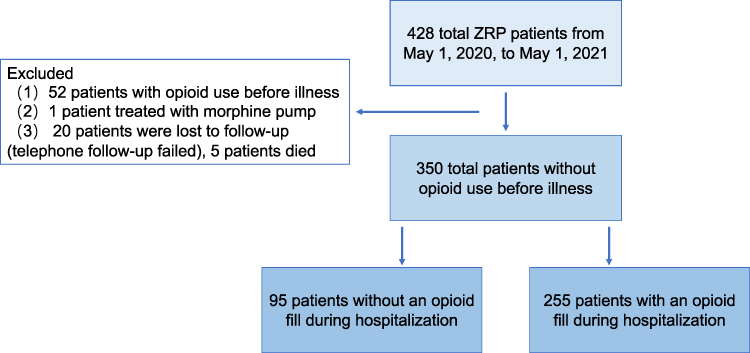 |
Figure 1 Flow diagram of inclusion and exclusion criteria in the construction of the final cohort. Abbreviation: ZRP, zoster-related pain. |
Cohort Characteristics
In terms of patients’ general conditions, compared with patients without an opioid during hospitalization, patients with opioids had longer hospitalization days [9(7–10) days vs 8(7–12) days], and their disease duration was more than 1 month (84.0% versus 67.4%). The VAS score at admission was slightly higher [7(6–7) vs 6(5–6)], and the difference was considered statistically significant. However, in order to facilitate the analysis of results and evaluate the actual clinical significance of patient-reported results better, based on the IMMPACT recommendations and relevant study,18 the minimal clinical important difference (MCID) was determined as 1.1 for mild pain (VAS ≤ 3), 1.4 for moderate pain (4 ≤ VAS ≤ 7), and 1 for severe pain (VAS > 7). The difference in VAS between groups greater than the MCID was considered as clinically meaningful. Therefore, the difference in VAS score on admission was not considered as clinically meaningful (difference < 1.4).
In terms of in-hospital treatment, compared with patients without opioids during hospitalization, patients with opioids had a higher proportion of interventional pain procedure (78.8% vs 50.5%), lidocaine intravenous infusion (40.8% vs 15.8%), and antineuropathic drugs (100.0% vs 95.8%). VAS remission rate during hospitalization was slightly less [63% (56–71%) vs 75% (67–89%)], but the proportion of non-steroidal anti-inflammatory drugs (NSAIDs) use was less (3.5% vs 9.5%) (P < 0.05). The most common adverse events during hospitalization in the whole study cohort were constipation and dizziness. Descriptive data are displayed in Table 1.
 |
Table 1 Descriptive Statistics Reporting Differences Between Patients Who Did and Did Not Use an Opioid Prescription During Hospitalization |
Opioid Use and Associated Risk Factors
In the study, 255 patients (72.9%) were administered with opioids during hospitalization, and the persistent opioid use after discharge was 38%. However, 95 patients (27.1%) were not administered with opioids during hospitalization, and the persistent opioids use after discharge was 2.1% (P < 0.05) (Figure 2). When compared with patients without opioids during hospitalization, the adjusted odds ratio of persistent opioid use after discharge in patients who did fill was 20.74 (95% CI, 4.504–95.474) (P < 0.01), after adjustment for patients’ factors. Other covariates independently associated with new persistent opioid use after discharge were age (AOR = 1.51, 95% CI, 1.057–2.167), CCI value (AOR = 1.38, 95% CI, 1.139–1.662), pain with pruritus (AOR = 0.216, 95% CI, 0.058–0.799) (P < 0.05) (Table 2).
 |
Table 2 Multivariable Logistic Regression Analysis Demonstrating Factors Associated with Persistent Opioid Use |
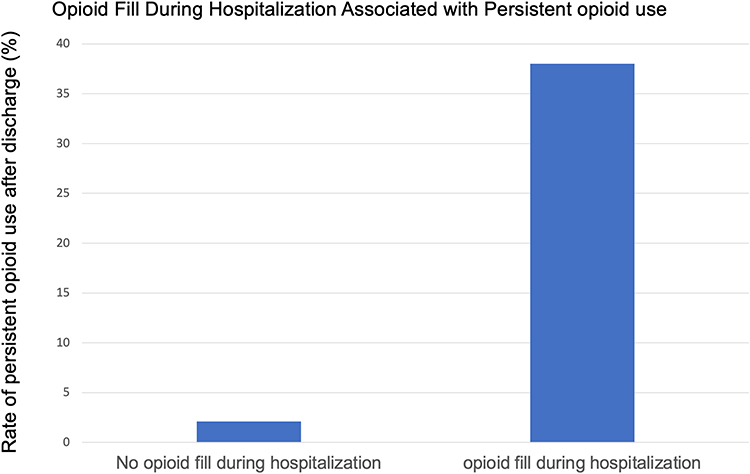 |
Figure 2 Unadjusted rates of persistent opioid use for patients who filled opioid prescription during hospitalization, those who did not fill a opioid prescription during hospitalization. |
In addition, we also further analyzed the general characteristics of patients with new persistent opioid use after discharge (n = 99, 28.3%). The results showed that compared with patients without persistent opioid use (n = 251, 71.7%), patients with new persistent opioid use after discharge had higher CCI [1(1–2) vs 1(0–2)] and lower VAS remission rate during hospitalization [60% (50–71%) vs 67% (57–80%)] (P < 0.05). The VAS score at discharge was slightly higher [3(2–3) vs 2(1–3)], and the difference was statistically significant but not clinically meaningful (difference < 1.1) (Table 3).
 |
Table 3 Descriptive Statistics Reporting Differences Between Patients with and without Persistent Opioid Use After Discharge |
Situations at Follow-Up
Analysis of follow-up data showed that compared with patients without an opioid fill during hospitalization, those who did fill had more restrictions in daily life, work or housework, and social activities; daily mood, diet, and sleep were worse (P < 0.01). The VAS score at follow-up was slightly higher [2(0–3) vs 1(0–2)], and the difference was statistically significant but not clinically meaningful (difference < 1.1). In general, the common adverse events after discharge were constipation, dizziness, and stomach discomfort (Table 4).
 |
Table 4 Follow-Up Information According to Whether Opioids Were Used During Hospitalization |
Furthermore, the analysis of follow-up data also showed that compared with patients without new persistent opioid use after discharge, the patients with new persistent opioid use had more restriction in daily life, work or housework, and social activities; daily mood, diet, and sleep were worse (P < 0.01). The VAS score at follow-up was slightly higher [3 (3–4) vs 2 (0–3)], the difference was statistically significant but not clinically meaningful (difference < 1.1) (Table 5).
 |
Table 5 Follow-Up Information According to Whether Opioids Were Persistent Used After Discharge |
Type of Opioids
Among the patients with opioids during hospitalization, the most common compound opioids were oxycodone-acetaminophen (n = 228,89.4%), and the most common traditional opioids were dezocine (n = 60.23.5%) and tramadol (n = 24.9.4%). Two types of opioids were used by 71 patients (27.8%). However, oxycodone-acetaminophen (n = 73.73.7%) still were the most frequently used combination opioids among patients with persistent opioid use after discharge, and the most common traditional opioid was tramadol (n = 7.7.1%). Only 1 patient (1.0%) took two opioids at the same time (Table 6).
 |
Table 6 Type of Opioids |
Finally, considering that some patients used opioids only for temporary control of breakthrough pain during hospitalization, our regrouping showed that 250 patients (71.4%) with opioids fill during hospitalization, and 37.6% (n = 94) of them became new persistent opioid users, in contrast to 5.0% (n = 5) who did fill opioid (n = 100, 28.6%) (P < 0.05). When compared with patients without an opioid fill during hospitalization, the adjusted odds ratio of persistent opioid use after discharge in patients who did fill was 8.45 (95% CI, 2.996–23.810) (P < 0.01).
Discussion
This study analyzed the use of opioids in ZRP in “real-life” clinical settings, which found that patients administered with opioids during hospitalization had higher odds of persistent opioid use after discharge, and opioids during hospitalization were independently associated with persistent opioids use after discharge. Furthermore, this study found that chronic opioids use had limited benefit on pain control and quality of life improvement in patients with ZRP. The finding was of great enlightenment to help clinicians further understand the use of opioids in ZRP patients whose main goal was to relief pain and life quality improvement.
Appropriate Timing of Filling Might Increase the Risk of Chronic Opioid Use
Nowadays, in the context of opioid crisis, the related issues of opioid use have attracted more attention. Current international guidelines have relatively consistent statements on when opioids can be used for chronic non-cancer pain, and all suggest that opioids can be considered when the pain is severe, and non-opioid treatment and non-pharmacological treatment are ineffective or intolerant.9,10,19 This study analyzed the ZRP this remarkable type of non-cancer pain. Based on the cohort characteristics, patients with moderate or severe pain, disease duration of more than 1 month at admission, antineuropathic drug use, lidocaine intravenous infusion, and interventional pain management, but with low VAS remission rate had a higher chance to be filled with opioids (Table 1). Thus, although the types of opioids might have varied according to the prescribing clinician, the results generally reflect that the timing of opioid administration during hospitalization in this cohort was relatively reasonable.
Several previous studies have shown that for opioid native patients, perioperative or discharge opioid exposure was an important and independent risk factor for chronic opioid use. In a retrospective study of 6689 discharged patients without previous opioid use, Calcaterra et al13 found that patients who were prescribed opioids at discharge were more likely to become chronic opioid users after discharge (4.1% vs 1.3%, P < 0.05) and was independently associated with opioid prescription at discharge. Southren et al12 reviewed 1249 patients who were opioid native and had radiofrequency ablation for chronic back pain, showed that the proportion of new persistent opioid use in patients with periprocedural opioid fill was significantly higher (5.6% vs 2.8%, P < 0.05), and new exposure to opioids is an independent risk factor for persistent use in such patients. Ung et al20 found that among 14,841 patients undergoing ophthalmic surgery who had not previously opioids use, the incidence of persistent opioid use was 3.4% in those who had used opioids during the perioperative period (0.6% for perioperative non-users, P < 0.05).
Similarly, our study demonstrates that patients with opioids fill during hospitalization were more likely to have persistent opioid use after discharge compared with those who did not (38.0% vs 2.1%, P < 0.01), although the difference in VAS at admission was not clinically meaningful. After adjustment for patients’ factors, opioid fill during hospitalization was independently associated with persistent opioid use after discharge [AOR = 20.74 (95% CI, 4.504–95.474), P < 0.01]. This was consistent in direction with the results of a few previous studies on new persistent use of opioids. It was surprising to note that patients with opioids fill during hospitalization had lower VAS scores at discharge [2(2–3)] and at follow-up [2(0–3)] but continued to use opioids after discharge. This might also demonstrate the extremely small potential possibility of opioid use disorder in such patients to some extent and remind doctors that they should establish a more complete follow-up system, strengthen the medication supervision of such patients after discharge, and facilitate the adjustment of medication regimens.
However, in this cohort, ZRP patients with opioid fill during hospitalization had a higher rate of persistent opioid use after discharge than those in previous studies, and the risk of becoming persistent opioid users was significantly greater. First, this might be related to the definition of persistent opioid use. At present, the definition of persistent opioid use was not consistent between studies, making interpretation of estimates and comparison across studies challenging. More importantly, the ability of different definitions to reflect the potential risks or associated adverse events of persistent opioid use in patients was also quite different. At the beginning of the design of this study, referring to the results of a systematic literature search on the same cohort using 29 different definitions published in ANESTHESIOLOGY in 2020,15 the persistent opioid use was defined at least 120 days after discharge, which was more suitable for the cohort size and reflected the potential risks of chronic opioid use. Secondly, ZRP itself is a painful disease, rather than a concomitant symptom of a certain disease or after a certain procedure. Therefore, the high value of this result also suggested that ZRP patients had a higher relative risk of chronic opioid use, which conversely demonstrates the clinical characteristics of ZRP, which was extremely painful and prolonged.
In addition, the patients with persistent opioid use after discharge were more likely to be older and had higher CCI score, which were associated with risk factors for the new persistent opioid use in our study. Firstly, it might be because previous studies had shown that the degree and duration of pain in ZRP patients were significant associative with age and comorbidities.21 It could be speculated that older patients and those with more comorbidities may have more pain or discomfort in addition to ZRP, and multiple chronic comorbidities may also bring anxiety and depression. Therefore, under the influence of multiple pain and discomfort with negative emotions, they might be more likely to depend on opioids to relieve their emotions and pain. It was also worth noting that the initial dose of opioid use disorder in the elderly population may be lower and the onset may be more insidious.22
Chronic Opioid Use Had Limited Benefit on Pain and Quality of Life with ZRP
First, patients reporting higher pain scores, treated for longer duration, and with higher CCI indicate a more complex patient overall, yet VAS scores were lower during admission with opioid use indicating improved control of their pain on opioids during their hospitalization. However, compared with patients who did fill opioids during hospitalization, patients who did not had a lower VAS remission rate during hospitalization (63% (67–89%) vs 75% (56–71%), P < 0.05) and a slightly higher VAS score at follow-up [(2 (0–3) vs 1 (0–2), P < 0.05, without clinically meaning]. On the other hand, patients who with persistent opioids use after discharge had a lower VAS remission rate during hospitalization than those who without [60% (50–71%) vs 67% (57–80%), P < 0.05], and VAS score at follow-up was also higher [3 (3–4) vs 2 (0–3), P < 0.05, without clinically meaning]. These results demonstrate that ZRP patients with opioid fill in this cohort had limited VAS relief, and the difference in VAS scores, although not clinically meaningful, did not show better pain control for at least 120 days. Secondly, the quality of life of patients was also investigated from six dimensions: daily life, work or housework, social activities, daily emotions, diet, and sleep. The results showed that patients with opioid fill during hospitalization or persistent opioids use after discharge had more restrictions and worse quality. This demonstrates that the benefit is limited in terms of long-term quality of life among the patients who use opioids throughout their disease duration.
In general, opioids fill during hospitalization makes ZRP patients had a higher risk of becoming chronic opioid users, and the contribution of opioid fill in the whole duration of the disease to the long-term pain control and quality of life improvement was not satisfactory. It has been shown in large databases that long-term opioid treatment of chronic noncancer pain is associated with a higher all-cause mortality.23,24 However, if opioids were helpful to relief the pain without better alternatives, it made sense to use them even if there was a risk of adverse side effects.
However, for ZRP patients with severe pain, how to develop opioids use regimens? First, multimodal analgesia may be helpful in further relieving pain and reducing unnecessary opioid use. In addition, physical rehabilitation, traditional Chinese medicine, psychological intervention, and other treatments can also be beneficial.21 Secondly, opioids should be used when necessary for ZRP patients with severe pain, but strict supervision and follow-up are needed. When the pain of patients is relieved, gradual reduction of the dosage of opioids should be considered in time. Studies had found that current clinical practice guidelines mostly agree on when and how to deprescribe opioid analgesics, but there were barriers to the feasibility of implementing specific measures.25 A more individualized multimodal medication strategy may be the focus of future efforts.
Strength and Limitations
One of the strengths of this study was that it targeted ZRP patients, a special type of pain group, and focused on opioid use, quantifying the risk of chronic opioid use in these patients. Secondly, most of the current studies on the persistent opioids used capture opioid prescription information through Medicare prescription claims data or large pharmacies, so these studies captured less information based on the real situation of individuals and all age groups. However, the missing information may include the true whereabouts of the opioids and other real conditions other than pain. Although the information captured through telephone interviews in our study was limited and sometimes inaccurate, it represented a relatively true condition of the patients.
Despite the many strengths, there were some limitations to our study. First, because this was a study performed in a “real” clinical setting and patients were not randomly assigned to either of the two groups, they were not perfectly comparable at baseline. In this retrospective study, participants were selected from patients enrolled in the established ZRP database, which pooled each hospitalized patient’s basic informations such as hospitalization medical records, prescription, imaging, and related laboratory data. Because of this, the information we can collect is limited by the content of the database. The results of this study could demonstrate an important potential risk, which needed to be verified by more complete, in-depth, and larger sample size studies in the future. Second, we did not perform a detailed collation and calculation of the specific dose and time of opioid use during hospitalization. Third, in this real cohort, involving opioids were mainly composed of compound opioid analgesics, less strong opioids, it was associated with China history, and more stringent controls on opioid drugs in China. But the study also suggested we should avoid the blind and repeated use of opioids due to the easy availability and concealability of compound opioid analgesics, which might increase the risk of abuse.
Conclusion
This study demonstrated that opioids administration during hospitalization might increase the risk of ZRP patients becoming chronic opioid users, and the use of opioids during the whole duration of ZRP had limited benefits in pain control and quality of life improvement. Although opioids would be better to help patients with ZRP, it is still necessary to consider repeatedly when prescribing and continuing to use opioids, combine with other effective analgesic methods as much as possible, strengthen medication supervision and follow-up, so as to gain long-term benefits for patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funded by grant 2023HXFH036 1·3·5 project for disciplines of excellence–Clinical Research Fund, West China Hospital, Sichuan University, supported by grant 2022NSFSC0710 from the Science and Technology Department of Sichuan Province and grant 2022-YF05-01343-SN from the Chengdu Science and Technology Bureau.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weinberg JM. Herpes zoster: epidemiology, natural history, and common complications. J Am Acad Dermatol. 2007;57(6 Suppl):S130–135. doi:10.1016/j.jaad.2007.08.046
2. Torcel-Pagnon L, Bricout H, Bertrand I, et al. Impact of Underlying Conditions on Zoster-Related Pain and on Quality of Life Following Zoster. J Gerontol a Biol Sci Med Sci. 2017;72(8):1091–1097. doi:10.1093/gerona/glw189
3. Yang F, Yu S, Fan B, et al. The Epidemiology of Herpes Zoster and Postherpetic Neuralgia in China: results from a Cross-Sectional Study. Pain Ther. 2019;8(2):249–259. doi:10.1007/s40122-019-0127-z
4. Liu T, Yang J, Wang Y, Jiang W, Luo Y, Feng X and Mei W. (2023). Interfascial plane block: a new anesthetic technique. APS, 1(4), 10.1007/s44254-023-00028-0
5. Cruccu G, Truini A. A review of Neuropathic Pain: from Guidelines to Clinical Practice. Pain Ther. 2017;6(Suppl 1):35–42. doi:10.1007/s40122-017-0087-0
6. Bates D, Schultheis BC, Hanes MC, et al. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019;20(Suppl 1):S2–s12. doi:10.1093/pm/pnz075
7. Katz J, Cooper EM, Walther RR, Sweeney EW, Dworkin RH. Acute pain in herpes zoster and its impact on health-related quality of life. Clin Infect Dis. 2004;39(3):342–348. doi:10.1086/421942
8. Drolet M, Brisson M, Schmader KE, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. Cmaj. 2010;182(16):1731–1736. doi:10.1503/cmaj.091711
9. Häuser W, Morlion B, Vowles KE, et al. European* clinical practice recommendations on opioids for chronic noncancer pain - Part 1: role of opioids in the management of chronic noncancer pain. Eur J Pain. 2021;25(5):949–968. doi:10.1002/ejp.1736
10. Sommer C, Klose P, Welsch P, Petzke F, Häuser W. Opioids for chronic non-cancer neuropathic pain. An updated systematic review and meta-analysis of efficacy, tolerability and safety in randomized placebo-controlled studies of at least 4 weeks duration. Eur J Pain. 2020;24(1):3–18. doi:10.1002/ejp.1494
11. Brummett CM, Waljee JF, Goesling J, et al. New Persistent Opioid Use After Minor and Major Surgical Procedures in US Adults. JAMA Surg. 2017;152(6):e170504. doi:10.1001/jamasurg.2017.0504
12. Southren DL, Moser S, Abu-Amara H, et al. Opioid Fills for Lumbar Facet Radiofrequency Ablation Associated with New Persistent Opioid Use. Anesthesiology. 2020;132(5):1165–1174. doi:10.1097/ALN.0000000000003164
13. Calcaterra SL, Yamashita TE, Min SJ, Keniston A, Frank JW, Binswanger IA. Opioid Prescribing at Hospital Discharge Contributes to Chronic Opioid Use. J Gen Intern Med. 2016;31(5):478–485. doi:10.1007/s11606-015-3539-4
14. Bicket MC, Lin LA, Waljee J. New Persistent Opioid Use After Surgery: a Risk Factor for Opioid Use Disorder? Ann Surg. 2022;275(2):e288–e289. doi:10.1097/SLA.0000000000005297
15. Jivraj NK, Raghavji F, Bethell J, et al. Persistent Postoperative Opioid Use: a Systematic Literature Search of Definitions and Population-based Cohort Study. Anesthesiology. 2020;132(6):1528–1539. doi:10.1097/ALN.0000000000003265
16. Zhou BF. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15(1):83–96.
17. Tan KC. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
18. Kelly AM. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg Med J. 2001;18(3):205–207. doi:10.1136/emj.18.3.205
19. Lara-Solares A, Aguayo Zamora C. Latin-American guidelines for opioid use in chronic nononcologic pain. Pain Manag. 2017;7(3):207–215. doi:10.2217/pmt-2016-0065
20. Ung C, Yonekawa Y, Waljee JF, Gunaseelan V, Lai YL, Woodward MA. Persistent Opioid Use after Ophthalmic Surgery in Opioid-Naive Patients and Associated Risk Factors. Ophthalmology. 2021;128(9):1266–1273. doi:10.1016/j.ophtha.2021.04.021
21. Chen LK, Arai H, Chen LY, et al. Looking back to move forward: a twenty-year audit of herpes zoster in Asia-Pacific. BMC Infect Dis. 2017;17(1):213.
22. Maree RD, Marcum ZA, Saghafi E, Weiner DK, Karp JF. A Systematic Review of Opioid and Benzodiazepine Misuse in Older Adults. Am J Geriatr Psychiatry. 2016;24(11):949–963. doi:10.1016/j.jagp.2016.06.003
23. Sordo L, Barrio G, Bravo MJ, et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ. 2017;357:j1550. doi:10.1136/bmj.j1550
24. Häuser W, Schubert T, Vogelmann T, Maier C, Fitzcharles MA, Tölle T. All-cause mortality in patients with long-term opioid therapy compared with non-opioid analgesics for chronic non-cancer pain: a database study. BMC Med. 2020;18(1):162. doi:10.1186/s12916-020-01644-4
25. Hamilton M, Kwok WS, Mathieson S, et al. Opioid deprescribing in patients with chronic non-cancer pain: a systematic review of international guidelines. Pain. 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.