Back to Journals » Journal of Pain Research » Volume 15
Open-Label Adhesion Performance Study of a Prescription Lidocaine Topical System 1.8% versus Three Lidocaine-Containing Over-the-Counter Patches in Healthy Subjects
Authors Fudin J ![]() , Vought K, Patel K, Lissin D, Maibach H
, Vought K, Patel K, Lissin D, Maibach H
Received 12 April 2022
Accepted for publication 29 June 2022
Published 26 July 2022 Volume 2022:15 Pages 2051—2065
DOI https://doi.org/10.2147/JPR.S369128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Jeffrey Fudin,1– 3 Kip Vought,4 Kalpana Patel,4 Dmitri Lissin,4 Howard Maibach5
1Pain Management and PGY2 Pharmacy Pain Residency, Samuel Stratton Department of Veterans Affairs Medical Center, Albany, NY, USA; 2Remitigate Therapeutics, Delmar, NY, USA; 3Department of Pharmacy, Albany College of Pharmacy and Health Sciences, Albany, NY, USA; 4Clinical Development, Scilex Pharmaceuticals Inc, Palo Alto, CA, USA; 5Dermatology Department, University of California San Francisco, San Francisco, CA, USA
Correspondence: Dmitri Lissin, Clinical Development, Scilex Pharmaceuticals Inc, 960 San Antonio Road, Palo Alto, CA, 94303, USA, Tel +1 650.516.4310, Email [email protected]
Purpose: This study evaluates and compares the clinical adhesion performance of a prescription lidocaine topical system 1.8% versus two different over-the-counter (OTC) lidocaine patches 4% and an OTC combination menthol and lidocaine patch 1%/4% in human subjects.
Patients and Methods: This study was an open-label, randomized, four-treatment, four-sequence, Phase 1 adhesion performance study in healthy adult volunteers (N = 24). Lidocaine topical system 1.8% (R) and the three OTC patch products (T1, T2, and T3) were separately applied for 12 hours. Adhesion of all products was scored at 0, 3, 6, 8, and 12 hours post-application.
Results: There were no issues with the conduct of the study. Overall, the majority (≥ 59.1%) of subjects treated (“patched”) with the lidocaine topical system 1.8% (R) demonstrated ≥ 90% adhesion (FDA adhesion score 0) throughout the 12-hour administration period versus 27.3% of subjects treated with OTC lidocaine patch 4% (T1), 22.7% of subjects treated with OTC lidocaine patch 4% (T2), and 18.2% of subjects treated with OTC menthol/lidocaine patch 1%/4%. Only one subject (4.5%) treated with lidocaine topical system 1.8% was observed with < 75% adhesion (FDA adhesion score < 2) versus 11 (50.0%) and 10 (45.5%) for the two OTC lidocaine patches 4% (T1 and T2), respectively, and 13 (59.1%) subjects for the OTC menthol/lidocaine patch 1%/4%. There were no complete detachments observed for lidocaine topical system 1.8%, whereas 50.0% and 31.8% complete detachments were observed for the two OTC lidocaine patches 4% (T1 and T2), and 27.3% complete detachments were observed for the OTC menthol/lidocaine patch 1%/4%. No adverse events were observed for any of the treatments.
Conclusion: Lidocaine topical system 1.8% demonstrated superior adhesion relative to the three lidocaine-containing OTC products over the 12-hour treatment period.
Keywords: lidocaine topical system, lidocaine patch, menthol/lidocaine patch, over-the-counter, adhesion, postherpetic neuralgia, external analgesic
Introduction
Lidocaine, a well-established topical analgesic in the treatment of neuropathic pain, is available in prescription and over-the-counter (OTC) products in dosage forms including gels, salves, liquids, sprays and patches/topical systems.1 The rising importance of topical lidocaine in the treatment of neuropathic pain is a culmination of its safety relative to oral OTC and prescription analgesics (ie, acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and opioids) that have not demonstrated meaningful efficacy in the treatment of neuropathic pain in large adequately controlled clinical studies and have well-documented treatment-limiting toxicities,2–6,44–46 and its multimodal analgesia for neuropathic pain due to its interruption of the pain signals along the neural pathways in skin.7,8 These properties recently led the Centers for Disease Control (CDC) to recommend that clinicians consider topical agents, including lidocaine, as alternative first-line therapies for neuropathic pain treatment.9 There is an overall trend towards the use of topical products in general for the pharmacologic treatment of pain due to reduced systemic toxicities. In fact, the 2019 American College of Rheumatology (ACR) guideline suggests that topical therapies (ie, NSAIDs and capsaicin) should be considered for first-line pharmacologic treatment of osteoarthritis.40
Lidocaine is an amide-type local anesthetic agent that stabilizes neuronal membranes by inhibiting the ionic fluxes required for initiation and conduction of nerve impulses (ie, pain signals).10 Because topically applied lidocaine penetrates only about 8 to 10 mm into skin, it is well suited for targeted use in peripherally localized pain.11,12 Penetration of lidocaine after application of the lidocaine patch 5% was sufficient to produce an analgesic effect in the treatment of pain associated with post-herpetic neuralgia (PHN), but less than the amount necessary to produce a complete sensory block.13 In 1999, the US Food and Drug Administration (FDA) granted approval for Lidoderm® (lidocaine patch 5%; Endo Pharmaceuticals Inc., Malvern, PA) as the first medication specifically indicated for the treatment of PHN pain.13–15
In February 2018, the FDA approved ZTlido® (lidocaine topical system 1.8%; Scilex Pharmaceuticals Inc., San Diego, CA), which is also approved by the FDA for the treatment of pain associated with PHN in adults based, in part, on the demonstration of bioequivalence to lidocaine patch 5% allowing for comparable pain relief with greater lidocaine bioavailability.16,17 While delivering comparable drug level as lidocaine patch 5%, lidocaine topical system 1.8% contrasts with lidocaine patch 5% as a thinner and flexible anhydrous delivery system with a significantly reduced drug load per system (36 mg vs 700 mg).18,19 In addition to the demonstration of bioequivalence to lidocaine patch 5%, lidocaine topical system 1.8% was clinically characterized for the effects of heat and exercise, dermal safety, and adhesion performance.17–21 Lidocaine topical system 1.8% was recently evaluated for adhesion performance and pharmacokinetics under water stress conditions of bathing and swimming leading to labeling allowing patients to use the product under these conditions.22
The FDA published guidance to create standards for the quality of prescription new and generic topical and transdermal systems, adhesion performance, dermal safety, and residual drug levels after product use.23–27 Paramount to safe and effective use of patches and topical systems is the maintenance of adequate adhesion throughout the prescribed administration period and under the labeled conditions of use (eg, normal use, exercise, etc.).23 This is especially the case for lidocaine patches and topical systems as the drug is compounded within the adhesive formulation for these products; therefore, any area of lifting of the product from the skin results in diminished drug delivery.1,28–30
The FDA has received numerous reports of adhesion failure for prescription lidocaine patch 5% products —including edge curling, partial lifting, or complete detachment of patches—resulted in improper dosing as well as repeat application, leading to increased cost.31 Approximately 75% of AEs reported to the FDA Adverse Event Reporting System (FAERS) for topical lidocaine 5% patches from 2018 to 2021 were related to product adhesion issues (1050 adhesion issues out of 1367 reported total AE cases).31 In contrast, lidocaine topical system 1.8% has 27 out of 88 (30%) AEs related to product adhesion issues during the same period.31 This disparity is expected given that lidocaine topical system 1.8% demonstrated superior clinical adhesion performance relative to the lidocaine patches 5%. Specifically, across the three studies, ≥75% of subjects treated with lidocaine topical system 1.8% demonstrated ≥90% adhesion throughout a 12-hour administration period versus 13.6% subjects treated with lidocaine patch 5% and 0% subjects treated with a generic lidocaine patch 5%. There were no complete detachments for lidocaine topical system 1.8% versus 4.5% and 29% complete detachments for lidocaine patch 5% and a generic lidocaine patch 5%, respectively.21
Over-the-counter lidocaine patches are commonly utilized in treating acute and chronic pain, however their pharmacokinetics, safety, efficacy, and adhesion performance have not been formally evaluated via clinical studies that would support OTC market applications.1,32–35 Consequentially, these lidocaine-containing OTC products have not undergone FDA review to ensure they meet the same clinical and quality standards established for prescription patch or topical system products.1 Instead, these lidocaine-containing OTC patch products are purported to conform with the tentative final monograph (TFM) for external analgesics (21 CFR Part 348).37 Of note, the only OTC external analgesic patch product that has been formally reviewed and approved by the FDA is Salonpas® Methyl Salicylate 10% + Menthol 3% Patch, which is not a lidocaine-containing product.41
Many OTC patch products lack pharmacokinetic or efficacy data.1,32 While these products are purported to conform with the external analgesic TFM, the FDA formally designated external analgesic OTC topical patches, plasters, and poultices as Category III (ie, safety and efficacy unknown). The FDA stated that in order for these dosage forms to be generally recognized as safe and effective, further data would be required including concentration of the drug ingredient(s); extent of percutaneous absorption under occlusion; length of contact time that it is safe to leave the product on skin; how often the plaster or poultice needs to be changed for optimal use; frequency of application considered safe and effective; whether or not directions and a warning are necessary regarding checking the area at specified intervals for erythema to prevent blistering; the age groups for whom poultices and plasters are recommended for safe use; and the adequacy of labeling of currently marketed analgesic.36,37 Nevertheless, these OTC topical analgesic products, OTC lidocaine patch products in particular, remain marketed and widely used with their safety and efficacy primarily extrapolated from prescription products without robust comparisons.32–35
Given the importance of adhesion for the safety and efficacy of OTC lidocaine-containing patches, a clinical study was performed to characterize and compare the adhesion performance of two OTC lidocaine patches 4% (Salonpas®, Lot WCA09, Hisamitsu Pharmaceutical Co., Inc.; and Aspercreme®, Lot 020, Chattem, Inc.) and one OTC menthol/lidocaine patch 1%/4% (IcyHot® Max, Lot A051, Chattem, Inc.) versus prescription lidocaine topical system 1.8% (ZTlido®, Lot 201201, Scilex Pharmaceuticals Inc.) (Table 1) in 22 normal healthy subjects over a 12-hour administration period.
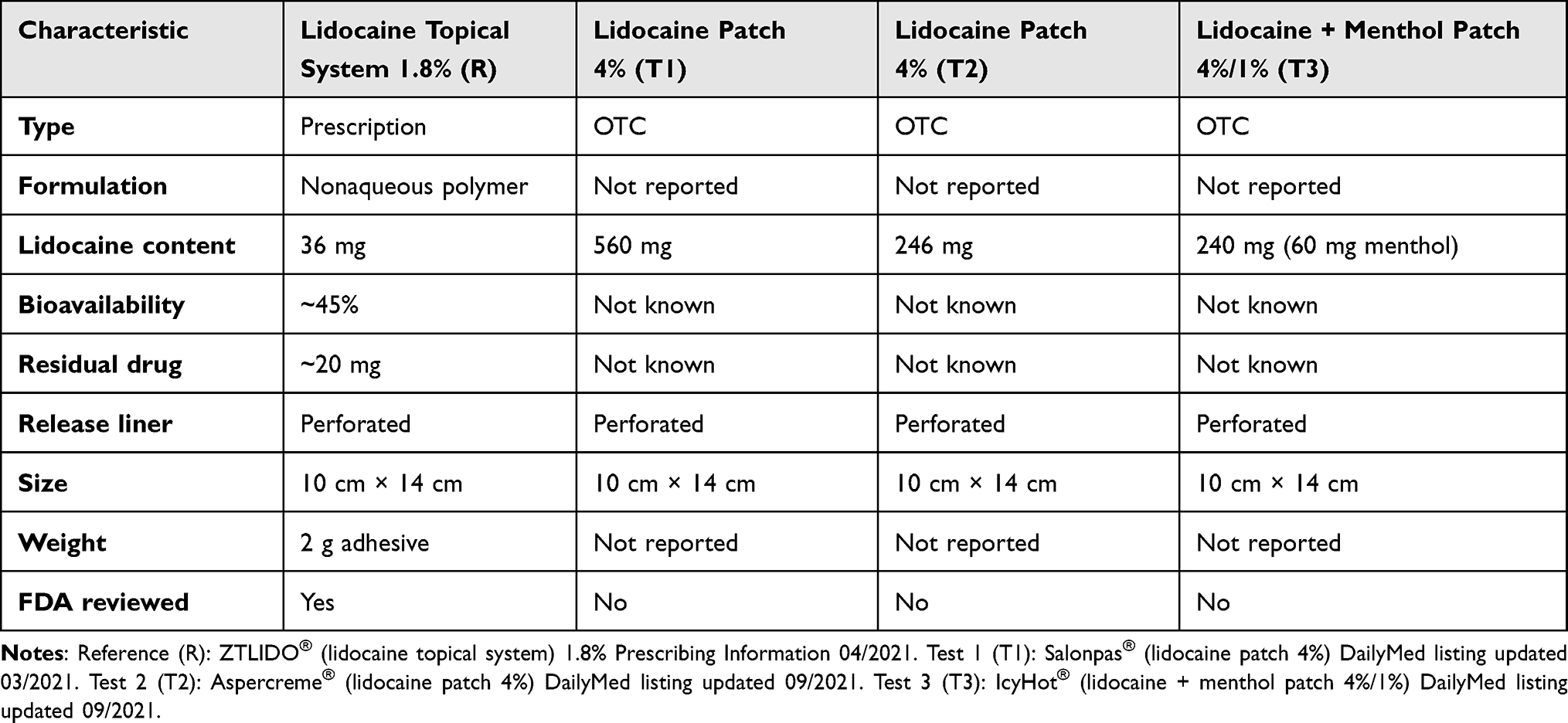 |
Table 1 Characteristics of Studied Lidocaine Topical Products |
Methods
Study Design
This was an open-label, randomized, four-treatment, four-sequence, four-period, crossover, single-application study evaluating and comparing product adhesion of lidocaine topical system 1.8% (Reference) versus lidocaine patch 4% (Salonpas®, Test 1), lidocaine patch 4% (Aspercreme®, Test 2), and menthol/lidocaine patch 1%/4% (IcyHot, Test 3) in healthy, adult human subjects. The Reference product was selected as it has established the quality attributes and adhesion performance as outlined in FDA guidance. The Test 1, 2, and 3 products were selected because they were lidocaine-containing at 4% ratio of drug to adhesive and are widely marketed in the United States (US).
The study was conducted at AXIS Clinicals, Dilworth, MN, from July 16 to 20, 2021, and was approved by the WCG Institutional Review Board (IRB) located in Puyallup, WA, and conducted in accordance with the ethical principles originating from the Declaration of Helsinki and amendments, ICH Guideline for Good Clinical Practice, FDA Guidance for Industry: Assessing Adhesion With Transdermal and Topical Delivery Systems for ANDAs, and local regulatory requirements.25,38,39,43 The study was conducted in accordance with the FDA’s guidance for assessing adhesion for generic products submitted as abbreviated new drug applications (ANDAs) to test the hypothesis that the Test products (OTC lidocaine-containing patches) have noninferior adhesion performance relative to the Reference product (lidocaine topical system 1.8%). The study is registered at ClinicalTrials.gov with the clinical trial registration number: NCT05106400.
Subjects
The study was performed in healthy adult human volunteers. Eligible subjects were men or women ≥18 years of age, with a body mass index (BMI) between 18.0 and 32.49 kg/m2 inclusive (within the BMI range of previous adhesion studies performed on lidocaine topical system 1.8%).21 The subjects were nonsmokers and healthy, as documented by medical history, physical examination (including evaluation of cardiovascular, gastrointestinal, respiratory, musculoskeletal, and central nervous systems), and vital sign assessments, with no evidence of underlying disease during check-in and screening performed within 28 days of check-in. Female subjects could not be pregnant or lactating, and those of childbearing age were instructed to practice medically acceptable contraception throughout the study. All subjects provided prior written informed consent and were able to comply with study procedures.
Exclusion criteria included allergy or known hypersensitivity to lidocaine, local anesthetics of the amide type, or any of the components of the lidocaine topical system formulations; any major illness in the last 3 months or any significant ongoing chronic medical illness; history of addiction, abuse, and misuse of any drug; history of mental illness; presence or history of a clinically significant disorder involving the cardiovascular, respiratory, renal, hepatic, dermatologic, musculoskeletal, gastrointestinal, immunologic, hematologic, endocrine or neurologic system(s) or psychiatric disease; participation in any clinical trial within 30 days; use of antiarrhythmic drugs and local anesthetics within 14 days; and use of nicotine containing products within 30 days. Subjects needed to test negative for drugs of abuse and alcohol breath analysis prior to product administration.
Of relevance to dermatologic adhesion studies, subjects could not have the following: history of significant dermatologic cancers (eg, melanoma, squamous cell carcinoma), except basal cell carcinomas that were superficial and did not involve the investigative site; presence of any current dermatologic condition (eg, psoriasis, eczema, atopic dermatitis) or any skin conditions such as scratches, cuts, scars, abrasions, excessive hair, tattoos, moles, recently shaved skin, uneven skin texture, irritated skin (redness, rash, blisters, etc), or excessively oily skin at the application areas that may have affected the application or adhesive properties of the study products; and medical history of hyperhidrosis or otherwise history of excessive sweating under non-exercising conditions. Subjects were also excluded if they presented with inflamed or injured skin, such as active herpes zoster lesions, atopic dermatitis or wounds where the product would be placed.
Subjects were confirmed to have a negative SARS-CoV-2 PCR virus test within 4 days prior to each period check-in or a negative SARS-CoV-2 rapid detection antigen test (regardless of vaccine status) at each period check-in. Subjects were to adhere to the COVID-19 guideline provided by the clinic and exercise precautions such as using hand sanitizer, washing hands, wearing a mask, and maintaining physical distancing.
Treatments
This was a four-period study (Periods I, II, III, and IV) with subjects randomized to receive either the reference product (R) or one of the three test products (T1, T2, or T3). The treatment sequences consist of R/T1/T2/T3, T1/T2/T3/R, T2/T3/R/T1, and T3/R/T1/T2 where the Reference Product (R) was ZTlido® (lidocaine topical system 1.8%), Test Product 1 (1) was Salonpas® (lidocaine patch 4%), Test Product 2 (T2) was Aspercreme® (lidocaine patch 4%), and Test Product 3 (T3) was IcyHot® (lidocaine 4% + menthol 1% patch). A single topical system was applied for each treatment, and there was an 11.75-hour washout period between treatments.
Prior to product application, hair on the application site was clipped if necessary (not shaved) by clinical staff, and the site gently cleansed with water and patted dry with dry gauze. No soaps or any cleansing agents were allowed to clean the application site. The application area was also checked to ensure absence of any skin condition abnormalities (eg, broken skin, moles, and uneven skin texture) and ensure that the site had not recently shaved, had excessive hair, or covered with tattoos or similar embodiments. Subjects were asked and confirmed to have avoided clothing lines or areas where the adhesions of the product may be compromised by rubbing.
The approximate location of the application site was outlined on the predetermined area on the right or left side of the mid to upper back according to the randomization schedule. Each product (R, T1, T2, and T3) was applied to the same area for each subject. Application involved pressing the product firmly into place, holding it with the palm of the hand for up to 15 seconds, and smoothing it to prevent air bubble trapping. No overlays, adhesive tapes, bandages, or similar products were applied during the application period. Subjects were also continuously monitored to ensure sitting with their back pressed against the back of chairs. Subjects were not allowed to lie in beds or recliners during the 12-hour treatment period. Subjects were housed in the clinic from ~12 hours prior to Period I until at least 14 hours post-application of the test article in Period IV.
Each product was worn for 12 hours (±15 minutes) in each application period, which occurred during daylight hours (morning to evening). If the product detached during the treatment period, the date and time of detachment was recorded with no application of a new product. Subjects with complete detachment were assigned a score of 0% adhesion (FDA adhesion score of 4) for all the remaining observations in the application period and continued with the study into the subsequent periods.
After the 12-hour administration period, the product was removed and the application site gently wiped with gauze. The used products were folded in half with the adhesive sides facing each other and saved in a Ziploc bag along with the product envelope.
Snacks and meals were provided, and water was allowed ad libitum.
Subject Compliance
Subjects were not allowed to shower or bathe up to one hour prior to product application and throughout the administration period and were instructed to avoid getting the product wet during the confinement period. Use of soap or topical products (eg, lotion, oil, makeup, and powder) was not permitted on the study product application site for 48 hours prior to product application and throughout the entire study duration. Subjects were instructed to avoid rubbing, pulling, scratching, or touching the product or performing any other activity that might cause product displacement. Specifically, they were to avoid putting pressure between the product and other objects (eg, walls, chairs, and beds) and could not participate in strenuous activity (eg, rigorous exercise) but could ambulate and perform activities freely if these required no physical exertion or otherwise could hamper product adhesion. They were not allowed to press down or readhere any product that was lifting or detaching. Instead, subjects were instructed to notify clinical staff of detached products. Subjects were also required to avoid exposing the product to external sources of direct heat (eg, hair dryers, heating pads, heat lamps, and saunas) and prolonged direct sunlight throughout the confinement period in the study facility.
Prior and Concomitant Therapy
Subjects could not use prescription medications, except for hormonal contraception, within 14 days prior to the first product application and throughout the study. Over-the-counter medications were not allowed within the prior 5 days, but occasional use of acetaminophen, supplements, and vitamins was permitted. In addition, subjects refrained from using antiarrhythmic drugs, such as tocainide and mexiletine, and local anesthetics within 14 days prior to product application and throughout the study. Subjects were prohibited from using nicotine-containing products (eg, e-cigarettes, patches, gum, chewing tobacco) within 30 days prior to product application and from consuming caffeine and/or xanthine-containing products (ie, coffee, tea, chocolate, and caffeine-containing soda, etc.), grapefruit, grapefruit-containing products, alcohol, and poppy seed–containing foods within 48 hours prior to product application.
Study Objectives
The primary objective was to evaluate and compare the clinical adhesion performance of lidocaine topical system 1.8% of Scilex Pharmaceuticals Inc. (Reference (ZTlido®)) versus 2 OTC lidocaine patches 4% (Test 1 (Salonpas®) and Test 2 (Aspercreme®)) and an OTC menthol/lidocaine patch 1%/4% (Test 3 (IcyHot®)), when each is applied to clean, dry, hairless, intact healthy skin on the mid to upper back and worn for 12 hours in healthy, adult, human subjects. An additional secondary objective was to assess the safety and tolerability of the regimens (ie, Treatments Reference, Test 1, Test 2, and Test 3) in subjects. All reference and test products shared the same dimensions of 10 cm × 14 cm.
Study Assessments
Adhesion
Adhesion was assessed immediately after application (0 hours) and at 3, 6, 8, 10, and 12 hours (±15 minutes) after each product application (R, Test 1, Test 2, and Test 3). The 8-hour time point was specifically selected as the Test 1 product is labeled to be administered for 8 hours while all other products are labeled for up to a 12-hour administration. Degree of adhesion was assessed by a trained scorer using a transparent grid with evenly spaced dots. The grid was demarcated to the exact size of each product (ie, 10 × 14 cm). The dot matrix grid was gently laid over the product on the skin, and areas of adhesion were outlined; dots excluded from adhering areas were counted to identify the exact surface area of “lift-off”, allowing the determination of the total amount of product adhesion as a percentage (ie, percent adhesion). Percent adhesion for each individual product was also transposed to the FDA 5-point scale as follows:
- 0: ≥90% adhered (essentially no lift off the skin)
- 1: ≥75% to <90% adhered (some edges only lifting off the skin)
- 2: ≥50% to <75% adhered (less than half of the TDS lifting off the skin)
- 3: >0% to <50% adhered (not detached, but more than half of the TDS lifting off the skin without falling off)
- 4: 0% adhered (TDS detached; completely off the skin).
For products that had completely detached prior to the end of a 12-hour application period, 0% adhesion and a score of 0% (FDA adhesion score of 4) was carried through in the adhesion analysis for all the remaining observations in that application period. At baseline and at each adhesion observation time point, a picture of the application was taken.
Safety
Subjects were monitored and documented for any adverse events (AEs). Subjects were required to inform study personnel of any AEs that may occur during the study. A medically qualified designee was available during confinement at the clinical facility. Dermal AEs were reported, but no formal skin irritation assessments were performed. Subjects also filled out a subject well-being questionnaire (SWBQ).
Statistical Analyses
Statistical analyses were performed using SAS® Version 9.4 (SAS Institute Inc., Cary, NC). Weighted mean adhesion score (MAS) was calculated for individual subjects at each time point, and descriptive statistics (ie, N, mean, and standard deviation) was calculated for weighted MAS. Descriptive statistics (ie, mean, standard deviation, median, minimum, and maximum) were generated for the cumulative weighted MAS for each product (Reference, Test 1, Test 2, and Test 3).
The primary analysis for this study was determined based on the distribution of the MAS data of individual Reference, Test 1, Test 2, and Test 3 products. General Linear Model (GLM) Analysis of Variance (ANOVA) was performed, in which the weighted MAS was treated as the dependent variable. Sequence, Period, and Treatment were treated as fixed effects and subject nested in sequence as a random effect.
The following hypotheses was tested at the significance level of 0.05:
H0: μt1 − μR ≥ δ and μt2 − μR ≥ δ H1: μt1 − μR < δ and μt2 − μR < δ
Where μR, μt1 and μt2 are the population means for the mean percent adhesion for Reference, Test 1, Test 2, and Test 3, respectively.
In addition to mean percent adhesion, the following secondary endpoints for evaluation of adhesion (descriptive statistics only) to assess the potential treatment group difference in clinically meaningful extreme values or events are:
- Proportion of subjects with an FDA adhesion score ≥2 (≥50% to <75% adhered (less than half of the TDS lifting off the skin)) at any time point, compared between four test products (Reference, Test 1, Test 2, and Test 3).
- Proportion of subjects with a Reference weighted MAS greater than the corresponding Test 1, Test 2, and Test 3 weighted MAS by FDA adhesion score >1 (≥75% to <90% adhered (some edges only lifting off the skin)), compared to the proportion of subjects with a Test 1-, Test 2-, and Test 3-weighted MAS greater than the corresponding Reference weighted MAS by FDA adhesion score >1.
- Time to an FDA adhesion score >2 (≥50% to <75% adhered (less than half of the TDS lifting off the skin)) compared between four products (Reference, Test 1, Test 2, and Test 3).
The number of complete detachments (ie, 0% and FDA score of 4) observed over the treatment period for each product was also assessed.
Because of the absence of any adhesion data in the public domain for Test 1, Test 2, and Test 3, a formal power analysis could not be performed. Instead, a sample size of 24 was determined for this 4-way crossover design based on the analysis of data from previous comparative adhesion studies between lidocaine topical system 1.8% and lidocaine patches 5%.24 In those studies, a sample size of 24 was sufficient to detect a difference in adhesion performance between the products in normal healthy populations where in separate studies the lidocaine topical system 1.8% demonstrated superior adhesion to the lidocaine patch 5% products (ie, Lidoderm® 5% manufactured by Endo Pharmaceuticals, Inc.) and associated generic (ie, lidocaine patch 5% manufactured by Mylan Pharmaceuticals Inc).24
While Test Product 1 is labeled to be administered up to 8 hours (versus 12 hours for the Reference and other Test Products), all statistical analyses are based on 12-hour administration data. Separate ad hoc 8-hour adhesion analyses would be performed between Test Product 1 and the Reference Product if the former presented distinctive performance (eg, improved performance) over the shorter treatment duration warranting the additional evaluation.
Results
Subject Disposition and Baseline Characteristics
Relative to the target population size of 24 subjects, a total of 22 subjects were enrolled and completed study. No subjects discontinued due to AEs (eg, unacceptable skin irritation) or were excluded due to a protocol deviation, and all 22 subjects received all four treatments (ie, R, T1, T2, and T3) and are included in the per protocol population for assessment (PPPA).
Overall, subjects ranged from 19 to 70 years of age with a mean of 37.86 ± 16.45 years and a median of 30.50 years. The population was evenly balanced (50:50) on gender (Table 2). All subjects were healthy, with vital signs within the normal range.
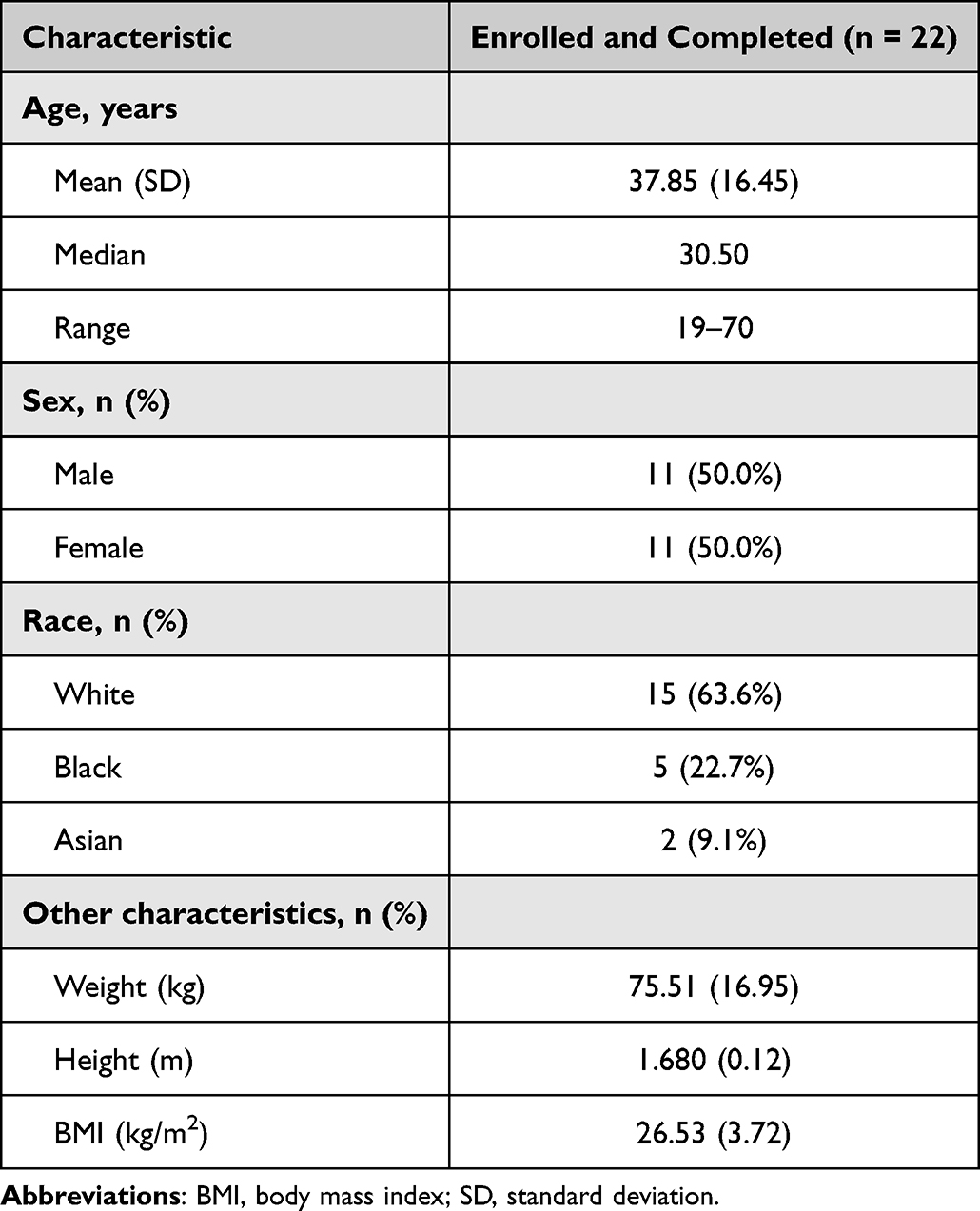 |
Table 2 Subject Demographics and Baseline Characteristics |
Adhesion Analysis
All 22 subjects received all four treatments (R, T1, T2, and T3) with adhesion evaluations performed at the time of application (ie, Time 0) and then at 3, 6, 8, 10, and 12 hours. For the Reference Product (lidocaine topical system 1.8%), the mean adhesion score decreased from 99.6% at Time 0 to 92.7% at 12 hours. This contrasts with Test Products 1 and 2 (Lidocaine Patches 4%) that saw decreases ranging from 99.0 to 45.1% and 99.3 to 58.8% over the same evaluation period, respectively. Test Product 3 (Lidocaine + Menthol Patch 4%/1%) saw a decrease from 98.7 to 58.2% over the same 12-hour evaluation period (Table 3 and Figure 1). No complete detachments (0% adhesion) was observed for the Reference Product, but 50% (11/22) complete detachments was observed for Test Product 1 (7/22 (31.8%) at 8 hours), 31.8% (7/22) for Test Product 2, and 27.3% (6/22) for Test Product 3 (Table 3). The mean cumulative adhesion across all time points was 94.0% (R), 56.7% (T1), 65.9% (T2), and 71.9% (T3) (Table 4).
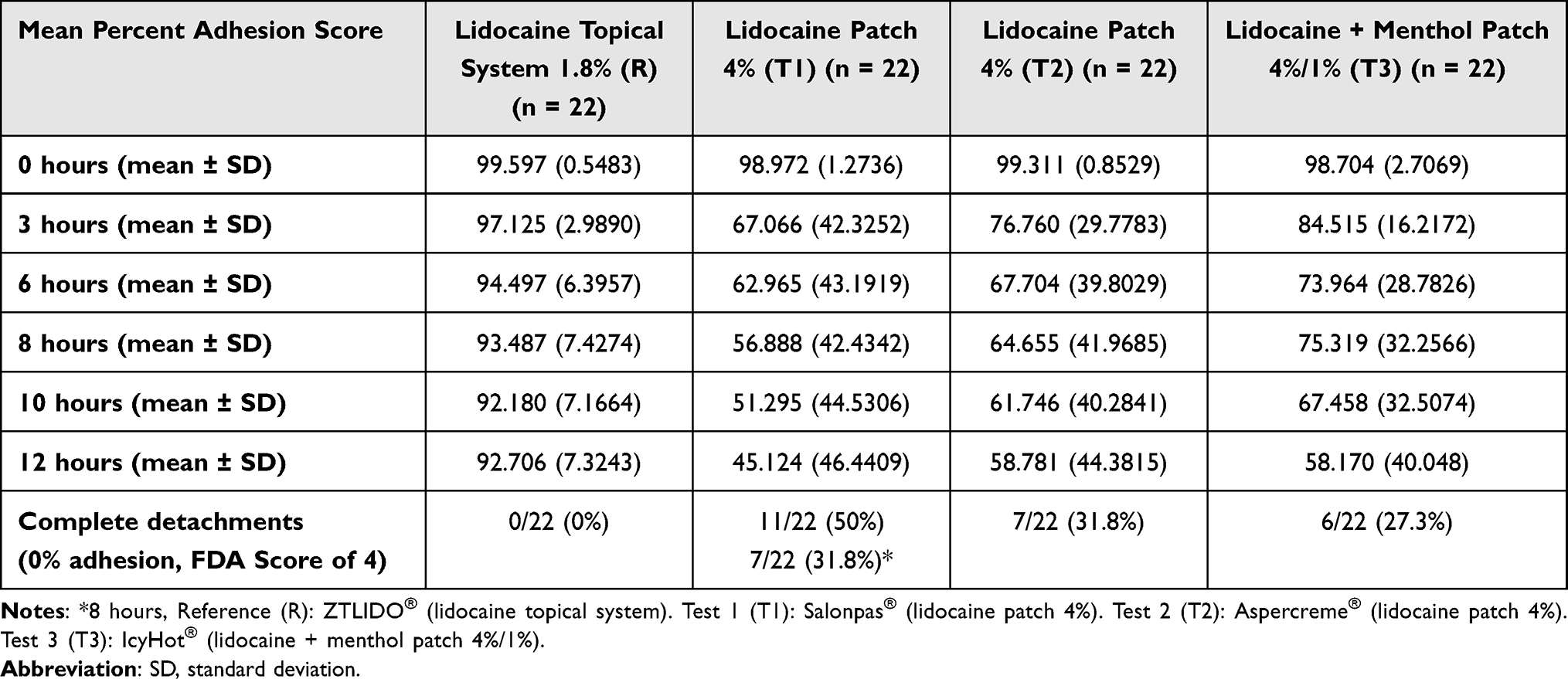 |
Table 3 Mean Percent Adhesion Over Time by Treatment and Number of Complete Detachments (R, T1, T2, and T3) |
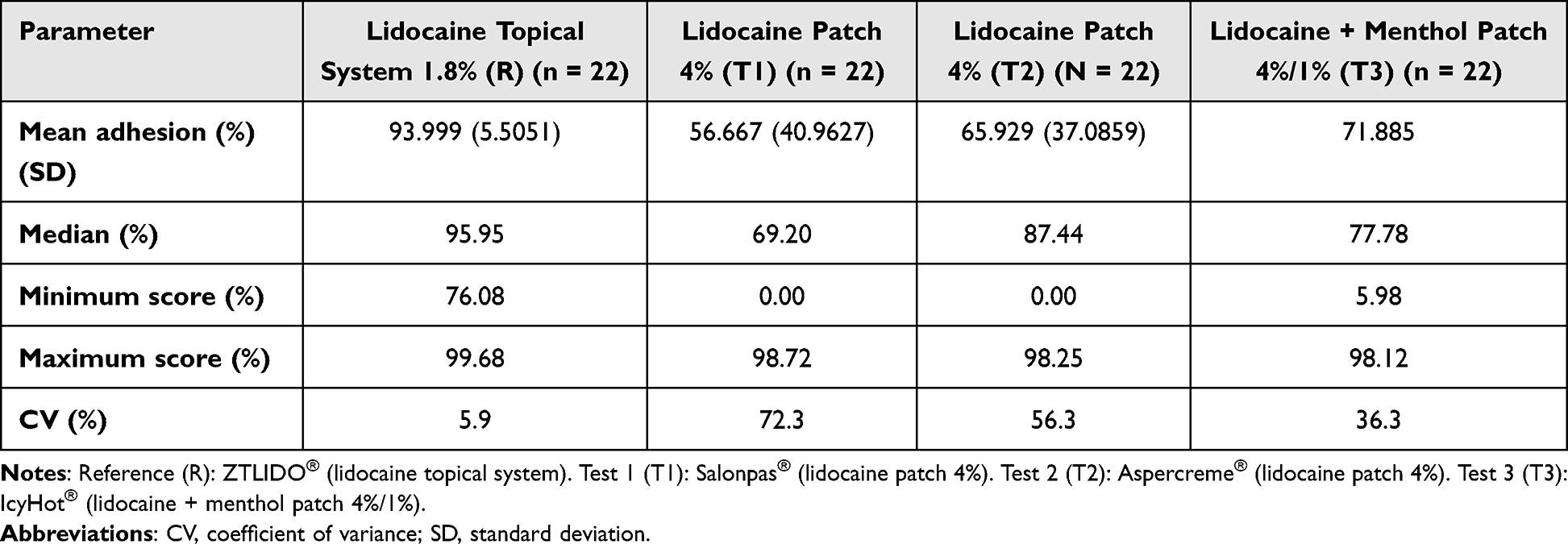 |
Table 4 Descriptive Statistics of Mean Percent Adhesion Scores by Treatment (R, T1, T2, and T3) (per Protocol Population for Adhesion) |
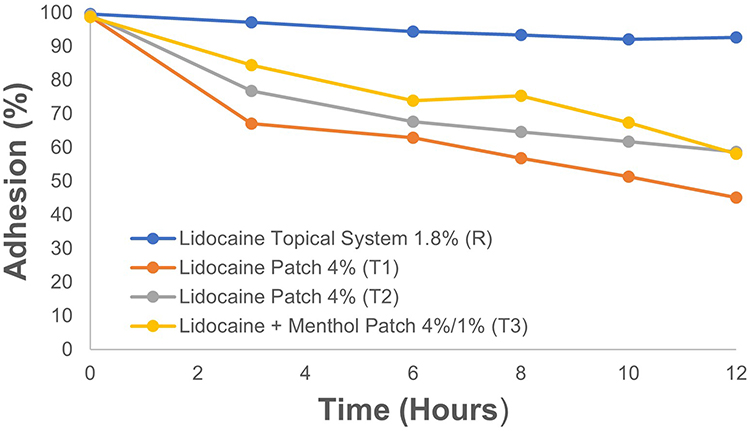 |
Figure 1 Mean percent adhesion over time by treatment (R, T1, T2, and T3). Reference (R): ZTLIDO® (lidocaine topical system). Test 1 (T1): Salonpas® (lidocaine patch 4%), test 2 (T2): Aspercreme® (lidocaine patch 4%), test 3 (T3): IcyHot® (lidocaine + menthol patch 4%/1%). |
When evaluating percent adhesion status at <10, <30, <50, and <90% adhesion, no subjects (0%) had adhesion scores of <10%, <30%, or <50% for the Reference Product. Nine (9) subjects (40.91%) demonstrated <90% adhesion at a mean time of 7.22 hours for the Reference Product. In contrast, 11 subjects (50%) were observed for OTC Product Test 1 to have <10%, <30% and <50% adhesion with respective mean time to these percent adhesion status ranging from 6 to 7 hours. For OTC Product Test 2, 7 subjects (31.82%) had <10% adhesion with a mean time to status of ~6 hours. Eight (8) subjects (36.36%) had <30% and <50% adhesion each for OTC Product Test 2 with respective mean times to status ranging between 6 and 7 hours. For OTC Product Test 3, 6 subjects (27.27%) had <10% and <30% adhesion each with respective mean times of ~9 hours. Nine (9) subjects (40.91%) were observed to have <50% adhesion with a mean time of ~8 hours. Most subjects (16–17 or 72.73 to 77.27%) with the OTC Test Products Test 1, Test 2, and Test 3 had <90% adhesion with a mean time to status of 4–5 hours (Table 5).
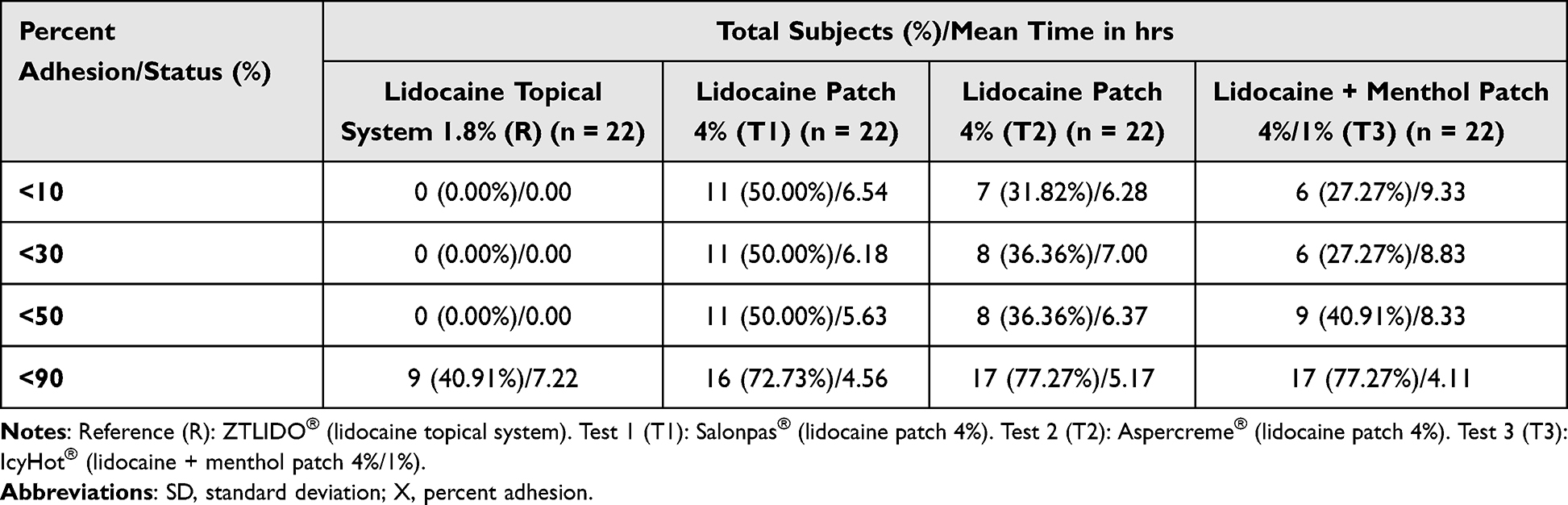 |
Table 5 Proportion of Subjects with Adhesion Score at Any Time Point/Time to Adhesion Score <X |
The lower limit of the confidence interval (CI) (ie, the upper 95% confidence bound) for the difference in Reference minus Test 1, Test 2, and Test 3 least-squares means of the mean percent adhesion scores was greater than zero. Therefore, the adhesive performance of the Reference Product (R) exceeded that of each of the OTC Test Products (ie, T1, T2, and T3). Likewise, the difference in the overall weighted mean adhesion scores for Test 1-Reference (T1-R), Test 2-Reference (T2-R), and Test 3-Reference (T3-R) were greater than that of non-inferiority (NI) margin of 0.15 (Table 6); therefore, the OTC Test Products (Test 1, Test 2, and Test 3) did not have superior adhesion performance to that observed for the Reference Product.
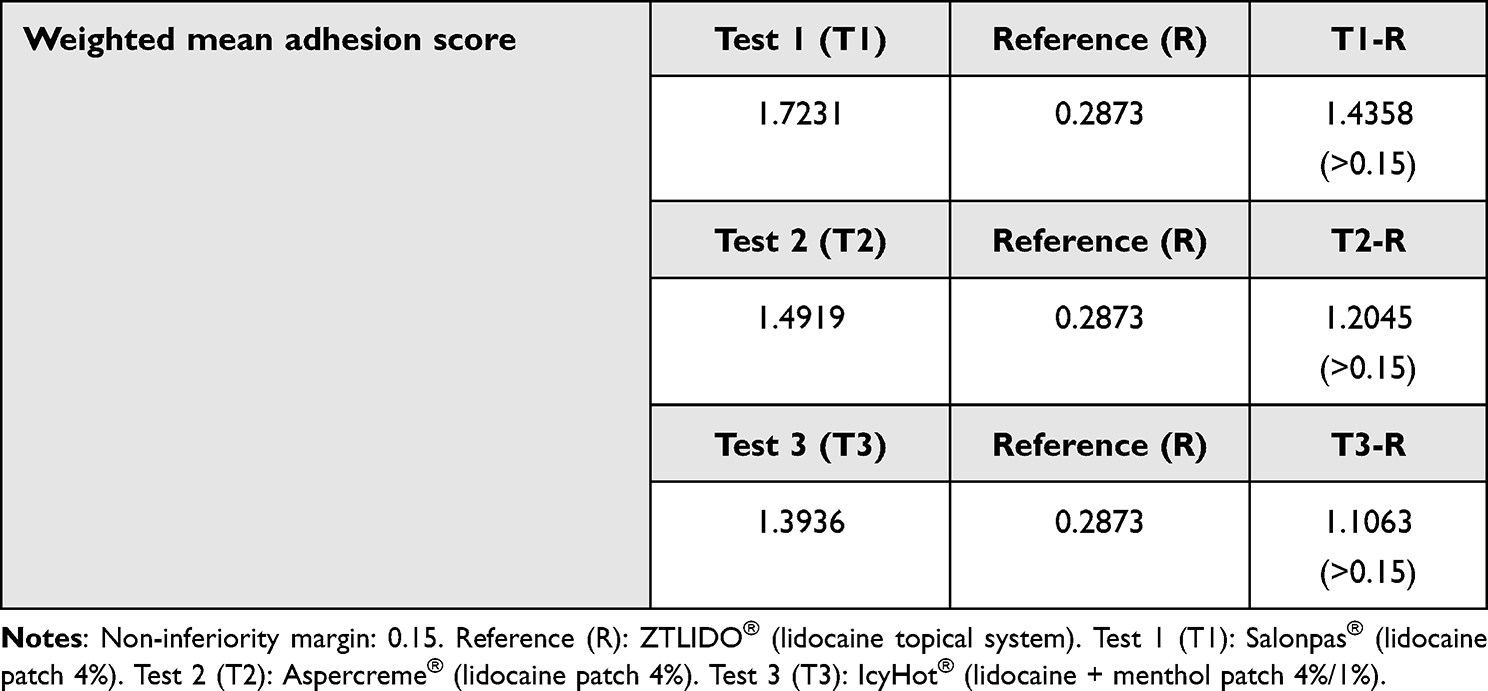 |
Table 6 Non-Inferiority Test for Evaluation of Adhesion Performance Between Test and Reference Products |
The lower 90% CI (ie, the upper 95% confidence bound) on the difference SAS estimate for the weighted mean adhesion scores of the Test 1-to-Reference (T1-R), Test 2-to-Reference (T2-R), and Test 3-to-Reference (T3-R) were 0.96, 0.73, and 0.63, respectively (Table 7). Because the lower 90% CI on the difference estimates for the weighted mean adhesion scores is greater than zero, the adhesion performance for the Reference Product was superior to that observed for the OTC Test Products (T1, T2, and T3).
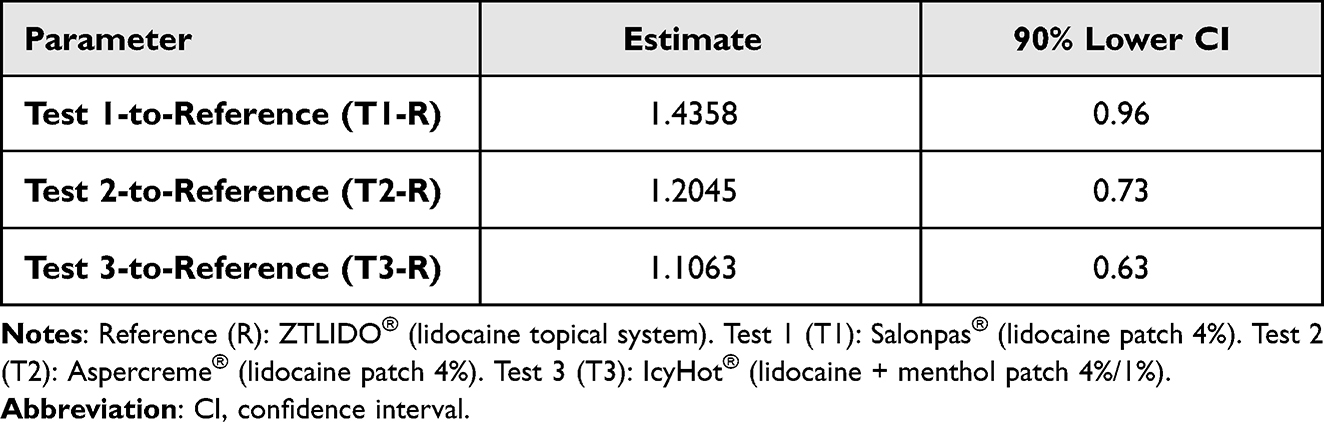 |
Table 7 90% Confidence Interval for Weighted Mean Percent Adhesion Score |
Because OTC Test Product 1 did not present significantly improved adhesion performance within 8 hours of treatment relative to the Reference Product or other OTC Test Products, additional ad hoc 8-hour statistical analyses were not warranted. Such analyses would likely confirm inferior adhesion performance for Test Product 1 relative to the Reference Product over 8 hours. Specifically, the mean percent adhesion for OTC Test Product 1 (56.9%) at 8 hours was below the mean adhesion observed for OTC Test Products 2 and 3 at 12 hours (ie, 58.8% and 58.2%, respectively). Likewise, the number of complete detachments for OTC Test Product 1 (7/22) was comparable to the number of complete detachments observed for OTC Test Products 2 and 3 (ie, 7/22 and 6/22, respectively).
Descriptively, the proportion of subjects with an FDA adhesion score ≥2 (ie, ≥50% to <75% adhered (less than half of the patch lifting off the skin)) for the Reference Product (0.0455, 1/22) were significantly less than that observed for the Test Products Test 1 (0.5000, 11/22), Test 2 (0.4545, 9/22, and Test 3 (0.5909, 13/22)) (Table 8). No subjects were observed with a weighted mean FDA adhesion score ≥1 (ie, ≥75% to <90% adhered (some edges only lifting off the skin)) for the Reference Product (0.000, 0/22), whereas the proportion of subjects with a weighted FDA mean adhesion score ≥1 for the OTC Test Products were significantly higher: Test 1 (0.500, 11/22), Test 2 (0.4091, 9/22), and Test 3 (0.5455, 12/22) (Table 9). While formal statistics were not performed, these differences are anticipated by the authors to be significant.
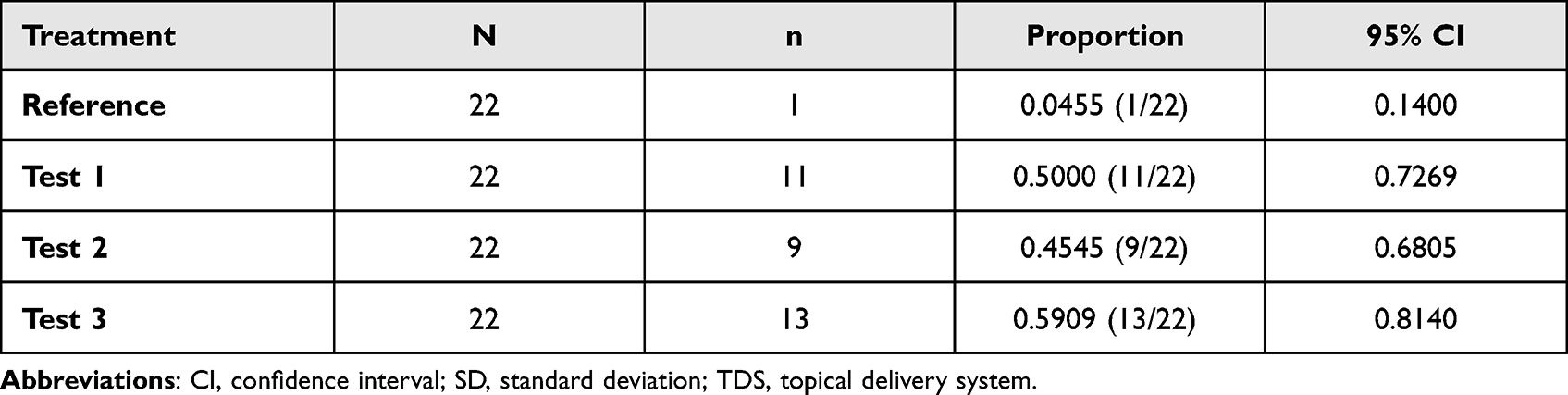 |
Table 8 Proportion of Subjects Having FDA Adhesion Score ≥2 (≥50% to <75% Adhered, Less Than Half of the TDS Lifting off the Skin) |
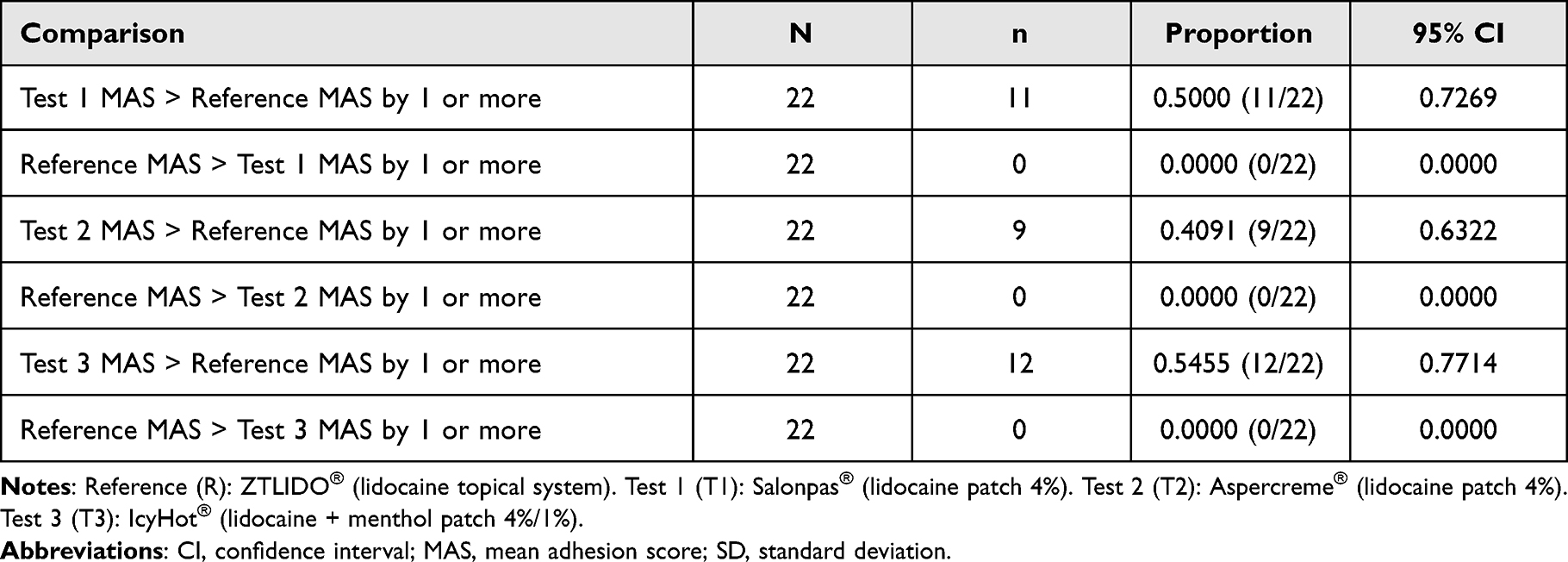 |
Table 9 Proportion of Subjects Having FDA Mean Adhesion Score (MAS) >1 (≥75% to <90% Adhered, Some Edges Only Lifting off the Skin) or More Among Treatments |
No subject was observed to have an FDA adhesion score >2 for the reference product. Eleven (11), 3, and 9 subjects were observed to have an FDA adhesion score >2 for OTC Test Products 1, 2, and 3 with a time to event ranging for these subjects between 3 and 10 hours, 3 hours, and 3–4 hours, respectively.
Safety
No AEs or serious adverse events (SAEs) were reported. While not formally assessed, there were no reports of skin irritation AEs for any of the treatments. All subjects’ vital signs were within normal range or considered not clinically significant by the investigator. All subjects were in normal health status at baseline, and all were found to be in normal health status at post-study examination.
Discussion
Adhesion is a critical attribute of a topical delivery system (TDS) regardless of whether it is a prescription or OTC product,23,28,29 and is especially the case for drug-in-adhesive (DIA) systems such as the Reference (lidocaine topical system 1.8%) and OTC Test Products (lidocaine patches 4% (Test 1 and 2) and lidocaine + menthol patch 1%/4% (Test 3)) where the drug is in and delivered from the adhesive itself and lack of contact between the product and skin compromises proper delivery of drug to the skin to allow palliation of the indicated pain. A TDS product with poor adhesion performance also presents a safety risk as a detached product can be ingested by small children and pets, and a lifting patch can allow the transfer of drugs to clothing and bedding.42
The lidocaine topical system 1.8% demonstrated target adhesion performance in previously reported studies21 and replicated these findings here along with the demonstration of superior adhesion to three lidocaine-containing OTC patch products. This performance is attributed to its unique DIA nonaqueous polymer system specifically formulated to maintain tackiness over time optimizing skin contact over the 12-hour administration period. The contrast in performance between lidocaine topical system 1.8% and the comparator OTC Test Products is possibly attributed to the OTC Product not having undergone regulatory review or otherwise required to meet an adhesion performance standard (or other critical product attributes) in order to be on the market.
One (1) subject (4.6%) treated with the lidocaine topical system 1.8% experienced product detachment of 50% or greater compared with OTC Products Test 1 (lidocaine patch 4%) (50%), Test 2 (lidocaine patch 4%) (45.5%), or Test 3 (lidocaine (59.1%). More than one-third of subjects experienced substantial detachment (reduction to <10% adhesion) of the generic lidocaine patch 5%. No lidocaine topical system 1.8% became completely detached, whereas 11, 7, and 6 detachments 50.0%, 31.8%, and 27.3%) were observed for OTC Products Test 1, Test 2, and Test 3, respectively.
The lack of detachments for lidocaine topical system 1.8% is attributed to the product maintaining tackiness over the treatment period. The differences in adhesion performance for the three OTC products relative to lidocaine topical system 1.8% and between each other are inexplicable as the exact composition of the adhesive formulations relative to the active and inactive ingredients is not publicly disclosed. While the OTC products are consistent in having 4% lidocaine (and 1% menthol for Test 3 product), this product strength is strictly a ratio of drug to adhesive and does not indicate the exact amount of drug in the adhesive or the amount of drug delivered by the product.
These differences in adhesion are expected to be clinically important. The data suggest that approximately 30% to 50% of patients using these OTC products might require product replacement due to complete detachment with a greater percentage experiencing overall poor adhesion. The inferior adhesion performance of these OTC products compared to prescription lidocaine topical system 1.8% is problematic in that the individuals may not receive optimum drug delivery for the treatment of their pain resulting in abandonment of otherwise safe topical therapy for oral therapies that have more significant safety risks. This is also problematic for health care providers when attempting to prescribe prescription TDS therapies to patients that have already had a negative experience as consumers of OTC TDS products.
Several study limitations should be mentioned. The products studied here were applied to the upper back, and such placement was selected as a standardized area of administration and convenience for frequent assessments. It is not known whether their adhesive capacity can be extrapolated to other anatomical sites, especially those labeled for the OTC products (eg, lower back, hip, arms, legs, neck, knees and elbows, and shoulders). Subjects were also restricted to performing activities such as strenuous exercise, exposure to water, and excessive heat or sweating that could affect product adhesive properties outside a clinical study setting. These restrictions and other factors, such as climate differences (eg, temperature and humidity), may affect the generalizability of the results. In a separate study, the lidocaine topical system 1.8% withstood conditions of moderate physical exercise (exercise bike) and heat (heating pad) with no meaningful degree of lifting.20 In addition, products were only evaluated during 12-hour daylight periods, but many patients in particular with PHN (labeled indication for lidocaine topical system 1.8%) experience nighttime pain and would be expected to use lidocaine products while sleeping. Likewise, patients may use the OTC products at night to palliate against nighttime pain, allowing for more restful sleep. It is not known how these variables would affect adhesion of the lidocaine topical system 1.8% or the OTC products, nor whether the superior adhesion observed for lidocaine topical system 1.8% relative to the OTC products reported in this study would be maintained. Regardless, the lidocaine topical system 1.8% demonstrated superior adhesion to the comparator products tested.
Conclusions
The lidocaine topical system 1.8% demonstrated superior adhesion performance compared to three lidocaine-containing OTC products. Adhesion superiority was consistently demonstrated versus three comparator OTC products—two lidocaine patches 4% and one lidocaine + menthol patch 4%/1%—over 12 hours of wear, using actual mean percent adhesion scores with conversion to FDA scale scores. No detachments of the lidocaine topical system 1.8% occurred. Complete detachments of the three OTC products were observed for approximately 30 to 50% of the subjects. Application and use of all lidocaine topical products were safe and well tolerated. For patients with pain associated with PHN, these results support the use of the lidocaine topical system 1.8% as an effective and practical treatment that may be preferable to other topical lidocaine options.
Data Sharing Statement
The authors certify that this manuscript reports original clinical trial data. Individual participant data that underlie the results reported in this article after deidentification (text, tables, figures, and appendices) are available, including the study protocol. Data requests should be submitted in the form of a research proposal to [email protected] for up to 36 months after the publication date.
Acknowledgments
The authors thank the clinical investigators and clinical staff at Axis Clinicals, and the volunteers who made these studies possible.
Funding
This study was performed at Axis Clinicals and funded by Scilex Pharmaceuticals Inc.
Disclosure
Dr. Fudin is a speaker for Abbott Laboratories; advisory board, speakers bureau, and consulting for AcelRx Pharmaceuticals, collaborative publications, advisory board, and consulting for BioDelivery Sciences International; consulting to Firstox Laboratories; collaborative non-paid poster presentations for GlaxoSmithKline; Advisory board for Hisamitsu America Inc. and Hikma Pharmaceuticals; speakers’ bureau, advisory boards, and consultant to Salix Pharmaceuticals; lecturer and nonspeakers’ bureau for Torrent Pharmaceuticals; educational studio recording for Collegium Pharmaceutical; owns stocks from Modoscript; meeting registration support (ASHP 2021) for poster presentation for Lilly Pharmaceuticals, and collaborative non-paid publications for Scilex Pharmaceuticals. Mr. Vought is a former employee of and currently is a consultant to Scilex Pharmaceuticals Inc. Dr. Patel was an employee of Scilex Pharmaceuticals Inc. at the time of the study. Dr. Lissin is an employee of Scilex Pharmaceutical Inc. Dr. Maibach reports receiving consultancy fees from Scilex Pharmaceuticals Inc. as a Principal Scientist. The authors report no other conflicts of interest in this work.
References
1. Gudin J, Nalamachu S. Utility of lidocaine as a topical analgesic and improvements in patch delivery systems. Postgrad Med. 2020;132(1):28–36. doi:10.1080/00325481.2019.1702296
2. Bhala N, Emberson J, Merhi A, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomized trials. Lancet. 2013;382(9894):769–779.
3. Lee WM. Public health: acetaminophen (APAP) hepatotoxicity – isn’t it time for APAP to go away? J Hepatol. 2017;67:1324–1331. doi:10.1016/j.jhep.2017.07.005
4. Kumar L, Barker C, Emmanuel A. Opioid-induced constipation: pathophysiology, clinical consequences, and management. Gastroenterol Res Pract. 2014;2014:1–6. doi:10.1155/2014/141737
5. Bawor M, Dennis BB, Samaan MC, et al. Methadone induces testosterone suppression in patients with opioid addiction. Sci Rep. 2014;4:6189. doi:10.1038/srep06189
6. Brennan MJ. The effect of opioid therapy on endocrine function. Am J Med. 2013;126(Suppl 1):S12–S18. doi:10.1016/j.amjmed.2012.12.001
7. Basbaum AI, Bautista DM, Scherrer G, et al. Cellular and molecular mechanisms of pain. Cell. 2009;139(2):267–284. doi:10.1016/j.cell.2009.09.028
8. Institute of Medicine (US) Committee on Pain, Disability, and Chronic Illness Behavior. Pain and disability: clinical, behavioral, and public policy perspectives. Osterweis M, Kleinman A, Mechanic D, editors. The Anatomy and Physiology of Pain. US: National Academies Press; 1987. Available from: https://www.ncbi.nlm.nih.gov/books/.
9. Center for Disease Control. Nonopioid treatments for chronic pain: principles of chronic pain treatment. Available from: https://www.cdc.gov/drugoverdose/pdf/nonopioid_treatments-A.pdf.
10. Scilex Pharmaceuticals Inc. ZTlido® (Lidocaine Topical System) Prescribing Information. San Diego (CA): Scilex Pharmaceuticals Inc; 2018.
11. Fornasari D. Pharmacotherapy for neuropathic pain: a review. Pain Ther. 2017;6(suppl 1):25–33. doi:10.1007/s40122-017-0091-4
12. Leppert W, Malec-Milewska M, Zajaczkowska R, et al. Transdermal and topical drug administration in the treatment of pain. Molecules. 2018;23(3):681. doi:10.3390/molecules23030681
13. Davies PS, Galer BS. Review of lidocaine patch 5% studies in the treatment of postherpetic neuralgia. Drugs. 2004;64(9):937–947. doi:10.2165/00003495-200464090-00002
14. LIDODERM®. Lidocaine patch 5% [prescribing information]. Malvern (PA): Endo Pharmaceuticals Inc.; 2020.
15. US Food and Drug Administration. Drug approval package: lidoderm (lidocaine) patch; 2005. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/99/20612.cfm.
16. ZTLIDO®. lidocaine topical system 1.8% [prescribing information]. San Diego (CA): Scilex Pharmaceuticals Inc.; 2021.
17. US Food and Drug Administration. Drug approval package: ZTlido (lidocaine) topical system; 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/207962Orig1s000TOC.cfm.
18. ZTlido. ZTlido – a new lidocaine patch for postherpetic neuralgia. Med Lett Drugs Ther. 2019;61(1568):41–42.
19. Gudin J, Argoff C, Fudin J, et al. A Randomized, open-label, bioequivalence study of lidocaine topical system 1.8% and lidocaine patch 5% in healthy subjects. J Pain Res. 2020;13:1485–1496. doi:10.2147/JPR.S237934
20. Fudin J, Wegrzyn EL, Greuber E, et al. A randomized, crossover, pharmacokinetic and adhesion performance study of a lidocaine topical system 1.8% during physical activity and heat treatment in healthy subjects. J Pain Res. 2020;13:1359–1367. doi:10.2147/JPR.S238268
21. Gudin J, Webster LR, Greuber E, et al. Open-label adhesion performance studies of a new lidocaine topical system 1.8% versus lidocaine patches 5% and lidocaine medicated plaster 5% in healthy subjects. J Pain Res. 2021;14:513–526. doi:10.2147/JPR.S287153
22. Vought K, Greuber E, Patel K, et al. A randomized, crossover, adhesion performance and pharmacokinetic study of a lidocaine topical system under conditions of water exposure in healthy subjects. J Pain Res. 2021;14:2459–2467. doi:10.2147/JPR.S323789
23. US Food and Drug Administration. Draft guidance for industry: transdermal and topical delivery systems – product development and quality considerations; 2019.
24. US Food and Drug Administration. Draft guidance for industry: assessment of adhesion for topical and transdermal systems submitted in new drug applications; 2021.
25. US Food and Drug Administration. Draft guidance for industry: assessing adhesion with transdermal and topical delivery systems for ANDAs; 2018.
26. US Food and Drug Administration. Guidance for industry: assessing the irritation and sensitization potential of transdermal and topical delivery systems for ANDAs; 2018.
27. US Food and Drug Administration. Guidance for industry: residual drug in transdermal and related drug delivery systems; 2011.
28. Wokovich AM, Prodduturi S, Doub WH, et al. Transdermal drug delivery system (TDDS) adhesion as a critical safety, efficacy and quality attribute. Eur J Pharm Biopharm. 2006;64(1):1–8. doi:10.1016/j.ejpb.2006.03.009
29. Cilurzo F, Gennari CG, Minghetti P. Adhesive properties: a critical issue in transdermal patch development. Expert Opin Drug Deliv. 2012;9:33–45. doi:10.1517/17425247.2012.637107
30. Nalamachu S, Gudin J. Characteristics of analgesic patch formulations. J Pain Res. 2020;13:2343–2354. doi:10.2147/JPR.S270169
31. US Food and Drug Administration. FDA Adverse Events Reporting System (FAERS) public dashboard. Data between November 2018 and October 2021; 2021.
32. Lisi DM. OTC Transdermal analgesic patches in pain management. US Pharm. 2019;44:15–21.
33. Wick JY. Topical analgesics provide pain relief. Pharm Times. 2019;85:9.
34. Pergolizzi JV, Raffa RB, Taylor R, et al. Pain specialists awareness of topical analgesics and their use in pain control: survey results. J Anesth Surg. 2016;3(1):114–118.
35. Terrie YC. OTC transdermal analgesic patches can relieve pain. Pharm Times. 2019;85:9.
36. US Food and Drug Administration. External analgesic drug products for over-The-counter human use; Tentative final monograph. Fed Regist. 1983;48(27):5852.
37. US Food and Drug Administration. External analgesic drug products for over-the-counter human use; reopening of the administrative record and amendment of tentative final monograph. Fed Regist. 2003;68:42324.
38. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
39. FDA Guidance for Industry: ICH E6(R2) Good Clinical Practices: Integrated Addendum to ICH E6(R1), March 2018. Available from: https://www.fda.gov/files/drugs/published/E6%28R2%29-Good-Clinical-Practice--Integrated-Addendum-to-ICH-E6%28R1%29.pdf. Accessed July 19, 2022.
40. Kolansinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
41. Drugs@FDA. Salonpas (Menthol; Methyl Salicylate); NDA 022029; patch; topical. Hisamitsu Pharm Co.
42. Salocks CB, Hui X, Lamel S, et al. Dermal exposure to methamphetamine hydrochloride contaminated residential surfaces II. Skin surface contact and dermal transfer relationship. Food Chem Toxicol. 2014;66:1–6. doi:10.1016/j.fct.2013.12.044
43. Bista SR, Hardy J, Tapuni A, et al. Validation of a fentanyl transdermal adhesion scoring tool for use in clinical practice. J Pain Symptom Manage. 2015;49(5):934–938. doi:10.1016/j.jpainsymman.2014.09.017
44. Moore R, Chi C, Wiffen PJ, Derry S, Rice ASC, Oral nonsteroidal anti-inflammatory drugs for neuropathic pain. Cochrane Database Syst Rev. 2015;10:CD010902. doi:10.1002/14651858.CD010902.pub2
45. Wiffen PJ, Knaggs R, Derry S, Cole P, Phillips T, Moore RA. Paracetamol (Acetaminophen) with or without codeine or dihydrocodeine for neuropathic pain in adults (Review). Cochrane Database Syst Rev. 2016;2016(12):CD012227.
46. McNicol ED, Midbari A, Eisenberg E, Opioids for neuropathic pain. Cochrane Database Syst Rev. 2013;8:CD006146. doi:10.1002/14651858.CD006146.pub2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.