")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
One-Year Evolution of Symptoms and Health Status of the COPD Multi-Dimensional Phenotypes: Results from the Follow-Up of the STORICO Observational Study
Authors Incalzi RA, Blasi F , Scichilone N , Zullo A, Simoni L, Canonica GW
Received 1 December 2020
Accepted for publication 22 March 2021
Published 20 April 2021 Volume 2021:16 Pages 1007—1020
DOI https://doi.org/10.2147/COPD.S289697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Raffaele Antonelli Incalzi,1 Francesco Blasi,2,3 Nicola Scichilone,4 Alessandro Zullo,5 Lucia Simoni,5 Giorgio Walter Canonica6 On Behalf of STORICO study group
1Internal Medicine and Geriatrics Department Biomedical Campus University of Rome, Rome, Italy; 2Internal Medicine Department, Respiratory Unit and Cystic Fibrosis Adult Center, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; 3Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy; 4DIBIMIS, University of Palermo, Palermo, Italy; 5Medineos Observational Research, Modena, Italy; 6Personalized Medicine Asthma & Allergy Clinic, Humanitas University, Humanitas & Research Hospital-IRCCS, Rozzano (Milan), Italy
Correspondence: Raffaele Antonelli Incalzi
Biomedical Campus, University of Rome, Via Alvaro Del Portillo, 21, Rome, 00128, Italy
Tel +39 06 22541 1365
Fax +39 06 22541 456
Email [email protected]
Aim: Describing the 1-year evolution of symptoms and health status in COPD patients enrolled in the STORICO study (observational study on characterization of 24-h symptoms in patients with COPD) classified in multidimensional phenotypes (m-phenotypes).
Methods: In our previous study, we performed an exploratory factor analysis to identify clinical and pathophysiological variables having the greatest classificatory properties, followed by a cluster analysis to group patients into m-phenotypes (mild COPD (MC), mild emphysematous (ME), severe bronchitic (SB), severe emphysematous (SE), and severe mixed COPD (SMC)). COPD symptoms were recorded at baseline, 6-, and 12-month follow-up and their evolution was described as frequency of patients with always present, always absent, arising’, ‘no more present symptoms. QoL and quality of sleep were evaluated using the SGRQ and CASIS questionnaires, respectively.
Results: We analyzed 379 subjects (144 MC, 71 ME, 96 SB, 14 SE, 54 SMC). M-phenotypes were stable over time in terms of presence of symptoms and health status with selected differences in evolution of symptoms in mild vs severe m-phenotypes. Indeed, 28.1% SB, 50.0% SE and 24.1% SMC vs 0.7% MC and 5.6% ME with night-time symptoms at baseline had no more symptoms at 6-month (p-value night-time symptom evolution MC vs SB, SE, SMC and ME vs SB, SE, SMC < 0.0001). All m-phenotypes improved in quality of sleep, more markedly the severe than the mild ones (p-values CASIS score change between baseline and 6- or 12-month in MC, ME vs SB, SE, SMC < 0.0001). QoL did not change during observation, irrespectively of m-phenotype.
Conclusion: Over 1 year, severe m-phenotypes showed an improvement in night-time symptoms and quality of sleep, but not QoL. Being stable over time, m-phenotypes seem worthy of testing for classificatory and prognostic purposes.
Keywords: phenotype, evolution, quality of sleep, quality of life, real world, cohort study
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is an umbrella definition encompassing a variety of clinical conditions with different pathology and pathophysiological bases.1 Thus, many attempts have been made and are ongoing to sort out phenotypes, or at least treatable traits, in order to tailor the therapy to the true needs of the patients.2–6
Such an objective has been originally pursued by identifying clinical phenotypes (mainly bronchitic, emphysematous, asthma-like, frequent exacerbator).7,8 Increasing awareness of clinical variability within individual clinical phenotypes and of the role of comorbid diseases in conditioning the health status have prompted alternative, more complex classificatory strategies variably including biological markers. This marks the passage from the phenotype to the endotype.9 Complex analytical procedures, such as network analysis and machine learning, have been used to improve classification.10–13 However, these classifications, by focusing on systemic features of COPD and comorbid diseases, carry some risk of neglecting core respiratory symptoms. Indeed, dyspnea, cough and phlegm remain the triad characterizing the COPD patient, even if other symptoms, like fatigue and depressed mood, are highly prevalent and disabling.14
At variance with the numerous comprehensive “systemic” classifications of COPD recently proposed, the STORICO study (STudio Osservazionale sulla caratteRizzazione dei sIntomi delle 24 ore nei pazienti con broncopneumopatia cronica ostruttiva, observational study on characterization of 24-h symptoms in patients with COPD) attempts to overcome the recognized weakness of the traditional clinical classification by deepening the clinical assessment rather than making it an almost marginal component of a multidimensional assessment. The well-recognized classificatory properties of symptoms, if properly assessed, ie, if collected in their circadian sequence, constitute the foundations of the philosophy of the STORICO study.15 Furthermore, assessing the circadian rhythm of symptoms allows an evaluation of the classificatory properties of nocturnal symptoms. Commonly neglected in the clinical assessment of COPD patients, night-time symptoms are worthy of attention as they have many determinants, they significantly impact the health status and have potential prognostic implications.16 Indeed, the baseline assessment of a real-life COPD population enabled us to identify 5 cluster of patients (named multidimensional phenotypes, hereinafter named m-phenotypes) with distinctive clinical profiles built up by the analysis of the circadian rhythm of symptoms and the quality of life rated by the Saint George Respiratory Questionnaire (SGRQ). These clusters were characterized by quantitatively and qualitatively different burdens of disease, which might pave the way to tailored therapies as well as to goal-directed treatment.
The present analysis aimed to describe the 1-year clinical evolution (in terms of circadian rhythm of symptoms, occurrence of exacerbations, and lung function) and health status (in terms of quality of life, quality of sleep, and level of anxiety and depression) in COPD patients classified according to m-phenotypes.
Methods
Study Design and Population
STORICO (study registration number: NCT03105999) is an Italian, multicenter, observational study conducted in 40 pulmonology centers. Patients were consecutively recruited from February 2016 to April 2017 and follow-up visits were scheduled after 6 and 12 months from baseline. Last patient last visit occurred in June 2018. The study was approved by the Ethic Committee of the coordinating center (Fondazione Toscana G. Monasterio Pisa, Italy) and was conducted in accordance with the Declaration of Helsinki and the Good Clinical Practices guidelines for observational studies, in compliance with all the requirements of Italian regulations. Patients provided written, informed consent before study participation.
Subjects enrolled were aged ≥50, current or ex-smokers with smoking history ≥10 pack-years, with a diagnosis of COPD, free from exacerbations (defined according to GOLD 201417 guidelines) at enrolment visit and in the month before.
For the present analysis, we considered patients who completed baseline and follow-up visits within 6 (±2) and 12 (±3) months, respectively, and with available information on the frequency of COPD symptoms during each part of the 24-h day at baseline and both follow-up visits. The methodology of the STORICO study has been fully described elsewhere.15
Patients were classified at enrollment into five m-phenotypes, through a series of steps that have been extensively described in our previous paper.17
These steps can be briefly summarized here as follows: (i) An exploratory factor analysis (EFA) was performed to find independent latent constructs (factors), not directly measurable and influencing responses on observed variables. EFA is a variable reduction technique which does not impose any preconceived structure on the outcome and the observed variables included in the model are a linear combination of the underlying factors. The following items from the symptoms questionnaire were included in the factor analysis: presence/absence of shortness of breath or breathlessness, cough, bringing up phlegm or mucus, each symptom evaluated during the 24 hours (ie, in the early-morning, day-time and night-time). The value of the FEV1% predicted, (symptoms, activity, impact) SGRQ scores, demographic variables (age and gender), and presence/absence of relevant comorbidities (cardiac ischemic disease, arterial hypertension, heart failure, atrial fibrillation, diabetes, osteoporosis, depression, kidney insufficiency) were also included in the model. Orthogonal VARIMAX rotation was applied; factors having an eigenvalue >1.0 and individual variables with higher-than-0.5 loadings on retained factors were retained. EFA identified 2 factors and, with them, the clinical and pathophysiological variables having the greatest classificatory properties (ie, the circadian rhythm of symptoms (dyspnea, bringing up phlegm or mucus and cough) and quality of life (as assessed by the SGRQ)). (ii) Then, the variables included in the two factors were evaluated and, whenever possible, combined into a new classificatory variable (a classificatory variable for each factor was defined). (iii) A cluster analysis with classificatory variables mentioned at step (ii) as input was performed, and patients were thus grouped into m-phenotypes. Average linkage was chosen as clustering method and average distance between clusters equal to 0.70 was taken as reference to cut the dendrogram.
These m-phenotypes were denominated according to the dominant clinical trait as “emphysematous” or “bronchitic” depending upon whether dyspnea or productive cough (bringing up phlegm or mucus) was the dominant symptom, and “mixed”, in case both “emphysematous” and “bronchitic” traits were present.
The m-phenotypes were, therefore, the following: mild COPD (MC), characterized by absence of night-time symptoms without a prevalent bronchitic or emphysematous trait, mild emphysematous (ME), with prevalent dyspnea in the early-morning and day-time, but not by night, severe bronchitic (SB), with nocturnal and diurnal cough and phlegm, but no nocturnal dyspnea, severe emphysematous (SE), presenting nocturnal and diurnal dyspnea and severe mixed COPD (SMC), reporting the higher frequency of symptoms during 24h.
Clinical Assessment
At baseline, socio-demographic characteristics and clinical history were recorded.
At study visits, spirometry was performed according to the recommendations of the American Thoracic Society and of the European Respiratory Society: forced expiratory volume in the first second (FEV1) and Forced Vital Capacity (FVC) were collected, and, where available, Residual Volume (RV), Total Lung Capacity (TLC), and diffusion capacity for carbon monoxide (DLCO) were also recorded.
An exacerbation was defined as an acute event characterized by a worsening of the patient’s respiratory symptoms beyond day-to-day variations which led to a change in medication during follow-up. At enrolment visit, anamnestic data about number of COPD exacerbations/year in the 5 years before enrolment were collected by the clinical investigator. The occurrence and severity of exacerbations during the study were assessed as well.
Outcome Measures
The frequency of COPD symptoms (breathlessness, coughing, bringing up phlegm or mucus, chest tightness, chest congestion, and wheezing) during each part of the day (early-morning, day-time, and night-time) was assessed at study visits by means of the Night-time, Morning, and Day-time Symptoms of COPD questionnaire.18 The level of perceived breathlessness and the extent to which it affected mobility were assessed using the modified Medical Research Council (mMRC) dyspnea scale ranging from 0 (breathless with strenuous exercise) to 4 (too breathless to leave the house/breathless when dressing or undressing).19 Presence of dyspnea was defined as a mMRC scale score ≥2.
QoL was evaluated using the SGRQ, including the subject’s perception of recent respiratory problems (Symptoms component), disturbances to daily physical activity (Activity component), and disturbances of psycho-social function (Impact component); total score was also calculated. Scores range between 0 (no impairment) and 100 (highest impairment).20,21
Anxiety and depression states were investigated through the Hospital Anxiety and Depression Scale (HADS),22 with a total score (emotional distress) ranging between 0 and 42; anxiety and depression subscale scores (ranging 0–21) were also computed, with higher scores indicating more distress.
The impact of respiratory symptoms on sleep was assessed with the COPD and Asthma Sleep Impact Scale (CASIS),23 a self-administered, 7-item scale evaluating sleep impairment associated with COPD and asthma. The total score ranges 0–100 (higher scores indicating greater sleep deterioration). Permissions have been obtained from authors for the use of the questionnaires/scales.
Data Quality Assurance
The data entered into the electronic case report forms (eCRFs) by investigational staff were reviewed for completeness and accuracy and site personnel was instructed to enter data into the eCRFs and make any required corrections or additions during the phone training.
The scales and questionnaires were filled out by patients and the data were entered into the eCRFs by qualified personnel. The eCRF was provided with online edit checks. Two cleaning waves were performed by running post-entry checks by means of validation programs and data listings specific for the study. During this process, if clarifications were needed, queries were raised through the eCRF. Designated investigator site personnel was required to respond to the query and make the correction to the database.
Statistical Analysis
Our analysis was descriptive and no formal statistical hypotheses were set. The continuous, normally distributed variables were expressed as a mean ± standard deviation (SD) or median and interquartile range (IQR) in case of not normally distributed parameters, while absolute and relative frequencies were provided for qualitative data. Missing values were not replaced and did not contribute to the analysis of the variable.
According to the Night-time, Morning, and Day-time Symptoms of COPD questionnaire, presence of COPD symptoms in the early-morning (or in the night-time or day-time) was defined as occurrence of at least one symptom (among breathlessness, coughing, bringing up phlegm or mucus, chest tightness, chest congestion, and wheezing) in the early-morning (or in the night-time or day-time) during the week before visit, irrespective of severity and frequency.
The evolution of (night-time, early-morning, and day-time) COPD symptoms during follow-up was described in terms of frequency of patients with symptoms: (i) “always present”, ie, present at two subsequent visits (baseline and 6-month follow-up or 6- and 12-month follow-up), (ii) “always absent”, ie, absent at two subsequent visits (baseline and 6-month follow up or 6- and 12-month follow up), (iii) “arising”, ie, present at one follow up visit but not at the previous (baseline or 6-month follow-up) visit, and (iv) “no more present”, ie, not present at the follow-up visit but present at the previous (baseline or 6-month follow-up) visit.
For descriptive purposes, and for a better contextualization of results, changes of therapies for COPD during study were also evaluated; a therapy was considered changed if interrupted, in case of dosage increase/decrease, or if the patient started a new therapy.
Comparisons between patients included vs not included in the analyses were performed by means of t-test or non-parametric Wilcoxon rank sums test for numerical variables and Chi-square test in case of categorical variables. Analysis of variance (for normally distributed variables) and Kruskal–Wallis test by ranks (for non-normally distributed variables) on means and medians, respectively, and Chi-square or Fisher exact test (for categorical variables) were used to compare variables vs m-phenotype (variable in 5 classes). Then, depending on the statistical significance of these tests, Mann–Whitney test on medians (for non-normally distributed variables), t-test (for normally distributed variables), and Chi-square or Fisher exact tests (for categorical variables) were applied to compare variables among specific pairs of m-phenotypes. Alpha with Bonferroni correction was set to 0.0001 considering the total number of performed tests.
Correlation between not normally distributed variables was assessed using the Spearman’s rank correlation coefficient.
Site monitoring, data management, and statistical analysis were performed by MediNeos (Modena, Italy). Statistical analysis was performed using SAS v9.4 and Enterprise Guide v7.1.
Results
Subjects’ Characteristics
Among the 683 COPD-diagnosed patients enrolled in the STORICO study, 77 were excluded because they did not satisfy inclusion/exclusion criteria of the study and another 92 subjects were excluded because of missing information on variables analyzed in the factor and cluster analyses used to identify m-phenotypes; thus, 514 patients were classified at baseline visit into the five m-phenotypes: MC, ME, SB, SE and SMC.
One-year follow-up data were available for 379 (73.8%) subjects (144 MC, 71 ME, 96 SB, 14 SE, 54 SMC) included in the present analysis, whereas 135 patients were not considered evaluable for the analyses, for the reasons detailed in Figure 1.
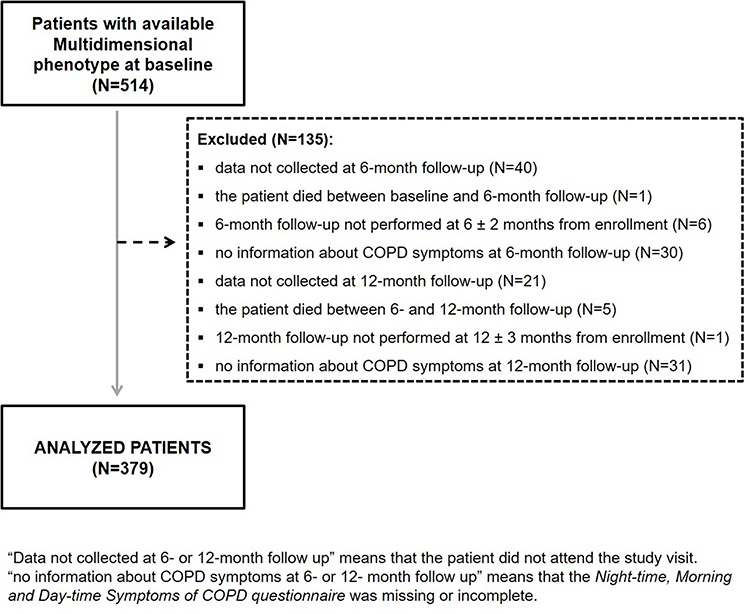 |
Figure 1 Disposition of patients. |
Patients evaluable for the analyses did not differ at baseline in gender, age, number of COPD exacerbations/year in the 5 years before baseline, FEV1 and DLCO % predicted, RV, TLC, SGRQ scores compared to not evaluable patients (see Supplementary Table 1). Baseline characteristics of analyzed patients are shown in Table 1. The distribution of patients according to ongoing therapies for COPD during the study is shown in Table 2. Overall, therapies for COPD were stable during the study with no significant changes between m-phenotypes (Chi-square test p-value presence/absence of changes vs m-phenotype>0.05). Changes of therapies during the study occurred, in fact, in 9 (6.3%) MC, 5 (7.0%) ME, 8 (14.8%) SMC, 11 (11.5%) SB, and 2 (14.2%) SE patients.
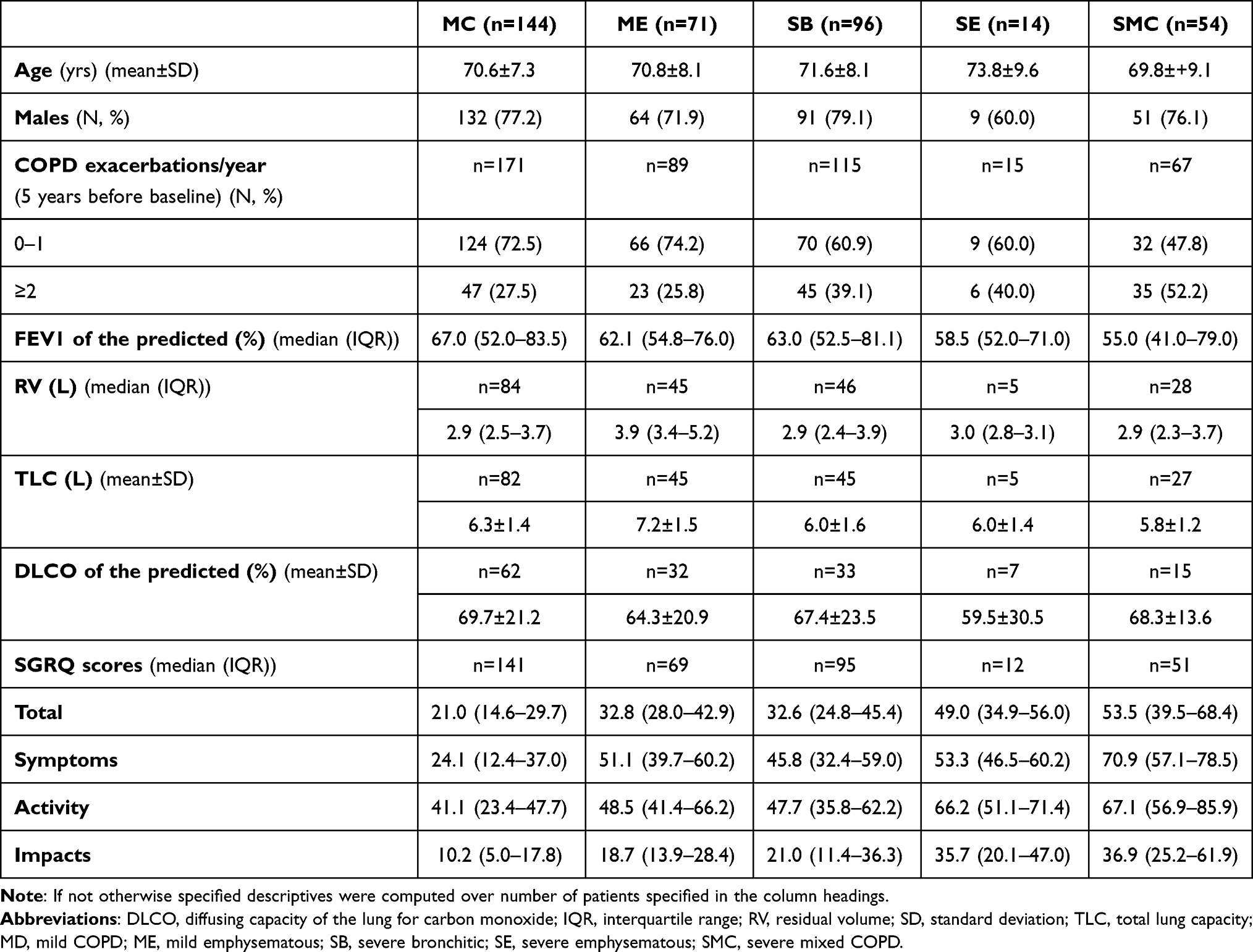 |
Table 1 Baseline Characteristics of Analyzed Patients |
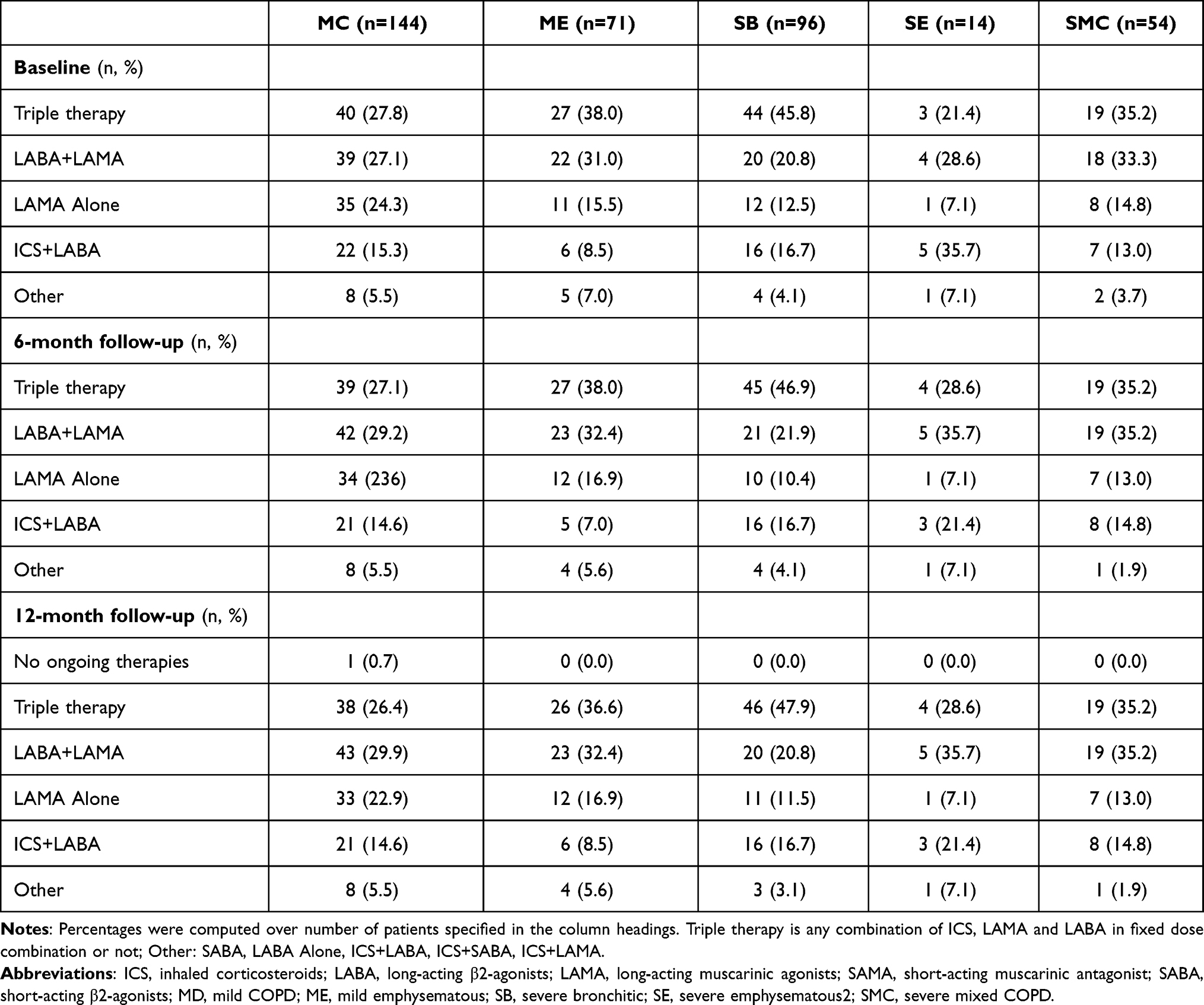 |
Table 2 Therapies for COPD Ongoing at Study Visits (by Multidimensional Phenotype) |
Circadian Rhythm of Symptoms
The proportion of patients with at least one night-time, early-morning, and day-time symptom (in the week before visit) at study visits in the different m-phenotypes is reported in Figure 2A–C.
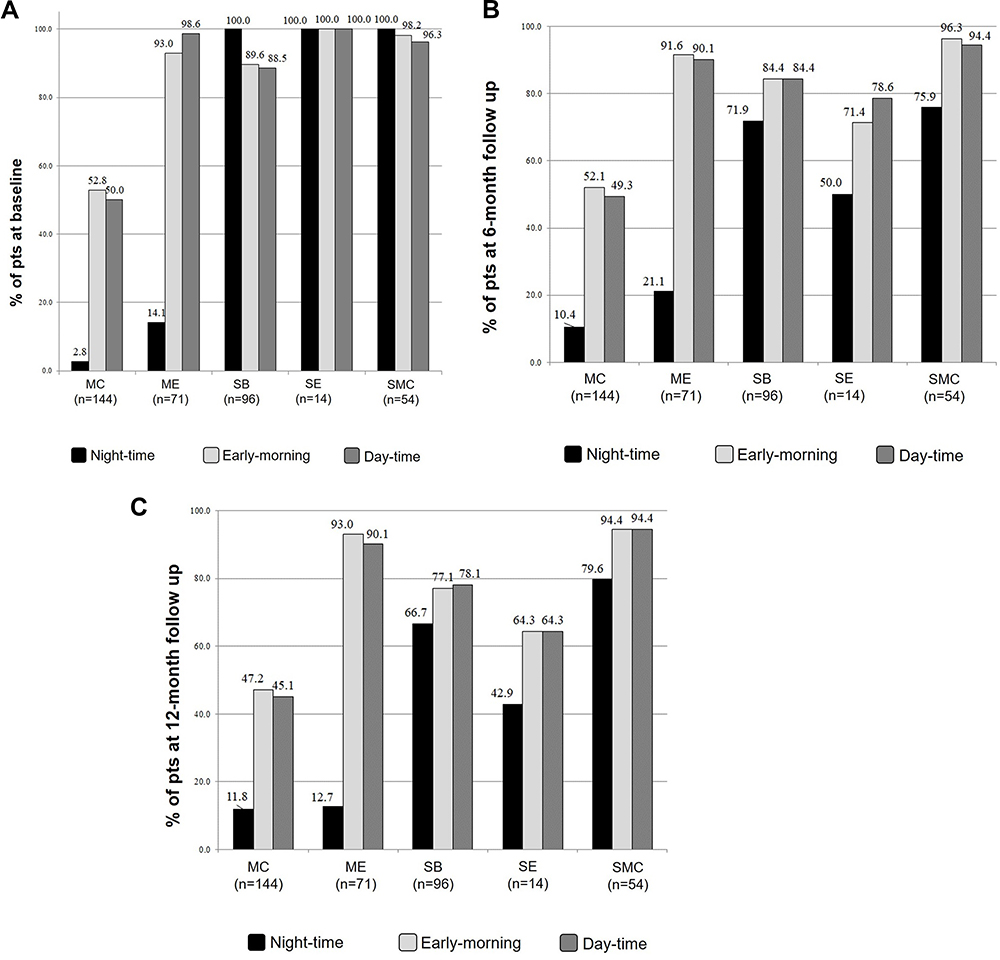 |
Figure 2 (A) Frequency of patients with COPD symptoms by multidimensional phenotype at baseline. (B) Frequency of patients with COPD symptoms by multidimensional phenotype at 6-month follow-up. (C) Frequency of patients with COPD symptoms by multidimensional phenotype at 12-month follow-up. |
Night-time symptoms were more prevalent in SB, SE, and SMC vs MC and ME m-phenotypes both at baseline (Chi-square test p-value frequency of symptoms at baseline vs m-phenotype <0.0001) and at follow-up visits (Chi-square test p-value frequency of symptoms at 6-, and 12-month follow-up vs m-phenotype <0.0001), showing a stability of m-phenotypes in their dominant clinical traits.
Symptom prevalence significantly decreased during follow-up in all m-phenotypes (Chi-square test p-values frequency of COPD symptoms at study visits vs m-phenotype <0.0001), in particular in the severe m-phenotypes and more evidently for the night-time symptoms (Figure 2A–C). During follow-up, 28.1% SB, 50.0% SE, and 24.1% SMC patients with night-time symptoms at baseline had no more symptoms at 6-month follow-up vs 0.7% MC and 5.6% ME patients; 8.3% MC and 12.7% ME patients without night-time symptoms at baseline reported them at 6-month follow up visit vs 0.0% in SB, SE, SMC (p-values night-time symptom evolution (baseline➔6-month follow-up) MC vs SB, SE, SMC and ME vs SB, SE, SMC <0.0001) (Table 3).
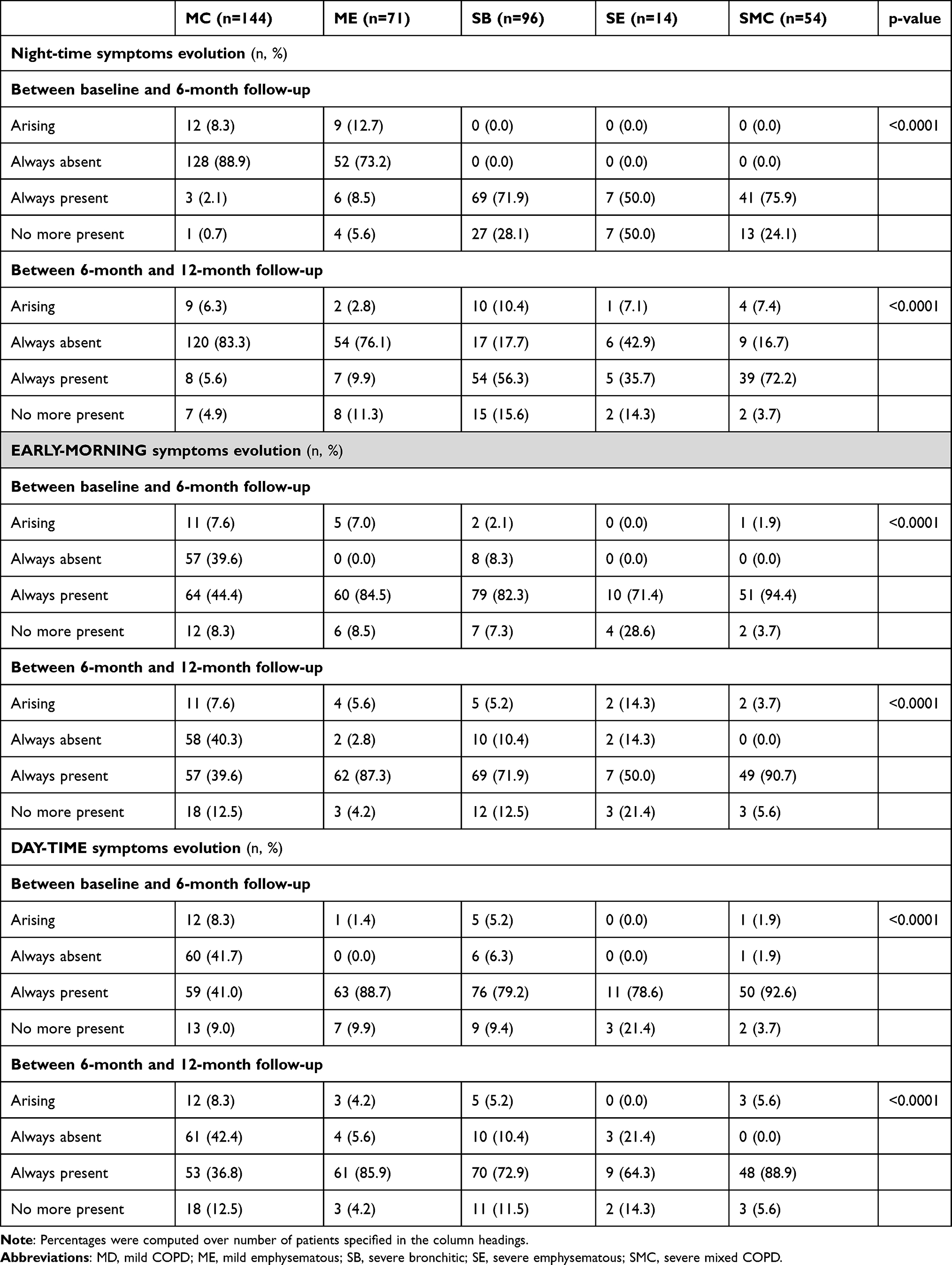 |
Table 3 1-Year Evolution of COPD Symptoms (by Multidimensional Phenotype) |
The proportion of patients with night-time symptoms present at 6-month follow-up and no more symptoms at 12-month follow-up was 15.6%, 14.3%, 3.7% in SB, SE, and SMC patients, respectively, compared to 4.9% and 11.3% in MC and ME patients, respectively. Moreover, 10.4%, 7.1%, 7.4% SB, SE, and SMC patients without night-time symptoms at 6-month follow-up had new symptoms at 12-month follow-up vs 6.3%, 2.8% in MC and ME (p-values night-time symptom evolution (6-month follow-up➔12-month follow-up) MC vs SB, SE, SMC and ME vs SB, SE, SMC <0.0001).
The highest prevalence of patients free from early-morning and day-time symptoms (ie, always absent) was observed in MC compared to other m-phenotypes both at 6 and at 12 months (Table 3).
COPD Exacerbations and Lung Function
At enrollment, the median (IQR) number of COPD exacerbations/year (in the 5 years before baseline) ranged between 1.0 (0.0–3.0) in MC and 3.0 (1.0–5.0) in SMC patients. The 1-year incidence of exacerbations did not distinguish m-phenotypes: 29 (20.1%) MC, 22 (31.0%) ME, 24 (25.0%) SB, 4 (28.6%) SE and 18 (33.3%) SMC had at least one exacerbation (Chi-square test p-value frequency of patients with exacerbations vs m-phenotype >0.05).
At baseline, the only significant difference in lung function parameters emerged in RV of MC vs ME patients (median (IQR): 2.9 (2.5–3.7) L vs 3.9 (3.4–5.2) L; Mann–Whitney test p-value (MC vs ME)<0.0001) (see Supplementary Table 2). Between baseline and 6-month follow-up, TLC decreased more in ME patients (median (IQR): −1.4 (−2.3–0.2) L) than in SB (median (IQR): 0.1 (−0.2–0.8) L; Mann–Whitney test p-value (ME vs SB)<0.0001). The frequency of patients with dyspnea at different time points is reported in Supplementary Table 2; it appears to be stable during time within m-phenotypes. The level of dyspnea is significantly lower at study visits in MC compared to other m-phenotypes (Chi-square test p-value presence of dyspnea in MC vs other m-phenotypes <0.0001).
Quality of Life and Sleep, Anxiety/Depression
The quality of life did not change during 12 months of observation, irrespective of m-phenotype. It was always better in MC (Mann–Whitney test p-values (MC vs ME, SB, SE, SMC) <0.0001 for SGRQ symptoms, activity, impacts and total scores at baseline, 6-month and 12-month follow-up). Quality of life was worse in SMC (Mann–Whitney test p-value (SMC vs ME and SB) <0.0001 for symptoms, activity, impacts and total scores at baseline, 6-month and 12-month follow-up) (see Supplementary Table 3).
At all visits, MC had better quality of sleep than the other m-phenotypes (Mann–Whitney test p-values CASIS total score in MC vs other m-phenotypes <0.0001), while SMC had a worse quality of sleep compared to ME and SB patients (Mann–Whitney test p-value CASIS total score SMC vs ME and SB <0.0001) (see Supplementary Table 3). Between baseline and follow-up visits, all m-phenotypes showed improved quality of sleep, more markedly in severe (SB, SE, SMC) compared to mild (MC, ME) phenotypes (Mann–Whitney test p-values change of CASIS total score between baseline and 6- or 12-month follow-up in MC, ME vs SB, SE, SMC <0.0001).
Perceived quality of life did not improve with improving quality of sleep (Spearman correlation coefficients of change baseline-6-month follow-up and baseline-12-month follow-up of CASIS total score vs SGRS activity, impacts, symptoms, total scores <0.3).
At all study visits, levels of anxiety and depression were low (see Supplementary Table 3). SMC had higher levels of anxiety and depression than MC and SB (Mann–Whitney test p-values HADS scores at all study visits in SMC vs MC, SB <0.0001). Significant differences between ME and MC also emerged during the study in favor of MC (Mann-Whitney test p-values HADS scores at all study visits in ME vs MC <0.0001). HADS scores appeared stable over time in all m-phenotypes.
Discussion
We found that m-phenotypes are characterized by stable distinctive clinical (ie, presence of symptoms) and health status (ie, quality of life, quality of sleep, level of anxiety and depression) features. Night-time symptoms were more prevalent in SB, SE and SMC vs MC and ME m-phenotypes both at baseline and at follow-up visits and SMC constantly had higher levels of anxiety and depression than MC and SB. Thus, contrasting anxiety and depression seems an objective worthy of consideration in SMC m-phenotype. Analogously, showing that SMC constantly had the worst perceived health status might drive dedicated interventions. Indeed, classifying COPD patients according to the m-phenotype would enable physicians to measure the effects of a given intervention on the main m-phenotype specific problems of the individual patient.
The current longitudinal analysis also showed that severe m-phenotypes had greater improvement in nocturnal symptoms as opposed to mild m-phenotypes. Moreover, quality of sleep improved across all m-phenotypes, more markedly in severe than mild ones. On the other hand, the prevalence of early-morning and day-time symptoms remained high, with the majority of study participants (78.1% of SB, 64.3% of SE, and 94.4% of SMC) still suffering from day-time symptoms one year after enrolment. The lack of improvement in dyspnea and quality of life testifies to this unfavorable trend. Thus, the improvements in nocturnal symptoms and quality of sleep did not translate into better health-related quality of life.
Once a forgotten dimension of COPD, nocturnal symptoms have become a specific target of pharmacological treatment. In a real-world treatment setting,24 sleep disturbances were common and, if left unmanaged, encroached on daytime activities, worsening health status. Indeed, night-time symptoms have been proved to be the main correlate of depressed mood in the Assess study.18 Furthermore, in a mixed Asthma-COPD population aged over 65 years, their prevalence increases with age.25 Of note, in the CanCOLD study26 impaired sleep quality was associated with increased rate of exacerbations over a period of 18 months. Finally, sleep disturbances have recently been proved to correlate with respiratory symptoms, poor lung function, exacerbations during the previous year, and depression in a large COPD cohort.
We assessed the evolution of respiratory symptoms in COPD patients in real-life, ie, in the absence of planned interventions. This condition may be, to some extent, compared to the placebo arm of RCTs, with regard to indexes exploring health status, dyspnea, and respiratory function tests; however, the evolution of the circadian rhythm of symptoms has never been assessed so far. In the placebo group of the two largest trials on the pharmacological treatment of COPD, namely the UPLIFT and TORCH studies, neither health status nor lung function showed clinically significant changes over a 4- and 3-year interval, respectively.26–28 Similar findings were documented for perceived dyspnea in the pooled Flight 1 and Flight 2 trials after one year of observation.29 Finally, in a real-world population of COPD patients in conditions of usual care (the SALFORD study), overall dyspnea did not change significantly as it improved in 26.8% of patients but worsened in 20.9% over 12 months.30 Thus, our findings about the evolution of respiratory symptoms are in line with comparable observations centered on overall symptoms and not on their circadian rhythm.
Surprisingly, in our patients’ quality of life did not improve with improving quality of sleep. This likely reflects the dominating role of activities in the SGRQ; indeed, this scale largely relies upon the physical dimension –ie, basic and instrumental activities of daily living– which mainly depends upon diurnal rather than nocturnal symptoms, and no question explores quality of sleep or sleep-related symptoms. This very likely explains our finding, ie, the decoupling between nocturnal symptoms/quality of sleep and health-related quality of life and this decoupling cautions against overestimating the potential effects of improving nocturnal control of airway obstruction.
Alternatively, one might hypothesize that in ours and in previous series, dyspnea –which is strictly related to activity–, is the main determinant of perceived health status. Finally, it cannot be excluded that m-phenotypes also reflect some constitutive affective trait conditioning enteroception and mood.
The reasons accounting for the positive evolution of nocturnal symptoms in a notable fraction of patients, mainly belonging to the severe m-phenotypes, are unclear. Indeed, pharmacological therapy changed marginally during follow-up with no relevant differences between m-phenotypes. Average change of SGRQ scores between study visits was negligible due to diverging and reciprocally compensating changes within a class. Some “research effect”, ie, a greater attention to optimize the care of enrollees, cannot be excluded. Furthermore, we lacked information on non-pharmacological therapies such as rehabilitation, which might have contributed to modify the symptoms. Nevertheless, day-time symptoms showed a less positive trend as if effort-related symptoms were less modifiable than sleep-related ones. Indeed, nocturnal symptoms variously reflect changes in bronchial tone, defective clearance of mucus and late onset symptoms, waning pharmacological effects, all of which are modifiable through a tailored approach in terms of timing and choice of therapy. Day-time symptoms, instead, are primarily related to effort-related ventilatory demand. Fulfilling such a demand requires efficient gas exchanges and bronchial patency, which may partly benefit from improved pharmacological therapy, but also preserved muscle mass and strength, and adaptative mechanisms of the breathing pattern to the physical effort. These latter determinants of the response to exercise are less likely to improve in response to pharmacological measures. Furthermore, selected comorbidities like anemia or renal failure might contribute to blunt the response to exercise. These mechanisms might underlie the decoupling in the evolutions of nocturnal and day-time symptoms in our patients. Finally, this decoupling seems to exclude that improvement of nocturnal symptoms in the most diseased patients reflects regression to the mean.
Exacerbations were distinctly rare in our populations. Interestingly, the rate of exacerbations in a population-based sample of a longitudinal observational investigation (CanCOLD study) was 0.50 per year,26 in the entire trial population of the SALFORD study, which had selecting criteria comparable to those of the STORICO study, 31% of patients had no COPD exacerbations in the year of follow-up.31 These findings likely reflect a secular trend: in the recent TRIBUTE study, patients with severe to very severe COPD and a reported exacerbation rate of 1.2 per year actually had 0.5 and 0.59 exacerbations over one year while assuming triple or dual bronchodilating therapy.32 Analogously, the rate of exacerbations dramatically declined in patients enrolled and treated with triple or double Trilogy.33 In a large survey of over 99574 COPD patients up to 10 years, the vast majority had no exacerbations in the baseline year and a quarter of the patients remained free from exacerbations over the whole 10-year observation period.34 An improvement of the whole therapeutic approach to COPD is likely to account for this favorable trend.
Our work has some limitations. First, a large fraction of enrolled patients was excluded from the analyses due to missing information. However, followed-up and excluded patients did not differ in baseline characteristics. Second, we collected symptoms throughout the 24 hours, but we had no measure of symptom severity available. Theoretically, an unchanged prevalence of symptoms in a given time frame might correspond to a different intensity of symptoms. However, the fact that both dyspnea (mMRC) and quality of life (SGRQ) did not change over time is consistent with the recorded symptoms being stable in intensity over time. Third, the improvement of night-time symptoms in a substantial fraction of severe m-phenotype patients might, at least to some extent, depend upon the effective treatment of non-respiratory causes of disturbed sleep like urologic and affective problems. Indeed, we could not assess this possibility. Finally, present data are worthy of being confirmed in a testing population. Thus, they should be considered preliminary in nature. However, based on the real life and purely observational dimension of this study, they are very likely to reflect a biologically plausible and clinically convenient clustering of COPD patients.
Conclusions
Over a 1-year period, a considerable decrease of night-time symptoms occurred in severe m-phenotypes confirmed by the evolution of CASIS score, but sleep improvement did not translate in better quality of life and day-time symptoms continued to be highly prevalent at the end of the follow-up.
The m-phenotypes define clusters of patients with stable and distinctive health status profiles and clinical trajectories and, thus, might help tailor therapeutic interventions and measure therapy effects with regard to the specific characteristics of the m-phenotype. Furthermore, according to these preliminary data, the proposed m-phenotype, a symptom- and QoL-based classification of COPD patients, seems worthy of testing also for research purposes. Indeed, designing a multi-outcome trial, ie, one measuring different outcomes for different m-phenotypes, might improve trial design and results by capturing what is of primary interest for the individual patient. Thus, m-phenotypes might become a working tool in the future of precision medicine.
Abbreviations
CASIS, COPD and Asthma Sleep Impact Scale; COPD, chronic obstructive pulmonary disease; DLCO, diffusion capacity for carbon monoxide; FEV1, forced expiratory volume in the first second; HADS, Hospital Anxiety and Depression Scale; ICS, inhaled corticosteroids; IQR, interquartile range; LABA, long-acting β2-agonists; LAMA, long-acting muscarinic agonists; MC, mild COPD; ME, mild emphysematous; mMRC, modified Medical Research Council; RV, residual volume; SB, severe bronchitic; SD, standard deviation; SE, severe emphysematous; SGRQ, St. George’s Respiratory Questionnaire; SMC, severe mixed COPD; TLC, total lung capacity.
Data Sharing Statement
The data supporting the findings of this study are available from Raffaele Antonelli Incalzi, Francesco Blasi, Nicola Scichilone, Alessandro Zullo, Lucia Simoni, Giorgio Walter Canonica and Laboratori Guidotti, Italy but restrictions apply to the availability of these data, which were used under license for the current study, and are therefore not publicly available. There are legal and ethical restrictions since data contain potentially sensitive patient information. Data are however available from ì Raffaele Antonelli Incalzi, Francesco Blasi, Nicola Scichilone, Alessandro Zullo, Lucia Simoni, Giorgio Walter Canonica and Laboratori Guidotti upon reasonable request. Data request may be sent to the first author ([email protected]) and to Stefania Barsanti (Laboratori Guidotti, [email protected]).
Acknowledgments
We are grateful to Sara Rizzoli for her help in analyzing data and drafting the manuscript. We are also grateful to the participating centers, involved in data collection.
Members of the STORICO Study Group – Participating centers.
Pietro Schino (Acquaviva delle Fonti); Giuseppina Cuttitta (Palermo); Maria Pia Foschino (Foggia); Renato Prediletto (Pisa); Carmelindo Mario Enrico Tranfa (Napoli); Maria Cristina Zappa (Roma); Pasquale Patriciello (Pollena Trocchia); Luciana Labate (Bari); Salvatore Mariotta (Roma); Stefano Nava (Bologna); Alessandro Vatrella (Salerno); Michele Mastroberardino (Avellino); Riccardo Sarzani (Ancona); Antonio Iuliano (Milano); Lamberto Maggi (Bergamo); Anna Zedda (Casoria); Alberto Pesci (Monza); Giuseppe Sera (Torino); Antonello Nicolini (Sestri Levante); Salvatore Walter Di Donato (Mondragone); Silvia Forte (Roma); Mario Del Donno (Benevento); Federica Rivolta (Abbiategrasso); Mauro Ferliga (Chiari); Antonio Filippo Raco (Menaggio); Luigi Di Re (Teramo); Gaetano Cabibbo (Modica); Rosario Maselli (Catanzaro); Carlo Gulotta (Orbassano); Stefano Nardini (Vittorio Veneto); Enrico Eugenio Guffanti (Casatenovo); Walter Castellani (Firenze); Luca Triolo (Roma); Giovanni Passalacqua (Messina); Bianca Beghè (Modena); Salvatore Lo Cicero (Milano); Enzo Faccini (Dolo); Elena Atzeni (Nuoro); Roberto Tazza (Terni); Piercarlo Giamesio (Asti).
Author Contributions
All authors made a significant contribution to the work reported, either in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; they have been involved in drafting, revising or critically reviewing the article; they have approved the final version to be published, have chosen the journal to which the article has been submitted and have agreed to be accountable for all aspects of the work.
Funding
The study was supported by a grant from Laboratori Guidotti and Malesci, Italy. The funding sources were not involved in study design, in the collection, analysis and interpretation of data, and in the preparation of the article for publication.
Disclosure
Francesco Blasi reports grants and personal fees from AstraZeneca, grants and personal fees from BAYER, grants and personal fees from CHIESI, personal fees from GSK, personal fees from GUIDOTTI, grants and personal fees from GRIFOLS, grants from INSMED, personal fees from MENARINI, personal fees from NOVARTIS, grants and personal fees from PFIZER, personal fees from TEVA, grants from VERTEX, personal fees from ZAMBON, outside the submitted work. Alessandro Zullo and Lucia Simoni are employees of Medineos Observational Research. The other authors declare that they have no competing interests.
References
1. Lange P, Halpin DM, O’Donnell DE, MacNee W. Diagnosis, assessment, and phenotyping of COPD: beyond FEV1. Int J Chron Obstruct Pulmon Dis. 2016;11 Spec Iss:3–12. doi:10.2147/COPD.S85976
2. Wan ES, Castaldi P, Cho MH, et al. B13 any time at all: disease progression and emerging phenotypes in COPD. Unsupervised clustering methods predict future development COPD among subjects with preserved ratio impaired spirometry (PRISm) in the COPDGene study. Am J Respir Crit Care Med. 2015;191:1.
3. Burgel PR, Paillasseur JL, Caillaud D, et al. Clinical COPD phenotypes: a novel approach using principal component and cluster analyses. Eur Respir J. 2010;36(3):531–539. doi:10.1183/09031936.00175109
4. Burgel PR, Paillasseur JL, Peene B, et al. Two distinct chronic obstructive pulmonary disease (COPD) phenotypes are associated with high risk of mortality. PLoS One. 2012;7(12):e51048. doi:10.1371/journal.pone.0051048
5. Celli BR, Locantore N, Tal-Singer R, et al. Emphysema and extrapulmonary tissue loss in COPD: a multi-organ loss of tissue phenotype. Eur Respir J. 2018;51(2):
6. Agusti A. The disease model: implications for clinical practice. Eur Respir J. 2018;51(4):
7. Miravitlles M, Calle M, Soler-Cataluna JJ. Clinical phenotypes of COPD: identification, definition and implications for guidelines. Arch Bronconeumol. 2012;48(3):86–98. doi:10.1016/j.arbr.2012.01.003
8. Calle Rubio M, Casamor R, Miravitlles M. Identification and distribution of COPD phenotypes in clinical practice according to Spanish COPD guidelines: the FENEPOC study. Int J Chron Obstruct Pulmon Dis. 2017;12:2373–2383. doi:10.2147/COPD.S137872
9. Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015
10. Garcia Aymerich J, Gómez FP, Benet M, et al. Identification and prospective validation of clinically relevant chronic obstructive pulmonary disease (COPD) subtypes. Thorax. 2011;66(5):430–437. doi:10.1136/thx.2010.154484
11. Burgel PR, Paillasseur JL, Roche N. Identification of clinical phenotypes using cluster analyses in COPD patients with multiple comorbidities. Biomed Res Int. 2014;2014:420134. doi:10.1155/2014/420134
12. Esteban C, Arostegui I, Aburto M, et al. Chronic obstructive pulmonary disease subtypes. Transitions over time. PLoS One. 2016;11(9):e0161710. doi:10.1371/journal.pone.0161710
13. Augustin IML, Spruit MA, Houben-Wilke S, et al. The respiratory physiome: clustering based on a comprehensive lung function assessment in patients with COPD. PLoS One. 2018;13(9):e0201593. doi:10.1371/journal.pone.0201593
14. Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345–349. doi:10.1183/09059180.00007813
15. Canonica GW, Blasi F, Scichilone N, et al. Characterization of circadian COPD symptoms by phenotype: methodology of the STORICO observational study. Eur J Intern Med. 2017;43:62–68. doi:10.1016/j.ejim.2017.05.021
16. Agusti A, Hedner J, Marin JM, Barbé F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183–194. doi:10.1183/09059180.00004311
17. Antonelli Incalzi R, Canonica GW, Scichilone N, et al. The COPD multi-dimensional phenotype: a new classification from the STORICO Italian observational study. PLoS One. 2019;14(9):e0221889. doi:10.1371/journal.pone.0221889
18. Miravitlles M, Worth H, Soler Catalauña JJ, et al. Observational study to characterize 24-hour COPD symptoms and their relationship with patient-reported outcomes; results from the ASSESS study. Respir Res. 2014;21(15):122. doi:10.1186/s12931-014-0122-1
19. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
20. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure for chronic airflow limitation. The St George’s respiratory questionnaire. Am Rev Respir Dis. 1992;145(6):1321–1327. doi:10.1164/ajrccm/145.6.1321
21. Meguro M, Barley EA, Spencer S, Jones PW. Development and validation of an improved COPD-specific version of the St George’s respiratory questionnaire. Chest. 2007;132(2):456–463. doi:10.1378/chest.06-0702
22. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
23. Pokrzywinski RF, Meads DM, McKenna SP, Glendenning GA, Revicki DA. Development and psychometric assessment of the COPD and Asthma Sleep Impact Scale (CASIS). Health Qual Life Outcomes. 2009;7(1):98. doi:10.1186/1477-7525-7-98
24. Ding B. Smal M Treatment trends in patients with asthma–COPD overlap syndrome in a COPD cohort: findings from a real-world survey. Int J Chron Obstruct Pulmon Dis. 2017;12:1753–1763. doi:10.2147/COPD.S136314
25. Bellia V, Catalano F, Scichilone N, et al. Sleep disorders in the elderly with and without chronic airflow obstruction: the SARA study. Sleep. 2003;26(3):318–323. doi:10.1093/sleep/26.3.318
26. Shorofsky M, Bourbeau J, Kimoff J, et al. Impaired sleep quality in COPD is associated with exacerbations: the CanCOLD cohort study. Chest. 2019;156(5):852–863.
27. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. doi:10.1056/NEJMoa0805800
28. Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. doi:10.1056/NEJMoa063070
29. Mahler DA, Kerwin E, Ayers T, et al. FLIGHT1 and FLIGHT2: efficacy and safety of QVA149 (Indacaterol/Glycopyrrolate) versus its monocomponents and placebo in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(9):1068–1079. doi:10.1164/rccm.201505-1048OC
30. Doward L, Svedsater H, Whalley D, et al. Salford Lung Study in chronic obstructive pulmonary disease (SLS COPD): follow-up interviews on patient-centred outcomes. NPJ Prim Care Resp Med. 2017;22:66. doi:10.1038/s41533-017-0066-2
31. Whalley D, Svedsater H, Doward L, et al. Follow-up interviews from The Salford Lung Study (COPD) and analyses per treatment and exacerbations. NPJ Prim Care Respir Med. 2019;29(1):20. doi:10.1038/s41533-019-0123-0
32. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. The Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
33. Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. The Lancet. 2016;388(10048):963–973. doi:10.1016/S0140-6736(16)31354-X
34. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice–based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.