Back to Journals » Drug Design, Development and Therapy » Volume 20
One-Day Aminoglycosides versus Three-Day Ceftazidime for Perioperative Prophylaxis and Postoperative Sepsis Risk in Patients with Urinary Calculi: A Propensity Score-Matched Retrospective Cohort Analysis
Authors Sun S, Guo J ![]() , Zhang Z, Guo D, Li J, Cai X
, Zhang Z, Guo D, Li J, Cai X
Received 11 January 2026
Accepted for publication 14 March 2026
Published 19 March 2026 Volume 2026:20 594549
DOI https://doi.org/10.2147/DDDT.S594549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Shuangshuang Sun,1,* Jinlin Guo,2,* Zhijia Zhang,3 Donglin Guo,1 Jun Li,4 Xinfeng Cai4
1Department of Laboratory Medicine, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, People’s Republic of China; 2Department of Pharmacy, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, People’s Republic of China; 3Department of Urology, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, People’s Republic of China; 4Department of Pharmacy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated with Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated with Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Li, Department of Pharmacy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated with Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated with Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China, Email [email protected] Xinfeng Cai, Department of Pharmacy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated with Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated with Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China, Email [email protected]
Background: Perioperative antimicrobial prophylaxis reduces infectious complications after urinary stone removal, but the optimal agent to prevent postoperative sepsis remains uncertain amid rising drug-resistant gram-negative bacteria. We compared aminoglycoside prophylaxis versus ceftazidime for prevention of postoperative sepsis.
Methods: In this retrospective propensity score-matched cohort study, clinical data were retrospectively extracted from the electronic medical record system after completion of routine clinical care. Among 420 matched patients undergoing endourological or percutaneous stone removal (210 receiving ceftazidime prophylaxis and 210 receiving aminoglycoside prophylaxis), propensity score matching was performed using age and baseline white blood cell count, and missing data were handled by multiple imputation. The primary outcome was postoperative sepsis. Multivariable conditional logistic regression was used to evaluate the independent association between prophylactic regimen and postoperative sepsis, with sensitivity analyses using an extended adjustment model and Firth penalized logistic regression.
Results: Postoperative sepsis occurred in 18 of 210 patients receiving ceftazidime and in 21 of 210 patients receiving an aminoglycoside (8.57% vs. 10.00%, P=0.614). Secondary outcomes, including mortality, postoperative antibiotic duration, renal function parameters, and microbiological eradication rates, were similar between groups. After adjustment, prophylactic regimen was not independently associated with postoperative sepsis (aOR: 1.12, 95% CI: 0.56– 2.21, P=0.753). Independent predictors of postoperative sepsis included failure of microbiological eradication, higher baseline C-reactive protein, and larger stone burden. Findings were consistent in sensitivity analyses.
Conclusion: In this propensity score-matched retrospective cohort, aminoglycoside versus ceftazidime prophylaxis was not independently associated with postoperative sepsis. These findings support consideration of shorter prophylactic strategies in carefully selected patients, but do not establish noninferiority and require confirmation in prospective adequately powered studies.
Keywords: urinary calculi, antibiotic prophylaxis, aminoglycosides, ceftazidime, sepsis, propensity score matching
Introduction
Urolithiasis is one of the most common diseases of the urinary system worldwide.1 Endourological procedures, including ureteroscopic lithotripsy and percutaneous nephrolithotomy (PCNL), have become standard treatment modalities. However, intraoperative manipulation may facilitate bacterial translocation into the bloodstream,2 leading to severe infectious complications such as urosepsis.3 Therefore, perioperative antibiotic prophylaxis is widely regarded as a key strategy to reduce the risk of postoperative infections.4–6
According to current clinical guidelines, patients with positive urine cultures or a large stone burden are usually recommended to receive approximately one week of antibiotic prophylaxis prior to retrograde urinary tract interventions.4 Ceftazidime is one of the commonly used agents for this purpose, exhibiting strong antimicrobial activity against frequent uropathogens such as Escherichia coli. Approximately 95% of ceftazidime is excreted unchanged by the kidneys, resulting in high urinary concentrations and a favorable safety profile.7 Notably, clinical practice at our center suggests that shortening the prophylactic course to three days may still provide effective infection prevention. Nevertheless, ceftazidime has limited activity against extended-spectrum β-lactamase (ESBL)–producing organisms,8 a limitation of increasing concern in the context of escalating antimicrobial resistance.
In contrast, aminoglycosides (eg, amikacin and netilmicin) achieve extremely high urinary concentrations and exhibit a pronounced post-antibiotic effect.9 These agents maintain robust activity against a broad range of Gram-negative pathogens, including ESBL-producing strains. Based on their pharmacokinetic and pharmacodynamic characteristics, the 2024 Infectious Diseases Society of America (IDSA) guidelines recommend that single-dose aminoglycoside therapy may be considered for the treatment of lower urinary tract infections caused by resistant organisms.10 Although nephrotoxicity and ototoxicity remain important safety concerns, short-term or single-dose administration has been shown to substantially reduce these risks.11
Against this background, an important clinical question arises: does a three-day ceftazidime regimen or a single-day aminoglycoside regimen provide superior efficacy and safety in preventing postoperative sepsis following urolithiasis surgery? To address this issue, we conducted a retrospective cohort study comparing these two prophylactic strategies in real-world clinical practice, aiming to generate evidence to inform and optimize perioperative antibiotic decision-making.
Materials and Methods
Study Design and Population
This retrospective cohort study was conducted at the Department of Urology, Shanxi Provincial People’s Hospital. All treatment decisions, including prophylactic antibiotic selection, were made as part of routine clinical care before study conception. After completion of treatment, clinical data were retrospectively extracted from the electronic medical record system for all eligible patients who underwent minimally invasive surgery for urolithiasis between January 1, 2022 and February 28, 2025.
The study protocol was approved by the Ethics Committee of Shanxi Provincial People’s Hospital (ID: 2025175), and the requirement for informed consent was waived due to the retrospective nature of the study. Patient data were de-identified/anonymized prior to analysis, confidentiality was strictly maintained, and the study was conducted in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Patients were eligible for inclusion if they met all of the following criteria: Age ≥ 18 years; Imaging and clinical diagnosis of ureteral stones, bladder stones, or renal stones, with or without hydronephrosis; undergoing minimally invasive stone procedures, including ureteroscopic lithotripsy (URS), cystoscopic lithotripsy, or percutaneous nephrolithotomy (PCNL); Receiving preoperative prophylactic antibiotics with either an aminoglycoside (amikacin or netilmicin) or ceftazidime. Patients were excluded if they met any of the following conditions: Presence of sepsis or septic shock prior to surgery; Known allergy to cephalosporins or aminoglycosides; Renal dysfunction before surgery (estimated glomerular filtration rate, eGFR < 50 mL/min/1.73 m2); Pre-existing hearing impairment or vestibular dysfunction; Concomitant use of other nephrotoxic medications during the perioperative period; Conversion to open surgery; Use of systemic antimicrobial agents within one month prior to surgery; Pregnancy or lactation; Microbiological cultures indicating intrinsically resistant organisms, including Gram-positive cocci, fungi, or Mycoplasma species; neither preoperative CRP nor preoperative PCT was available. The detailed patient selection process and propensity score matching procedure are presented in Figure 1.
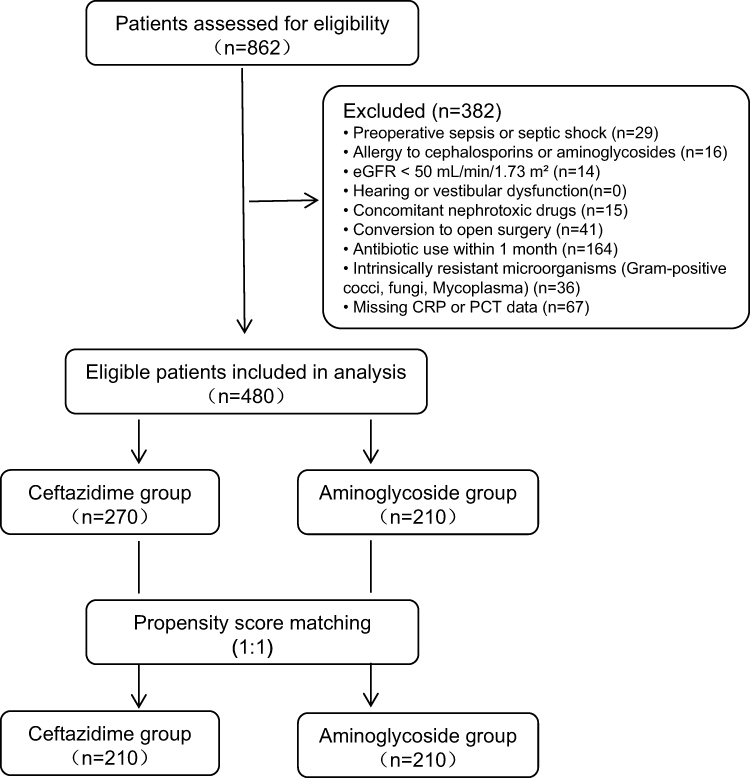 |
Figure 1 Flow chart of patient selection and propensity score matching. Among 862 patients assessed for eligibility, 382 were excluded according to the predefined exclusion criteria. A total of 480 patients were included in the final analysis and assigned to the ceftazidime group (n = 270) or the aminoglycoside group (n = 210). Propensity score matching (1:1) was performed, resulting in 210 matched patients in each group. |
Grouping and Definitions
Patients were categorized into two groups according to the preoperative prophylactic antibiotic regimen: Ceftazidime group: ceftazidime 2 g administered every 12 h for three consecutive days before surgery; Aminoglycoside group: amikacin 0.6 g once daily or netilmicin 0.2 g every 8 h, administered for one day before surgery. The choice was determined by the treating physician based on clinical judgment, patient condition, and drug availability; this was not assigned by a study protocol and should not be interpreted as randomization. Postoperative sepsis was defined according to the Sepsis-3 criteria as suspected or documented infection with acute organ dysfunction, operationalized as an increase in Sequential Organ Failure Assessment (SOFA) score of ≥2 points after surgery based on available clinical and laboratory data. Large stone burden was defined as a stone diameter ≥ 1 cm, with or without moderate to severe hydronephrosis. Length of hospital stay was defined as the duration from surgery to discharge. Microbiological eradication was defined as the absence of the originally identified pathogens in urine culture collected within 72 h after completion of the prophylactic antibiotic course. AKI was defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. Postoperative serum creatinine was monitored from the end of surgery until hospital discharge; any serum creatinine measurement obtained during this period was used for AKI ascertainment.
Data Collection
Demographic characteristics (age, sex), comorbidities, stone characteristics, surgical information, laboratory parameters (baseline renal function, serum creatinine, liver function tests, albumin, urinary white blood cell count, urine culture, CRP, and PCT), and antimicrobial treatment details were collected from the electronic medical record system.
Urine cultures were obtained within 24 h before initiation of prophylactic antibiotics and within 24 h after completion of prophylaxis. During hospitalization, urine cultures were repeated every 2–3 days as clinically indicated.
Statistical Analysis
This retrospective cohort study employed a series of statistical methods to analyze the data. No a priori sample size calculation was performed because of the retrospective design; instead, all eligible patients within the predefined study period were included. Continuous variables were summarized using means and standard deviations (for normally distributed data) or medians with interquartile ranges (for non-normally distributed data), and normality was assessed using the Shapiro–Wilk test before selecting the respective tests. Categorical variables were reported as counts and percentages. For intergroup comparisons, appropriate statistical tests were utilized: the Student’s t-test for normally distributed data, the Mann–Whitney U-test for non-normally distributed data, and the chi-square test or Fisher’s exact test, as appropriate, for categorical variables.
To account for baseline differences between the Ceftazidime and Aminoglycoside groups, propensity score matching (PSM) was performed at a 1:1 ratio with a caliper width of 0.02 using age and baseline white blood cell count as matching variables. All subsequent analyses were conducted on the matched cohort to strengthen the validity of our comparisons.
Missing data regarding inflammatory biomarkers, specifically procalcitonin (missing rate 18.62%) and C-reactive protein (missing rate 8.51%), were addressed through multiple imputation using chained equations, assuming the data were missing at random. Ten imputed datasets were created, incorporating all variables related to outcomes and the patterns of missingness.
Multivariable conditional logistic regression analyses were conducted on the pooled imputed datasets to identify independent risk factors associated with postoperative sepsis. The type of prophylactic regimen was included as a forced variable in the multivariate model to evaluate its impact on the risk of postoperative sepsis alongside other potential confounding factors.
Sensitivity analyses included an extended multivariable model additionally adjusting for diabetes mellitus and Firth penalized logistic regression to assess robustness under a limited number of events.
To examine potential heterogeneity in treatment effects across clinically relevant subgroups, prespecified subgroup analyses were performed within the propensity score-matched cohort. Subgroups were defined based on microbiological culture status (culture negative, non-drug-resistant bacterial infection, and drug-resistant bacterial infection) and stone burden (large, with a maximum diameter ≥1 cm, vs. small, <1 cm). Within each subgroup, the incidence of postoperative sepsis was compared between treatment groups, employing the chi-square test or Fisher’s exact test as appropriate. Crude odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated, with the aminoglycoside group serving as the reference category. A two-sided interaction P value <0.05 was regarded as indicative of statistically significant heterogeneity in treatment effects.
All statistical analyses were performed using xsmartanalysis software (achieved from: https://www.xsmartanalysis.com, this software is based on R version 4.3.0), and a two-sided P value <0.05 was considered statistically significant.
Results
Study Population and Baseline Characteristics
Between January 2022 and February 2025, a total of 480 adult patients undergoing minimally invasive surgery for urinary tract calculi met the eligibility criteria and were included in the analysis. Among them, 270 patients received preoperative prophylaxis with ceftazidime and 210 patients received aminoglycosides.
Before adjustment, baseline inflammatory parameters, including C-reactive protein (CRP) and white blood cell (WBC) count, differed significantly between the two treatment groups. To reduce baseline imbalance, propensity score matching (PSM) was performed at a 1:1 ratio, yielding 210 matched pairs. After matching, baseline characteristics were substantially improved and generally well balanced between the two groups, although residual differences remained in some inflammatory parameters (Table 1).
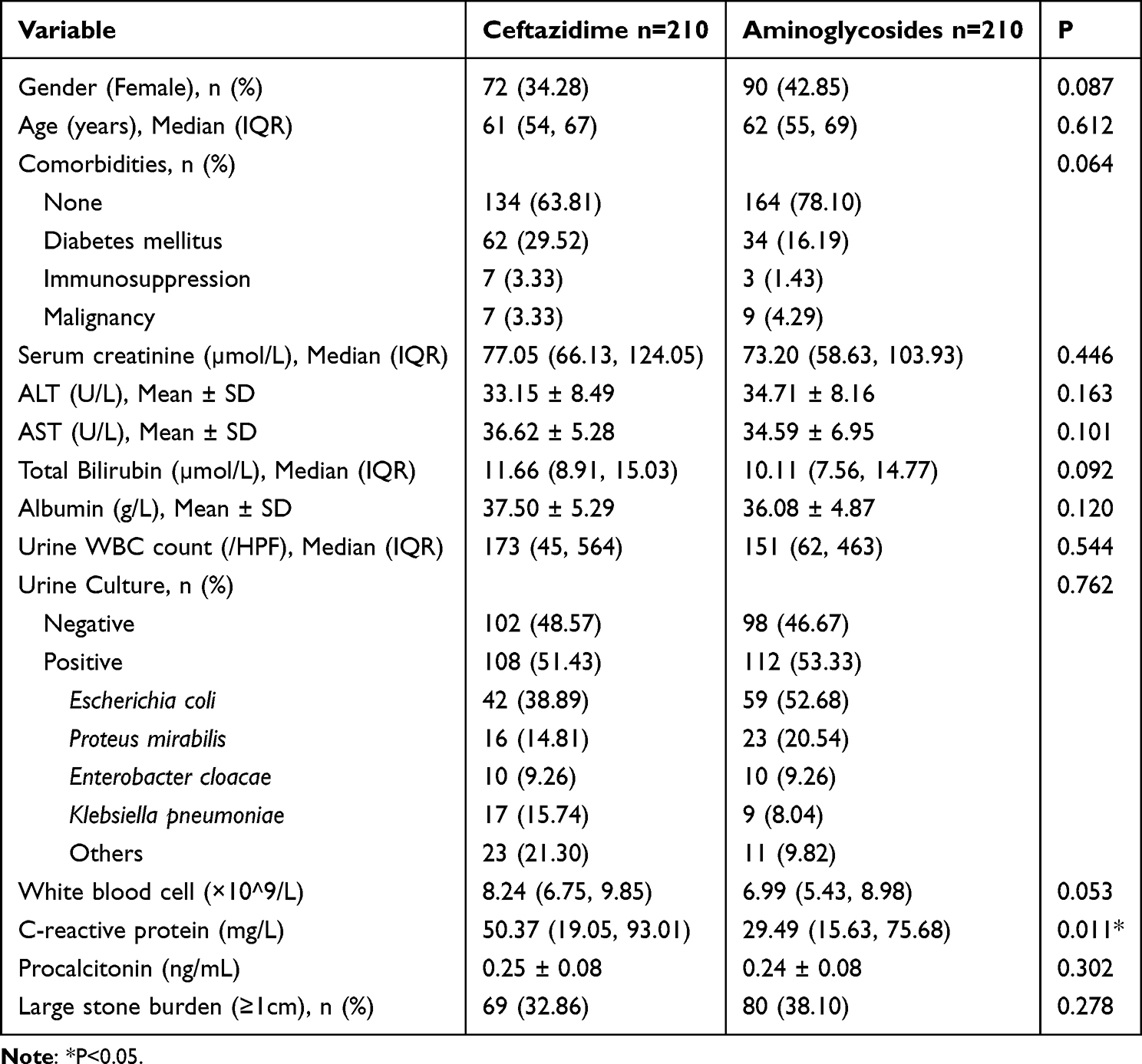 |
Table 1 Baseline Characteristics of Patients in the Propensity Score-Matched Cohort |
Postoperative Outcomes
In the propensity score–matched cohort, postoperative sepsis occurred in 8.57% of patients in the ceftazidime group and 10% of patients in the aminoglycoside group, with no statistically significant difference between the two regimens (P = 0.614). No in-hospital deaths were recorded in either group. Other postoperative outcomes were similar between groups (Table 2). The duration of postoperative antibiotic therapy, length of hospital stays, and postoperative serum creatinine levels did not differ significantly. No cases of acute kidney injury were observed during hospitalization in either group.
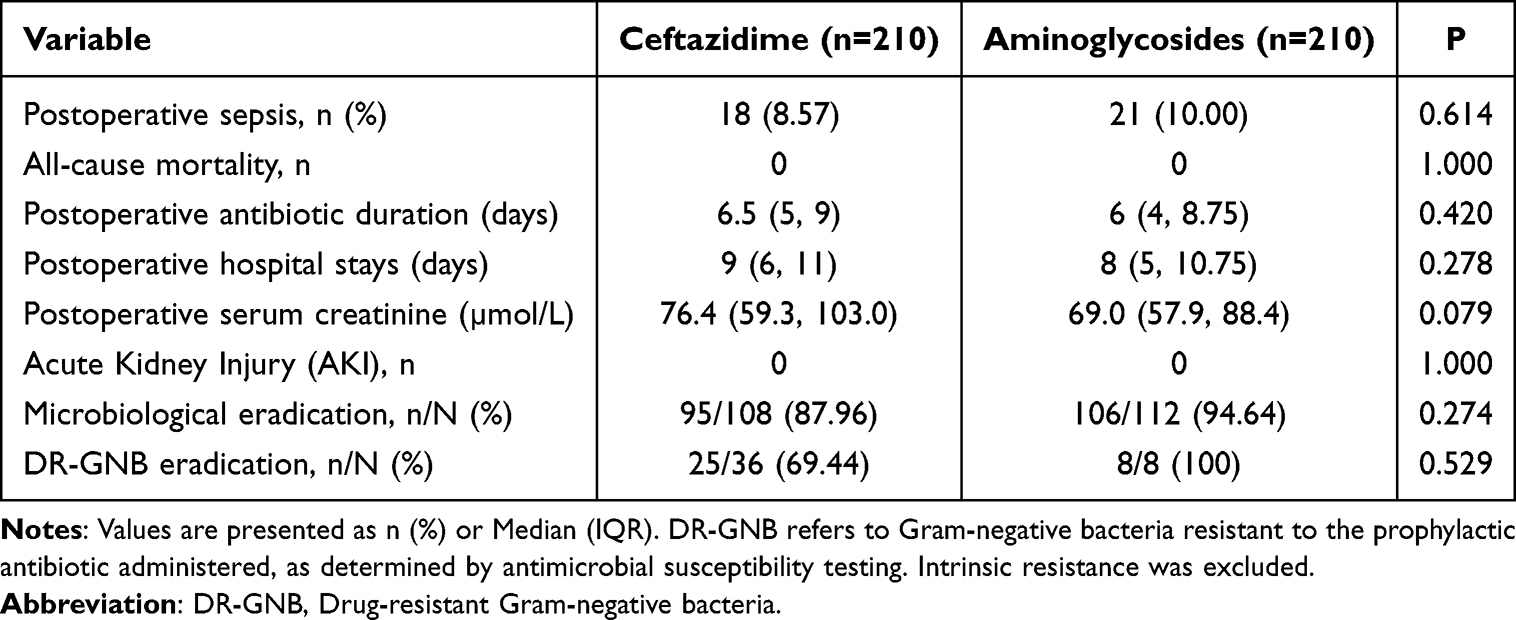 |
Table 2 Comparison of Clinical Outcomes Between Prophylactic Regimens |
Microbiological outcomes were also comparable. The overall microbiological eradication rate was 87.96% in the ceftazidime group and 94.64% in the aminoglycoside group (P = 0.274). Among patients with infections caused by drug-resistant Gram-negative bacteria, eradication rates were 69.44% and 100%, respectively, with no statistically significant difference (P = 0.529). Postoperative serum creatinine levels remained stable compared with baseline within both groups, and no clinically relevant deterioration in renal function was observed.
Factors Associated with Postoperative Sepsis
Univariate and multivariate conditional logistic regression analyses were performed to identify factors associated with postoperative sepsis. In multivariate analysis, failure of microbiological eradication, higher baseline CRP levels, and large stone burden were independently associated with an increased risk of postoperative sepsis (P < 0.05 for all). After adjustment for potential confounders, the type of prophylactic regimen was not independently associated with postoperative sepsis (Table 3).
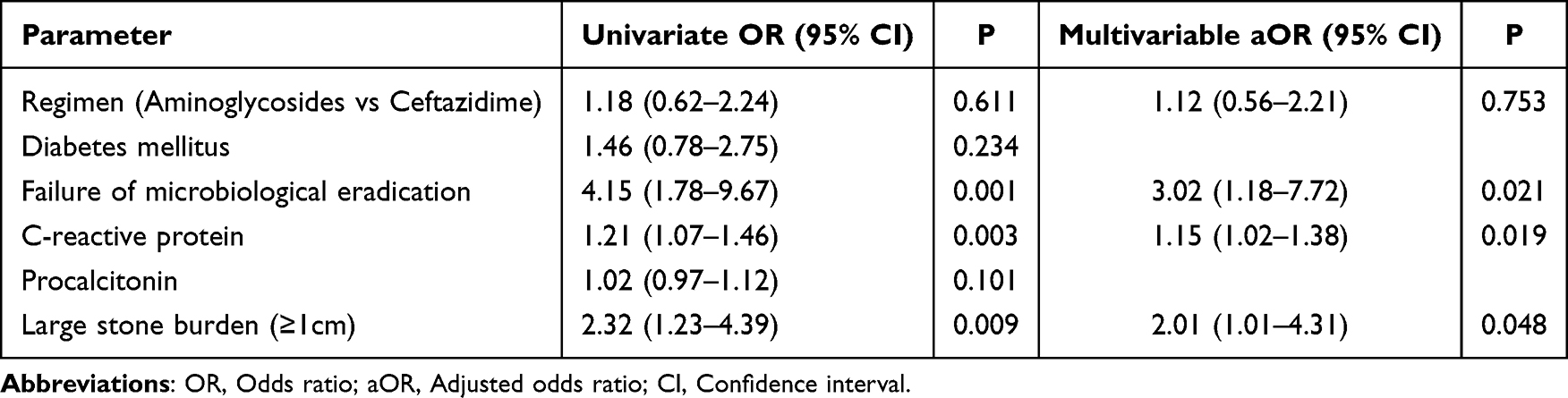 |
Table 3 Univariate and Multivariable Analysis of Risk Factors for Postoperative Sepsis |
Sensitivity Analyses
To evaluate robustness of the primary findings, we conducted two additional sensitivity analyses. First, an extended multivariable model additionally adjusting for diabetes mellitus yielded a similar estimate for prophylactic regimen, which remained not independently associated with postoperative sepsis (adjusted OR 1.10, 95% CI 0.55–2.20; P = 0.790). Diabetes mellitus was not independently associated with postoperative sepsis in the extended model (adjusted OR 1.25, 95% CI 0.62–2.53; P = 0.534). Second, using Firth penalized logistic regression to reduce small-sample bias, the association between prophylactic regimen and postoperative sepsis remained non-significant (adjusted OR 1.08, 95% CI 0.50–2.17; P = 0.813), and the direction/magnitude of the key predictors were generally consistent with the primary analysis (Tables S1 and S2).
Subgroup and Interaction Analyses
Predefined subgroup and interaction analyses were conducted within the propensity score–matched cohort to explore potential heterogeneity of treatment effects. No statistically significant interaction was observed between prophylactic regimen and DR-GNB status (adjusted odds ratio [aOR] = 0.41, 95% CI 0.05–3.29; P = 0.441). Similarly, no significant interaction was identified between prophylactic regimen and stone burden (aOR = 1.27, 95% CI 0.39–4.16; P = 0.698) (Table 4).
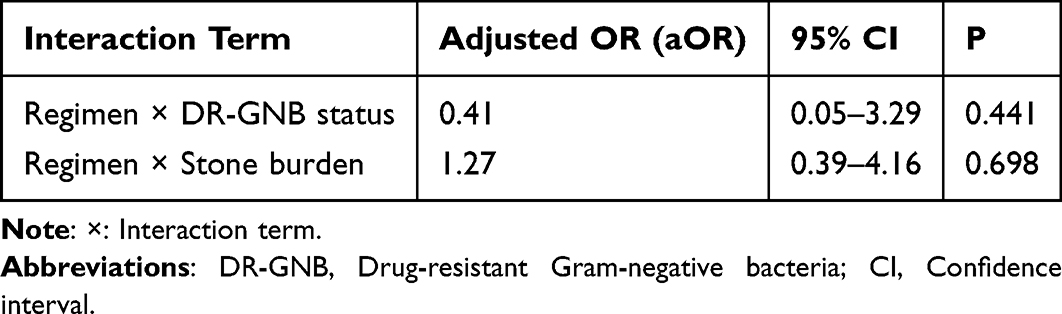 |
Table 4 Interaction Analysis Between Prophylactic Regimen and Patient Characteristics |
In exploratory subgroup analyses, the incidence of postoperative sepsis among patients with drug-resistant bacterial infections was numerically higher in the aminoglycoside group than in the ceftazidime group (12.50% vs. 8.33%); however, this difference was not statistically significant (P = 0.566). No significant differences in sepsis incidence were observed between treatment groups in subgroups defined by culture status, resistance profile, or stone burden (Table S3). Given the limited sample size and number of events in certain subgroups, these findings are reported as descriptive and were not interpreted as evidence of differential treatment effects.
Discussion
In summary, our matched retrospective analysis found no statistically significant difference in short-term postoperative sepsis between a one-day aminoglycoside protocol and a three-day ceftazidime protocol. These results may support consideration of shorter prophylactic courses in carefully selected patients—consistent with antimicrobial stewardship goals—but do not establish noninferiority. Prospective randomized trials or well-powered noninferiority studies, ideally with detailed microbiological and pharmacokinetic assessments and longer follow-up for safety endpoints, are required before broad changes to guideline recommendations can be endorsed.
Multivariable analysis demonstrated that failure of microbiological eradication, elevated baseline C-reactive protein levels, and large stone burden (≥1 cm) were independently associated with an increased risk of postoperative sepsis. These findings are consistent with prior studies,12,13 indicating that bacterial burden and baseline inflammatory status play important roles in infectious complications after endourological procedures. In contrast, no clear difference in preventive effectiveness was detected between one-day aminoglycosides and three-day ceftazidime within the limits of this retrospective analysis. Formal interaction analyses did not identify significant effect modification by drug-resistant Gram-negative bacteria status or stone burden, suggesting that the observed findings were generally consistent across clinically relevant subgroups.
Importantly, our conclusions regarding regimen choice were robust across sensitivity analyses. Given the modest number of sepsis events, we examined potential model instability by (i) extending the primary multivariable model to include diabetes mellitus, a clinically plausible confounder, and (ii) applying Firth penalized logistic regression to mitigate small-sample bias and overfitting. Both approaches produced effect estimates for prophylactic regimen that were close to the primary analysis and remained statistically non-significant, supporting the consistency of the main finding that regimen selection was not an independent determinant of postoperative sepsis in this cohort.
Previous studies have demonstrated that preoperative antibiotic prophylaxis plays an important role in reducing infectious complications after stone surgery.14–16 While some investigations have focused on prolonged prophylactic courses in high-risk patients,17,18 the present study suggests that short-term regimens may provide similar short-term protection against postoperative infectious complications, as reflected by comparable sepsis rates observed in this cohort. These results do not support the routine extension of prophylactic duration solely for the purpose of reducing postoperative sepsis in unselected patients.
From a clinical and public health perspective, shorter prophylactic regimens may offer several potential advantages. Reduced antibiotic exposure is consistent with antimicrobial stewardship principles and may decrease treatment costs and the selective pressure for antimicrobial resistance.19 In addition, shorter courses may lower the cumulative risk of drug-related adverse effects, including nephrotoxicity and ototoxicity.20,21 Despite in vitro resistance to ceftazidime observed in some cases, comparable clinical outcomes were still achieved. One possible explanation is that high urinary antibiotic concentrations,22,23 together with intraoperative reduction of bacterial burden through stone fragmentation and drainage, may partially account for the observed clinical effectiveness; however, this hypothesis was not directly tested in the present study and should be interpreted as speculative.
Several methodological strengths support the credibility of our findings, including the use of propensity score matching to reduce baseline imbalances and multiple imputation to address missing data in key inflammatory biomarkers. Nevertheless, several limitations should be acknowledged. First, as a single-center retrospective observational study, residual confounding due to unmeasured factors—such as surgeon experience, intraoperative complexity, and subjective considerations influencing antibiotic selection—cannot be fully excluded. Second, the limited sample size and number of events in certain high-risk subgroups reduce statistical power to detect small differences between regimens. In addition, because the number of events was modest relative to the number of covariates, we performed penalized (Firth) logistic regression as a sensitivity analysis, and the results were consistent with the primary model. Fourth, antimicrobial susceptibility testing may not fully reflect in vivo effectiveness in the urinary tract, where drug concentrations are influenced by urinary flow, pH, and local pharmacokinetics. Finally, the present analysis focused on short-term in-hospital outcomes; long-term adverse effects, antimicrobial resistance evolution, and recurrence of infection were not systematically evaluated.
In summary, within the limitations of this retrospective analysis, one-day aminoglycoside and three-day ceftazidime regimens were associated with similar short-term postoperative outcomes in patients undergoing minimally invasive surgery for urinary tract calculi. These regimens may be considered as potential prophylactic options in carefully selected patients, with decisions guided by individual risk assessment and local antimicrobial resistance patterns. Further large-scale prospective studies are needed to confirm these findings and to define the optimal duration and selection of prophylactic antibiotics in this clinical setting.
Conclusions
In this retrospective propensity score-matched cohort of patients undergoing endourological or percutaneous stone removal, we observed no statistically significant difference in postoperative sepsis between the ceftazidime and aminoglycoside prophylaxis groups. These findings should not be interpreted as evidence of noninferiority or equivalence, given the observational design and residual confounding. Prospective randomized studies are needed to confirm comparative effectiveness and safety.
Ethics Approval
The study protocol was approved by the Ethics Committee of Shanxi Provincial People’s Hospital (ID: 2025175), and the requirement for informed consent was waived due to the retrospective nature of the study. Patient data were de-identified/anonymized prior to analysis, confidentiality was strictly maintained, and the study was conducted in accordance with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Raheem OA, Khandwala YS, Sur RL, Ghani KR, Denstedt JD. Burden of urolithiasis: trends in prevalence, treatments, and costs. Eur Urol Focus. 2017;3(1):18–9. doi:10.1016/j.euf.2017.04.001
2. Ripa F, Cerrato C, Tandoğdu Z, et al. Clinical significance of stone culture during endourological procedures in predicting post-operative urinary sepsis: should it be a standard of care—evidence from a systematic review and meta-analysis from EAU section of Urolithiasis (EULIS). World J Urol. 2024;42(1). doi:10.1007/s00345-024-05319-0
3. Akram M, Jahrreiss V, Skolarikos A, et al. Urological guidelines for kidney stones: overview and comprehensive update. J Clin Med. 2024;13(4):1114. doi:10.3390/jcm13041114
4. Calculi EOWGoPICaAAiPwUUT. Expert opinions on perioperative infection control and antibiotic application in patients with upper urinary tract calculi (2023 edition). Chin J Urol. 2023;44(7):481–485.
5. Urology CECGoPoSSIi. Chinese expert consensus on prevention of surgical site infection in urology (2019 edition). Chin J Urol. 2019;40(6):401–404.
6. Xu P, Zhang S, Zhang Y, et al. Preoperative antibiotic therapy exceeding 7 days can minimize infectious complications after percutaneous nephrolithotomy in patients with positive urine culture. World J Urol. 2021;40(1):193–199. doi:10.1007/s00345-021-03834-y
7. Rains CP, Bryson HM, Peters DH. Ceftazidime. Drugs. 1995;49(4):577–617. doi:10.2165/00003495-199549040-00008
8. Alidjanov JF, Fritzenwanker M, Hoffman I, Wagenlehner FM. Ceftazidime-avibactam: novel antimicrobial combination for the treatment of complicated urinary tract infections. Future Microbiol. 2017;12(8):655–670. doi:10.2217/fmb-2016-0213
9. Wood MJ, Farrell W. Comparison of urinary excretion of tobramycin and gentamicin in adults. J Infect Dis. 1976;134 Suppl(Supplement 1):S133–S136. doi:10.1093/infdis/134.Supplement_1.S133
10. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clinl Infect Dis. 2024;2024:ciae403.
11. Goodlet KJ, Benhalima FZ, Nailor MD. A systematic review of single-dose aminoglycoside therapy for urinary tract infection: is it time to resurrect an old strategy? Antimicrob Agents Chemother. 2019;63(1). doi:10.1128/AAC.02165-18
12. Teh K, Tham T. Predictors of post-percutaneous nephrolithotomy sepsis: the Northern Malaysian experience. Urol Ann. 2021;13(2):156. doi:10.4103/UA.UA_28_20
13. Ganesan V, Brown RD, Jiménez JA, De S, Monga M. C-reactive protein and erythrocyte sedimentation rate predict systemic inflammatory response syndrome after percutaneous nephrolithotomy. J Endourol. 2017;31(7):638–644. doi:10.1089/end.2016.0884
14. Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American urological association/endourological society guideline, PART I. J Urol. 2016;196(4):1153–1160. doi:10.1016/j.juro.2016.05.090
15. Gravas S, Montanari E, Geavlete P, et al. Postoperative infection rates in low risk patients undergoing percutaneous nephrolithotomy with and without antibiotic prophylaxis: a matched case control study. J Urol. 2012;188(3):843–847. doi:10.1016/j.juro.2012.05.007
16. Skolarikos A, Somani B, Neisius A, et al. Metabolic evaluation and recurrence prevention for urinary stone patients: an EAU guidelines update. Eur Urol. 2024;86(4):343–363. doi:10.1016/j.eururo.2024.05.029
17. Danilovic A, Talizin TB, Torricelli FCM, et al. One week pre-operative oral antibiotics for percutaneous nephrolithotomy reduce risk of infection: a systematic review and meta-analysis. Int Braz J Urol. 2023;49(2):184–193. doi:10.1590/s1677-5538.ibju.2022.0544
18. Sur RL, Krambeck AE, Large T, et al. A randomized controlled trial of preoperative prophylactic antibiotics for percutaneous nephrolithotomy in moderate to high infectious risk population: a report from the EDGE Consortium. J Urol. 2021;205(5):1379–1386. doi:10.1097/JU.0000000000001582
19. Schnabel MJ, Wagenlehner FME, Schneidewind L. Perioperative antibiotic prophylaxis for stone therapy. Curr Opinion Urol. 2019;29(2):89–95. doi:10.1097/MOU.0000000000000576
20. Dagan A, Epstein D, Neuberger A, Isenberg J. Amikacin treatment in urinary tract infection patients: evaluating the risk of acute kidney injury – a retrospective cohort study. J Chemother. 2024;36(5):398–402. doi:10.1080/1120009X.2024.2319454
21. Ben-Ami R, Weiss-Meilik A, Zadka H, Elbaz M. Effectiveness and safety of an institutional aminoglycoside-based regimen as empirical treatment of patients with pyelonephritis. J Antimicrob Chemother. 2020;75(8):2307–2313.
22. Schentag JJ, Jusko WJ. Renal clearance and tissue accumulation of gentamicin. Clin Pharmacol Ther. 1977;22(3):364–370. doi:10.1002/cpt1977223364
23. Zieck SE, de Vroom SL, Mulder FP, et al. Pharmacokinetic/pharmacodynamic target attainment of ceftazidime in adult patients on general wards with different degrees of renal function: a prospective observational bicenter cohort study. Antibiotics. 2023;12(3):469. doi:10.3390/antibiotics12030469
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.