Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Oncology Healthcare Providers’ Knowledge, Attitudes, and Practices Regarding Chemotherapy-Induced Myelosuppression in Ovarian Cancer in Haikou, China
Received 9 April 2025
Accepted for publication 13 September 2025
Published 15 October 2025 Volume 2025:18 Pages 6733—6744
DOI https://doi.org/10.2147/JMDH.S533373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Xiaohang Liu,1 Jiashou Tao2
1Department of Gynecology, Hainan General Hospital, Hainan Affiliated Hospital of Hainan Medical University, Haikou, Hainan, 570311, People’s Republic of China; 2Department of Hepatobiliary Surgery, Hainan Cancer Hospital, Haikou, Hainan, 570000, People’s Republic of China
Correspondence: Jiashou Tao, Email [email protected]
Purpose: Chemotherapy-induced myelosuppression can profoundly affect patient prognosis. This study assessed the knowledge, attitude, and practice (KAP) of oncology healthcare providers regarding chemotherapy-induced myelosuppression in patients with ovarian cancer.
Patients and Methods: This cross-sectional study was conducted at Hainan General Hospital from September 14 to December 12, 2023, and enrolled oncology healthcare providers. A self-designed questionnaire (Cronbach’s α=0.826) was used to collect participant characteristics and KAP scores. Multivariable logistic regression and structural equation modeling (SEM) analyses were performed to determine the factors influencing KAP and the relationships among KAP dimensions.
Results: The analysis included 516 participants. The median knowledge, attitude, and practice scores were 31 (19, 35) (/36, 86.11%), 23 (18, 27) (/35, 65.71%), and 39 (29, 45.5) (/50, 78.00%), respectively. The multivariable analysis showed that the female gender (OR=0.481, 95% CI: 0.259– 0.893, P=0.020), oncologist (OR=0.451, 95% CI: 0.220– 0.923, P=0.029), gynecology nurse (OR=2.530, 95% CI: 1.121– 5.709, P=0.025), oncology nurse (OR=2.225, 95% CI: 1.061– 4.664, P=0.034), knowledge score > 31 (OR=13.969, 95% CI: 7.615– 25.625, P< 0.001), and attitude score > 23 (OR=9.127, 95% CI: 5.111– 16.300, P< 0.001) were independently associated with a practice score > 39. In the adjusted SEM, knowledge directly influenced attitude (β=0.817, P=0.010) and practice (β=0.349, P=0.010), attitude directly influenced practice (β=0.566, P=0.010), and knowledge indirectly influenced practice (β=0.462, P=0.010).
Conclusion: This study revealed that oncology healthcare providers in oncology and obstetrics/gynecology in Haikou, China, had good knowledge and practice but moderate attitudes regarding chemotherapy-induced myelosuppression in patients with ovarian cancer. This study identified categories of healthcare providers who would benefit from educational activities and training. Improving the KAP toward chemotherapy-induced myelosuppression in cancer patients could help improve patient outcomes. Policymakers should also facilitate the KAP improvements in healthcare professionals.
Keywords: ovarian cancer, chemotherapy, myelosuppression, healthcare providers, KAP, cross-sectional study
Introduction
Ovarian cancer is a leading cause of death from gynecologic malignancy,1 with a lifetime risk estimated at 1 in 50–70 women.2–4 The highest incidence of ovarian cancer is reported in individuals aged 60–64 years, with most ovarian cancer diagnoses occurring in individuals over age 50 years.2,3 Symptoms of ovarian cancer often do not present until the advanced stages of the disease.2–4 The treatment of ovarian cancer is multidisciplinary and includes surgery, chemotherapy, targeted therapy, and radiation therapy.5–7 Chemotherapy is a mainstay of treatment and aims at controlling cancer growth if inoperable, eradicating the microscopic residual disease after surgery, and killing the cancer cells that might have spread distantly.8
Chemotherapy has numerous side effects of variable nature and intensity depending upon the exact drugs being used. The most feared side effect by the patients is alopecia,9 but it is a benign side effect from a medical point of view. On the other hand, one of the most fearful side effects of chemotherapy is myelosuppression, which results in anemia, thrombocytopenia, neutropenia, and/or leukopenia, all of which have potentially serious detrimental impacts on prognosis and can lead to death.10–12 Chemotherapy-induced myelosuppression places a substantial real-world burden on patients in the community cancer care setting.13 In addition to anemia and increased risks of bleeding and infections, myelosuppression can lead to chemotherapy delays or discontinuation, impacting cancer prognosis.10–12 Febrile neutropenia is a serious adverse event in patients receiving chemotherapy and is a medical emergency that can lead to death.14 Furthermore, myelosuppression significantly impacts the patient’s quality of life.15
Therefore, healthcare providers working with patients with gynecological cancers, including medical oncologists and gynecologists, must be aware of the possibility of myelosuppression in patients with ovarian cancer treated with chemotherapy. Healthcare providers play crucial roles in detecting, diagnosing, and managing myelosuppression. Early management using transfusion of blood products or antibiotic treatment is often required.16 Knowledge, attitude, and practice (KAP) studies are designed to provide quantitative and qualitative data about the gaps, misconceptions, and misunderstandings that can impede the optimal performance of a given subject.17,18 KAP studies are particularly useful to determine the points that should be targeted by future educational activities. No previous studies examined the KAP of healthcare providers toward chemotherapy-induced myelosuppression in patients with ovarian cancer, but previous studies reported poor to moderate KAP among healthcare providers toward safety issues and neutropenia in China,19 the Sultanate of Oman,20 Iran,21 the United States of America,22 Turkey,23 and Belgium.24 Although those studies can provide hints on the KAP toward myelosuppression in cancer patients,19–24 they are not specific to ovarian cancer. The chemotherapy regimens used in ovarian cancer carry a high risk of myelosuppression, with the carboplatin plus paclitaxel regimen being associated with an incidence of 27.5% for grade 3–4 neutropenia and 3.2% of grade 3–4 thrombocytopenia.25 In addition, ovarian cancer patients carrying BRCA1/2 mutations (5%–15% of all ovarian cancers) are more likely to develop significant anemia (greater falls in hemoglobin), require more red blood cell transfusions, and have more treatment delays or dose reductions due to hematologic toxicity compared to non-carriers.26
Therefore, the present study aimed to assess the KAP of healthcare providers in oncology and obstetrics/gynecology in Haikou, China, regarding chemotherapy-related myelosuppression in patients with ovarian cancer. The results will help determine the points to be improved through educational activities, possibly translating into better patient care and prognosis.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted at Hainan General Hospital from September 14 to December 12, 2023, and enrolled oncology healthcare providers in oncology and gynecology. The study was approved by the ethics committee of Hainan General Hospital ([2024]230). All informed consent was confirmed through an electronic questionnaire.
The inclusion criteria were 1) Healthcare providers involved in managing cancer and chemotherapy patients in the Department of Gynecology and Oncology, and 2) provided informed consent for the study. The exclusion criteria were 1) completion time of the questionnaire in <90 s (ie, 2 s to answer single-choice items and 3 s for multiple-choice items (n=43),27 rounded down to 90s) or >1800s, 2) work experience of <1 year.
Questionnaire introduction
The questionnaire design drew inspiration from relevant guidelines and literature, specifically the Standardized Management Guidelines for Chemotherapy-Related Neutropenia by the Chinese Society of Clinical Oncology (CSCO)28 and the Expert Consensus on the Diagnosis and Treatment of Myelosuppression Caused by Antitumor Drugs in Integrative Chinese and Western Medicine. After the initial design, feedback was sought from two gynecology specialists and one oncology specialist from Hainan General Hospital, leading to modifications. The preliminary questionnaire draft underwent a pilot study involving 46 participants, and the Cronbach’s α coefficient was 0.826, indicating good internal consistency reliability.
The final questionnaire comprised four dimensions: demographic data, knowledge dimension, attitude dimension, and practice dimension (Appendix). The knowledge dimension included 18 questions, with 2 points awarded for correct answers and 1 point for incorrect or unclear responses, resulting in a score range of 18–36 points. The attitude dimension encompassed seven questions, using a 5-point Likert scale ranging from very positive (5 points) to very negative (1 point), resulting in a score range of 7–35 points. The practice dimension consisted of 10 questions, using a 5-point Likert scale ranging from always (5 points) to never (1 point), with a score range of 10–50 points. Good KAP was defined as scores of >75%, moderate as 50%-74%, and poor as <50%.29 Hence, the cutoffs for the knowledge, attitude, and practice scores were ≥31.5/27-31.5/<27, ≥28/21-28/<21, and ≥40/30-39/<30, respectively.
Questionnaire Collection
Ten tertiary hospitals in the Hainan region were initially approached through phone calls and emails. During this process, approximately 1000 healthcare providers meeting the research criteria were identified. Due to the inability to establish contact or refusal to participate, three hospitals were excluded. Eventually, a collaborative relationship was established with seven hospitals and 700 healthcare providers, of which 526 expressed willingness to participate in the study. A team of six research assistants was set up to assist in the questionnaire collection process. These research assistants were experienced healthcare providers in specialties such as gynecology and oncology, received professional training, and obtained GCP certification.
In the participant recruitment process, contact information for department heads was obtained through the hospitals. Through phone calls, adding contacts on WeChat, and setting up WeChat groups, the department heads transmitted the questionnaires to the WeChat groups and clarified any doubts. In addition, professionals were stationed at display boards or in consultation rooms to offer one-on-one guidance and answer questions about completing the questionnaire. The participants were given small gifts upon completing the questionnaire to encourage participation.
Following the completion of the questionnaire collection, data cleaning and organization were conducted, checking for potential errors in responses, leading to exclusion. This series of rigorous steps aimed to ensure the accuracy and reliability of the research data.
Sample Size
The formula n[(z1-α/2)/δ]2×P×(1-P) can be used to calculate the sample size of cross-sectional surveys. In the formula, n represents the sample size for each group, α represents the type I error (which is typically set at 0.05), Z1-α/2=1.96, δ represents the allowable error (typically set at 0.05), and p is set at 0.5 (as setting it at 0.5 maximizes the value and ensures a sufficiently large sample size). Hence, the calculated sample size was 384. Considering an estimated questionnaire response rate of 90%, a minimum of 430 questionnaires were needed.
Statistical Analysis
Descriptive analysis was used for the scores in each dimension. Based on the normality test results, data distribution was presented using means ± standard deviation or median (25th percentile, 75th percentile). Categorical data were presented as n (%). Differences in scores between survey subjects with different demographic characteristics were compared: depending on the normality of data distribution, Student’s t-test and the Wilcoxon-Mann–Whitney test were used for two-group comparisons, and ANOVA and the Kruskal–Wallis test were used for multiple group comparisons. Pearson or Spearman correlation coefficients were used for correlation analysis. Univariable and multivariable analyses were conducted to identify factors influencing practice (with the median as the cutoff for each dimension). Variables for inclusion in the multivariable regression were based on univariable P<0.10 or P<0.25. A stepwise approach was used for variable selection in the model, where P<0.05 was considered statistically significant. A structural equation modeling (SEM) analysis was used to analyze the relationships between the dimensions of the questionnaire and to explore the mediating role of attitude on knowledge and practice.
Results
Characteristics of the Participants
A total of 526 questionnaires were collected. After excluding 10 questionnaires with response times <90 s or >1800 s, 516 valid questionnaires remained. The formal study’s Cronbach’s α coefficient was 0.951, and the KMO value was 0.885.
The participants were 34.5 (31, 40) years old. Most participants were 30–35 years old (31.0%), female (64.7%), with a bachelor’s degree (51.0%), were working in public tertiary hospitals (35.5%), had no professional title (30.0%), had 5–15 years of work experience (54.2%), were gynecologists (40.5%), and were ever treated a patient with chemotherapy for ovarian cancer (72.3%) (Table 1).
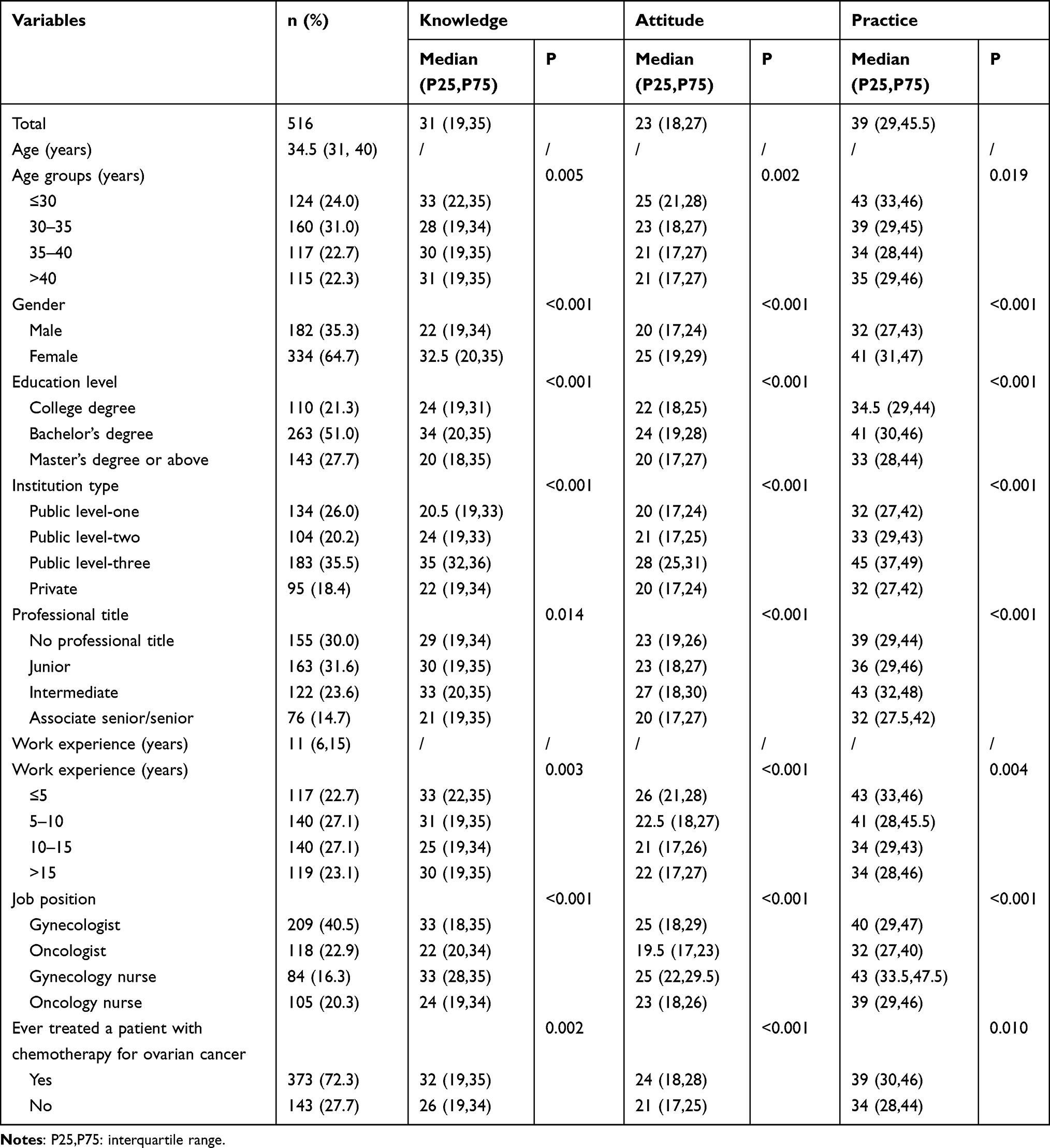 |
Table 1 Characteristics of the Participants and KAP Score |
Knowledge, Attitude, and Practice
The median knowledge score was 31 (19, 35) (/36, 86.11%) (Table 1). A higher mistake rate was observed for K5 (22.3% mistake; “Febrile neutropenia is the most severe clinical complication”) (Table S1). The median attitude score was 23 (18, 27) (/35, 65.71%) (Table 1). Table S2 presents the distribution of the responses to the attitude items. The median practice score was 39 (29, 45.5) (/50, 78.00%) (Table 1). Table S3 presents the distribution of the responses to the practice items.
Females had consistently higher KAP scores than males, gynecologists had higher KAP scores than oncologists, and gynecology nurses had higher KAP scores than oncology nurses (Table 1). As shown in Table S4, there were significant differences in the distribution of genders among positions, with females being underrepresented among oncologists. Females had higher practice scores than males among gynecologists (43 (34.5.58) vs 30 (25,41), P<0.001) and oncologists (34 (30,43) vs 30 (26,37.5), P=0.003). There were no gender differences among gynecology and oncology nurses (Table S5).
Correlations
As shown in Table S6, the knowledge scores were correlated to the attitude (r=0.728, P<0.001) and practice (r=0.742, P<0.001) scores, and the attitude scores were correlated to the practice scores (r=0.743, P<0.001).
Multivariable Analysis of Practice
The multivariable analysis showed that the female gender (OR=0.481, 95% CI: 0.259–0.893, P=0.020), oncologist (OR=0.451, 95% CI: 0.220–0.923, P=0.029), gynecology nurse (OR=2.530, 95% CI: 1.121–5.709, P=0.025), oncology nurse (OR=2.225, 95% CI: 1.061–4.664, P=0.034), knowledge score >31 (OR=13.969, 95% CI: 7.615–25.625, P<0.001), and attitude score >23 (OR=9.127, 95% CI: 5.111–16.300, P<0.001) were independently associated with a practice score >39 (Table 2).
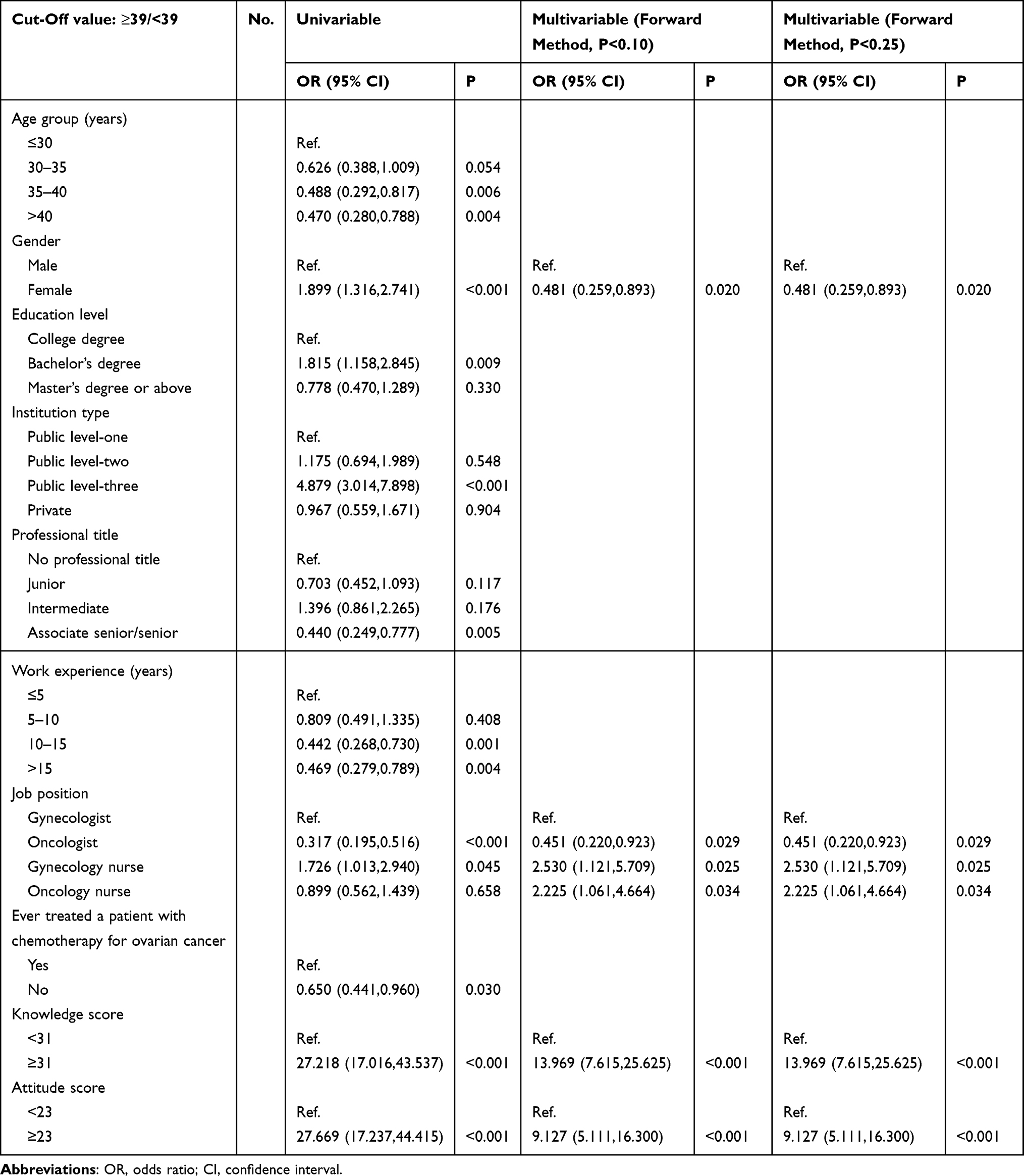 |
Table 2 Factors of Practice Based Univariable and Multivariable Logistic Regression |
Differences in Scores According to Gender and Position
As shown in Table 3, the KAP scores and the scores for all individual practice items were higher in females compared with males and all lower in oncologists compared with gynecologists, gynecology nurses, and oncology nurses (all P<0.05).
 |
Table 3 Specific Differences in KAP Among Doctors of Different Genders and Positions |
Structural Equation Modeling Analysis
The SEM is illustrated in Figure 1. Table 4 shows that the model’s fit was good before and even better after adjustment. After adjustment, knowledge directly influenced attitude (β=0.817, strong effect, P=0.010) and practice (β=0.349, moderate effect, P=0.010), attitude directly influenced practice (β=0.566, strong effect, P=0.010), and knowledge indirectly influenced practice through attitude (β=0.462, moderately strong effect, P=0.010) (Table 5).
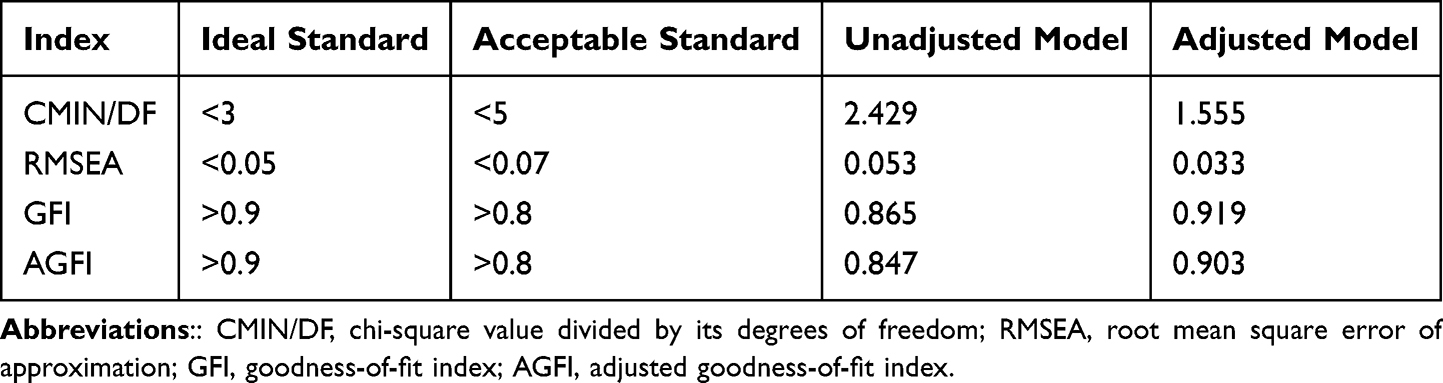 |
Table 4 Fit Indices of the SEM Before and After Model Adjustment |
 |
Table 5 Bootstrap Analysis of Mediating Effect Significance Test for the Final Mode |
 |
Figure 1 The structural equation model (SEM) before and after model adjustment. (A) Before model adjustment. (B) After model adjustment. The structural equation model is a comprehensive statistical approach to testing hypotheses about relations among observed (Knowledge, Attitude, and Practice) and latent variables (the questions for each dimension, such as K1~K15). 1) Graphic shape: The latent variables are represented by ellipses or circles, observed variables are depicted as rectangles or squares, and error terms are illustrated by small circles connected to the corresponding observed variables. 2) Arrows: The arrows and coefficients among the three KAP constructs indicate both the direction and strength of the relationships between the latent variables. The small circles associated with A and P represent the residual terms. A unidirectional arrow signifies the direction of causation, specifically from cause to effect. When an arrow points from one latent variable to another, it indicates that the former exerts a direct effect on the latter. Conversely, if the latent variable is directed from the observed variable, it signifies that the latent variable is represented by that observed variable. 3) Number: The numerical value on the arrow connecting the latent variable to the observed variable signifies the factor loading, which reflects the strength of the association between the observed variable and the latent variable, specifically the regression coefficient of the observed variable with respect to the latent variable. A positive value indicates a positive correlation, suggesting that as the latent variable increases, the observed variable also tends to increase; conversely, a negative value indicates a negative correlation, implying that as the latent variable increases, the observed variable tends to decrease. |
Discussion
Chemotherapy-induced myelosuppression can profoundly affect patient prognosis. This cross-sectional study assessed the KAP of healthcare providers in oncology and obstetrics/gynecology in Haikou, China, regarding chemotherapy-induced myelosuppression in patients with ovarian cancer. The results suggest that healthcare providers in oncology and obstetrics/gynecology had good knowledge and practice but moderate attitudes regarding chemotherapy-induced myelosuppression in patients with ovarian cancer. This study identified categories of healthcare providers who would benefit from educational activities and training.
Myelosuppression is an important side effect of cytotoxic chemotherapy and can even be fatal.10–12 Therefore, a proper knowledge of myelosuppression among healthcare providers involved in cancer treatment is crucial. No previous studies specifically examined the KAP of healthcare providers toward chemotherapy-induced myelosuppression in patients with ovarian cancer. Still, a study revealed poor KAP among hospital pharmacists regarding the safety issues of post-discharge antitumor agents in China.19 Another study in Oman revealed moderate KAP of nurses toward neutropenia.20 Naghdi et al21 reported suboptimal knowledge of neutropenia among nurses, with <20% having adequate practice regarding infection control. In Turkey, a study revealed that although nurses’ knowledge of infection control among neutropenic patients was good, their practice was poor.23 A study from New York showed that 80% of the oncology nurses followed the National Comprehensive Cancer Network (NCCN) guidelines on chemotherapy-induced neutropenia and febrile neutropenia,22 suggesting that the level of economic development might play a role in the KAP toward chemotherapy-induced myelosuppression.
The present study showed a gap in attitude among the participants. Several factors could contribute to such results. Indeed, Chinese physicians often operate in a system that favors physician-led decision-making, with less emphasis on patient involvement compared to Western countries. This stems from deeply rooted Confucian cultural values prioritizing hierarchical authority and collective well-being, leading physicians to make treatment decisions with minimal patient input.30,31 There can be a higher reliance on traditional Chinese medicine or culturally familiar treatment modalities, which may affect attitudes toward Western chemotherapy protocols and adverse event management.31 Chinese patients are generally accustomed to defaulting to physician judgment, reducing the need for physicians to communicate risks or engage in patient-centered planning, which can further reinforce traditional attitudes toward chemotherapy side-effect management.30 Physician attitudes are influenced by hospital level. Tertiary hospitals and well-resourced institutions tend to foster more progressive, patient-centered attitudes, while secondary and private hospitals may reinforce traditional, hierarchical relationships and practices.30 Overburdened hospitals and high patient loads can limit time for detailed communication and individualized care, potentially leading to underreporting or underrecognition of chemotherapy-induced myelosuppression.32 Pressures from institutional policies, such as performance evaluations linked to diagnosis-related groups (DRGs) and remuneration issues, can affect physician attitudes and engagement with best practices, leading to gaps between knowledge and actual clinical practice.33,34 China’s medical education system features varied training tracks (3–8 years), and significant quality gaps exist, particularly in less-developed regions. This leads to uneven physician competencies and attitudes toward chemotherapy management.35 Traditional training has focused more on disease-centered problem solving and less on communication skills or patient-centered care, resulting in physicians who may be less attuned to the psychosocial aspects of myelosuppression and its impact on patients.30,35 Opportunities for standardized, ongoing training in chemotherapy-induced adverse event management remain sporadic, with newer reforms only recently targeting these issues.35,36 Studies show that increased knowledge among physicians does not consistently lead to improved attitudes or practice, especially in the absence of effective incentives or practical training modules.33
In the present study, knowledge positively influenced attitude and practice, and attitude positively influenced practice, as also supported by the multivariable analysis. Therefore, improving knowledge should also improve practice. In the present study, the main knowledge gap was about febrile neutropenia. Interestingly, febrile neutropenia was also identified as being the main gap in a pan-European study performed in the early 2000s when planning a Europe-wide training program in hematological toxicities.24 Febrile neutropenia is a common cause of treatment delays and discontinuations and can be life-threatening.37 Hence, knowledge about febrile neutropenia should be improved and emphasized. According to the multivariable analysis, practice should be improved among females and oncologists. Gynecologists and nurses showed higher practice scores than oncologists, probably because healthcare providers work more closely with patients than oncologists.
This study had limitations. Only seven hospitals participated in the study, all from a single geographical area, limiting the generalizability of the conclusions. Only physicians and nurses in obstetrics and gynecology were enrolled, and the KAP toward myelosuppression among healthcare providers from other departments is unknown. In addition, pharmacists were not enrolled. The cross-sectional design prevented the analysis of causality. A SEM analysis was performed as a surrogate for causality among KAP dimensions, but SEM analyses provide a statistical estimation of causality based on predefined hypotheses.38–40 Hence, the results must be taken with caution. All KAP studies are subject to the social desirability bias, in which the participants can answer what they know they should think or do instead of what they are really thinking or doing.41,42
Conclusions
In conclusion, healthcare providers in oncology and obstetrics/gynecology in Haikou, China, appeared to have good knowledge and practice but moderate attitudes regarding chemotherapy-induced myelosuppression in patients with ovarian cancer. This study identified categories of healthcare providers in Haikou who would benefit from educational activities and training. Improving the KAP toward chemotherapy-induced myelosuppression in cancer patients could help improve patient outcomes. Policymakers should also facilitate the KAP improvements in healthcare professionals. There is also a need for a nationwide study on the subject; the results could help standardize the care of chemotherapy-induced myelosuppression. The questionnaire could eventually be used for international studies to help design national and international training, but cross-cultural validation will be necessary.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Statement
All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The study was approved by the ethics committee of Hainan General Hospital ([2024]230). All informed consent was confirmed through an electronic questionnaire. All methods were carried out in accordance with relevant guidelines and regulations.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(6):vi24–32. doi:10.1093/annonc/mdt333
3. National Institute for Health Care and Excellence (NICE). Ovarian Cancer: Recognition and Initial Management. Clinical Guideline [CG122]. National Institute for Health Care and Excellence; 2023.
4. American College of O. Gynecologists’ Committee on Practice B-G. Practice Bulletin No. 174: evaluation and Management of Adnexal Masses. Obstet Gynecol. 2016;128(5):e210–e226. doi:10.1097/AOG.0000000000001768.
5. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer. Version 1.2024. National Comprehensive Cancer Network; 2024.
6. Colombo N, Sessa C, du Bois A, et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent diseasedagger. Ann Oncol. 2019;30(5):672–705. doi:10.1093/annonc/mdz062
7. Komiyama S, Katabuchi H, Mikami M, et al. Japan Society of Gynecologic Oncology guidelines 2015 for the treatment of ovarian cancer including primary peritoneal cancer and fallopian tube cancer. Int J Clin Oncol. 2016;21(3):435–446. doi:10.1007/s10147-016-0985-x
8. Zafar A, Khatoon S, Khan MJ, Abu J, Naeem A. Advancements and limitations in traditional anti-cancer therapies: a comprehensive review of surgery, chemotherapy, radiation therapy, and hormonal therapy. Discov Oncol. 2025;16(1):607. doi:10.1007/s12672-025-02198-8.
9. Ozusaglam E, Can G. The Impact of the Perception of Chemotherapy-Induced Alopecia on Psychosocial Life. Florence Nightingale J Nurs. 2021;29(3):361–370. doi:10.5152/FNJN.2021.19098
10. Wang Y, Probin V, Zhou D. Cancer therapy-induced residual bone marrow injury-Mechanisms of induction and implication for therapy. Curr Cancer Ther Rev. 2006;2(3):271–279. doi:10.2174/157339406777934717
11. Epstein RS, Basu Roy UK, Aapro M, et al. Cancer Patients’ Perspectives and Experiences of Chemotherapy-Induced Myelosuppression and Its Impact on Daily Life. Patient Prefer Adherence. 2021;15:453–465. doi:10.2147/PPA.S292462
12. Goldschmidt J, Monnette A, Shi P, Venkatasetty D, Lopez-Gonzalez L, Huang H. Burden of chemotherapy-induced myelosuppression among patients with ES-SCLC in US community oncology settings. Future Oncol. 2022;18(35):3881–3894. doi:10.2217/fon-2022-0754
13. Epstein RS, Weerasinghe RK, Parrish AS, Krenitsky J, Sanborn RE, Salimi T. Real-world burden of chemotherapy-induced myelosuppression in patients with small cell lung cancer: a retrospective analysis of electronic medical data from community cancer care providers. J Med Econ. 2022;25(1):108–118. doi:10.1080/13696998.2021.2020570
14. Hashiguchi Y, Kasai M, Fukuda T, Ichimura T, Yasui T, Sumi T. Chemotherapy-induced neutropenia and febrile neutropenia in patients with gynecologic malignancy. Anticancer Drugs. 2015;26(10):1054–1060. doi:10.1097/CAD.0000000000000279
15. Crawford J, Herndon D, Gmitter K, Weiss J. The impact of myelosuppression on quality of life of patients treated with chemotherapy. Future Oncol. 2024;20(21):1515–1530. doi:10.2217/fon-2023-0513
16. Lyman GH, Kuderer NM, Aapro M. Improving Outcomes of Chemotherapy: established and Novel Options for Myeloprotection in the COVID-19 Era. Front Oncol. 2021;11:697908. doi:10.3389/fonc.2021.697908
17. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and Conducting Knowledge, Attitude, and Practice Surveys in Psychiatry: practical Guidance. Indian J Psychol Med. 2020;42(5):478–481. doi:10.1177/0253717620946111
18. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. 2008. Available from: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf.
19. Xu X, Yang Y, Fan Q, Zhu Z. The knowledge, attitude and practice of hospital pharmacists on the safety issues of antitumor agents for the patients discharged in China. Transl Cancer Res. 2021;10(1):201–209. doi:10.21037/tcr-20-2418
20. Al Qadire M, Ballad CAC, Aljezawi M, et al. Nurses’ knowledge of chemotherapy-induced neutropenia and its management: a cross-sectional survey. J Cancer Res Clin Oncol. 2023;149(7):2893–2901. doi:10.1007/s00432-022-04140-9
21. Naghdi H, Azizzadeh Forouzi M, Dehghan M. Iranian Nurses’ Knowledge of Neutropenia and Their Practice for Infection Prevention in Patients with Cancer. J Cancer Educ. 2021;36(3):547–555. doi:10.1007/s13187-019-01663-7
22. Nirenberg A, Reame NK, Cato KD, Larson EL. Oncology nurses’ use of National Comprehensive Cancer Network clinical practice guidelines for chemotherapy-induced and febrile neutropenia. Oncol Nurs Forum. 2010;37(6):765–773. doi:10.1188/10.ONF.765-773
23. Tarakcioglu Celik GH, Korkmaz F. Nurses’ knowledge and care practices for infection prevention in neutropenic patients. Contemp Nurse. 2017;53(2):143–155. doi:10.1080/10376178.2016.1254566
24. Foubert J, Kearney N, Ouwerkerk J, Uhlenhopp M, Vaessen G. Knowledge of haematological toxicities amongst European nurses--a learning needs assessment. Eur J Oncol Nurs. 2005;9(3):239–247. doi:10.1016/j.ejon.2004.09.009
25. Mahner S, Meier W, du Bois A, et al. Carboplatin and pegylated liposomal doxorubicin versus carboplatin and paclitaxel in very platinum-sensitive ovarian cancer patients: results from a subset analysis of the CALYPSO Phase III trial. Eur J Cancer. 2015;51(3):352–358. doi:10.1016/j.ejca.2014.11.017
26. Christie A, Che Bakri A, Roxburgh P, et al. Chemotherapy-induced myelosuppression in ovarian cancer patients with germline BRCA1/2 mutations: a case control study. J clin oncol. 2013;31(15_suppl):5571. doi:10.1200/jco.2013.31.15_suppl.5571
27. Ulitzsch E, Pohl S, Khorramdel L, Kroehne U, von Davier M. A Response-Time-Based Latent Response Mixture Model for Identifying and Modeling Careless and Insufficient Effort Responding in Survey Data. Psychometrika. 2022;87(2):593–619. doi:10.1007/s11336-021-09817-7
28. Chinese Society of Clinical Oncology Guidance Working C. Guidelines for standardizedmanagement of neutropenia induced by chemotherapy and radiotherapy. Zhonghua Zhong Liu Za Zhi. 2017;39(11):868–878. doi:10.3760/cma.j.issn.0253-3766.2017.11.011.
29. Ahlgren M, Funk T, Marimo C, Ndiaye C, Alfven T. Management of noma: practice competence and knowledge among healthcare workers in a rural district of Zambia. Glob Health Action. 2017;10(1):1340253. doi:10.1080/16549716.2017.1340253
30. Liang H, Reiss MJ, Isaacs T. Factors affecting physicians’ attitudes towards patient-centred care: a cross-sectional survey in Beijing. BMJ open. 2023;13(4):e073224. doi:10.1136/bmjopen-2023-073224
31. Zhao H, Zhang R, Chen Y. The Influencing Role of Cultural Values on Attitudes of the Chinese Public Towards Traditional Chinese Medicine (TCM) for the Control of COVID-19. Patient Prefer Adherence. 2023;17:3589–3605. doi:10.2147/ppa.s443713
32. Wang HN, Wang JH, Zhao X, et al. What are the Bad Habits and Behaviors of Inconsiderate Doctors in Chinese Inhabitants’ Mind? A Cross-Sectional Study. Risk Manag Healthc Policy. 2022;15:583–595. doi:10.2147/RMHP.S358680
33. Xu C, Zhang H, Yin S. Knowledge, attitudes, and practices among oncologists regarding the implementation of DRGs payment system: a cross-sectional study in Beijing. Original Research. Front Public Health. 2024;12:1453962. doi:10.3389/fpubh.2024.1453962
34. Tie H, Luo Y, Chen D. Thinkings on the reform of medical education system in China. Medl Educ Online. 2024;29(1):2302677. doi:10.1080/10872981.2024.2302677
35. Wang W. Medical education in China: progress in the past 70 years and a vision for the future. BMC Med Educ. 2021;21(1):453. doi:10.1186/s12909-021-02875-6
36. Sun X, Zhang M, Lu Z, et al. Turnover intention and related factors among resident physicians in China under the standardised residency training programme: a cross-sectional survey. BMJ open. 2022;12(4):e061922. doi:10.1136/bmjopen-2022-061922
37. Punnapuzha S, Edemobi PK, Elmoheen A. Febrile Neutropenia. StatPearls. StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC. 2025.
38. Beran TN, Violato C. Structural equation modeling in medical research: a primer. BMC Res Notes. 2010;3(1):267. doi:10.1186/1756-0500-3-267
39. Fan Y, Chen J, Shirkey G. Applications of structural equation modeling (SEM) in ecological studies: an updated review. Ecol Process. 2016;5(1):19. doi:10.1186/s13717-016-0063-3
40. Kline RB. Principles and Practice of Structural Equation Modeling (Fifth Edition). The Guilford Press; 2023.
41. Bergen N, Labonte R. “Everything Is Perfect, and We Have No Problems”: detecting and Limiting Social Desirability Bias in Qualitative Research. Qual Health Res. 2020;30(5):783–792. doi:10.1177/1049732319889354
42. Latkin CA, Edwards C, Davey-Rothwell MA, Tobin KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict Behav. 2017;73:133–136. doi:10.1016/j.addbeh.2017.05.005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.