Back to Journals » Nature and Science of Sleep » Volume 18

Once-Nightly Pregabalin for Co-Occurring Nightmares, Poor Sleep, and Headaches: A Case Series
Authors Bates JH ![]() , Rosin SB, Tobin JA
, Rosin SB, Tobin JA ![]()
Received 1 February 2026
Accepted for publication 19 May 2026
Published 17 July 2026 Volume 2026:18 600495
DOI https://doi.org/10.2147/NSS.S600495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
James H Bates,1 Sophia Brooke Rosin,2 Joshua A Tobin1,3
1University of Arizona College of Medicine – Phoenix, Phoenix, AZ, USA; 2University of Michigan, Ann Arbor, MI, USA; 3Banner - University Medical Center Phoenix, Neurosciences Institute, Phoenix, AZ, USA
Correspondence: Joshua A Tobin, Banner - University Medical Center Phoenix; University of Arizona College of Medicine, Phoenix, AZ, USA, Email [email protected]
Background: Nightmares, nonrestorative sleep, and headaches co-occur, are common, underdiagnosed, and contribute to substantial disability. Pregabalin modulates excitatory neurotransmission, increases slow-wave sleep, and suppresses REM sleep, suggesting a potential therapeutic role in nightmares and sleep disturbance. Pregabalin’s effect on nightmares has not been systematically studied. Although sedation is a common side effect when prescribed 2– 3 times daily according to the package insert, the efficacy and tolerability of once-nightly administration remain poorly characterized.
Methods: Our retrospective case series included 23 outpatients seen in the neurology department of a tertiary care center from November 2022 to August 2025. They were prescribed once-nightly pregabalin for nightmares, nonrestorative sleep, and headaches. Clinical data were extracted from medical records, including nightmare frequency, fraction of 24-hour periods with restorative sleep, headache frequency, severity, and duration, and MIDAS scores. Within-subject pre–post comparisons were performed using paired t-tests or Wilcoxon signed-rank tests. All p-values were Holm–Bonferroni adjusted.
Results: Nightmare frequency decreased 81% (17.5 to 3.3/month, padj=0.006). Nightmares decreased numerically more for those who transitioned from gabapentin to pregabalin (91%) than for those not initially taking gabapentin (73%). Restorative sleep frequency increased 127% (1.8 to 4.0/week, padj=0.006). Headache frequency decreased 50% (17.0 to 8.5/month, padj=0.040). Migraine Disability Assessment Questionnaire scores decreased numerically by 34% (38.0 to 24.0) but did not reach statistical significance after correction (padj=0.084). Six patients reported side effects, and 19 continued pregabalin at three months.
Conclusion: Once-nightly pregabalin was associated with robust reductions in nightmare frequency, nonrestorative sleep, and headache frequency. The improvement in nightmares validates two prior case reports through systematic cohort evaluation. Nightmares improved even among patients transitioning from gabapentin to pregabalin, suggesting that pregabalin may be superior to gabapentin. No prior studies have addressed these three co-occurring problems simultaneously. Larger controlled studies are needed to test the hypothesis that once-nightly pregabalin may be useful for this patient population.
Keywords: pregabalin, nightmare, sleep, poor sleep, headache, case series
Introduction
Nightmares, Nonrestorative Sleep, and Headaches
Nightmares are a significant and underrecognized medical problem. Nightmare disorder affects about 4% of adults and can significantly impair quality of life.1 However, nightmares are underdiagnosed and underreported in clinical practice, even among patients with significant sleep complaints.2 Insomnia and nightmares are associated and may be mutually causal.3 Compared to healthy controls, subjects with frequent nightmares have increased nocturnal awakenings, reduced sleep efficiency, increased wakefulness, decreased slow-wave sleep (SWS), increased rapid eye movement (REM) sleep, and increased depressive and anxious symptomology.4 Frequent nightmares are associated with poor sleep quality and impaired daytime functioning, possibly due to increased sympathetic nervous system activation during nightmares.5
Current treatments for nightmare disorder are limited by incomplete efficacy. For example, prazosin, one of the most used pharmacologic treatments for trauma-related nightmares, failed to demonstrate efficacy in reducing nightmare frequency or improving sleep quality in a large randomized controlled trial of veterans with PTSD.6 This finding highlights the need for additional therapeutic options for patients with persistent nightmares.
Nonrestorative sleep (NRS), defined as unrefreshing sleep despite sufficient duration, affects approximately 11% of adults and is associated with fatigue, impaired daytime physical, cognitive, and emotional functioning, poorer health outcomes, and increased healthcare utilization.7,8 Roth et al9 found that NRS may occur without other insomnia symptoms and that individuals with NRS alone can experience daytime impairments as severe as those with sleep-onset or sleep-maintenance difficulties.
Headache disorders, particularly migraines and tension-type headaches, represent a significant global health burden, affecting nearly three billion people in 2016.10 Migraines are also associated with substantial socioeconomic challenges, disproportionately affecting those in their prime working and child-rearing years, and disproportionately affecting the unemployed and those with a family income of less than $35,000.11
The relationship among nightmares, poor sleep, and headaches is best understood as bidirectional and interdependent rather than unidirectional. Sleep disturbances are among the most common triggers for both migraine and other primary headaches.12 Poor sleep quality and other related factors have been associated with a higher likelihood of migraine attack the next day.13 Some coping strategies, such as going to bed early to relieve symptoms, may actually worsen sleep patterns. Chronic migraine, tension-type headache, and medication overuse headache are all associated with sleep disturbances. Sleep disruptions, including both insufficient and excessive sleep, often trigger tension-type headache. This bidirectional relationship creates a cycle in which poor sleep exacerbates headaches, which further impairs sleep.14 Poor sleep quality, along with unhelpful sleep beliefs and behaviors, is significantly associated with increased headache frequency and disability.15
Hence, nightmares contribute to poor sleep, and poor sleep contributes to headaches. Logically, nightmares may therefore contribute to headaches, and, in a community study, patients with migraine were 4.3 times more likely to report persistent nightmares of childhood onset compared to healthy first-degree relatives.16 In adolescents, nightmare frequency correlated positively with unadjusted headache prevalence, before adjustment for confounders.17 Gazerani noted that nightmares can trigger migraine and that both disorders are comorbid with depression, anxiety, and insomnia.18
The prevalence of nightmares in patients with insomnia was reported at 18%, and patients with concurrent headache and sleep problems have similarly been estimated at 18%.19,20 While the exact prevalence of the triad of nightmares, NRS, and headaches has not been specifically assessed, even assuming no selective co-localization of nightmares with headaches, the prevalence of this triad may be 3%, meaning that this triad may be common and underrecognized. To our knowledge, no study has specifically evaluated patients simultaneously affected by all three conditions.
Pregabalin
Pregabalin is a gabapentinoid, originally developed for diabetic peripheral polyneuropathy, that binds presynaptic voltage-gated calcium channels at the α2δ1 subunit, reducing release of excitatory neurotransmitters including glutamate, norepinephrine, and substance P.21 It decreases sleep latency and awakenings, increases SWS, and decreases REM sleep.22 It may also reduce central sensitization, a key factor in chronic headache disorders.23
Pregabalin improved sleep quality in multiple populations, including patients with fibromyalgia,24 neuropathic pain,25 generalized anxiety disorder (GAD),26 and localization-related epilepsy.27 Pregabalin has also demonstrated benefit in several headache conditions including post–dural puncture headaches,28,29 cervicogenic headache,30 migraine,31 and chronic migraine.32 Hence, data support the use of pregabalin both for headaches of various types and for poor sleep.
However, pregabalin has not been systematically studied as a treatment for nightmares, nor for NRS in patients with nightmares, nor for headaches in patients with nightmares. Notably, most dreaming as well as most nightmares occur in REM sleep, and pregabalin’s effect of increasing SWS and decreasing REM is the opposite of those seen in patients with frequent nightmares.33
Also receiving little discussion in the literature is the timing of pregabalin administration. The package insert specifies that it should be administered 2 or 3 times daily. Somnolence is a common side effect, but its half-life of 6 hours suggests the solution of once daily dosing before bed,34 a strategy that may be especially effective for addressing problems that occur at night, such as nightmares and NRS. Finally, chronic pain patient surveys suggest that once-daily dosing improves adherence as well as sleep.35–37
Herein, we present a case series of patients, each with the triad of nightmares, NRS, and headaches, for whom these three problems improved with pregabalin, dosed once daily about one hour before bed.
Methods
Study Design and Setting
This retrospective case series was conducted at Banner – University Medical Center Phoenix, a tertiary care academic medical center. Patients were identified from the outpatient clinical practice of a neurologist, Dr. Joshua Tobin, between November 2022 and August 2025. Consecutive patients who met inclusion criteria during this time period were included.
PICO Framework
This study was structured according to the PICO framework:
- Population (P): Adults with clinically significant nightmares, nonrestorative sleep, and headaches managed in a neurology outpatient setting
- Intervention (I): Pregabalin administered once nightly with dose titration
- Comparison (C): Pre-treatment baseline (within-subject control)
- Outcomes (O): Nightmare frequency, nonrestorative sleep frequency, headache frequency, headache severity and duration, and MIDAS score
Patient Selection and Inclusion Criteria
Patients were included if they had significant nightmares, NRS, and headaches, received pregabalin, and provided written informed consent. They took pregabalin once daily, one hour before bed. Patients were instructed to start at 75 mg and increase as tolerated in 75 mg weekly intervals until sleep was restorative, generally to a maximum of 300 mg. Response or lack of response to pregabalin was not an inclusion or exclusion criterion.
Clinical Data Collection and Outcome Measures
Clinical data were collected retrospectively and included patient-reported pre- and post-treatment nightmare frequency, restorative sleep frequency, headache characteristics (frequency, severity, duration), and Migraine Disability Assessment Questionnaire (MIDAS) score. Nightmare frequency was defined as the patient-reported number of nightmares per month. Nonrestorative sleep was quantified by its opposite, the number of nights per week with restorative (refreshing) sleep. Headache frequency was defined as the number of headache days per month, while severity and duration were based on patient-reported descriptions documented in the medical record. All outcomes were collected as part of routine clinical care and recorded in the electronic medical record.
These patient-reported clinical measures documented during routine care were used to maximize sample inclusion and reflect real-world practice. Analyses were performed using available data for each outcome (complete-case analysis). A patient datum was included for a given outcome measure only when both a pre-intervention and post-intervention datum for that outcome measure was available. While subjective, these measures are commonly used in clinical decision-making and allowed for within-subject pre–post comparisons.
Pre-treatment metrics were always reported by the patients before starting pregabalin and post-treatment metrics were recorded after 3 months of stable dosing on pregabalin. Pre- and post-treatment metrics were compared to assess treatment response. All identifiable patient data were anonymized.
Statistical Analysis
Normality of pre-post differences were assessed using the Shapiro–Wilk test. Paired t-tests were used for normally distributed outcomes (nightmare frequency, NRS frequency, headache frequency, headache severity, and headache duration). A nonparametric Wilcoxon signed-rank test was applied to the MIDAS scores due to their non-normal distribution. Standardized effect sizes were reported as Hedges’ g to account for small sample bias. Portions of the statistical analysis were assisted by the Julius AI tool. We used Holm-Bonferroni p-values to account for multiple outcome measures. The authors manually reviewed and validated all results.
Results
Clinical and demographic characteristics of all 23 patients, including comorbidities, pregabalin dosing, reported side effects, and whether they were initially on gabapentin prior to pregabalin treatment, are summarized in Table 1. The median age was 45 years (range 18–64), and 21 (91%) were female. The headache diagnosis in 22 (96%) of the 23 patients was migraine, supporting the use of MIDAS scores for headache-related disability assessment. Patient 9 had new daily persistent headache.
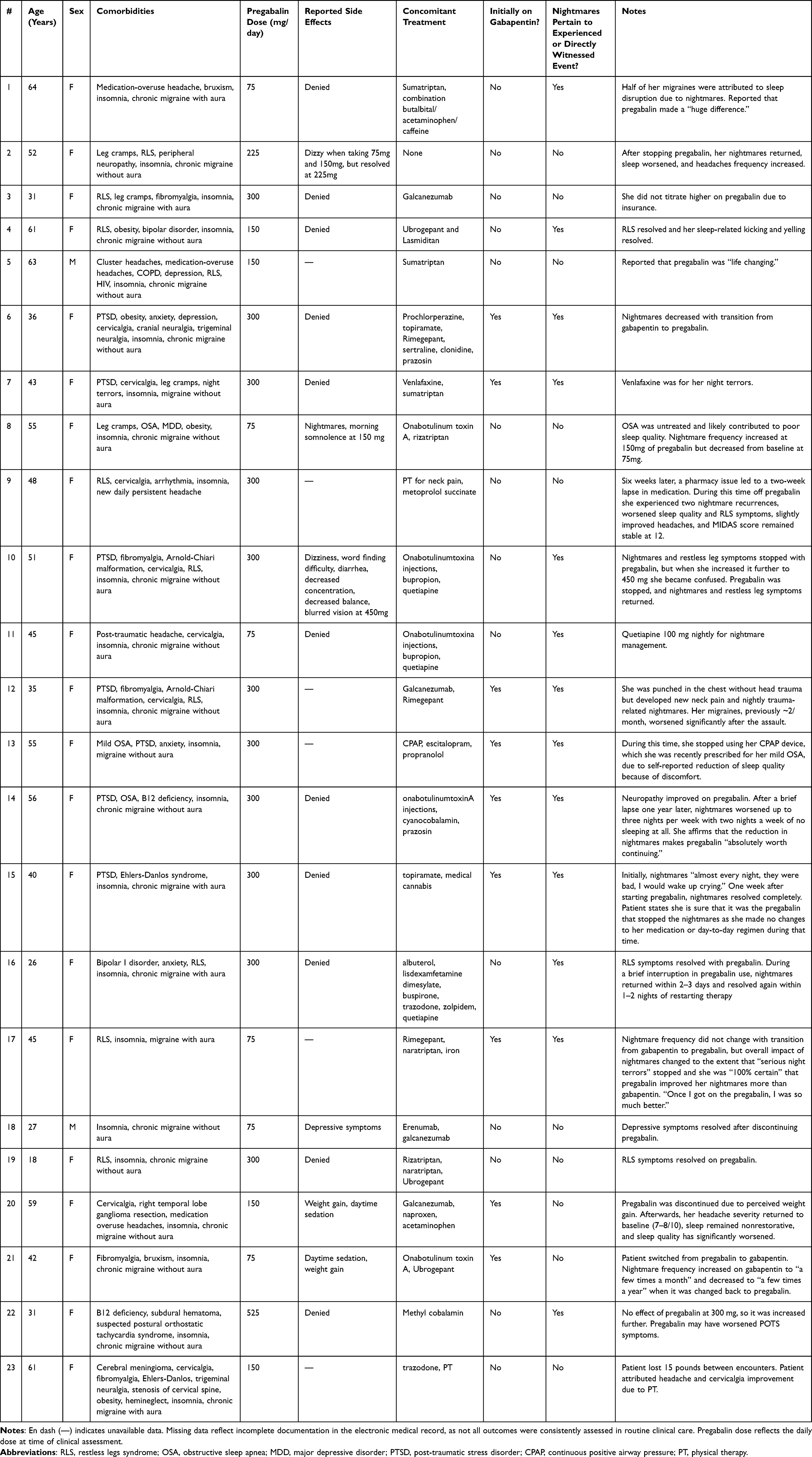 |
Table 1 Clinical and Demographic Characteristics of Patients |
We assessed six patient-reported outcomes: nightmare frequency, restorative sleep frequency, headache frequency, headache severity, headache duration, and headache-related disability.
Table 2 summarizes these outcome measures before and after treatment with pregabalin, and Table 3 summarizes the corresponding statistical analyses.
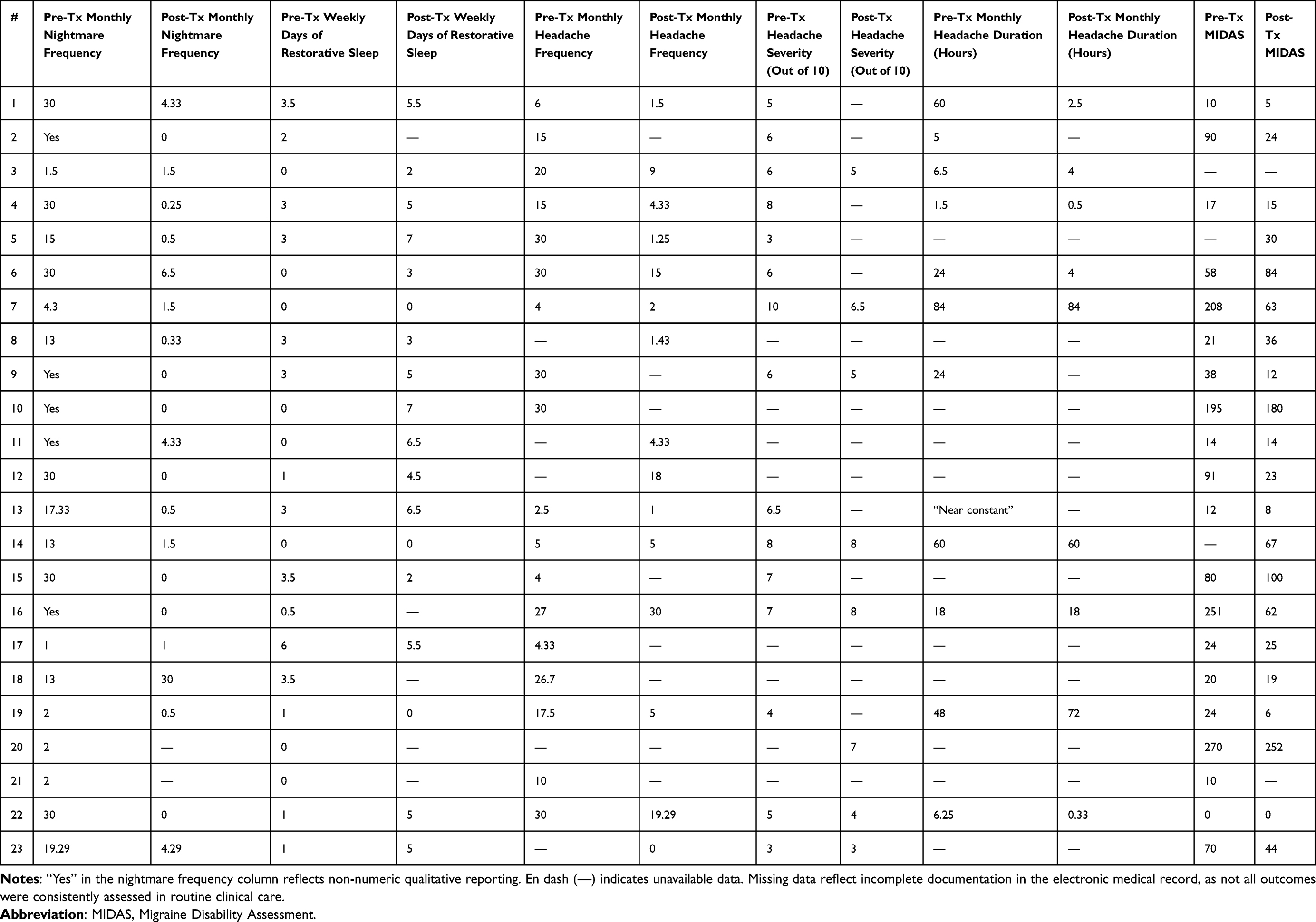 |
Table 2 Clinical Outcomes Before and After Pregabalin Treatment |
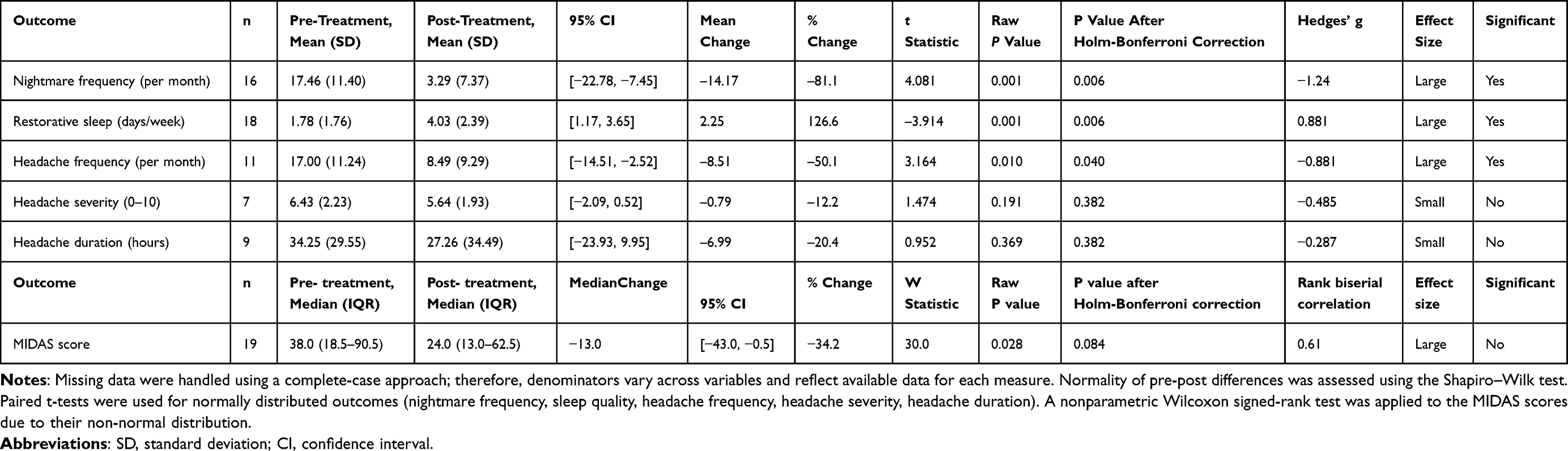 |
Table 3 Statistical Summary of Clinical Outcomes Before and After Pregabalin Treatment |
Nightmare frequency significantly decreased from a mean of 17.5 episodes/month at baseline to 3.3 episodes/month after treatment ([95% CI −22.78, −7.45], t(15) = 4.08, p = 0.001, padj=0.006, Hedges’ g = −1.24, large effect), an 81% reduction. Among 7 transitioning from gabapentin to pregabalin, nightmare frequency decreased 91% (16.4 fewer nightmares/month), vs. 73% for those not initially on gabapentin (12.5 fewer nightmares/month).
The number of nights per week with restorative sleep significantly increased from 1.8 to 4.0 (p =0.001, padj=0.006, g=0.881, large effect), a 127% improvement. Headache frequency decreased by 50%, from 17.0 to 8.5 headaches per month (p=0.010, padj=0.040, g=−0.881, large effect). The decreases in headache severity and duration were not statistically significant.
Migraine-related disability improved, though significantly only before correction (p = 0.028, padj=0.084), with median MIDAS scores decreasing from 38.0 (IQR 18.5–90.5) to 24.0 (IQR 13.0–62.5), a 34% reduction in burden and reflecting a large effect size (rank-biserial correlation = 0.61).
Among the 17 patients with side effect data, 11 (65%) reported no side effects. Reported adverse effects included daytime somnolence, dizziness, weight gain, cognitive slowing, and mood changes. Most adverse effects were mild and transient. At three months, 19 of 23 patients (83%) elected to continue pregabalin therapy.
Discussion
Nightmares
Two prior case reports describe nightmare reduction with pregabalin, both in patients with post-traumatic stress disorder.38,39 This case series is the first to systematically explore the use of pregabalin for nightmares across a cohort of patients. Pregabalin use was associated with a conspicuous reduction in nightmare frequency, with significant improvements in NRS and headache frequency, all of which demonstrated large effect sizes. There are four mechanisms whereby pregabalin could improve NRS: nightmare reduction, reduction of pain interference in sleep, its side effect of somnolence, and SWS increase. Ours is the first case series describing pregabalin’s effect on nightmares.
Prior studies support the use of pregabalin for sleep disturbance and, independently, for certain headache disorders. However, no previous study has demonstrated its simultaneous effectiveness across all three domains of nightmares, sleep disturbance, and headaches.22,30 This distinction is clinically important given the potentially high prevalence and under-recognition of this triad and suggests that pregabalin may offer a convenient therapeutic strategy for patients with this triad.
The hypothesis that nightmares cause headaches via sleep disruption is consistent with patient #1’s attribution of half her migraines to sleep disruption due to nightmares.
Patient Perspective
Multiple patient comments reflected pregabalin’s significant positive impact on their quality of life, including patient #1’s observation that pregabalin made a “huge difference,” patient #5’s characterization of pregabalin as “life changing,” patient #14 noting that pregabalin was “absolutely worth continuing,” and patient #15’s certainty that pregabalin was responsible for the complete cessation of her nightmares which were previously “almost every night, they were bad, I would wake up crying.”
Pregabalin vs. Gabapentin: A Potential Change to the American Academy of Sleep Medicine’s Position Paper for the Treatment of Nightmare Disorder in Adults?
The American Academy of Sleep Medicine (AASM) states that gabapentin “may be used for PTSD associated nightmares” based on a retrospective case series in veterans.1 However, nightmare frequency decreased 91% in those who transitioned from gabapentin to pregabalin, compared to 73% for patients not initially on gabapentin, suggesting not only potential superior efficacy of pregabalin over gabapentin for nightmare reduction but actually raising a preliminary question of whether gabapentin increases nightmares. Indeed, patient #17 stated she was “100% certain” that pregabalin improved her nightmares more than gabapentin, noting “I was so much better,” and patient #21’s nightmares increased while she was taking gabapentin and decreased when she stopped it. While these two drugs are structurally and mechanistically similar,21 gabapentin increases REM,40 whereas pregabalin decreases REM, a potential explanation for their difference in effect on nightmares.
Nightmares also improved more in patients who reported that the nightmares pertained to experienced or directly witnessed events (93% vs. 42%), possibly because more of them were taking gabapentin (7/13 or 54%) than those whose nightmares did not pertain to experienced or directly witnessed events (2/10 or 20%).
NRS
Restorative sleep increased less in those transitioning from gabapentin (59%) than in those not initially taking gabapentin (176%), but nonetheless improved, which suggests that while gabapentin does improve sleep quality, pregabalin improves it more in patients with nightmares.
Interestingly, gabapentin’s effect of improving sleep despite potentially worsening nightmares provides a possible explanation for the AASM’s inclusion of gabapentin as an option for PTSD associated nightmares. The single retrospective study upon which this conclusion was based used the Clinical Global Impressions scale to evaluate the combined effect of gabapentin on both insomnia and/or nightmares.1 In other words, gabapentin’s effect on nightmares was not specifically evaluated, but rather nightmares were lumped together with insomnia with a single outcome measure. In contrast, our study assessed nightmares separately.
Treatments for Nightmares - Prior Literature
Skeie-Larsen et al conducted a systematic review and meta-analysis of placebo-controlled, randomized clinical trials of medications for nightmares. Positive effect sizes in this analysis reflect reductions in nightmare distress, intensity, or frequency. The synthetic cannabinoid nabilone yielded the largest effect size (Hedges’ g = 1.86), followed by the antihistamine hydroxyzine (g = 1.17) and alpha-1 antagonist prazosin (g = 0.54). Three agents showed no significant effect: clonazepam (g = –0.11), cyproheptadine (g = –0.35), and doxazosin (g = –0.04).41
Zhang et al performed a network meta-analysis evaluating both pharmacological and psychotherapeutic treatments for trauma-related nightmares. Only image rehearsal therapy (IRT; SMD = –0.62) and prazosin (SMD = –1.02) demonstrated significant benefit compared with controls; other interventions—including hydroxyzine, nabilone, risperidone, paroxetine, CBTI, combinations such as CBTI + IRT or IRT + PE, prolonged exposure (PE), CPT, and others—did not differ significantly from control conditions.42
Taken together, these conclusions reflect the need for additional effective treatments for nightmares.
Once-Nightly Dosing
Except for one above case report,38 ours is the first study to explicitly describe pregabalin administered once nightly rather than the more commonly prescribed two- or three-times-daily dosing regimen for nightmares, or for NRS, or for headaches. For other disorders, one study compared once-nightly vs. twice-daily pregabalin for fibromyalgia, showing no significant outcome differences.43 For restless legs syndrome, one study of nightly pregabalin showed efficacy,44 and another did not.45 Given pregabalin’s relatively short half-life and the high prevalence of somnolence as an adverse effect, once-nightly dosing may be particularly advantageous for conditions that manifest primarily at night such as nightmares and nonrestorative sleep, while potentially improving tolerability and adherence.34
Pregabalin was generally well tolerated in this cohort, with most adverse effects being mild and not leading to discontinuation. The observed side effect profile is consistent with prior studies, in which somnolence, weight gain, and dizziness are among the most reported adverse effects.34 However, significant psychological side effects have been reported,46 and in this series, patient #18 stopped pregabalin due to depressive symptoms. The retrospective design and incomplete side effect documentation limit our ability to fully characterize pregabalin’s safety profile in our population.
Headache Outcome Measures
Headache frequency also significantly improved overall, with a 50% reduction in monthly episodes, consistent with pregabalin’s proven efficacy in neuropathic pain and other headache disorders.
Migraine-related disability decreased, albeit nonsignificantly after Holm-Bonferroni correction. Headache characteristics and MIDAS score changes were clinically comparable in those transitioning from gabapentin as in those not initially taking gabapentin, consistent with the hypothesis that gabapentin does not affect headaches in patients with nightmares.
Our numerical reductions in headache severity and duration did not reach statistical significance, possibly reflecting smaller sample sizes available for these measures. Also, 22 of the 23 patients were receiving concomitant therapies for headache management, potentially confounding results, and a limitation of this study. Prospective, larger studies with longer follow-up are warranted to further evaluate these metrics.
Strengths and Limitations
This study has several strengths. All patients with the above triad who received pregabalin were offered inclusion, as opposed to just those who responded well. Pre-treatment metrics were collected prior to starting pregabalin, reducing the risk of recall bias. We used within-subject comparisons and evaluated multiple clinically relevant domains. Several clinically related outcomes including nightmare, restorative sleep, and headache frequency each demonstrated highly statistically significant improvement even after adjustment for multiple comparisons, with moderate-to-large effect sizes. Additionally, diagnostic assessment always included a complete history and physical; the major diagnostic challenge was our documentation of inherently subjective symptoms for which there is no diagnostic exam technique or test.
Limitations include the retrospective design and lack of a control group, raising the potential for statistical flaws such as the placebo effect and regression to the mean. However, were the latter actually a factor, we would not have expected subsequent cessation of pregabalin to result in symptoms worsening in multiple patients. For example, nightmares stopped completely with pregabalin for patients #2, #9, #10, and #16, but then returned when it was stopped, at which time patient #2 also reported worsening of her NRS and headache frequency; patient #9 experienced two nightmares along with worsened sleep quality during a two week lapse in pregabalin, patient #10 noted return of nightmares which were “kind of bad” as well as return of restless legs symptoms, and patient #16 noted return of nightmares within 2–3 days of stopping pregabalin and resolution again within 1–2 nights of restarting it. In addition, patient #14’s nightmares decreased from 13 to 1.5 per month on pregabalin, but when it was stopped one year later her nightmares increased up to 3 nights per week with 2 nights a week of not sleeping at all, and her comment at the time was that the pregabalin was “absolutely worth continuing.” In addition, when patient #20 stopped pregabalin, her headache severity returned to baseline and subjective sleep quality worsened.
A key limitation is the potential confounding effect of concomitant therapies. 22 out of the 23 patients were receiving additional treatments for headache, sleep disturbance, and psychiatric comorbidities, including preventive and abortive headache medications, sleep aids, and psychotropic agents. These co-interventions were not standardized and may have been initiated, discontinued, or dose-adjusted during the study period. As such, the observed improvements cannot be definitively attributed to pregabalin alone. Concomitant therapies may have led to an overestimation of pregabalin’s effect if they contributed independently to symptom improvement, or conversely, may have obscured its effect in patients with treatment-refractory symptoms. Additionally, the absence of temporal separation between interventions limits the ability to determine causality or isolate treatment effects. Future prospective studies should control for or stratify by concurrent therapies to better define pregabalin’s independent contribution.
Small sample sizes limit generalizability and statistical power. The cohort was predominantly female (91%), which may limit applicability to males. Of the two male participants, one 63-year-old patient reported marked benefit from pregabalin, whereas the 27-year-old patient discontinued treatment due to worsening depressive symptoms, underscoring potential sex- and age-related differences in tolerability and response that warrant further study. Given the small sample size, multivariable analyses were not performed, as the study was underpowered to reliably estimate independent predictor effects.
Additionally, datasets were incomplete, which may introduce bias. Of the 9 patients who transitioned from gabapentin to pregabalin, 2 did not have both pre- and post-pregabalin treatment nightmare frequency. For example, neither pre- nor post-treatment nightmare frequency was specifically documented for patient #21, though she verbally reported that her nightmare frequency increased on gabapentin and decreased when she stopped it.
Our patients’ heterogeneity, comorbidities and concomitant treatments are confounding factors. For example, 7 (29%) had PTSD, 11 (46%) patients had RLS, and 5 (21%) had fibromyalgia. Pregabalin is effective for the latter two conditions, meaning pregabalin could have improved their sleep via improvement in these conditions rather than via improvement in nightmares. That said, another perspective is that these comorbidities and concomitant treatments also make this study “real world,” and, that nightmares consistently improved across this spectrum suggests that pregabalin’s effect on this outcome measure might be broad. Future studies might focus on more uniform populations, such as PTSD related nightmares only, to see if response differs.
Taken together, these limitations mean that our data should be viewed as hypothesis generating pilot data, rather than producing definitive conclusions about pregabalin’s utility in this patient population. We do not advocate widespread off-label use of pregabalin for nightmares, or for the triad of nightmares, NRS, and headaches unless larger controlled studies confirm our preliminary observations. Despite these limitations, our case series provides preliminary evidence that pregabalin may offer a multifaceted benefit for patients with nightmares, NRS, and headaches, a potentially common and underrecognized triad.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This case series was reviewed by the Institutional Review Board of Banner University Medical Center and deemed exempt due to its retrospective nature. Written informed consent for inclusion and publication of de-identified clinical information was obtained from all patients whose data are reported. This study adheres to the Declaration of Helsinki.
Acknowledgments
The authors thank the patients whose clinical data contributed to this study.
Author Contributions
All authors meet the ICMJE authorship guidelines. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
JB: data curation, formal analysis, and visualization, writing – original draft, writing – review and editing.
SR: investigation, project administration, methodology, formal analysis, conceptualization, writing – original draft, writing – review and editing.
JT: conceptualization, methodology, project administration, validation, and supervision, writing – original draft, writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they have no competing interests relating to this work.
References
1. Morgenthaler TI, Auerbach S, Casey KR, et al; American Academy of Sleep Medicine. Position paper for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2018;14(6):1041–14. doi:10.5664/jcsm.7178
2. Nadorff MR, Nadorff DK, Germain A. Nightmares: under-reported, undetected, and therefore untreated. J Clin Sleep Med. 2015;11(7):747–750. doi:10.5664/jcsm.4850
3. Delage JP, Côté J, Journault WG, Lemyre A, Bastien CH. The relationships between insomnia, nightmares, and dreams: a systematic review. Sleep Med Rev. 2024;75:101931. doi:10.1016/j.smrv.2024.101931
4. Simor P, Horváth K, Gombos F, Takács KP, Bódizs R. Disturbed dreaming and sleep quality: altered sleep architecture in subjects with frequent nightmares. Eur Arch Psychiatry Clin Neurosci. 2012;262(8):687–696. doi:10.1007/s00406-012-0318-7
5. Paul F, Alpers GW, Reinhard I, Schredl M. Nightmares do result in psychophysiological arousal: a multimeasure ambulatory assessment study. Sleep. 2019;42(2):zsy229. doi:10.1093/sleep/zsy229
6. Raskind MA, Peskind ER, Chow B, et al. Trial of prazosin for post-traumatic stress disorder in military veterans. N Engl J Med. 2018;378(6):507–517. doi:10.1056/NEJMoa1507598
7. Ohayon MM. Prevalence and correlates of nonrestorative sleep complaints. Arch Intern Med. 2005;165(1):35–41. doi:10.1001/archinte.165.1.35
8. Takano Y, Ibata R, Machida N, Okajima I. Nonrestorative sleep and its association with insomnia severity, sleep debt, and social jetlag in adults. Nat Sci Sleep. 2022;14:1961–1971. doi:10.2147/NSS.S377010
9. Roth T, Zammit G, Lankford A, et al. Nonrestorative sleep as a distinct component of insomnia. Sleep. 2010;33(4):449–458. doi:10.1093/sleep/33.4.449
10. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
11. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States. Headache. 2018;58(4):496–505. doi:10.1111/head.13281
12. Pellegrino ABW, Davis-Martin RE, Houle TT, Turner DP, Smitherman TA. Perceived triggers of primary headache disorders: a meta-analysis. Cephalalgia. 2018;38(6):1188–1198. doi:10.1177/0333102417727535
13. Seng EK, Martin PR, Houle TT. Lifestyle factors and migraine. Lancet Neurol. 2022;21(10):911–921. doi:10.1016/S1474-4422(22)00211-3
14. Ferini-Strambi L, Galbiati A, Combi R. Sleep disorder-related headaches. Neurol Sci. 2019;40(Suppl 1):107–113. doi:10.1007/s10072-019-03817-9
15. Sullivan DP, Martin PR, Boschen MJ, Bandarian-Balooch S. Dysfunctional sleep beliefs and behaviours: psychological factors in sleep-related headaches. J Behav Med. 2019;42(1):132–140. doi:10.1007/s10865-018-9978-0
16. Vgontzas A, Cui L, Merikangas KR. Are sleep difficulties associated with migraine attributable to anxiety and depression? Headache. 2008;48(10):1451–1459. doi:10.1111/j.1526-4610.2008.01175.x
17. Bierhals IO, de Oliveira GSP, Santos IS, et al. Relationship between sleep problems and headaches among adolescents: pelotas 2004 Birth cohort. Sleep Med X. 2023;6:100079. doi:10.1016/j.sleepx.2023.100079
18. Gazerani P. Nightmares in migraine: a focused review. Behav Sci. 2021;11(9):122. doi:10.3390/bs11090122
19. Ohayon MM, Morselli PL, Guilleminault C. Prevalence of nightmares and their relationship to psychopathology and daytime functioning in insomnia subjects. Sleep. 1997;20(5):340–348. doi:10.1093/sleep/20.5.340
20. Lund N, Westergaard ML, Barloese M, Glümer C, Jensen RH. Epidemiology of concurrent headache and sleep problems in Denmark. Cephalalgia. 2014;34(10):833–845. doi:10.1177/0333102414543332
21. Sills GJ. The mechanisms of action of gabapentin and pregabalin. Curr Opin Pharmacol. 2006;6(1):108–113. doi:10.1016/j.coph.2005.10.003
22. Hindmarch I, Dawson J, Stanley N. A double-blind study in healthy volunteers to assess the effects on sleep of pregabalin compared with alprazolam and placebo. Sleep. 2005;28(2):187–193. doi:10.1093/sleep/28.2.187
23. Frampton JE. Pregabalin: a review in generalized anxiety disorder. CNS Drugs. 2014;28(9):835–854. doi:10.1007/s40263-014-0180-5
24. Crofford LJ, Mease PJ, Simpson SL, et al. Pregabalin for the treatment of fibromyalgia syndrome: results of a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2005;52(4):1264–1273. doi:10.1002/art.20983
25. Kapustin D, Bhatia A, McParland A. et al. Evaluating the impact of gabapentinoids on sleep health in patients with chronic neuropathic pain: a systematic review and meta-analysis. Pain. 2020;161(3):476–490. doi:10.1097/j.pain.0000000000001743
26. Holsboer-Trachsler E, Prieto R. Effects of pregabalin on sleep in generalized anxiety disorder. Int J Neuropsychopharmacol. 2013;16(4):925–936. doi:10.1017/S1461145712000922
27. Bazil CW, Dave J, Cole J, Stalvey J, Drake E. Pregabalin increases slow-wave sleep and may improve attention in patients with partial epilepsy and insomnia. Epilepsy Behav. 2012;23(4):422–425. doi:10.1016/j.yebeh.2012.02.005
28. Salem DAE, Elnady MM, Alagamy SA, Mowafy SM. Comparative study between the analgesic effect of prednisolone and pregabalin in managing post dural puncture headache after lower limb surgeries. Pain Physician. 2024;27(10):E1045–E1054.
29. Huseyinoglu U, Huseyinoglu N, Hamurtekin E, Aygun H, Sulu B. Effect of pregabalin on post-dural-puncture headache following spinal anesthesia and lumbar puncture. J Clin Neurosci. 2011;18(10):1365–1368. doi:10.1016/j.jocn.2011.02.029
30. Boudreau GP, Marchand L. Pregabalin for the management of cervicogenic headache: a double-blind study. Can J Neurol Sci. 2014;41(5):603–610. doi:10.1017/cjn.2014.2
31. Pizzolato R, Villani V, Prosperini L, Ciuffoli A, Sette G. Efficacy and tolerability of pregabalin as preventive treatment for migraine: a 3-month follow-up study. J Headache Pain. 2011;12(5):521–525. doi:10.1007/s10194-011-0338-0
32. Calandre EP, García-Leiva JM, Rico-Villademoros F, Slim M, Torres LM, Hidalgo J. Pregabalin in the treatment of chronic migraine: an open-label study. Clin Neuropharmacol. 2010;33(1):35–39. doi:10.1097/WNF.0b013e3181bf1dbe
33. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, text rev. American Psychiatric Association Publishing; 2022.
34. Pregabalin. Package insert. Pfizer Laboratories; 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021446s035%2C022488s013lbl.pdf.
35. Müller-Schwefe GH, Wimmer AM, Dejonckheere J, Eggers A, Vellucci R. Patients’ and physicians’ perspectives on opioid therapy for chronic cancer and musculoskeletal pain in Germany, Italy, and Turkey: pAin RESearch (PARES) survey. Curr Med Res Opin. 2014;30(3):339–347. doi:10.1185/03007995.2013.861349
36. Timmerman L, Stronks DL, Groeneweg JG, Huygen FJPM. Prevalence and determinants of medication non-adherence in chronic pain patients: a systematic review. Acta Anaesthesiol Scand. 2016;60(4):416–431. doi:10.1111/aas.12697
37. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. doi:10.1016/S0149-2918(01)80109-0
38. Paslakis G, Gilles M, Deuschle M. Pregabalin in the treatment of posttraumatic stress disorder: a case report. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(4):1160–1161. doi:10.1016/j.pnpbp.2011.02.005
39. Strawn JR, Dowling BP, Geracioti TD. Pregabalin treatment of posttraumatic stress disorder. J Clin Psychopharmacol. 2008;28(5):596–597. doi:10.1097/JCP.0b013e318184c8f2
40. Placidi F, Diomedi M, Scalise A, Marciani MG, Romigi A, Gigli GL. Effect of anticonvulsants on nocturnal sleep in epilepsy. Neurology. 2000;54(5 Suppl 1):S25-32. PMID: 10718681
41. Skeie-Larsen M, Stave R, Grønli J, et al. The effects of pharmacological treatment of nightmares: a systematic literature review and meta analysis of placebo controlled, randomized clinical trials. Int J Environ Res Public Health. 2023;20(1):777. doi:10.3390/ijerph20010777
42. Zhang Y, Ren R, Vitiello MV, et al. Efficacy and acceptability of psychotherapeutic and pharmacological interventions for trauma related nightmares: a systematic review and network meta analysis. Neurosci Biobehav Rev. 2022;139:104717. doi:10.1016/j.neubiorev.2022.104717
43. Nasser K, Kivitz AJ, Maricic MJ, Silver DS, Silverman SL. Twice daily versus once nightly dosing of pregabalin for fibromyalgia: a double-blind randomized clinical trial of efficacy and safety. Arthritis Care Res. 2014;66(2):293–300. doi:10.1002/acr.22111
44. Allen R, Chen C, Soaita A, et al. A randomized, double-blind, 6-week, dose-ranging study of pregabalin in patients with restless legs syndrome. Sleep Med. 2010;11(6):512–519. doi:10.1016/j.sleep.2010.03.003
45. Sunwoo JS, Cho YW, Shin WC, Byun JI, Shin JW, Jung KY. Efficacy and safety of pregabalin for restless legs syndrome in korean adults: a randomized, double-blind, placebo-controlled trial. J Clin Neurol. 2025;21(4):325–331. doi:10.3988/jcn.2025.0092
46. Gudla SS, Bhumireddy SKA, Vadaga AK, Nandula MS. A systematic review of pregabalin: therapeutic benefits, psychological risks, and case reports analysis. Trop Doctor. 2026;56(2):407–414. doi:10.1177/00494755251405379
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Longitudinal Findings on the Oneiric Activity Changes Across the Pandemic
Scarpelli S, Alfonsi V, Camaioni M, Gorgoni M, Albano A, Musetti A, Quattropani MC, Plazzi G, De Gennaro L, Franceschini C
Nature and Science of Sleep 2023, 15:435-447
Published Date: 8 June 2023