Back to Journals » Infection and Drug Resistance » Volume 19
Omadacycline - Associated Anticardiolipin Antibody Positivity and Hypercoagulable State: A Case Report and Review of Tetracycline - Induced Immune Dysregulation
Authors Wang N, Liu Y, Liu Y, Gong J, Ge H, Chen H, Li X
Received 3 December 2025
Accepted for publication 3 February 2026
Published 12 February 2026 Volume 2026:19 583185
DOI https://doi.org/10.2147/IDR.S583185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Na Wang,1,* Yuzhi Liu,2,* Yunting Liu,1 Jilin Gong,1 Haiyan Ge,1 Hefeng Chen,1 Xiangyang Li1
1Department of Pulmonary and Critical Care Medicine, Huadong Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 2Department of Radiation Oncology, Huadong Hospital, Fudan University, Shanghai, 200040, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haiyan Ge, Department of Pulmonary and Critical Care Medicine, Huadong Hospital, Fudan University, 221# West Yan’ an Road, Shanghai, People’s Republic of China, Email [email protected] Hefeng Chen, Department of Pulmonary and Critical Care Medicine, Huadong Hospital, Fudan University, 221# West Yan’ an Road, Shanghai, People’s Republic of China, Email [email protected]
Abstract: We present the case of an 18-year-old previously healthy female diagnosed with Mycoplasma pneumoniae pneumonia who developed marked elevation in D-dimer and fibrinogen degradation products, along with de novo positivity for both IgG and IgM anticardiolipin antibodies, shortly after initiating intravenous omadacycline therapy. These findings occurred in the absence of known antiphospholipid syndrome or other autoimmune conditions. The patient also experienced gastrointestinal symptoms and skin rashes. After discontinuation of omadacycline and supportive care, her condition improved. This case highlights the temporal association between omadacycline administration and the emergence of immune-coagulative dysregulation. Given that Mycoplasma pneumoniae infection itself can cause similar extrapulmonary manifestations, a definitive causal link cannot be established. This case suggests a probable, though rare, association between omadacycline and immune-coagulative dysregulation. Clinicians should be vigilant for such signals, particularly in patients developing early cutaneous or gastrointestinal symptoms during therapy.
Keywords: omadacycline, Mycoplasma pneumoniae pneumonia, anticardiolipin antibody, hypercoagulable state, drug-induced immune response
Introduction
Mycoplasma pneumoniae is a common cause of atypical pneumonia, particularly among adolescents and young adults. It accounts for up to 40% of community-acquired pneumonia cases in this age group.1 Although most cases are self-limiting, a subset of patients develop extrapulmonary manifestations, including neurological, dermatological, and immunological complications.1 Macrolides are traditionally used as first-line agents; however, increasing resistance has led to the adoption of alternative antibiotics such as fluoroquinolones and tetracyclines.2 Omadacycline, a semi-synthetic tetracycline derivative, demonstrates potent activity against respiratory pathogens and is approved for CABP due to its favorable pharmacokinetics and high tissue penetration.3,4 Despite its efficacy and generally favorable safety profile in clinical trials, post-marketing surveillance is essential to identify rare adverse events.5–8 Notably, other tetracyclines have been implicated in immune-mediated phenomena, raising the question of whether omadacycline shares this potential.9,10
We report this case to alert clinicians to this potential adverse effect, systematically review similar events with other tetracyclines, explore possible mechanisms, and provide monitoring recommendations.
Case Presentation
An 18-year-old previously healthy female presented with a one-week history of cough, yellow sputum production, and high-grade fever up to 40°C. She recently returned from overseas and tested weakly positive for SARS-CoV-2 antigen. After seeking medical care, she was prescribed VV116 by a physician, but her symptoms did not improve, prompting her to seek further care at our hospital. Physical examination revealed normal vital signs and symmetric breath sounds bilaterally, without audible rales or wheezes. Laboratory evaluation showed elevated inflammatory markers, normal white blood cell count, and positive IgM antibodies (87.18AU/mL, ref: <20AU/mL) against Mycoplasma pneumoniae. No evidence of bacterial coinfection was found on sputum culture or blood cultures. Chest CT confirmed right middle lobe pneumonia in Figure 1S. On admission, she was diagnosed with non-severe community-acquired pneumonia based on clinical findings and chest CT.
The patient was initiated on intravenous omadacycline 200 mg loading dose followed by 100 mg daily. Within two days, she developed a mild rash on the infusion arm in Table 1S. On Hospital Day (HD) 3 (2025/1/2), she experienced nausea, vomiting, diarrhea and transient syncope. On HD4 (2025/1/3), she had an episode of generalized pruritic rash, prompting discontinuation of omadacycline. The patient was switched to ceftriaxone and azithromycin, but developed recurrent rash after azithromycin administration and was subsequently transitioned to levofloxacin. On HD5 (2025/1/4), laboratory results showed markedly elevated D-dimer (36.15mg/L, ref: <0.5mg/L) and FDP (88.91mg/L, ref: <5mg/L) levels, indicating a hypercoagulable state in Figure 2S. Hematology consultation recommended initiation of enoxaparin. Liver enzymes were also significantly elevated on HD8 (2025/1/7), necessitating hepatoprotective therapy. On HD7 (2025/1/6), laboratory results revealed elevated levels of serum immunoglobulin M (IgM 4.49g/L, ref: <2.8g/L) and immunoglobulin E (IgE 448.4g/L, ref: ≤375IU/mL), along with increased complement component 3 (C3). Autoimmune screening showed de novo positivity for both IgG and IgM anticardiolipin antibodies (IgG: 29.56 GPL/mL, ref: <20 GPL/mL; IgM: 28.15 MPL /mL, ref: <20 MPL/mL), while lupus anticoagulant testing remained negative. Notably, anti-nuclear antibody (ANA) was also positive at a titer of 226 U/mL (ref: <55 U/mL), but further autoantibody testing on the same day, including anti-dsDNA, anti-ribosomal P protein, anti-Scl-70, anti-mitochondrial, anti-PCNA, anti-nucleosome, anti-Jo-1, anti-histone, anti-U1-nRNP, anti-smooth muscle, and anti-centromere antibodies, were all negative. Additionally, tests for anti-glomerular basement membrane antibodies and anti-intrinsic factor antibodies were within normal limits. These findings raise the possibility of drug-induced immune stimulation rather than underlying autoimmunity. As part of routine follow-up, serum Mycoplasma pneumoniae IgM antibody titers (228AU/mL, ref: <20AU/mL) were monitored throughout hospitalization and peaked on HD7 (2025/1/6), consistent with active infection. While M. pneumoniae infection itself can cause extrapulmonary immunological complications, the temporal clustering of these marked coagulation and immune abnormalities shortly after omadacycline initiation was striking.
The final diagnoses included Mycoplasma pneumoniae pneumonia, hypercoagulable state, possible drug-induced antiphospholipid-like syndrome and sinus arrhythmia. After discontinuation of omadacycline and appropriate supportive care, the patient’s condition improved, and she was discharged with plans for outpatient follow-up.
Literature Review
For now, some cases of tetracycline -induced immune activation or coagulation disturbances have been reported, but no systematic reviews have been conducted to summarize the literature. In order to perform a thorough literature review, we searched the literature published in PubMed prior to December 2026 to identify case reports of immune activation or coagulation disturbances associated with tetracyclines. These search terms consist of “omadacycline or tetracycline or doxycycline or minocycline or tigecycline or eravacycline”, “case report” and linked to the logical word “and”. After screening and assessment, a total of 25 eligible articles were included for analysis in Table 1. Our review indicates that among tetracyclines, minocycline is most frequently associated with systemic autoimmune syndromes (eg, lupus, hepatitis), while tigecycline is linked primarily to coagulopathies like hypofibrinogenemia. Reports for doxycycline and omadacycline are scant, making the present case a novel contribution to the safety profile of the latter.
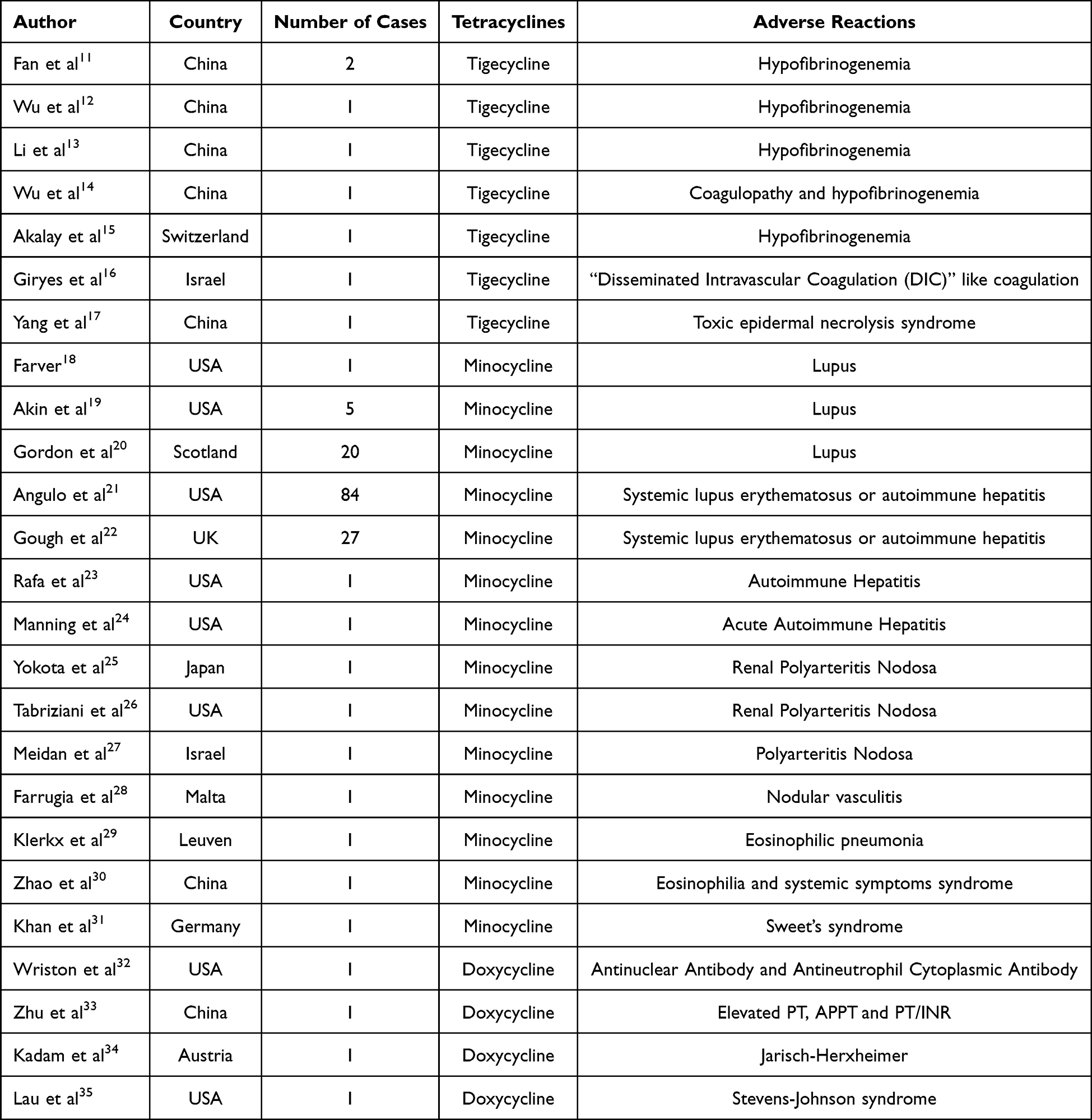 |
Table 1 Different Cases of Immune Activation or Coagulation Disturbances Associated with Tetracyclines Administration |
Discussion
Omadacycline is generally considered safe and effective for CABP. However, post-marketing surveillance and recent case reports have begun to reveal rare but significant adverse effects, including gastrointestinal disturbances, hepatic enzyme elevation, and now possibly immune-coagulative dysregulation.5–8 In this case, the patient developed a dramatic increase in D-dimer and FDP levels shortly after initiating omadacycline. These findings persisted even after discontinuation of the drug, suggesting that omadacycline might trigger a transient procoagulant state. Importantly, no underlying conditions or concurrent medications typically associated with hypercoagulability (eg, estrogen-containing contraceptives, malignancy, inherited thrombophilia) were present. It is crucial to acknowledge that M. pneumoniae infection is strongly associated with hypercoagulability and elevated D-dimer levels. However, in this case, the degree of D-dimer elevation was markedly higher than typically observed in uncomplicated mycoplasma pneumonia, and its rapid decline post-discontinuation suggests an additional drug-induced component. The concurrent emergence of autoimmune markers further supports this possibility.
This case aligns with recent observations in the literature. Xu et al reported a case of acute pancreatitis following omadacycline use, highlighting the need for clinicians to remain vigilant about unexpected side effects.8 Several drugs within the tetracycline class have been implicated in immune-mediated adverse effects. Minocycline, in particular, has been most frequently associated with drug-induced lupus, serum sickness-like reactions, and antiphospholipid syndrome.20,30,36,37 Doxycycline has been described in association with cutaneous hypersensitivity, autoimmune hepatitis, and rarely, hemolytic anemia.38–40 While omadacycline differs structurally from minocycline and doxycycline, it still belongs to the tetracycline family and may possess similar immunomodulatory properties. Our case further expands the spectrum of potential immune-related complications associated with this newer tetracycline derivative.
Potential Mechanisms of Immune Activation and Coagulopathy Associated with Omadacycline
Although the exact pathophysiology underlying omadacycline-associated immune activation and coagulopathy remains incompletely understood, several plausible mechanisms have been proposed in the literature that may help explain the observed clinical phenomena in this case.
One potential pathway is drug-induced molecular mimicry, a process by which certain medications, including antibiotics, may structurally resemble host antigens or phospholipids, thereby triggering an inappropriate immune response that leads to the formation of autoantibodies such as anticardiolipin antibodies.41–43 This phenomenon has been described with various drug classes and could serve as a possible explanation for the de novo appearance of these antibodies during omadacycline therapy. This mechanism may specifically account for our patient’s development of transient IgG and IgM anticardiolipin antibody positivity in the absence of prior autoimmune disease.
Additionally, mitochondrial interference has been increasingly recognized as a mechanism through which tetracycline-class antibiotics may exert immunomodulatory effects. Tetracyclines are known to inhibit mitochondrial protein synthesis, potentially leading to mitochondrial dysfunction and the induction of cellular stress responses. These disturbances may activate innate and adaptive immune pathways, contributing to systemic inflammation and immune dysregulation.44–47 The widespread cellular stress induced by this mechanism could underlie the multi-system hypersensitivity reactions observed in our patient, including the maculopapular rash and gastrointestinal symptoms.
A third potential mechanism involves endothelial activation, which can be induced either by direct drug effects or indirectly via infection-related inflammatory cytokine release. Endothelial cell activation may result in upregulated expression of procoagulant molecules such as tissue factor and von Willebrand factor, both of which play central roles in promoting thrombosis and a hypercoagulable state.48,49 This provides a direct link to the marked elevation in D-dimer and fibrinogen degradation products seen in our patient, reflecting active intravascular coagulation.
Finally, accumulating evidence suggests that certain antibiotics—including those in the tetracycline family—may also trigger complement system activation, a key mediator of both immune and coagulation dysregulation. Complement activation can enhance immune-inflammatory signaling and promote thromboinflammatory processes, further linking drug exposure with the development of abnormal coagulation profiles and immune markers.50–52 The amplification of inflammatory cascades through this pathway may contribute to the concurrent rise in acute-phase reactants (eg, C-reactive protein) and the overall severity of the immune-coagulative dysregulation in this case.
Taken together, these mechanisms provide a theoretical framework for understanding how omadacycline might contribute to immune-mediated adverse events and hypercoagulability, particularly in susceptible individuals. However, given the limited number of reported cases and the complexity of drug-immune-coagulation interactions, further mechanistic studies are warranted to better define the role of omadacycline in such rare but clinically significant complications.
Assessing the Likelihood of Drug-Induced Antiphospholipid Syndrome
Notably, the patient tested positive for both anticardiolipin antibodies IgG and IgM during hospitalization, although no clinical features of antiphospholipid syndrome (APS), such as thrombosis or pregnancy-related complications, were observed.53,54 Given that baseline anticardiolipin antibody status prior to omadacycline initiation was unknown, we describe this as a de novo detection of anticardiolipin antibody positivity, which emerged during treatment. However, due to the lack of follow-up testing after the initial positive result, the persistence or clearance of these antibodies remains undetermined. In the context of drug-induced immune phenomena, a single measurement is insufficient to confirm transient or persistent positivity; therefore, serial monitoring would be necessary in future cases to better characterize the temporal dynamics and clinical relevance of such findings. It is important to consider the possibility of Mycoplasma pneumoniae itself contributing to immune activation and coagulation changes. Mycoplasma pneumoniae infections are well recognized to be associated with extrapulmonary manifestations, including neurological, dermatological, hematologic, and immunological complications.55–57 However, the emergence of hypercoagulability and anticardiolipin antibody positivity occurred during omadacycline therapy, with no prior history of autoimmune disease or known thrombophilic conditions. Although a definitive causal relationship cannot be established due to the lack of baseline and follow-up testing for anticardiolipin antibodies, the temporal association between drug administration and the appearance of these immune and coagulation abnormalities suggests a potential contributory role of omadacycline in triggering immune activation and subsequent coagulation disturbances.
The patient initially developed skin rash and gastrointestinal symptoms, which appeared within the first few days of omadacycline administration. These early adverse events are increasingly recognized as potential harbingers of more complex immune or systemic reactions.58–60 Notably, these reactions were followed by more serious manifestations, including hypercoagulability and immune marker abnormalities, suggesting a progressive pattern of multi-system involvement. Drug-induced immune activation may involve several mechanisms, including T-cell-mediated responses, cytokine release, mitochondrial dysfunction, and the formation of autoantibodies, all of which warrant further investigation to better understand the role of omadacycline in immune-mediated adverse events.
Assessing the Likelihood of Omadacycline-Induced Coagulopathy
To evaluate the likelihood that omadacycline was responsible for the coagulation abnormalities (Table 2), we applied the Naranjo Adverse Drug Reaction Probability Scale.61,62 The Naranjo Adverse Drug Reaction Probability Scale is a widely used tool for evaluating the likelihood of a drug-induced adverse event.61,62 It consists of a structured questionnaire that assesses factors such as temporal relationship, alternative causes, and response to drug discontinuation or specific treatment. A total score ≥9 indicates a “definite” association between the drug and the observed reaction, while scores between 5–8 suggest a “probable” link, and scores ≤4 indicate “possible” or “doubtful” causality. It yielded a score of 6, indicating a probable association between omadacycline administration and the development of coagulative abnormalities in this patient. The score was primarily limited by the absence of a rechallenge and the potential confounding role of the underlying M. pneumoniae infection, which precluded completely ruling out an alternative cause. The clinical and laboratory improvement observed after the discontinuation of omadacycline may be partly attributable to the natural resolution of the underlying M. pneumoniae infection. However, the rapid normalization of the markedly elevated D-dimer and anticardiolipin antibodies provides supportive evidence for a significant contribution from the withdrawal of the suspected agent. This assessment supports the hypothesis that omadacycline may have contributed to the observed hypercoagulable state, although a definitive causal relationship cannot be established due to the lack of rechallenge and potential confounding factors such as Mycoplasma pneumoniae infection.
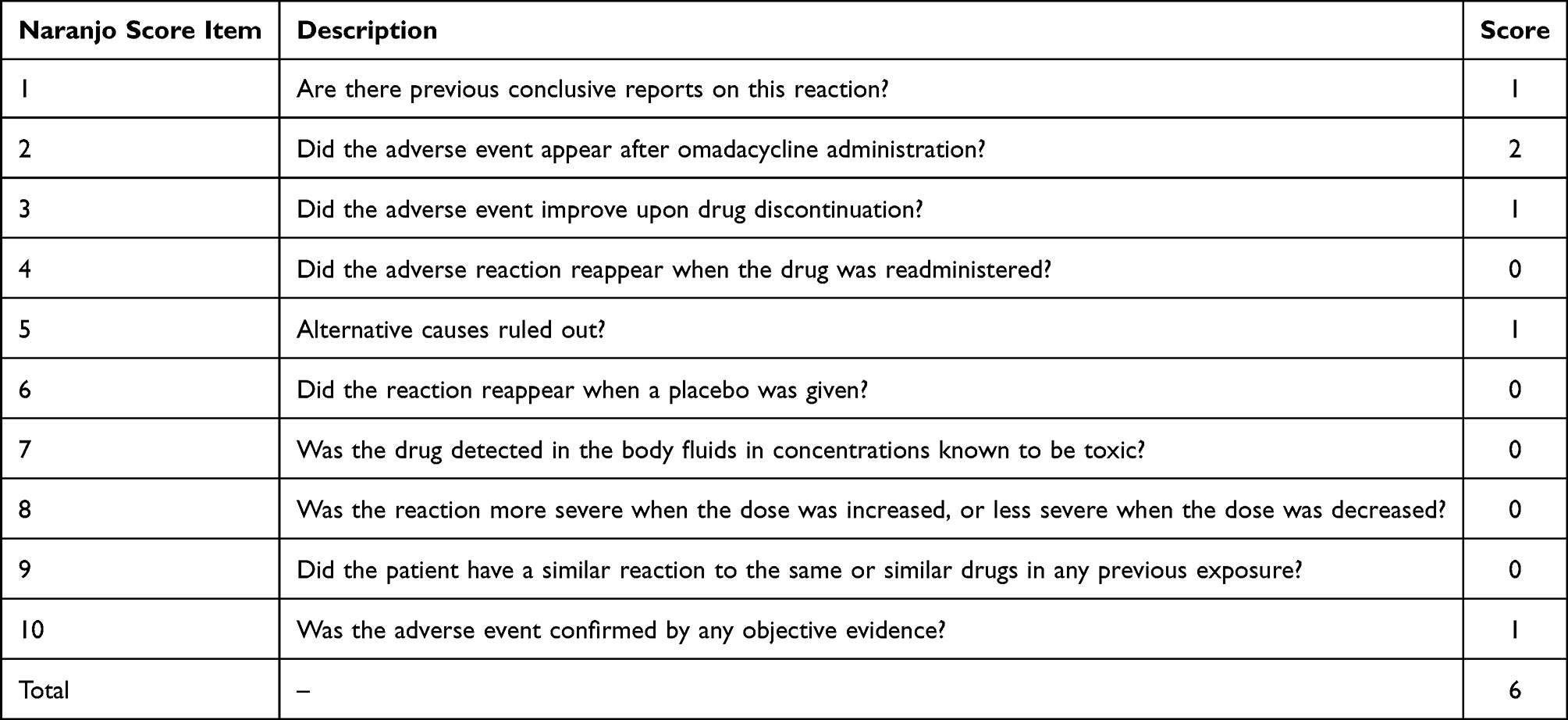 |
Table 2 Naranjo Adverse Drug Reaction Probability Scale Assessment |
Clinical Implications and Monitoring Recommendations
Given the rarity of these events, they are unlikely to be captured in large randomized controlled trials. Therefore, real-world case reports play a crucial role in identifying and understanding such associations. The development of a rash or significant gastrointestinal symptoms within the first few days of omadacycline therapy, as seen in this case, may serve as a clinical harbinger and should prompt consideration of early discontinuation and laboratory evaluation for coagulation or immune abnormalities. Clinicians should consider monitoring coagulation profiles (including D-dimer, fibrinogen, and APTT) and autoimmune markers (such as anticardiolipin antibodies and lupus anticoagulant) in patients receiving omadacycline, especially those with unexplained bleeding, thrombosis, or skin reactions. Particularly in young patients, who may not have established risk factors for thrombosis or autoimmune disease, the development of new-onset coagulation abnormalities or immune markers warrants thorough investigation into medication use and infectious triggers. Although omadacycline appears to be well tolerated overall, this case underscores the importance of maintaining a high index of suspicion for immune and coagulation-related adverse effects in atypical clinical scenarios.
Limitations and Future Research Directions
As with any single-case report, the causal relationship between omadacycline and the development of anticardiolipin antibody positivity and hypercoagulability cannot be definitively established. Confounding factors such as the presence of Mycoplasma pneumoniae infection must also be considered. Moreover, the lack of long-term follow-up data limits our ability to assess the persistence of these abnormalities or their clinical significance over time. Further research is necessary to clarify the mechanisms behind these findings and to determine whether they represent a broader class effect among tetracycline derivatives. Prospective observational studies or registries evaluating the incidence and characteristics of immune and coagulation abnormalities in patients treated with omadacycline would be valuable. In vitro and animal models could also help elucidate the molecular pathways involved.
Conclusion
This case highlights a possible association between omadacycline and immune-coagulative dysregulation, particularly in younger individuals without traditional thrombotic or autoimmune risk factors. Although causality cannot be definitively established, the Naranjo score suggests a probable adverse drug reaction. Clinicians should remain vigilant for unusual immune or coagulation abnormalities during treatment and consider switching to alternative regimens when appropriate.
Data Sharing Statement
Data and materials are provided within the manuscript.
Ethics and Consent Statements
This study was approved by the Clinical Research Ethics Committee of Huadong Hospital, Fudan University (Approval Number: 20250088). As this is a retrospective case report and does not involve patient tissue or blood samples, written informed consent for publication was waived by the ethics committee. However, all personal identifiable information has been anonymized to protect patient privacy. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the signed consent form is available for review by the editor if necessary.
Acknowledgments
Na Wang and Yuzhi Liu are co-first authors for this study. We acknowledge the assistance of Qwen, a large language model developed by Alibaba Cloud, in refining the language and structure of this manuscript. All scientific content, including data analysis and interpretations, remains original and conducted by the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82502755), the Shanghai Pujiang Talent Program (24PJD029), Huadong Hospital Clinical Medical Research Center and Key Discipline Development (ZDXK2216) and Shanghai Innovation Medical Device Application Demonstration Project (23SHS05000 −07).
Disclosure
The authors declare no competing interests in this work.
References
1. Waites KB, Talkington DF. Mycoplasma pneumoniae and its role as a human pathogen. Clin Microbiol Rev. 2004;17(4):697–9. table of contents. doi:10.1128/CMR.17.4.697-728.2004
2. Wang YS, Zhou YL, Bai GN, et al. Expert consensus on the diagnosis and treatment of macrolide-resistant Mycoplasma pneumoniae pneumonia in children. World J Pediatr. 2024;20(9):901–914. doi:10.1007/s12519-024-00831-0
3. Zhanel GG, Esquivel J, Zelenitsky S, et al. Omadacycline: a novel oral and intravenous aminomethylcycline antibiotic agent. Drugs. 2020;80(3):285–313. doi:10.1007/s40265-020-01257-4
4. Waites KB, Crabb DM, Liu Y, Duffy LB. In vitro activities of omadacycline (PTK 0796) and other antimicrobial agents against human mycoplasmas and ureaplasmas. Antimicrob Agents Chemother. 2016;60(12):7502–7504. doi:10.1128/AAC.01734-16
5. Gao W, Yang J, Zhang X, et al. Omadacycline for diverse infections in China: a real-world analysis of efficacy and safety. Infect Dis Ther. 2024;13(12):2509–2526. doi:10.1007/s40121-024-01065-3
6. Opal S, File TM, van der Poll T, Tzanis E, Chitra S, McGovern PC. An integrated safety summary of omadacycline, a novel aminomethylcycline antibiotic. Clin Infect Dis. 2019;69(Suppl 1):S40–s7. doi:10.1093/cid/ciz398
7. Liang W, Yin H, Chen H, Xu J, Cai Y. Efficacy and safety of omadacycline for treating complicated skin and soft tissue infections: a meta-analysis of randomized controlled trials. BMC Infect Dis. 2024;24(1):219. doi:10.1186/s12879-024-09097-3
8. Xu Q, Sang Y, Zhang H, Zhao Q. Possible omadacycline induce acute pancreatitis: a case report and literature review. BMC Infect Dis. 2024;24(1):1072. doi:10.1186/s12879-024-09983-w
9. Gérardin C, Bihan K, Salem JE, et al. Drug-induced antiphospholipid syndrome: analysis of the WHO international database. Autoimmun Rev. 2022;21(5):103060. doi:10.1016/j.autrev.2022.103060
10. Risse J, Vieira M, Beuret F, Petitpain N, Zuily S, Wahl D. Reversible drug-induced antiphospholipid syndrome. Lupus. 2018;27(2):333–335. doi:10.1177/0961203317712463
11. Fan Q, Huang W, Weng Y, Xie X, Shi Z. Hypofibrinogenemia induced by high-dose tigecycline-case report and review of literature. Medicine. 2020;99(43):e22638. doi:10.1097/MD.0000000000022638
12. Wu PC, Wu CC. Tigecycline-associated hypofibrinogenemia: a case report and review of the literature. IDCases. 2018;11:56–57. doi:10.1016/j.idcr.2018.01.003
13. Li ZK, Zheng P. Acute pancreatitis caused by tigecycline and furosemide combination treatment and hypofibrinogenemia caused by tigecycline: a case report. Int J Clin Pharmacol Ther. 2023;61(10):466–470. doi:10.5414/CP204337
14. Wu X, Zhao P, Dong L, Zhang X. A case report of patient with severe acute cholangitis with tigecycline treatment causing coagulopathy and hypofibrinogenemia. Medicine. 2017;96(49):e9124. doi:10.1097/MD.0000000000009124
15. Akalay S, Vanassche T, De Munter P. Tigecycline-induced life-threatening coagulopathy in a patient with a Mycobacterium abscess: a case report and step-by-step diagnostic approach. Acta Clin Belg. 2021;76(5):410–414. doi:10.1080/17843286.2020.1747197
16. Giryes S, Azzam ZS, Ismael-Badarneh R, Krivoy N, Berger G. Severe coagulation disorder and thrombocytopenia associated with tigecycline - case report and review of literature. Curr Drug Saf. 2017;12(1):7–9. doi:10.2174/1574886311666160920090714
17. Yang J, Wu F, Luo D, et al. Toxic epidermal necrolysis syndrome induced by tigecycline: a case report. J Int Med Res. 2020;48(5):300060520922416. doi:10.1177/0300060520922416
18. Farver DK. Minocycline-induced lupus. Ann Pharmacother. 1997;31(10):1160–1163. doi:10.1177/106002809703101009
19. Akin E, Miller LC, Tucker LB. Minocycline-induced lupus in adolescents. Pediatrics. 1998;101(5):926. doi:10.1542/peds.101.5.926
20. Gordon MM, Porter D. Minocycline induced lupus: case series in the West of Scotland. J Rheumatol. 2001;28(5):1004–1006.
21. Angulo JM, Sigal LH, Espinoza LR. Coexistent minocycline-induced systemic lupus erythematosus and autoimmune hepatitis. Semin Arthritis Rheum. 1998;28(3):187–192. doi:10.1016/S0049-0172(98)80035-8
22. Gough A, Chapman S, Wagstaff K, Emery P, Elias E. Minocycline induced autoimmune hepatitis and systemic lupus erythematosus-like syndrome. BMJ. 1996;312(7024):169–172. doi:10.1136/bmj.312.7024.169
23. Rafa O, Basile EJ, Frankini E, Ahmed A. Rapid development of autoimmune hepatitis secondary to minocycline. Cureus. 2022;14(3):e23038. doi:10.7759/cureus.23038
24. Manning DH, DeBuck E, Simchick M. A tale of unequal substitution: minocycline and acute autoimmune hepatitis. J Pharm Technol. 2014;30(2):69–72. doi:10.1177/8755122513520400
25. Yokota K, Kurihara I, Nakamura T, et al. Remission of angiographically confirmed minocycline-induced renal polyarteritis nodosa: a case report and literature review. Intern Med. 2022;61(1):103–110. doi:10.2169/internalmedicine.7340-21
26. Tabriziani H, Wilcox CS, Gilbert ON, Lipkowitz MS. Minocycline-induced renal polyarteritis nodosa. BMJ Case Rep. 2012;2012:bcr2012006503. doi:10.1136/bcr-2012-006503
27. Meidan R, Lahav D, Eshed I, Meridor K, Elkayam O, Elalouf O. Minocycline-induced polyarteritis nodosa manifesting as tenosynovitis, edema, and rash: a case report. Isr Med Assoc J. 2025;27(4):255–257.
28. Farrugia S, Cachia M, Betts A, Clark E. Nodular vasculitis (erythema induratum) associated with systemic minocycline. Australas J Dermatol. 2024;65(2):167–170. doi:10.1111/ajd.14195
29. Klerkx S, Pat K, Wuyts W. Minocycline induced eosinophilic pneumonia: case report and review of literature. Acta Clin Belg. 2009;64(4):349–354. doi:10.1179/acb.2009.056
30. Zhao Z, Lu M, Ying Y. Case Report: minocycline-induced drug reaction with eosinophilia and systemic symptoms syndrome: a case report and literature review. Front Pharmacol. 2024;15:1355774. doi:10.3389/fphar.2024.1355774
31. Khan Durani B, Jappe U. Drug-induced Sweet’s syndrome in acne caused by different tetracyclines: case report and review of the literature. Br J Dermatol. 2002;147(3):558–562. doi:10.1046/j.1365-2133.2002.04817.x
32. Wriston DJ, Norfolk ER, Smith LM, Chen G, Bulbin DH. Doxycycline-induced antinuclear antibody and antineutrophil cytoplasmic antibody associated vasculitis: a case report and literature review. Case Rep Rheumatol. 2020;2020:3853671. doi:10.1155/2020/3853671
33. Zhu XQ, Guo CF, Wen YG, et al. Elevated PT, APPT and PT/INR possibly associated with doxycycline and cefoperazone co-administration: a case report. J Clin Pharm Ther. 2018;43(1):141–144. doi:10.1111/jcpt.12600
34. Kadam P, Gregory NA, Zelger B, Carlson JA. Delayed onset of the Jarisch-Herxheimer reaction in doxycycline-treated disease: a case report and review of its histopathology and implications for pathogenesis. Am J Dermatopathol. 2015;37(6):e68–74. doi:10.1097/DAD.0000000000000093
35. Lau B, Mutyala D, Dhaliwal D. A case report of doxycycline-induced Stevens-Johnson syndrome. Cornea. 2011;30(5):595–597. doi:10.1097/ICO.0b013e3181f05773
36. Geddes MR, Sinnreich M, Chalk C. Minocycline-induced dermatomyositis. Muscle Nerve. 2010;41(4):547–549. doi:10.1002/mus.21487
37. He Y, Sawalha AH. Drug-induced lupus erythematosus: an update on drugs and mechanisms. Curr Opin Rheumatol. 2018;30(5):490–497. doi:10.1097/BOR.0000000000000522
38. Pan JJ, Promrat K. Doxycycline-induced autoimmune hepatitis. ACG Case Rep J. 2020;7(8):e00440. doi:10.14309/crj.0000000000000440
39. Brehon A, Lourenco J, Badaoui A, et al. Doxycycline-induced fixed drug eruption: the new epidemic? J Eur Acad Dermatol Venereol. 2025;39(4):e303–e5. doi:10.1111/jdv.20280
40. Qiao Y, Chen Y, Wang Q, et al. Safety profiles of doxycycline, minocycline, and tigecycline in pediatric patients: a real-world pharmacovigilance analysis based on the FAERS database. Front Pharmacol. 2024;15:1413944. doi:10.3389/fphar.2024.1413944
41. Rojas M, Herrán M, Ramírez-Santana C, et al. Molecular mimicry and autoimmunity in the time of COVID-19. J Autoimmun. 2023;139:103070. doi:10.1016/j.jaut.2023.103070
42. Chen Y, Xu Z, Wang P, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology. 2022;165(4):386–401. doi:10.1111/imm.13443
43. Talotta R. Molecular mimicry and HLA polymorphisms may drive autoimmunity in recipients of the BNT-162b2 mRNA vaccine: a computational analysis. Microorganisms. 2023;11(7):1686. doi:10.3390/microorganisms11071686
44. Mottis A, Li TY, El Alam G, et al. Tetracycline-induced mitohormesis mediates disease tolerance against influenza. J Clin Invest. 2022;132(17). doi:10.1172/JCI151540
45. Shao Q, Khawaja A, Nguyen MD, et al. T cell toxicity induced by tigecycline binding to the mitochondrial ribosome. Nat Commun. 2025;16(1):4080. doi:10.1038/s41467-025-59388-9
46. Moullan N, Mouchiroud L, Wang X, et al. Tetracyclines disturb mitochondrial function across eukaryotic models: a call for caution in biomedical research. Cell Rep. 2015;10(10):1681–1691. doi:10.1016/j.celrep.2015.02.034
47. Li X, Wang M, Denk T, et al. Structural basis for differential inhibition of eukaryotic ribosomes by tigecycline. Nat Commun. 2024;15(1):5481. doi:10.1038/s41467-024-49797-7
48. Gando S, Levi M, Toh CH. Disseminated intravascular coagulation. Nat Rev Dis Prim. 2016;2(1):16037. doi:10.1038/nrdp.2016.37
49. Iba T, Levy JH. Inflammation and thrombosis: roles of neutrophils, platelets and endothelial cells and their interactions in thrombus formation during sepsis. J Thromb Haemost. 2018;16(2):231–241. doi:10.1111/jth.13911
50. Ingham E. The effects of tetracyclines and erythromycin on complement activation in vitro. Acta Derm Venereol. 1990;70(6):531–534. doi:10.2340/00015555-70531534
51. Zipfel PF, Skerka C. Complement regulators and inhibitory proteins. Nat Rev Immunol. 2009;9(10):729–740. doi:10.1038/nri2620
52. de Cordoba SR, Tortajada A, Harris CL, Morgan BP. Complement dysregulation and disease: from genes and proteins to diagnostics and drugs. Immunobiology. 2012;217(11):1034–1046. doi:10.1016/j.imbio.2012.07.021
53. Knight JS, Branch DW, Ortel TL. Antiphospholipid syndrome: advances in diagnosis, pathogenesis, and management. BMJ. 2023;380:e069717. doi:10.1136/bmj-2021-069717
54. Manning JE, Arachchillage DJ. Dilemmas in the diagnosis and management of antiphospholipid syndrome. J Thromb Haemost. 2024;22(8):2156–2170. doi:10.1016/j.jtha.2024.03.027
55. Narita M. Classification of extrapulmonary manifestations due to Mycoplasma pneumoniae infection on the basis of possible pathogenesis. Front Microbiol. 2016;7:23. doi:10.3389/fmicb.2016.00023
56. Song S, Xu Y. A retrospective study of the clinical characteristics of 9 children with pulmonary embolism associated with Mycoplasma pneumoniae pneumonia. BMC Pediatr. 2023;23(1):370. doi:10.1186/s12887-023-04188-7
57. Waites KB, Xiao L, Liu Y, Balish MF, Atkinson TP. Mycoplasma pneumoniae from the respiratory tract and beyond. Clin Microbiol Rev. 2017;30(3):747–809. doi:10.1128/CMR.00114-16
58. Pai MP, Wilcox M, Chitra S, McGovern P. Safety and efficacy of omadacycline by body mass index in patients with community-acquired bacterial pneumonia: subanalysis from a randomized controlled trial. Respir Med. 2021;184:106442. doi:10.1016/j.rmed.2021.106442
59. O’Riordan W, Green S, Overcash JS, et al. Omadacycline for acute bacterial skin and skin-structure infections. N Engl J Med. 2019;380(6):528–538. doi:10.1056/NEJMoa1800170
60. Tanaka SK, Steenbergen J, Villano S. Discovery, pharmacology, and clinical profile of omadacycline, a novel aminomethylcycline antibiotic. Bioorg Med Chem. 2016;24(24):6409–6419. doi:10.1016/j.bmc.2016.07.029
61. Liang R, Borgundvaag B, McIntyre M, Thwaites C, Ragan K, Wyllie A. Evaluation of the reproducibility of the Naranjo adverse drug reaction probability scale score in published case reports. Pharmacotherapy. 2014;34(11):1159–1166. doi:10.1002/phar.1496
62. Seger D, Barker K, McNaughton C. Misuse of the Naranjo adverse drug reaction probability scale in toxicology. Clin Toxicol. 2013;51(6):461–466. doi:10.3109/15563650.2013.811588
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.