Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Older Persons’ Views on Important Values in Swedish Home Care Service: A Semi-Structured Interview Study
Authors Olsen M ![]() , Udo C, Dahlberg L
, Udo C, Dahlberg L ![]() , Boström AM
, Boström AM ![]()
Received 7 December 2021
Accepted for publication 25 March 2022
Published 2 May 2022 Volume 2022:15 Pages 967—977
DOI https://doi.org/10.2147/JMDH.S347886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Marie Olsen,1,2 Camilla Udo,1,3 Lena Dahlberg,1,4 Anne-Marie Boström2,5,6
1School of Health and Welfare, Dalarna University, Falun, Sweden; 2Department of Neurobiology, Care Sciences and Society, Division of Nursing, Karolinska Institutet, Stockholm, Sweden; 3Center for Clinical Research Dalarna-Uppsala University, Falun, Sweden; 4Department of Neurobiology, Care Sciences and Society, Ageing Research Centre, Karolinska Institutet, Stockholm, Sweden; 5Theme Inflammation and Ageing, Karolinska University Hospital, Huddinge, Sweden; 6R&D Unit, Stockholms Sjukhem, Stockholm, Sweden
Correspondence: Marie Olsen, School of Health and Welfare, Dalarna University, Falun, SE-788 91, Sweden, Tel +46 23 778453, Email [email protected]
Introduction: Knowledge of older person’s experiences of important values in home care service can facilitate the development and delivery of high-quality services supporting their well-being, dignity and participation in the care provided. To date, few studies have explored older person’s values and experiences of home care services.
Purpose: This study aimed to explore values that older person holds regarding home care services and their experiences of how these values manifest in home care service delivery.
Participants and Methods: The study has a qualitative exploratory design. Semi-structured interviews were conducted with 16 older persons aged 74– 90 who received home care service. Data were analysed using qualitative content analysis.
Results: Two themes (each with sub-themes) of values relating to the experience of home care service from the perspective of the 16 older persons were identified: to be supported as an autonomous person and to be supported as a relational being. The participants experience that these two values were only partly manifested in the home care services they received. They also noted that their well-being was negatively affected when staff failed to implement these values. The fundamental values identified in study related to the older person feeling safe, being autonomous, maintaining control and independence, and having relationships. The values constitute help to guide practice from the perspective of older persons who receive home care services.
Conclusion: The identified values are primarily interpersonal-level values. However, such values are also of importance for home care service organisations when promoting delivery of person-centred care. Taking such a position implies adopting a relation-oriented rather than a task-oriented approach in providing home care services for older persons.
Keywords: dignity, home care service, older persons, person-centered care, value, well-being
Introduction
As a result of demographic changes, the number of older persons needing support to manage their daily lives at home has steadily increased,1–3 and many have conditions affecting their functional capacity. Most Western countries, including Sweden, have shifted from institutional care to home care service.3 The ageing-in-place policy emphasises the importance of supporting older persons to remain in their homes for as long as possible through formal and informal support.4 Several studies have shown that older persons remain at home much longer before moving to special housing today than a decade ago.1 To meet the growing care needs of an ageing population, WHO recommends Person-Centered Services as a Global Strategy.5 In social services, this is commonly referred to a user-centered care or a user perspective. In Sweden, the local authorities are responsible for home care services for older persons under the Swedish Social Services Act.6 The Act states that care should be universal, equally distributed and based not on income but the specific needs of the older recipient. Thus, the Swedish care for older persons is funded mainly by municipal taxes and government grants. Local authorities can provide services or operate through private providers, and older persons can choose from the available providers.7 In Sweden in 2020, about 236,000 older persons (aged 65 years and older) were granted home care service.8 Home care service in Sweden not only includes personal care (eg, showering, dressing and undressing, personal hygiene, eating and drinking), but also household chores eg, cooking, cleaning, shopping, errands, laundry and support with social activities.6,9,10 Home care service means for older persons in need of care and support that they have to give up some autonomy and independence.11
The Social Service Act specifies that home care services for older persons should support an active lifestyle and participation in daily life that allows the retention of dignity and a sense of well-being.6 These fundamental values have been operationalised into the following aspects: older persons’ self-determination, security, meaning and context, privacy and personal integrity, personalisation and participation, and being treated with dignity and respect.12 In this paper, the term value refers to a basic belief or an attitude about a specific type of behaviour or state considered desirable and preferred, ie what is desirable, worthwhile and important to an individual.13,14 To implement these values in the care for older persons, the National Board of Health and Welfare launched and financed guidance materials and an educational program in 2012. The program has since been implemented in most municipalities.12
Research has thus far mainly focused on older persons’ perceived needs for and experience of receiving health care at home and, to a lesser extent, their perceptions of home care services.15 Elsewhere, older persons have described unmet needs primarily regarding the psychosocial domain.13 A review of qualitative studies of older persons’ experiences of receiving home care services revealed positive and negative perceptions. In addition, the values of reciprocity, respect, attentiveness, safety, and security were often named. Finally, engagement in decisions about care were common themes describing older persons’ perceptions across studies.15 Reciprocity was regarded as a balanced relationship that maintains self-reliance and a sense of self. Respectful and attentive interactions contributed to unity and helped maintain a meaningful life by participating in daily activities. Central to feeling safe and secure was a trustworthy relationship with staff, including increased continuity. They also relied on their care staff to be competent, spend enough time with them and act in their best interests. Older persons whose needs are met by home care services have been reported to experience better psychosocial and general well-being than those with unmet needs.13 Although the older person is best qualified to give a perspective on their care needs,16–18 in research, their views are often represented by others, such as relatives or health care professionals.
Knowledge of older persons’ experiences of important values in home care services can facilitate the development and delivery of a high-quality service supporting the older person’s well-being, dignity, and participation in society. However, there is a knowledge gap regarding evidence-based home care services to support older persons who need support and care from home care services.19 Thus, one starting point for an evidence-based home care service is to let older persons themselves describe what they value when receiving home care service. Unfortunately, few studies have explored older person’s values and experiences of home care services. Considering the ambitious Swedish initiatives to support the development of home care services based on values expressed in the law Social Service Act, it is of interest to study the experiences of older persons after implementing this educational program. Therefore, this study explores the values of older persons regarding home care services and their experiences of how these values manifest in home care service delivery.
Materials and Methods
Design
This study has a qualitative exploratory design using semi-structured interviews with older persons receiving home care services. A qualitative approach was chosen to gain a more in-depth understanding of the experiences of home care services from the perspective of the older person.
Setting and Sample
The study was conducted in a municipality in central Sweden with approximately 60,000 inhabitants. In this municipality, home care service is delivered by public and private providers. At the time of the study (2015–2016), there were 16 providers (13 public and three private). During 2012–2013, the municipality received funding from the National Board of Health and Welfare to implement the national values for the care of older persons, including training of 58 facilitators with responsibility for the education of all staff in home care services. Therefore, a purposeful recruitment procedure was used to include 16 participants aged ≥65 years receiving home care services from public and private providers (see further below). Inclusion criteria were 65 years or older, received home care service for at least one year, not been diagnosed with dementia, could understand, and speak Swedish, and was cognitively able to participate. Exclusion criteria were older persons not cognitive able to give consent to participate in the study. In addition, during the recruitment process, participants were recruited considering variance in gender, age, housing, service provider and length of service receipt.
Data Collection
Interviews were conducted from November 2015 to March 2016. A semi-structured interview guide,20 was used focusing on the older person’s experiences of receiving home care service, important values in home care service and whether they would like to change anything, including questions such as: Could you please tell me whether there are any specific values you find important when receiving home care service? Do home care services have characteristics that are particularly important to you? Can you describe what you consider to be good home care services? Where participants expressed uncertainty about the meaning of “value” the interviewer explained that values were the most important aspects of home care service.
Procedure
The first author informed all 19 frontline managers of home care service groups in one municipality about the study (orally and in writing). The frontline managers were asked to identify eligible participants based on the inclusion criteria. The frontline managers identified presumptive participants and informed the staff in each home care service group. The staff then asked the older person whether he or she would be interested in participating and, if so, whether a researcher could contact him or her for more information about the study before taking the final decision to participate. The researcher then contacted those who had accepted by phone, provided more information about the study, and asked for oral consent to participate. The older person was then given a few days to reflect about taking part before contacted again to book the interview if they were still interested.
The frontline managers and staff only identified participants who they assessed were cognitively able to participate. The researcher who conducted the interviews is a registered nurse, with long experience from working with older persons, was also able to assess that the participant was cognitive able to participate before giving consent and taking part in the interview. None of the participants in the study were assessed as cognitively unable to participate. All of them provided written informed consent. Participants were given the option to choose the time and location of the interview. As a result, eight interviews took place in the participant’s homes and eight at a daycare center. The same researcher conducted all 16 interviews. Member checking was done during the interviews, as the interviewer repeatedly checked that the older person was correctly understood by paraphrasing and summarization for clarification. The median interview length was 48 minutes. The interviews were digitally recorded and transcribed verbatim. Breaks were taken if desired by the participants.
Data Analysis
The analysis was performed manually using word sheets, ie, no software was used. The interviews were analysed using inductive qualitative content analysis, enabling findings to emerge from the data analysis rather than searching for specific predetermined themes. Content analysis is a viable approach when analysing multi-faceted and sensitive phenomena,21 such as older persons’ perceived values of home care. Initially, all interview transcripts were read thoroughly to acquire an overall impression of the content. Next, the authors repeatedly discussed the content before identifying meaning units. Then, the meaning units were condensed and labelled with codes, ie, short labels closely following the participants’ descriptions. The codes were recurrently checked against the meaning units and discussed between the authors, compared, and grouped into preliminary themes and sub-themes reflecting the participants’ narratives. The analysis process continued until the authors reached a consensus.
Ethical Approval
The study was approved by the Regional Ethical Review Board in Uppsala, Sweden (Reg. No. 2015/203) This study was undertaken according to the Declaration of Helsinki recommendations for research involving human subjects.22 Participants were given oral and written information about the study before participating. This information was repeated at the start of the interview to ensure that the participants understood the information provided. They were also informed that participating was voluntary and that they could withdraw from the study at any time without explanation. Informed written and verbal consent was obtained from all participants, including consent to the publication of anonymised responses. The quotes in this article are identified by numbers representing the person to maintain the informants’ anonymity. The interview material was handled confidentially in strict accordance with Swedish legislation.
Results
Sixteen older persons (11 women) aged 74–90 (median=82 years) was interviewed (Table 1). Of the 16 older persons, 14 lived alone; and 12 received home care service from a public provider. They had received home care service between 2 and 7 years. For 11 participants, such service was combined with informal care.
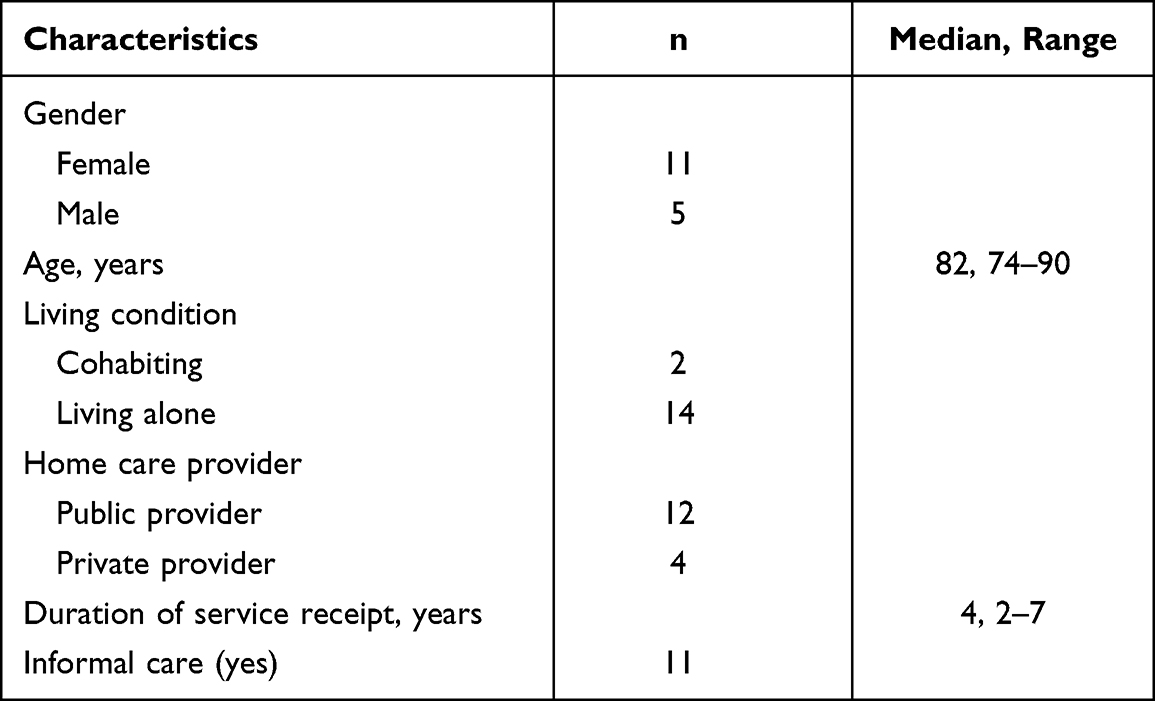 |
Table 1 Characteristics of Study Participants (n=16) |
In the analysis, we identified two themes of values from the older persons’ perspective in the context of home care services: 1) to be supported as an autonomous person and 2) to be supported as a relational being (Table 2). Each theme consisted of three sub-themes. The themes and sub-themes are presented below and are illustrated with verbatim quotations derived from the interviews.
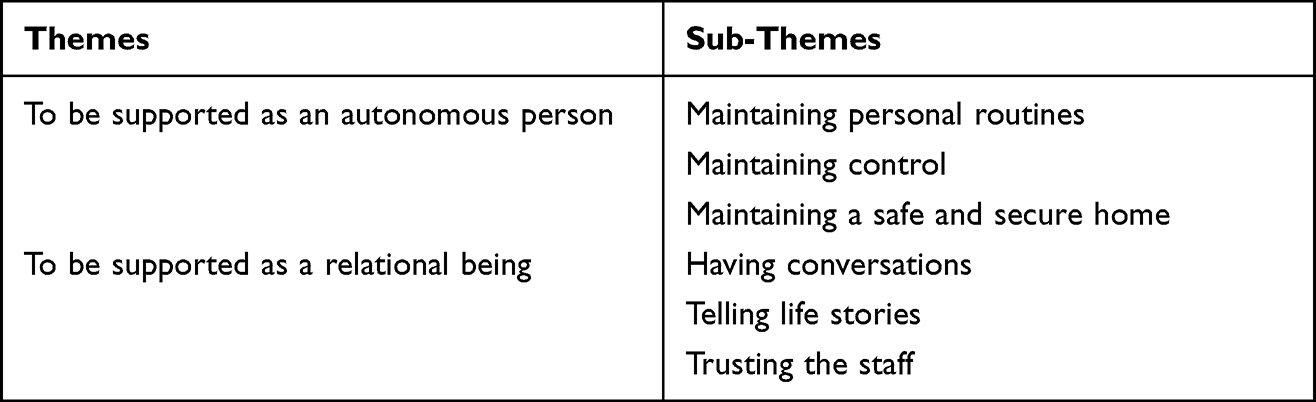 |
Table 2 Themes and Sub-Themes |
To Be Supported as an Autonomous Person
Participants expressed their wish to plan their home care service based on their current capacity to carry out daily tasks. They also wanted to be informed about changes in the service they received. More concretely, this concerned maintaining personal routines and control over what was happening in their home and maintaining a sense of safety while becoming increasingly dependent on support from home care services.
Maintaining Personal Routines
The participants’ ambition was to maintain their routines and continue life as usual for as long as possible. As part of this aspiration, they wanted to stay independent despite their functional limitations and need for support from home care services. The participants said they felt that home care service procedures were not always compatible with their routines, which they found problematic. For example, they detailed how they had to adapt to the service schedule and availability regarding what day and time they could shower, regardless of their routines and preferences. The participants underlined the importance of their routines and articulated they wanted staff to understand this aspect of their life. The participants wanted to be involved in the home care service and have the possibility to influence. The participants criticised the system saying they were given too little credit.
The persons [the staff] should not make all the decisions about me; instead, they should ask me nicely. (Interview 4)
And then, when they [the staff] change the schedule, I want them to reason with me. If I, for example, stand in the shower at 8 am, and without telling me, they suddenly come … (Interview 7)
The participants consistently reported the importance of having a limited number of home care service staff so that they and the personnel had the opportunity to learn to know each other. This was important since they felt that the staff needed to know them exceptionally well to understand their needs and routines. The participants also stated that, because there was little time for discussion, it was not easy having new staff members in their homes who did not know them or their preferences.
Maintaining Control
The participants sought to maintain control over what was happening in their homes. They also described how important it was that staff should not move their belongings without their knowledge and permission. The participants were frustrated because they had to explain their preferences and the items’ location repeatedly. For example, they wanted the plates and cups in their usual place to find them easily. The participants alleged how staff sometimes went ahead and entered a room without waiting for them, moving things before they had the chance to follow, and without asking while explaining why it was for the best. The participants relayed the importance of having staff who listened and was attentive to their needs.
They must listen to me if I say something, such as, Now I want you to help me with this or that and how I want to be helped … (Interview 12)
It is a bit difficult but … but you want certain things to be done at a specific time and a certain way. (Interview 2)
I am a little sensitive that people should try to control and decide for me. I told the staff; I do not accept that. Then she answered that she did not realise she did. (Interview 8)
The participants discussed the need to be informed about changes and decisions regarding home care services in advance. If their wishes regarding the service delivery were ignored, they felt like objects of charity and passive recipients of home care service. They disclosed how they had little or no control over changes in the home care services they received and were often not informed about such changes beforehand.
Maintaining a Safe and Secure Home
The participants described how important it was to feel safe and secure in their homes. They mentioned feeling insecure when a member of staff did not turn up as scheduled and, on occasion, would worry about whether the member of staff would come at all. The participants spoke of the importance of having a staff member arrive on schedule and knowing which staff was coming. When they were dependent on nighttime help and support, the participants worried about not knowing who would be coming while asleep or who would wake them in the morning. These concerns made them feel insecure, anxious, and fearful.
It was the middle of the night, and I did not know who would be coming through the door. I heard sounds from the door. Who is coming? Is it someone from the home care service, or is it someone else? It was terrible. I felt enormously anxious and wondered who was there. I felt scared and insecure. That cannot be right. (Interview 12)
However, they [the staff] rarely have any name tags. I have heard that they should have name tags on them. I have no idea what their names are. (Interview 16)
They [the new staff] should have someone experienced with them. Several times, someone totally new has come here. Yes, it is unsafe. They [new staff] should have someone who teaches them. (Interview 9)
Participants reported that they felt more secure with older and more experienced members of staff. New members of staff were perceived as insecure and having less confidence to perform slightly more advanced tasks such as displacement at bedtime.
To Be Supported as a Relational Being
For the participants, it was important to have a reciprocal relationship with the staff, as such a relationship enhances trust and reduces concern associated with relying on others. They described social interaction as equally important as the practical support from the staff. They also expressed a need to tell their life stories, showing the staff that they, too, had once been young and mobile with an active life.
Having Conversations
Participants recounted how conversations with the staff could often be more important than completing practical tasks. They sometimes asked the staff if they had time to sit down and talk instead of carrying out practical tasks. The participants observed staff members having different approaches to their work and having different relationships with the staff. However, for the most part, they appreciated and liked most of the staff members.
The staff members are very different. Some are in a rush, whereas others take the time to sit down. I usually ask the staff if they have time to sit down and talk … And now that two of the staff members are pregnant, I tell them that I am expecting grandchildren. (Interview 11)
The participants said they wished that the staff had more time for conversations and to ask relevant questions to extend their understanding of their needs. In addition, it had been a long time for some of the participants since they had talked to anybody, making conversation with staff and courteous treatment even more important.
I like it when they [the staff] come because then I have the chance to have conversations and practice talking. I discovered that my speech becomes a bit peculiar when I am not talking to anybody. However, when the staff arrive, I can talk to them and feel a little sense of involvement. (Interview 1)
You can talk [with the staff] about anything … so that you become more familiar, get to know each other … (Interview 9)
Sometimes, the participants felt that the staff openly ignored them, not asking questions, or not listening to their requests and troubles. The participants stated that it was as if the staff neither saw nor heard them, which they found humiliating.
Telling Life Stories
The participants expressed how important it was to tell the staff their life stories. They wanted to show photographs and talk about their past because they had lived long lives and wanted to share their memories and experiences.
I like to talk to them and tell them about my life when I was young in the old days. I enjoy telling them about what I have been through, which I think is important to me. (Interview 1)
The participants wanted the staff, especially the younger staff, to understand that they led a worthwhile and meaningful life. Some wished the staff would understand how different society had been when they were young. They hoped the staff would listen and hear what they had to say. Telling their life story was part of having a close personal relationship with staff members and was seen as a valuable aspect of home care service. They appreciated when the staff showed an interest in them as individuals and tried to get to know and learn from them.
Trusting the Staff
The participants emphasised the importance of a competent, skilled, and experienced staff because this made them feel calm and confident that they would receive professional service. The participants pointed out the importance of a trustworthy staff and having a staff member who offered a close and supportive relationship and paid attention to their needs. Knowing that staff had sufficient skills and knowledge contributed to their sense of safety. The participants felt that skills and knowledge came with age and said that older staff were more skilled than the younger personnel. They said that the older staff were more engaged with their work. They were also more often observant of the older person’s personal needs.
Consequently, participants said they generally trusted older staff more. Conversely, younger, and less experienced staff were perceived as less secure. Thus, the participants doubted whether the staff knew what to do in difficult and unexpected situations (eg, whether they would manage to help them if they fell or would give them the correct medication in emergencies).
I get scared because I ‘cannot stand up and ask the staff before leaving ‘who will be coming [to help] the next time. I need to know if the person can catch me if ‘ ‘I am falling and help me up. (Interview 5)
When they tell me that a young girl will be coming next time, I get a sore stomach. (Interview 12)
Yes, I am scared because, you know, I cannot stand on my feet. I tell the staff who is coming - you should know that I cannot stand on my feet, I do not want to scare you, but you should be aware of it. They must not think that now I am standing, and everything is ok because it is not … (Interview 10)
The participants also explained how they were concerned that new and young staff members would have negative attitudes towards them and thought that not all staff were suitable for working with older persons. Moreover, the participants remarked that they sometimes felt treated like a child and ridiculed by the staff. According to the participants, some staff members used inappropriate words in their presence. Such behaviour was depicted as contributing to a general lack of trust in the staff.
Discussion
Our findings show that older persons valued autonomy, ie, independence and control of their life and feeling safe and secure in their home during home care service encounters. To be seen and treated as a relational being was also central, ie, being of interest to the staff and having the opportunity to talk about life experiences and trusting the staff. The older persons expressed important values of a home care service and how they perceived whether staff adhered to these. The values held by the participants are similar to the values outlined in the Swedish national policy,6 and the findings are consistent with those reported in a systematic review by de São José et al.15 Even if the Swedish government has allocated considerable resources to implement values, such as participation, specified in national policy, our results indicate that these values are not fully manifested in home care service from the perspective of the older recipients.
The participants identified the core values of being autonomous, self-determined, and having relationships. Other studies have shown the importance of promoting older persons’ engagement when receiving home care services because this may contribute to their ability to live a more meaningful life and maintain their well-being.23–25 Breitholtz et al26 found that some older persons maintain control by supervising the staff. The authors specified that this should be understood as older persons losing their control and trying to regain it, but that can also be interpreted as a struggle to defend and guard their self-determination. Other researchers have found that if older persons feel that staff do not listen to them, it hinders their involvement in the home care service procedure27 as confirmed in our study. The degree of involvement and engagement is closely linked to a person’s experience of meaning and purpose in life.28 Being engaged in daily routines can offer a sense of filling the day with activities and sustaining a connection with life.15 Consequently, if older persons’ involvement in the home care service process decline and engagement is not supported, this may lower their sense of meaning.
Another important value was having an open and trusting relationship with the staff, which allowed the participants to share their life stories. Telling staff about their lives may be one way to show them that they are capable, independent, and autonomous. These results align with Kitwood,29 who argues that it is important for all humans to be respected and seen and treated by others as capable human beings. A recent qualitative study showed a similar result, where persons with dementia expressed that having a relationship with those who came to their homes (ie, socialising with the staff and being seen as an integral part of society) were vital components of receiving home care service.30
Based on older persons’ views about relationships, it seems important that the home care service organisation aims for staff continuity and communication with the older person as a human being. Researchers stress the importance of professional–person relationships in providing personal care.31,32 The relationship is a fundamental aspect of person-centred care, which implies a holistic approach that incorporates the various dimensions of well-being, including context and individual expression, preferences, and beliefs.33 Cleland et al argue that mutual relationships with respect and kindness positively impact older person’s quality of life and well-being.34 Having the opportunity to tell their personal life stories was a central value to the participants in our study. Life stories can also support continuity with the past and sustain a sense of self.15 According to McCormack35 it is crucial for delivering person-centered care to know a person, what they value in life, their needs, and preferences.
Our results indicate that if the ageing-in-place policy is promoted, staff in home care service must be relation-oriented and not merely task-oriented. Individually adapted home care service is consistent with person-centred care in which the life story is respected, and the person’s preferences constitute a basis for the service.33 It is important to understand a person’s needs, preferences and values to undertake a person-centred approach.36 However, care services in Sweden have undergone significant structural changes in recent years, for example, with substantial cutbacks in care homes.37 This means that more frail persons are living at home and that older persons who are granted home care services have increased complex care needs. This requires more time from staff and staff need to be trained to meet more demanding care needs.10 At the same time, staff often work alone and are under time pressure,38 which means that they have limited time during a visit to engage in social interactions. This approach is consistent with a recent study in which staff in home care service reported wanting to do more for older persons than their employer was willing to sanction and that older persons do not always receive the care they are granted.39
A stable and trustful relationship between older persons and staff is essential when receiving home care services.15 In 2012, the Swedish National Board of Health and Welfare published a set of national values as a basis for care for older persons. One of these values was that care should be delivered in a way that the older person can feel safe and secure.11 Many staff members in care of older persons do not have Swedish as first language.40 Although the participants in our study did not bring up this issue, this has been noted in previous research. For example, two Swedish studies conducted in nursing homes reported major misunderstandings between staff members and older persons with dementia, and that staff were not able to identify the needs of the older person and therefore could not deliver the needed care.41,42
Our study shows that it is important for older persons receiving home care service to feel safe and secure. One way to support their sense of safety to keep continuity in staff, preferably with educational training and experiences from working in home care services. Similar findings were described by Herrler et al43 who found that feelings of safety and security when care included individual adjustment.
The participants in our study sometimes felt that the staff neglected them or treated them disrespectfully. This finding concurs with Gregory et al research,38 who reported that staff sometimes use poor communication and show a lack of respect for older persons. In line with this, negative experiences from home care services were related to poor communication and lack of respect.44
Our results suggest that a condescending attitude can impact the older person’s trust in the home care service staff. Moreover, staff need to be committed to assisting older persons’ well-being and best interests. For example, friendly staff impact individuals’ quality of life and well-being.45 The participants in our study were often worried and anxious because of being dependent on nighttime assistance and support, especially when they had not been informed about the time, the staff would arrive, or which staff member would be on duty. Providing such information is, thus, one way to enhance feelings of safety and security in older persons receiving home care services.16
Implementing new routines based on complex values and incorporating staff attitudes and beliefs are the responsibility of staff members and the home care service organisation.7,13 Changing practice by following new guidelines will take time and require leadership and continuous feedback from managers.46 In addition, changing staff attitudes from task-oriented to relation-oriented will require changes to the work organisation if relations are to improve between older persons and their staff.47 Home care service providers must provide the conditions for staff to be able to perform person-centered care for older persons living at home.48
Strengths and Limitations of the Study
This study contributes to the knowledge on older “persons” values regarding home care services. In addition, the findings are based on accounts provided by the older participants, which strengthens the credibility of the study.
This study has some limitations. For practical reasons, the staff in the home care service organisation recruited the participants, which restricted our control over the selection process. Thus, there is a risk that credibility is compromised when the researcher asked staff to invite those who matched the inclusion criteria may thereby have acted as gatekeepers. However, given that the participants expressed negative views on home care services, this risk can be considered small.
The older person did not explicitly refer to the word “values” instead, they discussed various aspects experienced as important in home care service. In addition, they expressed their expectations on how the staff should behave when providing home care service. Still, the findings show that these aspects convey what is regarded as values in the research literature and policies, strengthening our study’s dependability.
Transferability is likely as national laws and regulations regulate all home care services in Sweden. However, important care decisions are made locally, and financial conditions vary across municipalities, impacting the delivery of home care services. In addition, transferability was restricted because only Swedish-speaking persons were included. Finally, this study is based on interviews with older persons receiving home care services without known cognitive impairment or dementia. Given that many older persons living with dementia in their own homes, future research needs to explore values regarding home care service in this group.
Conclusions
This study explored values particularly important to older persons receiving home care services. The themes of being supported as an autonomous person and as a relational being include fundamental values that matter to older persons when receiving home care service, that is, feeling safe, being autonomous, maintaining control and independence, and having relationships. In addition, our study shows how important it is for staff to adopt a relation-oriented approach in providing home care service. Also noteworthy is that, according to the older person, staff in home care service should have sufficient time for conversations, which facilitates the involvement of the older persons in their home care service, thereby contributing to their feeling of independence. The values described in our study constitute help to guide practice from the perspective of older persons who receive home care services. Such values are also of importance for home care service organisations when promoting delivery of person-centred care.
Implications for Practice and Research
The values identified in our study are primarily at the interpersonal level. However, integrating the values and translating them into actual daily home care service behaviour must be discussed and facilitated at an organisational level. Putting the values into daily practice is partly, but not entirely, the responsibility of each staff member. The home care service organisation also needs to take responsibility for conditions under which care is delivered, such as staff scheduling and schedule flexibility, giving sufficient time for each visit, and reflective practice.
Acknowledgments
The authors are grateful to all participants and the Swedish National Graduate School on Ageing and Health (SWEAH) for valuable support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
Falun Local Municipality and Dalarna University supported this work.
Disclosure
The authors declared no conflicts of interest for this work. An abstract of this paper was presented at the 24th Nordic Conference of Gerontology, Oslo, Norway, 2-4 May 2018 as a poster presentation with interim findings. The poster’s abstract was published in DiVA, an institutional repository for research publications and student theses written at 50 universities and research; available at: http://www.divaportal.org/smash/record.jsf?pid=diva2:1206975.
References
1. Schon P, Lagergren M, Kareholt I. Rapid decrease in length of stay in institutional care for older people in Sweden between 2006 and 2012: results from a population-based study. Health Soc Care Community. 2016;24(5):631–638. doi:10.1111/hsc.12237a
2. Ulmanen P, Szebehely M. From the state to the family or to the market? Consequences of reduced residential eldercare in Sweden. Int J Soc Welf. 2015;24(1):81–92.
3. Genet N, Boerma WGW, Kringos DS, et al. Home care in Europe: a systematic literature review. BMC Health Serv Res. 2011;11:1–4
4. Dahlberg L, Berndt H, Lennartsson C, Schön P. Receipt of Formal and informal help with specific care tasks among older people living in their own home. National trends over two decades. Soc Policy Adm. 2018;52(1):91–110.
5. World Health Organization. WHO global strategy on people-centred and integrated health services-Interim report; Geneva: Switzerland World Health Organization (WHO); 2015. Document number: WHO/HANS/SDS/2015.6. Available from: https://apps.who.int/iris/handle/10665/155002.
6. SFS. 453. Socialtjänstlagen [The Social Services Act]. Stockholm: Ministry of Health and Social Affairs; 2001. Avaible from: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453.
7. SFS. 962. Lag om valfrihetssystem [Act on Freedom of Choice Systems]. Stockholm: Ministry of Health and Social Affairs; 2008. Avaible from: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-2008962-om-valfrihetssystem_sfs-2008-962.
8. National Board of Health and Welfare. Vård och omsorg om äldre Lägesrapport 2020. [Status report on health and social care for older persons, 2020]. National Board of Health and Welfare (NBHW);. ISBN: 97891 2021.
9. Sandberg L, Nilsson I, Rosenberg L, Borell L, Bostrom AM. Home care services for older clients with and without cognitive impairment in Sweden. Health Soc Care Community. 2019;27(1):139–150. doi:10.1111/hsc.12631
10. Szebehely M, Trydegård G-B. Home care for older people in Sweden: a universal model in transition. Health Soc Care Community. 2012;20(3):300–309. doi:10.1111/j.1365-2524.2011.01046.x
11. Fjordside S, Morville A. Factors influencing older people’s experiences of participation in autonomous decisions concerning their daily care in their own homes: a review of the literature. Int J Older People Nurs. 2016;11(4):284–297. doi:10.1111/opn.12116
12. Socialstyrelsens föreskrifter och allmänna råd om värdegrunden i socialtjänstens omsorg om äldre. [The National Board of Health and Welfare’s regulations and general advice on the values in the social services’ care of the elderly]. (SOSFS 2012:3). Stockholm: Socialstyrelsen. [
13. Kadowaki L, Wister AV, Chappell NL. Influence of home care on life satisfaction, loneliness, and perceived life stress. Can J Aging. 2015;34(1):75–89. doi:10.1017/S0714980814000488
14. Rassin M. Nurses’ professional and personal values. Nurs Ethics. 2008;15(5):614–630. doi:10.1177/0969733008092870
15. de Sao Jose J, Barros R, Samitca S, Teixeira A. Older persons’ experiences and perspectives of receiving social care: a systematic review of the qualitative literature. Health Soc Care Community. 2016;24(1):1–11. doi:10.1111/hsc.12186
16. Jakobsson E, Nygård L, Kottorp A, Olsson CB, Malinowsky C. The use of everyday technology; a comparison of older persons with cognitive impairments’ self-reports and their proxies’ reports. Br J Occup Ther. 2020;84(7):446–455. doi:10.1177/0308022620954117
17. Kim S, Miller ME, Lin M, et al. Self- vs proxy-reported mobility using the mobility assessment tool-short form in elderly preoperative patients. Eur Rev Aging Phys Act. 2018;15(1):5. doi:10.1186/s11556-018-0194-x
18. Griffiths AW, Smith SJ, Martin A, Meads D, Kelley R, Surr CA. Exploring self-report and proxy-report quality-of-life measures for people living with dementia in care homes. Qual Life Res. 2020;29(2):463–472. doi:10.1007/s11136-019-02333-3
19. Statens beredning för medicinsk och social utvärdering. Kunskapsläget för bedömning och insatser inom äldreomsorgen. Identifiering av vetenskaplig kunskap och kunskapsluckor utifrån systematiska översikter. [The state of knowledge for assessment and efforts in care for older. Identification of scientific knowledge and knowledge gaps a systematic reviews] Stockholm Statens beredning för medicinsk utvärdering (SBU): 2019. Report No: 306. Avaible from: https://www.sbu.se/sv/publikationer/sbu-kartlagger/kunskapslaget-for-bedomning-och-insatser-inom-aldreomsorgen.
20. Kvale S, Brinkmann S. Den Kvalitativa Forskningsintervjun. [The Qualitative Research Interview]. 3 Rev. Uppl. Lund: Studentlitteratur; 2014.
21. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112.
22. Association WM. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
23. Kirkevold M, Moyle W, Wilkinson C, Meyer J, Hauge S. Facing the challenge of adapting to a life ‘alone’ in old age: the influence of losses. J Adv Nurs. 2013;69(2):394–403. doi:10.1111/j.1365-2648.2012.06018.x
24. Holm AL, Severinsson E. Perceptions of the need for improvements in healthcare after implementation of the Chronic Care Model. Nurs Health Sci. 2014;16(4):442–448. doi:10.1111/nhs.12136
25. Jarosz E. What makes life enjoyable at an older age? Experiential wellbeing, daily activities, and satisfaction with life in general. Aging Ment Health. 2021;28;1-11. 10.1080/13607863.2021.1916879.
26. Breitholtz A, Snellman I, Fagerberg I. Older people’s dependence on caregivers’ help in their own homes and their lived experiences of their opportunity to make independent decisions. Int J Older People Nurs. 2013;8(2):139–148. doi:10.1111/j.1748-3743.2012.00338.x
27. Jarling A, Rydström I, Ernsth-Bravell M, Nyström M, Dalheim-Englund AC. Becoming a guest in your own home: home care in Sweden from the perspective of older people with multimorbidities. Int J Older People Nurs. 2018;13(3):e12194. doi:10.1111/opn.12194
28. Drageset J, Haugan G, Tranvåg O. Crucial aspects promoting meaning and purpose in life: perceptions of nursing home residents. BMC Geriatr. 2017;17(1):254. doi:10.1186/s12877-017-0650-x
29. Kitwood T. Dementia Reconsidered: The Person Comes First. Buckingham: Open University Press; 1997.
30. Olsen M, Udo C, Boström AM, Hammar LM. Important aspects of home care service: an interview study of persons with dementia. Dementia. 2021;20(5):1649–1663. doi:10.1177/1471301220964393
31. Edvardsson D. Notes on person-centred care: what it is and what it is not. Nord J Nurs Res. 2015;35(2):65–66. doi:10.1177/0107408315582296
32. Rushton C, Edvardsson D. Reconciling conceptualizations of relationships and person-centred care for older people with cognitive impairment in acute care settings. Nurs Philos. 2018;19:2. doi:10.1111/nup.12169
33. Ekman I, Swedberg K, Taft C, et al. Person-centered care-ready for prime time. Eur J Cardiovasc Nurs. 2011;10(4):248–251. doi:10.1016/j.ejcnurse.2011.06.008
34. Cleland J, Hutchinson C, Khadka J, Milte R, Ratcliffe J. What defines quality of care for older people in aged care? A comprehensive literature review. Geriatr Gerontol Int. 2021;21(9):765–778. doi:10.1111/ggi.14231
35. McCormack B, Dewing J, Breslin L, et al. Developing person-centred practice: nursing outcomes arising from changes to the care environment in residential settings for older people. Int J Older People Nurs. 2010;5(2):93–107. doi:10.1111/j.1748-3743.2010.00216.x
36. Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1):195. doi:10.1186/s12877-019-1189-9
37. Schön P, Heap J, editors. Thematic Report on Challenges in Long-Term Care-Sweden: European Social Policy Network (ESPN). Brussels: European Union; 2018. doi:10.1007/s10433-021-00633-7
38. Gregory A, Mackintosh S, Kumar S, Grech C. Experiences of health care for older people who need support to live at home: a systematic review of the qualitative literature. Geriatr Nurs. 2017;38(4):315–324. doi:10.1016/j.gerinurse.2016.12.001
39. Sandberg L, Borell L, Edvardsson D, Rosenberg L, Bostrom AM. Job strain: a cross-sectional survey of dementia care specialists and other staff in Swedish home care services. J Multidiscip Healthc. 2018;11:255–266. doi:10.2147/jmdh.s155467
40. Statens offentliga utredningar. Stärkt kompetens i vård och omsorg - Betänkande av Utredningen Reglering av yrket undersköterska. [Strengthened competence in health and social care- The inquiry of regulation of the profession of assistant nurse]. Stockholm: Elanders Sverige AB; 2019. SOU 2019:20. Available from: https://www.regeringen.se/rattsliga-dokument/statens-offentliga-utredningar/2019/04/sou-201920/.
41. Rosendahl SP, Söderman M, Mazaheri M. Immigrants with dementia in Swedish residential care: an exploratory study of the experiences of their family members and Nursing staff. BMC Geriatr. 2016;16;16:18. doi:10.1186/s12877-016-0200-y
42. Söderman M, Rosendahl SP. Caring for ethnic older people living with dementia -experiences of Nursing staff. J Cross Cult Gerontol. 2016;31(3):311–326. doi:10.1007/s10823-016-9293-1
43. Herrler A, Kukla H, Vennedey V, Stock S. What matters to people aged 80 and over regarding ambulatory care? A systematic review and meta-synthesis of qualitative studies. Eur J Ageing. 2021. doi:10.1007/s10433-021-00633-7
44. Ogrin R, Meyer C, Appannah A, McMillan S, Browning C. The inter-relationship of diversity principles for the enhanced participation of older people in their care: a qualitative study. Int J Equity Health. 2020;19(1):16. doi:10.1186/s12939-020-1124-x
45. Cox C, Pardasani M. Aging and human rights: a rights-based approach to social work with older adults. J Hum Rights Soc Work. 2017;2:98–106. doi:10.1007/s41134-017-0037-0
46. Harvey G, Kitson A. PARIHS revisited: from heuristic to integrated framework for the successful implementation of knowledge into practice. Implement Sci. 2016;11:33. doi:10.1186/s13012-016-0398-2
47. Austrom MG, Carvell CA, Alder CA, Gao S, Boustani M, LaMantia M. Workforce development to provide person-centered care. Aging Ment Health. 2016;20(8):781–792. doi:10.1080/13607863.2015.1119802
48. Olsen CF, Bergland A, Debesay J, Bye A, Langaas AG. Striking a balance: health care providers’ experiences with home-based, patient-centered care for older people—A meta-synthesis of qualitative studies. Patient Educ Couns. 2019;102(11):1991–2000. doi:10.1016/j.pec.2019.05.017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.