Back to Journals » Drug Design, Development and Therapy » Volume 13
Ocular surface squamous neoplasia: angiographic characteristics and response to subconjunctival/perilesional 5-fluorouracil injections
Received 17 October 2018
Accepted for publication 5 February 2019
Published 29 April 2019 Volume 2019:13 Pages 1323—1334
DOI https://doi.org/10.2147/DDDT.S191161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sukesh Voruganti
Yuzhao Sun, Rui Hua
Department of Ophthalmology, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning 110001, People’s Republic of China
Introduction: To investigate the angiographic characteristics of ocular surface squamous neoplasia (OSSN) and to evaluate the efficacy of subconjunctival/perilesional 5-fluorouracil injections in OSSN cases.
Materials and methods: Six eyes of six patients with primary OSSN, received perilesional, subconjunctival, 25-mg/mL 5-fluorouracil injections at certain intervals. Anterior segment digital photography images, anterior segment optical coherence tomography (AS-OCT), and conjunctival indocyanine green angiography (ICGA) were obtained simultaneously with fluorescein angiography.
Results: The mean best-corrected vision acuity significantly improved after treatment. At baseline, the median of the largest thickness of OSSN was 905.0 (interquartile range: 492.0–1592.5) μm based on AS-OCT data. There was an abrupt transition between normal and abnormal epithelium, a thickened hyper-reflective epithelium, and a sharp plane of cleavage between the lesion and underlying tissue, all indicative of OSSN. The angiographic characteristics of OSSN included focal or seafan-shaped intratumoral and conjunctival feeding vessels visible via ICGA, and abnormal vascular leakage visible with fluorescein angiography. The median time to tumor regression after treatment was 35.0 (interquartile range: 32.0–45.5) days in five eyes without recurrence, and OSSN in one eye regressed partially 40 days after treatment.
Conclusion: This is the first report of the angiographic characteristics of OSSN and its response to subconjunctival/perilesional 5-fluorouracil injections by simultaneous conjunctival angiography and AS-OCT. The improved subconjunctival/perilesional 5-fluorouracil injection was an effective therapy for OSSN in both best-corrected vision acuity gain and anatomic outcomes.
Keywords: ocular surface squamous neoplasia, subconjunctival 5-flourouracil injection, conjunctival angiography, anterior segment optical coherence tomography
Introduction
Ocular surface squamous neoplasia (OSSN) was a term suggested by Lee and Hirst to describe all primary dysplastic and carcinomatous lesions that originate from the epithelium of the cornea or conjunctiva,1 including conjunctival and/or corneal intraepithelial neoplasia, intraepithelial carcinoma of the conjunctiva, and conjunctival squamous cell carcinoma.2 Although OSSN is described as a relatively low-grade malignancy,1 it can locally invade the sclera, uvea, eyelids, and orbit and has the ability to metastasize to distant sites, thus potentially becoming life threatening.3 This is evident especially in sub-Saharan Africa, where OSSN is more common and aggressive.4
The prognosis of OSSN can be studied using imaging methods. Anterior segment optical coherence tomography (AS-OCT) demonstrates a thickened hyper-reflective epithelium with an abrupt transition between abnormal and normal epithelium in OSSN lesions that also mimic histopathological findings.5 In addition, OCT can be used to monitor OSSN resolution during medical treatment. In several OSSN cases, high-resolution OCT can reveal subtle residual epithelial thickening not observed through clinical examinations, thus preventing a possible premature termination of treatment.6 Pathologically, OSSN has been described as elevated gelatinous, papilliform, or leukoplakic limbal lesions that move freely over the sclera with adjacent feeder vessels.5 However, there are no reports of the angiographic characteristics of OSSN measured by anterior segment angiography modalities such as conjunctival indocyanine green angiography (ICGA) and fluorescein angiography (FA).
Treatment modalities for OSSN include combinations of excision, cryotherapy, and topical chemotherapy including 5-fluorouracil, mitomycin C, and interferon alpha-2b.7–9 Medical treatment is especially advantageous in diffuse, multifocal lesions; annular lesions of the limbus; and recurrent disease cases. The major drawbacks of topical chemotherapy are the tumor thickness and a possible limbal stem cell deficiency (LSCD). The former may be related to the theoretically insufficient penetration of the drug into the tumor mass.10 LSCD may be another issue created by the direct stimulation of the topical contact with the ocular surface and toxic effects of frequent administration.11 Therefore, it is evident that there are defects in topical chemotherapy and the surgical excision of the OSSN in those with a sizeable thickness and/or a wide range of involvement (tumors larger than 5 mm in diameter, or tumors extending more than 2 mm onto the cornea/more than one-fourth of the limbus), and the possibility of recurrence caused by inadequate initial therapy.3,12 Furthermore, topical 5-fluorouracil, mitomycin C, and interferon alpha-2b are off label in China. Subconjunctival injection is a classic treatment for ocular diseases. Karp et al suggested perilesional subconjunctival recombinant interferon alpha-2b as a viable medical alternative for the treatment of OSSN.13 Compared with interferon alpha-2b and mitomycin C, 5-fluorouracil is an inexpensive drug;14 also, its side effects are mild, mainly transient, and resolve upon therapy termination. Therefore, the aims of this study were to investigate the angiographic characteristics of OSSN and to evaluate the efficacy of subconjunctival/perilesional 5-fluorouracil injection in OSSN treatment.
Material and methods
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of China Medical University. Patients were given detailed information regarding the off-label use of subconjunctival 5-fluorouracil injections before treatment and written informed consent was obtained from each patient.
We performed a retrospective study of six eyes of (one each from five male patients and one female patient) with primary OSSN confirmed by AS-OCT and exfoliative cytology (Figure 1). One patient had a medical history of diabetes. To localize the tumor lesions in the conjunctiva or cornea, we performed exfoliative cytology with a small modification: a 3-mm non-woven fabric was placed on the surface of the tumor using gentle pressure; then, the sample was placed on a microscope slide, fixed with 95% alcohol (Panjing pharmaceutical co., ltd, China), and stained using the Papanicolaou technique.15,16 The following AS-OCT features were indicative of OSSN: 1) a thickened hyper-reflective epithelial layer, 2) an abrupt transition from normal to abnormal epithelium, and 3) a distinct plane between the lesion and underlying tissue that could be noted in conjunctival intraepithelial neoplasia (seen in thinner tumors).16
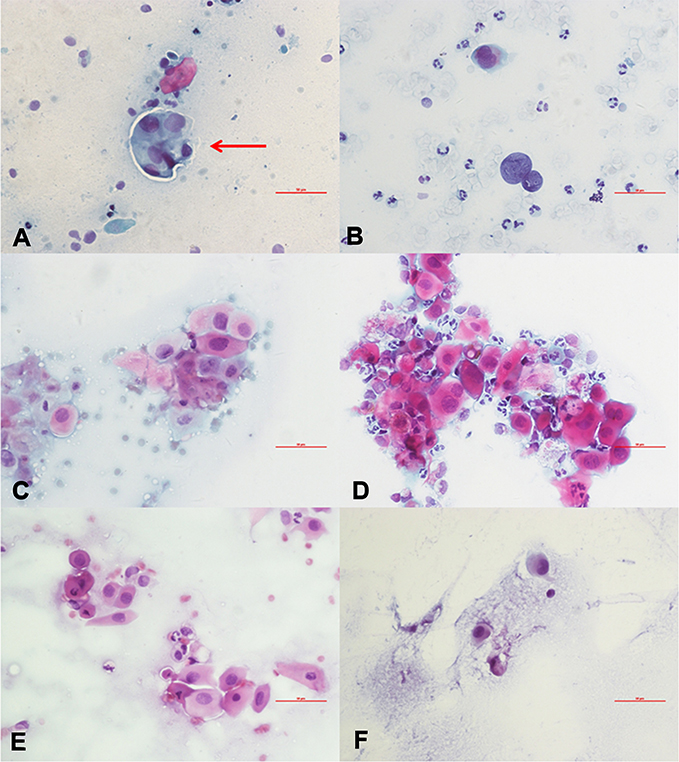 | Figure 1 Exfoliative cytopathology of six OSSN cases stained using a Papanicolaou technique (×40). The cells are scattered under the microscope; enlarged cell and nuclear sizes, an increased karyoplasmic ratio, and an uneven distribution of thickened chromatin are observed, all of which suggest abnormal proliferation of the cancerous cells. Especially, in panel A, multiple heteromorphic cells aggregated into a structure similar to the “carcinoma nest” (red arrow). (A) Case 1. (B) Case 2. (C) Case 3. (D) Case 4. (E) Case 5. (F) Case 6. The plotting scale in each image is 50 µm (red bar).Abbreviation: OSSN, ocular surface squamous neoplasia. |
In cases of adequate initial therapy and no recurrence, all patients received several multipoint subconjunctival injections of 25 mg/mL 5-fluorouracil (Shanghai Xudonghaipu Pharmaceutical Co., Ltd, China),17 adjacent to the lesion and 3 mm outside of the cornea limbus, as follows: during the first phase, the patients received 5 mg of 5-fluorouracil twice a week for 4–6 weeks until the tumor disappeared; during the second phase, the patients received a total of 7.5 mg of 5-fluorouracil weekly for 2–4 weeks. If there was no recurrence, the treatment was moved on to the last phase, which was comprised of 7.5 mg of 5-fluorouracil every for 10 days for 10–40 days. If the tumor recurred, we returned to the second phase of treatment. This treatment strategy was similar to the Karp et al.`study.13 The follow-up duration was more than 12 months in four cases and 8 months in two cases. Patients with a history of medical or surgical treatments were excluded from the study. Regional metastasis was ruled out in all patients by palpation of the cervical and periocular areas.
A complete ophthalmological examination, including best-corrected vision acuity (BCVA), anterior segment digital photography images (MediWorks, Shanghai, China), and AS-OCT (Spectralis OCT2; Heidelberg Engineering, Heidelberg, Germany), was performed to assess the prognosis of OSSN. The six fellow eyes were also examined as controls. ICGA (excitation, 787 nm; emission, 800 nm; field-of-view, 30° ×30° or 55°×55°) and FA (excitation, 488 nm; emission, 500 nm; field-of-view, 30°×30° or 55°×55°) were performed simultaneously using a multi-modality imaging system (Spectralis HRA+OCT; Heidelberg Engineering, Heidelberg, Germany) for conjunctival angiography and to investigate the angiographic characteristics of OSSN. Beginning at 30 seconds, movie mode was used to record the circulation of both intratumoral abnormal vessels and their conjunctival feeding vessels. AS-OCT with automatic real-time tracking was used to achieve data acquisition rates of up to 80,000 axial scans/second. Single-line images with 28 (18–43) frames were obtained, in automatic real-time mode, of the OSSN, conjunctiva, and cornea.
The examination also consisted of an analysis for hyper-reflectivity, which is an indicator for OSSN. Hyper-reflectivity in AS-OCT was defined as increased whiteness compared to tissue in the same location seen in healthy individuals, and hypo-reflectivity was defined as increased darkness compared to tissue in the same location seen in healthy people.6 The largest thickness of OSSN was measured by a distance-measuring tool (built into the Heidelberg software) semi-automatically. The AS-OCT examination also excluded the intraocular infiltration of these patients.
No punctual plugs were used. If corneal toxicity due to the 5-fluorouracil injection was observed, the patients were treated as follows: 0.3% sodium hyaluronate eye drops (preservative-free, Santan, Japan) four times a day for patients with mild punctuate epithelial erosion (PEE) and a bandage contact lens (PureVision of BAUSCH and LOMB Incorporated, USA) for those with moderate or severe corneal epithelial injuries. The frequency and dosage of 5-fluorouracil injections were adjusted according to tumor regression.
Statistical analyses were performed using SPSS (version 19.0; IBM Inc., Chicago, IL, USA). The data are expressed as the median (interquartile range). Changes in BCVA were analyzed by Wilcoxon matched-pair signed-rank tests. A P-value <0.05 was considered statistically significant.
Results
The median age of the patients was 58.5 (interquartile range: 53.0–75.3) years old. Three tumors were nasal in origin and the other three were temporal. One of the six cases had multifocal lesions, and the appearance of OSSN was nodular in two, papillomatous in three, and gelatinous in one. The median number of 5-fluorouracil injections was 15.5 (interquartile range: 9.8–24.0). The median treatment duration and follow up after final treatment was 13.0 (interquartile range: 5.8–20.3) weeks, and 13(interquartile range: 8–14) months respectively. The median BCVA after 5-fluorouracil treatment was 0.16 (interquartile range: 0.00–0.40), based on the logarithm of the minimum angle of resolution (LogMAR) values, which was better than the BCVA at baseline (0.61 [interquartile range: 0.073–1.40] LogMAR) (Z =2.023, P=0.043) (Table 1).
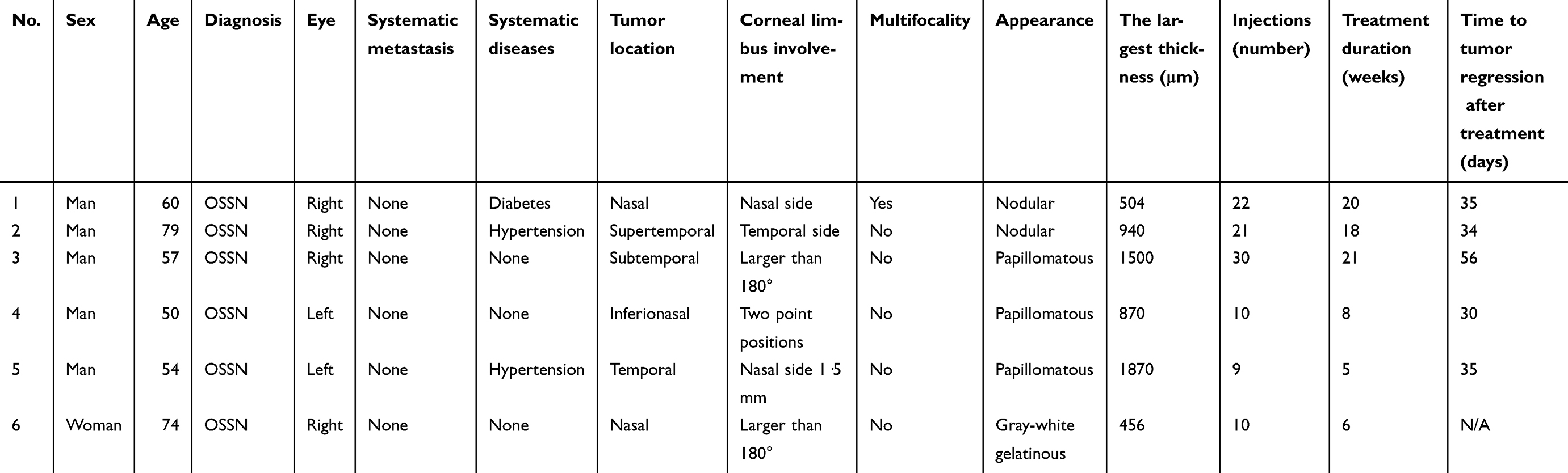 | Table 1 Characteristics of the study patients |
Baseline ICGA results showed focal or seafan-shaped intratumoral vessels and conjunctival feeding vessels. According to the 30 second movie mode, the intratumoral abnormal vessels filled immediately after the development of feeding vessels. After the 5-fluorouracil treatment, both intratumoral and conjunctival feeding vessels disappeared in five of the six cases, and patchy ischemic regions were observed in three of the six cases. Vascular rapid leakage on FA, initially observed in five eyes, was resolved during the follow-up (Figure 2–6). In the other eye, vascular leakage was resolved only partially; however, the presence of intratumoral vessels induced corneal edema and leakage, which was observed in the late stage FA (Figure 7). This patient did not receive the complete treatment for personal reasons.
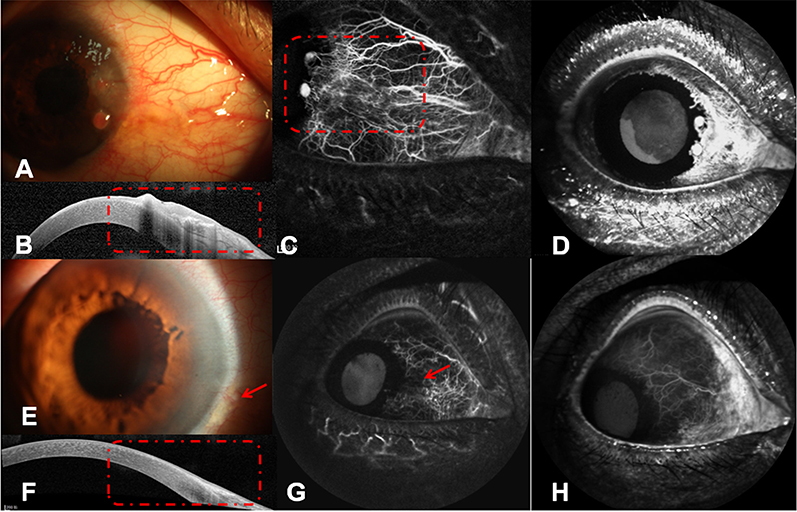 | Figure 2 Anterior segment images of Case 1 (right eye). (A) A nodular red tumor involving the cornea and limbus. (B) AS-OCT demonstrated a sharp delineation between normal and abnormal epithelia, a thickened and hyper-reflective epithelium, as well as a plane of cleavage between the lesion and the underlying tissue (red dots). (C) ICGA showed both focal pattern intratumoral vessels and conjunctival feeding vessels clearly (red dots). (D) Leakage from both the tumor and its feeding vessels observed via FA. (E) Complete disappearance of the tumor after treatment, with tiny palpebral fissures remaining (red arrow). (F) No clinical signs of the lesion were present on the AS-OCT image (red dots). (G) Both intratumoral vessels and conjunctival feeding vessels disappeared, and only a patched ischemic region was observed (red arrow) by anterior segment ICGA after treatment. (H) No leakage was found via FA after treatment.Abbreviations: AS-OCT, anterior segment optical coherence tomography; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography. |
The median of the baseline largest thickness of OSSN was 905.0 (interquartile range: 492.0–1592.5) μm based on AS-OCT data, and there was an abrupt transition between normal and abnormal epithelium, as noted by a rapid increase in both brightness and thickness of the epithelium, a thickened hyper-reflective epithelium, and a sharp plane of cleavage between the lesion and the underlying tissue in two eyes. In the other four eyes, which had large lesions, a shadow from the hyper-reflective epithelium obscured the plane of cleavage. AS-OCT at the last visit showed a normal-appearing cornea, limbus, and conjunctiva in five eyes; there was a bright white tear-film layer overlying the cornea and conjunctiva and the corneal epithelium was dark and thin, while that of the limbus and conjunctiva was thin but mildly hyper-reflective (Figure 2–6). The median time to tumor regression after treatment was 35.0 (interquartile range: 32.0–45.5) days.
Five of six patients could see tiny palpebral fissures in the primary tumor area after the tumor disappeared completely (Figure 2E, 3C, 4C, 5E, and 6C). Two patients had pterygium, but its size did not change after the 5-fluorouracil treatment (Figures 4C and 7C).
 | Figure 3 Anterior segment images of Case 2 (right eye). (A) A large nodular leukoplakic tumor involving the cornea and limbus. (B) AS-OCT demonstrated an abrupt transition between unremarkable and thickened hyper-reflective epithelia. However, in these large lesions, a shadow from the hyper-reflective epithelium sometimes obscured the plane of cleavage (red dots). (C) The tumor completely disappeared after treatment, with tiny palpebral fissures remaining (red arrow). (D) The neoplasm was completely replaced by a normal epithelium after treatment, as observed via AS-OCT (red dots). (E) No leakage was found through FA after treatment, and the patient wore a contact lens during angiography (yellow triangle). (F) ICGA anterior segment images revealed that both intratumoral vessels and conjunctival feeding vessels disappeared after treatment (red dots).Abbreviations: AS-OCT, anterior segment optical coherence tomography; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography. |
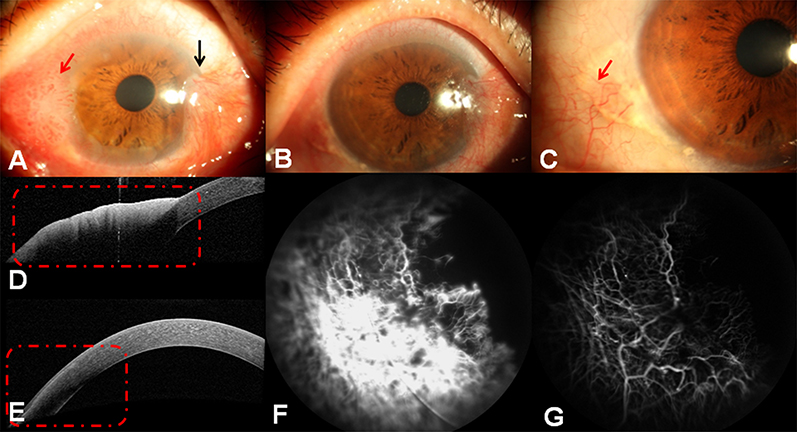 | Figure 4 Anterior segment images of Case 3 (right eye). (A) A large papillomatous tumor involving the temporal cornea, limbus, and conjunctiva (red arrow), with pterygia on the nasal side (black arrow). (B, C) The tumor completely disappeared after treatment, tiny palpebral fissures remained in the primary tumor area (red arrow), and the pterygia was unchanged. (D) AS-OCT demonstrated an abrupt transition between unremarkable and thickened hyper-reflective epithelium. However, in this large lesion, a shadow from the hyper-reflective epithelium sometimes obscured the plane of cleavage (red dots). (E) The neoplasm was completely replaced by a normal epithelium after treatment as shown using AS-OCT (red dots). (F) There were only a few dilated conjunctival vessels with partial leakage found through FA after treatment. (G) Both intratumoral vessels and conjunctival feeding vessels disappeared after treatment, as observed on anterior segment ICGA.Abbreviations: AS-OCT, anterior segment optical coherence tomography; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography. |
 | Figure 5 Anterior segment images of Case 4 (left eye). (A) A large papillomatous red tumor involving the cornea, limbus, and conjunctiva. (B) AS-OCT demonstrated an abrupt transition between unremarkable and thickened hyper-reflective epithelia. However, in this large lesion, a shadow from the hyper-reflective epithelium sometimes obscured the plane of cleavage (red dots). (C) ICGA showed both focal pattern intratumoral vessels clearly (red arrow). (D) Leakage from the tumor was observed via FA. (E) The tumor completely disappeared after treatment, with palpebral fissures remaining in the primary tumor area (red arrow). (F) No clinical signs of the lesion were present on the AS-OCT image (red dots). (G) Both intratumoral vessels and conjunctival feeding vessels disappeared, and only the patched ischemic region remained (red arrow), evident on anterior segment ICGA images, after treatment. (H) No leakage was found using FA after treatment. Abbreviations: AS-OCT, anterior segment optical coherence tomography; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography. |
 | Figure 6 Anterior segment images of Case 5 (left eye). (A) A papillomatous red tumor involving the temporal cornea and limbus (red arrow), with corneal grey and white elevation and central cavitation (black arrow). (B) A palpebral fissure was found in the nasal quadrant (red arrow). (C) The tumor completely disappeared after treatment, with tiny palpebral fissures remaining. (D) AS-OCT demonstrated an abrupt transition between unremarkable and thickened hyper-reflective epithelia. However, in this large lesion, a shadow from the hyper-reflective epithelium sometimes obscured that plane of cleavage (red dots) and a small plane of cleavage between the lesion and the underlying tissue in cornea (yellow dots region). (E) The neoplasm completely resolved, with palpebral fissures remaining after treatment (red dots). (F) The leakage from both the tumor and its feeding vessels (red arrow), as well as corneal neovascularization (black arrow) was observed through FA. (G) ICGA results showed both seafan-shaped intratumoral vessels and conjunctival feeding vessels (red arrow) clearly, as well as corneal neovascularization (black arrow). (H) No leakage was found, and the regression of corneal neovascularization was observed after treatment via FA. (I) Intratumoral vessels, conjunctival feeding vessels, and corneal neovascularization disappeared; only a patched ischemic region remained (red arrow) visible on anterior segment ICGA images after treatment.Abbreviations: AS-OCT, anterior segment optical coherence tomography; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography. |
 | Figure 7 Anterior segment images of Case 6 in her right eye. (A) A gray white gelatinous tumor involving the nasal cornea and limbus with corneal edema (red arrow). (B) A gray white gelatinous tumor involving the nasal cornea and limbus with pterygium and corneal edema (red arrow); this is the same eye as that in A but from a different perspective. (C) The tumor partially resolved after treatment with only pterygium remaining (red arrow); the previous corneal edema disappeared. (D) Leakage from both the tumor and its feeding vessels was observed on FA results. (E) ICGA images showed both seafan-shaped intratumoral vessels and conjunctival feeding vessels clearly. (F) AS-OCT demonstrated a sharp delineation between normal and abnormal epithelia and a thickened and hyperreflective epithelium, as well as a plane of cleavage between the lesion and the underlying tissue (red dots). (G) AS-OCT results demonstrated that the neoplasm was partially resolved after treatment (red dots). (H) FA results showed that both tumor-related vessels and their leakage reduced partially. (I) Anterior segment ICGA results showed both iris vessels and tumor-related vessels, with the latter regressing to some extent. The number of residual vessels was reduced. (J) Dye leakage from corneal edema was observed via FA in the late stage.Abbreviations: AS-OCT, anterior segment optical coherence tomography; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography. |
In five cases, OSSN disappeared completely without recurrence, and in one case, OSSN had regressed partially at her last visit. Punctuate epithelial erosion was seen in six patients at 4–6 weeks post-treatment and, in one patient with diabetes, at 2 weeks post-treatment. All cases complicated with PEE were cured by 0.3% sodium hyaluronate eye drops or bandage contact lenses. No other side effects were observed during the study period.
For the six normal fellow eyes, no intratumoral abnormal vasculature with conjunctival feeding vessels were observed by ICGA. Similarly, there was also no vascular leakage determined by FA. Correspondingly, AS-OCT demonstrated a normal-appearing cornea, limbus, and conjunctiva with a bright white tear-film layer overlay.
Discussion
The most common clinical presentation for OSSN is an elevated, vascularized lesion in the limbal region.14 However, the angiographic characteristics of OSSN in vivo have not been reported previously. In the present study, we observed intratumoral vessels, conjunctival feeding vessels, and vascular leakage using both ICGA and FA in six eyes with OSSN. Furthermore, we demonstrated the regression of vascular leakage, focal and seafan-shaped intratumoral vessels, and conjunctival feeding vessels in five eyes, and the formation of patched ischemic regions in three eyes treated with perilesional subconjunctival 5-fluorouracil injections. The intratumoral and conjunctival feeding vessels disappeared partially on ICGA images, and vascular leakage from the intratumoral vessels was relieved partially, based on FA, in one patient. Moreover, late stage FA revealed the presence of intratumoral vessels induced cornea edema and leakage in this case. Two possible reasons attribute to the presence of corneal edema. First, 5-fluorouracil injection induced PEE, which was common in tropical 5-fluorouracil cases and led to the destruction of the corneal epithelial barrier, causing corneal edema. Second, during the regression duration of OSSN after treatment, the intratumoral vessels atrophied partially and the tight junction between the vascular endothelial cells was broken, increasing vascular leakage and triggering secondary corneal edema. The application of anterior segment angiography offered a new perspective on the pathogenesis.
Vajzovic et al reported that ultra-high-resolution OCT of an OSSN lesion shows epithelial thickening and increased reflectivity of the epithelium with a distinct delineation of the tumor from nonaffected tissue.18 Similarly, we found that there was an abrupt transition between normal and abnormal epithelium, as a rapid increase in both brightness and thickness of the epithelium, thickened hyper-reflective epithelium, and a sharp plane of cleavage between the lesion and underlying tissue in two cases. However, in four cases, because of large lesions, a shadow from the hyper-reflective epithelium obscured the plane of cleavage. Moreover, we measured the largest thickness of OSSN by AS-OCT before the injections, and found that the median thickness was 905.0 (interquartile range: 492.0–1592.5) μm, which was greater than the thickness of 390 (124–1000) μm reported by Nanji et al.6 The increased OSSN thickness indicated that subconjunctival/perilesional 5-fluorouracil injections should be used for a higher penetration of drugs. Moreover, an epithelial thickness cutoff at >120 μm provided 100% sensitivity and specificity for differentiating OSSN from pterygia.6 AS-OCT prevented potentially premature cessation of topical treatments, which could have increased the risk of recurrent disease.5 There was a median delay between clinical and OCT resolution of approximately 16 weeks, with the longest delay being approximately 29 weeks.19 In our study, neoplasms were completely replaced by normal epithelia after treatment on AS-OCT in five of six cases. Also, there was a bright white tear-film layer overlying the cornea and conjunctiva.
5-Fluorouracil is a structural analogue of thymine, which inhibits deoxyribonucleic acid (DNA) formation by blocking the enzyme thymidylate synthetase. Rapidly multiplying cells, such as tumor cells, require more DNA and ribonucleic acid (RNA) than normal cells and therefore take up larger amounts of 5-fluorouracil, allowing selective targeting of cancerous lesions.20 Topical 5-fluorouracil is effective in the treatment of preinvasive ocular surface neoplasias14 and recurrent, incompletely excised, and selected untreated conjunctival squamous cell carcinomas.21 Gichuhi S, et al reported that topical fluorouracil after surgery substantially reduced recurrence of OSSN, was well-tolerated, and its use was recommended.8 Moreover, 5-fluorouracil has several theoretical advantages over mitomycin C and interferon alpha-2b including a lower cost of treatment, no requirements for refrigeration, and less-frequent dosing regimens.22 Additionally, the time to tumor resolution is generally faster with subconjunctival injections (average 1.4 months) as compared to topical interferon alpha-2b drops (average 2.8 months).13 Thus, subconjunctival perilesional 5-fluorouracil injections were used in our study. Advantages of this drug delivery include higher drug penetration, and perhaps a more direct delivery of 5-fluorouracil to the tumor site, more rapid tumor resolution, and ensured compliance when compared with topical 5-fluorouracil drops. Joag et al reported that nasal location was the only risk factor of non-response to therapy.20 Similarly, in our study, the partially recovered case had nasal location, with intratumoral and conjunctival feeding vessels.
However, frequent injections (twice a week in the first phase) did not cause any side effects in the present study. Patient compliance was reasonable and acceptable. Similarly, Karp CL, et al13 also mentioned that the initial cohort of patients injected with IFN α-2b thrice weekly, but because thrice weekly injections were difficult for the patient and physician, the routine was changed thereafter received weekly injections until clinical disease resolution. Moreover, the injection was conducted 3 mm outside of the cornea limbus, avoiding direct damage to limbal stem cells in our study.
Chaugule et al reported that the BCVA of giant OSSN eyes was stable or improved at the last visit after treatment with either 5-fluorouracil or interferon alpha-2b.23 Similarly, in the present study, the BCVA improved after treatment, which may due to better anatomic outcomes, regression of intratumoral and conjunctival feeding vessels, and less severe side effects. The most common side effect of topical 5-fluorouracil is pain, followed by tearing, photophobia, itching, swelling, and infection.20 In our study, the only side effect was PEE accompanied by a foreign body sensation and photophobia, which occurred at the first phase of injection, and gradually improved during the second and third phases, possibly because the focal perilesional subconjunctival injections impeded drug diffusion to surrounding normal tissue. Subconjunctival 5-fluorouracil was not complicated by side effects such as fever, chills, headache, myalgias, and arthralgias, which were seen with subconjunctival interferon alpha-2b.13
Since OSSN can recur years after treatment, follow-up is of high importance in continuing to evaluate the efficacy and side effects of various therapies. Madhura et al reported that recurrence rates at 1 and 2 years were 6% and 15%, respectively.20 In our study, recurrence was not observed in five of six patients at their last visit, suggesting improved drug delivery. Long-term follow-up should be performed in future investigations.
The main limitations of this study included the small cohort. Moreover, the lack of controls is a major source of bias, and a case series is weak evidence to support the efficacy of a new treatment modality. Thus, a larger study is being prepared in the future to confirm our present, preliminary findings.
Conclusion
OSSN consisted of focal and seafan-shaped intratumoral vessels with leakage and conjunctival feeding vessels, corresponding to the thickened hyper-reflective epithelium observed by AS-OCT. Improved perilesional subconjunctival 5-fluorouracil injections are an effective therapy for OSSN, as confirmed by the progression of abnormal vessels in angiography and the gain in BCVA.
Role of the funding source
The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Abbreviation list
AS-OCT, anterior segment optical coherence tomography; BCVA, best-corrected vision acuity; DNA, deoxyribonucleic acid; FA, fluorescein angiography; ICGA, conjunctival indocyanine green angiography; LSCD, limbal stem cell deficiency; LogMAR, logarithm of the minimum angle of resolution, OCT, optical coherence tomography; OSSN, ocular surface squamous neoplasia; PEE, punctuate epithelial erosion; RNA, ribonucleic acid.
Acknowledgments
We thank Prof. Guangping Wu, PhD (Department of Pathology, The First Affiliated Hospital of China Medical University) for the exfoliative cytology in this study. This study was funded by the Natural Science Foundation of Liaoning Province (No.20170541041), Fund for Scientific Research of The First Hospital of China Medical University (No. FSFH201712), and Clinical Genetics (Ophthalmology) Subject construction project of China Medical University (No.3110118049).
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee GA, Hirst LW. Ocular surface squamous neoplasia. Surv Ophthalmol. 1995;39:429–450. doi:10.1016/S0039-6257(05)80054-2
2. Erie JC, Campbell RJ, Liesegang TJ. Conjunctival and corneal intraepithelial and invasive neoplasia. Ophthalmology. 1986;93:176–183. doi:10.1016/S0161-6420(86)33764-3
3. Yousef YA, Finger PT. Squamous carcinoma and dysplasia of the conjunctiva and cornea: an analysis of 101 cases. Ophthalmology. 2012;119:233–240. doi:10.1016/j.ophtha.2011.08.005
4. Gichuhi S, Sagoo MS, Weiss HA, Burton MJ. Epidemiology of ocular surface squamous neoplasia in Africa. Trop Med Int Health. 2013;18:1424–1443. doi:10.1111/tmi.12203
5. Ong SS, Vora GK, Gupta PK. Anterior segment imaging in ocular surface squamous neoplasia. J Ophthalmol. 2016;2016:5435092. doi:10.1155/2016/5435092
6. Nanji AA, Sayyad FE, Galor A, Dubovy S, Karp CL. High-resolution Fourier-domain optical coherence tomography as an adjunctive tool in the diagnosis of corneal and conjunctival pathology. Ocul Surf. 2015;13:226–235. doi:10.1016/j.jtos.2015.02.001
7. Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol. 2004;49:3–24. doi:10.1016/j.survophthal.2003.10.008
8. Gichuhi S, Macharia E, Kabiru J, et al. Fluorouracil after surgery for ocular surface squamous neoplasia in Kenya: a randomised, double-blind, placebo-controlled trial. Lancet Glob Health. 2016;4(6):e378–e385. doi:10.1016/S2214-109X(16)30052-3
9. Bahrami B, Greenwell T, Muecke JS. Long-term outcomes after adjunctive topical 5-flurouracil or mitomycin C for the treatment ofsurgically excised, localized ocular surface squamous neoplasia. Clin Exp Ophthalmol. 2014;42(4):317–322. doi:10.1111/ceo.12184
10. Parrozzani R, Frizziero L, Trainiti S, et al. Topical 1% 5-fluorouracil as a sole treatment of corneoconjunctival ocular surface squamous neoplasia: long-term study. Br J Ophthalmol. 2017;101:1094–1099. doi:10.1136/bjophthalmol-2016-309219
11. Dudney BW, Malecha MA. Limbal stem cell deficiency following topical mitomycin C treatment of conjunctival-corneal intraepithelial neoplasia. Am J Ophthalmol. 2004;137:950–951. doi:10.1016/j.ajo.2003.10.048
12. Asoklis RS, Damijonaityte A, Butkiene L, et al. Ocular surface reconstruction using amniotic membrane following excision of conjunctival and limbal tumors. Eur J Ophthalmol. 2011;21:552–558. doi:10.5301/EJO.2010.6192
13. Karp CL, Galor A, Chhabra S, Barnes SD, Alfonso EC. Subconjunctival/perilesional recombinant interferon α2b for ocular surface squamous neoplasia: a 10-year review. Ophthalmology. 2010;117:2241–2246. doi:10.1016/j.ophtha.2010.03.052
14. Kim JW, Abramson DH. Topical treatment options for conjunctival neoplasms. Clin Ophthalmol. 2008;2:503–515. doi:10.2147/OPTH.S1606
15. Gelender H, Forster RK. Papanicolaou cytology in the diagnosis and management of external ocular tumors. Arch Ophthalmol. 1980;98:909–912.
16. Shousha MA, Karp CL, Perez VL, et al. Diagnosis and management of conjunctival and corneal intraepithelial neoplasia using ultra high-resolution optical coherence tomography. Ophthalmology. 2011;118:1531–1537. doi:10.1016/j.ophtha.2011.01.005
17. Gurung NK, Gautam P, Gurung S, Bhattarai B. Comparison of phacotrabeculectomy and phacotrabeculectomy with subconjunctival 5-Fluorouracil. J Nepal Med Assoc. 2014;52:1010–1013.
18. Vajzovic LM, Karp CL, Haft P, et al. Ultra high-resolution anterior segment optical coherence tomography in the evaluation of anterior corneal dystrophies and degenerations. Ophthalmology. 2011;118:1291–1296.
19. Thomas BJ, Galor A, Nanji AA, et al. Ultra high-resolution anterior segment optical coherence tomography in the diagnosis and management of ocular surface squamous neoplasia. Ocul Surf. 2014;12:46–58. doi:10.1016/j.jtos.2013.11.001
20. JoagMG, SiseA, MurilloJC, et al. Topical 5-fluorouracil 1% as primary treatment for ocular surface squamous neoplasia. Ophthalmology. 2016;123:1442–1448. doi:10.1016/j.ophtha.2016.02.034
21. Midena E, Angeli CD, Valenti M, de Belvis V, Boccato P. Treatment of conjunctival squamous cell carcinoma with topical 5-fluorouracil. Br J Ophthalmol. 2000;84:268–272. doi:10.1136/bjo.84.3.268
22. Reynolds JE, Martindale W. Martindale: The Extra Pharmacopoeia.
23. Chaugule SS, Park J, Finger PT. Topical chemotherapy for giant ocular surface squamous neoplasia of the conjunctiva and cornea: is surgery necessary? Indian J Ophthalmol. 2018;66:55–60. doi:10.4103/ijo.IJO_286_18
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.