Back to Journals » Clinical Optometry » Volume 18
Ocular Dimensional Changes After 12 Months of Orthokeratology and Single-Vision Spectacle Use: A Three-Dimensional Magnetic Resonance Imaging Study
Authors Low YC, Mohd-Ali B ![]() , Shahimin MM
, Shahimin MM ![]() , Mohidin N, Wan Abdul Halim WH
, Mohidin N, Wan Abdul Halim WH ![]() , Mokri SS, Abdul-Hamid H
, Mokri SS, Abdul-Hamid H
Received 9 April 2026
Accepted for publication 16 June 2026
Published 14 July 2026 Volume 2026:18 611080
DOI https://doi.org/10.2147/OPTO.S611080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
Yu Chen Low,1 Bariah Mohd-Ali,1 Mizhanim Mohamad Shahimin,1 Norhani Mohidin,1 Wan Haslina Wan Abdul Halim,2 Siti Salasiah Mokri,3 Hamzaini Abdul-Hamid4
1Department of Optometry and Vision Science & Research Centre for Community Health (REACH), Faculty of Health Sciences, UKM, Kuala Lumpur, Malaysia; 2Department of Ophthalmology, Faculty of Medicine, UKM, Kuala Lumpur, Malaysia; 3Department of Electrical, Electronics and System, Faculty of Engineering, UKM, Bangi Selangor, Malaysia; 4Department of Radiology, Faculty of Medicine, UKM, Kuala Lumpur, Malaysia
Correspondence: Bariah Mohd-Ali, Optometry and Vision Science Program, Research Centre for Community Health (REACH), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia, Tel +603 89213032, Email [email protected]
Purpose: This study investigated the 12-month impact of orthokeratology (Ortho-K) treatment on eyeball dimensions using magnetic resonance imaging (MRI). Results were compared with single-vision spectacle wearers (SVS).
Patients and Methods: A total of 70 Chinese schoolchildren (mean age: 8.31 ± 0.47 years) with myopia were assigned to Ortho-K (n = 45) and SVS (n = 25). Baseline spherical equivalent (SE), visual acuity (VA), and flat keratometry (FK) were measured. MRI was performed at baseline and at 12 months to measure three-dimensional ocular dimensions, including longitudinal axial length (LAL), horizontal width (HW), and vertical sagittal height (VSH). Standard slit-lamp examinations ensured ocular health at all follow-up visits.
Results: At 12 months, the Ortho-K group showed significant reductions in SE and FK (p < 0.001), whereas the SVS group exhibited a significant increase (p < 0.05). LAL was significantly shorter in the Ortho-K group compared to SVS (p < 0.05). Although individual HW and VSH did not reach independent significance, repeated measures analysis of variance confirmed significant between-group differences in global eyeball shape over 12 months (p < 0.05). Correlation analysis revealed a significant association between SE and LAL in the SVS group (p < 0.05). In the Ortho-K group, SE showed no significant correlation with ocular dimensional changes (p > 0.05). In contrast, FK in the Ortho-K group demonstrated significant correlations with all dimensional parameters (p < 0.05), a pattern not observed in the SVS group.
Conclusion: Findings indicate that myopic progression in the SVS group is primarily driven by axial elongation, whereas refractive changes in the Ortho-K group arise from corneal reshaping. Over 12 months, Ortho-K wear modifies ocular dimensions and inhibits AL elongation more significantly than SVS, providing a structural basis for controlling myopic progression.
Keywords: orthokeratology, myopia control, MRI, axial length, ocular dimension, myopia
Introduction
Myopia is a growing global public health concern, with rapidly increasing prevalence worldwide, particularly in East and Southeast Asia, where rates among school-aged children may exceed 50–80%.1 A recent local study indicates that at least 40% of Malaysian children and adolescents aged 13 to 18 likely have myopia, specifically females, individuals of Chinese ethnicity, and youth between the ages of 7 and 18.2 As myopia develops, the eye undergoes a transition toward a prolate profile due to disproportionate axial elongation, expanding 3.5 times faster in length (0.35 mm/D) than in width (0.10 mm/D).3 Such axial stretching causes the posterior pole to steepen relative to the periphery, creating a prolate-like ellipsoid that induces peripheral hyperopic defocus, in which light focuses behind the retina and signals further elongation.4
Orthokeratology (Ortho-K) is a reversible corneal reshaping treatment that slows myopia progression in children. Meta-analyses of randomized and controlled clinical trials have consistently demonstrated that Ortho-K significantly reduces axial elongation compared with single-vision spectacle (SVS) correction, supporting its effectiveness as a myopia control intervention in pediatric populations.5 Modern Ortho-K lenses employ a reverse-geometry design that flattens the central cornea while steepening the mid-peripheral cornea; thereby, inducing peripheral myopic defocus. This optical profile has been hypothesized to influence ocular growth patterns beyond axial length (AL) alone, potentially modifying peripheral retinal signaling mechanisms associated with myopia progression.6
To date, most studies investigating ocular changes associated with Ortho-K have relied on indirect measures, such as peripheral refraction, to infer alterations in eye shape.7 A previous study evaluated changes in eye shape following Ortho-K treatment using biometric measurements from Lenstar LS900 to assess peripheral eye length. Over a 12-month period, the authors reported reduced prolateness and increased symmetry compared with SVS wear.
In a subsequent study utilizing magnetic resonance imaging (MRI) to measure peripheral eye length (PEL), children in the Ortho-K group exhibited distinct differential growth patterns compared to the SVS cohort.8 Specifically, PEL at the nasal eccentricity increased more rapidly than all other peripheral and axial lengths (p<0.05). These findings demonstrate that while SVS wearers developed an increasingly prolate eye shape alongside myopia progression, Ortho-K wearers maintained a significantly less prolate ocular profile over the 12-month observation period.
Building upon previous findings, this study expands the investigation by using MRI to directly quantify global ocular dimensions and shape changes after 12 months of Ortho-K and SVS wear in myopic children. Through MRI-based 3D modeling of ocular geometry, the eyeball was analyzed as a whole, specifically assessing changes in axial length, height, and width. This comprehensive approach enables evaluation of both global and peripheral dimensional changes, providing robust structural evidence for the myopic defocus theory by correlating these alterations with previously reported refractive outcomes.8,9 Furthermore, this study examines whether Ortho-K is associated with distinct patterns of ocular dimensional and corneal curvature (D) changes compared with conventional SVS treatment over the study period.
Materials and Methods
Ethical Approval and Informed Consent
The study was approved by the University Kebangsaan Malaysia Research Ethics Committee (UKM PPI-800-1/1/5 JEP-2017-422) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from the parents or legal guardians of all participants.
Sample Size Calculation
Sample size was calculated using G*Power (version 3.1.9.3; Heinrich Heine University, Düsseldorf, Germany) based on previous data reporting AL changes of 0.36 mm (standard deviation [SD] = 0.24 mm) after 2 years of Ortho-K treatment.10 To detect a 0.24 mm difference in AL (SD = 0.24 mm; α = 0.05; power = 0.95), 14 participants per group were required. Accounting for a 17% dropout rate, at least 25 participants per group were recruited to maintain statistical power.
Study Participants
Seventy schoolchildren with myopia (35 females, 35 males) aged 8–9 years, with a myopia duration of at least 6 months, were recruited. Inclusion criteria required a best-corrected visual acuity (BCVA) of 0.0 logarithm of the minimum angle of resolution (logMAR) or better in both eyes, normal ocular and systemic health, a cycloplegic spherical equivalent (SE) refractive error between –0.75 and –4.00 D, and astigmatism ≤ –1.50 DC. All subjects have no history of wearing contact lenses, Ortho-K lenses or prior myopia control spectacles treatment. Group allocation to Ortho-K or SVS control was determined by parental preference.
Examinations and Measurements
Participants in the SVS group were prescribed full-time single-vision distance spectacles (refractive index 1.56; Integrated Lens Technology, Singapore). Prescriptions were updated if monocular aided visual acuity reached ≥0.18 logMAR or if the SE refraction changed by ≥–0.50 D. The Ortho-K group was fitted with overnight Ortho-K lenses (Z Night; Menicon, Nagoya, Japan) using proprietary software (Easyfit; Menicon) based on corneal topography and cycloplegic refraction. Baseline study methods and interventions have been previously described.8 Specific procedures for ocular dimensional measurements following 12 months of Ortho-K lens wear are detailed below.
MRI Segmentation
MRI datasets were analyzed using custom software developed in MATLAB (MathWorks, Natick, MA, USA) by a multidisciplinary team of engineers based on the Chan-Vese model.11 This approach offers computational efficiency, accurately resolving complex boundary curves and handling intricate geometric constraints such as angle production and curvature.12
Images were displayed and magnified using a commercially available DICOM viewer (OsiriX; Pixmeo SARL, Geneva, Switzerland). Axial images were viewed at 50X magnification, with contrast adjusted to optimize edge definition. To confirm the measurement standards, a 10 mm scale bar was utilized within the OsiriX DICOM viewer to ensure all calculations remained in millimeters (mm) and the raw data were processed and displayed using a square pixel (1:1) aspect ratio. The axial plane was reconstructed using 200 iterations due to its high symmetry and uniform shape allow the algorithm to efficiently produce high-quality images with minimal noise (Figure 1). In contrast, the sagittal view required 300 iterations to manage the increased anatomical complexity of the orbit: such as the eyelids and curved orbital floor, and to filter out vertical motion artifacts (Figure 2). Following these procedures, pertinent linear dimensions for the assessment of peripheral eye length (PEL) at 10° intervals and eyeball shape (longitudinal AL (LAL), horizontal width [HW], vertical sagittal height [VSH]) were automatically measured and analyzed (Figure 3). The reliability and measurement precision of these MRI-based ocular measurements have been previously established and reported in an MRI validation study.13
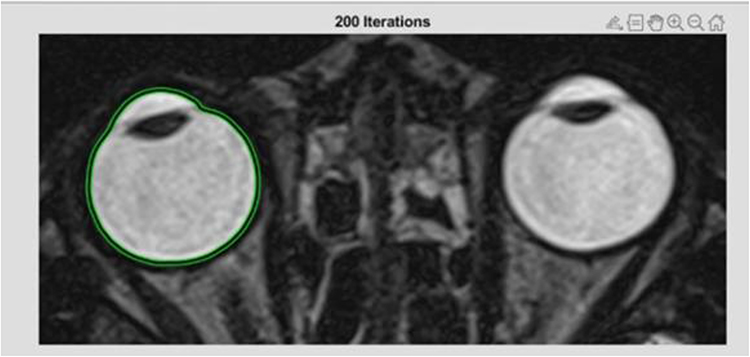 |
Figure 1 Axial orbital MRI. Green line - Delineation of the selected eyeball boundary in the axial plane, indicating the region of interest used for analysis. |
 |
Figure 2 Sagittal orbital MRI. Green line- Delineation of the selected eyeball boundary in the sagittal plane, indicating the region of interest used for analysis. |
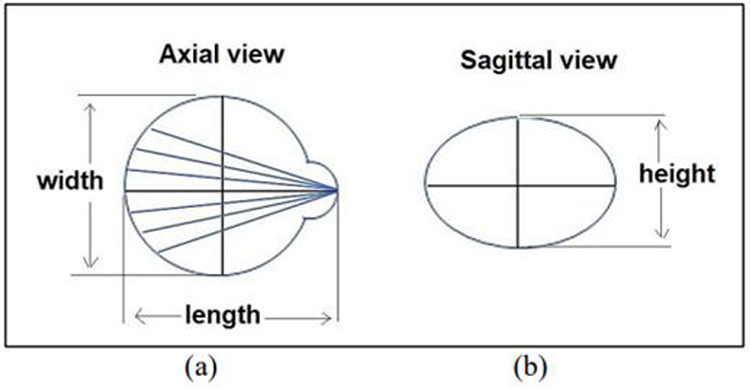 |
Figure 3 Schematic diagram of eyeball dimensions. (a) Axial view showing the measurement of ocular width, peripheral eye length and axial length. (b) Sagittal view showing the measurement of ocular height. |
All statistical analyses were performed using SPSS software (version 21.0; IBM Corp., Armonk, NY, USA). To account for potential inter-eye correlation, differences between right and left eye were initially evaluated using paired t-tests. As the variance between eyes was smaller than the variance between participants, only right eye data were included in the final analysis to avoid underestimation of true variance and inflation of Type I error. Normality of baseline demographic, refractive, and biometric variables was assessed using the Shapiro–Wilk test, whereas homogeneity of variance was evaluated using Levene’s test. Participant demographics were analyzed using frequencies and sample descriptive tests. Within-group comparisons before and after Ortho-K and SVS interventions were performed using paired t-tests. Longitudinal changes from baseline to 12 months were analyzed using one-way repeated-measures analysis of variance (ANOVA). Between-group differences were assessed using independent t-tests, with statistical significance set at p < 0.05. Spearman correlation was performed to examine relationships between SE, D, and ocular dimensional changes in the eyes of children with myopia.
Results
Demographic Data
No significant differences in baseline data were observed between the Ortho-K and SVS groups regarding age, sex, BCVA, SE, D, PEL, LAL, HW, or VSH (p > 0.05). Participants’ demographic data are summarized in Table 1.
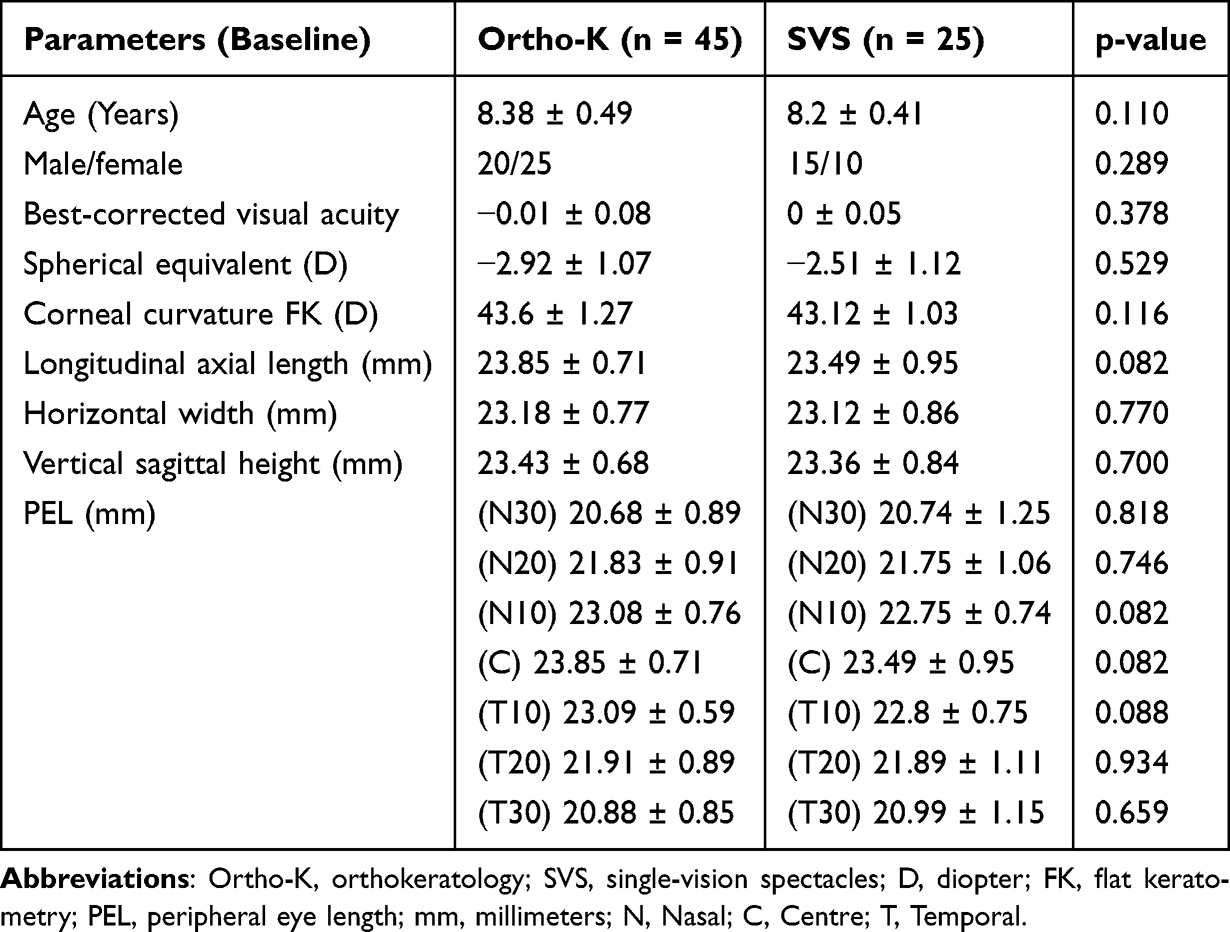 |
Table 1 Participant Demographics |
Refractive Components at Baseline and 12 Months
Baseline and 12-month refractive data for the Ortho-K and SVS groups are summarized in Table 2. After 12 months, the Ortho-K group demonstrated significant reductions in SE (from −2.92 ±1.07D to −0.06 ± 0.12D; p < 0.05) and flat keratometry FK (from 43.6 ± 1.27D to 40.69 ± 2.54D; p < 0.05). Conversely, the SVS group exhibited a significant increase in both SE (from −2.51 ± 1.12D to −3.77 ± 1.23D, p < 0.05) and FK (from 43.12 ± 1.03D to 43.47 ± 1.10D, p < 0.05) over the same period.
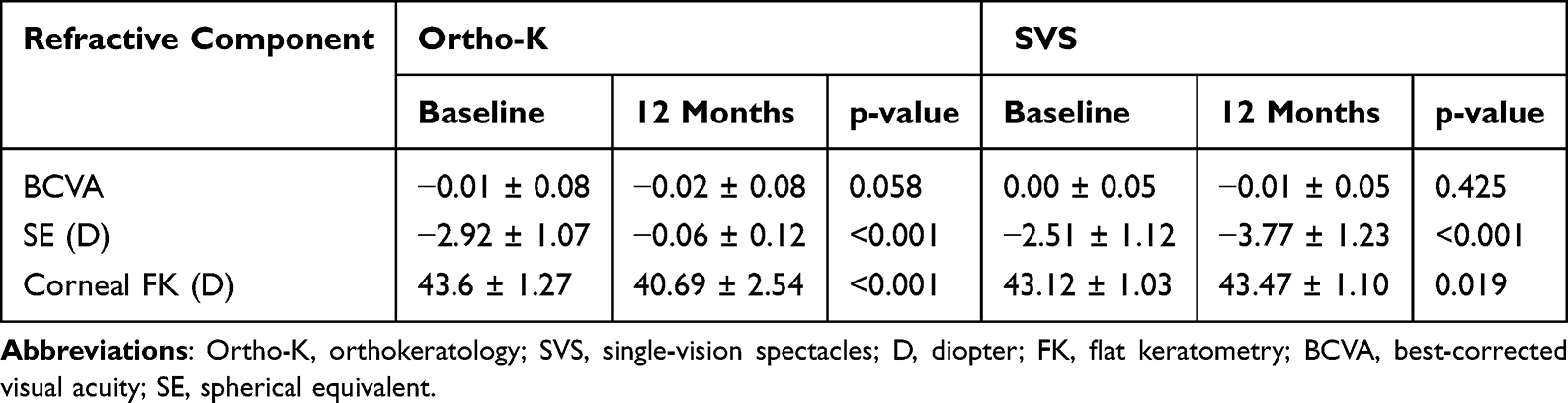 |
Table 2 Refractive Components in the Ortho-K and SVS Groups at Baseline and 12 Months |
Ocular Dimensions at Baseline and 12 Months
In the SVS group, LAL increased significantly over the 12-month period (23.45 ± 0.97 to 23.97 ± 0.59 mm; p < 0.05), while HW and VSH exhibited non-significant upward trends. Additionally, the SVS group demonstrated significantly increased PEL at all measured horizontal eccentricities (p < 0.05), except at N30. In contrast, the Ortho-K group showed significant PEL elongation only beyond 20° eccentricities, specifically at N20, N30, T20, and T30 (p < 0.05), with no significant elongation observed at N10 and T10. Rather, a significant reduction in LAL was detected in the Ortho-K group compared with baseline (23.85 ± 0.71 mm to 23.64 ± 0.74 mm; p < 0.05), whereas HW and VSH displayed downward trends that did not reach statistical significance (Table 3).
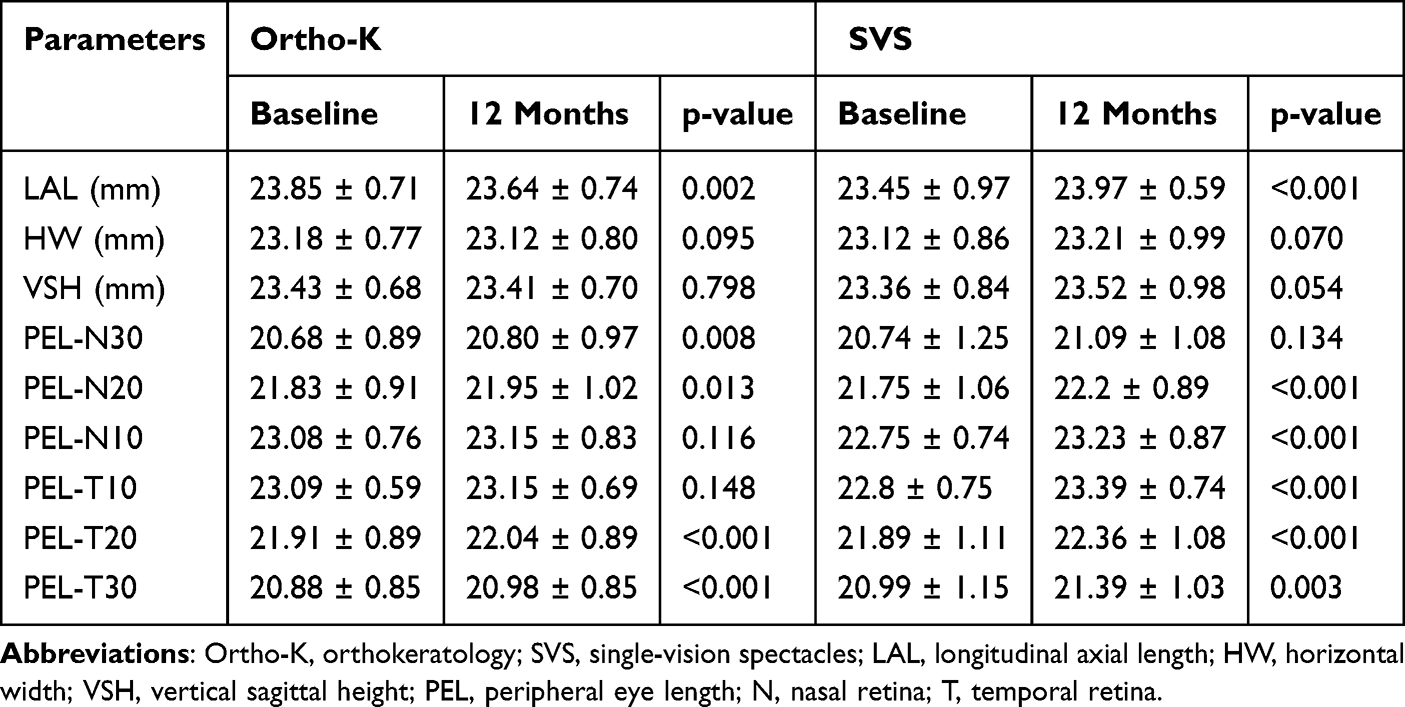 |
Table 3 Within-Group Eyeball Shape Measurements in Ortho-K and SVS Participants at 12 Months |
Within-Group Changes in Ocular Shape
Repeated measures ANOVA revealed significant changes in the overall eyeball shape within both the Ortho-K and SVS groups over 12 months (p < 0.05). At the 12-month follow-up, significant differences were observed among the three ocular biometric parameters in both the Ortho-K and SVS groups. In the Ortho-K group, the mean longitudinal axial length (LAL) was 23.64 ± 0.74 mm, which was significantly greater than both horizontal width (HW; 23.12 ± 0.80 mm) and vertical sagittal height (VSH; 23.41 ± 0.70 mm). Pairwise comparisons with Bonferroni adjustment indicated that all three parameters differed significantly from one another (p<0.05). In the SVS group, the mean LAL was 23.97 ± 0.59 mm, while HW and VSH were 23.21 ± 0.99 mm and 23.52 ± 0.98 mm, respectively. Bonferroni-adjusted pairwise comparisons showed that LAL differed significantly from both HW and VSH (p<0.05), whereas no significant difference was found between HW and VS (Table 4).
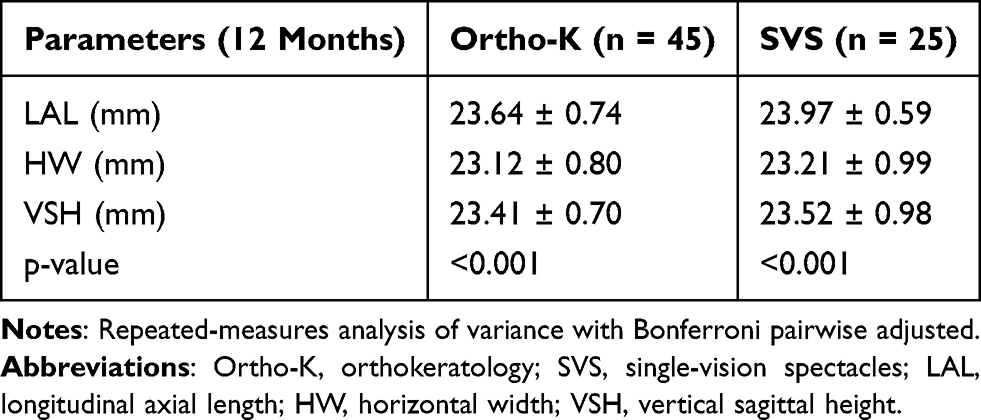 |
Table 4 Within-Group Eyeball Shape Changes Over 12 Months in Ortho-K and SVS Participants |
Between-Group Comparisons of Ocular Dimensions
At 12 months, independent t-tests indicated significant differences in the eyeball shape between the Ortho-K and SVS groups. The mean LAL was significantly lower in the Ortho-K group (23.64 ± 0.74 mm) compared to the SVS group (23.97 ± 0.59 mm) (p < 0.05). In contrast, no significant differences were observed between the two groups for horizontal width (HW) or vertical sagittal height (VSH). The mean HW values were 23.12 ± 0.80 mm in the Ortho-K group and 23.21 ± 0.99 mm in the SVS group (p = 0.698), while the mean VSH values were 23.41 ± 0.70 mm and 23.52 ± 0.98 mm, respectively (p = 0.650) (Table 5).
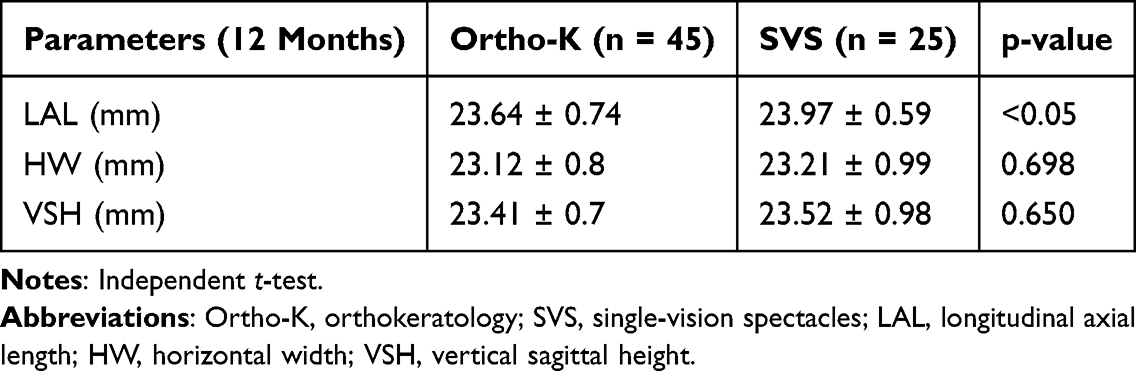 |
Table 5 Between-Group Eyeball Shape Comparison at 12 Months |
Correlation of Spherical Equivalent with Ocular Dimensions
In the Ortho-K group, changes in SE did not show significant correlations with LAL, HW, or VSH (all p > 0.05) (Table 6). In the SVS group, SE showed a significant positive correlation with LAL only (p < 0.05), with no significant associations with HW or VSH (Table 7).
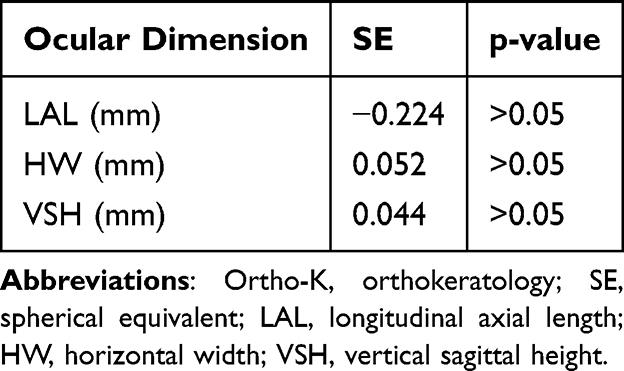 |
Table 6 Correlation Between Changes in SE and Ocular Dimensions in the Ortho-K Group |
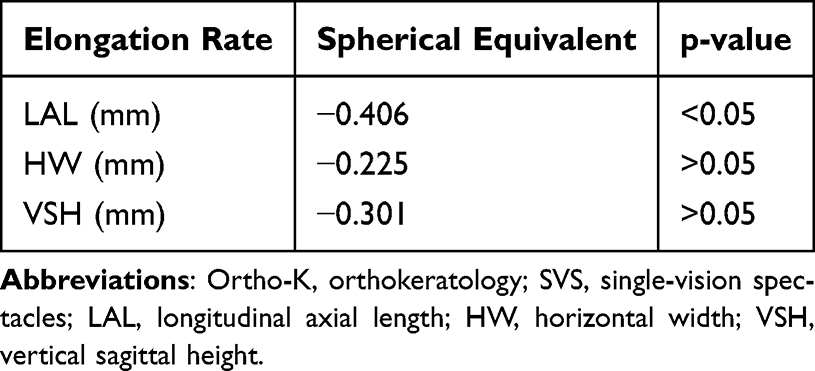 |
Table 7 Correlation Between Changes in SE and Ocular Dimensions in the SVS Group |
Correlation of Corneal Curvature with Ocular Dimensions
In the Ortho-K group, changes in FK were significantly correlated with all measured ocular dimensions (LAL, HW, VSH; all p < 0.05) (Table 8). In the SVS group, FK showed no significant correlations with any ocular dimensions (all p > 0.05), with the exception of SE showing a significant correlation with LAL (Table 9).
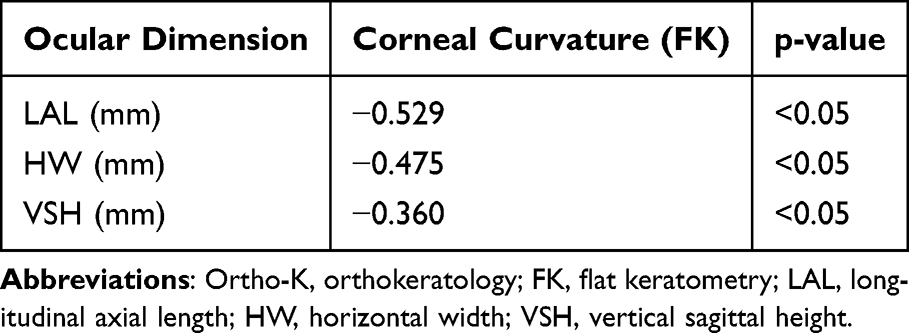 |
Table 8 Correlation Between Changes in Corneal Curvature (FK) and Ocular Dimensions in the Ortho-K Group |
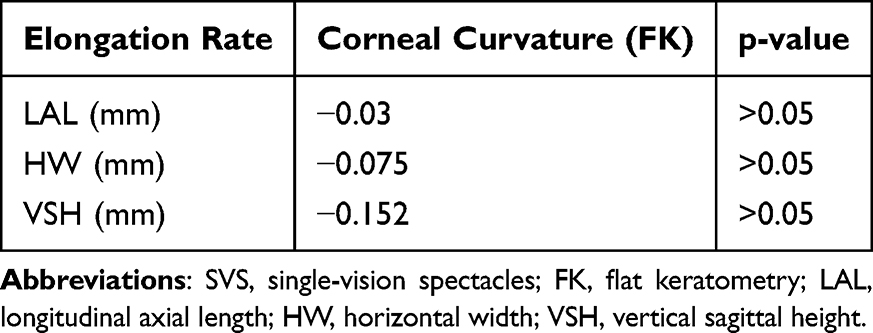 |
Table 9 Correlation Between Changes in Corneal Curvature (FK) and Ocular Dimensions in the SVS Group |
Discussion
This study examined 3D ocular dimensional changes in children with myopia after 12 months of Ortho-K lens wear and compared these changes with those of children wearing SVS. The SVS group served as a reference for the natural progression of childhood myopia without myopia control intervention.
At baseline, all participants with myopia exhibited a prolate globe morphology, with LAL as the dominant dimension, followed by VSH and HW. This pattern aligns with the axial expansion model described by Atchison et al3 and Matsumura et al14 Over 12 months, the SVS group demonstrated expansion across all ocular dimensions The most pronounced increase occurred in LAL (p < 0.05), followed by significant elongation of PEL at N20, N10, T10, T20, and T30 (all p < 0.05), reflecting overall prolate ocular growth. In contrast, the Ortho-K group exhibited a shift toward a less prolate ocular profile. These findings extend previous research10 reporting axial shortening accompanied by peripheral expansion between 10° and 30°. However, while the Ortho-K lens successfully halted LAL elongation, the stable transverse dimensions of HW and VSH indicate a less prolate ocular profile rather than a true global structural shift.
The results of this study also showed that in the Ortho-K group, significant PEL elongation occurred only beyond 20° peripheral eccentricity (N20, N30, T20, and T30; p < 0.05), accompanied by centre AL shortening (p<0.05). These findings indicate that Ortho-K treatment induces distinct structural modifications in the growing eye through central corneal flattening and mid-peripheral steepening,15 which collectively induce peripheral myopic defocus. By shifting the peripheral image shell anterior to the retina, this optical signal may act as a potent regulator of ocular growth, contributing to the reduced axial, horizontal, and vertical dimensions observed in the present Ortho-K cohort.16
The differential relationship between SE and AL observed in the SVS and Ortho-K groups further highlights the distinct mechanisms through which these modalities interact with ocular biometry. In the SVS group, changes in SE were significantly correlated with AL elongation, indicating that refractive progression was primarily driven by structural eye growth. Because spectacles do not alter ocular components such as the cornea or crystalline lens, the myopic shift largely results from axial elongation, with the retina moving posteriorly relative to the eye’s focal point.17,18 In contrast, this correlation was absent in the Ortho-K group, demonstrating a decoupling of SE and AL.19 The results indicate that Ortho-K lenses temporarily reshape the cornea by flattening the central epithelium and steepening the mid-periphery through reverse-geometry lens forces; thereby, neutralizing central refractive error. Consequently, changes in SE among Ortho-K wearers primarily reflect corneal reshaping rather than true axial elongation.8,15
To date, few studies have investigated the specific ocular dimensional changes associated with Ortho-K treatment.9,20 One study reported that central corneal flattening accompanied by peripheral corneal steepening leads to a more symmetric and less prolate ocular morphology in children with myopia.9 Another study suggested that Ortho-K lenses alter ocular tension dynamics, particularly by reducing tension in the posterior ciliary muscle–lens complex, which may explain the short-term axial shortening observed following treatment.20
Several limitations of this study warrant consideration. Firstly, the 12-month follow-up period restricts understanding of long-term structural trends; given that myopia management is a multi-year process, further longitudinal data is required to determine whether observed ocular changes persist or stabilize beyond the initial treatment period. Secondly, a key limitation of this study is that LAL measurements were not adjusted for the corneal flattening; since Ortho-K thins the central corneal epithelium by 10–20 microns,21 future studies should account for these corneal changes to ensure more accurate axial measurements. Thirdly, future research should explore the impact of varying treatment zone diameters on peripheral retinal contour to more clearly characterize the PEL data and evaluate its relationship with ocular dimension changes. Such investigations would provide critical data for the development of personalized Ortho-K algorithms; thereby, refining structural observations and optimizing customized lens geometries22 for enhanced long-term myopia control.
Conclusion
In summary, this study provides direct evidence of 3D ocular remodeling in children treated with Ortho-K, as quantified via MRI. Ortho-K slows axial elongation while actively modifying the global aspect ratio of the eye. By restricting LAL expansion to rates comparable with HW growth, Ortho-K effectively mitigates the pathological stretching and prolate distortion characteristic of rapid myopic progression.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Menicon Ltd., Japan (NN-2022-019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33(4 Suppl):27–9. doi:10.47102/annals-acadmedsg.V33N1p27
2. Tan ESY, Agarwal P, Teng CL. Prevalence of myopia in children and adolescents: a systematic review of Malaysian Prevalence Studies. Malays J Med Sci. 2026;33(1):14–26. doi:10.21315/mjms-08-2025-592
3. Atchison DA, Jones CE, Schmid KL, et al. Eye shape in emmetropia and myopia. Invest Ophthalmol Vis Sci. 2004;45(10):3380–3386. doi:10.1167/iovs.04-0292
4. Lau JK, Vincent SJ, Cheung SW, Cho P. Higher-order aberrations and axial elongation in myopic children treated with orthokeratology. Invest Ophthalmol Vis Sci. 2020;61(2):22. doi:10.1167/iovs.61.2.22
5. Si JK, Tang K, Bi HS, Guo DD, Guo JG, Wang XR. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015;92(3):252–257. doi:10.1097/OPX.0000000000000505
6. Smith EL. Optical treatment strategies to slow myopia progression: effects of the visual extent of the optical treatment zone. Exp Eye Res. 2013;114:77–88. doi:10.1016/j.exer.2012.11.019
7. Gifford KL, Gifford P, Hendicott PL, Schmid KL. Stability of peripheral refraction changes in orthokeratology for myopia. Cont Lens Anterior Eye. 2020;43(1):44–53. doi:10.1016/j.clae.2019.11.008
8. Low YC, Mohd-Ali B, Shahimin MM, Mohidin N, Abdul-Hamid H, Mokri SS. Peripheral eye length evaluation in myopic children undergoing orthokeratology treatment for 12 months using MRI. Clin Optom. 2024;16:35–44. doi:10.2147/OPTO.S448815
9. Huang Y, Li X, Ding C, Chen Y, Chen H, Bao J. Orthokeratology reshapes eyes to be less prolate and more symmetric. Cont Lens Anterior Eye. 2022;45(4):101532. doi:10.1016/j.clae.2021.101532
10. Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012;53(11):7077–7085. doi:10.1167/iovs.12-10565
11. Chan TF, Vese LA. Active contours without edges. IEEE Trans Image Process. 2001;10(2):266–277. doi:10.1109/83.902291
12. Wang XF, Huang DS, Xu H. An efficient local Chan–Vese model for image segmentation. Pattern Recognit. 2010;43(3):603–618. doi:10.1016/j.patcog.2009.08.002
13. Rayan JE, Mokri SS, Low YC, et al. Eyeball segmentation and measurement in MRI images of myopic children. J Phys Conf Ser. 2022;2312(1):012028.
14. Matsumura S, Kuo AN, Saw SM. An update of eye shape and myopia. Eye Contact Lens. 2019;45(5):279–285. doi:10.1097/ICL.0000000000000571
15. Swarbrick HA. Orthokeratology for myopia control: an optometrist’s view. Ann Eye Sci. 2018;3:17. doi:10.21037/aes.2018.02.01
16. Tang WT, Luo XN, Zhao WJ, et al. One-year results for myopia control of orthokeratology with different back optic zone diameters: a randomized trial using a novel multispectral-based topographer. Int J Ophthalmol. 2024;17(2):324–330. doi:10.18240/ijo.2024.02.15
17. Lee C-Y, Yang S-F, Chang Y-L, Huang J-Y, Lian I-B, Chang C-K. Comparison of myopic control between orthokeratology contact lenses and defocus incorporated multiple segments spectacle lenses. Int J Med Sci. 2024;21(7):1329–1336. doi:10.7150/ijms.93643
18. Cheung S-W, Cho P. Validity of axial length measurements for monitoring myopic progression in orthokeratology. Invest Ophthalmol Vis Sci. 2013;54(3):1613–1615. doi:10.1167/iovs.12-10434
19. Holmes M, Liu M, Singh S. Retrospective analysis of axial length changes in overnight orthokeratology in an academic myopia control clinic. Optom Vis Sci. 2023;100(9):597–605. doi:10.1097/OPX.0000000000002060
20. Meng ZY, Yang L, Zhou P. Analysis of axial shortening induced by orthokeratology lenses and its mechanical mechanisms. PLoS One. 2025;20(5):e0323546. doi:10.1371/journal.pone.0323546
21. Alharbi A, Swarbrick HA. The effects of overnight orthokeratology lens wear on corneal thickness. Invest Ophthalmol Vis Sci. 2003;44(6):2518–2523. doi:10.1167/iovs.02-0680
22. Zhang S, Zhang H, Li L, Yang X, Li S, Li X. Effect of treatment zone decentration on axial length growth after orthokeratology. Front Neurosci. 2022;16:986364. doi:10.3389/fnins.2022.986364
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optical Biometry Changes Throughout Childhood and Adolescence in Patients Wearing Ortho-K Lenses
Mahmoud O, Andrews C, Soeken T, Nallasamy S, Nallasamy N
Clinical Ophthalmology 2023, 17:1919-1927
Published Date: 4 July 2023
Visual Acuity Prior to Cataract Surgery and Risk of Retinal Detachment – A Population-Based Study
Thylefors J, Jakobsson G, Zetterberg M, Sheikh R
Clinical Ophthalmology 2023, 17:1975-1980
Published Date: 12 July 2023
The Impact of Vergence Dysfunction on Myopia Control in Children Wearing Defocus Spectacle Lenses
Ma J, Yang X, Liu Z, Fu H, Fan S, Wang K, Li Y, Huang L, Zhao M
Clinical Ophthalmology 2024, 18:799-807
Published Date: 12 March 2024
Impact of Forms of Visual Attenuation on Short-Term Eye Changes Under Controlled Reading Visibility

Su H, Chun RKM, De Lestrange-Anginieur E
Eye and Brain 2024, 16:133-146
Published Date: 4 December 2024
Long-Term Efficacy of CRT, Lucid, Euclid, and IBright Orthokeratology Lenses in Controlling Myopia Progression in Children and Adolescents: A 36-Month Retrospective Cohort Study
Xi W, Li H, Qi W, Tan T, Wang L
Clinical Ophthalmology 2025, 19:2423-2430
Published Date: 23 July 2025