Back to Journals » Clinical Ophthalmology » Volume 17
Optical Biometry Changes Throughout Childhood and Adolescence in Patients Wearing Ortho-K Lenses
Authors Mahmoud O, Andrews C, Soeken T, Nallasamy S, Nallasamy N ![]()
Received 11 April 2023
Accepted for publication 8 June 2023
Published 4 July 2023 Volume 2023:17 Pages 1919—1927
DOI https://doi.org/10.2147/OPTH.S413810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ossama Mahmoud,1,2 Chris Andrews,1 Timothy Soeken,1 Sudha Nallasamy,3,4 Nambi Nallasamy1,5
1Kellogg Eye Center Department of Ophthalmology and Visual Sciences, University of Michigan, Ann Arbor, MI, USA; 2School of Medicine, Wayne State University, Detroit, MI, USA; 3The Vision Center, Children’s Hospital Los Angeles, Los Angeles, CA, USA; 4USC Roski Eye Institute, Keck School of Medicine of the University of Southern California, LA, California, USA; 5Department of Computational Medicine and Bioinformatics, University of Michigan, Ann Arbor, MI, USA
Correspondence: Nambi Nallasamy, Kellogg Eye Center, University of Michigan, 1000 Wall St, Ann Arbor, MI, 48105, USA, Tel +1 734 763-5506, Fax +1 734 936-2340, Email [email protected]
Background: Orthokeratology has been shown to suppress progressive myopia in some children. We examine the changes in optical biometry parameters in orthokeratology (Ortho-K) patients, in a retrospective longitudinal study at a tertiary eye care center in Ann Arbor, MI, USA.
Methods: Optical biometry measurements obtained with the Lenstar LS 900 (Haag-Streit USA Inc, EyeSuite software version i9.1.0.0) were aggregated from 170 patients who had undergone Ortho-K for myopia correction between 5 and 20 years of age. Pre-intervention biometry measurements were compared with follow-up measurements done 6– 18 months after initiation of Ortho-K. Linear mixed models were used to quantify associations in biometry changes with age of intervention allowing for correlation between measurements on two eyes of the same patient.
Results: A total of 91 patients were included in the study. Axial length increased through the age of 15.7 ± 0.84 years for Ortho-K patients at our center. The growth curve in our Ortho-K population was comparable to previously published normal growth curves in Wuhan and Germany populations. Corneal thickness and keratometry decreased at a stable rate regardless of age of intervention (− 7.9 μm, 95% CI [− 10.2, − 5.7], p < 0.001).
Conclusion: In our population, Ortho-K did not appear to affect the overall trajectory of axial length progression when compared to normal growth curves, despite showing a previously described reduction in corneal thickness. As Ortho-K has been shown to have varying effects that differ from individual to individual, it continues to be important to reassess its effects on new populations to better understand its ideal uses.
Keywords: orthokeratology, biometry, pediatrics, axial length, corneal thickness
Background
Almost half of postnatal eye growth is believed to occur within the first 12–16 months of life. The second half continues throughout various stages of childhood, adolescence, and adulthood.1 These growth patterns are affected by many factors including genetics,2,3 environmental factors such as urban versus rural setting,4 sunlight exposure,2,5 near work,6,7 and level of education.8 Various interventions have been explored to slow the progression of myopia. In orthokeratology (Ortho-K), reverse geometry gas-permeable contact lenses are worn overnight to apply pressure to the cornea, temporarily flattening the central cornea and altering the corneal power.9,10 Ortho-K is also believed to steepen the peripheral cornea, thereby reducing peripheral hyperopia. The association of peripheral hyperopia with globe elongation has been the rationale for the study of Ortho-K as a potential method for slowing progression of axial myopia in children.9
Ocular biometric data during eye growth and development is needed to understand the process of emmetropization and to describe the development of refractive errors such as progressive myopia.11 Accelerated axial length growth can lead to retinal tears and premature vitreous detachment in adolescence. In addition, progressive myopia due to axial elongation increases the risk of many vision-threatening eye diseases such as myopic maculopathy, retinal detachment, glaucoma, and cataract formation.12 Accordingly, identifying safe treatment options to effectively slow the progression of myopia in children is important. Currently, there does not exist a definitive treatment regimen for progressive myopia in children, although studies have shown efficacy in the use of low dose atropine to slow myopic progression. There is, however, concern regarding the potential for myopic rebound after treatment is discontinued.13
Studies have shown that Ortho-K can slow axial length progression in myopic children to varying degrees9,14–16 with a potentially greater effect when initiated at an early age (6–8 years).9,14 When compared to spectacle correction, Ortho-K has shown a 40–60% mean reduction in axial length growth in various studies.14,15 However, these results vary from individual to individual, with some patients showing little or no myopic progression, and others progressing significantly with Ortho-K.
Ortho-K has also been shown to affect other components of the eye such as the cornea and the lens.17 Since the effects of Ortho-K vary from individual to individual, it can be valuable to investigate its effects in new populations using modern techniques such as optical biometry. We present here a study looking at the effects of the use of Ortho-K in a clinical setting on eye growth (as measured by optical biometry) in North American children who underwent Ortho-K for progressive myopia.
Methods
Biometry measurements captured between August 25, 2015, and June 27, 2019 were retrospectively retrieved from Lenstar LS900 optical biometers (Haag-Streit USA Inc, EyeSuite software version i9.1.0.0) at University of Michigan’s Kellogg Eye Center. Institutional review board approval was obtained for the study, and it was determined that informed consent was not required because of its retrospective nature and the anonymized data utilized in this study. The study was carried out in accordance with the tenets of the Declaration of Helsinki. Patients under the age of 20 undergoing orthokeratology at the University of Michigan Kellogg Eye Center were included. As part of standard of care for Ortho-K at our institution, patients were assessed pre-orthokeratology, where they were fitted with rigid, gas-permeable lenses and asked to wear them overnight. Patients were reassessed approximately 1 year after treatment initiation with optical biometry. Measurements were obtained by providers without a “washout” period in order to avoid the need for alternative correction for patients. Within-patient changes in axial length (AL), lens thickness (LT), central corneal thickness (CCT), and flat and steep keratometry (K1 and K2, respectively) were analyzed. In this cohort analysis, linear mixed models were used to investigate the association between changes in biometry measurements and age, allowing for correlation between measurements on two eyes of the same patient. Statistical analysis was done in R (v 4.1.0, R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 91 patients meeting the aforementioned criteria were included in the study. At our institution, patients undergoing Ortho-K tended to be of Asian descent. The average age of intervention in our study sample, as seen in Table 1, was 12 years (range, 6–17 years), with an average of 1.1 years between initiating Ortho-K (Table 2) and the post-initiation biometry measurement.
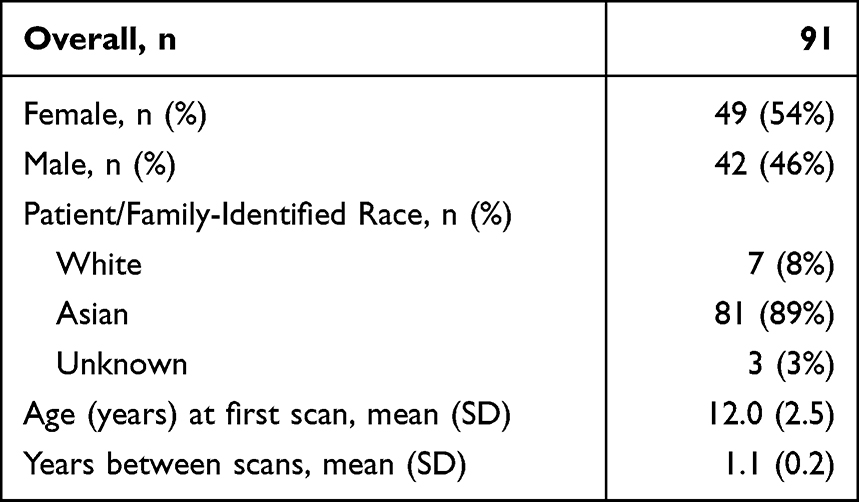 |
Table 1 Patient Demographics at Time of Pre-Ortho-K Intervention |
 |
Table 2 Average Biometry Measurements Taken at Pre-Ortho-K Intervention |
The average change in axial length from initiation of Ortho-K to 1-year post-initiation appeared to be linearly associated with age of intervention (p < 0.05) and increased for all patients, as seen in Table 3. Eyes with Ortho-K initiated at younger ages exhibited a greater increase in axial length after 1 year compared to those initiated at older ages, reflecting natural changes in rate of axial length growth across ages. Axial length grew 0.4 mm on average over 1 year for those initiating Ortho-K at 6 years of age, as seen in Figure 1. This rate of growth steadily decreased until age of initiation of 15.5 years (95% CI: [13.9, 17.0]), at which point axial length was found to be stationary.
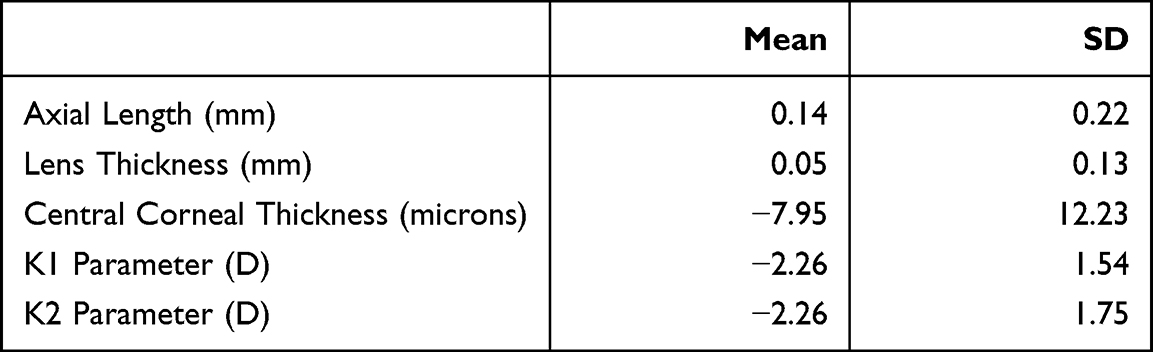 |
Table 3 Average Change in Biometry Measurements from Pre-Ortho-K Measurement to 1 Year After Ortho-K Measurement |
 |
Figure 1 Difference in axial length, in mm, between the first and second measurements taken approximately a year apart stratified by age at first measurement. A positive value at a certain age indicates patients of that age on average experienced an increase in axial length between the measurements. |
When compared to semi-parametric models of healthy axial length growth curves comprising both corrected myopic and non-myopic (Figure 2) our study population more closely match studies with a predominantly Asian population.18,19 The high degree of overlap between the normal growth curves found in Diez et al (Figure 2, purple curve) with the standard error of our study (Figure 2, green curve) indicates that in this population Ortho-K did not have significant effect on axial length progression.
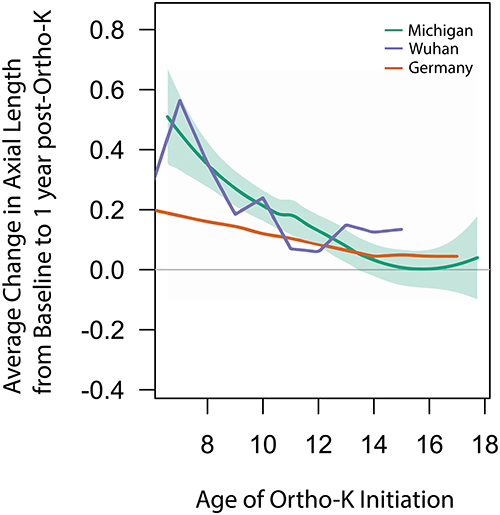 |
Figure 2 Comparison of semi-parametric model of yearly change in axial length, in mm, against age of intervention for Ortho-K patients or age of first measurement in healthy children (Purple: Diez et al 2019, Red: Truckenbrod et al 2021, Green: Our study). A positive value at a certain age indicates patients of that age on average experience an increase in axial length between the measurements taken about a year apart. |
Our results, shown in Figure 3, show very limited changes in lens thickness between baseline and 1 year after Ortho-K intervention (0.05mm, 95% CI: [0.03, 0.076]). This points to a very small change in lens thickness across adolescence. Furthermore, the age at which the Ortho-K intervention was started did not appear to affect the change in lens thickness post-intervention (p = 0.38).
 |
Figure 3 Average difference in lens thickness, in mm, between the pre-Ortho-K intervention and a second measurement taken approximately 1 year after Ortho-K intervention stratified by age at first measurement. A positive value at a certain age indicates patients of that age on average experience an increase in lens thickness between the measurements taken about a year apart. |
The change in central corneal thickness between baseline and follow up for patients with Ortho-K intervention did not appear to vary with age of intervention (p = 0.80), as seen in Figure 4. When modeled without age of intervention as a variable, change between baseline and 1 year after Ortho-K intervention appeared to decrease by 7.95µm (95% CI: [−10.2, −5.7]).
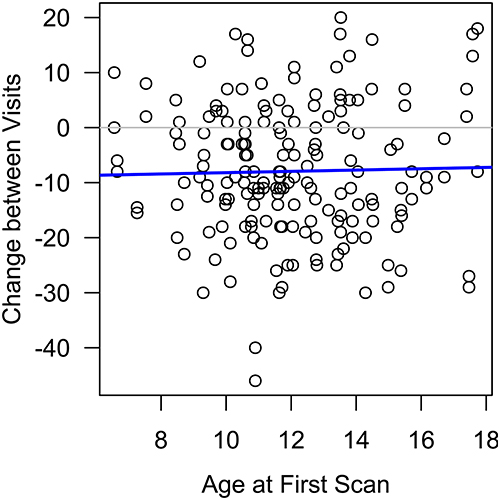 |
Figure 4 Average difference in central corneal thickness, in microns, between the pre-Ortho-K intervention and a second measurement taken approximately 1 year after Ortho-K intervention stratified by age at first measurement. |
Similarly, mean keratometry changes between baseline and 1 year after orthokeratology demonstrated a small but constant reduction in corneal power regardless of age of intervention, as seen in Figure 4. An average 1-year post-intervention change of about −2.26 D (95% CI [−2.5, −1.94]) and −2.26 D (95% CI [−2.61, −1.91]) was seen for K1 and K2, respectively.
To assess the impact of the varying duration of follow-up appointments on changes in biometry measurements, we investigated whether normalizing these measurements by dividing them by the time between appointments would affect our results. We also conducted a subgroup analysis that included only children of Asian descent. Our findings revealed that neither the normalization nor the subgroup analysis had a significant impact on the changes in biometry measurements. Specifically, the average 1-year post-intervention changes in axial length, lens thickness, central corneal thickness, K1, and K2 were 0.14 mm, 0.05 mm, 7.66 µm, 2.17 D, and 2.13 D, respectively.
Discussion
Biometry measurements throughout childhood can provide an understanding of the growth patterns of the human eye. Orthokeratology has been proposed as a treatment option for highly progressive myopia.15 Understanding the patterns associated with eye development and growth during Ortho-K treatment provides ophthalmologists with key pieces of information when assessing and treating pediatric patients.
Year of birth or ethnicity of participants did not have a significant impact on changes in biometry measurements; this is suspected to be due to a majority of patients having similar birth years and ethnicities in our dataset. Biometry measurements such as axial length are also influenced by seasonal and diurnal changes.20,21 By considering year-to-year changes in biometry measurements, seasonal changes were mitigated as measurements for a given patient typically occurred in the same season. The scale of change seen diurnally in prior studies (0.046 ± 0.022 mm) appears to be an order of magnitude smaller than the average year-to-year change seen in the present study and as such we do not expect diurnal changes to substantially affect year-to-year changes.21
In our study, patients undergoing orthokeratology treatment exhibited axial length growth at rates comparable to published growth patterns in populations with similar ethnic make-up. Although, ideally a control group not undergoing Ortho-K therapy would serve as the best comparison group for the available ortho-K treatment data, identification of such a control group can be difficult in the clinical setting, where biometry measurements are usually done after a pathological indication or as part of a treatment plan. Previous studies have established that axial length increases throughout childhood, and to account for normal growth patterns, we compared the growth curves from our Ortho-K population with growth curves for normal healthy axial length growth in children. Diez et al in 2019, Truckenbrod et al in 2020, and He et al in 2023 performed large-scale longitudinal studies to examine axial length progression for healthy schoolchildren in Wuhan (China), Germany, and Shanghai (China), respectively.18,22,23 When comparing our Ortho-K data to the data from Diez et al, we found that the age-matched rate of growth of axial length for untreated eyes of randomly sampled children matched the rate of growth for the Ortho-K patients we studied. Our Ortho-K patients demonstrated higher rates of axial length growth than those in the Truckenbrod study. A possible explanation for this is that our patient population was primarily of Asian descent, which closely matched the ethnicity of the study done by Diez et al in China, but differed significantly from the primarily Caucasian population studied by Truckenbrod et al. In the Shanghai population studied by He et al, axial length continued to grow at a significant rate (approximately 0.2mm/year) through age 17. This was in contrast to the Wuhan population, German population, and our own population of Ortho-K patients, wherein axial length largely stabilized by 15 years of age. Differences in baseline characteristics among the populations and risk factors such as limited outdoor time may have contributed to these differing growth trajectories. In our population, similar changes in axial length among patients undergoing Ortho-K treatment were found when compared to those not undergoing Ortho-K in the Wuhan population, indicating the need for further work to identify which patient characteristics are most suitable for Ortho-K treatment, as it appears its effects may differ from population to population.
Previous studies looking at axial length progression in Ortho-K patients found a reduction in the progression of axial length growth of about 0.23mm and 0.36mm when compared to controls prescribed single-vision spectacles after 1 year, and 2 years of Ortho-K treatment, respectively.15 In one study, axial length growth in children undergoing Ortho-K was compared to children wearing soft contact lenses.24 Axial length progression appeared to be 0.16 mm per year less for Ortho-K wearers than soft contact lens wearers. However, this study suffered from high dropout rate of 30%, which may have resulted in a biased representation of the effect of Ortho-K. An additional concern with reported reductions in axial length growth for Ortho-K patients is Ortho-K’s effect on thinning the cornea, a component of axial length. This likely leads to an overestimation of axial length growth suppression in Ortho-K patients, especially if there is no washout period when taking post-initiation measurements.25
Given the previously published observational reports and case series of infectious keratitis with Ortho-K,26–28 clarifying patient populations in which Ortho-K may not affect axial length growth may offer a way to limit risk to patients.
Our results show only very slight increases in lens thickness across adolescence and adulthood after treatment with Ortho-K; this differs from previous investigations done on healthy eyes. In a study examining changes in lens thickness, wherein 864 children were followed annually for three years, lens thickness was found to decrease between the ages of 6–10, followed by a period of stabilization until the age of 14.29 This difference could be attributed to Zadnik’s use of A-scan ultrasonography to measure biometry instead of the more precise optical biometry. Our results are consistent with those of a recent study that found lens thickness did not change 6 months after initiation of Ortho-K treatment when compared to initial pre-Ortho-K measurements.30
Central corneal thickness and keratometry are clinically relevant for planning surgical procedures to correct astigmatism and myopia. In healthy eyes, central corneal thickness (CCT) appears to be stable after 1.5 years of age in children.31 For patients undergoing Ortho-K, our results point to a 7.9 micron (95% CI: [−10.2, −5.7]) reduction 1 year post-Ortho-K initiation. This change also appears to not be influenced by the age of orthokeratology initiation. Recent studies have also shown a reduction in CCT after Ortho-K initiation in as little as 1 week unrelated to age.32,33 This reduction has been demonstrated in prior studies to be confined to the corneal epithelial layer.34,35
There is limited research on corneal keratometry changes post Ortho-K. Khan et al, in a study comparing baseline keratometry K1 and K2 parameters before initiating Ortho-K and 12 weeks after initiation, found a reduction in K1 and K2 of 1.50 D (95% CI [0.49, 2.52]) and 1.68 D (95% CI [0.49, 2.87]), respectively.36 Our results point to a similar but slightly amplified decrease in both flat and steep keratometry values by 2.26 D (95% CI [−2.5, −1.94]). It is important to note that these changes were observed without a washout period of Ortho-K lens wear. As such, these changes in keratometry are unlikely to be persistent.
As a preliminary study on tracking Ortho-K in the clinical setting, we identify several limitations that need to be addressed in future studies. The lack of a control group not undergoing Ortho-K in our study limits our ability to draw a definitive efficacy conclusion from the available data. Further studies to evaluate this finding using a control group within the same population would be of value.
Conclusion
Axial length, lens thickness, and corneal thickness change throughout childhood until stabilization in young adulthood. Orthokeratology has been shown to affect these parameters in prior studies. Ortho-K patients in our study population of children of predominantly Asian descent demonstrated similar axial length growth trajectories when compared to randomly sampled children in a population of 90% myopia prevalence from Wuhan.
Due to the use of historic growth curves as comparators, multiple baseline differences in the populations compared can exist, limiting the generalizability of these results. As Ortho-K is not without risks, continuous monitoring of Ortho-K’s efficacy in different regions is warranted. Using optical biometry to understand growth patterns during orthokeratology treatment and how they compare to normal growth patterns in different populations may aid in the study and understanding of axial length progression in children.
Abbreviations
Ortho-K, Orthokeratology; AL, Axial length; LT, lens thickness; CCT, central corneal thickness; K1, flat keratometry; K2, steep keratometry.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available to protect patient privacy but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Institutional review board approval (University of Michigan’s Human Research Protection Program (HRPP)) was obtained for the study from the Institutional review board of University of Michigan. Additionally, Institutional review board of University of Michigan has waived informed consent for the study because of its retrospective nature and the anonymized data utilized in this study. The study was carried out in accordance with the tenets of the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Supported by GME Innovations Fund, The Doctors Company Foundation, and NIH K12EY022299.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fledelius HC, Christensen AS, Fledelius C. Juvenile eye growth, when completed? An evaluation based on IOL-Master axial length data, cross-sectional and longitudinal. Acta Ophthalmol. 2014;92(3):259–264. doi:10.1111/aos.12107
2. Read SA. Ocular and environmental factors associated with eye growth in childhood. Optom Vis Sci. 2016;93:1031–1041. doi:10.1097/OPX.0000000000000915
3. Saw SM, Chua WH, Gazzard G, Koh D, Tan DTH, Stone RA. Eye growth changes in myopic children in Singapore. Br J Ophthalmol. 2005;89(11):1489–1494. doi:10.1136/bjo.2005.071118
4. Rudnicka AR, Kapetanakis V, Wathern AK, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. Br J Ophthalmol. 2016;100(7):882–890. doi:10.1136/BJOPHTHALMOL-2015-307724
5. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–1285. doi:10.1016/J.OPHTHA.2007.12.019
6. Gajjar S, Ostrin LA. A systematic review of near work and myopia: measurement, relationships, mechanisms and clinical corollaries. Acta Ophthalmol. 2022;100(4):376–387. doi:10.1111/AOS.15043
7. Huang HM, Chang DST, Wu PC. The association between near work activities and myopia in children—A systematic review and meta-analysis. PLoS One. 2015;10(10):e0140419. doi:10.1371/JOURNAL.PONE.0140419
8. Mirshahi A, Ponto KA, Hoehn R, et al. Myopia and level of education: results from the Gutenberg Health Study. Ophthalmology. 2014;121(10):2047–2052. doi:10.1016/J.OPHTHA.2014.04.017
9. VanderVeen DK, Kraker RT, Pineles SL, et al. Use of orthokeratology for the prevention of myopic progression in children: a report by the American Academy of Ophthalmology. Ophthalmology. 2019;126(4):623–636. doi:10.1016/J.OPHTHA.2018.11.026
10. Lipson MJ, Brooks MM, Koffler BH. The role of orthokeratology in myopia control: a review. Eye Contact Lens. 2018;44(4):224–230. doi:10.1097/ICL.0000000000000520
11. Rauscher FG, Francke M, Hiemisch A, Kiess W, Michael R. Ocular biometry in children and adolescents from 4 to 17 years: a cross-sectional study in central Germany. Ophthalmic Physiol Opt. 2021;41(3):496–511. doi:10.1111/opo.12814
12. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622–660. doi:10.1016/J.PRETEYERES.2012.06.004
13. Pineles SL, Kraker RT, VanderVeen DK, et al. Atropine for the prevention of myopia progression in children: a report by the American Academy of Ophthalmology. Ophthalmology. 2017;124(12):1857–1866. doi:10.1016/J.OPHTHA.2017.05.032
14. Charm J, Cho P. High myopia-partial reduction ortho-k: a 2-year randomized study. Optom Vis Sci. 2013;90(6):530–539. doi:10.1097/OPX.0B013E318293657D
15. Zhu MJ, Feng HY, He XG, Zou HD, Zhu JF. The control effect of orthokeratology on axial length elongation in Chinese children with myopia. BMC Ophthalmol. 2014;14(1):1–9. doi:10.1186/1471-2415-14-141/FIGURES/3
16. Swarbrick HA, Alharbi A, Watt K, Lum E, Kang P. Myopia control during orthokeratology lens wear in children using a novel study design. Ophthalmology. 2015;122(3):620–630. doi:10.1016/J.OPHTHA.2014.09.028
17. Wang Z, Meng Y, Wang Z, et al. Crystalline lens thickness change is associated with axial length elongation and myopia progression in orthokeratology. Contact Lens Anterior Eye. 2021;45:101534. doi:10.1016/J.CLAE.2021.101534
18. Sanz Diez P, Yang LH, Lu MX, Wahl S, Ohlendorf A. Growth curves of myopia-related parameters to clinically monitor the refractive development in Chinese schoolchildren. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):1045–1053. doi:10.1007/S00417-019-04290-6
19. Lu TL, Wu JF, Ye X, et al. Axial length and associated factors in children: the Shandong Children Eye Study. Ophthalmologica. 2016;235(2):78–86. doi:10.1159/000441900
20. Nilsen NG, Gilson SJ, Pedersen HR, Hagen LA, Knoblauch K, Baraas RC. Seasonal variation in diurnal rhythms of the human eye: implications for continuing ocular growth in adolescents and young adults. Invest Ophthalmol Vis Sci. 2022;63(11):20. doi:10.1167/IOVS.63.11.20
21. Read SA, Collins MJ, Iskander DR. Diurnal variation of axial length, intraocular pressure, and anterior eye biometrics. Invest Ophthalmol Vis Sci. 2008;49(7):2911–2918. doi:10.1167/IOVS.08-1833
22. Truckenbrod C, Meigen C, Brandt M, et al. Longitudinal analysis of axial length growth in a German cohort of healthy children and adolescents. Ophthalmic Physiol Opt. 2021;41(3):532–540. doi:10.1111/opo.12817
23. He X, Sankaridurg P, Naduvilath T, et al. Clinical science Normative data and percentile curves for axial length and axial length/corneal curvature in Chinese children and adolescents aged 4–18 years. Br J Ophthalmol. 2021;2021:1–9. doi:10.1136/bjophthalmol-2021-319431
24. Walline JJ, Jones LA, Sinnott LT. Corneal reshaping and myopia progression. Br J Ophthalmol. 2009;93(9):1181–1185. doi:10.1136/BJO.2008.151365
25. Heng LS, Khoo CY. Can contact lenses control the progression of myopia? Singapore Med J. 1994;35(4):367–370.
26. Cope JR, Collier SA, Schein OD, et al. Acanthamoeba keratitis among rigid gas permeable contact lens wearers in the United States, 2005 through 2011. Ophthalmology. 2016;123(7):1435–1441. doi:10.1016/J.OPHTHA.2016.03.039
27. Van Meter WS, Musch DC, Jacobs DS, Kaufman SC, Reinhart WJ, Udell IJ. Safety of overnight orthokeratology for myopia: a report by the American Academy of Ophthalmology. Ophthalmology. 2008;115(12):2301–2313.e1. doi:10.1016/J.OPHTHA.2008.06.034
28. Young AL, Leung ATS, Cheng LL, Law RWK, Wong AKK, Lam DSC. Orthokeratology lens-related corneal ulcers in children: a case series. Ophthalmology. 2004;111(3):590–595. doi:10.1016/J.OPHTHA.2003.06.003
29. Zadnik K, Mutti DO, Fusaro RE, Adams AJ. Longitudinal evidence of crystalline lens thinning in children. Investig Ophthalmol Vis Sci. 1995;36(8):1581–1587.
30. Cheung SW, Cho P. Validity of axial length measurements for monitoring myopic progression in orthokeratology. Investig Ophthalmol Vis Sci. 2013;54(3):1613–1615. doi:10.1167/iovs.12-10434
31. Muir KW, Duncan L, Enyedi LB, Stinnett SS, Freedman SF. Central corneal thickness in children: stability over time. Am J Ophthalmol. 2006;141(5):955–957. doi:10.1016/j.ajo.2005.11.052
32. Wan K, Yau HT, Cheung SW, Cho P. Corneal thickness changes in myopic children during and after short-term orthokeratology lens wear. Ophthalmic Physiol Opt. 2021;41(4):757–767. doi:10.1111/OPO.12824
33. Li F, Jiang ZX, Hao P, Li X. A meta-analysis of central corneal thickness changes with overnight orthokeratology. Eye Contact Lens. 2016;42(2):141–146. doi:10.1097/ICL.0000000000000132
34. Kim WK, Kim BJ, Ryu IH, Kim JK, Kim SW. Corneal epithelial and stromal thickness changes in myopic orthokeratology and their relationship with refractive change. PLoS One. 2018;13(9):e0203652. doi:10.1371/JOURNAL.PONE.0203652
35. Zhang J, Li J, Li X, Li F, Wang T. Redistribution of the corneal epithelium after overnight wear of orthokeratology contact lenses for myopia reduction. Contact Lens Anterior Eye. 2020;43(3):232–237. doi:10.1016/J.CLAE.2020.02.015
36. Khan MA, Gupta A, Ahluwalia TS, Moulick PS, Gurunadh VS, Gupta S. A prospective interventional study of effect of accelerated orthokeratology on the corneal curvature and refraction among young adults with myopia. Med J Armed Forces India. 2016;72(2):125. doi:10.1016/J.MJAFI.2016.02.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Cataract Surgery on IOP and Ocular Structures in Normotensive Patients and Primary and Exfoliation Open-Angle Glaucoma Patients
Xirou V, Xirou T, Siganos C, Ntonti P, Georgakopoulos C, Stavrakas P, Makri OE, Kanakis M, Tsapardoni F, Fragkoulis I, Garnavou-Xirou C, Kozobolis V
Clinical Ophthalmology 2023, 17:1047-1055
Published Date: 5 April 2023
Relative Behavior of Modern Intraocular Lens Power Calculation Formulas Across a Realistic Range of Biometry Values
Rossip MG, Hastings J, Burwinkel H, Lavrova E, Steinbrenner R, Bensaid N, Cooke DL, Pantanelli SM
Clinical Ophthalmology 2025, 19:2037-2045
Published Date: 28 June 2025
Long-Term Efficacy of CRT, Lucid, Euclid, and IBright Orthokeratology Lenses in Controlling Myopia Progression in Children and Adolescents: A 36-Month Retrospective Cohort Study
Xi W, Li H, Qi W, Tan T, Wang L
Clinical Ophthalmology 2025, 19:2423-2430
Published Date: 23 July 2025
Intra- and Inter-Observer Agreement of a Portable A-Scan Ultrasound Biometer in Sitting and Supine Positions and Validity Against an Optical Biometer
Jeyandran J, Roberts CJ, Yuhas PT
Clinical Optometry 2025, 17:283-296
Published Date: 5 September 2025
Ocular Dimensional Changes After 12 Months of Orthokeratology and Single-Vision Spectacle Use: A Three-Dimensional Magnetic Resonance Imaging Study
Low YC, Mohd-Ali B, Shahimin MM, Mohidin N, Wan Abdul Halim WH, Mokri SS, Abdul-Hamid H
Clinical Optometry 2026, 18:611080
Published Date: 14 July 2026