Back to Journals » Clinical Ophthalmology » Volume 17
Visual Acuity Prior to Cataract Surgery and Risk of Retinal Detachment – A Population-Based Study
Authors Thylefors J ![]() , Jakobsson G
, Jakobsson G ![]() , Zetterberg M, Sheikh R
, Zetterberg M, Sheikh R ![]()
Received 14 March 2023
Accepted for publication 19 May 2023
Published 12 July 2023 Volume 2023:17 Pages 1975—1980
DOI https://doi.org/10.2147/OPTH.S410585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Joakim Thylefors,1 Gunnar Jakobsson,2 Madeleine Zetterberg,2 Rafi Sheikh1
1Ophthalmology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden; 2Department of Ophthalmology, Sahlgrenska University Hospital, Mölndal, Västra Götaland, Sweden
Correspondence: Joakim Thylefors, Ophthalmology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Kioskgatan 1A, Lund, SE - 22242, Sweden, Tel +46 40 333 134, Email [email protected]
Purpose: To analyze preoperative visual acuity before cataract surgery regarding the risk of rhegmatogenous retinal detachment (RRD) after cataract surgery.
Methods: The preoperative visual acuity in an observational cohort study of patients undergoing cataract surgery in Skåne, southern Sweden, during 2015– 2017 was analyzed with data retrieved from the Swedish National Cataract Register. This was then cross-referenced with patients undergoing surgery for retinal detachment at the Skåne University Hospital in Lund from 2015 to 2020. The main outcome was the risk–benefit ratio of measuring preoperative visual acuity before cataract surgery and the risk of RRD.
Results: The mean visual acuity in the whole study group (N=58,624), expressed as LogMAR, was 0.40 ± 0.32 (SD). In the group with RRD (n=298), the mean visual acuity was 0.44 ± 0.36 (p=0.07). In the subgroups of RRD, those aged < 60 years 0.49 ± 0.44 (p=0.07), aged < 60 years and axial length (AL) > 25 mm 0.42 ± 0.38 (p=0.68), and in those aged < 60 years, AL > 25 mm and male sex 0.44 ± 0.39 (p=0.53). However, there is considerable variations in visual acuity of the various groups and in the high-risk group with RRD aged < 60 years with AL> 25 mm, 15% had a visual acuity of 0.8 or better in the operated eye.
Conclusion: There must be strong indications for performing cataract surgery in those with a high risk of retinal detachment, and the patient must be given adequate information on the risk of retinal detachment.
Keywords: cataract surgery, myopia, retinal detachment, axial length
Introduction
Cataract is the leading cause of blindness worldwide today,1 and phacoemulsification followed by replacement of the crystalline lens with an artificial plastic lens is one of the most common forms of surgery. There is concern that the increasing rate of cataract surgery over recent decades2 has led to an increase in the post-surgical incidence of complications such as rhegmatogenous retinal detachment (RRD). There is a tendency towards operating younger patients2 who may have a greater risk of RRD as they have a longer life expectancy, and have often not developed posterior vitreous detachment.3 Despite immediate surgery, RRD remains one of the most common causes of emergency surgical intervention resulting in significant loss of vision in a high proportion of patients.4 The indications for cataract surgery have shifted as both per-operative and immediate post-operative complications have become less common,5,6 however, little attention has been devoted to long-term complications such as RRD.
We have previously published the findings of a study on the risk of RRD after cataract surgery.7 We found that the risk of RRD depended mainly on age, axial length (AL) and sex. In the whole study group, consisting of 58,624 eyes, the overall risk of developing RRD within the follow-up period of 4.7 years was 0.51%, in agreement with previous studies.8–15 However, the increased risk is mainly correlated to lower age, increased AL and male sex. In the group <60 years of age, 2.4% developed RRD, and when combined with AL >25 mm in the risk increased to 6.4%. When male sex was included, the risk of developing RRD increased to 9.5%.
The purpose of the study presented here was to investigate visual acuity before cataract surgery and compare it to the risk of subsequent RRD to determine whether there is a risk–benefit ratio that has not previously been exposed in this way.
Patients and Methods
Data were extracted on all cataract surgeries performed from 1 January 2015 to 31 December 2017 in the region of Skåne, southern Sweden, from the Swedish National Cataract Register.2 Exclusion criteria were cataract surgery in combination with pars plana vitrectomy, corneal or glaucoma surgery, or age less than 30 years.
The visual acuity in the operated eye and the fellow eye were analyzed and then compared to the results of a previous study on the risk of RRD in the same population.7 The visual acuity, measured using the Snellen chart, was converted to LogMAR to allow parametric calculations.
The study was approved by the Regional Ethics Committee of Stockholm, Sweden (No. 2020–07214) and was carried out in accordance with the Declaration of Helsinki of 2013. It is a retrospective study and based on anonymized data and according to Regional Ethics Committee no informed consent was needed to participate.
Statistical Analysis
Differences in LogMAR, age, sex, and AL were analyzed using Welch’s t-test. When analyzing non-parametric data, the chi-squared test was used. Statistical analysis was performed using R (R Core Team (2020), Vienna, Austria. URL https://www.R-project.org/) for Mac software, and Prism 9.1.0 (GraphPad Software, San Diego, California USA). A p-value of less than 0.05 was considered statistically significantly different.
Results
A total of 59,044 phacoemulsification cataract surgeries were performed in the region during the years 2015–2017. The inclusion criteria were met in 58,624 cases, distributed over 37,059 patients, and thus both eyes were operated on in 21,565 cases.
The patient data are presented in Table 1, and divided between all eyes and those who had RRD. No statistically significant difference was found between visual acuity, expressed as LogMAR, in the operated eye between the groups. A statistically significant difference was found between the groups in the non-operated eye (p<0.001); the RRD group showing better visual acuity.
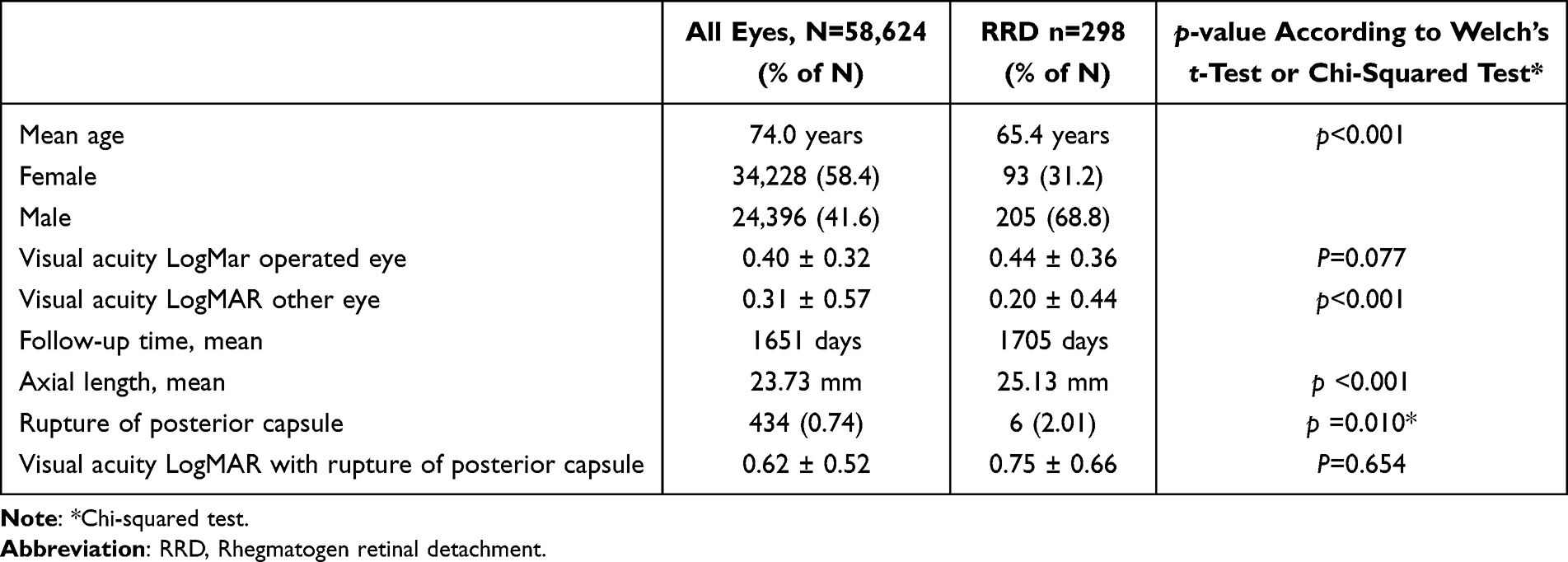 |
Table 1 Patient Data, and the results of Welch’s t-Test and the Chi-Squared Test |
When taking the effects of age, sex, and AL into account, a significant increase in the incidence of RRD was seen, as in our previous publication.7 The data presented in Table 2 shows these subgroups with high risk of RRD with the pre-operative Snellen vision of patients seeing better then 0.5 and 0.8, respectively. Looking at the parametric calculation the pre-operative visual acuity in LogMAR boxplot for the same groups with and without RRD is presented in Figure 1. In the group with RRD mean ± SD was 0.44 ± 0.36 (p=0.07), RRD with age below 60 years LogMAR mean 0.49 ± 0.44 (p=0.07), age below 60 years and AL >25 mm LogMAR mean 0.42 ± 0.38 (p=0.68) and with age below 60 years, AL >25 mm and male sex mean 0.44 ± 0.39 (p=0.53). The p-value is compared to the whole patient data minus the group in question.
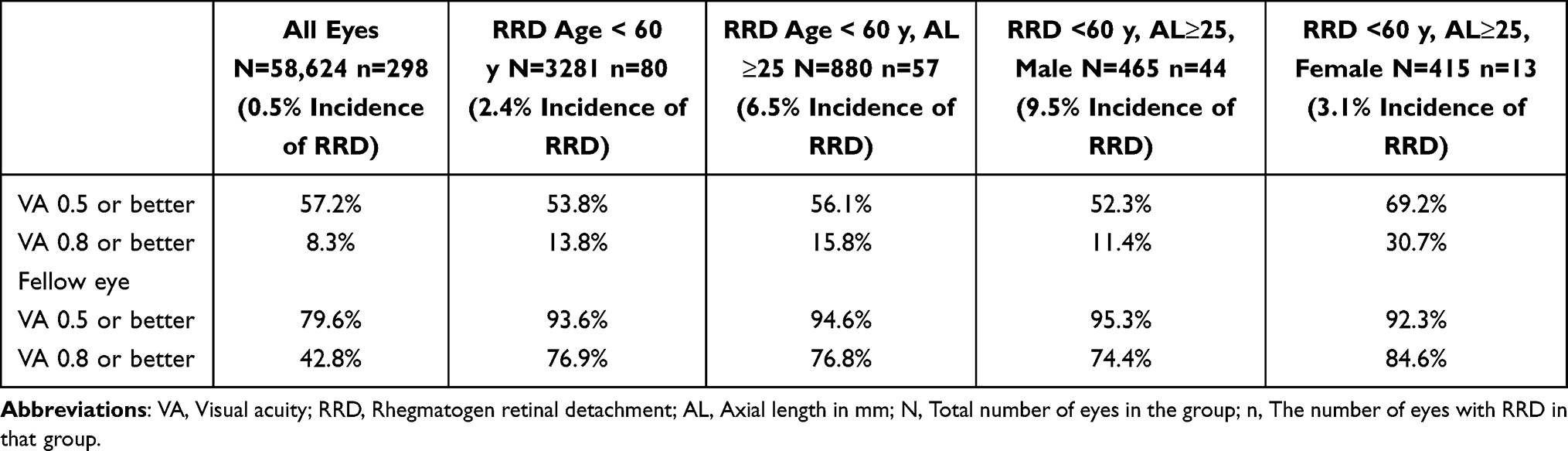 |
Table 2 Incidence of RRD After Surgery of Cataract According to Sex, Age and Axial Length (AL) During the Study Period (Mean 4.67 Years) in Relation to Pre-Operative Visual Acuity in Snellen |
 |
Figure 1 Boxplot of LogMAR pre-operative visual acuity for whole study group, RRD group, cataract surgery <60 y, RRD <60 y, RRD <60 y and AL≥25 mm, RRD <60 y, AL≥25 mm and male sex. |
Discussion
The discussion on the indications for cataract surgery has been mainly related to the implantation of the intra-ocular lens, and the short- and long-term complications after surgery.6 The pre-operative visual acuity of those undergoing cataract surgery is now higher than previously, as found in a Finish study, where at least 20% saw Snellen 0.8 or better, and these patients could probably obtained equally good vision by purchasing new spectacles.16 Correcting refraction during cataract is currently an option, although it is not always performed. In the present study, we have compared pre-operative visual acuity to the actual incidence of developing RRD almost 5 years after cataract surgery. In the group of patients under 60 years with an axial length over 25 mm with a 6.4% risk of RRD in less than 5 years, more than 15% saw 0.8 or better. The risk–benefit ratio is subjective to each patient, but in our opinion, these patients could have avoided cataract surgery and obtained the same improvement in vision with better spectacles. As this RRD group is quite small, and there is considerable variation in the visual acuity within the group, it is therefore important to inform patients with relative good visual acuity that new spectacles may be an alternative to cataract surgery. Also, in the same RRD group, more than 55% saw better than 0.5, where below that previously used to be the indications in several regions for surgery. In a study carried out in Spain17 published in 2010, only 15% of the patients saw 0.5 or better. In that study, cataract surgery was usually deemed inappropriate in patients whose visual function was not impaired or only slightly impaired. In our study, the fellow eye not undergoing cataract surgery, the mean visual acuity was 0.31 ± 0.57 LogMAR, which can be compared to that in the RRD group of 0.20 ± 0.44 (p<0.001). This means that the patients with RRD had similar visual acuity in the operated eye as the whole study group, but there was a large difference in the fellow eye, where the RRD patients had better visual function. This indicates that cataract surgery is not necessary for many who have a risk for RRD as their binocular vision is still adequate.
Many of the patients probably underwent cataract surgery on the eye with poorer vision, and then later on the better eye, especially in the case of myopic patients to avoid anisometropia. Post-operative refraction must be considered when choosing the intra-ocular lens for the first eye to avoid putting them at risk for RRD with cataract surgery on the fellow eye.
Very few complications during surgery and shortly after, such as corneal edema, cystoid macular edema and infection, have been reported following cataract surgery by experienced surgeons.2 However, based on the findings of this study, we concluded that a greater awareness of the long-term risk of RRD is required in high-risk patients when considering cataract surgery.
Visually based grading systems can be used for cataracts, such as the AREDS18 and LOCS III.19 These show a certain degree of correlation to the severity of the cataract, but neither of these can predict the outcome of cataract surgery.20 The expected postoperative visual outcome is important when advising the patient on whether or not to undergo surgery. In a systematic review and meta-analysis, Kessel et al found that the Swedish NIKE (National Indication for Cataract Extraction) system was the only system with a documented association between pre-operative grading and outcome of cataract surgery.5 However, the NIKE system does not take into account the age of the patient or the axial length of the eye, so it does not take the long-term risk of RRD into consideration. Ideally, the patients’ individual risk should be calculated and presented on the biometry before the surgery to enable a risk–benefit discussion.
Capsular rupture is a well-known risk factor for RRD.12,21–23 In the present study, 2.01% of the patients with RRD had capsular rupture, compared to 0.74% in the whole study group. The group with capsule rupture had poorer visual acuity preoperatively than the whole study group (p=0.01) indicating that cataract surgery could be more difficult in these cases.24 Knowing that their vision is worse, the indications to do surgery is stronger, so the risk of complications may be more acceptable.
The risk of developing RRD was found to decrease gradually with time during the present study. This is reported by several other studies that the risk is increased and maintained for several years.25,26 For how long is hard to know, but it was reported from a study in Minnesota, USA,10 that the risk continued for up to 20 years after surgery. These studies indicate that the risk for RRD is elevated not only for a short period but probably for a long time.
A weakness of this study is that only visual acuity was analyzed as an indication for cataract surgery. Some patients with good pre-operative visual acuity may have had other cataract-associated symptoms, such as increased light sensitivity or reduced night vision.
Conclusion
In our previous study,7 we identified the pseudophakic patients with a high risk of long-term complications such as RRD, especially men under the age of 60 with axial length exceeding 25 mm who had almost 10% risk within 5 years. These patients should be thoroughly informed of the risks associated with cataract surgery, and the indications for cataract surgery should be strong. We illustrate in this study that many times the visual acuity for these patients is surprisingly good preoperative of cataract surgery where perhaps the best option for the patient is to wait with the surgery. We hope that in the future there will be an individual risk assessment for each patient to consider before doing the surgery.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thylefors B, Negrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull World Health Organ. 1995;73(1):115–121.
2. Behndig A, Montan P, Stenevi U, Kugelberg M, Lundstrom M. One million cataract surgeries: Swedish National Cataract Register 1992–2009. J Cataract Refract Surg. 2011;37(8):1539–1545. doi:10.1016/j.jcrs.2011.05.021
3. Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94(6):678–684. doi:10.1136/bjo.2009.157727
4. Barrie T. Debate overview. Repair of a primary rhegmatogenous retinal detachment. Br J Ophthalmol. 2003;87(6):790. doi:10.1136/bjo.87.6.790
5. Kessel L, Andresen J, Erngaard D, Flesner P, Tendal B, Hjortdal J. Indication for cataract surgery. Do we have evidence of who will benefit from surgery? A systematic review and meta-analysis. Acta Ophthalmol. 2016;94(1):10–20. doi:10.1111/aos.12758
6. Lundstrom M, Stenevi U. Indications for cataract surgery in a changing world. Acta Ophthalmol. 2016;94(1):9. doi:10.1111/aos.12820
7. Thylefors J, Jakobsson G, Zetterberg M, Sheikh R. Retinal detachment after cataract surgery: a population-based study. Acta Ophthalmol. 2022;100. doi:10.1111/aos.15142
8. Clark A, Morlet N, Ng JQ, Preen DB, Semmens JB. Risk for retinal detachment after phacoemulsification: a whole-population study of cataract surgery outcomes. Arch Ophthalmol. 2012;130(7):882–888. doi:10.1001/archophthalmol.2012.164
9. Daien V, Le Pape A, Heve D, Carriere I, Villain M. Incidence, risk factors, and impact of age on retinal detachment after cataract surgery in France: a national population study. Ophthalmology. 2015;122(11):2179–2185. doi:10.1016/j.ophtha.2015.07.014
10. Erie JC, Raecker ME, Baratz KH, Schleck CD, Robertson DM. Risk of retinal detachment after cataract extraction, 1980–2004: a population-based study. Trans Am Ophthalmol Soc. 2006;104:167–175.
11. Haug SJ, Bhisitkul RB. Risk factors for retinal detachment following cataract surgery. Curr Opin Ophthalmol. 2012;23(1):7–11. doi:10.1097/ICU.0b013e32834cd653
12. Javitt JC, Vitale S, Canner JK, Krakauer H, McBean AM, Sommer A. National outcomes of cataract extraction. I. Retinal detachment after inpatient surgery. Ophthalmology. 1991;98(6):895–902. doi:10.1016/s0161-6420(91)32204-8
13. Kim J, Ryu SY, Hong JH, Chung EJ. Incidence and risk factors for retinal detachment after cataract surgery in Korea: a nationwide population-based study from 2011 to 2015. Graefes Arch Clin Exp Ophthalmol. 2019;257(10):2193–2202. doi:10.1007/s00417-019-04423-x
14. Lois N, Wong D. Pseudophakic retinal detachment. Surv Ophthalmol. 2003;48(5):467–487. doi:10.1016/s0039-6257(03)00083-3
15. Olsen T, Jeppesen P. The incidence of retinal detachment after cataract surgery. Open Ophthalmol J. 2012;6:79–82. doi:10.2174/1874364101206010079
16. Falck A, Virtanen P, Tuulonen A. Is more always better in cataract surgery? Acta Ophthalmol. 2012;90(8):e653–4. doi:10.1111/j.1755-3768.2012.02535.x
17. de Larrea NF, Blasco JA, Aguirre U, et al. Appropriateness of phacoemulsification in Spain. Int J Qual Health Care. 2010;22(1):31–38. doi:10.1093/intqhc/mzp052
18. Age-Related Eye Disease Study Research G. The age-related eye disease study (AREDS) system for classifying cataracts from photographs: AREDS report no. 4. Am J Ophthalmol. 2001;131(2):167–175. doi:10.1016/s0002-9394(00)00732-7
19. Siik S, Chylack Jr. LT Jr, Friend J, et al. Lens autofluorescence and light scatter in relation to the lens opacities classification system, LOCS III. Acta Ophthalmol Scand. 1999;77(5):509–514. doi:10.1034/j.1600-0420.1999.770504.x
20. Skiadaresi E, McAlinden C, Pesudovs K, Polizzi S, Khadka J, Ravalico G. Subjective quality of vision before and after cataract surgery. Arch Ophthalmol. 2012;130(11):1377–1382. doi:10.1001/archophthalmol.2012.1603
21. Jakobsson G, Montan P, Zetterberg M, Stenevi U, Behndig A, Lundstrom M. Capsule complication during cataract surgery: retinal detachment after cataract surgery with capsule complication: Swedish Capsule Rupture Study Group report 4. J Cataract Refract Surg. 2009;35(10):1699–1705. doi:10.1016/j.jcrs.2009.05.028
22. Tuft SJ, Gore DM, Bunce C, Sullivan PM, Minassian DC. Outcomes of pseudophakic retinal detachment. Acta Ophthalmol. 2012;90(7):639–644. doi:10.1111/j.1755-3768.2011.02124.x
23. Quek DT, Lee SY, Htoon HM, Ang CL. Pseudophakic rhegmatogenous retinal detachment in a large Asian tertiary eye centre: a cohort study. Clin Exp Ophthalmol. 2012;40(1):e1–7. doi:10.1111/j.1442-9071.2011.02610.x
24. Gonzalez N, Quintana JM, Bilbao A, et al. Factors affecting cataract surgery complications and their effect on the postoperative outcome. Can J Ophthalmol. 2014;49(1):72–79. doi:10.1016/j.jcjo.2013.09.013
25. Sheu SJ, Ger LP, Ho WL. Late increased risk of retinal detachment after cataract extraction. Am J Ophthalmol. 2010;149(1):113–119. doi:10.1016/j.ajo.2009.08.006
26. Boberg-Ans G, Henning V, Villumsen J, la Cour M. Longterm incidence of rhegmatogenous retinal detachment and survival in a defined population undergoing standardized phacoemulsification surgery. Acta Ophthalmol Scand. 2006;84(5):613–618. doi:10.1111/j.1600-0420.2006.00719.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optical Biometry and Lens Power Calculations in 500 Phakic Patients: Axial Length and Corneal Curvature in the Fellow Eye
Kristianslund O, Hassaf SE, Drolsum L
Clinical Ophthalmology 2022, 16:2775-2780
Published Date: 23 August 2022
Pars Plana Vitrectomy for Retained Lens Fragments After Cataract Surgery: Outcomes Based on Timing of Surgery
Rohowetz LJ, Jabbehdari S, Yannuzzi NA, Sridhar J, Smiddy WE, Berrocal AM, Albini TA, Townsend JH, Fortun JA, Flynn HW Jr
Clinical Ophthalmology 2023, 17:479-485
Published Date: 1 February 2023
Impact of Cataract Surgery on IOP and Ocular Structures in Normotensive Patients and Primary and Exfoliation Open-Angle Glaucoma Patients
Xirou V, Xirou T, Siganos C, Ntonti P, Georgakopoulos C, Stavrakas P, Makri OE, Kanakis M, Tsapardoni F, Fragkoulis I, Garnavou-Xirou C, Kozobolis V
Clinical Ophthalmology 2023, 17:1047-1055
Published Date: 5 April 2023
The Impact of Vergence Dysfunction on Myopia Control in Children Wearing Defocus Spectacle Lenses
Ma J, Yang X, Liu Z, Fu H, Fan S, Wang K, Li Y, Huang L, Zhao M
Clinical Ophthalmology 2024, 18:799-807
Published Date: 12 March 2024
Impact of Forms of Visual Attenuation on Short-Term Eye Changes Under Controlled Reading Visibility

Su H, Chun RKM, De Lestrange-Anginieur E
Eye and Brain 2024, 16:133-146
Published Date: 4 December 2024