Back to Journals » International Journal of General Medicine » Volume 18
Ocular Biometric Parameters of Acute Primary Angle Closure with Varying Degrees of Lens Zonular Laxity
Authors Wang Q ![]() , Wang X
, Wang X ![]() , Huang B, Liu Y, Zhang S, Lu H
, Huang B, Liu Y, Zhang S, Lu H
Received 6 August 2025
Accepted for publication 19 November 2025
Published 10 December 2025 Volume 2025:18 Pages 7425—7432
DOI https://doi.org/10.2147/IJGM.S558791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Brian C. Gilger
Qian Wang,1 Xinyu Wang,2 Bingyao Huang,1 Yanjing Liu,1 Shengnan Zhang,1 Hui Lu1
1Department of Ophthalmology, Zibo Central Hospital, Zibo, Shandong, 255000, People’s Republic of China; 2Shandong Second Medical University, Weifang, Shandong, 261053, People’s Republic of China
Correspondence: Hui Lu, Department of Ophthalmology, Zibo Central Hospital, Zibo, Shandong, 255000, People’s Republic of China, Tel +86-18678187916, Email [email protected]
Background: Acute primary angle closure (APAC) is a leading cause of irreversible blindness. Recent studies suggest lens zonular laxity plays a critical role in APAC pathogenesis, though its clinical detection remains challenging due to overlapping symptoms with cataract. This study investigates the prevalence of subclinical zonular degeneration in APAC patients and its correlation with ocular biometric parameters.
Methods: This retrospective cohort study included 65 APAC patients (mean age 62.3 ± 8.7 years) undergoing phacoemulsification at Zibo Central Hospital (November 2021–May 2023). Patients were stratified into three groups based on intraoperative zonular status: normal zonula (APAC-NZ, n=14), mild zonular laxity (APAC-ZL, n=39), and significant zonular laxity (APAC-SZL, n=12). Preoperative axial length (AL), lens thickness (LT), and anterior chamber depth (ACD) were measured using IOLMaster 5.0 and swept-source UBM.
Results: A high prevalence (78.5%, 51/65) of undiagnosed zonular degeneration was observed. Significant differences were found in sitting ACD (2.25 ± 0.17 mm vs 1.75 ± 0.19 mm), supine ACD (1.72 ± 0.11 mm vs 1.27 ± 0.12 mm), and LT (5.10 ± 0.28 mm vs 5.41 ± 0.38 mm) between APAC-NZ and APAC-SZL groups (P< 0.05). Similar differences were noted between APAC-SZL and APAC-ZL groups (P< 0.05).
Conclusion: This study introduces a novel stratification of APAC patients by zonular laxity severity and reveals distinct biometric profiles across subgroups. We demonstrate a high prevalence of undiagnosed zonulopathy in APAC patients, associated with thicker lenses and shallower anterior chambers. A key limitation is the subjective classification of zonular laxity, based solely on intraoperative observations. Future studies should develop objective imaging protocols for improved detection and management.
Keywords: acute primary angle closure, zonular laxity, axial length, lens thickness, anterior chamber depth
Introduction
Acute primary angle closure (APAC) is a sight-threatening ophthalmic emergency that requires immediate intervention to prevent severe and irreversible vision loss.1,2 Emerging evidence suggests that lens zonular abnormalities play a significant role in the pathogenesis of APAC, contributing to the displacement of the iris-lens diaphragm, anterior chamber shallowing, and angle closure.3,4 Notably, reported prevalence rates of zonular laxity in APAC vary considerably across studies, ranging from approximately 30% to over 70%, highlighting the need for more standardized diagnostic criteria.4–7
Recent studies have significantly advanced our understanding of zonulopathy in angle closure disease. Salimi et al5 first systematically documented the high prevalence of zonulopathy in primary angle closure disease, reporting a rate of 69% in their cohort and highlighting the clinical significance of this underdiagnosed condition. Subsequent work by Zhang et al6 further delineated biometric characteristics associated with zonular weakness, identifying several anterior segment parameters that may serve as preoperative predictors. More recently, Chen et al7 conducted a comprehensive analysis of ocular biometric characteristics in acute angle closure with and without zonular laxity, providing valuable insights into the distinct anatomical features associated with zonular insufficiency. Our study builds upon this growing body of evidence by introducing a novel three-tier stratification system for zonular laxity and investigating its relationship with multiple biometric parameters under varying positional conditions.
Zonulopathy not only exacerbates the disease but also complicates surgical management, as patients with zonular abnormalities are at higher risk of intraoperative and postoperative complications.8–10 In recent years, phacoemulsification with intraocular lens implantation combined with goniosynechialysis has emerged as the primary surgical intervention for APAC.11,12 Intraoperative assessment of zonular laxity, particularly through observations during continuous curvilinear capsulorhexis (CCC), such as capsular bag displacement and anterior capsule wrinkling, has proven to be a reliable method for evaluating zonular instability.5,10 These subtle indicators, frequently undetectable during preoperative examination, offer crucial intraoperative guidance for surgical planning and technique modification.10,13
This study aims to analyze ocular biometric parameters in APAC patients with varying degrees of zonular laxity, focusing on identifying differences in these parameters among patient subgroups. By exploring the relationship between zonular laxity and specific biological markers, this research seeks to establish effective diagnostic indicators for zonulopathy severity. The findings may provide a theoretical foundation for improving preoperative diagnosis and optimizing surgical strategies for APAC patients with zonular abnormalities.
Materials and Methods
Study Design and Patients
This retrospective study was conducted at Zibo Central Hospital, Shandong Province, China, following approval from the hospital’s Human Research Ethics Committee and in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
Medical records of patients diagnosed with both acute primary angle closure (APAC) and cataract, who underwent cataract surgery between November 1, 2021, and May 31, 2023, were retrospectively reviewed from November 1, 2023, to November 30, 2023. All patients underwent comprehensive preoperative ocular examinations, including best-corrected visual acuity, slit-lamp microscopy, gonioscopy, Goldmann intraocular pressure (IOP) measurements, fundus examinations, and biometric assessments using the IOL Master. Key ocular biometric parameters, such as axial length (AL), anterior chamber depth (ACD), and lens thickness (LT), were recorded. Additionally, ultrasound biomicroscopy (UBM) was performed by a single experienced ophthalmologist to evaluate lens position and supine ACD. Both sitting and supine ACD were measured, allowing for a more comprehensive assessment of anterior chamber dynamics under different positional conditions. All surgical procedures were conducted by the same experienced surgeon.
Based on intraoperative observations of zonular laxity, patients were categorized into three groups: the normal zonule group (APAC-NZ), the mild zonular laxity group (APAC-ZL), and the significant zonular laxity group (APAC-SZL). This stratification allowed for comparative analysis of ocular biometric parameters among the groups.
Inclusion and Exclusion Criteria
Acute angle closure was described as14 (1) having at least two of the following symptoms: pain in the eye or around the eye; feelings of nausea and/or episodes of vomiting; and a past of vision becoming unfocused intermittently with haloes; (2) having an IOP reading higher than 21 mmHg during a Goldmann applanation tonometry test; (3) showing at least three of the following signs: redness in the conjunctiva, swelling in the corneal epithelium, pupil that is partially dilated and unresponsive to light, and a shallow space in the front of the eye; and (4) having evidence of angle closure observed during a gonioscopy examination.
All participants received surgery for APAC, where the phacoemulsification cataract extraction with intraocular lens implantation along with goniosynechialysis were performed by a single ophthalmologist. During surgery, CCC was performed using capsulorhexis forceps and no capsular tension rings were implanted in any of the cases. Previous research has indicated that eyes exhibiting movement of the complete capsular bag during the capsular flap propagation, anterior capsule striae during CCC, and lack of zonular dehiscence were identified as APAC with zonular laxity.7,9,10 In this study, the movement of the entire capsular bag during propagation of the capsular flap and anterior capsule striae during CCC intraoperatively without zonular dehiscence was defined as APAC with zonular laxity. In addition, in some cases, the capsular bag was unstable during phacoemulsification and cortex infusion. Elongated lens zonule without zonular dehiscence, equator of lens, irregular anterior capsule orifice and fold of posterior capsule were found after the cortex infusion, which were diagnosed as APAC with significant zonular laxity. Patients with shallow anterior chamber and narrow angle in both eyes, but lacking indications of zonular laxity, were identified as APAC without zonular laxity.7
The exclusion criteria for this study included individuals with a history of acute angle closure (AAC) attack or primary angle closure glaucoma in either eye, lens subluxation due to zonular dehiscence detected preoperatively by ultrasound biomicroscopy scan or during surgery, history of ocular surgeries such as peripheral iridotomy or iridoplasty, or trauma, and AAC caused by other ocular diseases like pseudoexfoliation syndrome, retinitis pigmentosa, Marfan syndrome, homocystinuria, Weill-Marchesani syndrome.7
Statistical Analysis
The statistical analysis was conducted using version 27.0 of SPSS (IBM Corporation, Armonk, NY, USA). The mean ± standard deviation was used to express quantitative data. One-way analysis of variance was applied to analyze quantitative data. The Chi-squared test was used to analyze categorical data. A significance level of P < 0.05 was utilized to determine statistical significance.
Results
This study included 65 participants with a total of 65 eyes affected. No zonular abnormalities were found in 65 cases through detailed preoperative examination. According to the intraoperative observation of zonular status, 39 eyes belonged to the cohort with zonular laxity, while 12 eyes belonged to the cohort with significant zonular laxity, and 14 eyes belonged to the normal zonule cohort. Table 1 summarizes the demographics and past trauma histories of the 3 groups. Although there was a higher number of females in both groups, the variation in the gender ratio between the groups did not demonstrate any statistical significance (P = 0.773). None of the subjects exhibited any prior eye or head injuries. The age distribution demonstrated no noteworthy variations across the three cohorts (P = 0.941). It should be noted that the relatively small sample size in the APAC-SZL group (n=12) may limit the statistical power for detecting more subtle group differences.
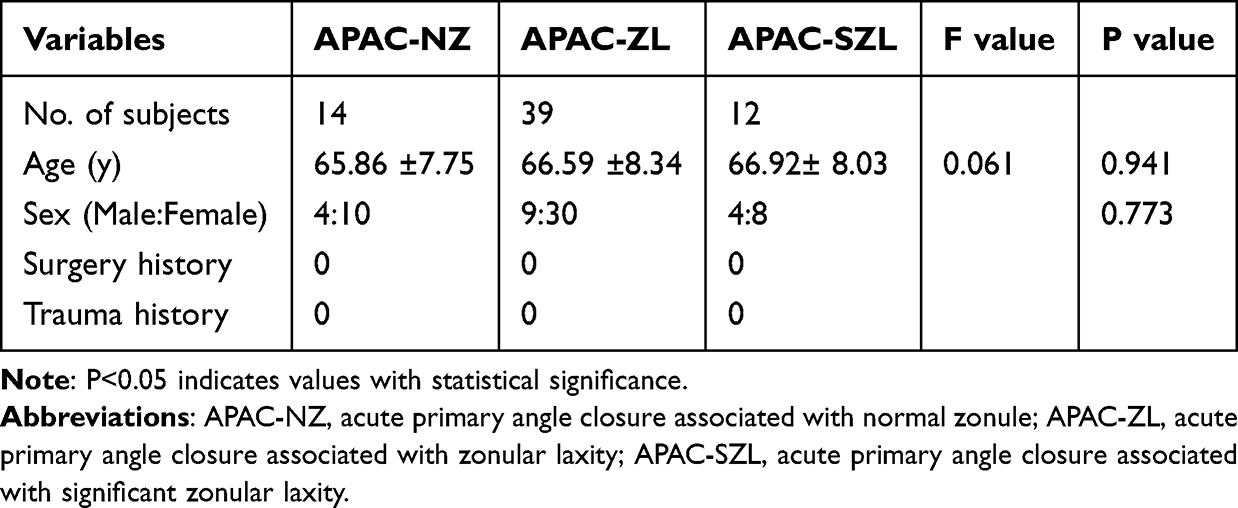 |
Table 1 The Demographic and Past Histories of the Normal Zonule, Zonular Laxity and Significant Zonular Laxity Cohorts |
Table 2 illustrates inter-eye comparisons between the affected eyes and their corresponding unaffected eyes of the APAC-NZ group, the APAC-ZL group and the APAC-SZL group. The ACD, LT and AL of the affected eyes show no significant difference with the unaffected eyes in both groups (all P > 0.05). Our results stand in contrast to several previous studies that consistently reported significant interocular asymmetries in anterior segment parameters among APAC patients.7 First, unlike previous studies that included patients with unilateral anatomical predisposition, our cohort exclusively comprised bilateral narrow angle cases, creating a more symmetric baseline population. Second, the limited sample size in our APAC-SZL subgroup (n=12) reduces statistical power to detect subtle inter-eye differences. Third, zonular laxity in APAC may represent a fundamentally bilateral process, with acute attacks being precipitated by dynamic factors such as pupillary block rather than anatomical asymmetry—a view corroborated by Zhang et al6 who reported similar bilateral involvement.
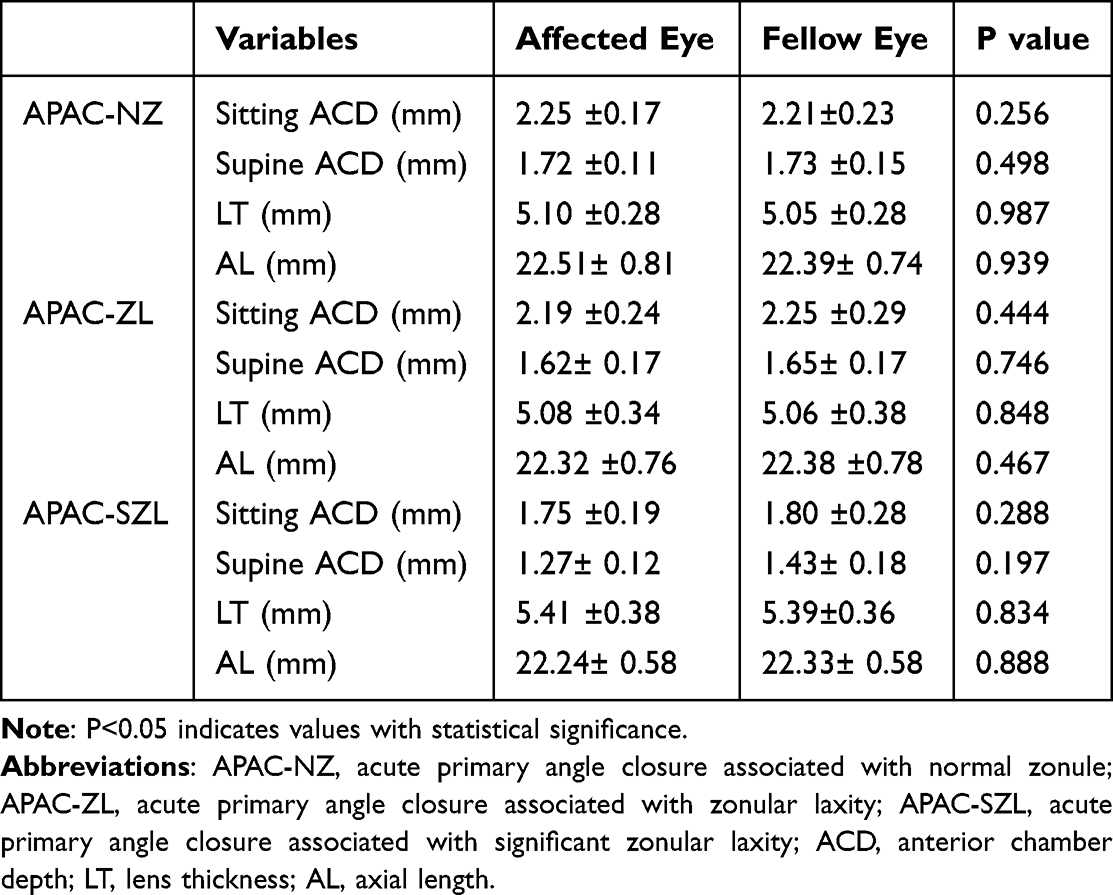 |
Table 2 The Intereye Comparison of Subjects in the the Normal Zonule, Zonular Laxity and Significant Zonular Laxity Groups |
Tables 3 and 4 present the ocular biometric data of the 3 cohorts. There was no statistically difference in sitting ACD [(2.25 ±0.17) mm vs (2.19 ±0.24) mm], supine ACD[(1.72 ±0.11) mm vs (1.62± 0.17) mm], LT[(5.10 ±0.28) mm vs (5.08 ±0.34) mm] and AL[(22.51± 0.81) mm vs (22.32 ±0.76) mm] between APAC-NZ group and the APAC-ZL group (P=0.396, P=0.052, P=0.804, P=0.423). Sitting ACD[(2.25 ±0.17) mm vs (1.75 ±0.19) mm], supine ACD[(1.72 ±0.11) mm vs (1.27± 0.12) mm] and LT[(5.10 ±0.28) mm vs (5.41 ±0.38) mm] showed statistical difference between APAC-NZ group and the APAC-SZL group (P=0.000, P=0.000, P=0.027). Comparing the APAC-SZL group to the APAC-ZL group, sitting ACD[(1.75 ±0.19) mm vs (2.19 ±0.24) mm], supine ACD[(1.27± 0.12) mm vs (1.62± 0.17) mm], LT[(5.41 ±0.38) mm vs (5.08 ±0.34) mm] reached statistical significance (P=0.000, P=0.000, P=0.006).
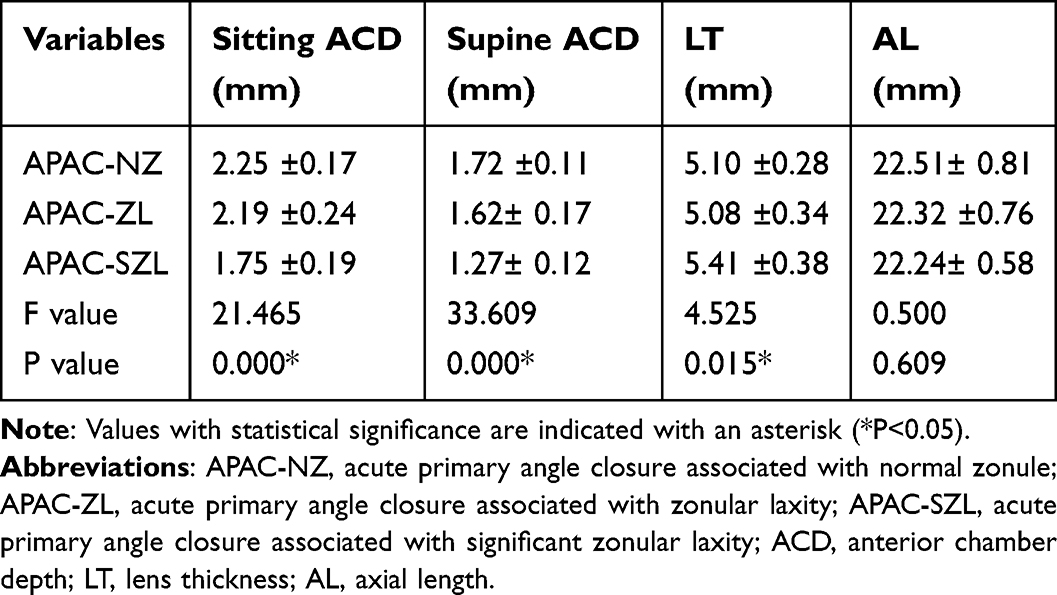 |
Table 3 The Ocular Biometric Data from Affected Eyes of the Normal Zonule, Zonular Laxity and Significant Zonular Laxity Cohorts |
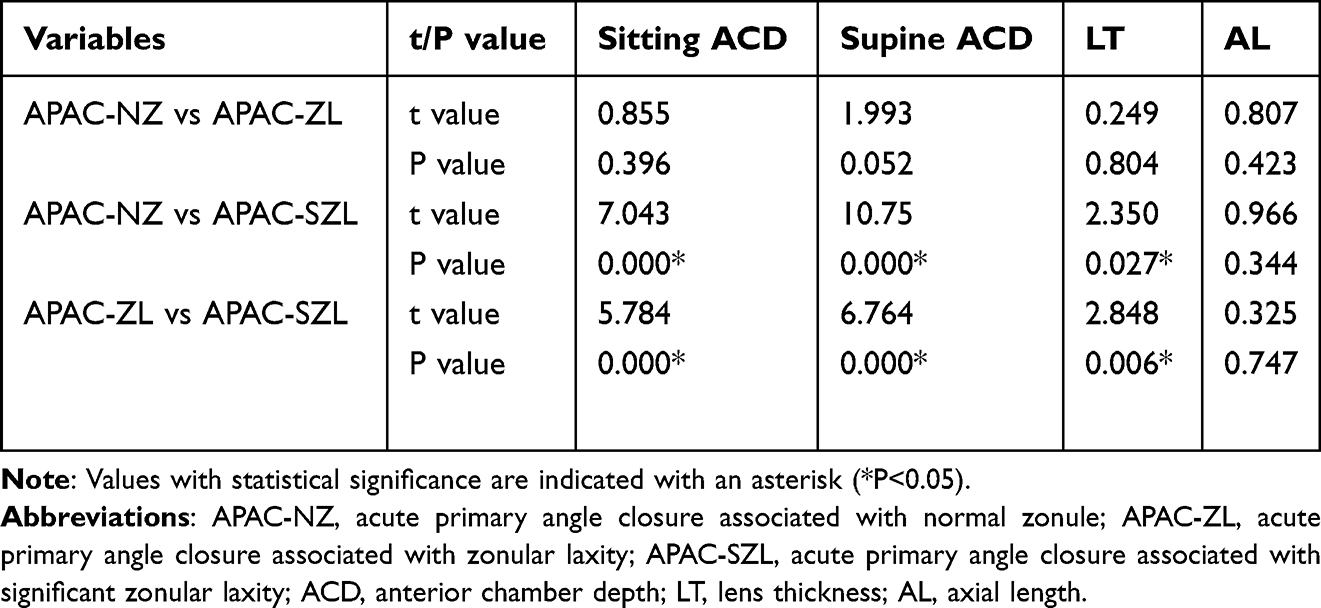 |
Table 4 The Pairwise Comparison of Ocular Biometric Data from the Normal Zonule, Zonular Laxity and Significant Zonular Laxity Cohorts |
Compared with the other two groups, the values of ACD and LT in the APAC-SZL group were significantly different, which indicated that the zonula may be significant abnormal in APAC patients with a thicker LT and a shallower ACD.
Figure 1A–C, show representative cases from the APAC-SZL group, the APAC-ZL group and the APAC-NZ group respectively. Before the cataract surgery, a 70-year-old woman experienced an APAC attack in her left eye, characterized by a peak IOP of 60mmHg. After duration of around 2 weeks, surgical intervention was performed on her left eye. The UBM images obtained prior to the surgery exhibited indications of a shallow anterior chamber depth in both eyes. During the operation, wrinkles appeared in the anterior capsule during CCC. The capsular bag was unstable during phacoemulsification and cortex infusion. Intraocular hypertension and iris prolapse were observed during phacoemulsification. Anterior capsule orifice is irregular after implantation of the IOL because of significant zonular laxity (Figure 1A). The capsular bag instability, intraocular hypertension and iris prolapse were observed during phacoemulsification in 8 of the 12 cases in the APAC-SZL group. Figure 1B shows the images of a 77-year-old man with a history of APAC attack in his right eye. His peak IOP was 45mmHg. During the operation, there were wrinkles in capsulorhexis, no rupture of the zonule and no significant change in capsulorhexis after injection and suction of the cortex. A 75-year-old man suffering from APAC for two weeks underwent phacoemulsification combined with goniosynechialysis. The the capsular bag were stable and no anterior capsule striae were found during CCC intraoperatively (Figure 1C).
 |
Figure 1 The UBM image, anterior segment photography and observations during cataract phacoemulsification surgery. (A1 and B1 and C1) Anterior segment photography and (A2 and B2 and C2) UBM image indicate shallow anterior chamber. (A3) Blue arrow shows irregular wrinkles of the anterior capsule during continuous circular capsulorhexis. (B3) Blue arrow shows regular wrinkles of the anterior capsule during continuous circular capsulorhexis. (C3) Blue arrow shows no wrinkles of the anterior capsule during continuous circular capsulorhexis. (A4) Yellow arrows indicate the irregular anterior capsule orifice after implantation of the IOL. (B4 and C4) Yellow arrows indicate the regular anterior capsule orifice after implantation of the IOL. |
Discussion
The lens has been strongly implicated as a central anatomical factor in APAC development.4,5,15,16 Pathogenic mechanisms primarily include increased lens thickness and anterior positioning, heightened anterior lens curvature leading to anterior segment crowding, as well as pupillary and lenticular blocks, all of which may precipitate elevated intraocular pressure.6,15,16
In the present study, we observed a higher prevalence of zonular abnormalities in APAC eyes. These compromised zonular fibers were associated with characteristic lenticular changes, including lens thickening and anterior protrusion, manifesting as a steeper anterior lens curvature, greater lens vault, and anterior displacement of the iris-lens diaphragm. The resultant forward shift of the lens secondary to zonular incompetence appears closely related to angle narrowing and closure, underscoring its significant contribution to APAC pathogenesis.
The present study analyzed ocular biometric parameters in APAC patients with age-related cataracts who showed no preoperative signs of zonular laxity on slit-lamp or UBM examination but were intraoperatively confirmed to have zonular weakness. Notably, 78.5% of the cohort exhibited intraoperative zonular laxity that had been missed by conventional preoperative screening. These findings underscore the diagnostic challenges associated with subtle zonular insufficiency. As reported in the literature, conventional slit-lamp examination rarely identifies early zonular weakness in the absence of marked phacodonesis or lens subluxation.17 Although UBM allows improved visualization of the ciliary body and zonular structures, its resolution remains inadequate for reliably detecting partial or diffuse zonular degeneration.18,19 In our series, UBM missed 78.5% of surgically confirmed zonular weakness cases. This high miss rate aligns with the established sensitivity range of 45–65% and specificity of 70–85% reported for UBM in detecting such abnormalities.18,19 The 78.5% prevalence of zonular abnormalities observed in our APAC cohort is notably higher than the 60–70% range reported in most previous studies.5,6 We have identified several factors that may explain this discrepancy. Our study specifically enrolled APAC patients requiring surgery, who likely represent a more advanced disease stage than those in broader APAC cohorts. Furthermore, our systematic intraoperative assessment protocol was designed to capture subtle signs of zonular weakness—such as anterior capsule wrinkling during capsulhexis and mild capsular bag instability—that are often missed in routine surgical documentation.
At present, the standard for diagnosing zonular laxity is based on intraoperative manifestations.4–6 In this study, the degree of zonular laxity was graded according to intraoperative findings, and the results varied greatly among different degrees. There was no statistically difference in ACD, LT or AL between the APAC-NZ group and the APAC-ZL group. However, compared with APAC-SZL group, the differences in ACD and LT were statistically significant. Salimi et al5 also found that a shallower ACD may indicate lens zonular abnormality through a logistic regression analysis. An earlier study discovered that shallow ACD and thick LT were associated with increased proportion of zonulopathy.6 Chen’s research7 showed that ACD was smaller in APAC patients with zonular laxity than in patients without zonular laxity and were smaller in affected eyes than in fellow eyes in APAC patients. Our results revealed that there were no significant difference in ACD, LT, and AL between affected eyes and fellow eyes in both groups. The small sample size may be the reason for the discrepancy in the results.
Significant zonular laxity is a concerning factor that has been linked to various complications during surgery and negative outcomes after surgery. These complications include vitreous prolapse, capsular rupture or contraction, and IOL decentration or dislocation.8–10 Previous research6,15,16 has indicated that eyes exhibiting movement of the complete capsular bag during the capsular flap propagation, anterior capsule striae during CCC, and lack of zonular dehiscence were identified as APAC with zonular laxity. This study found that in addition to the above manifestations, in some cases the capsular bag was unstable during phacoemulsification and cortex infusion. Elongated lens zonule without zonular dehiscence, equator of lens, irregular anterior capsule orifice and fold of posterior capsule were found after the cortex infusion, which were diagnosed as APAC with significant zonular laxity. There was no significant difference in the biological parameters of these cases with zonular laxity compared with the other two groups, while there was a significant difference between the cases with significant zonular laxity compared with the other two groups. In previous studies on zonular laxity, the degree of laxity was not graded. The difference in biological parameters of significant zonular laxity is more clinically significant and can provide greater guidance for surgery.
The intraoperative use of a capsular tension ring (CTR) has been shown to be beneficial in eyes with evidence of zonular weakness, as it can help prevent complications both during and after surgery.5,20 The CRT serves the important function of maintaining the circular contour of the capsule, while also distributing forces equally over the weakened zonula. This helps to minimize the risk of applying excessive and uneven force to areas with zonular weakness, reducing the likelihood of further damage or complications. Some researchers have found that the implantation of CRT is related to the occurrence of malignant glaucoma.21,22 The contact of CTR and the ciliary body could induce an apparent ciliary block.21,22 In this study, in the APAC-SZL group, the IOL was implanted with no CRT implanted, and the 1-year follow-up showed that the IOL was located in a good position, indicating that good surgical results could be achieved without the CRT.
There are some limitations to our study that should be discussed. The sample size of this study is relatively small, which limited the statistical power of our analysis and maybe the reason for the low proportion of significant zonular laxity. In addition, the lack of extended patient surveillance may have potentially contributed to the underestimation of adverse events in the long-term. Further well-designed and large-sized studies may be required to further study the relationship between zonule and angle-closure glaucoma. Furthermore, an important limitation of this study is the inherent subjectivity in classifying zonular laxity, as it relied entirely on intraoperative observation in the absence of objective, quantifiable metrics. Future research efforts should therefore be directed toward establishing standardized parameters to objectify this assessment.
Conclusions
The proportion of underdiagnosed zonulopathy among APAC patients is high. Our data suggest an association between more severe zonular abnormality and a combination of a thicker lens and a shallower anterior chamber in APAC patients. However, this preliminary finding necessitates further large-sized investigations to establish its clinical validity and diagnostic value.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang H, Cao K, Jia H, et al. Clinical characteristics, rates of blindness, and geographic features of PACD in China. Can J Ophthalmol. 2021;56(5):299–306. doi:10.1016/j.jcjo.2020.12.010
2. Prum BE, Herndon LW, Moroi SE, Mansberger SL, Stein JD, Lim MC. Primary angle closure preferred practice pattern guidelines. Ophthalmology. 2016;123(1):P1–P40. doi:10.1016/j.ophtha.2015.10.049
3. Allingham RR, Damji KF, Freedman SF, Moroi SE, Rhee DJ. Shields MB. Shields’ Textbook of Glaucoma.
4. Kwon J, Sung KR. Factors associated with zonular instability during cataract surgery in eyes with acute angle closure attack. Am J Ophthalmol. 2017;183:118–124. doi:10.1016/j.ajo.2017.09.003
5. Salimi A, watt H, Harasymowycz P, Abu‐Nada M, Wang A, Harasymowycz P. Prevalence of zonulopathy in primary angle closure disease. Clin Exp Ophthalmol. 2021;49(8):1018–1026. doi:10.1111/ceo.13983
6. Zhang H, Zhang Y, Zhang S, et al. Zonulopathy identified during cataract extraction in patients with primary angle closure disease. J Glaucoma. 2023;32(9):783–791. doi:10.1097/IJG.0000000000002247
7. Chen H, Ye L, Chen L, et al. Ocular biometric characteristics in preoperative diagnosis of acute angle closure with and without zonular laxity. J Glaucoma. 2024;33(3):195–205. doi:10.1097/IJG.0000000000002307
8. Dureau P. Pathophysiology of zonular diseases. Curr Opin Ophthalmol. 2008;19(1):27–30. doi:10.1097/ICU.0b013e3282f29f01
9. Miyoshi T, Fujie S, Yoshida H, Iwamoto H, Tsukamoto H, Oshika T. Effects of capsular tension ring on surgical outcomes of premium intraocular lens in patients with suspected zonular weakness. PLoS One. 2020;15(2):e0228999. doi:10.1371/journal.pone.0228999
10. Shingleton BJ, Neo YN, Cvintal V, Shaikh AM, Liberman P, O’Donoghue MW. Outcome of phacoemulsification and intraocular lens implantation in eyes with pseudoexfoliation and weak zonules. Acta Ophthalmol. 2017;95(2):182–187. doi:10.1111/aos.13110
11. Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389–1397. doi:10.1016/S0140-6736(16)30956-4
12. Qiao C, Zhang H, Cao K, et al. Changing trends in glaucoma surgery over the past 5 years in China. J Glaucoma. 2022;31(5):329–334. doi:10.1097/IJG.0000000000002004
13. Yaguchi S, Asano Y, Aoki S, et al. Categorization and surgical techniques of weak zonule based on findings at capsulorhexis during cataract surgery. J Clin Exp Ophthalmol. 2015;6(2):407.
14. Sng CC, Aquino MC, Liao J, et al. Pretreatment anterior segment imaging during acute primary angle closure: insights into angle closure mechanisms in the acute phase. Ophthalmology. 2014;121(1):119–125. doi:10.1016/j.ophtha.2013.08.004
15. Lee BW, Lau FS, Wong EL, et al. Lessons from management: perioperative phacoemulsification planning following resolution of acute angle closure. Cureus. 2021;13(4):e14331. doi:10.7759/cureus.14331
16. Pei X, Qing G. Biometric characteristics of primary angle closure glaucoma with zonular abnormality found during cataract surgery. Yan Ke Xue Bao. 2021;30(4):264–269.
17. Jacobi PC, Dietlein TS, Krieglstein GK. Comparative study of slit-lamp biomicroscopy and ultrasound biomicroscopy in the evaluation of the anterior segment in pseudophakic eyes. J Cataract Refract Surg. 2001;27(11):1842–1848.
18. Miki A, Shirakashi M, Kunikata H, et al. Comparison of ultrasound biomicroscopic findings between acute primary angle closure and eyes with narrow angles. Am J Ophthalmol. 2017;178:118–125.
19. Kumar DA, Agarwal A, Jacob S, Prakash G. Ultrasound biomicroscopy in the management of zonular weakness in pseudoexfoliation. Ophthalmology. 2020;127(11):1541–1550.
20. Weber CH, Cionni RJ. All about capsular tension rings. Curr Opin Ophthalmol. 2015;26(1):10–15. doi:10.1097/ICU.0000000000000118
21. Modesti M, Pasqualitto G, Appolloni R, Pecorella I, Sourdille P. Preoperative and postoperative size and movements of the lens capsular bag: ultrasound biomicroscopy analysis. J Cataract Refract Surg. 2011;37(10):1775–1784. doi:10.1016/j.jcrs.2011.04.035
22. Lin H, Zhou G, Zhang S, Huang F, Liang Y. One-year outcome of low dose laser cyclophotocoagulation for capsular tension ring-induced malignant glaucoma: a case report. Medicine. 2020;99(6):e18836. doi:10.1097/MD.0000000000018836
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation of Ocular Biometry with Axial Length in Elderly Japanese
Tanaka T, Nishitsuka K, Obata H
Clinical Ophthalmology 2024, 18:351-360
Published Date: 3 February 2024
Intra- and Inter-Observer Agreement of a Portable A-Scan Ultrasound Biometer in Sitting and Supine Positions and Validity Against an Optical Biometer
Jeyandran J, Roberts CJ, Yuhas PT
Clinical Optometry 2025, 17:283-296
Published Date: 5 September 2025