Back to Journals » Infection and Drug Resistance » Volume 15
Occult Hepatitis B Virus Infection and Its Risks of Cryptic Transmission in Southern Ethiopia
Authors Beykaso G, Mulu A, Giday M, Berhe N ![]() , Selamu M
, Selamu M ![]() , Hailu D, Teklehaymanot T
, Hailu D, Teklehaymanot T
Received 15 October 2021
Accepted for publication 7 February 2022
Published 24 February 2022 Volume 2022:15 Pages 619—630
DOI https://doi.org/10.2147/IDR.S344668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Gizachew Beykaso,1,2 Andargachew Mulu,3 Mirutse Giday,1 Nega Berhe,1 Markos Selamu,2 Dawit Hailu,3 Tilahun Teklehaymanot1
1Aklilu Lemma Institute of Pathobiology, Department of Molecular Biology and Immunology, Addis Ababa University, Addis Ababa, Ethiopia; 2College of Medicine and Health Sciences, Department of Public Health, Wachemo University, Hossana, Ethiopia; 3Armauer Hansen Research Institute, Department of Virology, Addis Ababa, Ethiopia
Correspondence: Gizachew Beykaso, Tel +251-912066531, Email [email protected]
Background: The detection of hepatitis B virus surface antigen (HBsAg) in serum remains the mainstay in diagnosing and screening of hepatitis B virus (HBV) in most developing countries. The absence of HBsAg in the blood may not indicate the absence of circulating HBV and might be infectious. Thus, this study aimed to estimate the burden and its cryptic transmission risks of occult hepatitis B infection (OBI) among HBsAg negative healthy individuals in Southern Ethiopia.
Methods: A community-based cross-sectional study was conducted from September 2020 to January 2021. Serum samples were collected and assayed for HBsAg and HBV core antibody (anti-HBc) seromarkers using enzyme-linked immunosorbent assay (ELISA). In anti-HBc positive samples, HBV DNA was detected using real-time polymerase chain reaction (RT-PCR). Data were entered into Epi-Data version 3.1, cleaned, and analyzed using SPSS version 21.0. Descriptive and logistic regression analyses were employed. Statistical significance was decided at p < 0.05.
Results: A total of 346 were individuals included in this study; 34 (9.8%) were tested positive for HBsAg. The rest 312 (90.2%) negatively tested were further assayed for anti-HBc, and 115 (36.7%) were found positive implying previous exposure to HBV, and 21 (18.3%) out of 115 anti-HBc positives had HBV DNA signifying OBI. The HBV DNA concentration below 200 IU/mL was 85.7%. A high rate of OBI was observed among individuals who had multiple sexual contacts, a family history of hepatitis, and tattooing.
Conclusion: In this study, the prevalence of OBI is high. This indicates the burden of HBV is considerable since screening is exclusively dependent on HBsAg which will not eliminate the possibility of residual cryptic transmission through blood donation, organ transplantation, perinatal transmission, and other contacts. Our results demonstrate that nucleic acid-based testing (NAT) should be an essential part of screening to prevent missing OBI.
Keywords: anti-HBc, HBV, HBV DNA, OBI, Southern Ethiopia
Introduction
HBV infection remains the primary cause of liver cirrhosis, and hepatocellular carcinoma (HCC), which are major contributors to global morbidity and mortality.1,2 The concurrent presence of HBsAg and HBs antibodies (anti- HBs) are observed in both acute and chronic HBV infection. The persistence of serum HBsAg for more than 6 months after acute infection is clinically defined as chronic HBV infection.3 Chronically infected individuals potentially have high levels of anti-HBc in their serum in addition to HBsAg.4 Chronic HBV carriers’ state is characterized by the presence of HBsAg and anti-HBc, as it produces the hepatitis B envelope antigen (HBeAg) during an active replication phase.5–7 Anti-HBc occurs in individuals who have experienced natural infection with HBV and its presence in the absence of HBsAg is usually interpretable as evidence of previous HBV exposure.8,9 The presence of anti-HBc without both HBsAg and anti-HBs is referred to as isolated anti-HBc (IA HBc).9 The positivity of anti-HBc provides not only evidence of prior infections but also a risk of an ongoing OBI.10,11
OBI is the presence of HBV DNA in the liver, with detectable or undetectable HBV DNA in the serum, of HBsAg-negative individuals12,13 and is variably called serologically silent HBV infection or cryptic HBV infection.14 It is associated with the long-term persistence of viral covalently closed circular DNA (cccDNA) in the nuclei of hepatocytes.15 The possible reasons include low-copy numbers of HBV DNA, epigenetic regulation,16 altered host immune response,17 genetic variations of the S gene,18 viral DNA integration in the host genome,19 immune complexes in which HBsAg is hidden,17,20 and interference of other viruses such as HCV21,22 and HIV.23,24 In most resource-limited settings, OBI is commonly detected by the investigation of serum samples as liver biopsy examinations are not routinely available. When detectable, the amount of HBV DNA in the serum is usually very low (<200 IU/mL).16 About 20% of all OBIs are negative for all serological HBV markers which are termed as seronegative OBI, with the rest 80% being seropositive OBI, positive for anti-HBc and/or anti-HBs in the serum.1,25
The prevalence of anti-HBc and OBI varies depending on the endemicity of the HBV. In low endemic areas, anti-HBc is found in 10–20% of all individuals with HBV markers.26 In high endemic sub-Saharan and Asian regions, the prevalence of anti-HBc has been reported in up to 50% among the general population.27,28 The correlation levels of HBV DNA and HBV seromarkers among individuals with OBI, the lowest HBV DNA level was reported in individuals who were negative for all seromarkers or seronegative, intermediate in anti-HBc negative and anti-HBs positives, and highest (10–80%) in individuals who were anti-HBc positive but anti-HBs negative or anti-HBc only.29,30 Individuals in this last group are more likely to be infectious, suggesting that anti-HBc does not result in complete HBV exclusion.31 Blood and blood products containing anti-HBc without detectable HBsAg might be infectious.32 Reports indicated the evidence of HBV transmission through sexual contact, perinatal transmission, hemodialysis, blood transfusion, and organ transplantation are among the clinical consequences of OBI in the absence of HBsAg.28,33 Additionally, OBI can cause cryptogenic cirrhosis, acute exacerbation, or fulminant hepatitis and development of HCC,17 however, an individual’s immune status and HBV DNA numbers of copies determine the clinical outcome of occult HBV transmission.34,35
Ethiopia is grouped among HBV high endemic countries; however, there is no report on the epidemiology of OBI so far among the general population. This indicates that the burden of OBI has a significant public health implication due to the possibility of HBV transmission through blood transfusion, organ transplantation, perinatal transmission, and transmission due to other contacts in addition to reactivation of liver diseases, as screening is exclusively dependent on HBsAg testing. Thus, this study aimed to determine the magnitude of OBI among the general population in Southern Ethiopia.
Materials and Methods
Study Setting and Period
The study was conducted from September 2020 to January 2021 in three zonal districts of Southern Ethiopia: Hadiya, Kambata, and Silte districts.
Study Design
A community-based cross-sectional study was conducted to identify OBI and its hidden transmission risks among the general population of Southern Ethiopia.
Study Population
The study participants were all individuals age 5 years and above, residents of the study districts, and volunteered to participate in the study. The study was carried out in HBsAg negative and anti-HBc positive individuals for HBV DNA extraction, amplification, and quantification.
Sample Size Estimation and Sampling Method
The sample size was calculated with the assumptions pooled seroprevalence of HBsAg in community-based studies 8.036 with 95% confidence interval, 3% margin of error, and finally by 10% further increased sample size to account for contingencies such as non-response and recording errors. Accordingly, these resulted in a minimum sample size of 346. Based on these estimations, 139 individuals from Hadiya, 122 from Kambata, and 85 from Silte districts were involved by proportional allocation. The households from each district were selected using a systematic random sampling technique after getting the Kth value by dividing the total number of households by the sample size. From each selected household, one participant was randomly recruited using the lottery method of these individuals who were in their houses during home visits. The study was carried out in 346 individuals for HBsAg, of which 312 individual samples were HBsAg negative. Finally, 115 anti-HBc positive samples from HBsAg negative individuals were used for HBV DNA extraction, amplification, and quantification.
Data Processing and Analysis
Data were cleaned and entered using Epi-Data version 3.1 and analyzed using SPSS version 21.0. Descriptive statistics; mean and standard deviation for continuous, and frequency for categorical variables were used. A binary logistic regression model was fitted to identify factors associated with seroprevalence for OBI infections. All significant variables in bivariate logistic analysis were taken as candidates for multivariate analysis. Those independent variables which indicated association in the binary logistic regression analysis were considered as final predictors of the dependent variable. The variables that indicated significant associations were reported by using p-value, odds ratios, and 95% CI. A p-value <0.05 was used statistically significantly.
Data Collection Process and Tools
About 5 mL of blood sample was collected from each individual using a sterile syringe. The serum was separated from the whole blood sample by centrifuging the blood at 2000 r/min for 5 minutes. Serums were collected and stored in a refrigerator at a temperature of below – 80°C until the tests were done.
Serological and Molecular Analysis
The serum samples were assayed for HBV using the standard procedure for Wantai AiDTM HBsAg ELISA test kits (Beijing Wantai Biological Pharmacy Enterprise Co., Ltd. China Laboratory Diagnosis). Reactive samples were retested in duplicate and considered to be reactive if at least one of the two repetitions also gave a positive result. The result was interpreted as positive or negative on the basis of the manufacturer’s recommended cut-off values using the mean absorbance of the positive and negative control values (cut-off value = negative control + 0.06).
The anti-HBc screening test was also performed by using BIORAD kits (Monolisa Anti-HBc PLUS, BIORAD, France) with 99.9% specificity and 99.5% sensitivity. For Anti-HBc reactive samples DNA extraction, amplification, and detection were conducted from 200 μL plasma using the ABBOTT m2000sp and m2000rt an automated sample preparation ABBOTT Real-Time PCR system designed to use magnetic micro-particle-based reagents for the purification of nucleic acids from samples (Abbott Laboratories, Abbott Park, IL, USA) with the lower quantification limit or sensitivity of 15 IU/mL for the 0.2 mL serum sample volume following the manufacturer’s instructions. An internal control DNA was introduced into the sample preparation method and managed along with the calibrators, controls, and samples. The presence of the amplified HBV DNA and internal control was detected through the extension and annealing step. The amplification cycle at which a standardized fluorescent signal identified by the Abbott m2000rt was inversely proportional to the log of the HBV DNA concentration present in the original sample. Each sample was then quantitated by an external calibration curve. To check for consistency, 10% of the samples were re-tested.
Result Calculation
The concentration of HBV DNA in a sample and control was measured from either a stored calibration curve or a curve formed by calibrators in a calibration or sample run. The Abbott m2000rt tool spontaneously reports the results on its workstation. Assay results were reported in IU/mL which is proportional with an average conversion factor of 3.41 (1 IU = 3.41 copies).
Quality Assurance
Samples were stored at –80°C until processed. The Manufacturer’s instructions and standard operating procedures were firmly followed during laboratory tests. ELISA test results were determined based on the manufacturer’s cut-off value instruction. Internal control kits with HBV negative, HBV low positive, and HBV high positive were used with each run to check the quality of reagents according to the manufacturer’s instructions.
Ethics Approval and Consent to Participate
Ethical permission was obtained from the ethical review board of the Aklilu Lemma Institute of Pathobiology, Addis Ababa University (Reference Number ALIPB IRB/002/2011/2018). Written permission letters were submitted to all the concerned administrative offices. Informed consent was attained from each participant who participated in the study after an explanation of the aim, the potential risks, and the importance of the study. The consent for participants’ age less than 18 years was obtained from their parents or legal guardians. The participants were assured that they had full right to take part or not to take part in the study. To maintain privacy, participants’ information was coded and all personal identifiers were removed. All methods were carried out in accordance with the Declaration of Helsinki and the national research ethics review guideline of Ethiopia.
Results
Socio-Demographic Characteristics of the Study Participants
In this study, a total of 346 (60.1% females, age 6–82 years, mean age ± SD = 31.74 ± 9.32 years) study participants were enrolled. Among the study participants, 139 (40.2%) were from Hadiya, 122 (35.3%) from Kambata, and the remaining 85 (24.5%) were from Silte districts. Majority of the study participants, 250 (72.3) were rural residents, and more than half (58.4%) of the participants were married (Table 1).
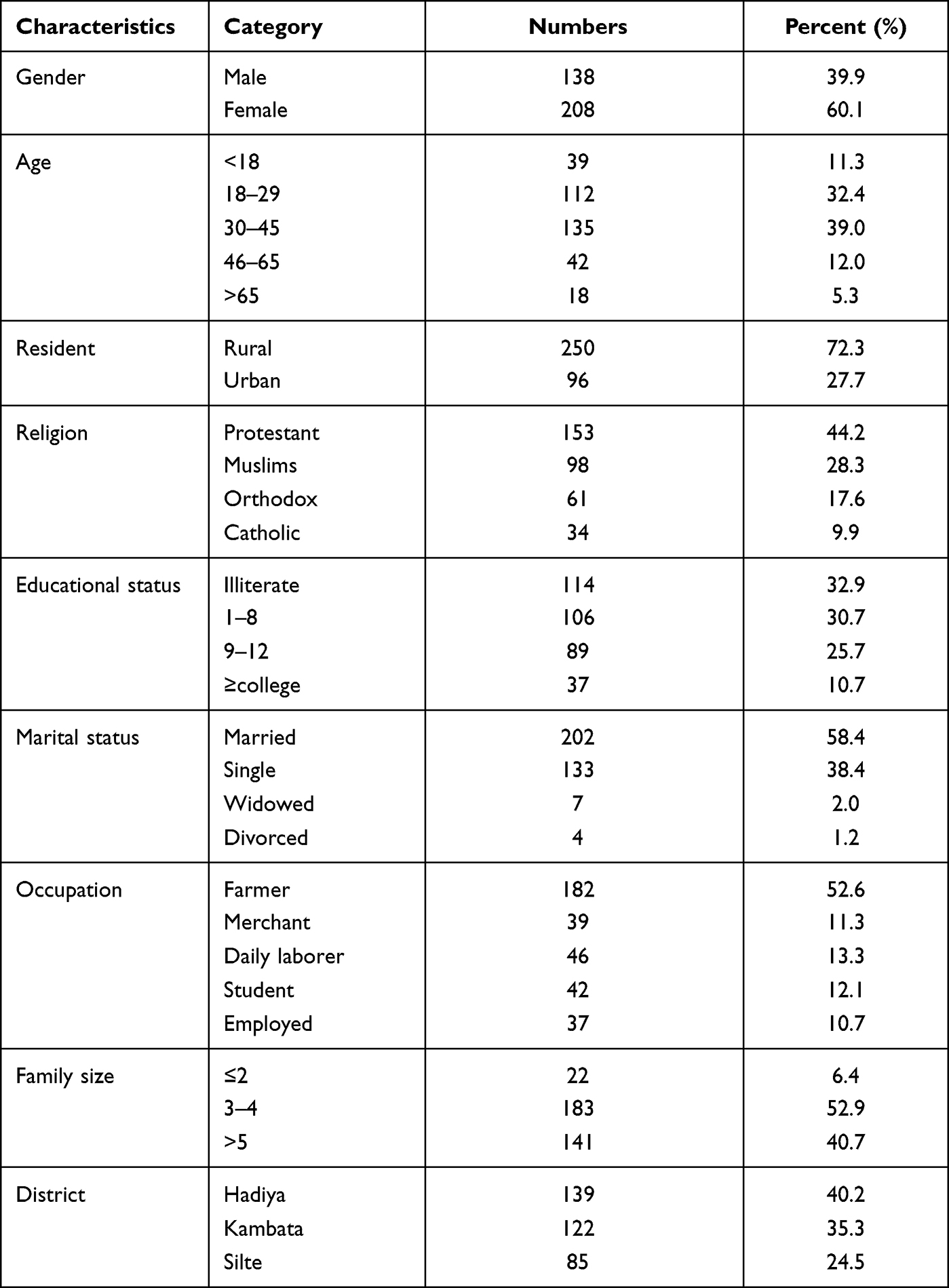 |
Table 1 Socio-Demographic Characteristics of the Study Participants, Southern Ethiopia |
The Distribution of Anti-HBc and HBV DNA in HBsAg Negative Study Participants
In this study, a total of 346 individuals were included, of which 34/346 (9.8%) were sero-positives and the rest 312 (90.2%) were sero-negatives by using the HBsAg ELISA test. From the total of 312 HBsAg sero-negative individuals, 115 (36.9%) were anti-HBc positive by using the anti-HBc ELISA test. Among 115 anti-HBc positive individuals’ samples, HBV DNA detection was observed in 21 (18.3%) samples or 6.1% among total population samples (Table 2). The HBV DNA concentration observed below 200 IU/mL among the OBI was 18/21 (85.7%). In three individuals, 3/21 (14.3%) of the observed HBV DNA concentration was above 200 IU/mL. The mean HBV DNA load in viremic anti-HBc positive individuals was 102.42 IU/mL (SD ± 58.29).
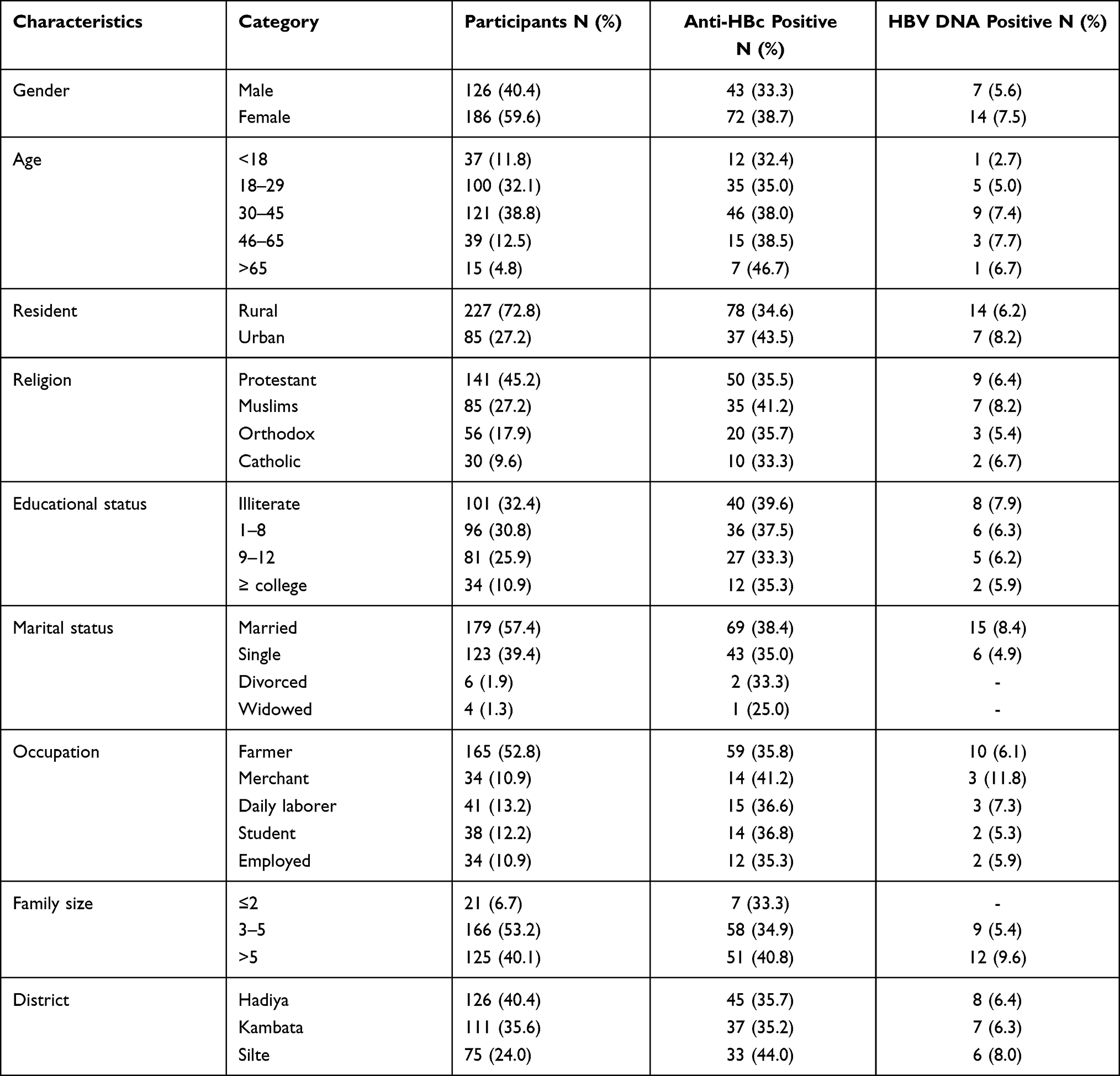 |
Table 2 The Distribution of Anti-HBc and HBV DNA in Study Participants (N = 312), Southern Ethiopia |
The Distribution of Anti-HBc and HBV DNA in Relation to Behavioral and Health-Characteristics
In this study, a high rate of OBI was observed with some risk factors characteristics of the study participants. Among participants with a family history of hepatitis infection (n = 6), individuals having multiple sexual contacts (n = 6), alcohol consumption (n = 7), history of hospital admission (n = 4), and tattooing or piercing (n = 10) the magnitude of OBI was 13.6%, 12.8%, 12.1%, 11.1%, and 10.4%, respectively. Whereas, the magnitude of contact for HBV by the distribution of anti-HBc was 53.1%, 52.8%, 51.1%, and 47.7% among participants with risk characteristics of tattooing or piercing, history of hospital admission, multiple sexual contacts, and family history of hepatitis infection, respectively (Table 3).
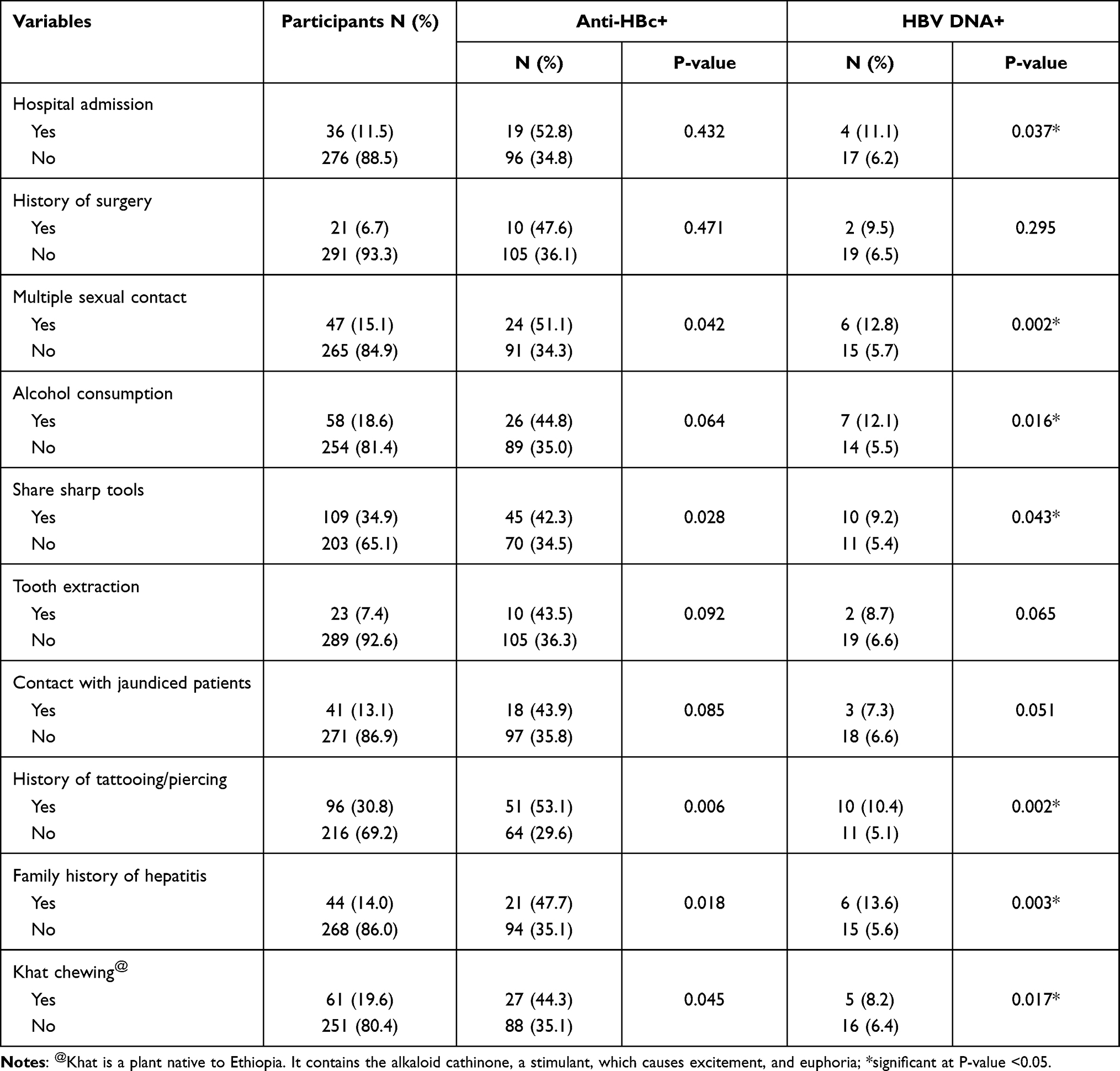 |
Table 3 The Distribution of Anti-HBc and HBV DNA in Relation to Behavioral and Health-Characteristics of Study Participants, Southern Ethiopia |
Factors Associated with OBI
Potential risk factors associated with OBI prevalence in the study district were analyzed. Multivariable analysis was used to control the possible confounders. In this regard, those individuals who had a family history of hepatitis were 7.6 times more likely associated with OBI compared to their counterparts (AOR = 7.6; 95% CI: 14.52, 22.84). Individuals who had multiple sexual contacts, history of tattooing or piercing, and sharing of sharp tools were 5.8, 4.3, and 2.4 times more likely associated with OBI (AOR = 5.8; 95% CI: 3.72, 8.45), (AOR = 4.3; 95% CI: 4.31, 17.34), (AOR = 2.4; 95% CI: 3.92, 9.48) compared to their counterparts, respectively (Table 4).
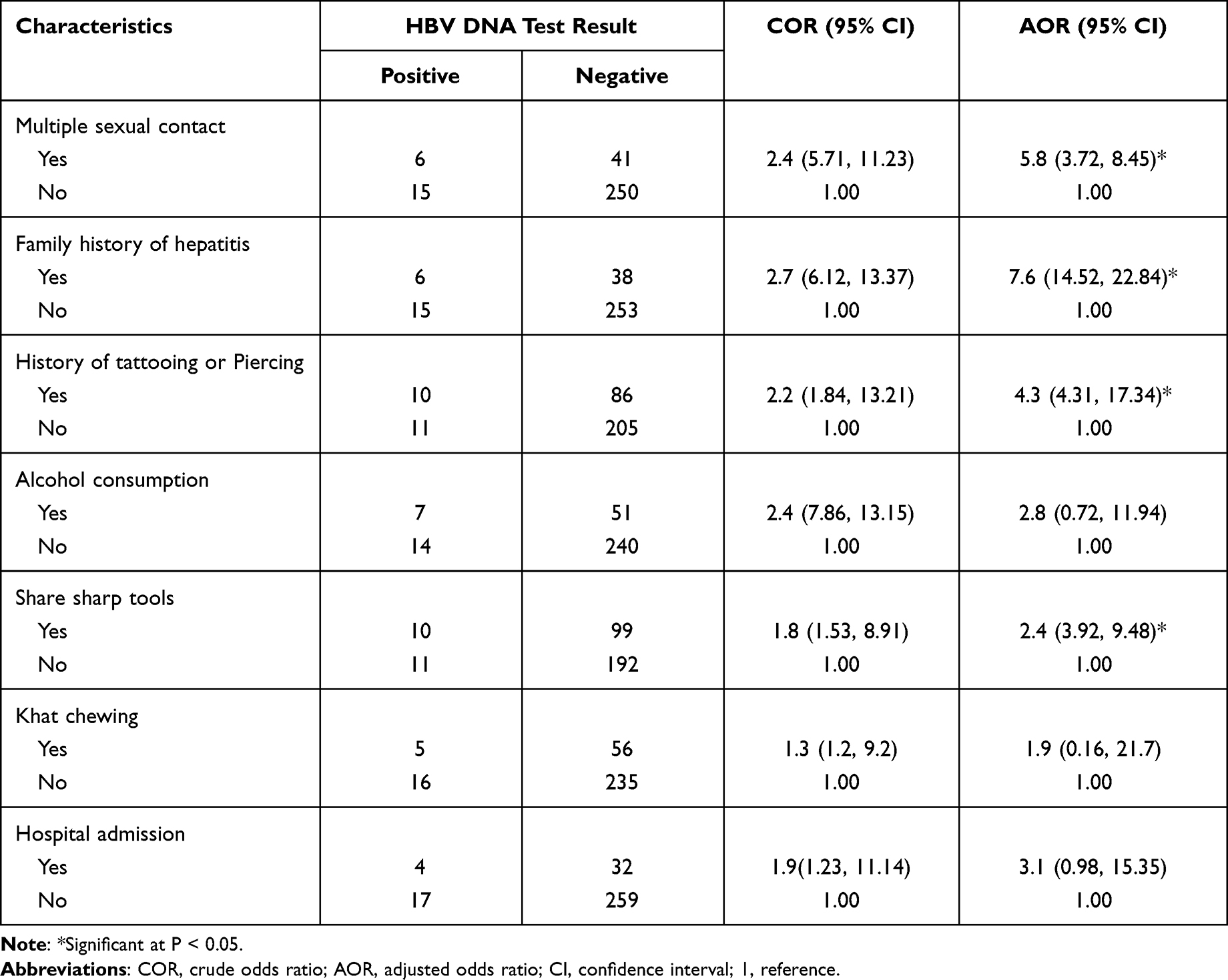 |
Table 4 The Distribution OBI Among Study Participants in Relation to Different Risk Factors Characteristics |
Discussion
HBV virus is prevalent in most African countries; including Ethiopia. In this study, the serological analyses revealed a high prevalence of HBV infection nearly one in ten individuals (9.52%) were positive with HBsAg. This makes the study area a high endemic setting for HBV infection according to WHO criteria (≥8.0%).37,38 Thus, this observed seroprevalence of HBsAg is higher than previous studies like the national pooled prevalence of 7.4% and subgroup meta-analysis prevalence of 8.0% in community-based studies in Ethiopia,36 and other East-African countries including 6.9% in Madagascar,39 2.1% in Kenya,40 and 6.1% in the whole African region, and 3.5% worldwide among the general population.41 Hence, this variation in a relative increase in the prevalence of HBsAg in the district as compared to the other areas suggests the current study area is one of the focus areas for the prevention and control of HBV in Ethiopia.
The prevalence of OBI varies to a great amount in different countries, depending on a number of reasons that comprise HBV endemicity, liver disease, HBV screening method,12,13 and primers used for NAT.14 This study revealed the overall OBI prevalence among previously tested HBsAg negative and anti-HBc positive apparently healthy individuals was found to be 18.3% (21/115). The data on OBI prevalence are limited in Ethiopia and sub-Saharan Africa. This study reported the prevalence of OBI among the general population in Ethiopia for the first time. Even though the data on OBI prevalence are limited, there are studies conducted shown in Easter region, Harar 6.4%42 and Northern region, Gondar 19.1%43 in HIV positive individuals, and 20.3%44 among antenatal care women in Ethiopia and other developing countries; 10% in Ivory 48Coast,45 16.48% in Sudan46 among blood donors, 18.7% in Kenya,47 8% in Nigeria,48 and 6.9% in Cameroon.49 Our study reported slightly a comparable burden of OBI to some of these reports from Ethiopia and other neighboring East African countries, Kenya and Sudan through the variations in the other studies. This variation may depend on a number of factors that possibly because of the actual differences in study design, study population, HBV endemicity, variation in occupation, geographical differences, and HIV endemicity. As it was identified, OBI has been reported to be more common in HIV-positive individuals50 and hence a known risk factor for the development of OBI24 due to down-regulation of HBsAg synthesis and surface antigen mutation.51 Moreover, the prescreening procedures and primers employed for NAT may also play a role in the observed variations.
HBsAg negative individuals with serum HBV DNA level below 200 IU/mL are considered true OBI,14 and individuals with serum HBV DNA level similar to HBsAg positive or overt infection, but are, on the other hand, HBsAg-negative, have been termed false OBI.3 This is commonly due to unusual S gene escape mutant’s infection, which produces an altered HBsAg that is not recognized by routinely used detection assays.15 In this study, we observed 18/21 (85.7%) OBI cases had HBV DNA count below 200 IU/mL. This indicates true OBI; even though, the true rate in a population may vary because some individuals can demonstrate intermittent HBV DNA positivity which may not be detected in a cross-sectional study.14,52
This study reported a total of 312 (90.2%) individuals were HBsAg sero-negatives and 115 (36.9%) were anti-HBc positive of these HBsAg sero-negatives. Among 115 anti-HBc positive samples, HBV DNA detection was observed in 21/115 (18.3%). Studies suggest optionally in the lack of very sensitive HBV DNA testing, the use of anti-HBc as a possible surrogate marker for detecting possible seropositive OBI in cases of blood and organ donation.42,52,53 This could be considered as one of the strategies to reduce transmission risk among recipients. Furthermore, anti-HBc screening may be a valuable procedure to find individuals earlier exposed to HBV and potentially bearing significant risk for HBV reactivation due to immunosuppression.42,53 In many countries, using HBsAg and anti-HBc has been the basis of screening tests for HBV,14,52 and this has significantly reduced but did not exclude transfusion-associated HBV infection.54 However, in developing countries like Ethiopia, where the prevalence of anti-HBc antibodies is high, screening leads to the rejection of more than a third of the donated blood and may not be applicable for blood and organ donor selection. Furthermore, not all anti-HBc positive individual samples are HBV DNA detectable, and anti-HBc antibody absence also does not exclude seronegative OBI.42
OBI can be seronegative or serologically negative for all markers, which accounts for approximately 20% of all OBI cases, and 80% seropositive (36% anti-HBs and 44% anti-HBc positive).55 Our study also revealed a high rate of HBV-DNA (18.3%) positivity among anti-HBc positive individuals, which is slightly comparable with previous studies elsewhere 10% to 80%.3,56 In our study, the number of HBV DNA positive cases looks high, and the findings have public health importance because of the possibility of post-transfusion or transplantation HBV infection in recipients of blood and organs from HBsAg alone negative donors.4 In Ethiopia, where HBsAg is the only screening test,57 in women within reproductive age with OBI the chance of vertical transmission should not be ignored during childbirth.
This study revealed a higher rate of OBI in larger family sizes than in small family sizes. Different studies have shown and suggested similar findings compared with the present study.28,37 Hence, this higher rate of OBI in larger family sizes could explain the presence of horizontal transmission of HBV infection within the family. In a large family, there might be increased close contact of family members that could create an increased chance of HBV transmission in the family environment. This study likewise showed the high rate of OBI infection in less-educated individuals which is somewhat similar to other studies conducted in Ethiopia43,44 and elsewhere.24 This relatively higher HBV seropositivity among the less educated might be attributed to poor awareness regarding mode of transmission and increased educational level might increase the awareness level for prevention practice for HBV infection by the community. It was also reported a higher rate of OBI among individuals having alcohol than their counterparts. Ethiopian studies indicated an association between drinking alcohol with unsafe sex more likely to have multiple sexual partners, which may predispose to infection with viral hepatitis.58,59
In this study, there are study participants who had a family history of hepatitis, practiced multiple sexual contacts, had a history of body tattooing, and sharing of sharp tools. In multivariable analysis, these variables are also associated with OBI. In this regard, those individuals who had a family history of hepatitis were 7.6 times more likely associated with OBI compared to their counterparts, and individuals who had the exposure of having multiple sex partners, history of body tattooing, and sharing of sharp tools were 5.8, 4.3 and 2.4 times more likely associated with OBI (p < 0.05) compared to their counterparts, respectively. They were found to be independent risk factors and supported by other studies conducted in Ethiopia,60,61 and other African countries.62–65 This indicates that the main way of transmission for HBV is cross-contamination of body fluids during body contact; hence, this could explain possibly the presence of close contact or sexual contact with hepatitis patients increase the chance of HBV transmission.
Limitations
This study assessed only serological detection of HBV DNA in the peripheral blood of HBsAg negative individuals for OBI due to resource limitations. Hence, HBV DNA amplification from peripheral blood may not be effectively sensitive as HBV latency within liver cells produces only sporadic HBV DNA in blood. This may underestimate the OBI cases and affected the true prevalence of OBI. Additionally, the lack of HBV genotypic sequenced data from occult infections may limit the information generated in terms of genetic variability.
Conclusions and Recommendations
In this study, we investigated the high prevalence of OBI among the healthy general population of Southern Ethiopia. This indicates the burden of OBI has a significant public health implication due to the possibility of HBV transmission through blood and blood products transfusion, organ transplantation, and vertical transmission since screening is exclusively reliant on HBsAg testing. Our results strongly justify that a complementary sensitive NAT by PCR for detecting HBV DNA remains a prerequisite to ensure the safety of blood transfusion need, organ recipients and for the avoidance of HBV vertical transmission risks in HBV endemic areas.
Data Sharing Statement
The data analyzed during this study are accessible from the corresponding author on a reasonable request.
Acknowledgments
The authors would like to express gratitude to the Office of Graduate Studies and Aklilu Lemma Institute of Pathobiology, Addis Ababa University, for sponsoring the study. We are also highly indebted to the administrative offices, participants who give pertinent information and blood sample. Our special thanks also go to the Southern Regional Blood Bank of Hossana District and Armauer Hansen Research Institute for their laboratory kits support, allowing facilities to perform procedures and storing the samples.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
Funding for this study was made possible through grants obtained by Addis Ababa University. The funder had no part in the conceptualization and designing of the study, data processing, and decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no known conflicts of interest.
References
1. Hollinger FB, Sood G. Occult hepatitis B virus infection: a covert operation. J Viral Hepat. 2010;17(1):1–5. doi:10.1111/j.1365-2893.2009.01245.x
2. Prati D, Gerosa A, Porretti L. Occult HBV infection and blood transfusion. J Hepatol. 2006;44(4):818. doi:10.1016/j.jhep.2005.12.009
3. Bréchot C, Thiers V, Kremsdorf D, Nalpas B, Pol S, Paterlini‐Bréchot P. Persistent hepatitis B virus infection in subjects without hepatitis B surface antigen: clinically significant or purely “occult”? Hepatology. 2001;34(1):194–203. doi:10.1053/jhep.2001.25172
4. Allain JP, Candotti D. Diagnostic algorithm for HBV safe transfusion. Blood Transfus. 2009;7(3):174. doi:10.2450/2008.0062-08
5. Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology. 2007;45(2):507–539. doi:10.1002/hep.21513
6. Ganem D, Prince AM. Hepatitis B virus infection-natural history and clinical consequences. N Engl J Med. 2004;350(11):1118–1129. doi:10.1056/NEJMra031087
7. Hadziyannis SJ, Vassilopoulos D. Hepatitis B e antigen-negative chronic hepatitis B. Hepatology. 2001;34(4):617–624. doi:10.1053/jhep.2001.27834
8. Weber B, Melchior W, Gehrke R, Doerr HW, Berger A, Rabenau H. Hepatitis B virus markers in anti‐HBc only positive individuals. J Med Virol. 2001;64(3):312–319. doi:10.1002/jmv.1052
9. Grob P, Jilg W, Bornhak H, et al. Serological pattern “anti‐HBc alone”: report on a workshop. J Med Virol. 2000;62(4):450–455. doi:10.1002/1096-9071(200012)62:4<450::AID-JMV9>3.0.CO;2-Y
10. Gerlich WH. Medical virology of hepatitis B: how it began and where we are now. Virol J. 2013;10(1):1–25. doi:10.1186/1743-422X-10-239
11. Bengsch B, Chang KM. Evolution in our understanding of hepatitis B virus virology and immunology. Clin Liver Dis. 2016;20(4):629–644. doi:10.1016/j.cld.2016.06.001
12. Pollicino T, Raimondo G. Occult hepatitis B infection. J Hepatol. 2014;61(3):688–689. doi:10.1016/j.jhep.2014.04.036
13. Kang SY, Kim MH, Lee WI. The prevalence of “anti‐HBc alone” and HBV DNA detection among anti‐HBc alone in Korea. J Med Virol. 2010;82(9):1508–1514. doi:10.1002/jmv.21862
14. Said ZN. An overview of occult hepatitis B virus infection. World J Gastroenterol. 2011;17(15):1927. doi:10.3748/wjg.v17.i15.1927
15. Raffa G, Maimone S, Cargnel A, et al. Analysis of occult hepatitis B virus infection in liver tissue of HIV patients with chronic hepatitis. C. Aids. 2007;21(16):2171–2175. doi:10.1097/QAD.0b013e3282eea504
16. Raimondo G, Pollicino T, Cacciola I, Squadrito G. Occult hepatitis B virus infection. J Hepatol. 2007;46(1):160–170. doi:10.1016/j.jhep.2006.10.007
17. Hu KQ. Occult hepatitis B virus infection and its clinical implications. J Viral Hepat. 2002;9(4):243–257. doi:10.1046/j.1365-2893.2002.00344.x
18. El Chaar M, Candotti D, Crowther RA, Allain JP. Impact of hepatitis B virus surface protein mutations on the diagnosis of occult hepatitis B virus infection. Hepatology. 2010;52(5):1600–1610. doi:10.1002/hep.23886
19. Kim SM, Lee KS, Park CJ, et al. Prevalence of occult HBV infection among subjects with normal serum ALT levels in Korea. J Infect. 2007;54(2):185–191. doi:10.1016/j.jinf.2006.02.002
20. Nishikawa H, Osaki Y. Clinical significance of occult hepatitis B infection in progression of liver disease and carcinogenesis. J Cancer. 2013;4(6):473. doi:10.7150/jca.6609
21. Coppola N, Onorato L, Pisaturo M, et al. Role of occult hepatitis B virus infection in chronic hepatitis C. World J Gastroenterol. 2015;21(42):11931. doi:10.3748/wjg.v21.i42.11931
22. Castillo I, Rodríguez‐Iñigo E, López‐Alcorocho JM, Bartolomé J, Pardo M, Carreño V. Comparative study on the clinical and virological characteristics among patients with single occult hepatitis B virus (HBV), single occult hepatitis C virus (HCV) and occult HBV and HCV dual infection. J Med Virol. 2007;79(3):236–241. doi:10.1002/jmv.20784
23. Re III VL, Frank I, Gross R, et al. Prevalence, risk factors, and outcomes for occult hepatitis B virus infection among HIV-infected patients. JAIDS. 2007;44(3):315–320. doi:10.1097/QAI.0b013e31802ea499
24. Mphahlele MJ, Lukhwareni A, Burnett RJ, Moropeng LM, Ngobeni JM. High risk of occult hepatitis B virus infection in HIV-positive patients from South Africa. J Clin Virol. 2006;35(1):14–20. doi:10.1016/j.jcv.2005.04.003
25. Dickens C, Kew MC, Purcell RH, Kramvis A. Occult hepatitis B virus infection in chacma baboons, South Africa. Emerg Infect Dis. 2013;19(4):598. doi:10.3201/eid1904.121107
26. Seeger C, Mason WS. Molecular biology of hepatitis B virus infection. Virology. 2015;479:672–686. doi:10.1016/j.virol.2015.02.031
27. Yan YP, Su HX, Ji ZH, Shao ZJ, Pu ZS. Epidemiology of hepatitis B virus infection in China: current status and challenges. J Clin Transl Hepatol. 2014;2(1):15. doi:10.14218/JCTH.2013.00030
28. Oluyinka OO, Tong HV, Bui Tien S, et al. Occult hepatitis B virus infection in Nigerian blood donors and hepatitis B virus transmission risks. PLoS One. 2015;10(7):e0131912. doi:10.1371/journal.pone.0131912
29. Hollinger FB. Hepatitis B virus infection and transfusion medicine: science and the occult. Transfusion. 2008;48(5):1001–1026. doi:10.1111/j.1537-2995.2008.01701.x
30. Coppola N, Sagnelli C, Pisaturo M, et al. Clinical and virological characteristics associated with severe acute hepatitis B. Clin Microbiol Infect. 2014;20(12):O991–7. doi:10.1111/1469-0691.12720
31. Tsubota A, Kumada H, Takaki K, et al. Deletions in the hepatitis B virus core gene may influence the clinical outcome in hepatitis B e antigen-positive asymptomatic healthy carriers. J Med Virol. 1998;56(4):287–293. doi:10.1002/(SICI)1096-9071(199812)56:4<287::AID-JMV1>3.0.CO;2-P
32. Shastry S, Bhat SS. Prevention of post-transfusion hepatitis by screening of antibody to hepatitis B core antigen in healthy blood donors. Mediterr J Hematol Infect Dis. 2011;3(1):e2011062. doi:10.4084/mjhid.2011.062
33. Allain JP, Mihaljevic I, Gonzalez‐Fraile MI, et al. Infectivity of blood products from donors with occult hepatitis B virus infection. Transfusion J. 2013;53(7):1405–1415. doi:10.1111/trf.12096
34. Squadrito G, Cacciola I, Alibrandi A, Pollicino T, Raimondo G. Impact of occult hepatitis B virus infection on the outcome of chronic hepatitis C. J Hepatol. 2013;59(4):696–700. doi:10.1016/j.jhep.2013.05.043
35. Lall S, Choudhary MC, Mahajan S, Kumar G, Gupta E. Performance evaluation of TRUPCR® HBV Real-time PCR assay for Hepatitis B virus DNA quantification in clinical samples: report from a tertiary care liver centre. Virusdisease. 2019;30(2):186–192. doi:10.1007/s13337-018-0502-0
36. Belyhun Y, Maier M, Mulu A, Diro E, Liebert UG. Hepatitis viruses in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2016;16(1):1–4. doi:10.1186/s12879-016-2090-1
37. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat. 2004;11(2):97–107. doi:10.1046/j.1365-2893.2003.00487.x
38. Spearman CW, Afihene M, Ally R, et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. Lancet Gastroenterol Hepatol. 2017;2(12):900–909. doi:10.1016/S2468-1253(17)30295-9
39. Al-Sadi AM, Al-Oweisi FA, Edwards SG, Al-Nadabi H, Al-Fahdi AM. Genetic analysis reveals diversity and genetic relationship among Trichoderma isolates from potting media, cultivated soil and uncultivated soil. BMC Microbiol. 2015;15(1):1. doi:10.1186/s12866-015-0483-8
40. Ochwoto M, Kimotho JH, Oyugi J, et al. Hepatitis B infection is highly prevalent among patients presenting with jaundice in Kenya. BMC Infect Dis. 2016;16(1):1–4. doi:10.1186/s12879-016-1409-2
41. Talla C, Itanyi IU, Tsuyuki K, et al. Hepatitis B infection and risk factors among pregnant women and their male partners in the Baby Shower Programme in Nigeria: a cross‐sectional study. Trop Med Int Health. 2021;26(3):316–326. doi:10.1111/tmi.13531
42. Ayana DA, Mulu A, Mihret A, Seyoum B, Aseffa A, Howe R. Occult Hepatitis B virus infection among HIV negative and positive isolated anti-HBc individuals in eastern Ethiopia. Sci Rep. 2020;10(1):1–9. doi:10.1038/s41598-020-79392-x
43. Patel NH, Meier-Stephenson V, Genetu M, et al. Prevalence and genetic variability of occult hepatitis B virus in a human immunodeficiency virus positive patient cohort in Gondar, Ethiopia. PLoS One. 2020;15(11):e0242577. doi:10.1371/journal.pone.0242577
44. Meier-Stephenson V, Deressa T, Genetu M, et al. Prevalence and molecular characterization of occult hepatitis B virus in pregnant women from Gondar, Ethiopia. Can Liver J. 2020;3(4):323–333. doi:10.3138/canlivj-2019-0031
45. N’Dri-Yoman T, Anglaret X, Messou E, et al. Short communication Occult HBV infection in untreated HIV-infected adults in Côte d’Ivoire. Antivir Ther. 2010;15:1029–1034. doi:10.3851/IMP1641
46. Mudawi H, Hussein W, Mukhtar M, et al. Overt and occult hepatitis B virus infection in adult Sudanese HIV patients. Int J Infect Dis. 2014;29:65–70. doi:10.1016/j.ijid.2014.07.004
47. Jepkemei KB, Ochwoto M, Swidinsky K, et al. Characterization of occult hepatitis B in high-risk populations in Kenya. PLoS One. 2020;15(5):e0233727. doi:10.1371/journal.pone.0233727
48. Nna E, Mbamalu C, Ekejindu I. Occult hepatitis B viral infection among blood donors in South–Eastern Nigeria. Pathog Glob Health. 2014;108(5):223–228. doi:10.1179/2047773214Y.0000000144
49. Salpini R, Fokam J, Ceccarelli L, et al. High burden of HBV-infection and atypical HBV strains among HIV-infected Cameroonians. Curr HIV Res. 2016;14(2):165–171. doi:10.2174/1570162X13666150930114742
50. Firnhaber C, Chen CY, Evans D, et al. Prevalence of hepatitis B virus (HBV) co-infection in HBV serologically-negative South African HIV patients and retrospective evaluation of the clinical course of mono-and co-infection. Int J Infect Dis. 2012;16(4):e268–72. doi:10.1016/j.ijid.2011.12.007
51. El-Zaatari M, Kazma H, Naboulsi-Majzoub M, et al. Hepatitis B virus DNA in serum of ‘anti-HBc only’-positive healthy Lebanese blood donors: significance and possible implications. J Hosp Infect. 2007;66(3):278–282. doi:10.1016/j.jhin.2007.04.010
52. Filippini P, Coppola N, Pisapia R, et al. Impact of occult hepatitis B virus infection in HIV patients naive for antiretroviral therapy. Aids. 2006;20(9):1253–1260. doi:10.1097/01.aids.0000232232.41877.2a
53. Urbani S, Fagnoni F, Missale G, Franchini M. The role of anti-core antibody response in the detection of occult hepatitis B virus infection. Clin Chem Labor Med. 2010;48(1):23–29. doi:10.1515/CCLM.2010.002
54. Mühlbacher A, Zdunek D, Melchior W, Michl U. Is infective blood donation missed without screening for antibody to hepatitis B core antigen and/or hepatitis B virus DNA? Vox Sang. 2001;81(2):139. doi:10.1046/j.1423-0410.2001.00086.x
55. Torbenson M, Thomas DL. Occult hepatitis B. Lancet Infect Dis. 2002;2(8):479–486. doi:10.1016/S1473-3099(02)00345-6
56. Sagnelli E, Stroffolini T, Mele A, Imparato M, Almasio PL. New features of an old disease-approaching the universal prevalence of hepatitis B e antigen-negative cases and the eradication of hepatitis D infection. Clin Infect Dis. 2008;46(1):110–113. doi:10.1086/524074
57. Ayana DA, Mulu A, Mihret A, Seyoum B, Aseffa A, Howe R. Hepatitis B virus seromarkers among HIV infected adults on ART: an unmet need for HBV screening in eastern Ethiopia. PLoS One. 2019;14(12):e0226922. doi:10.1371/journal.pone.0226922
58. Abebe D, Debella A, Dejene A, et al. Khat chewing habit as a possible risk behaviour for HIV infection: a case-control study. Ethiop J Health Dev. 2005;19(3):174–181.
59. Soboka M, Tesfaye M, Feyissa GT, Hanlon C. Khat use in people living with HIV: a facility-based cross-sectional survey from South West Ethiopia. BMC Psychiatr. 2015;15(1):1–7. doi:10.1186/s12888-015-0446-5
60. Tilahun M, Ayele G. Factors associated with Khat use among youths visiting HIV testing and counseling centers in Gamo Gofa, Southern Ethiopia. BMC Public Health. 2013;13(1):1–6. doi:10.1186/1471-2458-13-1199
61. Berhanu D, Diener-West M, Ruff A, Davis WW, Celentano DD, Go VF. Associations between Khat use and HIV risk and status among voluntary counseling and testing center clients in Addis Ababa, Ethiopia. J Addict Med. 2017;11(4):320. doi:10.1097/ADM.0000000000000304
62. Nwadigwe CE. ‘I want to be a star’: doping technology and the incidence of performance-enhancing drugs among actors in Nigeria. Afri Sociol Rev. 2008;12(2):144–154.
63. Chama D, Ahmed Y, Baboo KS, Halwindi H, Mulenga J. Transfusion transmissible infections among voluntary blood donors at the university teaching hospital, Lusaka, Zambia. Med J Zambia. 2015;42(3):90–95.
64. Fasola FA, Fadimu PA, Akpan VO. A seven year review of the Seroprevalence of transfusion transmitted infections in a hospital based blood bank in Ibadan, Nigeria. Clin Med Res. 2017;6(1):1–8. doi:10.11648/j.cmr.20170601.11
65. Loua A, Diallo MB, Magassouba FB, Camara M, Bah MA, Cisse A. Seroprevalence of hepatitis B in blood donors in Guinea. Medecine Tropicale. 2005;65(4):396–397.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.