")
Back to Journals » International Journal of Women's Health » Volume 12
Obstetric Outcomes of Pregnancy After Uterine Artery Embolization
Authors Jitsumori M, Matsuzaki S , Endo M, Hara T, Tomimatsu T, Matsuzaki S, Miyake T , Takiuchi T , Kakigano A, Mimura K , Kobayashi E, Ueda Y, Kimura T
Received 29 October 2019
Accepted for publication 20 February 2020
Published 6 March 2020 Volume 2020:12 Pages 151—158
DOI https://doi.org/10.2147/IJWH.S236443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Mariko Jitsumori,1,* Shinya Matsuzaki,1,* Masayuki Endo,1 Takeya Hara,1 Takuji Tomimatsu,1 Satoko Matsuzaki,2 Tatsuya Miyake,1 Tsuyoshi Takiuchi,1 Aiko Kakigano,1 Kazuya Mimura,1 Eiji Kobayashi,1 Yutaka Ueda,1 Tadashi Kimura1
1Department of Obstetrics and Gynecology, Osaka University Graduate School of Medicine, Osaka, Japan; 2Department of Obstetrics and Gynecology, Otemae Hospital, Osaka, Japan
*These authors contributed equally to this work
Correspondence: Shinya Matsuzaki; Aiko Kakigano
Department of Obstetrics and Gynecology, Osaka University Graduate School of Medicine, 2-2 Yamadaoka, Suita, Osaka 565-0871, Japan
Tel +81-6-6879-3355
Fax +81-6-6879-3359
Email [email protected]; [email protected]
Background: Uterine artery embolization (UAE) is used to treat severe postpartum hemorrhage (PPH). According to a few studies, UAE for PPH was associated with preterm birth, fetal growth restriction (FGR), and placenta accreta spectrum (PAS) in subsequent pregnancies. These previous studies, however, lacked controls, and to the best of our knowledge, no systematic literature reviews have been conducted thus far. We report the results of our retrospective case–control study of pregnancies after UAE at a single center and include a literature review to evaluate the risk of PAS in pregnancies after UAE.
Methods: We retrospectively reviewed data from deliveries at our hospital between January 2012 and October 2017. We divided the delivery data into cases with previous UAEs performed for PPH (the post-UAE group) and those without UAEs (the non-UAE group, which included women without previous PPH). We defined PAS as cases in which hysterectomy was performed and pathological examination confirmed the diagnosis. Results are presented as odds ratios (ORs) with 95% confidence intervals (95% CIs).
Results: We used data from 3155 patients in this study, of whom 16 patients had undergone UAE (post-UAE group) and 3139 had not (non-UAE group). We found no differences between the groups in terms of frequency of preterm births (12.5% versus 14.2%, respectively; OR, 0.863; 95% CI, 0.218 to 3.414; P = 0.84) or FGR (6.2% versus 10.0%, respectively; OR, 0.602; 95% CI, 0.104 to 3.584; P = 0.61). However, cases of PAS were significantly more common in the post-UAE group (37.5%) than in the non-UAE group (1.2%; OR, 50.303; 95% CI, 17.38 to 145.592; P < 0.01).
Conclusion: Our results suggest that previous UAE is a significant risk factor for PAS.
Keywords: placenta accreta, placenta accreta spectrum, uterine artery embolization, postpartum hemorrhage, obstetric outcomes
Background
Postpartum hemorrhage (PPH) occurs in 4% to 6% of deliveries, and 80% of cases are caused by atonic bleeding.1–3 Severe PPH is an obstetric emergency that occurs in 1% to 2% of live births and accounts for approximately 140,000 maternal deaths annually worldwide.4 Treatment strategies include pharmacological measures (eg, oxytocin administration), intrauterine tamponade (eg, Bakri balloon or Sengstaken–Blakemore tube), uterine artery ligation, hysterectomy, uterine compression sutures, and uterine artery embolization (UAE).5–12
A few publications have shown higher rates of preterm birth, fetal growth restriction (FGR), and placenta accreta spectrum (PAS) among women who became pregnant after UAE for PPH. However, these obstetric outcomes were not investigated with non-UAE cases in these studies.13,14 To the best of our knowledge, no studies have compared rates of PAS between patients who have undergone UAE and those who have not. Our aim was to determine the rates of preterm birth, FGR, PAS, and other obstetric adverse outcomes in subsequent pregnancies after UAEs for PPH.
Methods
We retrospectively reviewed the medical records of women who delivered at Osaka University Hospital, Osaka, Japan between January 2012 and October 2017. We divided these women into those who had previously undergone UAE for PPH (post-UAE group) and those who had not (non-UAE group).
We reviewed their medical records for perinatal outcomes, including gestational age at delivery, weight of infants, and blood loss at delivery. Our primary outcome was the rate of PAS. Our secondary outcomes included the rate of preterm births (delivery at <37 weeks of gestation) and rate of small for gestational age in infants (≤-1.5 standard deviations for birth weight). We excluded cases of abortion from our analysis.
We calculated the gestational age at delivery from the first day of the woman’s last menstrual period as previously described.15 If the gestational age estimated was inconsistent with that obtained from growth measurements estimated at the first ultrasound examination (within 5 days in the first trimester or within 14 days in the second trimester), we used the gestational age estimated from the ultrasound results. We defined PAS as cases in which hysterectomy had been performed and the diagnosis had been pathologically confirmed. Cases in which the diagnoses of PAS had not been histologically determined were defined as clinical PAS.
We performed a literature review to identify the possible risk factors for PAS in subsequent pregnancies following UAE procedures for PPH. We conducted an electronic search of the PubMed (https://www.ncbi.nlm.nih.gov/pubmed/) and Scopus (https://www.scopus.com) databases for literature from January 2002 to December 2017. We excluded articles written in languages other than in English and those published before 2002, with some modification of the method previously described.16–18 In addition, we excluded all articles related to UAE for uterine fibroids, cervical pregnancy, cesarean scar pregnancy, or uterine arteriovenous malformations. For our search, we used the following specific keywords for each database: “uterine artery embolization”, “subsequent pregnancy”, “uterine artery embolization” and “placenta accreta.”
The ethics committee of Osaka University approved the study (approval #18130, approved on August 1, 2018). The need for informed consent from patients was waived because of the retrospective nature of the study, whose design was based on computerized data with anonymous selection.
The effect of previous UAE on development of PAS was summarized using odds ratios (ORs) and 95% confidence intervals (95% CIs). We conducted our statistical analysis using the JMP Pro 13.0 software (SAS, Institute Inc., Cary, NC, USA). We used the Student’s t-test for continuous variables, χ2 test for categorical variables, and Fisher’s exact test for rare categorical variables. All p values <0.05 were considered statistically significant.
Results
We collected data from 3,155 deliveries that occurred during the study period. The post-UAE group included 16 cases and the non-UAE group included 3,139 cases. As shown in Table 1, groups did not differ significantly with regard to the maternal characteristics. Groups did, however, differ in the rate of previous cesarean deliveries (CD), rate of transfusion, and mean blood loss.
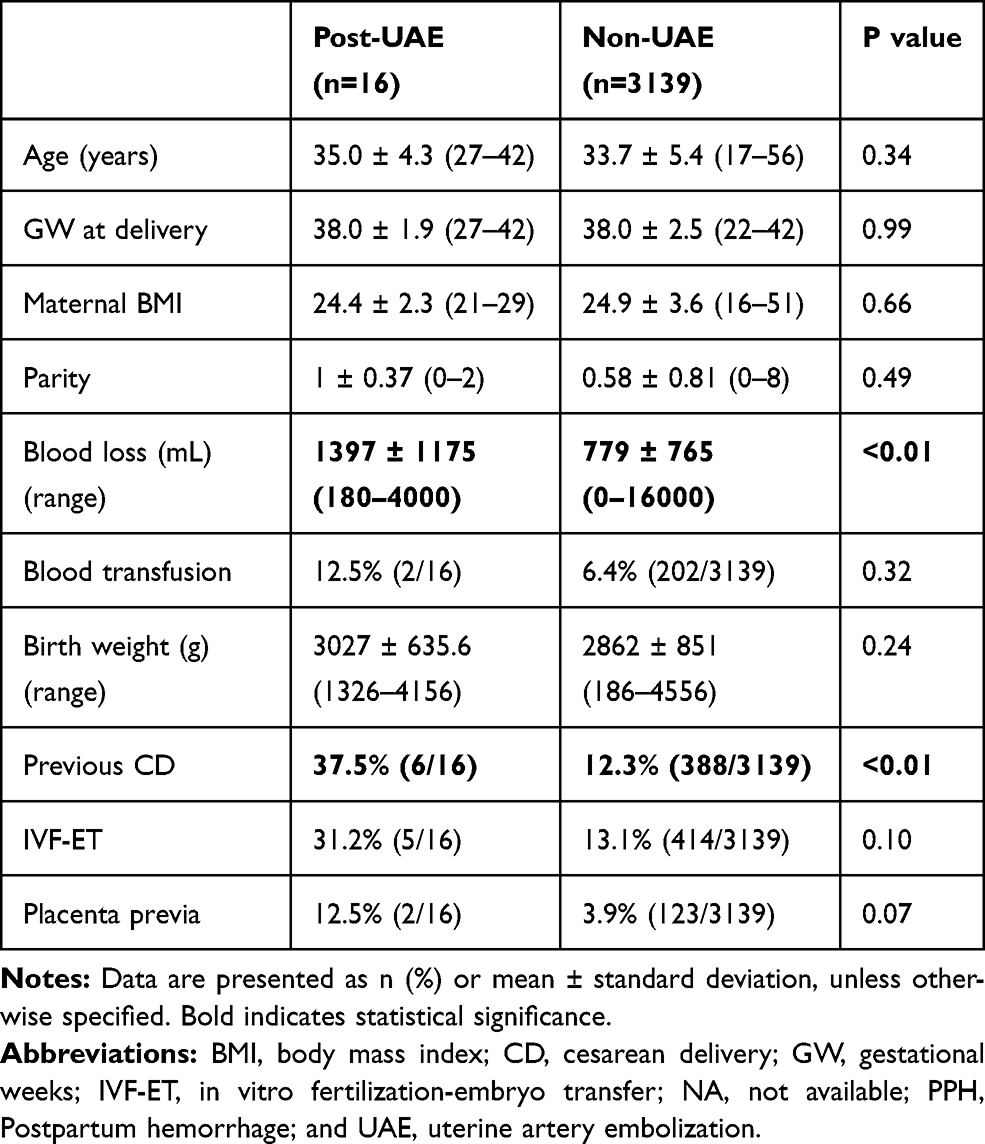 |
Table 1 Clinical Characteristics of the Post-UAE and Control Groups |
Approximately a third of patients in the post-UAE group (37.5%, 6/16) had a previous CD while 12.3% (388/3139) of patients in the non-UAE group had a previous CD (P < 0.01). The rate of transfusion was higher in the post-UAE group compared with the non-UAE group (12.5% vs 6.4%; P < 0.01). Mean total estimated blood loss was 1,397 mL (range, 180–4000 mL) in the post-UAE group and 779 mL (range, 0–16,000 mL) in the non-UAE group (P < 0.01). Detailed clinical information on the post-UAE group (n = 16) is shown in Table 2.
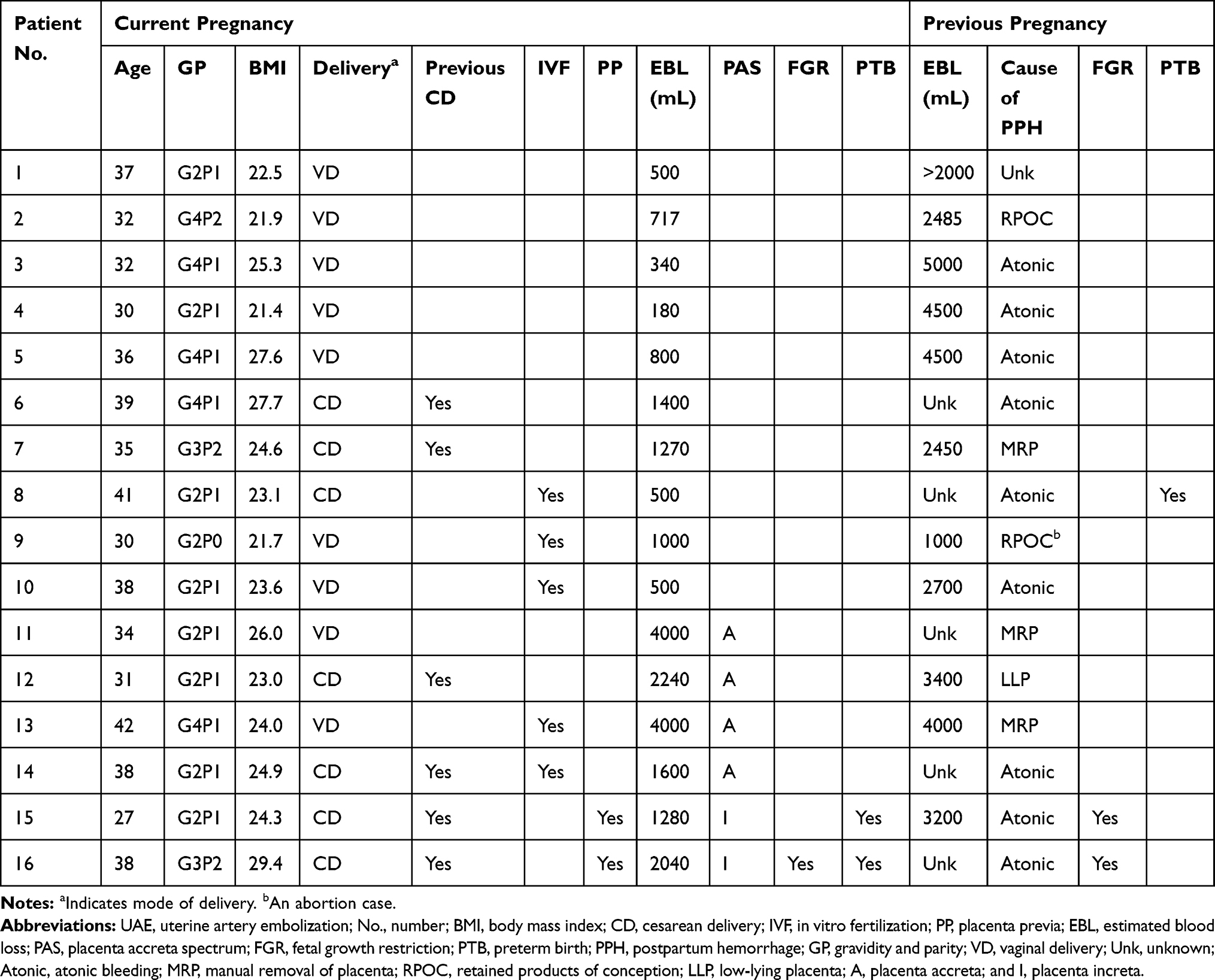 |
Table 2 Detailed Patient Information of the Post-UAE Group |
Table 3 presents the targeted obstetric outcomes of our study. PAS was significantly more common in the post-UAE group than in the non-UAE group (6/16 [37.5%] vs 1.2% [37/3139]; OR 50.303; 95% CI 17.38–145.59; P < 0.01). The other outcomes were not significantly different between the two groups. As placenta previa, previous CD, and IVF-ET are all major risk factors for PAS, we examined the risk of PAS while excluding patients with placenta previa, previous CD, and IVF-ET from both the post-UAE and non-UAE groups as shown in Figure 1 and Table 4. Various patterns were examined and all patterns, except those with placenta previa and previous CD but where IVF was excluded (P = 0.09), revealed a significantly higher rate of PAS in the post-UAE group than in the non-UAE group (all, P < 0.01).
 |
Table 3 Clinical Outcomes of Subsequent Pregnancies |
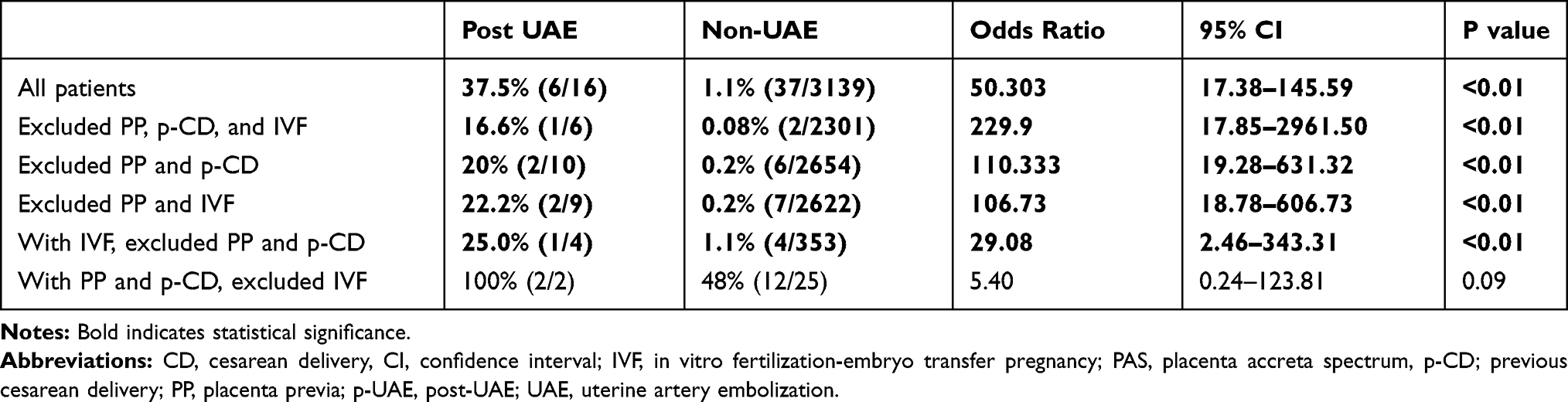 |
Table 4 Comparison of the Rate of Placenta Accreta in Various Patterns of Patient Baseline Characteristics |
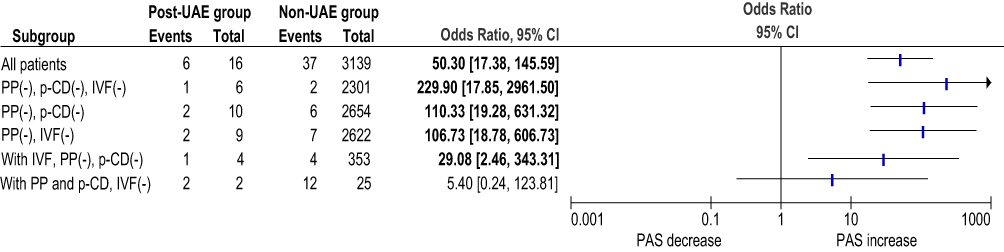 |
Figure 1 Forest plot of odds ratio of placenta accreta spectrum in post-UAE cases. Forest plots show the OR and 95% CI of the risk for PAS. Various combinations were determined, and we revealed that post-UAE is a significant risk factor for PAS except for the P-UAE with PP and p-CD groups. (-) indicates that the patients with pointed factor were excluded. Bold indicates statistical significance. Abbreviations: CD, cesarean delivery, CI, confidence interval; IVF, in vitro fertilization-embryo transfer pregnancy; PAS, placenta accreta spectrum, p-CD; previous cesarean delivery; PP, placenta previa; p-UAE, post-UAE; UAE, uterine artery embolization. |
Although we found that two of the three patients (66.7%) in the post-UAE group with a history of manual removal of placenta (MRP) had PAS (Table 2), we could not compare the effect of MRP on risk of PAS between the post-UAE and non-UAE groups as we did not have any data on MRP for the patients in the non-UAE group.
The results of our literature review are shown in Table 5. Out of the 95 nonduplicate records identified from the electronic databases search, we retrieved 95 full-text articles after screening the titles and abstracts. Then, after excluding the articles that did not meet the inclusion criteria (3 case series and 3 case reports), we included 6 articles in the review.13,19-23 Table 5 provides detailed information on the obstetric outcomes of those studies. All case series showed high rates of PAS (2/19 [10.5%], 5/30 [16.7%], 4/17 [23.5%]). We found that the reports lacked a good definition for PAS diagnosis and did not have well-described patient baseline characteristics.
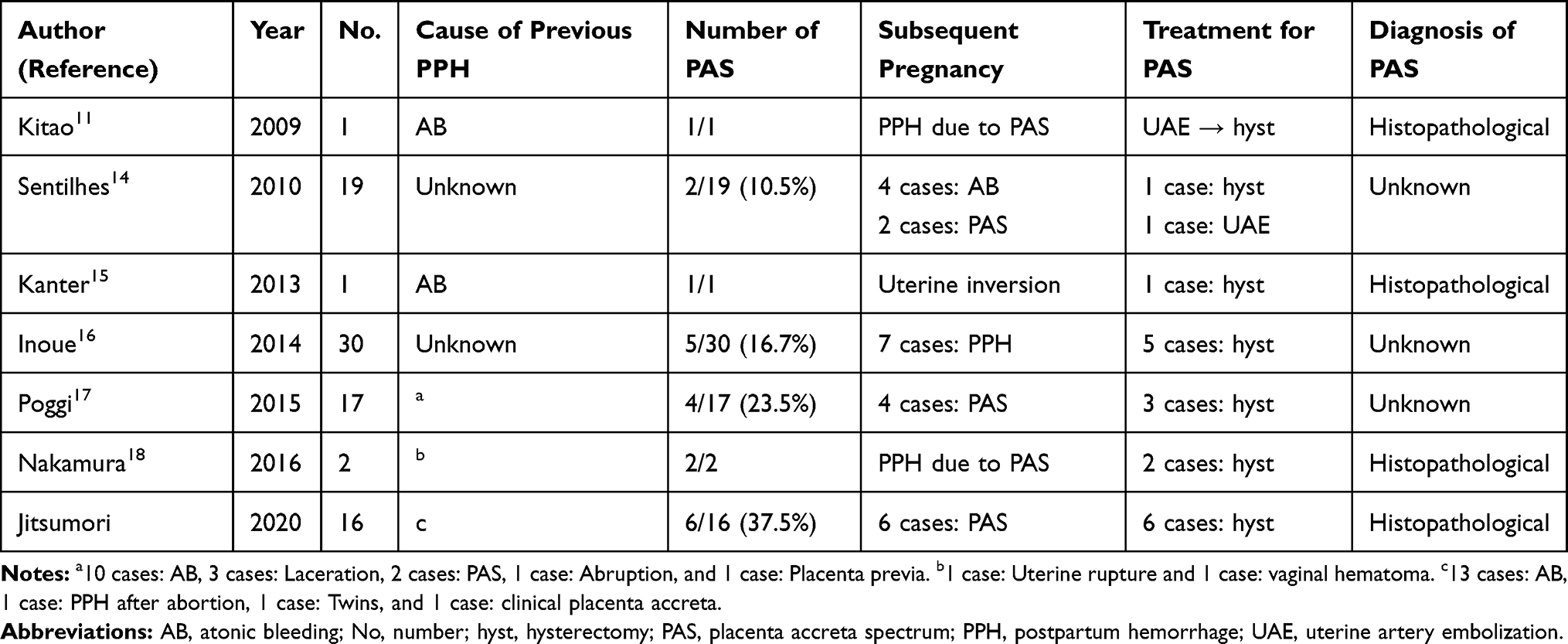 |
Table 5 Literature Review on the Rate of Placenta Accreta Spectrum in Subsequent Pregnancies Following Uterine Artery Embolization Due to Postpartum Hemorrhage |
Discussion
A key finding of our study was that previous UAE for PPH was a significant risk factor for PAS. A previous study reported an overall incidence of PAS of 1 in 553 cases.24 PAS is rare but results in high maternal morbidity and mortality rates.16,25,26 Various factors such as placenta previa, previous CD, and IVF have been recognized as risk factors for PAS, but the role of previous UAE as a risk factor was not well understood.27–29 Here, we identified previous UAE as a clear risk factor for PAS in the subsequent pregnancy.
Brown et al reported the first case of UAE for PPH in 1979.30 One of the purposes of UAE is to avoid hysterectomy (a last resort to stop severe bleeding). UAE can control PPH and is recommended in various obstetric guidelines. The clinical success rate of UAE for PPH is greater than 90%.31 However, the obstetric outcomes of subsequent pregnancies have been reported only in a few studies which have shown a higher rate of PAS. Inoue et al reported that five out of 28 women (16.6%) who underwent UAE for PPH had to receive a hysterectomy due to PAS.22 However, this and other reports did not compare the outcomes of patients with UAE to those without previous UAE, and differences in the patient characteristics were not considered.13,19-23
The study reported by Cho et al included 96 women and represents the largest study of subsequent pregnancy after UAE due to PPH.32 A multivariate-adjusted analysis showed that UAE during a first delivery increased the rate of UAE at a second delivery (0.10% vs 5.9%; odds ratio, 25.56; 95% CI, 9.86–66.23), but the authors did not investigate the causes of PPH or the PAS rates; thus, the study did not satisfy our criteria for inclusion in the literature review.
As shown in Table 5, few reports exist on PAS following UAE for PPH. From the results of these studies, we found that UAE is a major risk factor for PAS. Uterine necrosis is a complication of UAE for PPH, and we considered that the factors leading to uterine necrosis after UAE for PPH include reduced blood flow to the uterus and a damaged myometrium and endometrium.33 We speculate that the myometrial damage induced by UAE could be one of the causes of PAS in the same way as the damage of the endometrium-myometrial interface caused by uterine surgery, especially cesarean delivery, may induce PAS.34,35 Another mechanism could be the reduced thickness of the endometrium as patients with lower endometrial thickness, such as those undergoing cryopreserved embryo transfer, have been reported to have a higher risk for PAS (adjusted OR 3.87, 95% CI 1.08–13.81).
UAE is considered appropriate in the treatment of PPH because it reduces bleeding, avoids hysterectomy, and preserves fertility with high success rates and tolerable side effects.8,36,37 However, the procedure entails risks such as PAS in the subsequent pregnancy. Although there is little evidence, uterine compression sutures and uterine balloon tamponade (UBT) seem not to be associated with a higher risk of PAS in the subsequent pregnancy when compared with UAE.9,12,38-40 Therefore, if the situation allows, clinicians may try to control PPH using uterine compression sutures or UBT before performing UAE.
Although we revealed that previous UAE is a strong risk factor for PAS in the subsequent pregnancy, we should be aware that our study and previous studies could not exclude the effect of the presence of PAS as the cause of PPH in the first pregnancy. A previous report showed that the rate of recurrent PAS (including clinical PAS) is 19.9%.41 Therefore, if the cause of PPH in the first pregnancy is clinical PAS, diagnosis of histological PAS in subsequent pregnancies would increase. While there were only 3 cases of MRP as the cause of PPH, those with MRP treated with UAE showed a high risk of PAS (2 of 3 cases) in the subsequent pregnancy (Table 2). There is a possibility that these cases could have had clinical PAS in the previous pregnancy resulting in the higher rate of PAS observed in the subsequent pregnancy.
In our study, we included all patients without previous UAE in the non-UAE group to estimate the risk of PAS in the general pregnancies at our institution. Because the number of patients in the post-UAE group is small, we could not match the patients’ clinical characteristics well. To resolve this problem, propensity score matching could have been useful; however, we could not perform this analysis due to the limited number of cases. Moreover, we could not perform multivariate analysis due to the same reason. However, we believe that we managed to show the high rate of PAS in patients with previous UAE, and demonstrated that these patients should be treated as high-risk patients.
The major strengths of our study are that it is the first one to compare outcomes of subsequent pregnancies post-UAE with pregnancies without UAE, and it reveals that the incidence of PAS is increased in the subsequent pregnancy. In addition, we used a histopathological diagnosis for PAS. Therefore, we believe that our results are valuable to clinicians managing this extremely rare condition.
Our study has several limitations. First, our study was a single-center retrospective study with a small sample size; consequently, unmeasured bias may exist in the analysis. Second, we could not compare the outcomes between patients with PPH managed by UAE and those managed by other treatment modalities because our database did not have data on the other treatment modalities. This analysis is crucial; however, we could not investigate this comparison.
Third, we could not match the patient characteristics between post-UAE and non-UAE cases as the small sample size did not allow us to perform further analyses. In addition, we could not exclude the effect of clinical PAS in the first pregnancy which was the high risk of PAS in the subsequent pregnancy. Previous studies have also shown this limitation and one should be aware of this when reading-related topics of study. Last, because our institution is a referral hospital, there is a possibility that our non-UAE group comprised patients with a significant bias towards preterm birth and FGR. To clearly show that UAE is a high-risk factor for PAS in the subsequent pregnancy, a study using data from several institutions with large numbers of cases needs to be conducted. More robust studies such as prospective studies or randomized control studies are difficult to perform on this subject.
In conclusion, we provided evidence that UAE for PPH is a significant risk factor for PAS in the subsequent pregnancy.
Abbreviations
UAE, uterine artery embolization; PPH, postpartum hemorrhage; UCS, uterine compression suture; FGR, fetal growth restriction.
Ethical Approval and Consent to Participate
This study was approved by the Osaka University Hospital Institutional Review Board and the Ethics Committee (approval #18130, approved on August 1, 2018).
Data Sharing Statement
The dataset used and/or analyzed during the current study is available from the corresponding authors upon reasonable request.
Acknowledgments
The authors thank H. Abe and K. Sakiyama for their administrative assistance in the preparation of this manuscript. The authors would like to thank Editage and Dr. Nagase for the English language review.
Author Contributions
MJ, ShM, ME, TH, SaM, TM, KM, AK, and TTa made substantial contributions to conception and design and collected the clinical data. TTo, TTa, EK, YU, and TK contributed to the data analysis and helped draft the manuscript. AK made extensive English editing in the revised manuscript. TK conceived and supervised the study and gave final approval of the version to be published. All authors contributed to drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Tadashi Kimura reports personal fees from Nihon Kayasu Co. Ltd, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Bishanga DR, Charles J, Tibaijuka G, et al. Improvement in the active management of the third stage of labor for the prevention of postpartum hemorrhage in Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18:223. doi:10.1186/s12884-018-1873-3
2. Suzuki Y, Matsuzaki S, Mimura K, et al. Investigation of perioperative complications associated with use of uterine compression sutures. Int J Gynaecol Obstet. 2017;139:28–33. doi:10.1002/ijgo.2017.139.issue-1
3. Kearney L, Kynn M, Reed R, Davenport L, Young J, Schafer K. Identifying the risk: a prospective cohort study examining postpartum haemorrhage in a regional Australian health service. BMC Pregnancy Childbirth. 2018;18:214. doi:10.1186/s12884-018-1852-8
4. Matsuzaki S, Endo M, Ueda Y, et al. A case of acute Sheehan’s syndrome and literature review: a rare but life-threatening complication of postpartum hemorrhage. BMC Pregnancy Childbirth. 2017;17:188. doi:10.1186/s12884-017-1380-y
5. Dashtinejad E, Abedi P, Afshari P. Comparison of the effect of breast pump stimulation and oxytocin administration on the length of the third stage of labor, postpartum hemorrhage, and anemia: a randomized controlled trial. BMC Pregnancy Childbirth. 2018;18:293. doi:10.1186/s12884-018-1832-z
6. Kong CW, To WW. Prognostic factors for the use of intrauterine balloon tamponade in the management of severe postpartum hemorrhage. Int J Gynaecol Obstet. 2018;142:48–53. doi:10.1002/ijgo.12498
7. Ishii T, Sawada K, Koyama S, et al. Balloon tamponade during cesarean section is useful for severe post-partum hemorrhage due to placenta previa. J Obstet Gynaecol Res. 2012;38:102–107. doi:10.1111/j.1447-0756.2011.01625.x
8. Aoki M, Tokue H, Miyazaki M, Shibuya K, Hirasawa S, Oshima K. Primary postpartum hemorrhage: outcome of uterine artery embolization. Br J Radiol. 2018;91:20180132. doi:10.1259/bjr.20180132
9. Nishikawa A, Matsuzaki S, Mimura K, Kanagawa T, Kimura T. Short interpregnancy interval after B-Lynch uterine compression suture: a case report. Clin Exp Obstet Gynecol. 2016;43:434–436.
10. Committee on Practice B-O. Practice Bulletin No. 183: postpartum hemorrhage. Obstet Gynecol. 2017;130:e168–e86. doi:10.1097/AOG.0000000000002351
11. Matsuzaki S, Endo M, Tomimatsu T, et al. New dedicated blunt straight needles and sutures for uterine compression sutures: a retrospective study and literature review. BMC Surg. 2019;19:33. doi:10.1186/s12893-019-0495-7
12. Nagase Y, Matsuzaki S, Kawanishi Y, et al. Efficacy of prophylactic antibiotics in Bakri intrauterine balloon placement: a single-center retrospective analysis and literature review. AJP Rep. 2020.
13. Poggi SH, Yaeger A, Wahdan Y, Ghidini A. Outcome of pregnancies after pelvic artery embolization for postpartum hemorrhage: retrospective cohort study. Am J Obstet Gynecol. 2015;213:576 e1–5. doi:10.1016/j.ajog.2015.06.063
14. Takahashi H, Hayashi S, Matsuoka K, Kitagawa M. Placenta accreta following uterine artery embolization. Taiwan J Obstet Gynecol. 2010;49:197–198. doi:10.1016/S1028-4559(10)60041-1
15. Sawada M, Kakigano A, Matsuzaki S, et al. Obstetric outcome in patients with a unicornuate uterus after laparoscopic resection of a rudimentary horn. J Obstet Gynaecol Res. 2018;44:1080–1086. doi:10.1111/jog.2018.44.issue-6
16. Matsuzaki S, Yoshino K, Endo M, Kakigano A, Takiuchi T, Kimura T. Conservative management of placenta percreta. Int J Gynaecol Obstet. 2018;140:299–306. doi:10.1002/ijgo.12411
17. Matsuzaki S, Matsuzaki S, Ueda Y, et al. A case report and literature review of midtrimester termination of pregnancy complicated by placenta previa and placenta accreta. AJP Rep. 2015;5:e6–e11. doi:10.1055/s-0034-1395992
18. Tanaka M, Matsuzaki S, Kumasawa K, Suzuki Y, Endo M, Kimura T. Cervical varix complicated by placenta previa: a case report and literature review. J Obstet Gynaecol Res. 2016;42:883–889. doi:10.1111/jog.2016.42.issue-7
19. Kitao K, Makihara N, Morita H, et al. The development of placenta increta following pelvic transcatheter artery embolization for postpartum hemorrhage. Clin Exp Obstet Gynecol. 2009;36:53–54.
20. Sentilhes L, Gromez A, Clavier E, Resch B, Verspyck E, Marpeau L. Fertility and pregnancy following pelvic arterial embolisation for postpartum haemorrhage. BJOG. 2010;117:84–93. doi:10.1111/j.1471-0528.2009.02381.x
21. Kanter G, Packard L, Sit AS. Placenta accreta in a patient with a history of uterine artery embolization for postpartum hemorrhage. J Perinatol. 2013;33:482–483. doi:10.1038/jp.2012.99
22. Inoue S, Masuyama H, Hiramatsu Y; Multi-Institutional Study Group of Transarterial Embolization for Massive Obstetric Haemorrhage in C, Shikoku Area Society of O, Gynecology. Efficacy of transarterial embolisation in the management of post-partum haemorrhage and its impact on subsequent pregnancies. Aust N Z J Obstet Gynaecol. 2014;54:541–545. doi:10.1111/ajo.12228
23. Nakamura Y, Aoki S, Takebayashi S, Hirahara F. Effect of transarterial embolization for post-partum hemorrhage on subsequent pregnancy. J Obstet Gynaecol Res. 2016;42:1186–1189. doi:10.1111/jog.13029
24. Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: twenty-year analysis. Am J Obstet Gynecol. 2005;192:1458–1461. doi:10.1016/j.ajog.2004.12.074
25. Matsuzaki S, Yoshino K, Endo M, et al. Successful anticoagulant therapy for disseminated intravascular coagulation during conservative management of placenta percreta: a case report and literature review. BMC Pregnancy Childbirth. 2017;17:443. doi:10.1186/s12884-017-1634-8
26. Jauniaux E, Ayres-de-Campos D; Diagnosis FPA, Management Expert Consensus P. FIGO consensus guidelines on placenta accreta spectrum disorders: introduction. Int J Gynaecol Obstet. 2018;140:261–264. doi:10.1002/ijgo.12406
27. Kaser DJ, Melamed A, Bormann CL, et al. Cryopreserved embryo transfer is an independent risk factor for placenta accreta. Fertil Steril. 2015;103:1176–84 e2. doi:10.1016/j.fertnstert.2015.01.021
28. Silver RM, Fox KA, Barton JR, et al. Center of excellence for placenta accreta. Am J Obstet Gynecol. 2015;212:561–568. doi:10.1016/j.ajog.2014.11.018
29. Matsuzaki S, Yoshino K, Tomimatsu T, Takiuchi T, Kumasawa K, Kimura T. Placenta accreta following laparoscopic adenomyomectomy: a case report. Clin Exp Obstet Gynecol. 2016;43:763–765.
30. Brown BJ, Heaston DK, Poulson AM, Gabert HA, Mineau DE, Miller FJ
31. Delotte J, Novellas S, Koh C, Bongain A, Chevallier P. Obstetrical prognosis and pregnancy outcome following pelvic arterial embolisation for post-partum hemorrhage. Eur J Obstet Gynecol Reprod Biol. 2009;145:129–132. doi:10.1016/j.ejogrb.2009.03.013
32. Cho GJ, Shim JY, Ouh YT, et al. Previous uterine artery embolization increases the rate of repeat embolization in a subsequent pregnancy. PLoS One. 2017;12:e0185467. doi:10.1371/journal.pone.0185467
33. Poujade O, Ceccaldi PF, Davitian C, et al. Uterine necrosis following pelvic arterial embolization for post-partum hemorrhage: review of the literature. Eur J Obstet Gynecol Reprod Biol. 2013;170:309–314. doi:10.1016/j.ejogrb.2013.07.016
34. Jauniaux E, Collins S, Burton GJ. Placenta accreta spectrum: pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am J Obstet Gynecol. 2018;218:75–87. doi:10.1016/j.ajog.2017.05.067
35. Fitzpatrick KE, Sellers S, Spark P, Kurinczuk JJ, Brocklehurst P, Knight M. Incidence and risk factors for placenta accreta/increta/percreta in the UK: a national case-control study. PLoS One. 2012;7:e52893. doi:10.1371/journal.pone.0052893
36. Hardeman S, Decroisette E, Marin B, et al. Fertility after embolization of the uterine arteries to treat obstetrical hemorrhage: a review of 53 cases. Fertil Steril. 2010;94:2574–2579. doi:10.1016/j.fertnstert.2010.02.052
37. Liu Z, Wang Y, Yan J, et al. Uterine artery embolization versus hysterectomy in the treatment of refractory postpartum hemorrhage: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2020;33:693–705. doi:10.1080/14767058.2018.1497599
38. Matsuzaki S, Jitsumori M, Hara T, et al. Systematic review on the needle and suture types for uterine compression sutures: a literature review. BMC Surg. 2019;19:196. doi:10.1186/s12893-019-0660-z
39. An GH, Ryu HM, Kim MY, Han JY, Chung JH, Kim MH. Outcomes of subsequent pregnancies after uterine compression sutures for postpartum hemorrhage. Obstet Gynecol. 2013;122:565–570. doi:10.1097/AOG.0b013e31829e3b1d
40. Carlson L, Jackson C, Glover A, Webster C, Dotters-Katz S, Strauss R. Subsequent pregnancy outcomes following use of an intrauterine tamponade balloon for postpartum hemorrhage (PPH) [24C]. Obstet Gynecol. 2017;129:36S–37S. doi:10.1097/01.AOG.0000514338.16396.61
41. Cunningham KM, Anwar A, Lindow SW. The recurrence risk of placenta accreta following uterine conserving management. J Neonatal Perinatal Med. 2015;8:293–296. doi:10.3233/NPM-15915028
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.