Back to Journals » Journal of Pain Research » Volume 15
Objective and Quantitative Evaluation of Spontaneous Pain-Like Behaviors Using Dynamic Weight-Bearing System in Mouse Models of Postsurgical Pain
Authors Lu F ![]() , Kato J, Toramaru T, Sugai M, Zhang M, Morisaki H
, Kato J, Toramaru T, Sugai M, Zhang M, Morisaki H ![]()
Received 20 January 2022
Accepted for publication 17 May 2022
Published 2 June 2022 Volume 2022:15 Pages 1601—1612
DOI https://doi.org/10.2147/JPR.S359220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qi Fang
Fanglin Lu,1,2 Jungo Kato,2 Tomoko Toramaru,2 Megumi Sugai,2 Mengting Zhang,1,2 Hiroshi Morisaki2
1Keio University Graduate School of Medicine Doctoral Programs, Tokyo, Japan; 2Department of Anesthesiology, Keio University School of Medicine, Tokyo, Japan
Correspondence: Jungo Kato, Department of Anesthesiology, Keio University School of Medicine, 35 Shinanoamchi, Shinjuku-ku, Tokyo, 160-8582, Japan, Tel +81-3-3353-1211, Fax +81-3-3356-8439, Email [email protected]
Background: The paucity of objective and reliable measurements of pain-like behaviors has impeded the translatability of mouse models of postsurgical pain. The advanced dynamic weight-bearing (DWB) system enables evaluation of spontaneous pain-like behaviors in pain models. This study investigated the suitability and efficiency of the DWB system for assessing spontaneous pain-like behaviors and analgesic therapies in murine models of postsurgical pain.
Methods: Male adult C57BL/6JJcl mice were subjected to multiple surgical pain models with distinct levels of invasiveness, including a superficial incisional pain model involving only hind paw skin incision, deep incisional pain model that also involved incision and elevation of the underlying hind paw muscles, and orthopedic pain model involving tibial bone fracture and fixation with a pin (fracture and pinning [F/P] model). Spontaneous pain-like behaviors post-surgery were evaluated using weight distribution, pawprint area of the operated paw in the DWB system, and guarding pain score. Mechanical hypersensitivity was assessed using the von Frey test. The therapeutic effects of analgesics (diclofenac and buprenorphine for the deep incision model and diclofenac for the F/P model) were evaluated using the DWB system and von Frey test.
Results: The von Frey test demonstrated contradictory results between superficial and deep incisional pain models. The DWB system captured weight distribution changes in the operated hind paw, in accordance with the invasiveness and time course of wound healing in these surgical pain models. The reduction in weight-bearing on the operated paw correlated with guarding score, degree of paw swelling, and local expression of inflammatory mediators. DWB enabled accurate evaluation of the pharmacological effects of analgesics for detecting attenuation of surgery-induced weight-bearing changes in these models.
Conclusion: The DWB system serves as an objective and reliable method for quantifying pain-like behaviors and evaluating the therapeutic effects of analgesics in mouse models of postsurgical pain models.
Keywords: postoperative pain, surgery, animal models, dynamic weight-bearing, incisional pain, orthopedic pain
Introduction
More than 300 million patients undergo surgery annually worldwide.1 Despite recent advances in postsurgical pain management, a high proportion of patients still report moderate to severe acute pain. A subset of patients develops persistent postsurgical pain, which severely impacts their postsurgical rehabilitation and quality of life.2 Hence, there is an urgent need to elucidate the mechanisms underlying postsurgical pain using experimental animal models and in clinical settings to develop novel analgesic therapies with greater efficacy and lower risk of adverse effects.
Owing to the limitations and ethical considerations in human subject research, animal models are often employed to study pain. However, a major challenge is the validity of anthropomorphizing pain in animals and appropriate quantification of such pain-like behavioral responses, as interpretation of these responses exhibited by experimental animals is difficult. Conventional measurements used in postsurgical pain studies, such as the von Frey test and cold/hot plate test, investigate evoked responses to external noxious stimuli (ie, mechanical and thermal); however, they do not address stimulus-independent or spontaneous pain.3 Both stimulus- and non-stimulus-evoked pain are necessary to reproduce the complex postsurgical pain experience in humans. Therefore, reliable methods for assessing non-stimulus-evoked pain are required.
The advanced dynamic weight-bearing (DWB) apparatus analyzes weight-bearing behaviors in mice and exhibits good performance for evaluating spontaneous pain-like behaviors in multiple pain models, including inflammatory pain and antigen-induced arthritis.4–6
Here, we first tested the hypothesis that DWB provides a valid to assessment of spontaneous pain-like behavior in multiple postsurgical pain models with distinct levels of invasiveness in mice, including a superficial incisional pain model that only included hind paw skin incision, deep incisional pain model that also involved incision and elevation of underlying muscles in the hind paw, and orthopedic pain model in which the tibial bone was fractured and fixed with a pin (fracture and pinning [F/P] model). Second, we investigated the efficacy of DWB for evaluating analgesic therapies using these models.
Materials and Methods
Animals
The experiments were conducted using male C57BL/6JJcl mice (CLEA Japan, Inc. Tokyo, Japan) at 9–13 weeks old. All animals were housed in standard cages (four to five per cage) at an ambient temperature of 22°C under a 12:12-h light-dark cycle and were fed ad libitum. Mice were allowed to acclimatize to the laboratory facilities for at least 1 week before experimentation. All experiments were approved by the Animal Care and Utilization Committee of the Keio University School of Medicine, Tokyo, Japan (approval number #17022) and adhered to the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines (https://www.nc3rs.org.uk/arrive-guidelines). Data were collected in a manner blinded to group assignments. The exclusion criteria included the presence of severe non-surgery-related wounds, signs of systemic weakness (eg, significant weight loss [>20% of body weight] and lethargic appearance), and signs of surgical site infection. None of the mice used in this study met these criteria. Randomization for group allocation was performed based on the baseline mechanical threshold in the von Frey test, body weight, and weight distribution on the ipsilateral paw in DWB using a custom-made Excel macroprogram.
Surgical Incisional Pain Model
Deep/Superficial Incisional Pain Model
The hind paw incisional pain model was employed as described by Brennan et al7,8 with several modifications. Animals were placed in the prone position under 4% sevoflurane anesthesia. A drape was placed after disinfection with 10% povidone-iodine solution (popiyodon solution 10%; Yoshida Pharmaceutical Co., Ltd., Saitama, Japan). In the superficial incisional pain model, a 5-mm longitudinal incision was made through the skin with a scalpel blade, starting 2 mm from the proximal edge of the heel, and extending toward the toe (Figure 1A). In the deep incisional pain model, a 5-mm longitudinal incision was made in the same manner as that in the superficial incisional pain model, and the underlying plantaris muscle was incised and elevated for 5 min (Figure 1A and B). This model was similar to a previously reported model except for 5-minute suspension of the muscle elevation.8 This significant modification was implemented to better reproduce the clinical condition of deep incisional pain and to enhance the difference in invasiveness compared to the superficial incisional pain model. After hemostasis, the wound was closed using a 6–0 nylon suture and covered with bacitracin ointment (Baramycin ointment, TOYO Pharmaceutical Co., Ltd., Osaka, Japan) to prevent wound infection (Figure 1C). The sham surgery comprised 4% sevoflurane anesthesia, antiseptic preparation, and application of topical antibiotics without skin or muscle incision. To monitor the paw swelling post-surgery, the paw thickness was measured at the metatarsal level in the dorsal-plantar axis using a digital caliper (A&D Company, Tokyo, Japan).4
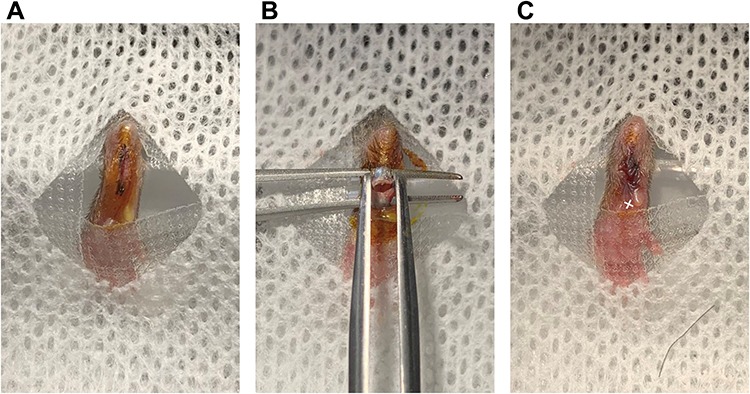 |
Figure 1 Representative photographs of surgical procedures of superficial and deep incisional pain model. Notes: (A) Superficial incisional pain model. After disinfection, 5-mm longitudinal incision was made through the skin, starting 2 mm from the proximal edge of the heel, and extending toward the toe. (B) Deep incisional pain model. In addition to the skin incision, the underlying plantaris muscle were incised and elevated for 5 min. (C) The wound was closed using a 6–0 nylon suture. The white cross indicates the point at which filaments were applied in the von Frey test. |
Orthopedic Pain Model (Fracture and Pinning Model)
The fracture and pinning (F/P) model was established as an orthopedic pain model as reported by Hiltunen et al,9 with modifications. Animals were placed in a supine position under 4% sevoflurane anesthesia, and the surgical site was shaved from the mid-tibia to mid-femur to expose the knee joint. After disinfection with 10% povidone-iodine solution, a 5-mm anterior longitudinal incision was made centered over the knee joint with a scalpel blade. The skin was opened via blunt dissection using scissors. An entry portal was created to breach the tibial plateau using a 26-gauge needle, which was then removed. A 30-gauge needle was inserted into the portal and guided down the medullary cavity with a reaming motion until resistance was felt to form an intramedullary pinning. The needle was retracted by 1 mm, and the end of the needle was cut with a wire cutter. The excess needle was then flushed with the articular surface. A transverse fracture was manually created with surgical scissors on the proximal tibia (3 mm below the tibial plateau) without cutting the inserted needle. The wound was closed using a 6–0 nylon suture and covered with bacitracin ointment. The sham operation comprised 4% sevoflurane anesthesia, antiseptic preparation, 5-mm longitudinal superficial incision, and topical antibiotics without intramedullary pinning or tibial fracture.
Administration of Analgesics
Diclofenac sodium salt (Sigma-Aldrich, St Louis, MO, USA) and buprenorphine hydrochloride (Lepetan, Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan) were dissolved in 0.9% saline. All drugs were subcutaneously (sc) administered in a 250-μL volume. Mice received subcutaneous injection of diclofenac (0.25 mg/250 μL), buprenorphine (1.67 × 10−3 mg/250 μL), or saline (vehicle control) thrice per day (9 am, 3 pm, and 9 pm) from the postoperative day (POD) 0 to POD 3. The postsurgical pain model was established 30 min after the animals received their first subcutaneous injection.
Behavioral Analysis
von Frey Test
Mechanical hypersensitivity was assessed using paw withdrawal thresholds in response to the von Frey filaments (OptiHair, Marstock Nervtest, Schriesheim, Germany). After 30 min of habituation to the plastic enclosure and the mesh platform, a calibrated monofilament was applied perpendicularly to the hind paw plantar surface at the midsole (Figure 1C), pressed upward, and left for approximately 3 s with Dixon’s up-down method.10 Brisk paw withdrawals, licking, or shaking of the paw were scored as positive responses. The mechanical force required to elicit paw withdrawal in 50% (50% withdrawal threshold) of animals was determined based on Dixon’s statistical formula, as previously described.11,12
Advanced Dynamic Weight-Bearing System
Spontaneous limb pain-like behavior was assessed using an advanced DWB apparatus (Bioseb, Vitrolles, Provence-Alpes-Côte D’Azur, France). Animals were placed in a transparent enclosure for approximately 5 min. A matrix comprising pressure sensors that captured the weight distribution data for each of the four paws was embedded in the floor. Each freely moving animal was filmed from above, and changes in postural equilibrium were synchronously and automatically tracked and analyzed by the software, as previously described.13 A zone was considered valid when the following parameters were detected: ≥0.8 g on one captor with a minimum of two adjacent captors recording ≥1.0 g. A time segment was considered valid if ≥3 stable pictures were detected. An observer manually validated each automatically presumed paw position to avoid subsequent error identification afterward. Weight distribution toward the ipsilateral paw over the total body weight and pawprint area on the ipsilateral paw over that of the contralateral paw were used as parameters.
Guarding Pain Score
Guarding behavior was assessed using a scoring method as described previously for rats.14,15 After 30 min of habituation to the plastic enclosure and the mesh platform, the operated area in the ipsilateral hind paw or the corresponding area in the contralateral paw was closely observed during a 5-second period repeated for 12 times. Scores of 0, 1, or 2 were assigned according to hind paw position, as follows: 0, full weight-bearing was presented as the observed area being blanched or distorted by the mesh; 1, the observed area slightly touched the mesh without blanching or distortion; 2, the paw was completely off the mesh. A cumulation of the 12 scores was calculated for each paw, and the guarding pain score was obtained by subtracting the cumulative score of the contralateral paw from that of the ipsilateral paw.
Quantitative Real-Time (qPCR) in Paw Plantar Skin Samples
Plantar skin samples, including the subcutaneous and muscle layers, were harvested under 2.5% sevoflurane anesthesia 6 hours after incision in each group. qPCR experiments were conducted as described previously.16 Briefly, total RNA was isolated from ipsilateral hind paw plantar skin using TRIzol reagent (15,596,026; Invitrogen, Carlsbad, CA, USA) and RNeasy Plus Mini Kit (74,134; Qiagen, Hilden, Germany). Real-time reverse transcription-PCR (RT-PCR) was performed with the ReverTra Ace qPCR RT kit (FSQ-101; TOYOBO, Osaka, Japan) and TaqMan Fast Universal PCR Master Mix (4,352,042; Applied Biosystems, Foster City, CA, USA) using a StepOne real-time PCR system (Applied Biosystems, Foster City, CA, USA). Predeveloped specific primer sets for Ilb1 (Mm00434228_m1), Tnf (Mm00443258_m1), Ngf (Mm00443039_m1), and Hprt1 (Mm01545399_m1) were used for mRNA analyses (all from Applied Biosystem, Foster City, CA, USA). The data were normalized to Hprt1 mRNA levels as a housekeeping gene and were expressed as relative to the naïve group.
Statistical Analysis
Data were analyzed using Prism software (GraphPad 9, San Diego, CA, USA) and are presented as the mean ± standard error of the mean (SEM). Two-way repeated-measures analysis of variance (ANOVA) and one-way ANOVA followed by Šídák’s multiple comparison test were performed to compare the mean differences between the corresponding groups. Pearson’s correlation test was used to analyze the correlation between DWB results and paw swelling, or guarding pain score differences, or relative mRNA expression of inflammatory factors. p-value of <0.05 was considered statistically significant.
Results
DWB is an Effective Method to Evaluate Nociception in the Incisional Pain Model in Mice
We first examined the effectiveness of the DWB system for discerning behavioral changes induced by surgical incisions with different invasiveness applied to unilateral hind paws in mice. Compared to that in naïve mice, both the superficial and deep incisional procedures elicited significant paw swelling that peaked at 6 h post-surgery and persisted for 2 weeks (F (2,29) = 23.03; p < 0.0001) (Figure 2A). The degree of swelling was more pronounced in the deep incision group than in the superficial group (mean ± SEM: 3.910 ± 0.095 mm vs 3.223 ± 0.083 mm; p < 0.0001), highlighting the difference in the invasiveness between the two models.
 |
Figure 2 Hind paw thickness, mechanical allodynia, and weight distribution changes in different incisional pain models. Abbreviations: BL, baseline; POD, postoperative day. Notes: Changes were evaluated at various time points (baseline, 6 h, POD 1, POD 4, POD 7, and POD 14) in the superficial incisional pain model (n = 13) and deep incisional pain model (n = 14) compared with naïve animals (n = 5). (A) Ipsilateral hind paw thickness (mm) measured using an electronic caliper. (B) Ipsilateral paw withdrawal threshold following the von Frey filament stimulation. (C) Weight distribution ratio of the ipsilateral paw to the total body weight assessed using the advanced dynamic weight-bearing (DWB) apparatus. (D) The paw print area ratio of the ipsilateral paw to the contralateral paw was assessed using DWB. Data are expressed as the mean ± SEM, assessed by two-way ANOVA with repeated measures followed by Šídák’s multiple comparisons test. *p < 0.05, ***p < 0.001, ****p < 0.0001 vs baseline; †p < 0.05; ††p < 0.01, †††p < 0.001, ††††p < 0.0001 vs naïve; ‡‡p < 0.01, ‡‡‡p < 0.001, ‡‡‡‡p < 0.0001 deep incision vs superficial incision. |
Relative to the baseline value (2.823 ± 0.199 g), the paw withdrawal threshold measured using the von Frey test was significantly decreased 6 h (1.508 ± 0.302 g; p = 0.0103) and on POD 1 (1.698 ± 0.312 g; p = 0.0281) after the superficial incisional procedure (Figure 2B). In the deep incisional group, however, the von Frey test failed to demonstrate postsurgical mechanical hypersensitivity (6 h: 3.311 ± 0.313 g vs baseline: 3.048 ± 0.232 g; p = 0.9777), possibly due to impaired paw movement induced by severe paw swelling and guarding behaviors or potential nerve damage. In contrast, the DWB system captured the presence of a relief posture with significant reduction in weight-bearing on the operated paw at 6 h post-surgery in both superficial (superficial: 0.276 ± 0.022 vs baseline: 0.424 ± 0.013; p < 0.0001) and deep incisional procedures (deep: 0.172 ± 0.016 vs baseline: 0.429 ± 0.012; p < 0.0001) (Figure 2C). These reductions in weight-bearing on the operated paw persisted until POD 14 in the deep incisional procedure (0.357 ± 0.018; p = 0.0279 vs baseline). Similar changes were observed in the pawprint area measured using the DWB system, with greater prominence in the deep incisional model (F (2, 29) = 6.496; p = 0.0047) (Figure 2D). The sham surgery did not produce remarkable changes from the naïve mice in either von Frey test or DWB-derived parameters (Supplementary Figure S1).
To further assess the validity of the DWB system, we assessed guarding pain behavior, another unprovoked pain-related behavior, following the incisional procedures. Compared to that in naïve mice, both superficial and deep incisions induced guarding pain behavior 6 h after incision. Mice in the deep incision group exhibited greater guarding pain behavior compared to those in the superficial incision group. A significant positive correlation was observed between the increase in guarding pain score and the reduction in weight-bearing captured by the DWB system (R2 = 0.6268; p < 0.0001; Figure 3A), supporting the validity of the DWB system for evaluating spontaneous pain-like behaviors after incision.
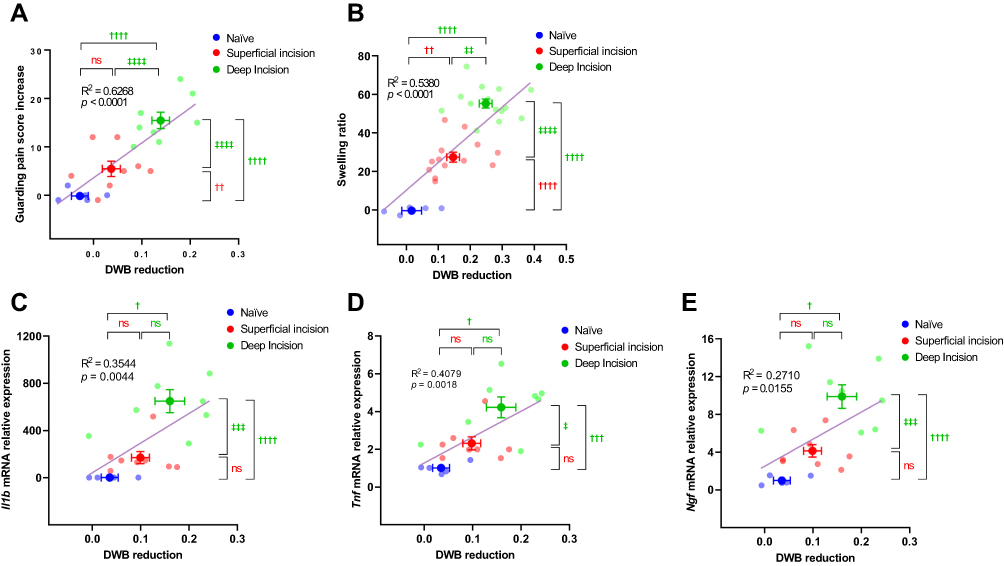 |
Figure 3 Evaluations of inflammatory responses and pain-like behaviors in different incisional pain models. Abbreviations: BL, baseline; POD, postoperative day; R2, Pearson’s correlation coefficient. Notes: Changes were evaluated at baseline and 6 h post-surgery in the superficial incisional pain model (n = 8) and deep incisional pain model (n = 8) compared with naïve animals (n = 5). (A) Correlation between the increase in the cumulative guarding pain score and reduction in weight distribution in the ipsilateral paw at 6 h post-surgery. (B) Correlation between the swelling ratio (increased ipsilateral hind paw thickness to baseline ratio) and reduction in weight distribution on ipsilateral paw at 6 h after surgery. (C–E) Correlation between the fold changes in mRNA expression of inflammatory factors Il1b (C), Tnf (D) and Ngf (E) in ipsilateral hind paw skins and the reduction in weight distribution on ipsilateral paw at 6 h after surgery. Data were expressed as mean ± SEM, assessed by two-way ANOVA with repeated measures followed by Šídák’s multiple comparisons test. †p < 0.05; ††p < 0.01, †††p < 0.001, ††††p < 0.0001 vs naïve; ‡p < 0.05, ‡‡p < 0.01, ‡‡‡p < 0.001, ‡‡‡‡p < 0.0001 deep incision vs superficial incision. |
In contrast to the paradoxical observations in the von Frey test, the reduction in weight-bearing on the operated paw captured by DWB mirrored the guarding behavior after the incisional surgery, which was positively correlated with the severity of the paw swelling (R2 = 0.5380; p < 0.0001) (Figure 3B). Further, we observed positive correlations between the reduction in weight-bearing captured by DWB and the relative mRNA expressions of the pro-inflammatory/nociceptive factors Il1b (R2 = 0.3544, p = 0.0044; Figure 3C), Tnf (R2 = 0.4079, p = 0.0018; Figure 3D), and Ngf (R2 = 0.2710; p = 0.0155) (Figure 3E) in the operated paw skin, with clear differences among the three groups. These results indicated that the DWB system may be useful for quantifying pain-like behaviors during spontaneous activity in surgical incisional pain models in mice.
DWB is a Valid Tool for Analgesic Drug Evaluation in a Deep Incisional Pain Model in Mice
To verify whether the DWB system qualified as an assessment tool for the analgesic effects of drugs in surgical incisional pain models in mice, we assessed two different classes of commonly used perioperative analgesics, diclofenac and buprenorphine, which were administered preemptively in the deep incisional procedure. Given the failure to observe the surgery-induced mechanical hypersensitivity, no significant differences were noted in the von Frey test between the two analgesic groups and the saline group (F (2, 31) = 0.5899; p = 0.5605) (Figure 4A). In contrast, the DWB system demonstrated an attenuation of weight-bearing changes caused by deep incision in both the diclofenac and buprenorphine groups 6 h post-surgery compared with the saline-treated group (F (2, 31) = 8.257; p = 0.0013) (Figure 4B). Similar analgesic effects of diclofenac and buprenorphine were observed for pawprint area (F (2, 31) = 6.865; p = 0.0034) (Figure 4C). These findings corroborated the utility of the DWB system for assessing the analgesic effects of drugs in surgical incisional pain models in mice.
 |
Figure 4 Effects of analgesics on pain-like behaviors after deep incision. Abbreviations: BL, baseline; POD, postoperative day. Notes: Changes were evaluated at two different time points (baseline and 6 h) in the diclofenac (n = 11) and buprenorphine (n = 11) groups, compared to the saline group (n = 12). (A) Ipsilateral paw withdrawal threshold following the von Frey filament stimulation. (B and C) Spontaneous pain-like behavior was assessed using advanced DWB apparatus. (B) Weight distribution ratio of the ipsilateral paw to the total body weight. (C) Pawprint area ratio of the ipsilateral paw to the contralateral paw. Data were expressed as mean ± SEM, assessed by two-way ANOVA with repeated measures followed by Šídák’s multiple comparisons test. *p < 0.05, ****p < 0.0001 vs baseline; †††p < 0.001, ††††p < 0.0001 vs time-matched saline-treated group. |
DWB is a Reliable Tool in Evaluating Nociception in an Orthopedic Pain Model in Mice
To further investigate the adaptability of the DWB to surgical pain models in mice, the DWB system was applied to the F/P model, which encapsulates different aspects of surgery-induced pain. The von Frey test applied to the plantar surface of the operated hind paw did not reveal any significant changes in mechanical sensitivity between the sham and F/P groups (F (1, 12) = 0.08895; p = 0.7706) (Figure 5A). In contrast, the DWB system revealed significant reductions in weight-bearing on the operated paw on POD 1 (0.263 ± 0.028 vs baseline 0.434 ± 0.009; p = 0.0041), which persisted for 2 weeks post-surgery (POD 15: 0.300 ± 0.019 vs baseline; p = 0.0035) (Figure 5B). Similarly, the DWB system revealed a significant reduction in the pawprint area on POD 1 (0.604 ± 0.054 vs baseline: 0.996 ± 0.048; p = 0.0065), which was evident until POD 11 (0.689 ± 0.054 vs baseline; p = 0.0262) (Figure 5C). No significant changes were observed in weight-bearing (F (5, 36) = 0.7455; p = 0.5947) or pawprint area (F (5, 36) = 1.107; p = 0.3740) throughout the observation period following sham surgery (Figures 5B and C).
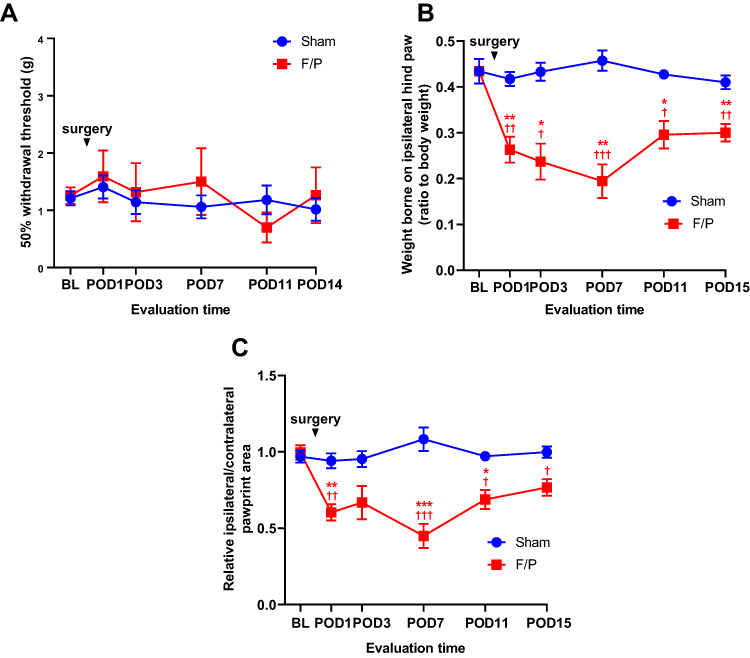 |
Figure 5 Mechanical allodynia and weight distribution changes in orthopedic pain model. Abbreviations: BL, baseline; F/P, fracture and pinning; POD, postoperative day. Notes: Changes were evaluated at various time points (baseline, POD 1, POD 3, POD 7, POD 11, POD 14, and POD 15) in F/P model (n = 7) and sham group (n = 7). (A) Ipsilateral paw withdrawal threshold following the von Frey filament stimulation. (B and C) Spontaneous pain-like behavior was assessed using advanced DWB apparatus. (B) Weight distribution ratio of the ipsilateral paw to the total body weight. (C) Pawprint area ratio of the ipsilateral paw to the contralateral paw. Data were expressed as mean ± SEM, assessed by two-way ANOVA with repeated measures followed by Šídák’s multiple comparisons test. *p < 0.05, **p < 0.01, ***p < 0.001 vs baseline; †p < 0.05, ††p < 0.01, †††p < 0.001 vs time-matched sham. |
DWB is Suitable for Pharmacological Evaluation of Analgesic Drugs in an Orthopedic Pain Model in Mice
Finally, we explored the applicability of the DWB system for evaluating analgesic effects in an F/P mouse model. No significant difference was observed in the von Frey test between saline-treated and diclofenac-treated fractured mice (F (1, 12) = 1.632; p = 0.2256) (Figure 6A). Moreover, preemptive diclofenac administration mitigated weight-bearing reductions in the operated paw on POD 3 (diclofenac 0.416 ± 0.028 vs saline 0.237 ± 0.039; p = 0.0212) (Figure 6B); however, this attenuation was diminished following cessation of diclofenac after POD 3. Similarly, the reduction in the paw print area of the operated hind paw measured using the DWB system was significantly attenuated in the diclofenac-treated group on POD 3 (diclofenac: 0.783 ± 0.078 vs saline: 0.433 ± 0.049; p = 0.0199) (Figure 6C). These findings highlighted the suitability of the DWB system for pharmacological evaluation of analgesic drugs in orthopedic surgery-induced pain models in mice.
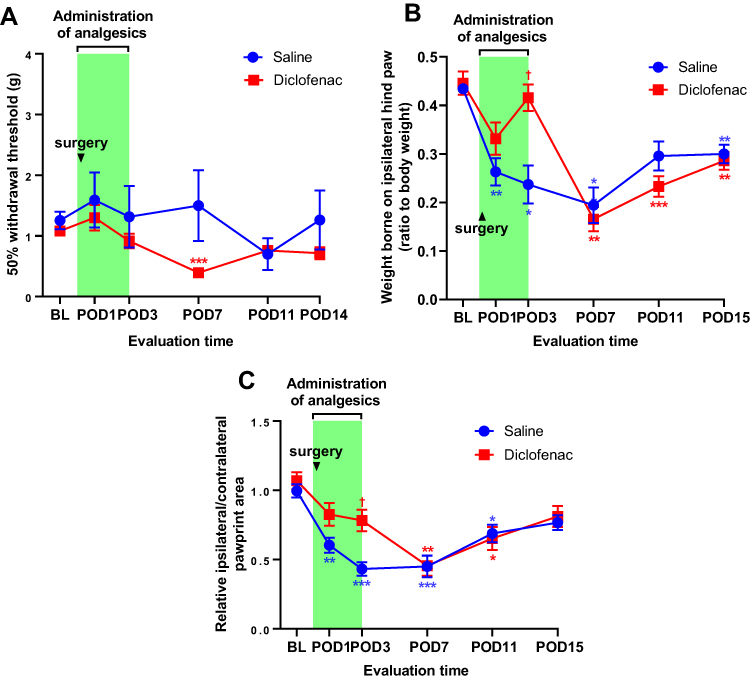 |
Figure 6 Effects of analgesics on pain-like behaviors after F/P surgery. Abbreviations: BL, baseline; F/P, fracture and pinning; POD, postoperative day. Notes: Changes were evaluated at various time points (baseline, POD 1, POD 3, POD 7, POD 11, POD 14, and POD 15) in the diclofenac (n = 7) and saline (n = 7) groups. (A) Ipsilateral paw withdrawal threshold following the von Frey filament stimulation. (B and C) Spontaneous pain-like behavior was assessed using advanced DWB apparatus. (B) Weight distribution ratio of the ipsilateral paw to the total body weight. (C) Pawprint area ratio of the ipsilateral paw to the contralateral paw. Data were expressed as mean ± SEM, assessed by two-way ANOVA with repeated measures followed by Šídák’s multiple comparisons test. *p < 0.05, **p < 0.01, ***p < 0.001 vs baseline; †p < 0.05 vs time-matched saline-treated group. |
Discussion
The present study demonstrated that the DWB system successfully captured behavioral changes in two distinct mouse models of postsurgical pain: the incisional pain model and orthopedic F/P model. Furthermore, DWB detected the mitigation of these changes by preemptive analgesic treatments in these models, further corroborating the accuracy, sensitivity, and applicability of DWB as a tool for assessing postsurgical pain in mice.
In previous studies, the main method for assessing pain-like behaviors in mouse models of postsurgical pain involved the detection of aversive behaviors in response to unpleasant stimuli using tools such as the von Frey filament stimulation and Randall–Selitto test.3 Skin incision has been reported to contribute to the development of mechanical hypersensitivity.14,15,17 Consistent with this, the superficial incision model in the current study produced postoperative mechanical hypersensitivity in the operated paw. Paradoxically, the von Frey test revealed insensitivity to mechanical stimuli in the deep incisional pain model. This discrepancy may partly be due to differences in model severity. Our deep incisional pain model employed 5-minute elevation of incised muscles to enhance the invasiveness relative to the superficial incisional pain model. This modification may have resulted in more pronounced guarding behaviors, severe paw swelling, or incisional numbness caused by collateral nerve damage,18,19 potentially leading to unresponsiveness. Moreover, owing to the prominent guarding behaviors observed in our deep incision model, it was difficult to apply von Frey filaments perpendicular to the point adjacent to the incision, as previously described.8 Rather, we applied filaments to the point distal to the incision. These differences in application points in the von Frey test may have also contributed to the discrepancies with previous reports. Moreover, the von Frey test, which was expected to mirror secondary hyperalgesia that developed on the plantar surface of the operated paw, failed to reveal significant changes in the F/P model. Given that the von Frey test only examines the presence of cutaneous mechanical hypersensitivity, it may not necessarily mirror pain in deep tissues induced by these models.
The reduction in weight-bearing of the ipsilateral hind paw observed in the DWB system exhibited a correlation with the degree of guarding behaviors potentially caused by surgery-induced pain perception, which was proportional to model invasiveness. In addition, significant positive correlations were observed between weight-bearing changes and expression of pro-inflammatory and nociceptive factors as well as the degree of swelling in the ipsilateral hind paw. Collectively, these findings support the utility of DWB as a relevant measure of inflammatory pain-related behavioral evaluation post-surgery.
As postsurgical pain is predominantly characterized by ongoing spontaneous pain and pain on motion,20 the DWB system may outperform the conventional methods used to assess stimulus-evoked responses by capturing those clinically relevant guarding behaviors and relief postures during free movements. Moreover, the observation of spontaneous activity in the DWB system rather than stimulus-evoked aversive behaviors may be advantageous. The stressful environment associated with the unpleasant stimuli and laboratory handling may be a confounding factor that complicates the data interpretation with either stress-induced analgesia or hyperalgesia.21,22 Although previous studies have already adopted assessments of spontaneous guarding behaviors using a visual scoring system has already been adopted in previous reports,14,15 DWB is distinct as it affords more objective and quantitative data in a less labor-intensive manner.
The ability to precisely evaluate the pharmacological effects of analgesics using the DWB system in the current study highlights its potential applicability in future studies. One potential application is the preclinical exploration of novel analgesics for postsurgical pain using mouse models. Additionally, given that the DWB system can detect weight distributions among different parts of the body separately, it may be feasible to apply DWB in other clinically relevant surgical pain models (eg, abdominal and thoracic pain models) in addition to the unilateral hind paw surgery models employed in the current study. The application of DWB in persistent postsurgical pain models in mice and the investigating underlying pathophysiological mechanisms warrants further investigation.
Several points should be considered when applying DWB for surgical pain assessment in mice. While the DWB is comparatively easy to perform and accessible for inexperienced experimenters, it is relatively expensive and only allows data acquisition from one mouse per period, making it a costly method with low throughput. Furthermore, DWB results can be misleading when extensive motor deficits are expected in certain pain models (eg, nerve injury model).
The current study has several limitations. First, young adult male mice were used in the current study, as per published protocols.23 Therefore, the effects of gender and age on the DWB-derived outcomes in the current study model remain uncertain. Second, we only tested the analgesic effects of subcutaneously injected diclofenac and buprenorphine as examples of analgesics commonly used worldwide in perioperative clinical settings.24 The ability to capture the effects of weak analgesics, such as diclofenac, indicates the high sensitivity of DWB for evaluating the analgesic potency of target drugs. However, changes in DWB-derived parameters may differ for other types of analgesics (eg, opioids, local anesthetics, and anti-depressants) or delivery routes (eg, intravenous, enteral, and spinal). Third, the current study only tested preemptively administered analgesics in our mouse models, given that preemptive analgesia is a common practice in anesthetic managements for better control of postoperative pain.24–26 However, the ability of DWB to sensitively capture the therapeutic effects of analgesics administered solely after the establishment of postoperative pain remains unclear. Information extracted from DWB analyses in the current study only included the weight loaded on the ipsilateral hind paw and pawprint area on the ipsilateral and contralateral hind paws. Notably, DWB can measure more parameters, such as front/rear weight ratio, different posture durations (eg, rearing and lying on four paws), and the total time spent on each paw throughout the experiment. Further studies addressing these issues may provide the additional value for DWB in postsurgical pain studies in mice.
Conclusion
The present study suggests that DWB is an objective and reliable method for quantifying pain-like behaviors and evaluating the therapeutic effects of analgesics in mouse postsurgical pain models. Thus, the DWB system may serve as a powerful tool with high translational value in the research on postsurgical pain in mice.
Acknowledgments
The authors thank Camilla I. Svensson and the colleagues of the Department of Physiology and Pharmacology, Karolinska Institute, Sweden, for their technical assistance.
Author Contributions
All authors have:
- Provided a significant contribution to this work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas.
- Drafted or written, or substantially revised or critically reviewed this article.
- Agreed on the journal to which this article will be submitted.
- Reviewed and agreed on all versions of this article before submission.
- Agreed to take responsibility and be accountable for the contents of this article.
Funding
This work was supported by JSPS KAKENHI (grant Number 20K17821).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Meara JG, Leather AJ, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Surgery. 2015;158(1):3–6. doi:10.1016/j.surg.2015.04.011
2. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
3. Deuis JR, Dvorakova LS, Vetter I. Methods used to evaluate pain behaviors in rodents. Front Mol Neurosci. 2017;10:284. doi:10.3389/fnmol.2017.00284
4. Griffioen MA, Dernetz VH, Yang GS, Griffith KA, Dorsey SG, Renn CL. Evaluation of dynamic weight bearing for measuring nonevoked inflammatory hyperalgesia in mice. Nurs Res. 2015;64(2):81–87. doi:10.1097/NNR.0000000000000082
5. Quadros AU, Pinto LG, Fonseca MM, Kusuda R, Cunha FQ, Cunha TM. Dynamic weight bearing is an efficient and predictable method for evaluation of arthritic nociception and its pathophysiological mechanisms in mice. Sci Rep. 2015;5(1):14648. doi:10.1038/srep14648
6. Robinson I, Sargent B, Hatcher JP. Use of dynamic weight bearing as a novel end-point for the assessment of Freund’s complete adjuvant induced hypersensitivity in mice. Neurosci Lett. 2012;524(2):107–110. doi:10.1016/j.neulet.2012.07.017
7. Brennan TJ, Vandermeulen EP, Gebhart GF. Characterization of a rat model of incisional pain. Pain. 1996;64(3):493–502. doi:10.1016/0304-3959(95)01441-1
8. Banik RK, Woo YC, Park SS, Brennan TJ. Strain and sex influence on pain sensitivity after plantar incision in the mouse. Anesthesiology. 2006;105(6):1246–1253. doi:10.1097/00000542-200612000-00025
9. Hiltunen A, Vuorio E, Aro HT. A standardized experimental fracture in the mouse tibia. J Orthop Res. 1993;11(2):305–312. doi:10.1002/jor.1100110219
10. Dixon WJ. Efficient analysis of experimental observations. Annu Rev Pharmacol Toxicol. 1980;20(1):441–462. doi:10.1146/annurev.pa.20.040180.002301
11. Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods. 1994;53(1):55–63. doi:10.1016/0165-0270(94)90144-9
12. Mills C, Leblond D, Joshi S, et al. Estimating efficacy and drug ED50ʹs using von Frey thresholds: impact of weber’s law and log transformation. J Pain. 2012;13(6):519–523. doi:10.1016/j.jpain.2012.02.009
13. Laux-Biehlmann A, Boyken J, Dahllof H, Schmidt N, Zollner TM, Nagel J. Dynamic weight bearing as a non-reflexive method for the measurement of abdominal pain in mice. Eur J Pain. 2016;20(5):742–752. doi:10.1002/ejp.800
14. Xu J, Brennan TJ. Guarding pain and spontaneous activity of nociceptors after skin versus skin plus deep tissue incision. Anesthesiology. 2010;112(1):153–164. doi:10.1097/ALN.0b013e3181c2952e
15. Xu J, Brennan TJ. Comparison of skin incision vs. skin plus deep tissue incision on ongoing pain and spontaneous activity in dorsal horn neurons. Pain. 2009;144(3):329–339. doi:10.1016/j.pain.2009.05.019
16. Oyaizu-Toramaru T, Suhara T, Hayakawa N, et al. Targeting oxygen-sensing prolyl hydroxylase for metformin-associated lactic acidosis treatment. Mol Cell Biol. 2017;37(16). doi:10.1128/MCB.00248-17
17. Brennan TJ. Pathophysiology of postoperative pain. Pain. 2011;152(3 Suppl):S33–S40. doi:10.1016/j.pain.2010.11.005
18. Itoh M, Itou J, Kuwashima U, Okazaki K. Correlation of patient-reported numbness around surgical scars with patient-reported outcome measures and joint awareness after knee replacement: a cohort study. BMC Musculoskelet Disord. 2022;23(1):14. doi:10.1186/s12891-021-04971-6
19. Coombs DM, Djohan R, Knackstedt R, Cakmakoglu C, Schwarz GS. Advances and current concepts in reconstructive surgery for breast cancer. Semin Oncol. 2020;47(4):217–221. doi:10.1053/j.seminoncol.2020.05.007
20. Srikandarajah S, Gilron I. Systematic review of movement-evoked pain versus pain at rest in postsurgical clinical trials and meta-analyses: a fundamental distinction requiring standardized measurement. Pain. 2011;152(8):1734–1739. doi:10.1016/j.pain.2011.02.008
21. Imbe H, Iwai-Liao Y, Senba E. Stress-induced hyperalgesia: animal models and putative mechanisms. Front Biosci. 2006;11:2179–2192. doi:10.2741/1960
22. Ferdousi M, Finn DP. Stress-induced modulation of pain: role of the endogenous opioid system. Prog Brain Res. 2018;239:121–177. doi:10.1016/bs.pbr.2018.07.002
23. Cowie AM, Stucky CL, Mouse A. Model of Postoperative Pain. Bio-Protocol. 2019;9(2). doi:10.21769/BioProtoc.3140
24. Doleman B, Leonardi-Bee J, Heinink TP, et al. Pre-emptive and preventive NSAIDs for postoperative pain in adults undergoing all types of surgery. Cochrane Database Sys Rev. 2021;6(6):Cd012978. doi:10.1002/14651858.CD012978.pub2
25. Campiglia L, Consales G, De Gaudio AR. Pre-emptive analgesia for postoperative pain control: a review. Clin Drug Investig. 2010;30(Suppl 2):15–26. doi:10.2165/1158411-S0-000000000-00000
26. Xu J, Li H, Zheng C, et al. The efficacy of pre-emptive analgesia on pain management in total knee arthroplasty: a mini-review. Arthroplasty. 2019;1(1):10. doi:10.1186/s42836-019-0011-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.