Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Nutritional and Inflammatory Predictors of All-Cause Mortality in COPD Patients with Hypercapnic Respiratory Failure: A Two-Center Prospective Cohort Study
Authors Zhang Z, Liu Y, Shen Z, Zhang K, Gao H, Chen Z, Liu Z
Received 11 August 2025
Accepted for publication 26 November 2025
Published 1 December 2025 Volume 2025:20 Pages 3907—3922
DOI https://doi.org/10.2147/COPD.S559986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vanesa Bellou
Zishu Zhang,1,* Yuexian Liu,2,* Zongbo Shen,3,* Koudong Zhang,4,* Honglan Gao,5 Zhimin Chen,5 Zhongxiang Liu4
1Department of Respiratory and Critical Care Medicine, The People’s Hospital of Xiangshui, Yancheng, 224600, People’s Republic of China; 2Department of Neurology, 920th Hospital of the Joint Logistic Support Force, Kunming, 650032, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, The People’s Hospital of Lincang, Lincang, 677000, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, The Yancheng Clinical College of Xuzhou Medical University, The First People’s Hospital of Yancheng, Yancheng, 224000, People’s Republic of China; 5Department of Clinical Nutrition, The Yancheng Clinical College of Xuzhou Medical University, The First People’s Hospital of Yancheng, Yancheng, 224000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhimin Chen, Department of Clinical Nutrition, The Yancheng Clinical College of Xuzhou Medical University, The First People’s Hospital of Yancheng, Yancheng, 224000, People’s Republic of China, Email [email protected] Zhongxiang Liu, Department of Respiratory and Critical Care Medicine, tHe Yancheng Clinical College of Xuzhou Medical University, The First People’s Hospital of Yancheng, Yancheng, 224000, People’s Republic of China, Email [email protected]
Background: Patients with chronic obstructive pulmonary disease (COPD) complicated by hypercapnic respiratory failure (HRF) often have a poor prognosis. Systemic inflammation and malnutrition are associated with adverse outcomes in COPD, yet the prognostic value of nutritional/inflammatory markers remains underexplored in COPD patients with HRF.
Methods: This prospective two-center cohort study enrolled 582 COPD complicated by HRF patients. Six indices, including Platelet-to-Lymphocyte Ratio (PLR), Neutrophil-to-Lymphocyte Ratio (NLR), Systemic Immune-Inflammation Index (SII), Prognostic Nutritional Index (PNI), Neutrophil Percentage-to-Albumin Ratio (NPAR), and Hemoglobin-Albumin-Lymphocyte-Platelet index (HALP), were calculated from admission biomarkers. Associations with 24-month all-cause mortality were evaluated using restricted cubic splines, Kaplan-Meier analysis, multivariable Cox regression, machine learning (Random Survival Forests, Boruta), threshold effect and subgroup analysis. Predictive performance was assessed via the receiver operating characteristic curve (ROC) analysis.
Results: Over 24 months, 263 patients (45.2%) died. Non-survivors exhibited significantly higher NLR, PLR, SII, and NPAR, but lower PNI and HALP (P < 0.05). Kaplan-Meier analysis and Cox models confirmed that higher PNI (HR=0.72, 95% CI:0.54– 0.96) and HALP (HR=0.55, 95% CI:0.41– 0.74) were negatively correlated with all-cause mortality, while elevated PLR (HR=1.39, 95% CI:1.04– 1.85), NLR (HR=1.39, 95% CI:1.02– 1.88), SII (HR=1.51, 95% CI:1.11– 2.05), and NPAR (HR=1.46, 95% CI:1.10– 1.95) were positively correlated with all-cause mortality. For each one-standard-deviation increase in the indicators, all-cause mortality statistically significantly increased or decreased (P for trend < 0.05), with the exception of SII. Machine learning and ROC analyses consistently identified HALP, PNI, and NPAR as top predictors, with HALP demonstrating the highest importance. Subgroup analyses confirmed consistent prognostic utility for PNI, HALP, and NPAR.
Conclusion: PNI, HALP, and NPAR are promising, readily available predictors of all-cause mortality in COPD patients with HRF, potentially enhancing risk stratification and personalized management.
Keywords: inflammation, nutrition, COPD, all-cause mortality, hypercapnic respiratory failure
Introduction
Chronic Obstructive Pulmonary Disease (COPD) remains a highly prevalent chronic respiratory disorder worldwide. As the third leading cause of mortality globally, COPD is responsible for approximately 3 million deaths annually.1 This disease is characterized by persistent respiratory symptoms and airflow limitation, resulting from abnormalities in the airways and alveoli.2 Among COPD patients, the development of hypercapnic respiratory failure (HRF) represents a particularly severe and life-threatening complication.3 HRF is defined by elevated arterial carbon dioxide levels accompanied by hypoxemia.4 It frequently occurs during acute exacerbations and end-stage disease, leading to increased hospitalization rates, healthcare resource utilization, and mortality.5–7 Despite advances in therapeutic strategies, the prognosis for COPD patients with HRF remains poor. This underscores the critical need for reliable prognostic markers to predict clinical outcomes and guide personalized treatment approaches.
Emerging research indicates that systemic inflammation and nutritional status significantly influence disease progression and adverse clinical outcomes in COPD.8,9 In COPD patients, inflammation extends beyond the lungs, involving a persistent systemic inflammatory response. This response is characterized by elevated circulating inflammatory markers, including C-reactive protein and cytokines which correlate strongly with accelerated lung function decline and increased exacerbation frequency.10,11 Concurrently, malnutrition and altered body composition, commonly observed in COPD, exacerbate respiratory muscle weakness and compromise immune responses.12 These impairments heighten the risk of lung function decline and mortality.13,14 Thus, assessing inflammatory and nutritional status may provide critical prognostic insights.
Composite indices derived from routine laboratory parameters, including nutritional and inflammatory markers, have emerged as promising tools for risk stratification in various chronic diseases, such as cancer and COPD.15,16 Indices such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and the combined nutritional and inflammatory indices hemoglobin-albumin-lymphocyte-platelet index (HALP) and neutrophil percentage-to-albumin ratio (NPAR) have been employed to predict outcomes in COPD patients.17–19 In a retrospective analysis of 793 patients hospitalized for acute exacerbation of COPD, Akbay et al found that a lower HALP level was significantly associated with an increased risk of in-hospital mortality (OR 0.758, 95% CI: 0.586–0.980, P = 0.034).18 However, their predictive value specifically for COPD patients with HRF remains inadequately explored. Understanding the prognostic utility of these indices within this high-risk subgroup may facilitate the early identification of patients most likely to experience adverse outcomes.
In this prospective two-center cohort study, we sought to evaluate the associations between six nutritional and inflammatory indices (PLR, NLR, HALP, NPAR, systemic immune-inflammation index (SII), and prognostic nutritional index (PNI)) and all-cause mortality in patients with COPD complicated by HRF. During a 24-month follow-up period, we assessed the predictive performance of these indices for all-cause mortality in this patient population. Furthermore, we employed comprehensive statistical approaches, including restricted cubic splines, survival analysis, Cox proportional hazards models, machine learning algorithms (Random Survival Forests and Boruta feature selection) and the receiver operating characteristic curve (ROC) analysis, to rigorously compare the indices and determine their relative prognostic importance. By establishing the prognostic value of these readily available indicators, this work aims to provide clinicians with practical tools for early risk stratification and personalized management of COPD patients facing this critical complication of HRF.
Materials and Methods
Research Subjects
We enrolled participants with chronic obstructive pulmonary disease (COPD) complicated by hypercapnic respiratory failure (HRF) from two centers. The first cohort was recruited from the Department of Respiratory and Critical Care Medicine and the Intensive Care Unit (ICU) at The First People’s Hospital of Yancheng between October 2020 and September 2021. The second cohort was recruited from the corresponding department and ICU at Jiangsu Provincial People’s Hospital from October 2021 to November 2021. Inclusion criteria comprised: (1) according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy, a post-bronchodilator FEV1/FVC < 0.7 as the diagnostic criteria for COPD;2 (2) HRF diagnosis confirmed by arterial oxygen tension (PaO2) < 8.0 kPa (60 mmHg) and arterial carbon dioxide tension (PaCO2) > 6.0 kPa (45 mmHg); and (3) age ≥ 18 years. Exclusion criteria were as follows: (1) age < 18 years; (2) death prior to data collection; (3) inability to provide informed consent due to conditions such as hearing/speech impairment, tracheostomy status, or cognitive impairment; (4) conditions potentially confounding values of nutritional or inflammatory indicators, including trauma, malignant tumors, hematological malignancies, or pregnancy; and (5) incomplete clinical records.
Data Collection
Within 24 hours of admission, we collected demographic data, comorbidities, and laboratory parameters. Demographic variables included age, sex, body mass index (BMI), and smoking status. Comorbidities assessed were hypertension, diabetes, cerebrovascular disease, cardiovascular disease, asthma, interstitial lung disease (ILD), bronchiectasis, and pneumonia. Laboratory data obtained within 24 hours of admission comprised arterial blood gas analysis (including pH, PaO2, and PaCO2), neutrophil percentage, hemoglobin, albumin, D-dimer, and lymphocyte percentage etc.
The following formulas were used to calculate nutritional and inflammatory indices: Platelet-to-lymphocyte ratio (PLR) = platelet count (109/L) / lymphocyte count (109/L); Neutrophil-to-lymphocyte ratio (NLR) = neutrophil count / lymphocyte count (109/L); Systemic immune-inflammation index (SII) = platelet count (109/L) × neutrophil count (109/L) / lymphocyte count (109/L); Prognostic nutritional index (PNI) = albumin (g/L) + 5 × lymphocyte count (109/L); Neutrophil percentage-to-albumin ratio (NPAR) = neutrophil percentage × 1000 / albumin (g/L); Hemoglobin, albumin, lymphocyte, platelet index (HALP) = hemoglobin (g/L) × albumin (g/L) × lymphocyte count (109/L) / platelet count (109/L).18–20
Outcomes
This prospective cohort study involved patient follow-up via telephone interviews for 24 months post-discharge. The primary outcome was 24-month all-cause mortality. Secondary outcomes included all-cause mortality at 3, 6, and 12 months.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation (SD) or median and interquartile range (IQR), while categorical variables are presented as counts and percentages (%). Group comparisons were performed using Student’s t-test or Mann–Whitney U-test for continuous variables, and chi-square tests for categorical variables. Associations between nutritional/inflammatory indicators and all-cause mortality were analyzed using restricted cubic splines (RCS) and multivariate Cox proportional hazards models. The proportional hazards assumption was confirmed by Schoenfeld residual plots. Patients were stratified by the median values of the indicators and survival analysis was performed using the Kaplan-Meier method. The group differences were compared with the Log rank test. Random Survival Forests (RSF) and Boruta feature selection were employed to evaluate indicator importance. Predictive performance was compared using the receiver operating characteristic curve (ROC) analyses. Threshold effect analysis was employed to further evaluate the association between the optimal indicator HALP and all-cause mortality. Subgroup analyses further explored indicator-mortality associations across strata. All analyses were conducted in R (version 4.4.2), with statistical significance defined as two-sided p < 0.05.
Results
Patient Characteristics
As shown in Figure 1, we enrolled 582 patients with chronic obstructive pulmonary disease (COPD) and hypercapnic respiratory failure (HRF) across two centers. After 24 months of follow-up, the cohort comprised 319 survivors and 263 non-survivors. Comparative data between these groups are presented in Table 1. Compared with survivors, non-survivors were significantly older and exhibited higher levels of bicarbonate, PaCO2, neutrophil percentage, neutrophil count, D-dimer, CK-MB, urea, and NT-proBNP (P < 0.05). Conversely, non-survivors showed significantly lower values for BMI, hemoglobin, albumin, total protein, overall survival, red blood cell count (RBC), lymphocyte percentage, lymphocyte count, cholinesterase, and eGFR (P < 0.05). Notably, non-survivors demonstrated elevated NLR, PLR, SII, and NPAR, alongside lower PNI and HALP values (P < 0.05).
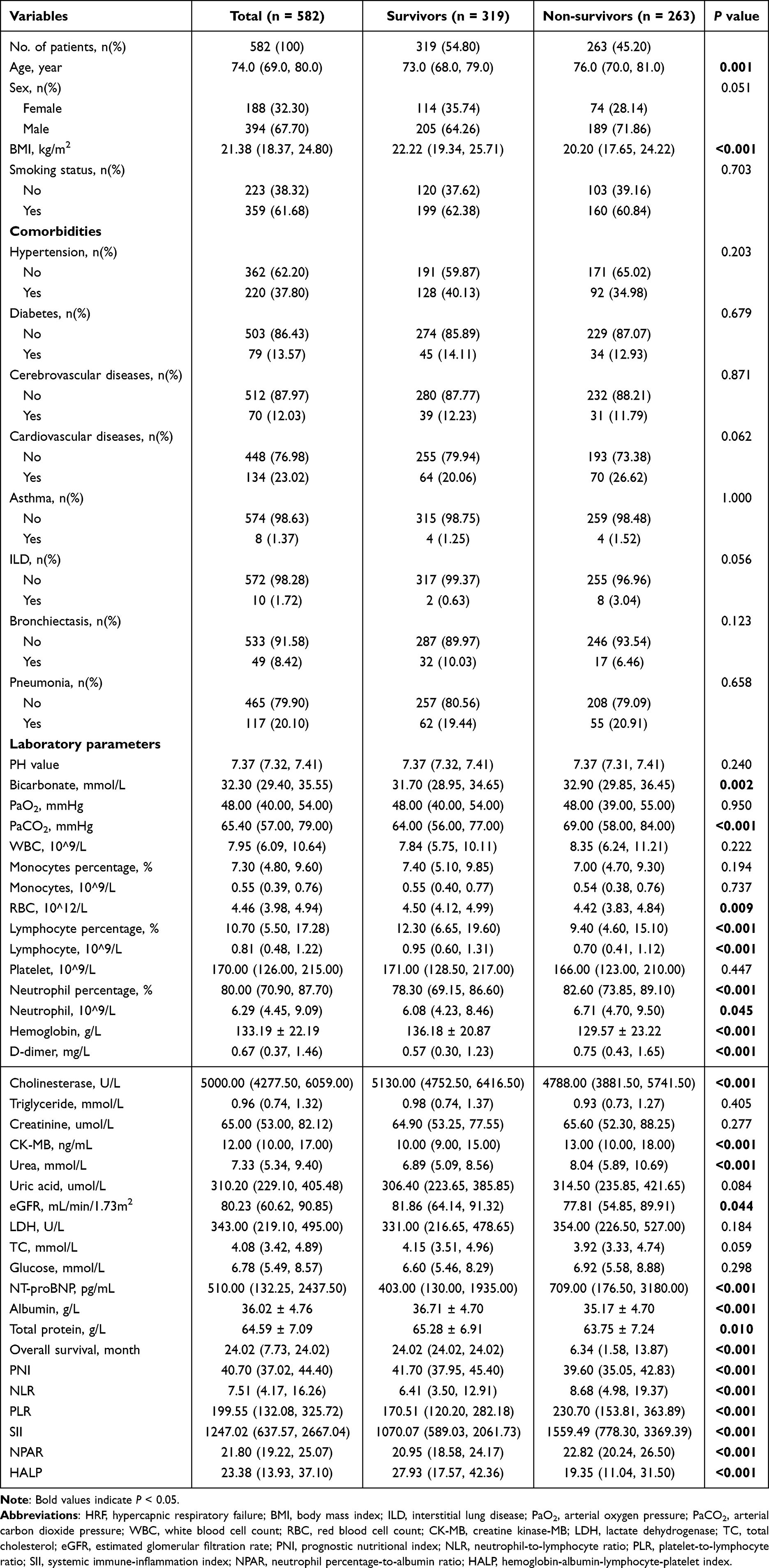 |
Table 1 Baseline Characteristics of Participants in COPD Patients with HRF |
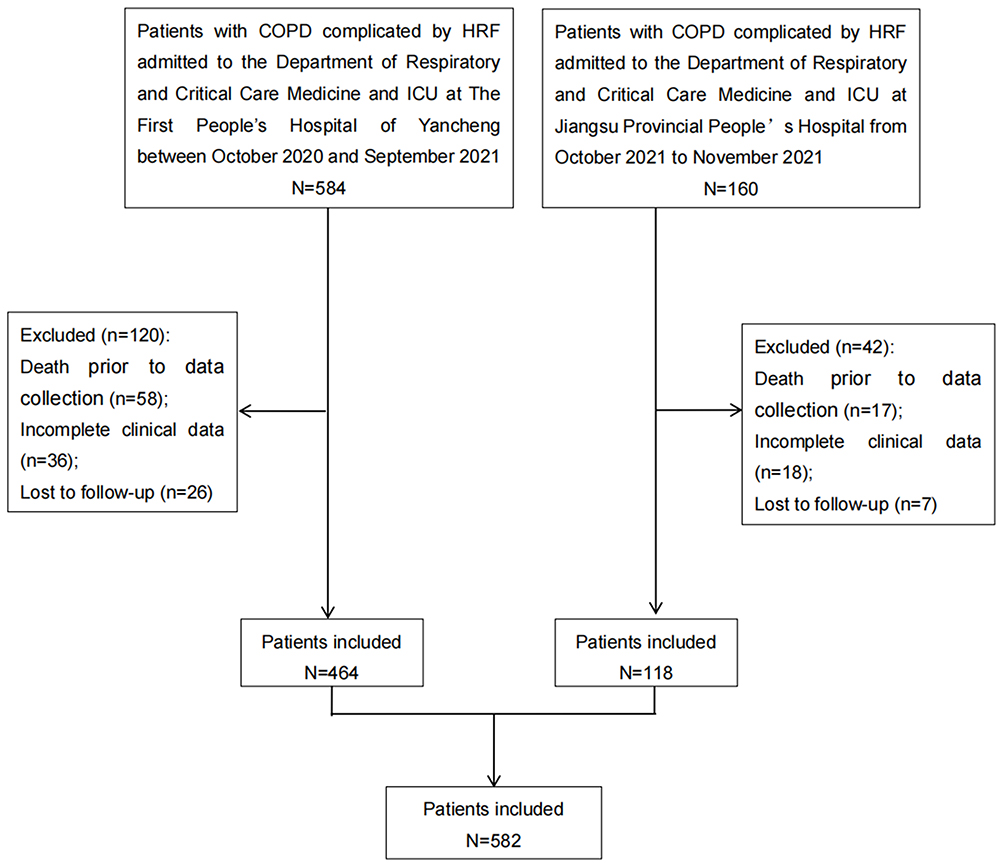 |
Figure 1 The flow diagram of sample selection in the study. |
Relationship Between Nutritional and Inflammatory Indicators and All-Cause Mortality in COPD Patients with HRF
As illustrated in Figure 2, restricted cubic spline (RCS) modeling was employed to evaluate nonlinear relationships between nutritional/inflammatory indicators and all-cause mortality among COPD patients with HRF. Following adjustment for age, sex, BMI, smoking status, hypertension, diabetes, cerebrovascular disease, cardiovascular disease, asthma, interstitial lung disease, bronchiectasia and pneumonia, the RCS analysis demonstrated linear associations of PLR, NPAR, and PNI with all-cause mortality (P for overall association < 0.05; P for nonlinear association > 0.05) (Figure 2A, D and E). Conversely, nonlinear associations were observed between NLR, SII, and HALP and all-cause mortality (P for nonlinear association < 0.05) (Figure 2B, C and F).
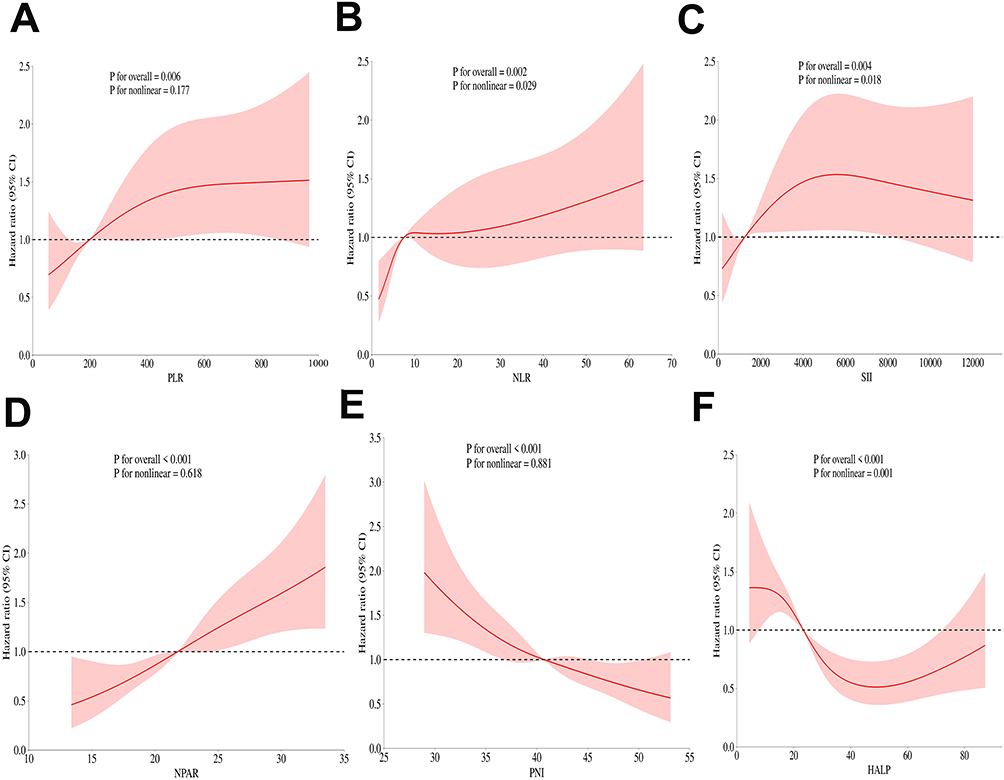 |
Figure 2 Restricted cubic spline curves for analyzing the nonlinear relationships between nutritional/inflammatory indices and all-cause mortality in patients with COPD complicated by HRF (A) PLR; (B) NLR; (C) SII; (D) NPAR; (E) PNI; (F) HALP. Note: Hazard ratios were adjusted for age, sex, BMI, smoking status, hypertension, diabetes, cerebrovascular diseases, cardiovascular diseases, asthma, ILD, bronchiectasis and pneumonia. |
Patients were stratified by median levels of indicators to evaluate cumulative survival rates by Kaplan-Meier survival curves (Figure 3). Among the six nutritional and inflammatory indicators analyzed, all groups dichotomized by median values showed statistically significant differences in 24-month all-cause mortality (log-rank P < 0.001). Furthermore, elevated PLR, NLR, SII, and NPAR levels were positively associated with all-cause mortality (Figure 3A–D), whereas higher PNI and HALP levels were negatively correlated with all-cause mortality (Figure 3E and F).
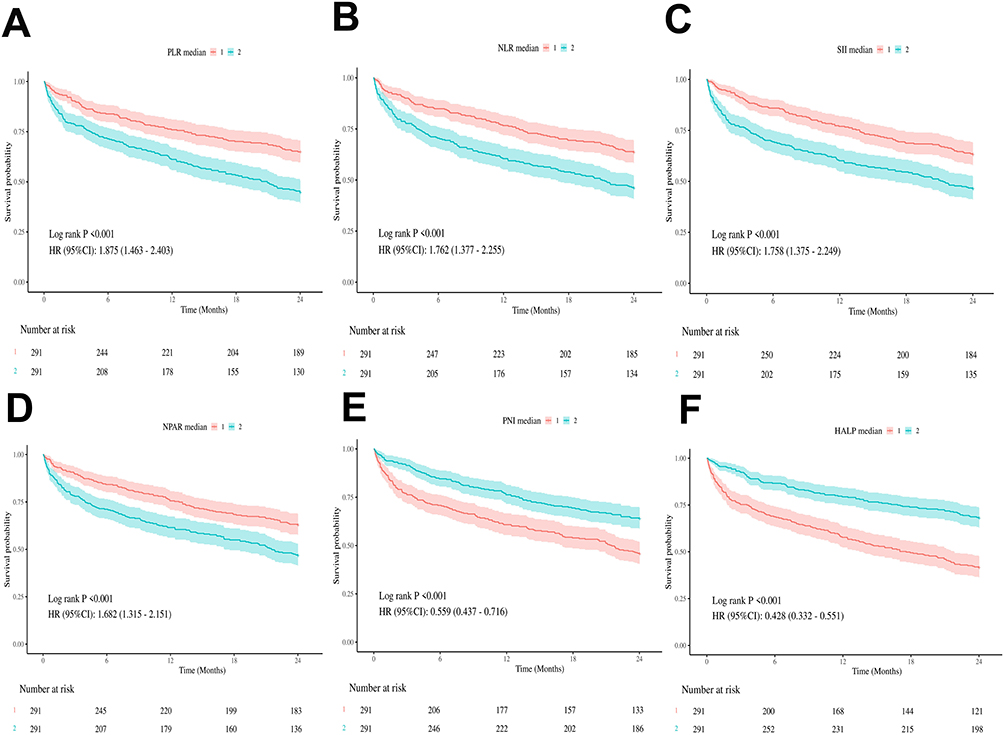 |
Figure 3 Kaplan-Meier curves for evaluating cumulative survival by medians of nutritional/inflammatory indicators (A) PLR; (B) NLR; (C) SII; (D) NPAR; (E) PNI; (F) HALP). |
To further investigate these relationships, three Cox proportional hazards regression models were developed. Table 2 summarizes the hazard ratios (HRs) and 95% confidence intervals (CIs) for each model. After adjusting for age, sex, BMI, smoking status, hypertension, diabetes, cerebrovascular disease, cardiovascular disease, asthma, ILD, bronchiectasis, pneumonia and laboratory parameters (Model 4), PLR, NLR, PNI, HALP and NPAR remained significantly associated with 24-month all-cause mortality. When analyzed as categorical variables (dichotomized by median values), the fully adjusted Model 4 demonstrated that patients with higher PNI and HALP levels had significantly lower all-cause mortality compared to those with low levels, with adjusted HRs (95% CI) of 0.72 (0.54–0.96) and 0.55 (0.41–0.74), respectively. Conversely, elevated PLR, NLR, SII, and NPAR levels were associated with increased mortality risk, yielding HRs (95% CI) of 1.39 (1.04–1.85), 1.39 (1.02–1.88), 1.51 (1.11–2.05), and 1.46 (1.10–1.95). Notably, although the hazard ratios (HRs) for the continuous variables of these indicators were statistically significant, their 95% confidence intervals (CIs) were narrow. For example, the HR for PLR was 1.01 (1.01–1.01). This may limit their clinical applicability. To address this limitation, we further evaluated these biomarkers using a per-one-standard-deviation (per-1-SD) increase approach. For each one-standard-deviation increase in PLR, NLR, PNI, HALP, SII and NPAR, the HRs (95% CI) for mortality were 1.19 (1.04–1.36), 1.22 (1.04–1.43), 0.76 (0.65–0.90), 0.79 (0.67–0.94), 1.13 (0.98–1.31), and 1.34 (1.16–1.55), respectively. This implies that each one-standard-deviation increase in PLR was associated with a 19% increase in mortality risk. Moreover, decreased levels of PNI and HALP, as well as increased levels of PLR, NLR, and NPAR, were significantly associated with a higher risk of all-cause mortality (P for trend < 0.05).
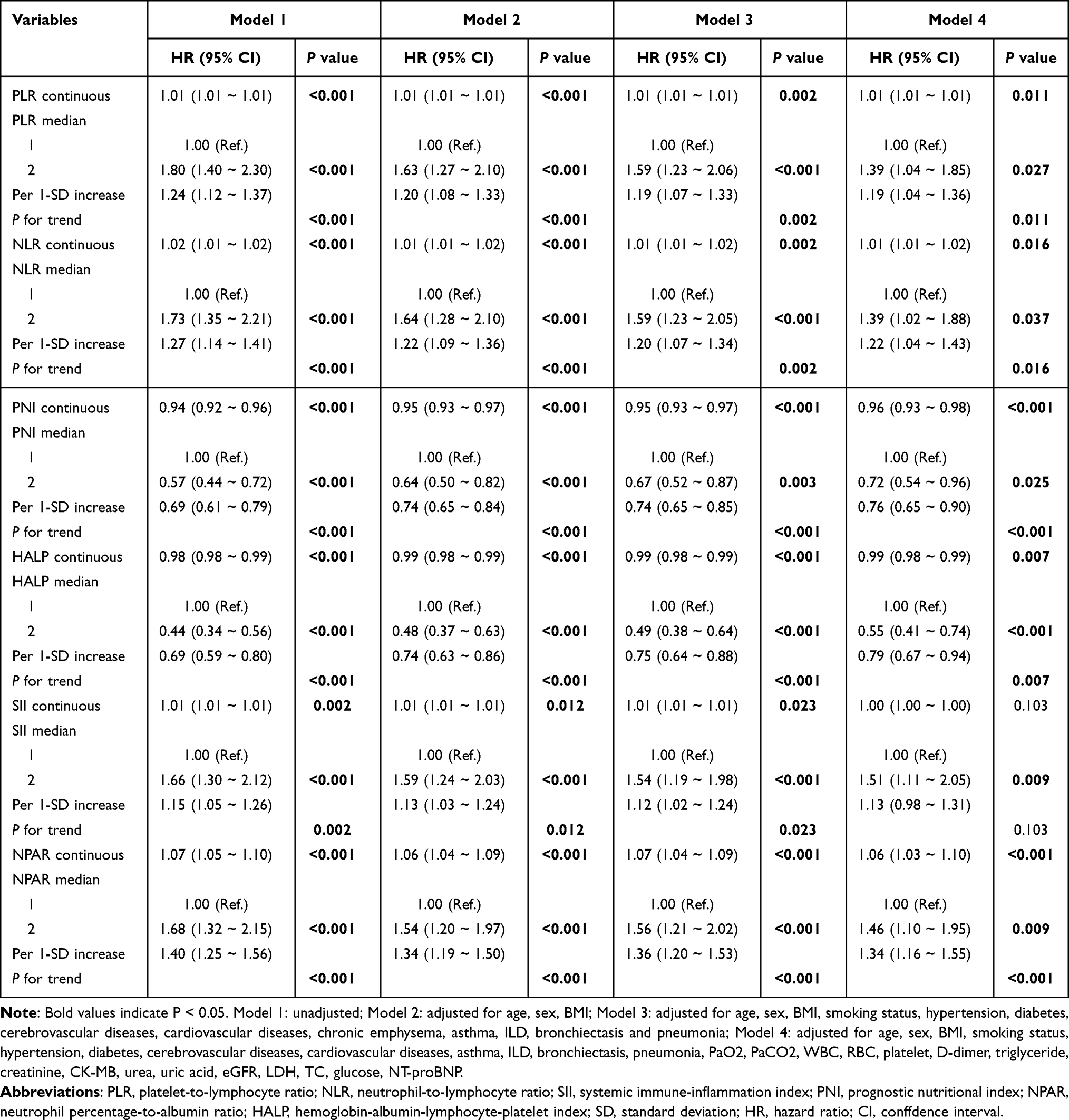 |
Table 2 Multivariate Cox Proportional Hazards Models for the Nutritional/Inflammatory Indicators and All-Cause Mortality |
Predictive Values of Nutritional and Inflammatory Indicators
To further evaluate the clinical significance and predictive performance of the six indicators, we performed Random Survival Forests (RSF), Boruta feature selection, and receiver operating characteristic (ROC) curve analyses. As depicted in Figure 4, both RSF analysis (Figure 4A) and Boruta algorithms (Figure 4B) ranked all variables by their importance for all-cause mortality prediction, with HALP, PNI, and NPAR consistently ranked among the top ten significant predictors. Notably, HALP achieved the highest and second-highest importance rankings in these respective algorithms.
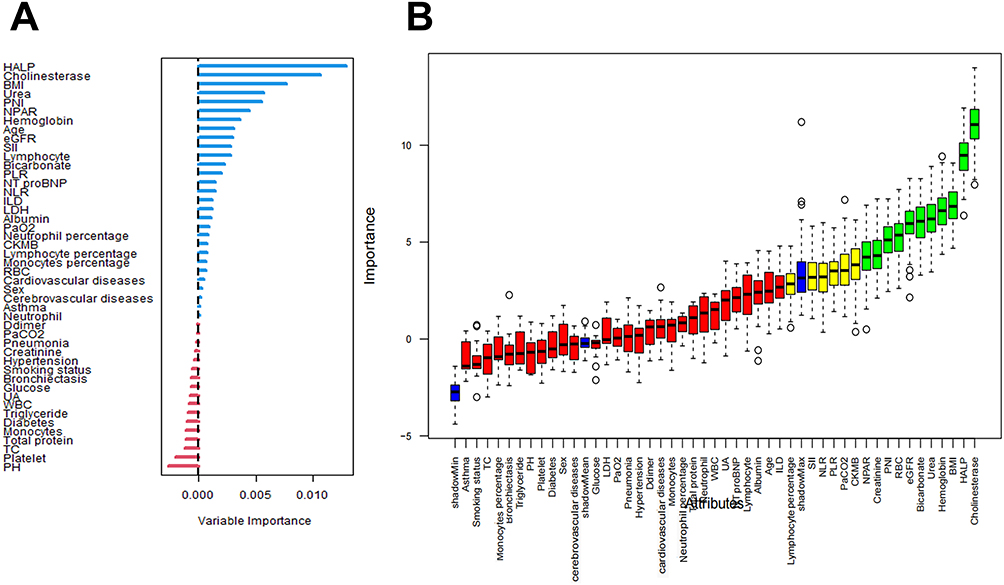 |
Figure 4 Random Survival Forests (RSF) and Boruta feature selection for ranking variable importance (A) RSF analysis; (B) Boruta feature selection). |
ROC curves evaluating indicator performance for predicting 3-, 6-, 12-, and 24-month mortality are presented in Figure 5A–D. Corresponding AUC values (95% CI) and statistical comparisons are detailed in Table 3. Comparisons between HALP and PLR ROC curves showed statistically significant differences across all four time points. PNI, HALP, and NPAR demonstrated superior predictive performance relative to PLR, NLR, and SII at all time points, although these differences were not statistically significant. These findings highlight the clinical utility of PNI, HALP, and NPAR as composite prognostic indicators in COPD patients with HRF.
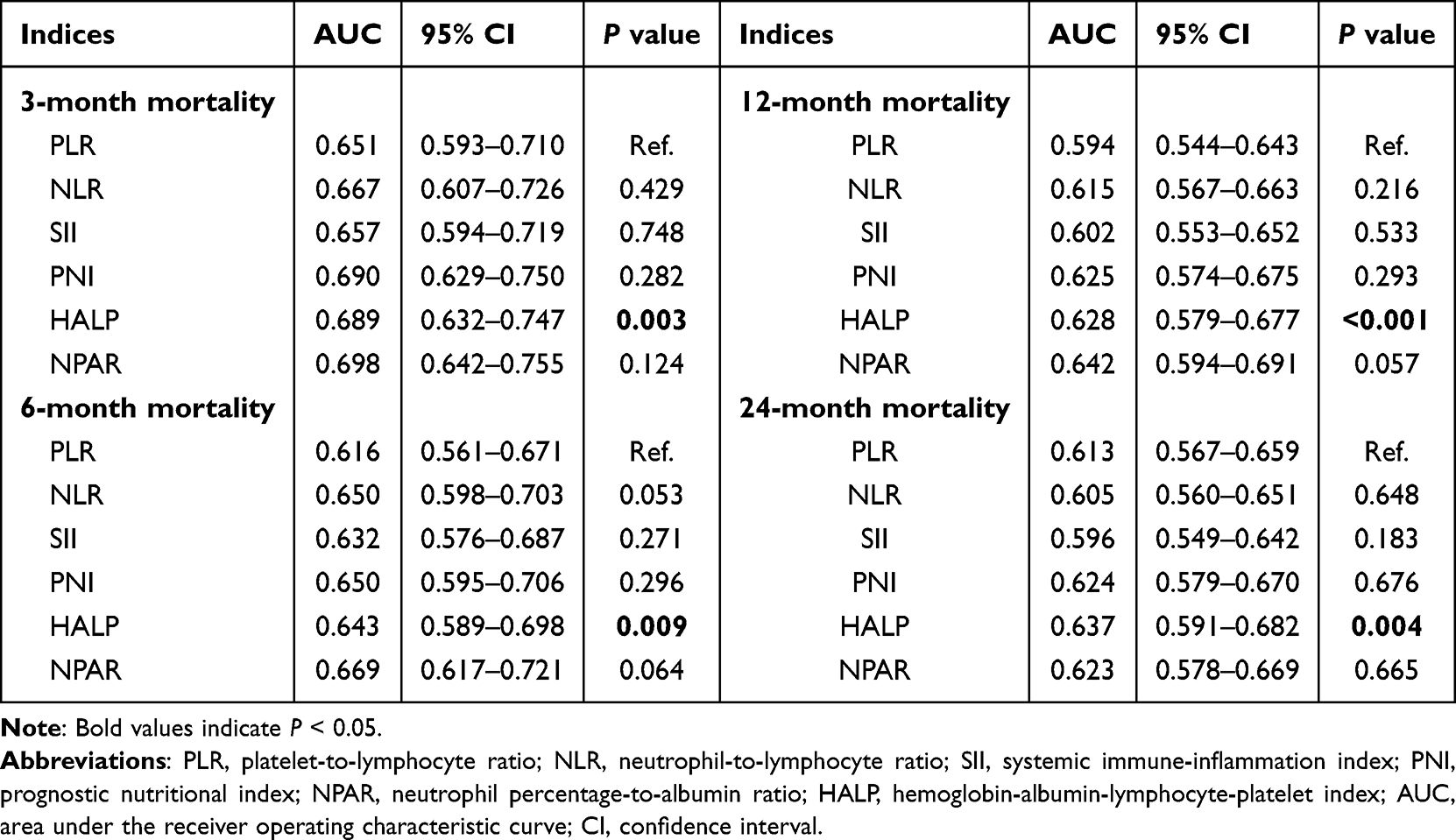 |
Table 3 The AUCs of Nutritional/Inflammatory Indicators for Predicting All-Cause Mortality |
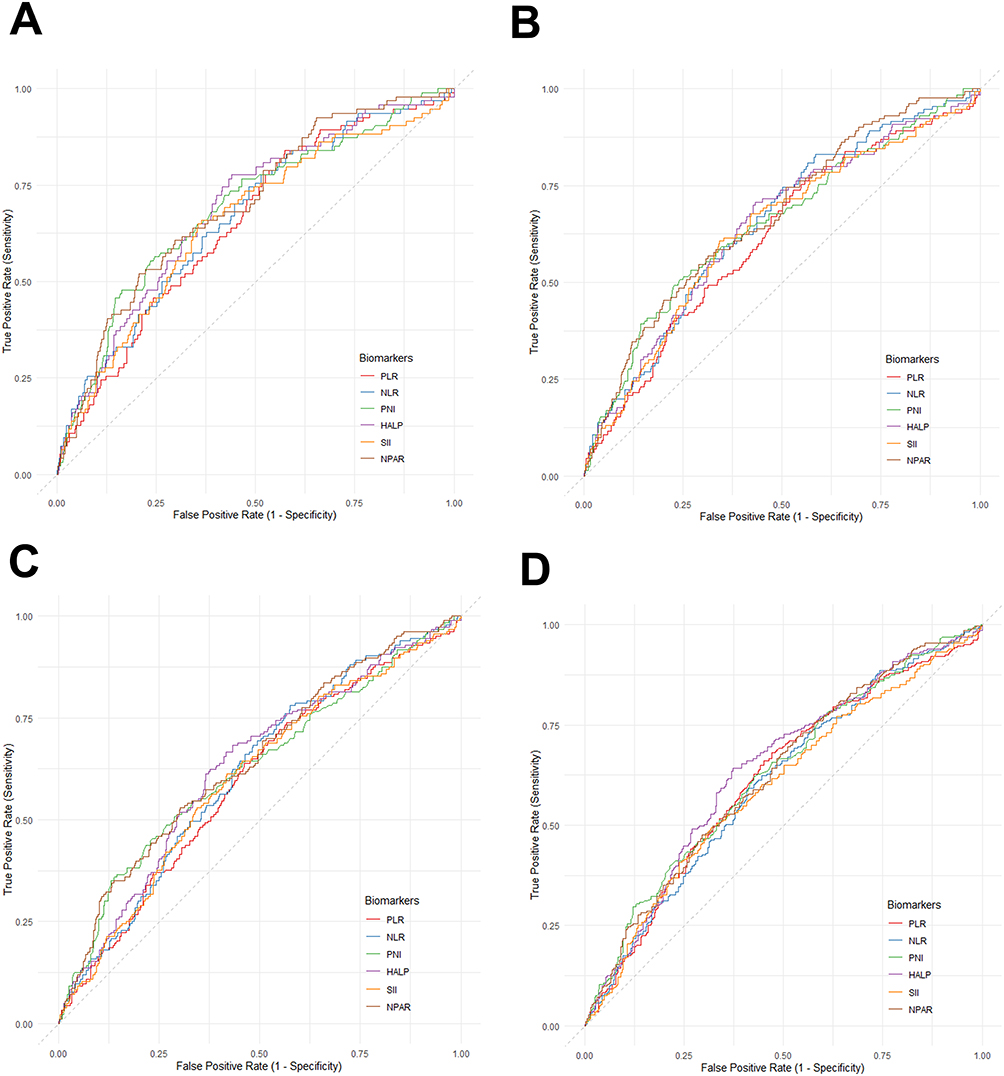 |
Figure 5 The receiver operating characteristic (ROC) curve analyses of nutritional/inflammatory indicators for predicting all-cause mortality. Note: (A) 3-month mortality; (B) 6-month mortality; (C) 12-month mortality; (D) 24-month mortality. |
Based on the above findings, we conducted a threshold effect analysis on the most promising indicator, HALP (Table 4). The results revealed a significant threshold effect between HALP and all-cause mortality in COPD patients complicated with HRF (likelihood ratio test P < 0.001). Overall, HALP was inversely associated with all-cause mortality (HR (95% CI): 0.99 (0.98–0.99), p < 0.001). Specifically, when HALP values were below 70.21, a negative correlation with all-cause mortality was observed. Conversely, when HALP exceeded 70.21, a positive association with all-cause mortality was identified (HR (95% CI): 1.09 (1.01–1.18), P = 0.037).
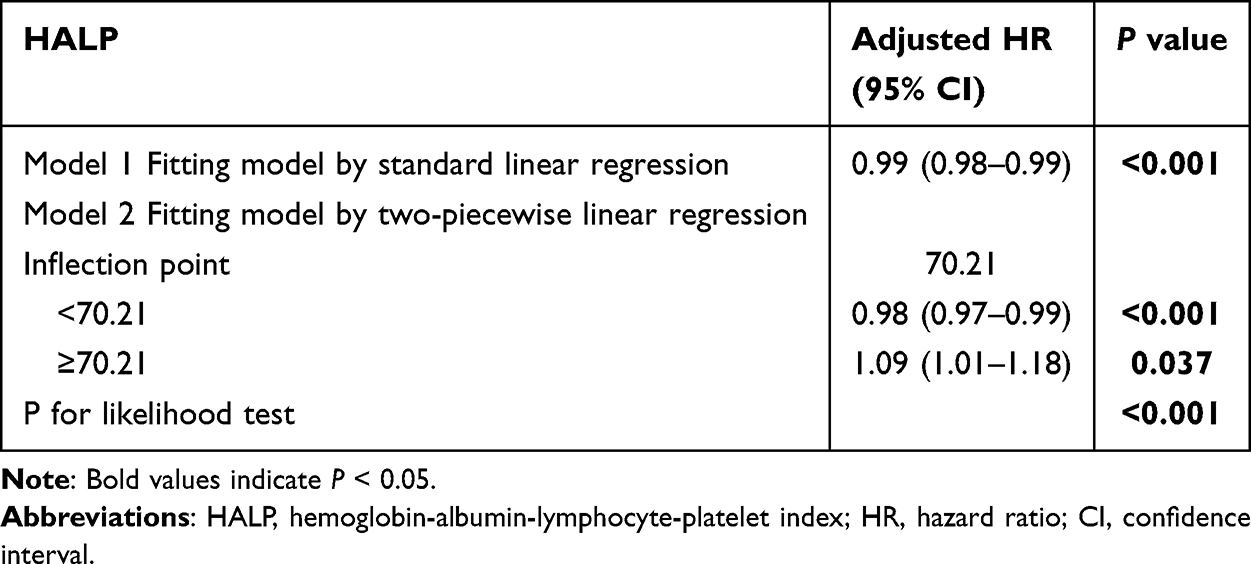 |
Table 4 Threshold Effect Analysis of HALP on COPD with HRF Using a Two-Piecewise Linear Regression Model |
Subgroup Analysis
To validate the consistency of associations between PNI, HALP, NPAR and 24-month all-cause mortality across subgroups of COPD patients with HRF, we performed subgroup analyses. As demonstrated in Figure 6, elevated HALP levels were significantly associated with reduced 24-month mortality risk in most subgroups (P < 0.05). Critically, no significant interaction effects were observed between HALP and most stratification variables (P for interaction > 0.05), indicating the robustness of this relationship across diverse patient profiles. Subgroup analyses for PNI and NPAR yielded comparable findings to HALP (Figures S1 and S2). Collectively, these findings reinforce the independent prognostic value of PNI, HALP, and NPAR in COPD patients with HRF.
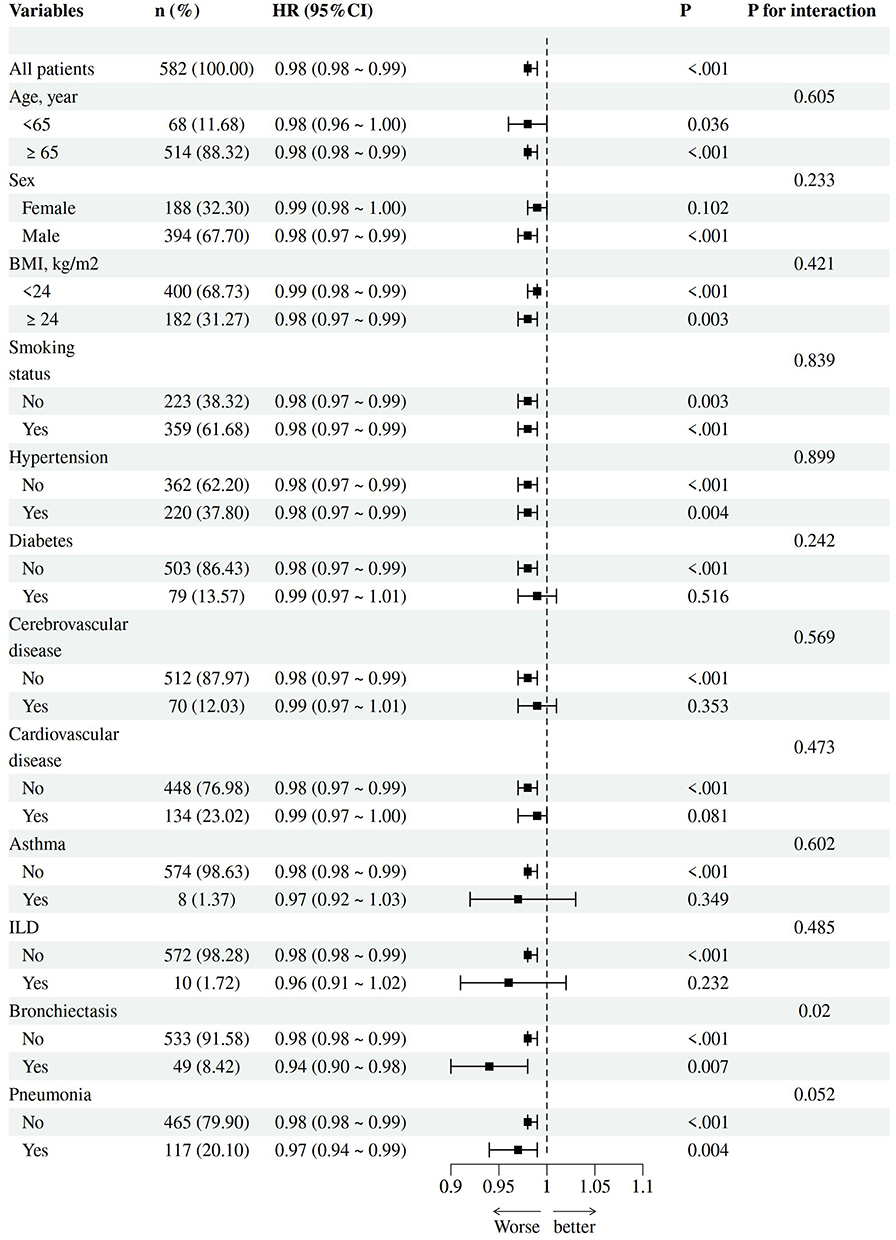 |
Figure 6 Subgroup analysis of the association between HALP and all-cause mortality. |
Discussion
This two-center prospective cohort study evaluated the prognostic significance of six nutritional and inflammatory indices (PLR, NLR, SII, PNI, NPAR, and HALP) in chronic obstructive pulmonary disease (COPD) patients with hypercapnic respiratory failure (HRF). Patients with COPD and HRF represent a particularly vulnerable population. HRF typically occurs during acute exacerbations or advanced stages of COPD, significantly increasing morbidity and mortality.21 Over a 24-month follow-up period encompassing 582 patients, we observed a mortality rate of 45.2% (263 deaths) among COPD patients with HRF. This high mortality underscores the critical need for effective prognostic tools in this high-risk group. Our study significantly advances the understanding of risk stratification in COPD with HRF by rigorously validating, using both statistical and machine learning methods, that specific indices reflecting nutrition and inflammation (HALP, PNI, and NPAR) demonstrate superior prognostic utility compared to more established inflammatory markers such as NLR, PLR, and SII. Systemic inflammation has long been implicated in the pathogenesis and progression of COPD.22 Sustained inflammatory responses may contribute to COPD exacerbations, reduced quality of life, and accelerated disease progression.22 Within this inflammatory milieu, both neutrophils and lymphocytes play significant roles.23 Established inflammatory markers such as the Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Systemic Immune-Inflammation Index (SII) reflect this inflammatory environment and have been associated with adverse COPD outcomes in prior studies.24 For instance, a retrospective observational study of 16,849 patients with acute exacerbations of COPD (AECOPD) identified NLR and PLR as independent risk factors for frequent exacerbations.25 Similarly, a retrospective cohort study utilizing the MIMIC-IV database demonstrated that elevated SII levels increased risks for respiratory failure (HR 1.19, 95% CI 1.12–1.28; P<0.001), in-hospital mortality (HR 1.22, 95% CI 1.07–1.39; P=0.003), and long-term mortality (HR 1.12, 95% CI 1.05–1.19; P<0.001) in COPD patients.26 Consistent with previous research, our findings confirm NLR, PLR, and SII as independent predictors of all-cause mortality in COPD patients with HRF. However, their predictive performance was surpassed by nutritional and inflammatory composite indices (HALP, PNI, and NPAR).
Malnutrition is prevalent in advanced COPD and is exacerbated by HRF. This nutritional impairment further intensifies disease severity by compromising respiratory muscle function and diminishing immune defense efficacy.12,27,28 Albumin serves as a critical common component in the Prognostic Nutritional Index (PNI), the Hemoglobin, Albumin, Lymphocyte, and Platelet index (HALP), and the Neutrophil Percentage-to-Albumin Ratio (NPAR). Inflammation and malnutrition can lower albumin concentrations through increased catabolism or reduced synthesis rates.29 Consequently, albumin levels simultaneously reflect nutritional reserves and inflammatory burden.30,31 Lymphocytes, integral to both HALP and PNI, decrease in number during immune exhaustion and impaired host defense, increasing susceptibility to infections and contributing to disease progression.32 Our study revealed that non-survivors exhibited significantly lower levels of albumin, hemoglobin, and lymphocytes, alongside markedly higher neutrophil percentages and counts (Table 1), indicative of a state characterized by heightened inflammation and compromised nutrition. Furthermore, COPD patients with HRF exhibiting higher PNI and HALP levels in this study demonstrated a lower mortality risk. Conversely, patients with elevated NPAR faced an increased mortality risk. These findings align with the predictive outcomes for COPD reported for these indices in prior studies.33–36
Notably, both the Random Survival Forest and Boruta feature selection methods consistently identified HALP, PNI, and NPAR as top predictors of mortality, with HALP demonstrating the highest importance. This prominence may stem from HALP’s unique capacity to concurrently capture nutritional depletion (via albumin and hemoglobin) and inflammatory dysregulation (via lymphocytes), offering a more comprehensive assessment of the patient’s pathophysiological state. Studies indicate that low hemoglobin concentrations are common in patients experiencing acute exacerbations of COPD and predict long-term mortality.37 Declining hemoglobin levels correlate with worsening nutritional status and systemic inflammation, leading to impaired quality of life, reduced survival rates, and an increased likelihood of hospitalization.38,39 Thus, the inclusion of hemoglobin likely underpins HALP’s superior predictive importance.
Interestingly, the threshold effect analysis for HALP revealed that it served as a protective factor when HALP was below 70.21, but became a risk factor when HALP exceeded this value. This phenomenon may be attributed to one of the components of HALP not yet discussed-platelet count. When the platelet count is sufficiently low, HALP levels increase, leading to a higher risk of all-cause mortality in COPD patients with HRF. This finding is consistent with a study of 472 patients admitted to the ICU for AECOPD, which reported higher mortality among those with comorbid thrombocytopenia.40 A potential explanation may be related to the significant downregulation of genes associated with platelet activation and wound healing in COPD patients, which could further impede the repair processes of lung tissue.41
Receiver operating characteristic (ROC) curve analysis confirmed the superior performance of PNI, HALP, and NPAR in predicting mortality at 3, 6, 12, and 24 months post-discharge. Although their predictive advantage over indices solely incorporating inflammatory markers did not reach statistical significance, HALP demonstrated statistically significant outperformance of PLR across all four time points. These findings underscore the enhanced prognostic accuracy achievable through composite indices integrating both nutritional and inflammatory parameters. Another noteworthy observation from our study is that the AUC values of the nutrition/inflammation indices exhibited a declining trend as the follow-up duration increased from 3 to 24 months. This pattern suggests that over longer periods, such as 24 months, mortality may be influenced by a broader array of factors not fully captured by baseline biomarkers, such as the development of new comorbidities, overall frailty status, and socioeconomic conditions. Although these indices remain important long-term predictors, their discriminative performance slightly diminishes over time, highlighting the potential need for dynamic reassessment of risk factors in the long-term management of these patients.
Importantly, subgroup analyses demonstrated the consistent prognostic utility of PNI, HALP, and NPAR across diverse patient populations stratified by demographic and clinical characteristics. No significant interactions were detected, suggesting these markers may be broadly applicable for risk stratification regardless of comorbidities or baseline differences. This generalizability positions them as practical candidates for guiding individualized management strategies.
Our study benefits from several strengths, including a prospective design, a relatively large sample size across two centers, a comprehensive analytical approach integrating conventional survival models with machine learning methodologies, and an extended 24-month follow-up period. These features enhance the reliability and clinical relevance of our findings. However, several limitations warrant consideration. First, the observational nature of the study precludes definitive causal inferences. Although we carefully adjusted for potential confounders using multivariable analysis, residual confounding by unmeasured factors (e.g, detailed medication history, socioeconomic status, or physical activity levels) may persist. Second, indicator measurements were limited to values obtained at hospital admission; consequently, the prognostic significance of their dynamic changes remains unexplored. Third, validation across diverse ethnic populations and healthcare settings is essential to confirm generalizability. Fourth, since all-cause mortality served as our primary endpoint, we were unable to determine whether the prognostic utility of these indicators is more strongly associated with COPD-specific progression or with a generalized frail state. Future research should focus on validating these findings in external cohorts, integrating these indices with other indicators to predict a broader range of clinical outcomes, investigating the impact of interventions guided by these indices (such as nutritional supplementation and anti-inflammatory strategies), and elucidating the underlying molecular mechanisms linking these composite indicators to mortality.
Conclusions
In summary, this two-center prospective cohort study validated six nutritional and inflammatory indices (PLR, NLR, SII, PNI, NPAR, and HALP) as independently associated with all-cause mortality in patients with COPD accompanied by HRF. Compared to inflammatory indices (NLR, PLR, and SII), these combined nutritional and inflammatory indices (PNI, NPAR, and HALP), especially HALP, represent more promising predictors of all-cause mortality in COPD patients with HRF, potentially enhancing risk stratification and personalized management. Our findings underscore the critical importance of assessing both nutritional and inflammatory status in COPD patients with HRF. Future research should validate these findings in external cohorts and integrate them with clinical assessments.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Ethics Committees of the First People’s Hospital of Yancheng (Approval Number: 2020-K062) and the People’s Hospital of Jiangsu Province (No. 2021-SR-346). Informed consent was obtained from all participants or their legal guardians prior to data collection.
Acknowledgments
We express our gratitude to all the participants who actively contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
3. MacIntyre NR. Acute hypercapnic respiratory failure in COPD. Respir Care. 2023;68(7):973–982. doi:10.4187/respcare.10560
4. Vykopal M, Mizera J, Jakubec P, Genzor S, Pobeha P. Hypercapnic respiratory failure - review. Hyperkapnické respirační selhání. Cas Lek Cesk. 2023;162(1):13–18.
5. Grünewaldt A, Fritsch N, Rohde G. Hypercapnic failure in acute exacerbated COPD patients: severe airflow limitation as an early warning signal. J Clin Med. 2022;12(1):258. doi:10.3390/jcm12010258
6. Adler D, Cavalot G, Brochard L. Comorbidities and readmissions in survivors of acute hypercapnic respiratory failure. Semin Respir Crit Care Med. 2020;41(6):806–816. doi:10.1055/s-0040-1710074
7. Trethewey SP, Edgar RG, Morlet J, Mukherjee R, Turner AM. Late presentation of acute hypercapnic respiratory failure carries a high mortality risk in COPD patients treated with ward-based NIV. Respir Med. 2019;151:128–132. doi:10.1016/j.rmed.2019.04.013
8. Laveneziana P, Palange P; ERS Research Seminar Faculty. Physical activity, nutritional status and systemic inflammation in COPD. Eur Respir J. 2012;40(3):522–529. doi:10.1183/09031936.00041212
9. Yao J, Wu P, Li Z, et al. Nutritional status and systemic inflammation in COPD: prognostic value of the advanced lung cancer inflammation index. Front Nutr. 2025;12:1550490. doi:10.3389/fnut.2025.1550490
10. Paone G, Leone V, Conti V, et al. Blood and sputum biomarkers in COPD and asthma: a review. Eur Rev Med Pharmacol Sci. 2016;20(4):698–708.
11. Ramya PA, Mohapatra MM, Saka VK, Kar R, Chakkalakkoombil SV, Vemuri MB. Haematological and inflammatory biomarkers among stable COPD and acute exacerbations of COPD patients. Sultan Qaboos Univ Med J. 2023;23(2):239–244. doi:10.18295/squmj.12.2022.062
12. Herzog R, Cunningham-Rundles S. Immunologic impact of nutrient depletion in chronic obstructive pulmonary disease. Curr Drug Targets. 2011;12(4):489–500. doi:10.2174/138945011794751500
13. Fekete M, Fazekas-Pongor V, Balazs P, et al. Effect of malnutrition and body composition on the quality of life of COPD patients. Physiol Int. 2021;108:238–250. doi:10.1556/2060.2021.00170
14. Keogh E, Mark Williams E. Managing malnutrition in COPD: a review. Respir Med. 2021;176:106248. doi:10.1016/j.rmed.2020.106248
15. Ding P, Yang J, Wu J, et al. Combined systemic inflammatory immune index and prognostic nutrition index as chemosensitivity and prognostic markers for locally advanced gastric cancer receiving neoadjuvant chemotherapy: a retrospective study. BMC Cancer. 2024;24(1):1014. doi:10.1186/s12885-024-12771-z
16. Du D, Zhang G, Xu D, et al. Association between systemic inflammatory markers and chronic obstructive pulmonary disease: a population-based study. Heliyon. 2024;10(10):e31524. doi:10.1016/j.heliyon.2024.e31524
17. Wang N, Wang G, Li M, et al. Construction and comparison of multiple serum-based prognostic models for predicting the prognosis of acute exacerbations of chronic obstructive pulmonary disease. J Inflamm Res. 2024;17:8395–8406. doi:10.2147/JIR.S461961
18. Akbay MO, Ernam D, Sertcelik L, Ozbaki F. Hemoglobin-albumin-lymphocyte-platelet index and risk of in-hospital mortality in 793 adult patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. Med Sci Monit. 2025;31:e947098. doi:10.12659/MSM.947098
19. Shi Y, Shi Y, Liu Y, Wang C, Qi M, Li C. Association between neutrophil percentage to serum albumin ratio and in-hospital mortality of patients with chronic obstructive pulmonary disease in intensive care unit: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2025;20:1227–1237. doi:10.2147/COPD.S508964
20. Fullerton R, Martell K, Khanolkar R, et al. Impact of immune, inflammatory and nutritional indices on outcome in patients with locally advanced cervical cancer treated with definitive (chemo)radiotherapy. Gynecol Oncol. 2024;190:291–297. doi:10.1016/j.ygyno.2024.09.005
21. Meservey AJ, Burton MC, Priest J, Teneback CC, Dixon AE. Risk of readmission and mortality following hospitalization with hypercapnic respiratory failure. Lung. 2020;198(1):121–134. doi:10.1007/s00408-019-00300-w
22. Ritchie AI, Wedzicha JA. Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
23. Xu J, Zeng Q, Li S, Su Q, Fan H. Inflammation mechanism and research progress of COPD. Front Immunol. 2024;15:1404615. doi:10.3389/fimmu.2024.1404615
24. Zinellu A, Zinellu E, Mangoni AA, et al. Clinical significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute exacerbations of COPD: present and future. Eur Respir Rev. 2022;31(166):220095. doi:10.1183/16000617.0095-2022
25. Fu Y, Wang Y, Wang Y, et al. Biomarkers (NLR, PLR, SII) for frequent COPD exacerbations: diagnostic and clinical management implications in a retrospective study. Int J Chron Obstruct Pulmon Dis. 2025;20:987–998. doi:10.2147/COPD.S510118
26. Zhang Y, Tan X, Hu S, Cui Z, Chen W. Relationship between systemic immune-inflammation index and risk of respiratory failure and death in COPD: a retrospective cohort study based on the MIMIC-IV database. Int J Chron Obstruct Pulmon Dis. 2024;19:459–473. doi:10.2147/COPD.S446364
27. Gea J, Pascual S, Casadevall C, Orozco-Levi M, Barreiro E. Muscle dysfunction in chronic obstructive pulmonary disease: update on causes and biological findings. J Thorac Dis. 2015;7(10):E418–E438. doi:10.3978/j.issn.2072-1439.2015.08.04
28. Girón R, Matesanz C, García-Río F, et al. Nutritional state during COPD exacerbation: clinical and prognostic implications. Ann Nutr Metab. 2009;54(1):52–58. doi:10.1159/000205960
29. Don BR, Kaysen GSA. relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
30. Almasaudi AS, Dolan RD, Edwards CA, McMillan DC. Hypoalbuminemia reflects nutritional risk, body composition and systemic inflammation and is independently associated with survival in patients with colorectal cancer. Cancers. 2020;12(7):1986. doi:10.3390/cancers12071986
31. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
32. Rodrigues SO, Cunha CMCD, Soares GMV, Silva PL, Silva AR, Gonçalves-de-Albuquerque CF. Mechanisms, pathophysiology and currently proposed treatments of chronic obstructive pulmonary disease. Pharmaceuticals. 2021;14(10):979. doi:10.3390/ph14100979
33. Zhou Z, Wang Y, Wang Y, et al. A diagnostic nomogram for predicting hypercapnic respiratory failure in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2024;19:1079–1091. doi:10.2147/COPD.S454558
34. Cao K, Miao X, Chen X. Association of inflammation and nutrition-based indicators with chronic obstructive pulmonary disease and mortality. J Health Popul Nutr. 2024;43(1):209. doi:10.1186/s41043-024-00709-x
35. Han H, Hu S, Du J. Predictive value of the hemoglobin-albumin-lymphocyte-platelet (HALP) index for ICU mortality in patients with acute exacerbations of chronic obstructive pulmonary disease (AECOPD). Intern Emerg Med. 2023;18(1):85–96. doi:10.1007/s11739-022-03132-4
36. Lan CC, Su WL, Yang MC, Chen SY, Wu YK. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: evidence from NHANES 2011–2018. Respirology. 2023;28(12):1136–1146. doi:10.1111/resp.14589
37. Toft-Petersen AP, Torp-Pedersen C, Weinreich UM, Rasmussen BS. Association between hemoglobin and prognosis in patients admitted to hospital for COPD. Int J Chron Obstruct PulmonDis. 2016;11:2813–2820. doi:10.2147/COPD.S116269
38. Takizawa A, Shimada T, Chubachi S, et al. Exploring the pathophysiology of anemia in COPD: insights from chest CT and longitudinal clinical data. Respir Med. 2025;240:108046. doi:10.1016/j.rmed.2025.108046
39. Sarkar M, Rajta PN, Khatana J. Anemia in Chronic obstructive pulmonary disease: prevalence, pathogenesis, and potential impact. Lung India. 2015;32(2):142–151. doi:10.4103/0970-2113.152626
40. Doganci M, Eraslan Doganay G. Prognostic significance of thrombocytopenia and mean platelet volume in COPD patients with acute exacerbations in ICU settings. Med Sci Monit. 2024;30:e944946. doi:10.12659/MSM.944946
41. Liu Y, Liu H, Li C, Ma C, Ge W. Proteome profiling of lung tissues in chronic obstructive pulmonary disease (COPD): platelet and macrophage dysfunction contribute to the pathogenesis of COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:973–980. doi:10.2147/COPD.S246845
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.