Back to Journals » Advances in Medical Education and Practice » Volume 11
Nursing Students Learn to Handle Stress and to Prioritize in a Complex Context During Workplace Learning in Acute Internal Medicine Care – An Ethnographic Study
Authors Hägg-Martinell A ![]() , Hult H, Henriksson P
, Hult H, Henriksson P ![]() , Kiessling A
, Kiessling A ![]()
Received 10 September 2019
Accepted for publication 3 December 2019
Published 13 January 2020 Volume 2020:11 Pages 21—30
DOI https://doi.org/10.2147/AMEP.S230476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Ann Hägg-Martinell, 1, 2 Håkan Hult, 3 Peter Henriksson, 2 Anna Kiessling 2
1Department of Health Sciences, The Swedish Red Cross University College, Huddinge, Sweden; 2Department of Clinical Sciences Danderyd Hospital, Karolinska Institutet, Stockholm; 3Department of Clinical Sciences, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden
Correspondence: Ann Hägg-Martinell
Department of Clinical Sciences Danderyd Hospital, Karolinska Institutet, 182 88, Stockholm SE-141 21, Sweden
Tel +46 70 755 59 15
Email [email protected]
Introduction: A common focus in many studies, in the short-term perspective, is to evaluate students’ workplace learning and its outcome. However, the outcome can be perceived differently depending on when it was evaluated. The aim of this study was to explore student nurses’ learning activities in an acute internal medicine unit and the nurses perceived learning outcome in a long-term perspective.
Material and Methods: Repetitive ethnographic observations were performed in an internal medicine care unit at a teaching hospital in Sweden between 2011 and 2013. Four student nurses and supervisors were repetitively observed. Two years later retrospective interviews were performed with four nurses who had performed workplace learning, as students, in this unit during the observation period. An inductive comparative analysis involving all interviews and observational data was applied.
Results: Three themes were identified: To handle shifting situations – illustrating how student nurses learnt to adapt to shifting situations, to manage stress, to create structure and space for learning and to deal with hierarchies; To build relationships – illustrating how student nurses learnt to collaborate and to interact with patients; To act independently – illustrating how student nurses trained to act independently in the unit, took responsibility, and prioritized in this complex context.
Conclusion: Learning activities in a complex acute medical unit setting were characterized by a high workload and frequent stressful situations, and a demand on students to interact, to take responsibility, and to prioritize. To learn in such a stressful context, have in a long-term perspective, a potential to develop students’ embodied understanding of and in practice, making them more prepared to work and independently apply their nursing expertise in similar contexts as graduated nurses.
Keywords: students nursing, nursing education research, clinical clerkship, ethnography
Plain Language Summary
Workplace learning is an appreciated cornerstone in nurse education. However, the long-term outcome of such learning is sparsely studied. The common focus of most studies has been to identify factors that facilitate or hinder students’ learning in a short-term perspective. Nurse students were repetitively observed during workplace learning in a stressful acute medicine care unit and follow-up interviews were conducted two years later. All data were qualitatively analyzed. Three themes emerged: To handle shifting situations, to build relationships, and to act independently. The results indicate that workplace learning in a stressful acute care unit, have in a long-term perspective, a potential to develop students’ understanding of own and others’ duties, responsibilities and roles in the workplace community, making them more prepared to work and independently apply their nursing expertise in similar contexts as graduated nurses.
Introduction
To become a professional nurse, it is important to participate in realistic workplace learning.1 Both the learning environment and the supervision influence the development of clinical competence.2 Student nurses often describe the value of such learning in the process of becoming professionals.3 However, workplace learning for student nurses takes place in an environment primarily organized to take care of patients.4
A valuable workplace learning provides continuing exposure to patients, to support the transformation of experience into knowledge and possibilities to take an active role and to receive feedback, and to have time and space for supervision.5 Furthermore, a valuable workplace learning environment is where management, planning and organization are aligned with and support learning.6
The theoretical base for this study is that learning takes place in a social context where interpersonal interactions allow an individual to integrate others’ experience in own learning.7 Further that the learning process supports relationships and inter-professional interactions.8 Wenger9 has described a social professional context as a community of practice. A community of practice can be described as a shared history of learning and defined as a mutual engagement in pursuing an initiative together to share some significant learning.9 Hagg-Martinell et al10 have clarified that the students’ task on arrival in a community of practice, is to understand and adapt to its culture, and to try to become accepted by the members of the community. The unit community consists of, shapes a pattern for, and creates prerequisites that challenge students’ adaptation and create a space for learning.
To summarize, to become a professional is a complex process. Interview and questionnaire studies have shown factors that influence student nurses’ workplace learning in a short-term perspective.5,6,11 However, the outcome of learning can be perceived different in a long-term perspective and the final goal is to support the becoming of a competent professional. This long-term perspective mirrored by how student nurses learn in a unit context needs to be studied in more depth.
The aim of the present study was to explore student nurses’ learning activities in an acute internal medicine unit, and how they perceived professional benefit from such learning in a long-term perspective.
Materials and Methods
Study Design
Based on ethnographic principles a wide data collection was performed during 2011–2013 observing workplace culture at an acute internal medicine care unit, including medical and nurse students’ interaction and opportunities to learn within this context. In one previous study of this material, the organization, the physical environment and learning culture of this unit has been described.10 During that analysis, it became obvious that in spite of simultaneous workplace learning in the same unit, the learning environment and learning activities differed a lot between the medical and the nursing students. Therefore, we decided to perform separate analyses on the medical, respectively, the nursing students. How medical students’ approach interact and socialize in this acute internal medicine unit culture, their opportunities to participate and to create space for learning in such a culture have been previously described.12
The above observation data formed the base for this study. Due to the long placements for nurse students at the unit, only four individual students could be observed during the study period. Therefore, we after a preliminary analysis decided to add interview data to capture perceived long-term learning outcomes among registered nurses, who had performed workplace learning in this specific unit.
Setting
The observed unit belonged to the department of internal medicine at a teaching hospital in Sweden. Patients in this unit had different internal medicine diseases, mainly severe infectious diseases, pulmonary diseases, deep venous thrombosis and pulmonary embolism, intoxications, convulsive disorders and allergic reactions. A central part of the unit was the observation area where staff treated and observed six patients in need of continuous observation and care due to unstable disease states.
Participants
Student nurses, nurse supervisors, consultant doctors, junior doctors, auxiliary nurses, patients and their relatives were observed in the unit. Four female student nurses were repeatedly observed during their 4–8 weeks of workplace learning scheduled in the last term of the nurse program.
Participants in the interviews were chosen based on purposive sampling. Nineteen graduated nurses, had, as students, performed workplace learning in the observed unit during the observation period 2 years earlier. They were contacted by e-mail or mail and invited to participate in individual interviews. They received written information on the purpose of the study and three reminders were sent out. However, 12 were not accessible, and three declined to participate. The remaining four nurses agreed to participate.
Data Collection
In total, 27 ethnographic observations and 15 short conversations were conducted from autumn 2011 to spring 2013. A consecutive sampling of observations and informal conversations were conducted when there were students present and if the observer was available, from Monday to Friday. Each observation session lasted 3–4 hrs. The total observation time was approximately 100 hrs and included: 50 hrs inter-professional board rounds, 25 hrs collaborative patient-related paperwork at offices, 20 hrs patient care and consultations, and 5-hrs informal patient-related interactions. The spontaneous conversations with participants were aimed at clarifying their thoughts, asking for explanations, and getting a deeper understanding of the observations. Field notes were taken and transcribed later the same day.13,14 The observation data consisted of 450 pages of single-spaced text. All observations were gathered by the “marginal participant’’ technique – in which the researcher plays only a minimal role in the social action they observe.13
Two years later, between September 2014 and December 2014, additional data were collected from four interviews with registered nurses. The interviews were performed with the aim to get a deeper understanding of important aspects of student nurses learning in a long-term perspective. Each interview lasted approximately 45–60 mins and was conducted in a conference room at the hospital where the observations were performed. The interviews were tape-recorded; listened to several times and transcribed verbatim by the first author.
The semi-structured interview guide consisted of open-ended and probing questions aimed to detect experiences of learning in the acute unit context. The interview guide was developed based on a preliminary analysis of the observation data in this study and on the results of two previous papers6,10 conceptualizing themes and cultural characteristics framing student learning in an acute healthcare context. Furthermore, the guide was influenced by Kolb’s theory on experiential learning15 and Wenger’s theory “Community of practice”.9
The first author performed all observations and interviews. Her only relationship to the participants was as a researcher. She had no relationship to them as a nurse or supervisor before, during or after. The last observation and interview mostly gained repetitive information; thus saturation was assumed.
Data Analysis
We applied an inductive comparative analysis involving all interview and observational data. Broad transcripts enabled the assembly of topic-focused data sets. This is an approach to visualize the conflict between theory and data, the “dialogue between ideas and evidence”.16 Each individual interview or observation was studied to be understood during the analysis process and the whole dataset were remembered during the analysis. The method gave an idea of the context that left space to study complex phenomena.
The first author coded data according to the framework, then the findings were repetitively discussed in the research group in a reflexive process, where the different perspectives and experiences contributed to build a comprehensive interpretation of the data. The process continued until agreement was reached. The analysis process is presented in Figure 1.
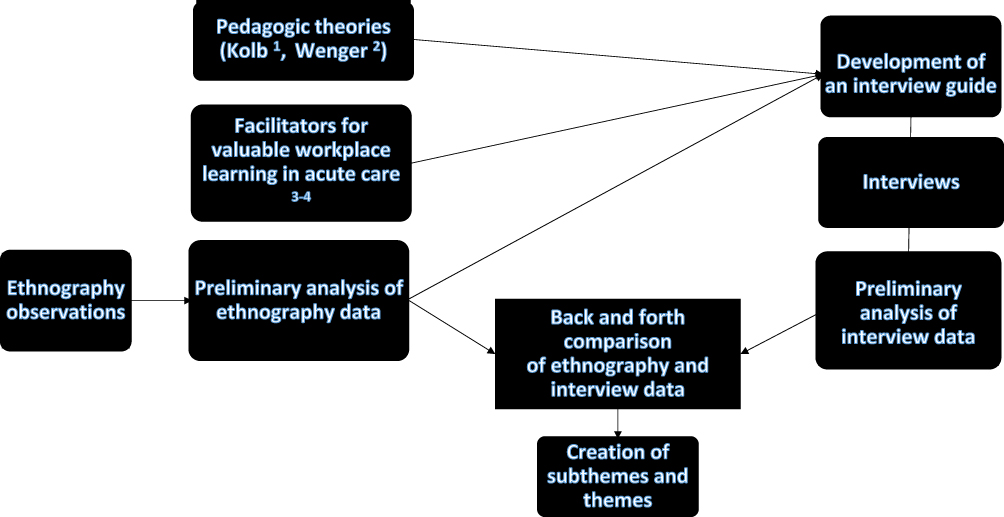 |
Figure 1 Illustration of the inductive comparative analysis process. Note: 1Kolb15;2Wenger9; 3Hägg Martinell et al6; 4Hägg Martinell et al.10 |
Results
Three themes were identified, describing student nurses’ learning activities in an acute internal medicine unit and their perceived learning outcome in a long-term perspective: to handle shifting situations, to build relationships, and to act independently. Themes and subthemes are presented in Table 1.
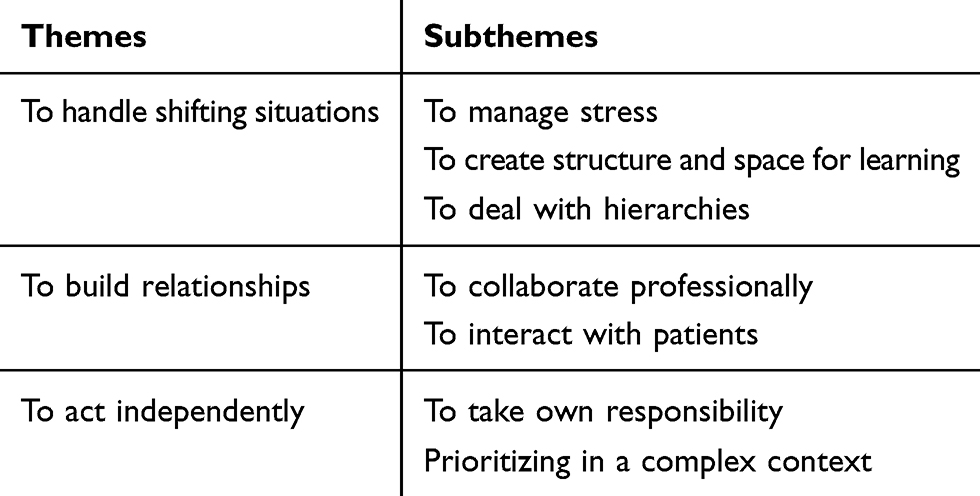 |
Table 1 Identified Themes and Subthemes |
To Handle Shifting Situations
This theme illustrates how student nurses learnt to adapt to shifting situations. The theme consists of three subthemes; to manage stress, to create structure and space for learning, and to deal with hierarchies.
To Manage Stress
During the observations, there were often a high workload with stressful situations. However, the observations also showed learning situations characterized by a peaceful atmosphere despite a surrounding stress.
The interviewed nurses emphasized the high workload and stressed that it was valuable to experience such stressful situations as a student, since they needed to be prepared for them as graduated nurses. Initially, it was difficult but over time they learnt to adapt to it.
It was a higher workload than I had experienced before, so I had to adapt to it as quickly as possible. It was hard to keep up in the beginning, but over time I learnt to deal with it, to accept it and to learn to prioritize during these circumstances
Furthermore, it was difficult for the students to understand how the staff could work under such a high workload.
“When we switched all the patients in the observation area twice within the time span of a few hours, I wondered how the staff managed to work with such high demands.”
The observations illustrated how the student nurses were thrown between altering and stressful situations. One such observation was when a student first participated in a board round and directly had to shift to welcome and take care of a new patient from the emergency department. The quick shifts between different situations sometimes seemed to make the learning fragmented. However, the observations also showed plenty of possibilities to practice various technical and hands-on skills.
The interviews indicated that this unit was perceived as a very exciting learning environment, partly due to these quick shifts in conditions, the high workload and the variety of learning activities. The interviewed nurses had experienced dissimilarities between different placements regarding whether they had possibilities to practice clinical skills or not.
To Create Structure and Space for Learning
There were situations when the management had not arranged a proper introduction at students’ arrival. Lack of introduction was observed when a new student nurse arrived to the unit as a surprise to the staff on duty. Newly arrived students had to adapt to the lack of planning and stayed close to their supervisor.
The interviews confirmed that the introduction to workplace learning sometimes failed. In spite of this, interviewed nurses still felt welcomed by their supervisors, who, in spite of planning errors managed to introduce the student nurses to the unit. However, if the management of the unit supported learning or not were not obvious to the interviewed nurses.
The observations indicated that it was difficult for both staff and students to manage the never-ending turnover of patients. In addition, overcrowding of patients was common, with no possibility to call in extra staff. Consequently, it was often difficult for the supervisors to maintain the planned supervision structure.
All interviewed nurses emphasized that a good learning environment is one where the organization creates structure and space for learning, so that supervisors had enough time to supervise and to give the students the necessary feedback.
To Deal with Hierarchies
Several observations illustrated hierarchies, e.g. when a consultant doctor decided on an action plan for a patient without discussion with the rest of the team.
In the interviews, the nurses described a hierarchic organization. The consultant doctors gave orders and the nurses and assistant nurses effectuated the work. The orders could consist of transferring patients to other rooms or other units or admitting new patients sometimes without having prepared beds for them. These orders were often given without asking if there were sufficient resources to take care of all patients.
Well, this hierarchy with the consultant doctors on top, the nurses in the middle and the assistant nurses at the bottom … . There were often situations when the consultant doctors ordered the staff, telling them to transfer patients to other rooms or other units, and the staff rushed to effectuate what they were told to do without arguing.
The observations indicated that patients with different diseases were approached differently, and that this was relatively openly discussed with the students. The unit was expected to have a high turnover of patients. At times, staff expressed the view that patients with a need for long-term care were not wanted and should be treated elsewhere due to lack of resources. Patients suffering from acute illnesses such as pulmonary embolism or convulsive disorders, could be prioritized above mentally ill or elderly patients, who could be seen as more complex and troublesome.
The interviews confirmed that the nurses in retrospect could remember hierarchies between patient groups. They especially remembered that mentally ill patients and elderly patients were placed at the bottom of such hierarchies.
Furthermore, the observations indicated that there were differences in the way different student groups were invited to participate. The interviews also indicated that medical students were regarded in some situations as more important than student nurses.
Oh yes, the medical students were seen as more important. When I was sitting in the observation area writing up a medical record on the computer, I was expected to interrupt my writing, so that a medical student could use the computer.
In contrast, the interviews stated that medical students did not have the same possibilities to participate in the patient-related duties on the unit as the student nurses. The medical students participated actively mostly during board rounds, while the student nurses often were given opportunities to be involved in all the duties.
To Build Relationships
This theme illustrates how student nurses learnt to build relationships during their placements. The themes consist of two sub-themes: To collaborate professionally and to interact with patients.
To Collaborate Professionally
The observations showed that if a student already as a newcomer participated in the duties it seemed easier to be accepted as a member of the team. The staff members first built relationships with student nurses and then invited them into the team. Inter-professional interactions with consultant doctors and junior doctors created learning opportunities, for example, while reporting patient cases during board rounds. Also, more organized inter-professional supervision occurred, e.g. when a consultant doctor explained the advantages and disadvantages of urinary catheters, and when an assistant nurse supervised a student nurse when putting in a urinary catheter. However, there were also situations when students were excluded from interaction in the team, e.g. when a junior doctor ignored the student nurse in an examination of a patient.
The interviews indicated that it was not always easy for student nurses to collaborate. The high turnover of students and junior doctors made it difficult to build relationships. The high turnover sometimes seemed to decrease the enthusiasm among the staff for new students. However, when students took their own initiatives to interact with staff members they often succeeded. Establishing relationships with team members also became easier when the team spent informal time together, for example, by taking a coffee break or having lunch together.
Though new students passed by all the time and there was a high turnover of junior doctors, I think that the staff did not manage to approach all newcomers with enthusiasm. However, when you took it upon yourself to talk to members of the staff, most of them were very nice.
To Interact with Patients
The observations showed how student nurses established relations with patients, for example, by introducing themselves or by listening to the patients describing how they felt. To administer drugs was a common situation for student nurses to enable them to interact with patients.
The interviews stated that nurses valued to learn from, build relations with and to interact with patients more than to study theory. Even if there were many patient dialogues, the nurses would have liked to have more opportunities to listen to the patients’ histories and get a more holistic picture of the individuals.
To Act Independently
This theme refers to whether and how the student nurses were able to train to take care of patients independently. The theme consists of two sub-themes: to take own responsibility and prioritizing in a complex context.
To Take Own Responsibility
The observations indicated that the student nurses over time developed increased competence and became able, with the support of their supervisor, to take more responsibility as nurses, for example, by taking care independently for a group of patients or to manage all nurse duties during a board round. To independently manage all nurse duties during a board round took only a few weeks for students with longer placements to reach. Even in cases when students did not manage a full responsibility, they were often given the responsibility for defined nurse duties, for example, administering drugs or taking blood samples.
The interviews indicated that lack of staff could create situations where the student nurses had to take responsibility for patients without sufficient supervision. These situations were perceived as unsafe and did not stimulate learning.
I remember a day when I was supposed to follow a nurse but there was a lack of staff. We had to divide the patients between us, and I had to work as a nurse during the whole working shift. As a student, you should not have to take that responsibility.
The observations showed that when students were not involved in the team by the staff, they often took own initiatives to learn, for example, by taking notes or gathering information in the medical records. Students who took a more passive approach as observers tended more often to be unnoticed by the staff than students with a more active approach.
All interviewed nurses clearly stated that as a student they had own responsibility to take up their space. They had to show that they wanted to participate, to learn, and that they could be trusted to perform nurse duties.
I think that you have to take up space as a student, put your best foot forward and show that you are trustworthy, take responsibility and show that you are interested to learn. Then you get opportunities to participate.
Prioritizing in a Complex Context
The observations illustrated the complexity of the care provided in the unit. There were constantly people coming and going, medical devices recurrently sounding alerts, and the students were supposed to learn in the middle of this. However, it was not obvious how this complexity was perceived by the student nurses.
However, the interviews provided indicated that they, by being in this complex context, had gained increased understanding of their future professional role and prepared them to act independently as nurses. They had encountered a large variety of patients with different diagnoses, which gave them a bit of everything and an increased understanding of the complexity of acute patient care.
Furthermore, the interviews indicated that the nurses, as students, had gained sufficient theoretical knowledge to act independently under supervision. They had the knowledge to discern why different decisions were needed. At the end of the placement, they had learnt to apply their theoretical knowledge in real clinical situations and thereby develop their prioritizing skills, when time was limited.
At the end of the placement you became fairly good at prioritizing when there was lack of time, and you learnt how to prioritize the most important issue. This was a positive result of the time constraint because it is difficult to discuss how to handle stress if you haven’t experienced it.
The interviews indicated that team participation in the observation area developed the nurses’ skills in overall control. In the beginning, they, as students, had followed their supervisors’ work, even if it was sometimes difficult for them to comprehend the complexity. The principles of prioritizing between duties were sometimes invisible to them. In addition, it was sometimes difficult to understand why duties were conducted in certain ways in acute situations. They needed to be involved more than once to know how to act. By repetitive participation, their level of experience increased, and it became easier to feel comfortable in acute situations. The nurses also learnt to prioritize between different patients, for example, by comparing how ill one patient appeared in comparison to other patients to determine who needed their attention first. Viewing and comparing the patients in the observation area helped them to grasp the big picture. They felt that earlier placements in ordinary units with beds in different rooms had not enabled them to develop this global understanding of how to act in practice.
Discussion
Student nurses’ learning in an acute internal medicine unit and their perceived learning outcome in a long-term perspective could be summarized in three themes: To handle shifting situations; to build relationships, and to act independently.
To Handle Shifting Situations
Stress can have dual effects on learning.17 Stress associated with challenges is beneficial for learning, but stress associated with hindrances is harmful for learning. Students experienced both stressed and shifting situations on the unit and we could not observe any signs that stress was supportive for learning. However, in retrospect, the interviewed nurses appreciated the experience of acting in stressed and shifting situations.
To reach a sense of capability to handle a high workload and shifting conditions was perceived as a valuable experience for their development as professional nurses. Alghamdi18 has described the workload for nurses as: the immensity of direct patient care; the amount of physical effort; the complexity of care; the quantity of time and the grade of competency.
Lamont et al19 have stated that student nurses were satisfied with their clinical placement if they were welcomed, when the staff had a positive attitude to the students, and when the students were able to participate in patient care. We saw that lack of; planning of learning, time for learning, and opportunities for feedback sometimes impaired the learning process. The complexity of care processes made it more difficult for students to actively participate and they often had to find their own strategy to make their learning as worthy as possible.
The hierarchic culture on the unit was evident to the students and it seemed to hinder learning in different ways. Sandberg20 state that a supportive working climate involving respect, cooperation, feedback and information is vital for nurses to be able to participate in a working team. We can only speculate as to whether this hierarchic culture affected student nurses’ views in a long-term perspective.
To Build Relationships
According to Wenger,9 students’ participation in a community can be legitimate but is often peripheral. During a placement a student should enter the community and pass through its boundary.21 We saw that the high number of students and junior doctors coming and going on the unit sometimes created a sense of resignation and a lack of motivation among staff to create relationships with newcomers and to invite them to join. Student nurses interacted with physicians and assistant nurses. However, several unexploited opportunities to highlight the inter-professional interactions for learning were also observed. Hallin and Kiessling22 have pinpointed that well-organized inter-professional training provides a supportive and permissive learning environment. With an increased support of students’ inter-professional interactions in regular units, potential valuable learning can be assured.
Learning to become a nurse is a multidimensional process that needs a supportive relationship with supervisors.23 We saw that if students related to their supervisors and took own initiative, they were easier invited into the community. To be a newcomer and have a new supervisor created a feeling of uncertainty. Papastavrou et al24 have shown that students with named supervisors were more satisfied with their placements than students without that kind of an established relationship.
To Act Independently
Students had opportunities to perform nurse tasks independently under supervision which provided them with new experiences. However, insufficient supervision with too much own responsibility for the student hindered learning and created an insecure feeling. In addition, the insecure feeling among the staff when they had to perform unfamiliar medical treatments created a stressed atmosphere that hindered students learning. Hood et al25 have shown that own engagement creates an opportunity to train a professional role, to independency and to see clearly what a profession is all about. We noticed that learning in this unit seemed to give students a holistic understanding of what it is, as a nurse, to take care of patients. This is in line with Dall’Alba and Sandberg26 who stated that development of professional competence has two dimensions – medical expertise and embodied an understanding of and in practice. The possibility to develop the second dimension depends on the needs and knowledge of the individual student, as well as on the possibilities to participate in a context where the profession is practiced. Based on the findings in this study we argue that the participants, in the long-term perspective, had developed their embodied understanding of and in practice. They realized that their previous workplace learning in this stressful context where they had to act independently, had made them more prepared to work independently and to apply their nursing expertise in similar contexts as graduated nurses.
Method Discussion
Qualitative studies are performed in a specific context which create an opportunity for a deeper analysis of the studied context. By ethnographic observations, we were able to gain a richer understanding of the student nurses’ learning activities in this acute internal medicine unit. Four individual nurse students were observed during repetitive different learning activities at the unit during 4–8 weeks, creating a possibility to follow their individual growing independency in patient care. The follow-up interviews added nurses’ long-term perspective on the outcome of their undergraduate learning in acute care. The comparative inductive analysis of the interview and observation data increased the findings’ trustworthiness and credibility. One limitation was that only four nurses were interviewed. However, as we wanted to restrict the data collection to focus on learning in this particular learning environment, there were no more than these four who were accessible to participate. However, the interview data were rich and coherent, and triangulated and deepened the understanding of the observational findings.27 A limitation of ethnographic observations is a risk of researcher bias, as the researcher is used as a tool during the observations. The observer (the first author) was a female-registered nurse with a long experience of nurse education in acute internal medicine care settings. This preunderstanding and experience of the context allowed the observations and the analysis to be performed in more depth. In contrast, a plausible bias of a researcher with preunderstanding and experience of a studied context may be that important aspects could remain unnoticed. Initially, some of the staff was a bit cautious, but they also expressed that the research question was important to investigate and that they wanted to contribute. Using the marginal participant technique, in which the observer plays only a minimal role in the interaction, should minimize the risk of disturbing what happens in the room, how participants were placed, and which interactions that took place. Furthermore, investigator triangulation was applied, and all researchers were engaged in the analysis, which meant that different professional perspectives and experiences (nurse, physician and educational researcher) could be applied in order to ensure credibility.
Conclusion
Learning activities in a complex acute medical unit setting were characterized by a high workload and frequent stressful situations, and a demand on students to interact, to take responsibility, and to prioritize. To learn in such a stressful context, have in a long-term perspective a potential to develop students’ understanding of own and others’ duties, responsibilities and roles in the workplace community. This development of an embodied understanding of and in practice, makes them more prepared to work and to independently apply their nursing expertise in similar contexts as graduated nurses.
Ethics Approval and Informed Consent
The observations were conducted in a busy setting where a lot of people such as staff, students, patients, spouses and other visitors were constantly passing by for longer or shorter time. It was therefore not possible to ask all for written informed consent. Further, the focus was on observing only those directly participating in the learning activities. All these participants gave oral-informed consent in accordance with the Declaration of Helsinki after receiving oral information about the purpose and method of the study, as well as the fact that participation was voluntary. The participants in the interviews gave written informed consent in accordance with the Declaration of Helsinki after receiving oral information about the purpose and method of the study, as well as the fact that participation was voluntary. Permission to carry out the study was given by the regional Ethical Review Board, Stockholm Sweden no 2011/1268-31/5. Permission to conduct the observations at this particular unit was given by the head of department.
Acknowledgements
The authors thank all the participants for giving their time to take part in this study.
Author Information
Ann Hägg-Martinell, PhD, RN, is a senior lecturer at The Swedish Red Cross University College and is an experienced medical educator and educational researcher.
Håkan Hult, PhD, is a professor at Karolinska Institutet and is an experienced medical educator. Peter Henriksson, MD, PhD, is a senior professor and a very experienced medical educator at Karolinska Institutet. Anna Kiessling, MD, PhD, is a senior lecturer at Karolinska Institutet and an experienced medical educator and educational researcher.
Author Contributions
AK took initiative to the study and HH came up with the idea to apply an ethnographic design. AHM performed, under the supervision of AK, all observations and acquisition of data and compiled the written documentation of the observational data. All four authors (AHM, HH, PH and AK) contributed substantially to the analysis and interpretation of data. AK and AHM performed the main part of drafting the work and then all authors (AHM, HH, PH and AK) contributed substantially in revising it critically for important intellectual content. All four authors (AHM, HH, PH and AK) have approved the final submitted version and all four authors (AHM, HH, PH and AK) have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The study was supported by grants provided by the Stockholm County Council, Sweden (ALF project).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gidman J, McIntosh A, Melling K, Smith D. Student perceptions of support in practice. Nurse Educ Pract. 2011;11(6):351–355. doi:10.1016/j.nepr.2011.03.005
2. Pitkanen S, Kaariainen M, Oikarainen A, et al. Healthcare students’ evaluation of the clinical learning environment and supervision - a cross-sectional study. Nurse Educ Today. 2018;62:143–149. doi:10.1016/j.nedt.2018.01.005
3. Papp I, Markkanen M, von Bonsdorff M. Clinical environment as a learning environment: student nurses’ perceptions concerning clinical learning experiences. Nurse Educ Today. 2003;23(4):262–268. doi:10.1016/S0260-6917(02)00185-5
4. Mennin S. Self-organisation, integration and curriculum in the complex world of medical education. Med Educ. 2010;44(1):20–30. doi:10.1111/j.1365-2923.2009.03548.x.
5. Ottenheijm RPG, Zwietering PJ, Scherpbier AJJA, Metsemakers JFM. Early student-patient contacts in general practice: an approach based on educational principles. Med Teach. 2008;30(8):802–808. doi:10.1080/01421590802047265
6. Hagg-Martinell A, Hult H, Henriksson P, Kiessling A. Students perceive healthcare as a valuable learning environment when accepted as a part of the workplace community. Educ Health (Abingdon). 2014;27(1):15–23. doi:10.4103/1357-6283.134296
7. Vygotskij L. The Collected Works of L.S. Vygotsky. The History of the Development of Higher Mental Functions. Vol. 4. New York: Plenum Press; 1997.
8. Bok HG, Teunissen PW, Favier RP, et al. Programmatic assessment of competency-based workplace learning: when theory meets practice. BMC Med Educ. 2013;13:123. doi:10.1186/1472-6920-13-123
9. Wenger E. Communities of Practice: Learning, Meaning, and Identity. Cambridge: Cambridge University Press; 1998.
10. Hagg-Martinell A, Hult H, Henriksson P, Kiessling A. Community of practice and student interaction at an acute medical ward: an ethnographic study. Med Teach. 2016;38(8):793–800. doi:10.3109/0142159X.2015.1104411
11. Midgley K. Pre-registration student nurses perception of the hospital-learning environment during clinical placements. Nurse Educ Today. 2006;26(4):338–345. doi:10.1016/j.nedt.2005.10.015
12. Hagg-Martinell A, Hult H, Henriksson P, Kiessling A. Medical students’ opportunities to participate and learn from activities at an internal medicine ward: an ethnographic study. BMJ Open. 2017;7(2):e013046. doi:10.1136/bmjopen-2016-013046
13. Hammersley M, Atkinson P. Ethnography: Principles in Practice.
14. Atkinson P. The Clinical Experience: The Construction and Reconstruction of Medical Reality.
15. Kolb D. Experimental Learning: Experience as the Source of Learning and Development. Englewood Cliffs, N.J: Prentice-Hall, cop; 1984.
16. Rihoux B. Bridging the gap between the qualitative and quantitative worlds? A retrospective and prospective view on qualitative comparative analysis. Field Methods. 2003;15(4):351–365. doi:10.1177/1525822X03257690
17. LePine JA, LePine MA, Jackson CL. Challenge and hindrance stress: relationships with exhaustion, motivation to learn, and learning performance. J Appl Psychol. 2004;89(5):883–891. doi:10.1037/0021-9010.89.5.883
18. Alghamdi MG. Nursing workload: a concept analysis. J Nurs Manag. 2016. doi:10.1111/jonm.12354
19. Lamont S, Brunero S, Woods KP. Satisfaction with clinical placement–the perspective of nursing students from multiple universities. Collegian. 2015;22(1):125–133. doi:10.1016/j.colegn.2013.12.005
20. Sandberg H. The concept of collaborative health. J Interprof Care. 2010;24(6):644–652. doi:10.3109/13561821003724034
21. Wenger E. Communities of practice and social learning systems. Organization. 2000;7(2):225–246. doi:10.1177/135050840072002
22. Hallin K, Kiessling A. A safe place with space for learning: experiences from an interprofessional training ward. J Interprof Care. 2016;30(2):141–148. doi:10.3109/13561820.2015.1113164
23. Warne T, Johansson UB, Papastavrou E, et al. An exploration of the clinical learning experience of nursing students in nine European countries. Nurse Educ Today. 2010;30(8):809–815. doi:10.1016/j.nedt.2010.03.003
24. Papastavrou E, Lambrinou E, Tsangari H, Saarikoski M, Leino-Kilpi H. Student nurses experience of learning in the clinical environment. Nurse Educ Pract. 2010;10(3):176–182. doi:10.1016/j.nepr.2009.07.003
25. Hood K, Cant R, Leech M, Baulch J, Gilbee A. Trying on the professional self: nursing students’ perceptions of learning about roles, identity and teamwork in an interprofessional clinical placement. Appl Nurs Res. 2014;27(2):109–114. doi:10.1016/j.apnr.2013.07.003
26. Dall’Alba G, Sandberg J. Unveiling professional development: a critical review of stage models. Rev Educ Res. 2006;76(3):383–412. doi:10.3102/00346543076003383
27. Patton M. Qualitative Research & Evaluation Methods: Integrating Theory and Practice. London: Sage; 2015.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.