Back to Journals » Journal of Inflammation Research » Volume 19
Nursing Management of Repeated Extubation Failure Following Colonic Volvulus Surgery in a Patient with Alstrom Syndrome: A Case Report
Authors Shen Y, Chen Y, Fu X, Jiang W, Li J
Received 25 February 2026
Accepted for publication 15 May 2026
Published 19 June 2026 Volume 2026:19 601374
DOI https://doi.org/10.2147/JIR.S601374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alberto Caminero
Yelin Shen,* Yuanting Chen,* Xia Fu, Wenxin Jiang, Jiazhao Li
Department of Intensive Care Unit, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, Guangdong, 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiazhao Li, Department of Intensive Care Unit, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, No. 106, Zhongshan 2nd Road, Yuexiu District, Guangzhou, Guangdong, 510080, People’s Republic of China, Email [email protected]
Background: Alstrom syndrome is a rare genetic disorder characterized by multi-system involvement, including metabolic, sensory, and cardiorespiratory impairments. Patients undergoing major surgery are at high risk of respiratory complications, though reports of repeated extubation failure are scarce.
Case Presentation: An 18-year-old male with a previous diagnosis of Alström syndrome was admitted for acute abdominal pain and diagnosed with colonic volvulus. An emergency exploratory laparotomy was performed, which included the reduction and decompression of the colonic volvulus, followed by a partial sigmoidectomy and stoma formation. Postoperatively, the patient was transferred to the ICU and experienced two episodes of extubation failure requiring reintubation. The failures were considered multifactorial, involving impaired airway clearance, limited cooperation with coughing and expectoration, secretion retention, possible aspiration risk, and concomitant pulmonary infection. Multidisciplinary interventions were implemented, including intensified inflammatory monitoring, secretion management, and systematic pre-extubation evaluation.
Interventions and Outcomes: Under coordinated medical and nursing care, tailored airway management was performed, including bronchoscopic hygiene, pharmacologic reduction of secretions, and continuous monitoring of infection markers. After a structured weaning process, the patient was successfully extubated on the third attempt and was eventually discharged in stable condition.
Conclusion: This case presents our clinical experience with repeated extubation failures in a patient with Alstrom syndrome following abdominal surgery, highlighting the profound complexities of postoperative airway management. It suggests that a multidisciplinary approach emphasizing vigilant infection control, personalized respiratory care, and systematic weaning planning proved essential for successful extubation in this specific complex scenario.
Keywords: alstrom syndrome, colonic volvulus, extubation failure, airway management
Introduction
Alström syndrome (AS) is an extremely rare autosomal recessive ciliopathy caused by biallelic mutations in the ALMS1 gene, with an estimated prevalence of approximately 1 in 1,000,000 to 10 in 1,000,000.1 This disorder can lead to multi-system damage, featuring complex and diverse clinical manifestations. These primarily include vision loss due to cone-rod dystrophy occurring in infancy, sensorineural hearing loss, childhood obesity, insulin resistance and type 2 diabetes, dilated cardiomyopathy, hypertriglyceridemia, hypertension, and progressive hepatic and renal dysfunction; however, cognitive function is typically normal.1 Additionally, AS can involve the gastrointestinal system, commonly presenting with epigastric pain and gastroesophageal reflux, whereas intestinal volvulus is relatively rare. To date, only one report describes siblings with spontaneous cecal volvulus;2 both patients were transferred to the ICU postoperatively and had concomitant basilar pneumonia, with one ultimately requiring a tracheotomy due to difficult extubation.2 In patients undergoing other types of emergency intestinal surgery, such repeated endotracheal extubation failures are exceedingly uncommon. Extubation failure is typically defined as the need for reintubation within 72 hours after removal of the endotracheal tube.3 Given the rarity and clinical complexity of Alström syndrome, cases complicated by intestinal volvulus are even scarcer. This article reports a case of a patient with Alström syndrome complicated by colonic volvulus and intestinal obstruction who was transferred to the ICU postoperatively and experienced two extubation failures. The nursing experience is summarized herein to provide clinical reference.
Case Presentation
General Information
An 18-year-old male (height: 170 cm; weight: 70 kg; BMI: 24.2 kg/m2) was admitted to the gastrointestinal surgery department on October 9, 2024, presenting with a 2-day history of abdominal distension and a 1-day history of abdominal pain. An abdominal CT scan at a local hospital suggested colonic volvulus with incomplete intestinal obstruction, indicated by a clockwise rotation at the root of the mesentery in the left lower abdomen involving the descending colon-sigmoid colon. Emergency surgery was performed that same afternoon, consisting of an exploratory laparotomy, lysis of abdominal adhesions, reduction of the colonic volvulus and colonic decompression, followed by a partial sigmoidectomy and colostomy. Postoperatively, the patient was transferred to the ICU. Admission diagnoses included intestinal obstruction, intestinal volvulus, obesity-retinal degeneration-diabetes syndrome (Alström syndrome), diabetes mellitus, fatty liver disease, and intellectual disability. Past medical history revealed a diagnosis of Alström syndrome at age 1. The patient had been diagnosed with Alström syndrome at an outside hospital during childhood; however, the detailed genetic testing report and specific ALMS1 variant information were not available for review during this admission. His phenotypic features were consistent with Alström syndrome, including severe cone-rod dystrophy with residual light perception only, sensorineural hearing loss, childhood-onset obesity, type 2 diabetes mellitus, fatty liver disease, and intellectual disability with a cognitive level equivalent to that of a 6-year-old child. Laboratory findings on admission were: white blood cell (WBC) count 16.56×109/L, high-sensitivity C-reactive protein (hs-CRP) 36.2 mg/L, and interleukin-6 (IL-6) 201.2 pg/mL. Preoperative basic blood tests showed hemoglobin 138 g/L, sodium 139 mmol/L, potassium 2.87 mmol/L, calcium 2.34 mmol/L, chloride 101.1 mmol/L, blood glucose 6.43 mmol/L, serum creatinine 23.55 μmol/L, and urea 3.95 mmol/L. These results indicated normal hemoglobin and preserved renal excretory function, with hypokalemia noted before surgery. Blood glucose levels during hospitalization ranged from 5.03 to 7.67 mmol/L.
Treatment and Outcome
The patient was transferred to the ICU at 01:45 on October 10 post-surgery for mechanical ventilation. On admission, his body temperature was 38.3°C; other vital signs were stable, with an APACHE II score of 6. Treatments included fluid resuscitation, maintenance of electrolyte balance, albumin supplementation, and prophylactic intravenous cefuroxime (1.5g bid) for anti-infection. Repeated infection markers showed a WBC count of 19.40×109/L, hs-CRP 24.7 mg/L, and IL-6201.2 pg/mL. The patient was conscious with adequate respiratory function, and the endotracheal tube was extubated at 13:15 on October 10, followed by oxygen inhalation via bilateral nasal cannula. At 04:40 on October 11, he developed acute respiratory distress with decreased oxygen saturation under a reservoir mask, necessitating immediate reintubation and mechanical ventilation. His temperature peaked at 39.3°C; abdominal drainage was turbid, inflammatory markers elevated, and head-chest-abdominal CT revealed pulmonary infection and colonic gas distension. Antibiotics were escalated to imipenem-cilastatin and teicoplanin on October 11. Following treatment, his peak temperature decreased, inflammatory markers improved, and intestinal function recovered. After 24 hours without ventilator support, the endotracheal tube was successfully removed at 09:12 on October 16. He was transferred back to the gastrointestinal surgery department at 15:35 on October 17. However, at 06:36 on October 18, he again developed respiratory distress, lethargy, with oxygen saturation dropping to 79%, blood pressure 155/90 mmHg, and heart rate 144 beats/min. Emergency reintubation was performed, and he was readmitted to the ICU for mechanical ventilation. Vital signs post-admission were: temperature 39.8°C, blood pressure 148/71 mmHg, heart rate 160 beats/min, and respiratory rate 43 breaths/min. Due to repeated extubation failure and persistent concern regarding infection and secretion retention, antibiotic therapy was adjusted to imipenem-cilastatin and vancomycin. Fiberoptic bronchoscopy was performed to assess and clear airway secretions, and bronchoalveolar lavage fluid samples were collected for smear, culture, and pathogen testing. Fiberoptic bronchoscopy was performed to assess and clear airway secretions, and bronchoalveolar lavage fluid samples were collected for smear, culture, and pathogen testing. Excessive oral secretions were managed with penehyclidine hydrochloride (0.5mg) to inhibit salivary and airway gland secretion. Mechanical ventilation was discontinued at 13:45 on October 22, and the endotracheal tube was successfully removed at 15:25. He was transferred back to gastrointestinal surgery two days later and was discharged on October 28.
Nursing Management
Integrated Medical-Nursing Rounds and Individualized Care
A comprehensive and collaborative approach was implemented. Firstly, upon the patient’s postoperative return to the ICU, detailed information regarding the intraoperative course and postoperative considerations was obtained through thorough communication with the gastrointestinal surgery and anesthesiology teams. Secondly, the assigned nurse participated in daily joint rounds conducted by ICU and gastrointestinal surgery physicians. This ensured a clear understanding of the daily treatment plan and goals, facilitated discussions about the patient’s condition and progress with both the attending and senior physicians, and allowed for collaborative identification of key nursing priorities and challenges. For this patient with Alström syndrome, the primary concerns involved the airway, intestinal function, and infection management, with no significant impairment of other organs (cardiac, renal, and hepatic functions were essentially normal), necessitating close monitoring and protection of these systems. His diabetes was managed effectively; blood glucose remained stable during hospitalization (5.03–7.67 mmol/L in the ICU), monitored every two hours while fasting. Recognizing that conventional ICU airway care protocols were insufficient due to the repeated extubation failures, nurses worked with physicians to analyze the causes and promptly adjust interventions. Preventing, monitoring, and controlling infection, particularly abdominal and pulmonary, was a major nursing focus.
Thirdly, considering the patient’s intellectual disability, severely impaired vision (light perception only), and hearing loss, which limited communication, cooperation, and often led to agitation—especially an inability to effectively cough and expectorate around extubation—nurses provided back percussion or mechanical vibration during each shift handover to promote sputum expulsion and reduce airway obstruction risk. A hybrid visitation model combining WeChat video calls and in-person ICU visits was used to involve family members in care, aiding in calming the patient and guiding him to cooperate with coughing and expectoration. Fourthly, individualized communication strategies were employed: as the patient only communicated in local dialect, nurses fluent in the dialect were assigned to his care whenever possible. This enhanced his sense of security and communication effectiveness. Using the local dialect to respond promptly to his feedback and concerns significantly reduced his agitation and crying, improving cooperation with nebulization and expectoration efforts. Fifthly, due to his visual impairment, nurses used verbal communication, sound cues, and gentle touching of his hands before shift changes or procedures to inform him of upcoming care activities, preparing him psychologically, reducing startle responses, and fostering better cooperation.
Monitoring of Inflammatory Markers and Related Care
Given the prolonged surgery (3 hours) involving major organs, elevating infection risk, a temperature-sensing urinary catheter was placed for continuous core temperature monitoring. Daily monitoring of hematologic parameters, interleukin-6 (IL-6), high-sensitivity C-reactive protein (hs-CRP), and procalcitonin (PCT) was performed (Figure 1). Nurses assisted physicians in collecting abdominal drainage fluid and bronchoalveolar lavage samples for pathogen testing and closely followed microbiological and imaging results. Nurses assisted physicians in collecting abdominal drainage fluid and bronchoalveolar lavage fluid samples for pathogen testing and closely followed microbiological and imaging results. No pathogen was detected in the abdominal drainage fluid. Bronchoalveolar lavage fluid obtained on October 14 was also negative for pathogens, whereas a small amount of Klebsiella aerogenes (2+) was detected in bronchoalveolar lavage fluid on October 20.
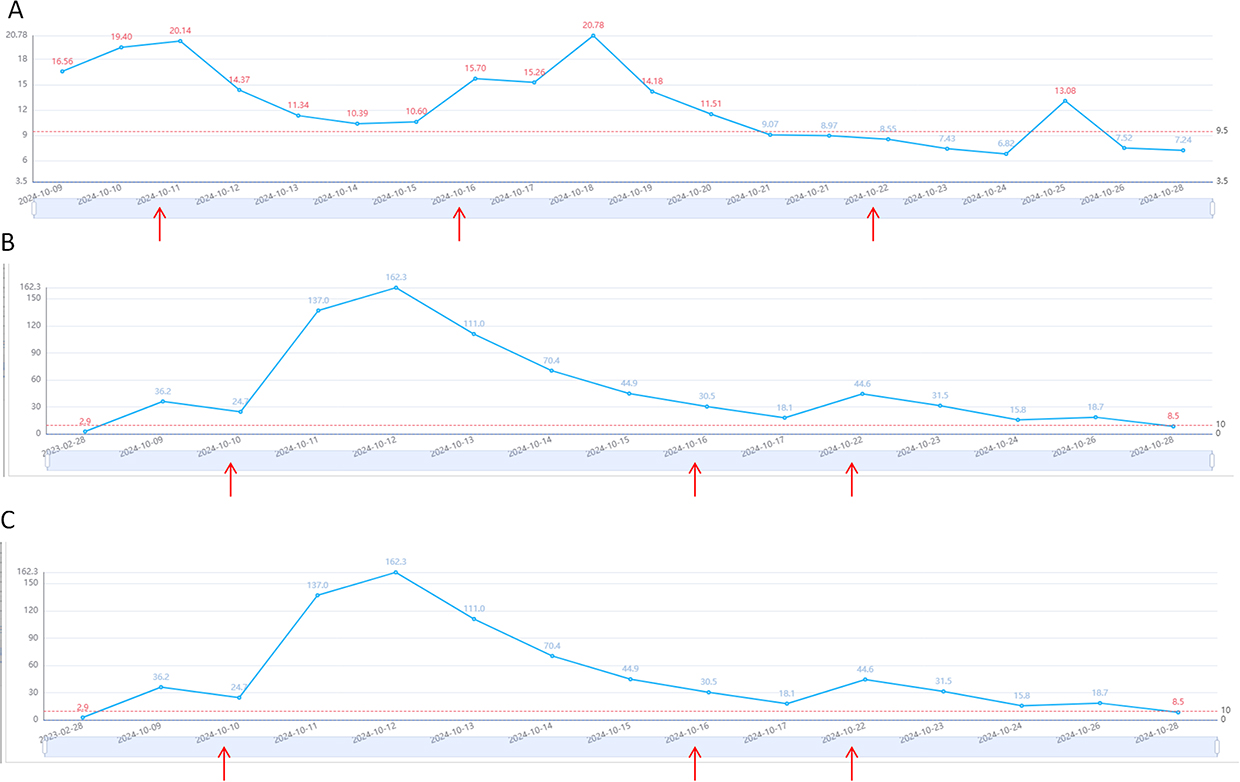 |
Figure 1 Dynamic trends of inflammatory markers during hospitalization. (A) White blood cell count (×109/L); (B) High-sensitivity C-reactive protein (hs-CRP) (mg/L); (C) Interleukin-6 (IL-6) (pg/mL). Notes: Red upward arrows indicate the timings of the three endotracheal extubation attempts (Oct 10, Oct 16, and Oct 22, respectively). The dashed line indicates the upper limit of normal. The significant increases in IL-6 and WBC after Oct 16 (following the second extubation attempt) were strongly associated with clinical deterioration and failure. The marked improvement in inflammatory markers after October 23 created conditions for the final successful extubation. |
Monitoring indicated an infectious state on admission (WBC 16.56×109/L, hs-CRP 36.2 mg/L, IL-6201.2 pg/mL, all significantly elevated). Prophylactic intravenous cefuroxime (1.5g bid) was administered as ordered. On October 10, although WBC rose further to 19.4×109/L, hs-CRP decreased to 24.7 mg/L; the patient was conscious with stable vital signs and good respiratory function, so antibiotic therapy was continued. From October 10 to 12, inflammatory markers trended significantly upward. Following an episode of acute respiratory distress and fever on October 11 at 04:40, requiring reintubation, CRP peaked on October 12 at 162.3 mg/L (approximately 4.5 times the admission level). Antibiotics were escalated to imipenem-cilastatin (1g tid) plus teicoplanin (400mg qd, with the first three doses at 400mg q12h), accompanied by intensified airway management. CRP levels subsequently declined.
After the first extubation, IL-6 increased markedly, peaking at 652.1 pg/mL on October 17, coinciding with a significant rise in WBC to 20.78×109/L. Following the second extubation failure on October 18, IL-6 remained elevated at 652 pg/mL, accompanied by high fever (39.8°C), tachycardia, and hypertension, indicating worsened infection strongly correlated with the extubation failures. Antibiotics were adjusted to imipenem-cilastatin (1g q8h) and vancomycin (1000mg q12h). Bronchoscopy was performed to clear airway secretions and obtain bronchoalveolar lavage fluid samples for pathogen analysis. With aggressive anti-infective treatment and comprehensive nursing interventions, the inflammatory markers gradually decreased. By October 23, WBC had normalized to 6.82×109/L, hs-CRP decreased to 15.8 mg/L, and IL-6 dropped to 4.2 pg/mL, nearing normal levels.
Abdominal Assessment and Care
Drainage tubes were securely fixed, with close monitoring of effluent, the surgical wound, and the stoma. The wound dressing remained clean and dry, with daily assessment for healing. Drainage fluid was turbid on postoperative day (POD) 1, prompting specimen collection for analysis. The volume of drainage decreased progressively: 210 mL in both the first 6 hours and on POD 1, 40 mL on PODs 2 and 3, and only 5 mL on POD 4, indicating effective control of abdominal infection. Stoma viability and stool characteristics were assessed each shift. The stoma appeared pink and viable, with 30 mL of yellow-green watery stool output on POD 3. To manage the persistent watery/loose stools, the stoma bag was connected via its opening to a suction tube system. A suction tube and the soft tubing from a scalp needle (with metal needle removed) were inserted ~1.5 cm into the stoma bag, secured with rubber bands and tape. The other end of the suction tube was connected to the inner canister of a suction bottle for continuous stool drainage, applying negative pressure of −100 to −150 mmHg if necessary.4 The fixed scalp needle tubing was also connected to an infusion set delivering 37°C ± 2°C normal saline for irrigation,5 performed promptly when stool was present in the bag. Stool characteristics and volume were monitored each shift, and the suction canister was replaced daily. Abdominal assessments each shift revealed no significant distension and good bowel sounds return. Gastric decompression postoperatively yielded no gastric fluid or air. Enteral nutrition via nasogastric tube was initiated on POD 5 without discomfort, indicating overall satisfactory abdominal recovery.
Airway Management and Extubation Process
First Extubation (Attempt 1)
Pre-Extubation Assessment (Oct 10)
The patient was conscious. Originally intubated for abdominal surgery, he had no preoperative signs of respiratory infection or radiologic evidence of pneumonia, prompting a plan for early extubation and ICU discharge. Sedation was gradually reduced starting at 06:00 on Oct 10 (POD 1) and discontinued 3 hours pre-extubation (RASS score −4 to −2 during sedation). He demonstrated smooth respiration, good spontaneous breathing, effective cough reflex, coarse breath sounds bilaterally without rales, a negative cuff leak test, and no evidence of laryngeal edema or upper airway obstruction. The ventilator was discontinued, and he received moderate-flow oxygen via the endotracheal tube. Pre-extubation arterial blood gas analysis under FiO2 40% showed PaCO2 40 mmHg and PaO2 129 mmHg, with an oxygenation index of 323, indicating acceptable oxygenation and ventilation before extubation. The endotracheal tube was removed after 1 hour off the ventilator.
Post-extubation care (Oct 10)
He received oxygen via bilateral nasal cannula at 4 L/min. Coarse breath sounds were occasionally noted, requiring oronasal suction to maintain airway patency. Given his intellectual disability and communication challenges impairing cough cooperation, family members were engaged to assist in guiding and encouraging cough and expectoration, which was moderately successful. Due to the risk of bacterial translocation from intestinal obstruction/volvulus and potential concomitant pneumonia, infection markers and respiratory status were closely monitored alongside continuous heart rate, blood pressure, respiration, and SpO2 monitoring. A bedside chest X-ray was obtained post-extubation. Post-extubation arterial blood gas analysis under FiO2 37% showed PaCO2 40 mmHg and PaO2 88 mmHg, with an oxygenation index of 237. The patient had smooth respiration at 15–16 breaths/min, and repeat chest radiography later that day showed only mild bilateral pulmonary inflammation. Body temperature, heart rate, and blood pressure remained stable while anti-infective therapy was continued. He subsequently developed respiratory distress and decreased SpO2 overnight, necessitating reintubation. The cause of this deterioration was investigated.
Second Extubation (Attempt 2)
Reintubation occurred merely 13 hours after the first extubation (Oct 11), raising concern for worsened infection or pneumonia. Post-intubation, infection markers were immediately checked, and a CT scan of the chest and abdomen was performed, revealing pulmonary infection and colonic distension (Figure 2A), alongside elevated temperature (max 39.3°C), turbid abdominal drainage, and rising inflammatory markers. Antibiotics were changed to imipenem-cilastatin and teicoplanin per orders. He was ventilated in a spontaneous breathing mode. A second extubation was planned after infection control. A follow-up CT (Oct 13, Figure 2B) showed persistent lung inflammation/atelectasis compared to the previous scan, with the endotracheal tube still in place.
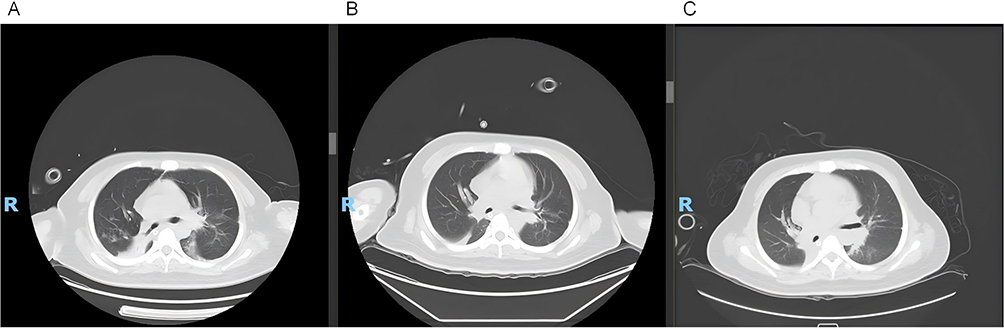 |
Figure 2 Serial Chest CT Imaging. (A) Oct 11 (Post first reintubation): Patchy and linear opacities, predominantly in the left lung, suggestive of pneumonia or atelectasis. Endotracheal tube in situ. (B) Oct 13 (Pre-second extubation attempt): Lung lesions showed no significant improvement compared to Oct 11, with persistent inflammation/atelectasis. Endotracheal tube in situ. (C) Oct 18 (Post second reintubation): Lung lesions showed no significant change from previous, with persistent inflammation/atelectasis. Endotracheal tube in situ. |
Evidence-based nursing practice was implemented, noting literature reports of Alström syndrome patients being prone to hypoxic episodes during minor procedures, anesthesia, or severe infection, recommending careful post-operative extubation after pre-oxygenation and close monitoring of oxygenation/cardiac status for 24 hours post-full recovery.6 In collaboration with physicians, a structured extubation plan was developed focusing on pre-extubation assessment/preparation, extubation execution, post-extubation management, and complication prevention.7 Extubation was planned for when inflammatory markers and respiratory function improved, aiming for transfer to general surgery 24 hours post-successful extubation. Post second intubation, increased airway secretions were managed with mechanical aspiration and maintaining fluid balance. After 3 days of ventilation, anti-infective, and supportive therapy, his spontaneous breathing, inflammatory markers, and gastrointestinal function improved. Ventilator support was stopped, and he received high-flow oxygen via the tube for 24 hours. Before the second extubation, arterial blood gas analysis under FiO2 40% showed PaCO2 38 mmHg and PaO2 147 mmHg, with an oxygenation index of 367. With smooth respiration, good oxygenation, and a negative leak test, the tube was removed at 09:12 on Oct 16 (POD 6, 5 days post second intubation), switching to mask oxygen. Secretions remained plentiful post-extubation, requiring suction every 2–3 hours, nebulization therapy, and mechanical vibration every 8 hours. His respiration was smooth, vitals stable, SpO2 98–100%, and secretions were manageable. Seven hours after extubation, arterial blood gas analysis under FiO2 45% showed PaCO2 34 mmHg and PaO2 192 mmHg, with an oxygenation index of 427. His vital signs remained stable without fever, suggesting that oxygenation impairment or overt uncontrolled pulmonary infection was unlikely to be the predominant cause of the subsequent extubation failure. He was transferred to general surgery 30 hours post-extubation. Given his cognitive impairment and poor cough effort, family was re-educated on encouraging activity, frequent back percussion before transfer, and detailed handover emphasized continued nebulization (bronchodilators/mucolytics), secretion clearance, SpO2 monitoring, and ABG checks. Anti-infective therapy continued as WBC and IL-6, though decreasing, remained elevated.
Third Extubation (Successful)
After transfer to the surgical ward on Oct 17 afternoon, he developed acute respiratory distress, lethargy (SpO2 79%, BP 155/90 mmHg, HR 144/min) at 06:36 on Oct 18, requiring emergency reintubation and readmission to ICU (Temp 39.8°C, BP 148/71 mmHg, HR 160/min, RR 43/min). CT post reintubation (Figure 2C) showed persistent lung abnormalities. The team analyzed causes for repeated extubation failure. Antibiotics were escalated to imipenem-cilastatin and vancomycin due to significant infection.
Care focused on inflammation control, enhanced mechanical vibration vomiting, strict head-of-bed elevation (30°-45°), and oral care every 6 hours. Shift assessments included mental status, secretions, infection markers, breath sounds, ventilator settings, and ABGs. Subsequent treatment led to markedly improved infection markers, afebrile status, smooth spontaneous respiration (SpO2 ≥98%), and good ABG oxygenation, albeit with persistent coarse breath sounds and copious oral secretions. Pre-extubation, fiberoptic bronchoscopy was repeated for secretion clearance and bacteriological sampling. Penehyclidine hydrochloride (0.5mg) was administered to inhibit secretions per order. On day 4 of the second ICU stay (POD 12), after a successful 1-hour spontaneous breathing trial and negative leak test, extubation was performed. Oxygen was administered via bilateral nasal cannula. Given the two prior failures, vital signs and secretion clearance were intensely monitored post-extubation. For safety, transfer from ICU occurred only after 48 hours of stable vitals. He was discharged 4 days after leaving ICU.
Discussion
Cases of AS complicated by intestinal volvulus and requiring surgery for intestinal obstruction are extremely rare. The multisystem nature of AS, including metabolic, sensory, cardiopulmonary, hepatic, renal, and gastrointestinal involvement, makes perioperative management particularly complex.6 To our knowledge, only one previous report described two siblings with AS and cecal volvulus; both required postoperative ICU care, and one eventually underwent tracheostomy because of difficult extubation.2 This prior experience is clinically relevant to the present case because it suggests that patients with AS undergoing emergency abdominal surgery may require more cautious postoperative airway assessment than patients with uncomplicated intestinal obstruction.
The repeated extubation failures in this patient should be interpreted in the context of both postoperative infection and AS-related functional vulnerability. Recent neurocognitive assessment has expanded the recognized phenotype of AS and reported buccofacial apraxia in affected patients.8 Buccofacial apraxia was not formally tested in the present patient, and therefore cannot be diagnosed retrospectively. However, the patient had intellectual disability, severe visual impairment, hearing loss, limited communication, and poor cooperation with cough and expectoration. These features may have functionally reduced his ability to coordinate effective coughing and airway clearance after extubation. This interpretation is consistent with recent evidence emphasizing that weak cough and ineffective airway clearance are important contributors to extubation failure and prolonged hospitalization in critically ill patients.9 Therefore, in future AS patients with postoperative ventilatory support, pre-extubation assessment should not be limited to oxygenation and spontaneous breathing trials, but should also include cough effectiveness, secretion burden, swallowing safety, and the patient’s ability to cooperate with airway clearance.
Pulmonary infection may have contributed to respiratory vulnerability in this case, but it was unlikely to be the sole or predominant cause of the repeated extubation failures. Before the first extubation, arterial blood gas analysis under FiO2 40% showed PaCO2 40 mmHg, PaO2 129 mmHg, and an oxygenation index of 323. After extubation, PaCO2 remained 40 mmHg and the oxygenation index was 237 under FiO2 37%, while respiration remained smooth at 15–16 breaths/min and chest radiography showed only mild bilateral pulmonary inflammation. Before the second extubation, the oxygenation index was 367 under FiO2 40%; seven hours after extubation, it increased to 427 under FiO2 45%, with stable vital signs and no fever. These findings suggest that oxygenation impairment or uncontrolled pulmonary infection was not the main explanation for the subsequent deterioration. In addition, no pathogen was detected in the abdominal drainage fluid or in bronchoalveolar lavage fluid obtained on October 14, and only a small amount of Klebsiella aerogenes (2+) was detected in bronchoalveolar lavage fluid on October 20. Therefore, the repeated extubation failures were more plausibly explained by a multifactorial process involving limited cooperation with cough and expectoration, secretion retention, possible aspiration risk, swallowing dysfunction, and AS-related functional vulnerability, with pulmonary infection acting as a contributing rather than dominant factor.
The final successful extubation was achieved only after infection control, repeated airway clearance, bronchoscopic secretion removal, pharmacologic reduction of excessive secretions, and more prolonged post-extubation ICU observation. This sequence suggests that infection management and airway clearance were both essential. Recent studies on extubation outcomes also support the concept that extubation failure is a multifactorial event, and that prediction should integrate respiratory mechanics, secretion burden, cough strength, neurological status, and systemic condition rather than relying on a single indicator.3,10,11 In the present case, the improvement in temperature, inflammatory markers, intestinal function, oxygenation, and secretion control created more favorable conditions for the third extubation. From a nursing perspective, this case highlights the importance of continuous vital-sign monitoring, dynamic interpretation of inflammatory markers, timely recognition of secretion retention, structured communication with physicians, and family-assisted cough guidance in patients with sensory and cognitive limitations.
Several limitations should be acknowledged. First, this is a single case report, and the causal relationship between AS, pulmonary infection, secretion retention, and extubation failure cannot be definitively established. Second, buccofacial apraxia, cough peak flow, diaphragmatic function, and instrumental swallowing assessment were not systematically evaluated, limiting our ability to quantify the relative contribution of impaired airway clearance. Third, although abdominal drainage fluid and bronchoalveolar lavage fluid samples were obtained, pathogen testing was largely negative, except for a small amount of Klebsiella aerogenes detected in bronchoalveolar lavage fluid on October 20. Therefore, microbiological results did not provide sufficient evidence to attribute the repeated extubation failures primarily to infection. Finally, because AS complicated by intestinal volvulus is extremely rare, the nursing strategies described here should be interpreted as individualized clinical experience rather than generalizable evidence. Nevertheless, this case suggests that postoperative extubation planning in AS should incorporate infection control, secretion management, cough cooperation, swallowing risk, and extended monitoring after extubation.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Guangdong Provincial People’s Hospital (approval number: KY2025-595-02). Informed consent was obtained from the patient. All methods were carried out in accordance with Declaration of Helsinki. The authors confirm that this case report adheres to the CARE (CAse REport) Guidelines. Furthermore, the patient has given written informed consent for the publication of their case details and any associated material.
Consent for Publication
The author obtained permission from the patient to publish this case report. The patient explicitly agreed to the anonymized reporting of their case details, in accordance with the Declaration of Helsinki and the Ethics Committee of Guangdong Provincial People’s Hospital ethical guidelines.
Author Contributions
Yelin Shen and Yuanting Chen are the co-first authors
Yelin Shen: Writing - original draft, Conceptualization, Supervision, Visualization
Yuanting Chen: Writing - original draft, Data curation, Resources,
Xia Fu: Methodology, Formal analysis
Wenxin Jiang: Project administration, Validation
Jiazhao Li: Writing - review & editing, Funding acquisition, Investigation, Software
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Guangdong Provincial Medical Research Fund (No. B2025436); Guangdong Provincial Medical Research Fund Project (No.B2021285).
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Waldman M, Han JC, Reyes-Capo DP, et al. Alström syndrome: renal findings in correlation with obesity, insulin resistance, dyslipidemia and cardiomyopathy in 38 patients prospectively evaluated at the NIH clinical center. Mol Genet Metab. 2018;125(1–2):181–9. doi:10.1016/j.ymgme.2018.07.010
2. Khoo EY, Risley J, Zaitoun AM, et al. Alstrom syndrome and cecal volvulus in 2 siblings. Am J Med Sci. 2009;337(5):383–385. doi:10.1097/MAJ.0b013e3181926594
3. Bansal V, Smischney NJ, Kashyap R, et al. Reintubation summation calculation: a predictive score for extubation failure in critically ill patients. Front Med. 2022;8:789440. doi:10.3389/fmed.2021.789440
4. Duan N, Lan YP. Application of ostomy care technology combined with negative pressure suction in patients with intestinal fistula. Contemporary Nurse. 2021;28(8):58–59.
5. Li D, Wang F, He QY. Research on the application of ostomy bag flushing and drainage device in home care of patients with intestinal ostomy. J Nurs Educ. 2021;36(20):1917–1919.
6. Tahani N, Maffei P, Dollfus H, et al. Consensus clinical management guidelines for Alstrom syndrome. Orphanet J Rare Dis. 2020;15(1):253. doi:10.1186/s13023-020-01468-8
7. Ren XL, Fan L, Tian JH, et al. Quality evaluation and content analysis of extubation guidelines for patients with tracheal intubation in ICU. Chin J Nurs. 2022;57(8):1001–1007.
8. Dassie F, Lorusso R, Benavides-Varela S, et al. Neurocognitive assessment and DNA sequencing expand the phenotype and genotype spectrum of Alström syndrome. Am J Med Genet A. 2021;185(3):732–742. doi:10.1002/ajmg.a.62029
9. Zhang SM, Muhetaer Y, Liu K. Assessments and exercises of cough strength in critically ill patients: a literature review. J Thorac Dis. 2025;17(2):1080–1102. doi:10.21037/jtd-24-1673
10. Torrini F, Gendreau S, Morel J, et al. Prediction of extubation outcome in critically ill patients: a systematic review and meta-analysis. Crit Care. 2021;25(1):391. doi:10.1186/s13054-021-03802-3
11. Zeng X, Chen X, Zhang Y, et al. Risk prediction models for extubation failure in critically ill patients: a systematic review. Front Med. 2025;12:1695394. doi:10.3389/fmed.2025.1695394
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.