Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Nursing Intervention and Summary of Evidence Pertaining to Neonatal Recurrent Hypoglycemia Induced by Terbutaline
Authors Wang MQ, Zhuang Y, Zheng YN
Received 7 June 2023
Accepted for publication 10 August 2023
Published 4 September 2023 Volume 2023:16 Pages 2677—2685
DOI https://doi.org/10.2147/DMSO.S422456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Meng-qin Wang,1,* Ying Zhuang,1,* Ya-ning Zheng2
1Department of Obstetrics, Nanjing Drum Tower Hospital, Nanjing, People’s Republic of China; 2Department of Gynecology Otolaryngology, Nanjing Drum Tower Hospital, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ya-ning Zheng, Email [email protected]
Background: Neonatal hypoglycemia (NH) is a common clinical symptom that can occur in both normal and critically ill neonates. The placenta is the site of material exchange between the mother and the fetus, a special organ shared by the mother and the fetus during pregnancy, and one of its important functions is to transfer nutrients from the mother to the fetus. Terbutaline is used to relax frequent uterine contractions before delivery, and it can penetrate the placental barrier and affect the normal decomposition of neonatal glycogen. The situation is neonatal hypoglycemia if not timely detection and interventions in time, the neonate may have recurrent hypoglycemia, leading to irreversible nervous system damage, such as neonatal hypoglycemic encephalopathy, and visual and cognitive impairment.
Case Report: The male neonate was a single fetus, with a birth weight of 3660 g and a length of 50 cm. The blood glucose at birth was 5 mmol/L, Apgar score was 9– 10, and body temperature was normal. The mother was healthy, was not diabetic, and had no other risk factors for neonatal hypoglycemia. She was injected with 0.25 mg of terbutaline 6 hours before delivery due to frequent uterine contractions. However, it was found that recurrent hypoglycemia occurred in the neonate even after adequate oral feeding.
Conclusion: We included evidence-based use of terbutaline 48 hours before delivery as a high-risk factor for hypoglycemia in the rooming-in neonatal hypoglycemia care program, and formulate the corresponding nursing process, with good effect.
Keywords: hypoglycemia, neonatal recurrent hypoglycemia, neonate, terbutaline
Background
It is normal for blood glucose levels (BGL) of healthy full-term neonates to show asymptomatic, transient, and mild decline in the first two hours of birth, caused by a continuous transition from placental glucose supply to intermittent breastmilk/formula feeding.1 Neonatal hypoglycemia is a relatively common metabolic disorder in newborns, defined as a lower than normal neonatal minimum blood glucose value, with a venous blood glucose <2.2 mmol/L. Recurrent or prolonged hypoglycemia in neonates can lead to irreversible nervous system damage, including neonatal hypoglycemic encephalopathy, visual and cognitive impairment, and so on if it is not detected and treated in time.2–4 Previous studies have found that low birth weight, preterm birth, multiple pregnancy, congenital metabolic disorder, maternal diabetes, and maternal drug treatment (β2-adrenergic agonist, sodium valproate, etc.) are risk factors for neonatal hypoglycemia.5,6
Terbutaline is used to prevent and delay uterine contraction before delivery, and can penetrate the placental barrier and affect the normal decomposition of glycogen.7 The incidence of neonatal hypoglycemia was increased in neonates delivered by mothers who had received β2-adrenergic agonists, while increased blood insulin and decreased blood glucose were found in neonates delivered by mothers who had received terbutaline. Several potential metabolic side effects of Terbutaline on the fetus. Recently, Epstein et al8 reported hypoglycemia in newborns after long-term administration of terbutaline. In addition, it was also shown that a single injection of terbutaline during labor had an effect on the blood glucose and insulin levels of mothers and infants, and terbutaline could cross the placenta and have an effect on the fetus.
It is possible that there are unknown risk factors for neonatal hypoglycemia despite the clinical practice of strict blood glucose monitoring for recognized high-risk infants with hypoglycemia, such as the use of Terbutaline. Furthermore, blood glucose assessment of the “healthy term neonate” may be inadequate, and more scientific tools are required to assist neonatal blood glucose monitoring.
In July 2022, a full-term neonate was delivered uneventfully, and the routine evaluation did not show any high-risk factors of hypoglycemia. However, we found that the neonate had recurrent hypoglycemia at 2 hours (2.5 mmol / L), 6 hours (1.8 mmol / L), 13 hours (2.2 mmol / L), and 22 hours (2.4 mmol / L) after birth. After close monitoring and medical intervention, the child was discharged in a stable condition. We have detailed our specific nursing experiences and interventions in the following sections.
Case Report
This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from patient guardians. The male neonate was a single fetus, with a birth weight of 3660 g and a length of 50cm. The blood glucose at birth was 5 mmol/L, PH value was 7.239, Apgar score was 9–10, and body temperature was normal. The neonate was admitted to the Neonatal Intensive Care Unit (NICU) due to “recurrent hypoglycemia” and was diagnosed with “neonatal hypoglycemia and perinatal infection.”
The mother of the neonate was 30 years old, who was admitted to the hospital due to irregular abdominal pain. The admission diagnosis was “38+5 weeks of gestation, pregnancy with uterine fibroids, pregnancy with hyperthyroidism”. The relevant examination was completed on admission. Findings were: The maternal cervix was not opened when vaginal exploration was done, and fetal adaptation to contractions was good in the oxytocin challenge test.
At 23:30 on the day of admission, the parturient was in excessive pain and could not sleep because of strong uterine contractions; the midwife conducted vaginal exploration and found that the cervix os of the parturient was the size of a fingertip. As instructed by the doctor, dolantin was injected intramuscularly to reduce the pain.
At 05:00, lumbar anesthesia analgesia was given to the parturient. At 05:09, the duration and interval of uterine contractions was 30s/2 min, accompanied by fetal heart deceleration. The parturient was given oxygen and lactated Ringer’s solution supplement, and as per the doctor’s advice, administered terbutaline 0.25 mg (Terbutaline) subcutaneously. Then, fetal heart rate restored to 122 beats/min, the duration and interval of maternal uterine contractions returned to 20s/3 min. At 11:00, the cervix os was completely opened and the fetal heart rate was normal. To prevent fetal distress, the midwife performed left episiotomy to expand the birth canal, and the fetus was delivered at 11:49.
Examination by pediatricians revealed no abnormal health conditions, and routine neonatal care was given. Peripheral blood glucose was measured at 2 hours after birth and found to be 2.5 mmol/L. Breastfeeding was initiated and strictly supervised by professional nurses to improve the neonate’s feeding. Surprisingly, the neonate’s blood glucose was only 1.8 mmol/L at 6 hours of age. What was more serious was that recurrent hypoglycemia (≤ 2.2 mmol/L) continued to remain after 10% glucose (30mL) intravenous treatment. Four hours after the glucose pumping was stopped, the child developed hypoglycemia (2.2 mmol/L) again. At 22 hours, the fourth episode of hypoglycemia was recorded and the level was 2.4 mmol/L, at which time the child developed shortness of breath and the respiratory rate was 70 times/min.
The neonate was then transferred to the NICU for continuous monitoring. Results of laboratory investigations: The neonate’s stool was normal, weight loss in 24 hours was 0.82%, white blood cells were 13.7 * 109/L, and C-reactive protein was 20.8 mg/L. The blood glucose was monitored every four hours as per the doctor’s advice and 10% glucose (30mL) + vitamin C (1g) + coenzyme A (100IU)+ vitaminB6 (0.1g)+ adenosine triphosphate (20mg) was pumped once. The respiratory rate improved and the blood glucose became more stable than before. On the day of discharge, the blood glucose was 3.6 mmol/L.
Finally, the blood glucose was stabilized and the neonate was discharged five days later.
The written informed consent was obtained from patient guardians.
Discussion
Summary of Evidence for Terbutaline Use 48 Hours Before Delivery as a Risk Factor for Neonatal Hypoglycemia
As per Shao et al9 and Jv et al research,2 high-risk factors of neonatal hypoglycemia are classified into maternal and neonatal factors. Maternal factors include: (1) Gestational diabetes; (2) Metabolic genetic disease in the mother; (3) Mother being treated with β-receptor blockers, antidepressants, dexamethasone, intravenous glucose infusion, etc., 24 hours before delivery.7 Neonatal factors include: small for gestational age, large for gestational age (LGA), preterm, intrauterine growth retardation, low birth weight, macrosomia, hypothermia, insufficient feeding, intrapartum hypoxia, polycythemia, meconium aspiration syndrome, and hemolytic anemia, amongst others.
Terbutaline is a β receptor agonist that can be used clinically to treat premature uterine contraction. The half-life test of the drug is 48–96 hours. The drug can pass through the placental barrier and 11% to 48% of the drug residues can be measured in the umbilical vein blood.10,11 This kind of drug can interfere with glycogen decomposition by blocking the effect of adrenaline. Before delivery, some drugs can reach the fetus through the placental barrier, leading to the risk of neonatal hypoglycemia. As early as 1979, Michael12 discovered that β sympathomimetic drugs (β Receptor agonists and β Receptor blockers) had significant metabolic effects on mothers and fetuses. Shimokawa et al13 found similar results in their retrospective study of sympathomimetic drugs on neonatal hypoglycemia. The Queensland Clinical Guidelines on neonatal hypoglycemia published in 2021 note that administering of terbutaline injection before delivery is considered as a high-risk factor for hypoglycemia. The best evidence related to the occurrence and precautions of neonatal hypoglycemia (receptor agonist) is as follows: ① When the parturient receives terbutaline within 48 hours before delivery, the neonate should be monitored as a high-risk infant with hypoglycemia1 (Level II evidence, Level A recommendation); ② Terbutaline is not recommended to be used for long-term abortion to prolong the delivery period, but can be used for short-term (48 hours) extension of pregnancy (Grade II evidence, Grade A recommendation);10 ③ For neonates at risk of hypoglycemia, they should be fed for the first time within 30 minutes after birth, or given skin-to-skin contact and fed for the first time within 1 hour (cesarean section), and then screened for blood glucose. If the first feeding is delayed, the child should be continuously monitored for 24–48 hours after birth, and the blood glucose concentration should be measured every 3–6 hours before feeding14 (Level II evidence, Level A recommendation); ④ Terbutaline received by the parturient within 48 hours before delivery as a uterine contraction inhibitor can increase the incidence of recurrent hypoglycemia in neonates8,12,15 (Level II I evidence, Level B recommendation).
Therefore, we propose to use the evidence summary in clinical practice in our department, and include terbutaline in the screening list of neonatal hypoglycemia high-risk factors (Table 1), improve the plan and process of neonatal hypoglycemia assessment and monitoring, and improve the quality of follow-up monitoring and impact evaluation.
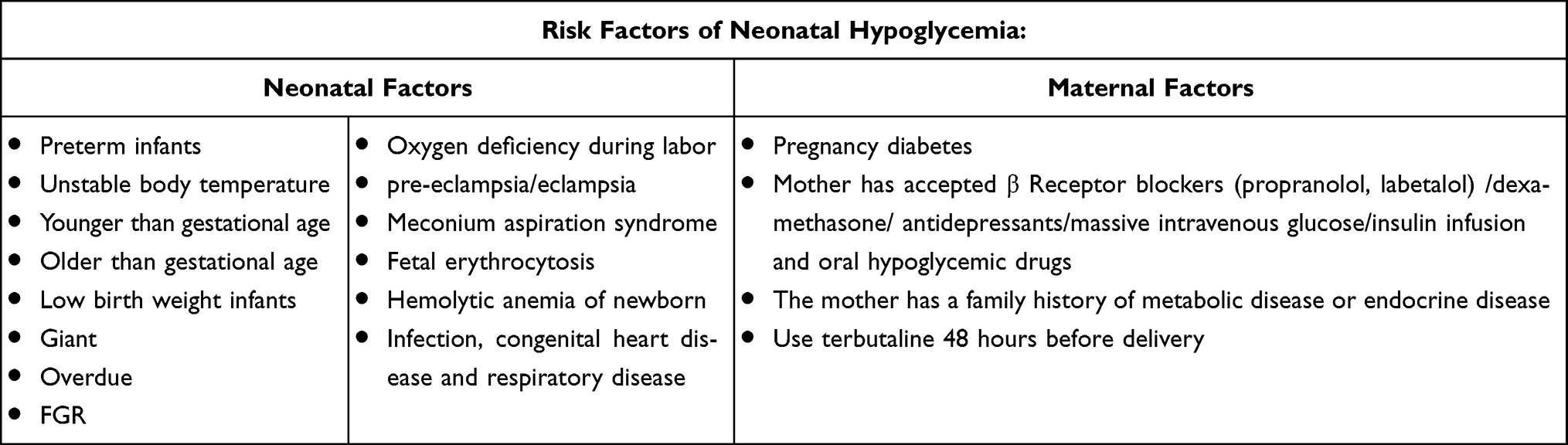 |
Table 1 Screening of Risk Factors of Neonatal Hypoglycemia |
Using the Breastfeeding Effectiveness Evaluation Scale to Improve the Feeding Impact of High-Risk Infants
Excessive hypoglycemia commonly occurs in neonates two hours after birth due to changes in the route of sugar supply,16 and it is difficult to ensure the effectiveness of feeding due to inexperienced feeding or physical discomfort of mothers. The timely initiation of lactation within 72 hours after delivery is particularly important for the subsequent sufficiency of breastmilk. Delay in the initiation of lactation can increase the risk of subsequent insufficient breastmilk and weaning. In addition, the delay in initiating lactation can also reflect as insufficient feeding of neonates, and the delay can be eliminated after 48 hours of gestation.17
In the case report we described earlier, the child was found to have hypoglycemia 2 hours after delivery, and 4 episodes of repeated hypoglycemia within 24 hours. We analyzed the causes, reviewed evidence-based practices, and utilized Bristol Breastfeeding Assessment Tool (BBAT)18 for evaluating the effectiveness of breastfeeding to improve the feeding impact of high-risk infants. The scale for evaluation of effectiveness of breastfeeding consists of four dimensions to assess the problems and effectiveness of breastfeeding: holding posture, receiving, sucking, and swallowing. Each dimension is rated on three grades: poor, medium, and good, with 0, 1, and 2 points, respectively. The maximum score is 8 points. If the score is less than 4 points, nurses need to intervene immediately to guide breastfeeding and improve neonate feeding.18
At the same time, the mother is given a checklist of breastfeeding problems, including the frequency of feeding, the duration of each feed, the quality of baby sucking, whether the baby is satisfied after feeding, and the baby’s stool and urine output. The mothers and their attendant family members can refer to the list to identify any problems that arise and inform the nurses, and the nurses can address these in time.
This scale does not include the feces and urine of neonates in evaluating the effectiveness of breastfeeding. According to the latest evidence, the feces and urine output in the first two days after delivery is neither sensitive nor specific, and even if the intake is insufficient, the baby may pass urine and stools. The correlation between infant intake and output is more reliable after three days of life (after the start of lactation). In this case, the urine and stool of the child were normal during the hypoglycemia period, but it could not be used as an indicator to evaluate whether the feeding was effective.
Update of the Nursing Plan for Neonates with Hypoglycemia with Rooming-in of Mothers and Infants, and Being on Alert for Recurrent Hypoglycemia of Neonates During Rooming-in
The Queensland Clinical Guidelines for Neonatal Hypoglycemia (2021) indicates that BGL< 2.6 mmol/L1 requires monitoring three or more times in a row; recurrent neonatal hypoglycemia can cause irreversible damage to the nervous system of the child and affect future growth and development. Therefore, we improved the neonatal hypoglycemia nursing process (see Figure 1). Identifying high-risk infants with hypoglycemia more comprehensively at an early stage and incorporating them into the hypoglycemia nursing process has considerable significance in reducing the occurrence of neonatal hypoglycemia and optimizing the management of rooming-in care: ① thorough identification of the high-risk factors of neonatal hypoglycemia, and improving the hypoglycemia nursing risk assessment process; ② Reminder for nurses to improve bedside education on breastfeeding for mothers of high-risk infants with hypoglycemia, implement early sucking and early initiation of breastmilk for neonates, and evaluate the impact of breastfeeding; ③ Train and evaluate mastery of neonatal hypoglycemia-related information among medical staff; ④ For children with neonatal hypoglycemia, remind the doctor to issue medical advice on blood glucose monitoring to avoid repeated and continuous hypoglycemia, thereby minimizing the failure of detecting the risk of the neonate in time; ⑤ Establish the blood glucose management and nursing process for high risk children with hypoglycemia in the postpartum rooming-in ward.
 |
Figure 1 Nursing process of neonatal hypoglycemia. Notes: Blood glucose monitoring refers to peripheral blood glucose (unit: mmol/L). |
In this case, the nurse strictly followed the updated neonatal hypoglycemia nursing process. With monitoring and treatment, the blood sugar of the baby was maintained at 3.2–6.3 mmol/L, breathing was stable, and the baby was fed a formula milk. The baby did not have convulsions, sweating, hypotonia and other symptoms. The second stool was normal, and the weight at discharge was 3730 g.
Improving Health Education for Family Members of Children with Hypoglycemia and Improving Family Support
Neonates are prone to hypoglycemia due to various factors pertaining to the mother and infant. Common clinical causes are premature delivery, hypothermia, improper feeding, mother having diabetes, and so on. With or without clinical symptoms such as tremors, sweating, irritability, weak sucking, weak crying, and even convulsions or nervous system damage, the condition requires additional treatment.
The rehabilitation of children with hypoglycemia requires not only the dedicated treatment and care of doctors and nurses, but also good follow-up care and support from families.19 Short-term hospitalization alone cannot meet the needs of neonate growth and development, and long-term family care is important.20,21 The traditional nursing plan consists of offering health education orally and through written materials. This model is relatively effective for parents to master the theoretical knowledge of childcare, however, the daily care of children requires more practical skills, especially for children with hypoglycemia. In developed countries such as the United States, neonatal intensive care units are open to parents, encouraging mothers to accompany children in hospitals and address their daily care.
Nurses play an important role as educators and facilitators. Research shows that when parents become the main caregivers of children, they can improve their ability to take care of children, so that when children return home, the parents have also developed adequate care abilities. Although the child is treated in the neonatal intensive care unit, when the condition is stable, the child is returned to the same room with the mother, so that the family can participate in the daily care of the child aided by scientific family health inputs and supervised by medical care professionals.19,20
The concerned nurse demonstrates the nursing inputs and guides the parents in aspects related to the daily care of the neonate, including bathing the neonate, umbilical cord disinfection, kangaroo care, breastfeeding, and the handling of neonatal problems such as neonatal cough and neonatal hypoglycemia. At the same time, the nurse again goes through the checklist of neonate feeding problems with the mother and family members to improve their recognition of these issues, thereby preventing the improper feeding of neonates or the occurrence of hypoglycemia that cannot be detected in time. In this way, the nurse facilitates and improves family support to reduce neonatal complications.
Paying Attention to Psychological Counseling and Addressing Negative Emotions in Parents
In the current case, the neonate suffered repeatedly from episodes of hypoglycemia, with 4 such occurrences in 24 hours and shortness of breath, which worried the mother and family. The neonate in this case was admitted to the NICU two days after birth due to recurrent hypoglycemia and perinatal infection, and the mother and baby were separated for a long time. In order to reduce parents’ separation anxiety and worry about the condition of the child, the concerned nurse often comforted the mother at the bedside to explain the conventional nursing and skills required for caring for the neonate, and encouraged the mother to express breastmilk every 2–3 hours and sent it to the NICU to feed the child, reducing the mother’s worries. At the same time, when the neonate’s course of treatment was over and his condition was stabilized, the nurse encouraged the mother to touch the child and participate in the daily routine care of the neonate. Seeing the condition of the child becoming more stable day by day, and improving their own skills of caring for the neonate with inputs from the nurse, mothers and family members can gradually gain more confidence and reduce their negative emotions.
Terbutaline is a β receptor agonist that can be used clinically to treat premature uterine contraction. The half-life test of this receptor agonist is 48–96 hours, and 11% to 48% of the drug residue can reach the umbilical vein blood through the placental barrier.15,16 It can be used clinically as an inhibitor of frequent uterine contractions in pregnant women. This kind of drug can interfere with glycogen decomposition by blocking the effect of adrenaline. Before delivery, some drugs can reach the fetus through the placental barrier, increasing the risk of neonatal hypoglycemia.
In this case, due to frequent uterine contractions, the parturient was frequently injected with terbutaline to inhibit uterine contraction within 7 hours before delivery, and no other hypoglycemia-influencing factors were found. The neonate had hypoglycemia once an hour after birth, and then had hypoglycemia three times within 24 hours. The latest clinical guidelines on neonatal hypoglycemia, the Queensland Clinical Guidelines released in 2021, mentions terbutaline injection before delivery as a high risk factor for hypoglycemia. Michael and Shimokawa et al12,13 reached similar conclusions, and suggested that β receptor agonists have significant metabolic effects on mothers and fetuses. However, from the evidence-based review, we found that the latest practice guidelines in China and expert consensus2,9 did not indicate β receptor agonists into the high-risk factors of neonatal hypoglycemia, especially the use of terbutaline 48 hours before delivery that it is found increase the incidence of recurrent neonatal hypoglycemia.
Therefore, to ensure the safety of neonates and prevent recurrent hypoglycemia of neonates, we propose to use evidence-based clinical practices in our department, such as including terbutaline in the screening list of high-risk factors of neonatal hypoglycemia, improving our process of neonatal assessment and monitoring of hypoglycemia, and improving the quality of follow-up monitoring and effect evaluation.
Relevant guidelines in China have established strict procedures for blood glucose monitoring of neonates with high risk factors following hypoglycemia, including blood glucose monitoring every hour. However, for general hospitals with a large proportion of high-risk pregnant women and serious illness, this has led to a serious burden on human resources and medical resources. In addition, frequent vein/peripheral skin puncture of neonates not only increases the pain of neonates, but also increases the negative emotions of parents.
In this study, the OGTT test of the mother of the child was normal, and the blood glucose monitoring in the hospital was within the normal range. The mother denied the genetic history of endocrine and Metabolic disorder. Analyze the case without neonatal factors, excluding other high-risk factors of the mother, and consider β Receptor blockers can interfere with Glycogenolysis by blocking the action of adrenaline, so, we explore the effect of terbutaline on neonatal hypoglycemia. The mother of the child was injected with terbutaline less than 6 hours before delivery, and the drug has been proven to have a half-life of 48 to 96 hours. The drug passes through the placental barrier and can measure 11% to 48% of the drug residue in umbilical vein blood. Due to the conversion of glycogen supply at birth, the blood sugar of newborns is relatively unstable, and their blood sugar is more susceptible to the influence of terbutaline. So, the hospital has included terbutaline as a high-risk factor for neonatal blood glucose screening and established the process for blood glucose monitoring and devised a nursing plan for normal neonates and hypoglycemic high-risk neonates when blood glucose is greater than or equal to 2.6 mmol/L with/without symptoms, less than 2.6 mmol/L with/without symptoms, 2.0–2.6mmol/L, and less than 2.0 mmol/L (A detailed evaluation of blood glucose frequency and strategy is shown in Figure 1), and apply it in clinical practice to further explore its practicability and feasibility.
The dynamic blood glucose monitor, a non-invasive and continuous automatic blood glucose monitoring device, is widely used to check adult blood glucose. One aspect to explore is whether this can be used to monitor the blood glucose of neonates with low blood glucose and high risk, as it can reduce puncture and nursing workload. Relevant research in the future can focus on the practicability of using dynamic blood glucose meters in neonates.
Conclusion
Hypoglycemia is one of the most common metabolic disorders in neonates. If hypoglycemia occurs repeatedly or continues to occur without timely detection and treatment, it can lead to irreversible neurological damage. Terbutaline can block the effect of fetal adrenaline through the placental barrier, interfere with glycogen decomposition, and increase the risk of neonatal hypoglycemia. Therefore, based on evidence, we included the use of terbutaline 48 hours before delivery as a high-risk factor for hypoglycemia in the maternal-infant rooming-in neonatal hypoglycemia care program. We also introduced several improvements in our nursing care program: evaluation of the effectiveness of breastfeeding and ensuring the feeding effect of high-risk infants; updating the nursing plan of hypoglycemia for neonates based on rooming-in of mothers and infants, and being alert to the occurrence of recurrent hypoglycemia for neonates during rooming-in; improving health education for family members of children with hypoglycemia and improving family support; paying attention to psychological care, reducing negative emotions of parents, and promoting the health of mothers and children.
Abbreviations
NH, Neonatal hypoglycemia; BGL, blood glucose levels; BG, blood glucose; NICU, Neonatal Intensive Care Unit; ECG, Electrocardiogram; H, hours; FGR, Fetal growth restriction.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Nanjing Drum Tower Hospital. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from patient guardians.
Consent for Publication
The patient guardians signed a document of informed consent to publish case details, including any clinical details and/or images.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Project of Chinese hospital reform and development institute, Nanjing University Aid project of Nanjing drum tower hospital health, education & research foundation (NO: NDYG2021054).
Disclosure
The authors declare that they have no competing interests.
References
1. Queensland Health. Queensland clinical guidelines: hypoglycaemia-newborn. Guideline No.MN19.8-V7R24. Queensland Health; 2019.
2. Group of Neonatology, Pediatric Society, Chinese Medical Association. Expert consensus on standard clinical management of neonatal hypoglycemia in China (2021). Zhongguo Dang Dai Er Ke Za Zhi. 2022;24(1):1–13. Chinese. doi:10.7499/j.issn.1008-8830.2108061
3. Thornton PS, Stanley CA, De Leon DD, et al.; Pediatric Endocrine Society. Recommendations from the pediatric endocrine society for evaluation and management of persistent hypoglycemia in neonates, infants, and children. J Pediatr. 2021;167(2):238–245. doi:10.1016/j.jpeds.2015.03.057
4. Wight N, Marinelli KA; Academy of Breastfeeding Medicine. ABM clinical protocol #1: guidelines for blood glucose monitoring and treatment of hypoglycemia in term and late-preterm neonates, revised 2014. Breastfeed Med. 2014;9(4):173–179. doi:10.1089/bfm.2014.9986
5. Williams AF. Hypoglycaemia of the newborn: a review. Bull World Health Organ. 1997;75:261–90.13.
6. Adamkin DH. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics. 2011;127:575–579. doi:10.1542/peds.2010-3851
7. Bateman BT, Patorno E, Desai RJ, et al. Late pregnancy β blocker exposure and risks of neonatal hypoglycemia and bradycardia. Pediatrics. 2016;138(3):e20160731. doi:10.1542/peds.2016-0731
8. Epstein MF, Nicholls E, Stubblefield PG. Neonatal hypoglycemia after beta-sympathomimetic tocolytic therapy. J Pediatr. 1979;94(3):449–453. doi:10.1016/S0022-3476(79)80600-9
9. Shao XM, Ye HM, Qiu XS. Practical Neonatology.
10. Hyagriv NS, Steve C. Inhibition of acute preterm labor; 2020.
11. Arieh R, Joseph A, Garcia-Prats A. Infants of women with diabetes; 2019.
12. Westgren M, Carlsson C, Lindholm T, Thysell H, Ingemarsson I. Continuous maternal glucose measurements and fetal glucose and insulin levels after administration of terbutaline in term labor. Acta Obstet Gynecol Scand Suppl. 1982;108:63–65. doi:10.3109/00016348209155348
13. Shimokawa S, Sakata A, Suga Y, et al. Incidence and risk factors of neonatal hypoglycemia after ritodrine therapy in premature labor: a retrospective cohort study. J Pharm Health Care Sci. 2019;5:7. doi:10.1186/s40780-019-0137-3
14. Rozance PJ. Pathogenesis, screening, and diagnosis of neonatal hypoglycemia; 2019.
15. Ingemarsson I, Westgren M, Lindberg C, Ahrén B, Lundquist I, Carlsson C. Single injection of terbutaline in term labor: placental transfer and effects on maternal and fetal carbohydrate metabolism. Am J Obstet Gynecol. 1981;139(6):697–701. doi:10.1016/0002-9378(81)90489-0
16. Wang L, Lu D, Wu WL, Zheng DT. Neonatal hypoglycemia and its treatment management. J Clin Pediatr. 2016;34(1):55–58.
17. Feldman-Winter L, Kellams A, Peter-Wohl S, et al. Evidence-based updates on the first week of exclusive breastfeeding among infants ≥35 weeks. Pediatrics. 2020;145(4):e20183696. doi:10.1542/peds.2018-3696
18. Balaguer-Martínez JV, Esquivel-Ojeda JN, Valcarce-Pérez I, et al. Translation to Spanish and validation of a scale for the observation of breastfeeding: the Bristol Breastfeeding Assessment Tool. An Pediatr. 2022;96(4):286–293. doi:10.1016/j.anpedi.2021.04.012
19. Meng JW, Chen H, Li B, et al. The influence of family centered nursing program on the care ability of parents of premature infants. J Nurs Sci. 2017;32(9):5–7.
20. Wang Y, Zhang J, Fan XH. Research progress on the influence of parent-child interaction on neuropsychological development of premature infants. J Nurs Sci. 2016;31(7):102–105.
21. Zheng HR. Effect of transitional nursing service on growth and development of discharged premature infants. J Nurs Sci. 2011;26(23):29–30.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.