Back to Journals » Journal of Pain Research » Volume 16
Nursing Dilemmas in Chemotherapy-Induced Peripheral Neuropathy: A Qualitative Study of a Tertiary Hospital in China
Authors Fan JX ![]() , Hu YC
, Hu YC ![]() , Chen X
, Chen X ![]() , Li Y
, Li Y
Received 21 February 2023
Accepted for publication 10 June 2023
Published 6 July 2023 Volume 2023:16 Pages 2299—2308
DOI https://doi.org/10.2147/JPR.S409580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Jia Xin Fan,1,2,* Ya Chen Hu,1,2,* XinXin Chen,1,2,* YuMei Li2
1School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Department of Nursing, Shanghai Pulmonary Hospital, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: YuMei Li, Department of Nursing, Shanghai Pulmonary Hospital, Tongji University, No. 507 Zheng Min Road, Shanghai, 200433, People’s Republic of China, Tel +86 13917922290, Fax +86 021-65115006-2185, Email [email protected]
Purpose: This study investigated the experience of oncology nurses caring for chemotherapy-induced peripheral neuritis patients.
Patients and Methods: Through phenomenological research method, 11 nurses in a tertiary hospital in Shanghai were interviewed using face-to-face semi-structured interviews. Data analysis was conducted with the thematic analysis approach.
Results: This analysis revealed the experiences of oncology nurses in caring for patients with CIPN and identified three themes: 1) stress in the nursing of CIPN (inadequate knowledge of CIPN among oncology nurses, oncology nurses’ CIPN nursing skills need to be improved, negative emotions of oncology nurses at work); 2) environmental dilemmas in nursing of CIPN (lack of effective care norms, busy schedules, doctors pay little attention to CIPN); 3) oncology nurses’ desire to improve their knowledge of CIPN to meet care needs.
Conclusion: Based on the perspective of oncology nurses, the care dilemma of CIPN is mainly influenced by individual and environmental factors. It is recommended to enhance the attention of oncology nurses to CIPN, set specific and feasible training courses, explore CIPN assessment tools that meet our clinical practice, and construct CIPN care programs to improve CIPN clinical care ability and reduce patient suffering.
Keywords: lung cancer, nursing experience, qualitative research, qualitative study
Introduction
The World Health Organization (WHO) reports that cancer has become an important contributing factor to disease burdens.1 Although chemotherapy technology has significantly prolonged cancer patient survival, it also causes a variety of long-term side effects, such as gastrointestinal reactions: nausea, vomiting, diarrhea; Bone marrow suppression: leukopenia, granulocyte, thrombocytopenia; Hair loss; Nephrotoxicity, hepatotoxicity, cardiotoxicity and neurotoxicity.2–6 Patients who suffer from chemotherapy-induced peripheral neuropathy (CIPN) often stop treatment or have a poor prognosis as a result of this neurotoxic side effect.7–9
CIPN is mainly manifested as numbness, tingling and paresthesia at the extremities, which is distributed in a “glove-sock” shape.10 In severe cases, it will cause physical dysfunction, the risk of falls and self-care defects, and affect the quality of life of patients.11 It has been reported that the incidence of CIPN in cancer patients can reach 68.1% in the first month after chemotherapy,3 and more than 20–30% of patients will acquire chronic CIPN, with related symptoms lasting for half a year.12 The factors closely related to the high incidence of CIPN are mainly divided into drug factors and individual factors. First of all, chemotherapeutic drugs can easily cause CIPN include taxanes, platinum drugs, proteasome inhibitors, vinca alkaloids and thalidomide, among which oxaliplatin (84%)13 and paclitaxel (59–87%)14 have the highest incidence of CIPN. Additionally, smoking, alcohol abuse, obesity, old age (>75 years), diabetes in the family or history of hereditary neuropathy, renal insufficiency, hypothyroidism, vitamin deficiency, human immunodeficiency virus (HIV) infection, autoimmune rheumatism, and underlying neuropathy all contribute to a high prevalence of CIPN.15
Researchers have extensively studied epidemiology and management strategies for CIPN, primarily focusing on preventive medicine,16–19 while the nursing is limited. Nurses play an important role in managing symptoms as disease caregivers.20 It is reported that oncology nurses lack the knowledgeand the ability to manage CIPN.21 The qualitative method allows the researcher to explore the essence through phenomena and is more likely to portray inner feelings. To provide a reference base for subsequent studies, this paper explores the experience of oncology nurses caring for CIPN patients, discussing hidden influencing factors.
Materials and Methods
Study Design
A purposive sampling method was used to select 11 oncology nurses from a tertiary hospital in Shanghai for semi-structured interviews in March 2022, with the sample size until the data were saturated and no new information emerged.
Inclusion criteria: ① registered nurses who had been working in oncology for more than 2 years; ② possessing a nurse’s qualification certificate; ③ giving informed consent and voluntarily accepting the interview; Exclusion criteria: ① trainees; ② nurses who were not on duty due to vacation. The names of the interviewed subjects were blurred according to serial numbers N1-N11 (Table 1). The study was reviewed by the ethics department of Shanghai Pulmonary Hospital (K22-239Y), and informed consent was obtained from the respondents.
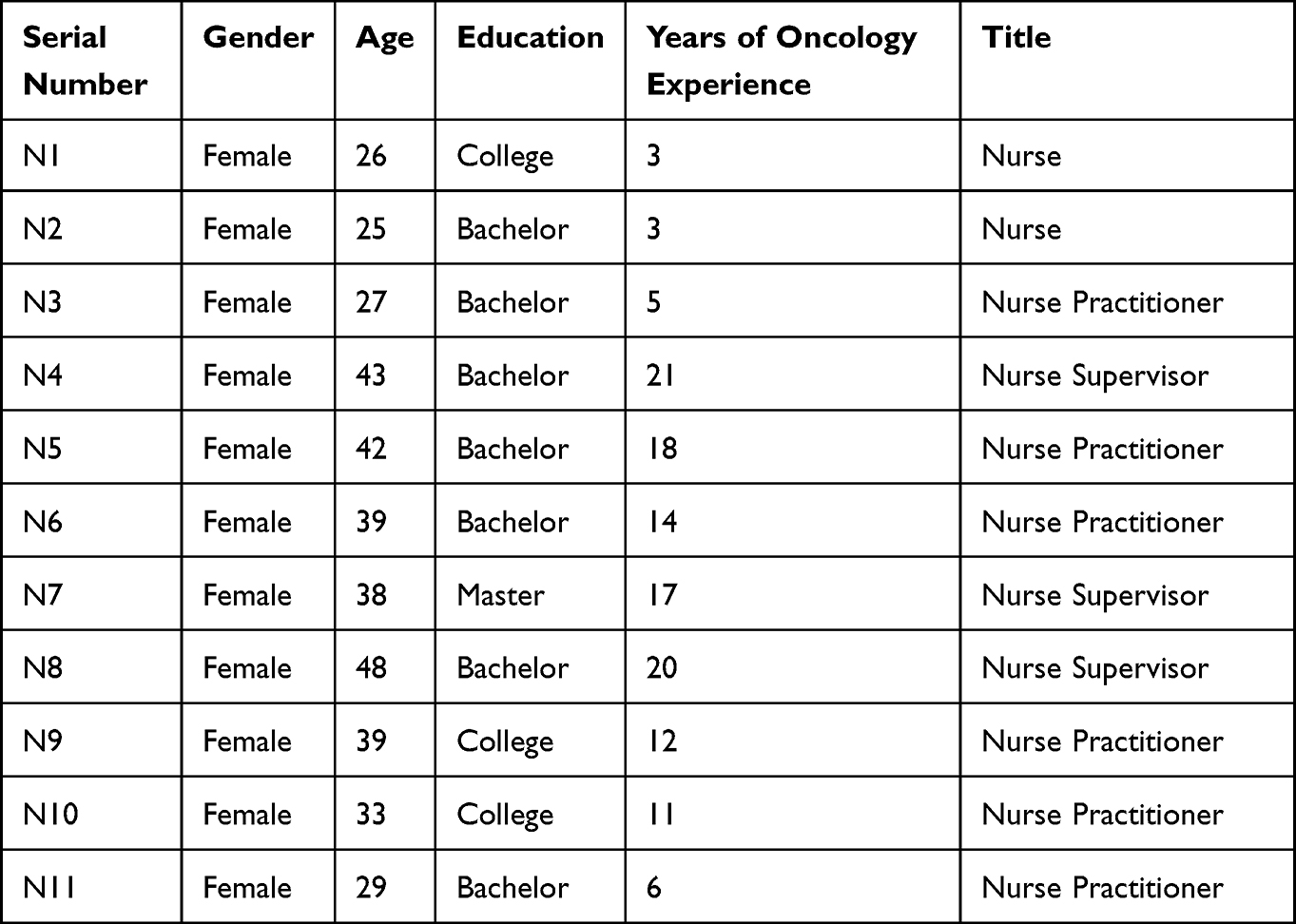 |
Table 1 Basic Information of Interviewees |
Data Collection
In this study, a phenomenological research method was used to explain the purpose, significance, and methods of this study to the interviewees before the interview, and their informed consent that included publication of anonymized responses was obtained. In order to protect privacy, serial numbers were used instead of the names of the interviewees.These interviews were conducted in a quiet environment, such as the office of the oncologist at the researcher’s affiliated hospital, to minimize interruptions and to protect patient privacy. The interviews lasted approximately 30 minutes. Personal information (age, gender, position, duration of employment, and education) of the oncology nurses was collected by the researcher at the end of the interviews.Theoretical saturation was considered to be reached when it was determined that there were no new interviews and that the content of the 10th and 11th interviews was repeated. In this study, an interview outline was developed through a literature review, and two nurses were pre-interviewed before the formal interview, and subject members revised the interview outline based on the interview results. The main contents of the interview outline were: ①How much do you know about CIPN? ②Can you describe the situation of the CIPN patient you recently cared for? ③What was your inner feeling at that time? ④How did you cope with the situation? ⑤What difficulties have you encountered in your caregiving work? ⑥What are your related needs or suggestions?After recording with the informed consent of the interviewee, the researcher should encourage the interviewee’s willingness to express, listen carefully to the relevant information, and follow up if there is any confusion, while observing the subtle changes in facial expression, voice tone and body movements until the interview information is saturated.
Data Analysis
The interview recordings was transcribed within 24 hours of the interview, and the recordings were not modified or deleted to ensure the authenticity, and the data were imported into NVivo 7.0 software for collation and analysis. Colaizzi 7-step analysis method in phenomenology was used to analyze the data (Table 2). Firstly, basic information about oncology nurses’ experiences of CIPN care was obtained through careful and repeated reading of the text by researchers Fan and Hu, respectively, and then meaningful statements related to oncology nurses’ experiences of CIPN care were identified through careful analysis and coded for repeated viewpoints.Secondly, the initial themes were formed by coding clusters through analysis and discussion by the research team members, and the final themes were constructed by repeated comparisons to identify and classify similar viewpoints, and the accuracy of the results was verified to the respondents.
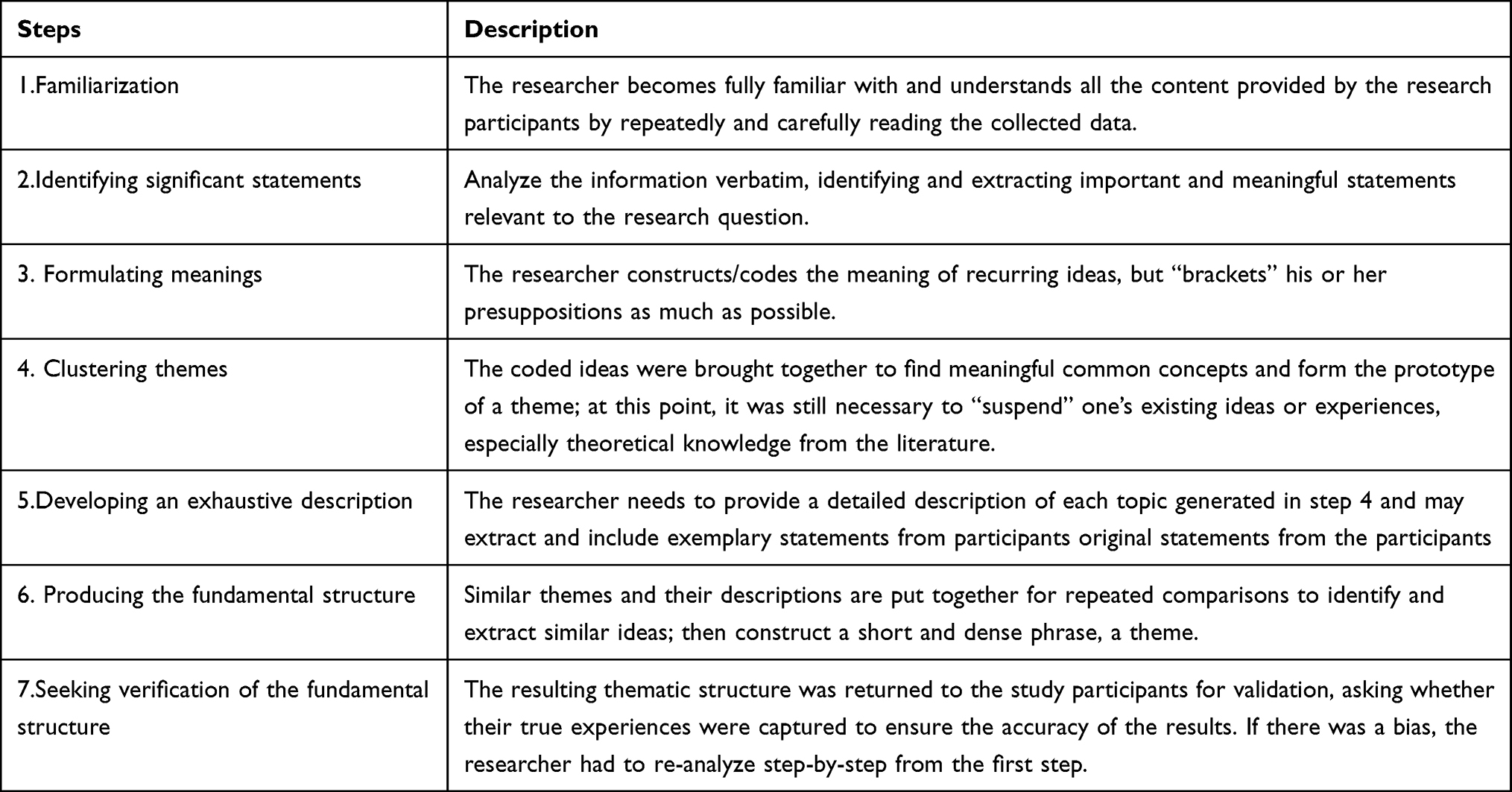 |
Table 2 Colaizzi-7-Step and Description |
Results
In this interview, no new themes emerged when the number of interviewees reached 10, and no new information emerged after continuing the interview for 1 case, so the information was considered saturated. A total of 11 participants were selected, and the age distribution was 23−48 years old (34.90±2.55) with a working time frame of 3–21 years (11.82±2.04).After summarizing and analyzing the text content through the researcher Fan and Hu, a total of 3 themes and 8 subthemes were obtained, the themes and sub-themes are shown in Table 3 and Figure 1.
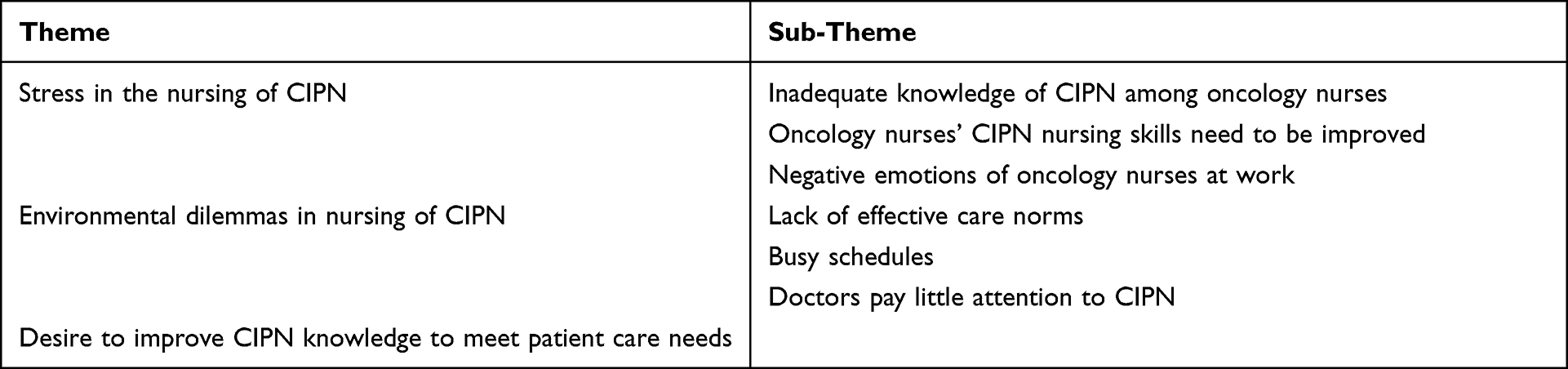 |
Table 3 Themes and Sub-Themes |
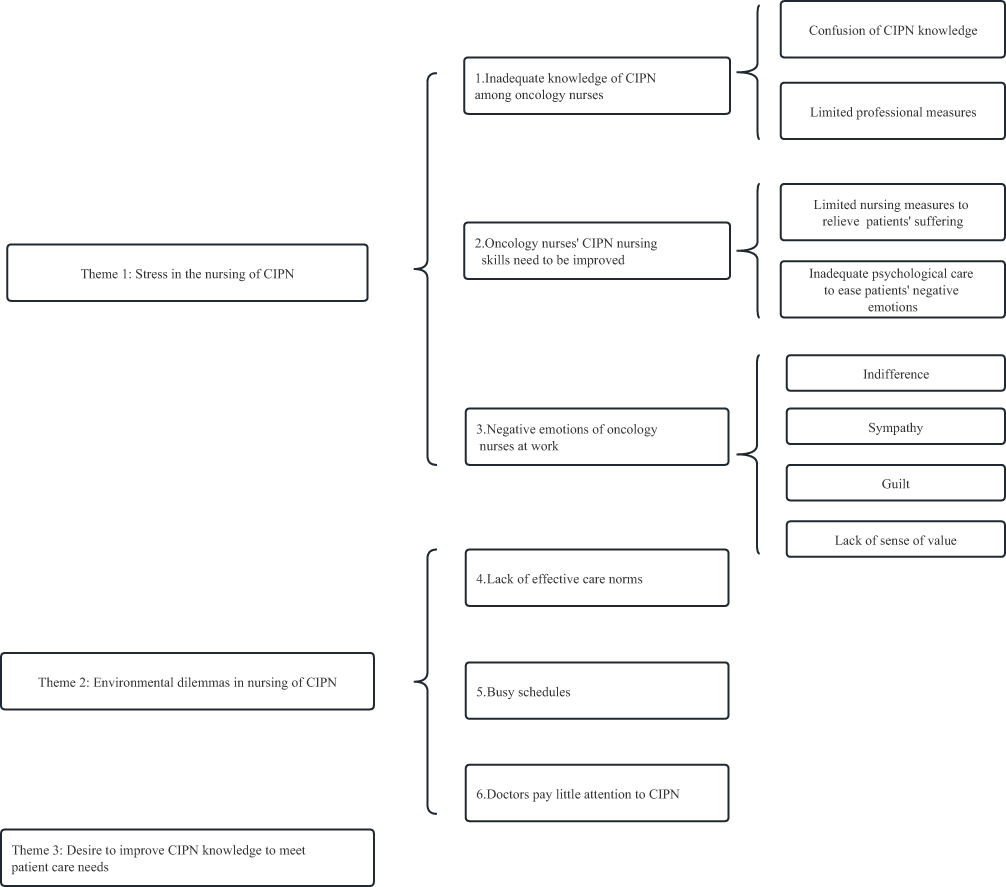 |
Figure 1 Themes and sub-themes. |
Theme 1: Stress in the Nursing of CIPN
Inadequate Knowledge of CIPN Among Oncology Nurses
CIPN often presents with numbness, tingling, muscle spasm, and sensory abnormalities in the extremities, and some patients also experience cold irritation, and the complexity of its symptoms is often difficult to distinguish. When nursing staff lack the relevant knowledge, the quality of nursing services is bound to be affected.
① Confusion of CIPN knowledge
When talking about CIPN, three nurses interviewed in this study would confuse it with other diseases.
N1:Patients say their hands hurt like pins and needles, and I am not sure if it is cancer pain or neuralgia, because they all hurt after having cancer.
N2:Some patients tell me that his hand is numb and painful, and I think it is phlebitis, so I choose the opposite hand for infusion.
N5:I don’t know anything about this disease, and I can’t explain it to patients when they ask.
N9:It sounds like metastatic pain, which I don’t really understand, cancer is usually accompanied by cancer pain, not necessarily neuritis. One nurse confessed not being familiar with the basics of the disease.
② Low awareness of assessment
Assessment of neurotoxicity is directly related to patient prognosis and occupies an important position in disease management. Eight caregivers in this study self-reported that they had not assessed CIPN symptoms.
N8:Their symptoms are usually mild and they get better naturally without chemotherapeutic drugs, without assessment.
Oncology Nurses’ CIPN Nursing Skills Need to Be Improved
CIPN nursing care is often limited to primary care measures, so nurses often feel stressed at work because they are unable to deal with the patient’s suffering.
① Limited nursing measures to relieve patients’ suffering
The lack of nursing measures to deal with neurotoxicity makes nurses seek only more specialized help.
N4:There seems to be no nursing measures to effectively relieve it, it’s an adverse reaction to the drug.
N6:I don’t know what to do, I have to hurry and inform the doctor, they know more than us.
N10:CIPN patients are suffering and I want to help them, but I don’t know how to do it, so I recommend patients to go to the psychological clinic in our hospital.
② Inadequate psychological care to ease patients’ negative emotions
Under the long-term torture of cancer and neurotoxicity, patients often show negative emotions such as depression and sadness, which inevitably reduce the quality of chemotherapy. Interviewees indicated that they should pay attention to patients’ psychological state in routine care to help them ease their sadness, improve the treatment effect and reduce the painful experience. However, when talking about psychological nursing skills, the nurses interviewed often stopped at verbal reassurance and did not mention how to communicate effectively and how to meet patients’ inner demands to enhance the sense of meaning in life.
N2:They are pessimistic and feel that there is no hope for treatment, and I often comfort them.
N3:After I talked with the patients, I found that they were sad, so I approached the teachers in the psychological group to communicate with them.
N4:I tell the patients that this is a normal reaction, that we are all the same, and that there is no need to be too nervous.
Negative Emotions of Oncology Nurses at Work
When caring for patients with CIPN, oncology nurses experienced mixed emotions.
① Indifference: respondents who had worked for more than 10 years considered CIPN to be an adverse reaction and did not need to pay much attention to it.
N6:I don’t feel anything, their numbness is mild and does not affect their daily life, I think it is a normal drug reaction and will naturally get better without medication.
② Sympathy: When patients report symptoms to caregivers, caregivers who have worked for a shorter period of time are more likely to feel sympathy.
N1:I feel sorry for them and worry about them. If I can fix it I will help.
N7:Many lung cancer patients would self-report numbness in their fingers and toes after several times of chemotherapy, and we understand very well that this is a side effect of chemotherapy drugs, and psychologically we sympathize with them very much, and also instruct to wear gloves and pay attention to keep warm, etc., but there is no better way to help them solve the numbness problem.
③ Guilt: Interviewees reported being unable to cope with CIPN episodes and were filled with guilt.
N11:I am also ashamed of the fact that they are usually asked to consult their doctors on how to deal with it, but what can I do?
④ Lack of sense of value: two nurses in this study reported starting to question their professional value.
N9:Over time, patients and families say that nurses don’t know this and go straight to the doctor. I was sad to hear that and kind of regret choosing this career.
N11:As the same health care worker, I sometimes doubt my own ability is not as good as doctors.
Theme 2: Environmental Dilemmas in Nursing of CIPN
Lack of Effective Care Norms
Respondents felt that they were often at a loss when working due to the lack of systematic and comprehensive nursing norms.
N4:Unlike cancer pain, there is no specific protocol or norm for CIPN, I don’t know the specific process, such as when to assess, how to assess, what to assess, what to follow up, how to do health education, what indications to observe, whether to use follow up or not, I don’t I only rely on word-of-mouth among colleagues to do basic care.
N7:Because there is no specific assessment standard, it is really neglected, and more importance is attached to the assessment of cancer pain and nausea and vomiting in clinical practice.
Busy Schedules
The workload makes nurses too busy to implement refined care.
N4:Patients usually stay for only two or three days and they have mild symptoms and are discharged in a few days.
N6:Of course I want to help them, but clinical work can’t be done that meticulously,and acupressure needs professional TCM doctors.
N10:I have to take care of a lot of patients, and be busy all day with infusions, so I really don’t have time to do it (sigh and rub temples).
Doctors Pay Little Attention to CIPN
At present, doctors are more concerned about patients’ survival and chemotherapy effects, and pay little attention to CIPN.
N8:After chemotherapy, our nurses will ask patients if they feel numbness in their hands and feet, and if they do, we promptly notify the doctor and ask him or her what to do, and he or she will say that it will slowly ease after stopping chemotherapy and no special treatment is needed.
N11:I saw that when the doctor checked the room and asked the patient if there was numbness in the hands and feet, and the patient said yes, the doctor would prescribe nerve-nourishing drugs for the patient to take orally, such as multivitamin tablets, and so on. But rarely do I see the doctor come in to check and ask about this symptom before the next chemotherapy.
Theme 3: Desire to Improve CIPN Knowledge to Meet Patient Care Needs
Respondents expressed that their low level of knowledge reserve could not meet the needs of their work, and they were eager to acquire knowledge in multiple ways to reduce patients’ disease burden.
N4:I will learn in WeChat public or webcast classes, and would like to attend lectures or popular science activities to learn about relevant knowledge so that patients can gain tangible benefits in health promotion.
N6:It would be good if there is relevant training in the department or hospital, so that you can learn systematically.
Discussion
Strengthening the Professional Knowledge and Assessment Awareness of Oncology Nurses to Improve the Quality of Nursing Services
The results of this study showed that the disease knowledge and management level of the nurses interviewed was low, mainly in terms of unclear concepts and knowledge confusion, which was consistent with the results of Binner.22 A cross-sectional study of 148 oncology nurses by Nijmeh23 showed that 58.8% of the subjects thought that CIPN assessment was necessary, but only 40.8% of the nurses had received relevant instruction, and most of them The majority felt that they had significant knowledge and practice deficits. Studies have shown that knowledge level, as one of the core competencies of oncology nurses, and nursing staff with extensive expertise are more competent in CIPN care.24 Knowledge-attitude-behavior theory (KAP) refers to the idea that individuals can form beliefs and eventually achieve behavioral change through repeated reflection after acquiring knowledge,25 and this theory has made an important contribution to the long development of nursing. Hospital administrators can hold relevant trainings based on this theory to enhance the professional level of nursing staff, clarify professional knowledge through teaching, and contextual training to achieve the integration of knowledge and practice. In addition, oncology nurses should be encouraged to improve their independent learning ability and take the initiative to expand their learning pathways, including expert lectures and continuing education courses.
Since the disease cannot be prevented, nursing staff should strengthen the awareness of assessment, focusing on high-risk groups (the elderly, smokers and alcoholics, those with high BMI, low creatinine clearance and low serum albumin, those taking cardiovascular and opioid medications, and those with comorbid underlying diseases,26,27 and achieve early, timely, and continuous assessment. In addition, there are numerous assessment tools for CIPN, commonly such as the Common Terminology Criteria for Adverse Events, the Total Neuropathy Score, and the CIPN Quality of Life Score, and nursing staff should determine the assessment tools for systematic assessment according to the clinical practice setting in their country, and the assessment of neurotoxicity mainly includes two parts: subjective assessment and objective assessment, which aims to measure the skin temperature of the patient’s extremities and check whether the patient’s sensory and motor nerves, deep The objective assessment aims to measure the skin temperature of the patient’s extremities and check whether the patient’s sensory and motor nerves and deep tendon reflexes are abnormal; the subjective assessment determines the severity of neurotoxicity based on a scale. It is recommended to combine these two types of assessments to ensure objective assessment. At the same time, nursing staff should do their duty to inform the patient before chemotherapy, detail the signs of adverse reactions, and prompt the patient to report them in a timely manner so that the patient can fully participate in disease decision making. Although there is a lack of uniform assessment standards and nursing guidelines, nursing staff should develop a scientific and feasible assessment strategy based on the facts. Focus on individualized reactions, identify symptoms in a timely manner and do positive management to relieve patients’ painful experiences.
Construct a Scientific and Feasible Nursing Program and Carry Out Effective CIPN Nursing Practice
The results of this study showed that compared with cancer pain and chemotherapy-induced nausea and vomiting, the management of CIPN is often limited to basic care, and no systematic nursing plan has been formed in clinical work. For example, the Chinese Nursing Association and the Beijing Nursing Association have promulgated expert consensus and industry standards for cancer pain care,28 which have laid a practical operational foundation for promoting standardized management of cancer pain and improving patient compliance. Currently, Bie et al29,30 have constructed a nursing protocol for CIPN based on the best evidence summary, which has 16 recommended entries, mainly including 3 aspects of assessment, prevention and management of chemotherapy-induced peripheral neurotoxicity. Hospital administrators can invite relevant experts to evaluate the protocol accordingly and carry out nursing practice for protocol translation. The process of translation needs to be combined with specific clinical settings and professional judgment, and the opinions and suggestions of stakeholder groups (patients, physicians, and nurse groups) need to be recorded in detail in order to facilitate the summary of impediments and facilitators, promote the translation of knowledge to practice, and objectively evaluate the effectiveness and feasibility of the nursing protocol. The care plan presents a clear model of care practice for nursing staff, which is conducive to achieving precision care, further improving the quality of nursing services, relieving patients’ painful experiences, and enhancing treatment confidence and sense of meaningfulness of life.
Emphasis on the Psychological Health of the Patient and Nurse Community
The heavy disease burden and economic burden inevitably cause pessimism in patients, and the side effects of chemotherapy exacerbate depression.31 A close association between negative mood and disease prognosis has been reported, and when patients suffer from chronic emotional distress, the level of symptom burden increases with each passing day.32 Therefore, maintaining a stable positive mood would be beneficial to the physical and mental health of cancer patients. The results of this study showed that oncology nurses were very concerned about the psychological status of patients, but they only stopped at verbal reassurance and lacked advanced psychological support skills. Communication is the first step in building a trusting relationship, and good communication can enhance patients’ subjective well-being.33 The SAGE&THYME communication skills model34 constructed by the University of Manchester, UK, contains eight elements, which are: ① Setting (creating environment); ② Ask (guiding expression); ③ Gather (collecting problems); ④ Empathy (active empathy); ⑤ Talk (facilitating discussion); ⑥ Help (seeking support); ⑦ You (discovering (Self); and (8) Me (Work with me)35 Nursing staff can establish good relationships accordingly, dig deeper into patients’ inner thoughts, and guide them to establish positive psychology through meaningful treatment, regain confidence in treatment, and enhance their sense of meaning.
In this study, the respondents agreed that chemotherapy-induced peripheral neuritis is insidious in its onset, complex in its symptoms, and difficult to identify, and that the work stress of nurses is significantly positively correlated with the symptom burden of patients, and the relationship between the two parties converges to a communal form.36 According to mirror neuron theory, negative patient experience and high workload make nurses prone to empathic fatigue and low professional value. Nursing managers should pay attention to nurses’ emotional experiences, help them release stress through group psychological counseling, strengthen their professional identity, cultivate a sense of professional ethics, and provide quality nursing services with the mission of saving lives and relieving illnesses. In addition, nurses should pay attention to their own psychology. They can practice positive meditation to release stress and pay attention to the practice of the present moment on a daily basis, and if necessary, they should seek professional psychological counseling services to actively adjust their emotional state and enhance positive psychology.
Conclusion
This study used a phenomenological study to conduct in-depth interviews with 11 nurses in the oncology department, aiming to explore the nursing experience of patients with chemotherapy-induced peripheral neuritis based on the perspective of oncology nurses. A total of 3 themes were extracted: individual factors of CIPN caregiving dilemma, environmental factors of CIPN clinical caregiving dilemma, and the desire to improve CIPN knowledge to meet caregiving needs. The results of the study showed that the management ability of oncology nurses for CIPN needs to be improved, and the level of group knowledge and assessment awareness should be strengthened to pay timely attention to the mental health of patients and nurse groups to improve the quality of care. In addition, this study still has certain limitations, such as small sample size and the sense of experience as a subjective feeling with large individual differences, and it is proposed to conduct a multicenter and large sample study later to further improve the subject matter.
Acknowledgments
Thanks Tongji University for providing financial support for this study (JS2210319), Teaching Reform and Construction Project of Tongji University (JS20221212).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Livshits Z, Rao RB, Smith SW. An approach to chemotherapy-associated toxicity. Emerg Med Clin North Am. 2014;32(1):167–203. doi:10.1016/j.emc.2013.09.002
3. Avallone A, Bimonte S, Cardone C, Cascella M, Cuomo A. Pathophysiology and therapeutic perspectives for chemotherapy-induced peripheral neuropathy. Anticancer Res. 2022;42(10):4667–4678. doi:10.21873/anticanres.15971
4. Jahn F, Wörmann B, Brandt J, Freidank A, Feyer P, Jordan K. The prevention and treatment of nausea and vomiting during tumor therapy. Dtsch Arztebl Int. 2022;119(21):382–392. doi:10.3238/arztebl.m2022.0093
5. Epstein RS, Aapro MS, Basu Roy UK, et al. Patient burden and real-world management of chemotherapy-induced myelosuppression: results from an online survey of patients with solid tumors. Adv Ther. 2020;37(8):3606–3618. doi:10.1007/s12325-020-01419-6
6. Paus R, Haslam IS, Sharov AA, Botchkarev VA. Pathobiology of chemotherapy-induced hair loss. Lancet Oncol. 2013;14(2):e50–9. doi:10.1016/s1470-2045(12)70553-3
7. Bhatnagar B, Gilmore S, Goloubeva O, et al. Chemotherapy dose reduction due to chemotherapy induced peripheral neuropathy in breast cancer patients receiving chemotherapy in the neoadjuvant or adjuvant settings: a single-center experience. Springerplus. 2014;3:366. doi:10.1186/2193-1801-3-366
8. Miaskowski C, Mastick J, Paul SM, et al. Impact of chemotherapy-induced neurotoxicities on adult cancer survivors’ symptom burden and quality of life. J Cancer Surviv. 2018;12(2):234–245. doi:10.1007/s11764-017-0662-8
9. Mols F, Beijers T, Vreugdenhil G, van de Poll-Franse L. Chemotherapy-induced peripheral neuropathy and its association with quality of life: a systematic review. Support Care Cancer. 2014;22(8):2261–2269. doi:10.1007/s00520-014-2255-7
10. Banach M, Juranek JK, Zygulska AL. Chemotherapy-induced neuropathies-A growing problem for patients and health care providers. Brain Behav. 2017;7(1):e00558. doi:10.1002/brb3.558
11. Chan CW, Cheng H, Au SK, et al. Living with chemotherapy-induced peripheral neuropathy: uncovering the symptom experience and self-management of neuropathic symptoms among cancer survivors. Eur J Oncol Nurs. 2018;36:135–141. doi:10.1016/j.ejon.2018.09.003
12. Flatters SJL, Dougherty PM, Colvin LA. Clinical and preclinical perspectives on Chemotherapy-Induced Peripheral Neuropathy (CIPN): a narrative review. Br J Anaesth. 2017;119(4):737–749. doi:10.1093/bja/aex229
13. Alejandro LM, Behrendt CE, Chen K, Openshaw H, Shibata S. Predicting acute and persistent neuropathy associated with oxaliplatin. Am J Clin Oncol. 2013;36(4):331–337. doi:10.1097/COC.0b013e318246b50d
14. Jones SE, Erban J, Overmoyer B, et al. Randomized phase III study of docetaxel compared with paclitaxel in metastatic breast cancer. J Clin Oncol. 2005;23(24):5542–5551. doi:10.1200/jco.2005.02.027
15. Jordan B, Margulies A, Cardoso F, et al. Systemic anticancer therapy-induced peripheral and central neurotoxicity: ESMO-EONS-EANO clinical practice guidelines for diagnosis, prevention, treatment and follow-up. Ann Oncol. 2020;31(10):1306–1319. doi:10.1016/j.annonc.2020.07.003
16. Kleckner IR, Kamen C, Gewandter JS, et al. Effects of exercise during chemotherapy on chemotherapy-induced peripheral neuropathy: a multicenter, randomized controlled trial. Support Care Cancer. 2018;26(4):1019–1028. doi:10.1007/s00520-017-4013-0
17. Burgess J, Ferdousi M, Gosal D, et al. Chemotherapy-induced peripheral neuropathy: epidemiology, pathomechanisms and treatment. Oncol Ther. 2021;9(2):385–450. doi:10.1007/s40487-021-00168-y
18. Dong ZB, Wang YJ, Cheng ML, et al. 2-Bromopalmitate decreases spinal inflammation and attenuates oxaliplatin-induced neuropathic pain via reducing Drp1-mediated mitochondrial dysfunction. PLoS One. 2022;17(10):e0275428. doi:10.1371/journal.pone.0275428
19. Jia M, Wu C, Gao F, et al. Activation of NLRP3 inflammasome in peripheral nerve contributes to paclitaxel-induced neuropathic pain. Mol Pain. 2017;13:1744806917719804. doi:10.1177/1744806917719804
20. Kanzawa-Lee GA. Chemotherapy-induced peripheral neuropathy: nursing implications. J Infus Nurs. 2020;43(3):155–166. doi:10.1097/nan.0000000000000368
21. Wang Y, Fu JF, Bai YN, Xie J, Jiao HX, Wang ZL. Knowledge, attitude and practice regarding Chemotherapy-Induced Peripheral Neuropathy assessment and management among oncology nurses. Chin Nurs Manage. 2018;18(03):382–387. doi:10.3969/j.issn.1672-1756.2018.03.021
22. Binner M, Ross D, Browner I. Chemotherapy-induced peripheral neuropathy: assessment of oncology nurses’ knowledge and practice. Article. Oncol Nurs Forum. 2011;38(4):448–454. doi:10.1188/11.ONF.448-454
23. Al-Atiyyat NM, Banifawaz AZ. Oncology nurses’ knowledge, practice, and confidence toward chemotherapy-induced peripheral neuropathy in Jordan. Saudi Med J. 2018;39(11):1158–1163. doi:10.15537/smj.2018.11.23303
24. Yang Y, Dong YG, Gu LL, et al. Construction of an evaluation index system for the core competence of chemotherapy specialist nurses. Chin J Nurs. 2017;52(10):1226–1231. doi:10.3761/j.issn.0254-1769.2017.10.015
25. Guo LX. Development and Application of Shared Decision Making Questionnaire Among Oncology Nurses Based on the Theory of Knowledge-Attitude-Practice. Master. Zhengzhou University; 2021.
26. Colvin LA. Chemotherapy-induced peripheral neuropathy: where are we now? Pain. 2019;160(Suppl 1):S1–s10. doi:10.1097/j.pain.0000000000001540
27. Seretny M, Currie G, Sena E, et al. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: a systematic review and meta-analysis. Pain. 2014;155(12):2461–2470. doi:10.1016/j.pain.2014.09.020
28. Meng AF. Jiangsu Province Adult cancer pain Care Standard (2020 version). Med High Vocation Educ Mod Nurs. 2020;3(4):229–244. doi:10.3969/j.issn.2096-501X.2020.04.001
29. Bie MJ, Hu JE, Xiang YH, Chen HY. Evidences for the evaluation and management of chemotherapy-induced peripheral neuropathy. Chin Clin Nurs. 2021;13(09):552–557. doi:10.3969/j.issn.1674-3768.2021.09.006
30. Bie MJ, Xiang YH, Zhang GP, Hu JE, Chen HY. Formulation of an evidence-based nursing program for chemotherapy-induced peripheral neurotoxicity based on best evidences. Mod Clin Nurs. 2021;20(08):63–72. doi:10.3969/j.issn.1671-8283.2021.08.010
31. Conley C, Kamen CS, Heckler CE, et al. Modafinil moderates the relationship between cancer-related fatigue and depression in 541 patients receiving chemotherapy. J Clin Psychopharmacol. 2016;36(1):82–85. doi:10.1097/JCP.0000000000000442
32. Morrison EJ, Novotny PJ, Sloan JA, et al. Emotional problems, quality of life, and symptom burden in patients with lung cancer. Clin Lung Cancer. 2017;18(5):497–503. doi:10.1016/j.cllc.2017.02.008
33. Rochmawati E, Minanton M. Embedded spiritual conversation in cancer communication: lived experiences of nurses and patients/relatives. Int Nurs Rev. 2021;68(3):289–298. doi:10.1111/inr.12634
34. Connolly M, Perryman J, McKenna Y, et al. SAGE & THYME: a model for training health and social care professionals in patient-focussed support. Patient Educ Couns. 2010;79(1):87–93. doi:10.1016/j.pec.2009.06.004
35. Gao XY. Construction and Effects Evaluation of Goals-of-Care Communication Mode for Advanced Cancer Patients. Master. Zhengzhou University; 2021.
36. Tang LY, Zhang W. Exploring the nurse-patient community from the perspective of the relationship between symptom of lung cancer patients undergoing chemotherapy and narses’negative emotions. J Nurs Sci. 2020;35(22):57–59. doi:10.3870/j.issn.1001-4152.2020.22.057
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Subjective Will and Psychological Experience of Home-Based Exercise in Lung Cancer Patients During Interval of Chemotherapy: A Qualitative Study
Hu Y, Chen X, Fan J, Huang Y, Ye J, Gu F, Li Y
Journal of Multidisciplinary Healthcare 2023, 16:663-674
Published Date: 9 March 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Applying the COM-B Model to Understand Adherence to Tele-Exercise Prehabilitation Among Older Patients with Lung Cancer: A Qualitative Study
Liu CQ, Liu MY, Chu H, Zhang Z, Huan SS, Ma YR
Patient Preference and Adherence 2026, 20:600152
Published Date: 7 May 2026
A Qualitative Study on the Psychological Experience of Lung Cancer Patients During the Perioperative Period
Lei XN, Wang Q, Yan LC, Lu L, Xiao YS, Yang LY, Guo YH
Cancer Management and Research 2026, 18:589437
Published Date: 8 May 2026