")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Nursing Care and Barriers for Prevention of Venous Thromboembolism in Total Knee and Hip Arthroplasty Patients: A Qualitative Study
Authors Al-Mugheed K , Totur Dikmen B , Bayraktar N, Farghaly Abdelaliem SM , Ahmed Alsenany S
Received 14 January 2023
Accepted for publication 20 February 2023
Published 28 February 2023 Volume 2023:16 Pages 547—556
DOI https://doi.org/10.2147/JMDH.S403383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Khalid Al-Mugheed,1 Burcu Totur Dikmen,2 Nurhan Bayraktar,3 Sally Mohammed Farghaly Abdelaliem,4 Samira Ahmed Alsenany5
1Adult Health Nursing Department, College of Nursing, Riyadh Elm University, Riyadh, 12734, Saudi Arabia; 2Surgical Nursing Department, Faculty of Nursing, Near East University, Nicosia, Cyprus; 3Nursing Department, School of Health Sciences, Atılım University, Golbasi, Ankara, Turkey; 4Department of Nursing Management and Education, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia; 5Department of Community Health Nursing, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia
Correspondence: Khalid Al-Mugheed, Adult Health Nursing Department, College of Nursing, Riyadh Elm University, Riyadh, 12734, Saudi Arabia, Email [email protected]
Purpose: To determine barriers to preventing venous thromboembolism in total knee and hip arthroplasty patients by surgical nurses.
Methods: This qualitative study used a phenomenological approach. The semi-structured interview questionnaire included two questions focused on nursing care practices for VTE prevention and barriers faced during VTE prophylaxis in total knee and hip arthroplasty patients. Study data were collected from 10 surgical nurses through semi-structured interviews in July 2021.
Results: After analyzing the data, two main themes, five categories, and fourteen subcategories were developed. The main themes included “Nursing care” and “Barriers.” Two categories were reflected in terms of nursing care: general care and mechanical prophylaxis. Regarding barriers, the analysis of the interview reflected three main categories: “lack of professional competence”, “work conditions challenges”, and “resistance from patients”.
Conclusion: Educational institutions must play a critical role in preparing surgical nurses by establishing clinical nurse specialist programs and post-graduate diplomas programs that sufficiently prepare nurses for clinical settings.
Keywords: venous thromboembolism, nursing care, barriers, surgical nurses
Introduction
Venous Thromboembolism (VTE) includes Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE), which occur from a blood clot formed in the venous circulation.1 VTE has become the third most significant common cardiovascular disease after stroke and myocardial infarction and is considered the main problem among medical and surgical patients.2,3
The estimated incidence rate of VTE among Asian populations is high. Estimates of VTE range from 11 to 88 cases per 10,000 admissions across 10 Asian countries.4 In China, VTE incidence is estimated at 17.5 per 100,000 patients annually,5 in South Korea, 13.83 per 100,000 patients annually,6 and in Japan, 12.6 per 100,000 patients annually.7 In the United Kingdom, the mortality rate resulting in VTE in hospitalized patients is higher than patients’ deaths due to breast and prostate cancer and road-traffic accidents annually.8,9 In the United States, DVT costs an estimated $700 to $1400 monthly per patient and $465 to $875 for non-pharmacological prophylaxis.10,11
Total knee and hip arthroplasty patients are considered a high-risk group for VTE.12 In a meta-analysis conducted on Asian populations, including 1947 patients, one study reported an incidence of symptomatic DVTs related to total knee arthroplasty was 1.9%.4 DVT and pulmonary embolism have been noted to occur after 0.45–5.30% of knee arthroplasties and 0.24–1.60% of total hip arthroplasties.13,14 In addition, follow-up findings noted that 9.3% of VTE patients experience a post-thrombotic syndrome following total knee and hip arthroplasty that highly impacts their quality of life.5
Several organizations have developed VTE guidelines to diminish the incidence of DVT and PE and standardize the provision of prophylaxis. Such organizations include the United Kingdom’s National Institute for Health and Clinical Excellence 15, and the American College of Chest Physicians.16
VTE guidelines provide trustworthy instructions for nurses in VTE prevention and have been indicated in clinical practice guidelines.15 Nurses if educate play a significant part in translating VTE prophylaxis guidelines into clinical practice to enhance patient safety and diminish the VTE burden.17,18 Previous studies showed that orthopedic nurses reported appropriate practice on mechanical and pharmacological prophylaxis for VTE patients.19–21 Implementing quality nursing care is vital for nurses to drive improvements in nursing practice changes and patients’ clinical outcomes.2
Although VTE prophylaxis guidelines are available, the translation of practice guidelines into routine clinical nursing practice continues to be challenging. Several studies reported that many hospitalized patients do not receive VTE preventive prophylaxis in a suitable way, impacting patient safety and lives.22,23 The literature mentions many barriers nurses face in adhering to VTE prophylaxis. For example, two-thirds of Brazilian nurses reported that the lack of a standardized protocol was considered the main barrier in VTE risk assessment.23 Lee et al, reported that a lack of VTE knowledge was the main barrier.19 In another study, nurses said that a higher patient-to-nurse ratio impacted anticoagulant administration rates.24 In Lloyd et al’s study, healthcare professionals stated that the lack of clear indications and contraindications for VTE prophylaxis and the risk of bleeding were barriers.25 The current study was conducted to determine nursing care and barriers to preventing venous thromboembolism in total knee and hip arthroplasty patients by surgical nurses.
Methodology
Design
The study was performed with a qualitative design using in-depth semi-structured interviews that adopted Colaizzi’s phenomenological data analysis method.26
Setting and Participants
The study was conducted in the surgical unit of a private teaching hospital, considered the best private teaching hospital in the area. The surgical unit comprised 19 beds for trauma and surgical patients. A purposive sample was recruited among 25 surgical nurses. Eligibility criteria were the desire to join, hold a bachelor’s degree in nursing, and work in a surgical unit. Nurse technicians, trainees, and students were excluded.
This research was a qualitative study utilizing in-depth interviews. The current study used in-depth interviews of 10 participants using a purposive sample, subject to saturation. Typically, these types of studies use fewer participants than survey-based research. No specific minimum number of respondents exists for in-depth interviews.27 Saunders et al, found that in semi-structured interviews the acceptable range of the sample size was 5 to 25.28 In this instance, it was 10 participants.
Semi-Structured Questionnaire
The descriptive information section included age, gender, experience as a surgical nurse, education related to VTE, and source of education. The semi-structured interview questionnaire included two questions focused on nursing care practices for VTE prevention and barriers faced during VTE prophylaxis in total knee and hip arthroplasty patients. The two questions were:
- What are your nursing care practices as preventions in total knee and hip arthroplasty patients at risk of venous thromboembolism?
- What barriers do you face during used VTE nursing care practices in total knee and hip arthroplasty patients at risk of venous thromboembolism?
Data Collection
Data were collected in July 2021 with individual semi-structured interviews. First, the researchers collected the participants’ contact information and then scheduled interview dates based on a participant’s desires. At the scheduled time, the nurses were invited to join the study via telephone, and they received a link to start the online interview via Google meet video conferencing platform. During the Covid-19 pandemic, the videoconference platform and online interviews were recommended as a data collection method instead of face-to-face interviews for qualitative studies.29
Interviews were performed when the participants were in their homes to prevent pressure work and clashing with patient care. Once a participant received a link and started the interview, the researchers explained the aim of the study and offered them the right to stop the interview and withdraw from the study at any time they were not comfortable In addition, they were assured that the information would remain confidential. To assure anonymity, each participant was assigned a code randomly. Permission was obtained from each participant to open the video cam and record during the interview. Interviews were recorded to monitor the feedback and responses of the participants. Interviews were recorded by the Google meet platform and saved directly after finishing the interview to Google drive on a researcher’s computer.
Two researchers attended each interview, one as an interviewer and the second as a reporter. During interviews, we encouraged interviewees to present clear interpretations and more clarifications in the event of any ambiguity. Turkish was the dominant language in interviews. The duration of each interview was organized according to the participant’s willingness and preparedness. Interviews took approximately 27–32 minutes. Pilot interviews were conducted among three surgical nurses to check interview questions, no modifications were made to the interview questions.
Rigor and Trustworthiness
Criteria for ensuring rigor and trustworthiness were used Lincoln and Guba.30 Credibility was gained by preserving transparency with the interviewees.The interviews were recorded, and field notes were taken. Interview instructions were used to obtain a detailed response and extend the answers. To ensure conformability, the audio-recording interviews were transcribed by the first author, and the second author listened to the audio-recording and reviewed the transcribed data for precision. Transferability was ensured by the third author to assure that data was the correct representation of the interviewee’s views. Memos of the author’s assumptions were saved throughout the data analysis.
Data Analysis
The data analysis was performed using Colaizzi’s method,26 interpreting the data by recognizing meaning units. The participants’ expressions were translated from Turkish into English by an expert fluent in both languages. Three researchers independently were responsible for analyzing data to avoid errors. The researchers transcribed the recorded interviews and reviewed each transcription repeatedly to obtain a comprehensive sense and understanding of the whole transcripts. Significant and meaningful statements respecting the phenomenon were drawn from the transcripts by all researchers. Categories and subcategories were then classified through shared views and mutual discussion, relying on similarities and differences. All emergent categories were defined in a comprehensive context. The discrepancy and overestimated or misused categories and subcategories were resolved by general consensus. The agreement categories were used in the final structure of the study. The findings were validated using member checking. The researchers sent descriptive findings to participants to check.
Ethical Considerations
Ethical approval from the Ethics Committee of a Near East University and the institutional permission from the hospital director of Near East Hospital was obtained. In addition, all nurses voluntarily participated, and their verbal and written permissions were obtained and the participant’s informed consent include the publication of anonymized responses.
Results
Demographic Data
All surgical nurses were female, and the average age was 28.6±5.3 years. The mean work experience of nurses was 5.23±2.6 years, and work experience as surgical nurses was 4.00±3.28 years. The source of venous thromboembolism education was courses in the training program for all of them (100%). Also, 23.07% of the participants had in-service education (Table 1).
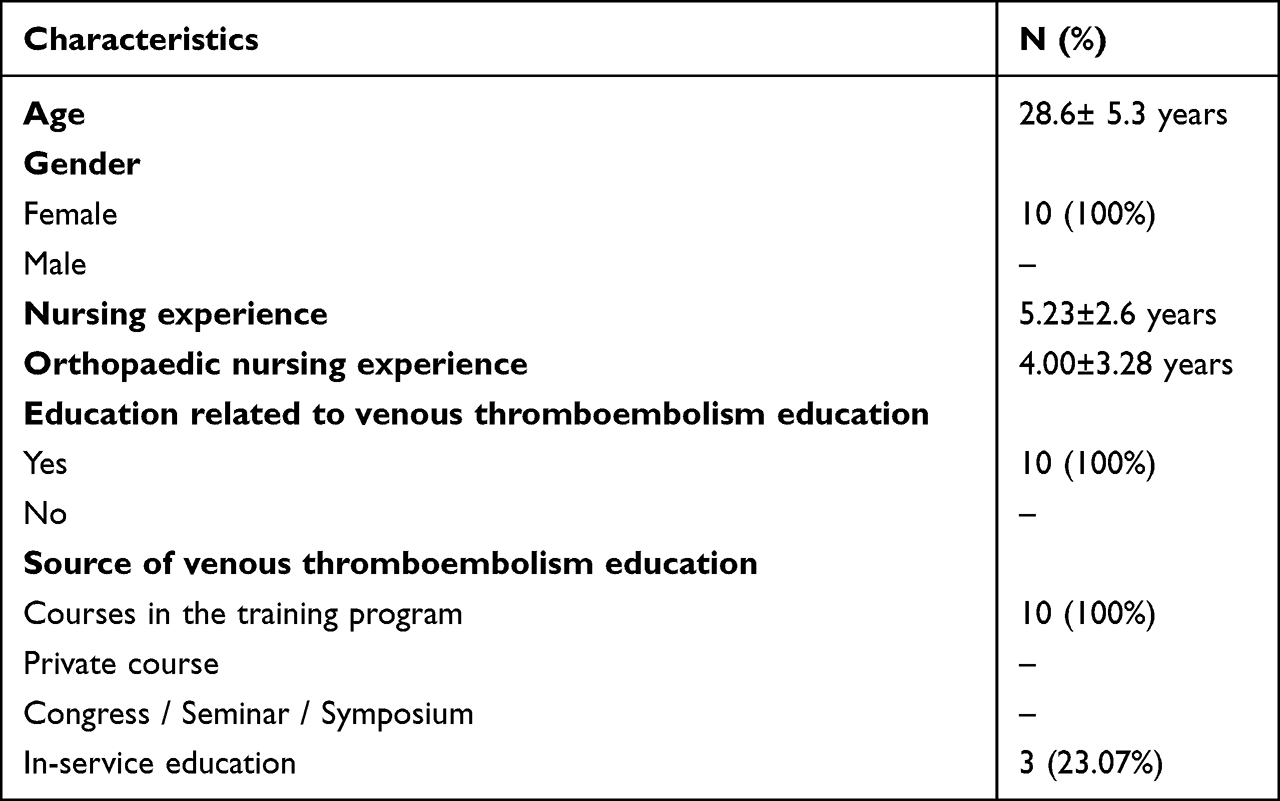 |
Table 1 Descriptive Data (n=10) |
After analyzing the data, the codes were extracted into two main themes, five categories, and fourteen subcategories. The main themes included “Nursing care” and “Barriers.” For nursing care, two categories included general care and mechanical prophylaxis. General nursing care themes included five subcategories “elevation”, “mobilization”, “foot-leg exercises”, “changing position in bed”, and “pain control.” The mechanical prophylaxis theme included two sub-themes, “Antiembolic stocking” and “Intermittent pneumatic compression device.”
Regarding barriers, the analysis of the interview reflected three categories: “lack of professional competence”, “work conditions challenges”, and “resistance from patients.” Lack of professional competence involved two subcategories “lack of knowledge and professional skills” and “lack of in-service training.” The second category was “work conditions challenges” and included four subcategories “workload”, “lack of appropriate protocols”, “unfavorable supervision”, and “safety concerns and fear of complications.” The categories “resistance from patients” reflected one subcategory, “refusal by the patients.” See Table 2.
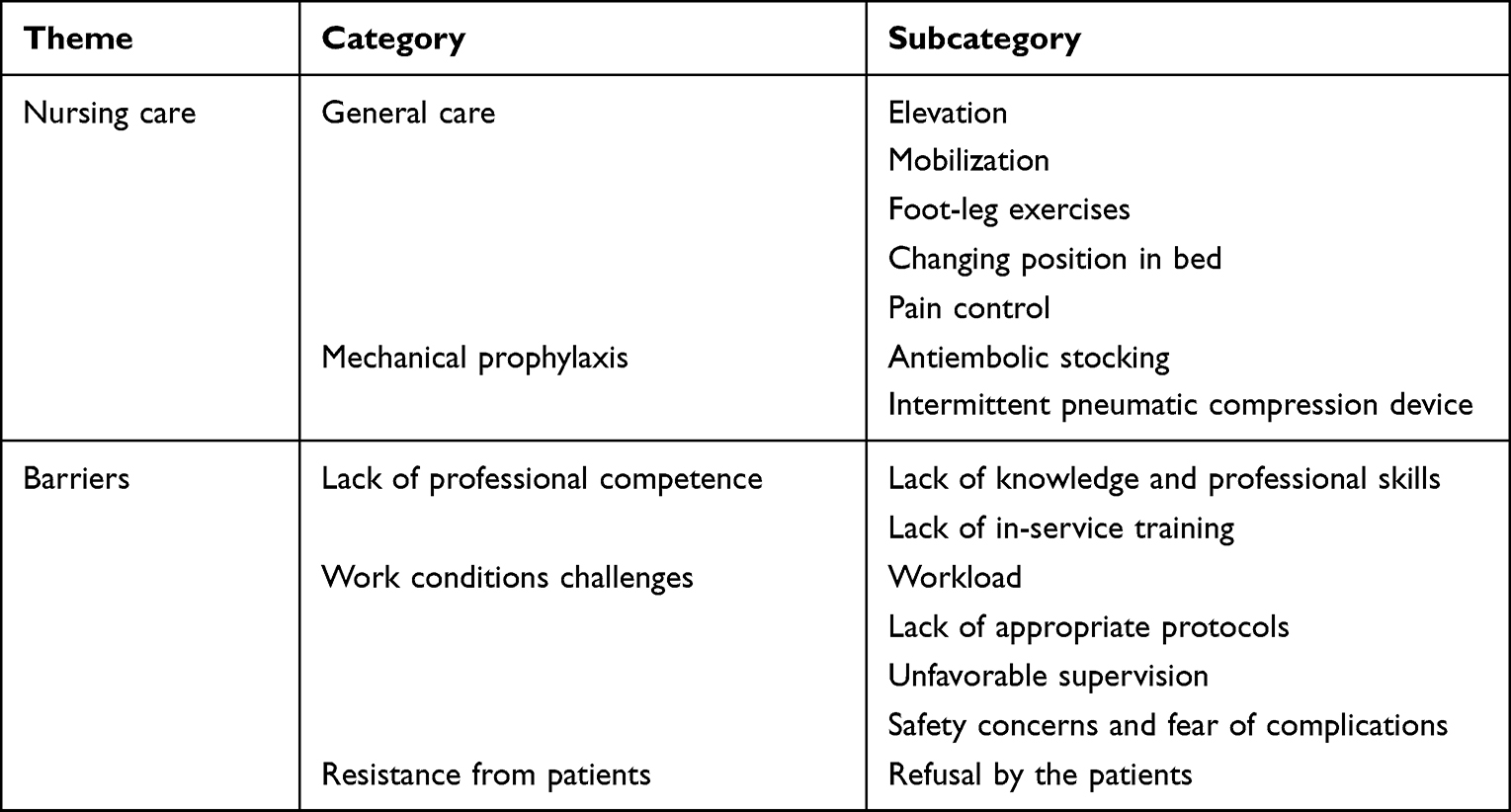 |
Table 2 Overview of the Study Themes, Categories, and Subcategories |
Nursing Care
General Care
The duties and responsibilities of surgical nurses with VTE patients included both psychological and physical care practices. The majority of the participants stated that they performed different physical care practices for the patients, such as elevation of the leg, early mobilization, teaching foot-leg exercises, and pain control in terms of pre-and post-operative nursing interventions for patients at risk for VTE and VTE mechanical prophylaxis devices.
In the post-operative period, controlling the pain in the leg and determining the type of the pain may facilitate distinguishing the sensation of pain, whether from the operation site or DVT pain. (N1)
In the preoperative period, we provide teaching about foot-leg exercise and elevation of the leg as a nursing care for VTE patients who will undergo knee and hip prosthesis surgery. (N6)
Early patient mobilization is the most important nursing intervention for the post-operative period because it reduces VTE occurrence. One nurse stated that;
The first intervention that encourages the patients when they come to our unit is early mobilization during the first 24 hours. We immobilize the patients if they have drains and encourage them to elevate the leg. (N7)
Mechanical Prophylaxis
Nurses stated that they used antiembolic stocking and intermittent pneumatic compression devices for mechanical protective measures.
In the preoperative period, we start to apply antiembolic stockings to our patients who are at risk of VTE around 22.00 before the operation. If antiembolic stockings are insufficient, we start the use of intermittent pneumatic compression devices under the physician’s order (N2)
In terms of psychological support, nurses stated that some patients suffered from post-thrombotic panic:
Participants often reported long-term concerns and panic related to the cause of VTE, if they will endure for a long time and how they will adapt to prophylaxis devices. We spent a lot of time talking to patients to calm their psychological conditions. (N8)
Barriers
Lack of Professional Competence
Lack of professional competence was one central category that surgical nurses recounted in this study. This theme was grouped into three subcategory: lack of knowledge, lack of professional skills, and in-service training.
Lack of Knowledge and Professional Skills
The majority of participants considered thorough knowledge a valuable aspect of VTE prevention. They highlighted a lack of knowledge of practice about VET prevention among some nurses, which completely obstructed effective patient care.
I think foot-leg exercises are not a priority… The use of socks is more beneficial. (N9)
In fact, I saw that some nurses didn’t do their tasks correctly, they removed graduated compression stockings (GCS) at night, and they thought it may contribute to relaxing muscles. (N4)
In obese patients, the size of the socks cannot measure correctly, or they can be long, so they might to be bent down and become ineffective. (N3)
Lack of In-Service Training
In-service staff training regarding VTE prevention can enhance a nurse’s skills and knowledge and upgrade the quality of care. However, most nurses recognized the ineffectiveness and inadequacy of continuing education.
I’m a beginner nurse and received orientation with the head nurse for only one week. I don’t believe this kind of orientation is enough. (N5)
How to maintain VTE mechanical prophylaxis competence was highlighted in the nursing challenge. Lack of educational support, particularly for novice nurses, was referred to in a negative light:
Most of the content materials are repetitive or copies of the same previous material. (N10)
The majority of in-service training activities are held during the daily work shift, and during the lesson, the units call us to fill the work gaps, so we face difficulty participating or have to attend after the shift. (N9)
Work Conditions Challenges
Nurses’ professional roles comprise a diversity of daily duties and challenges. Although numerous duties are built on trials and routine management, nurses are also under daily challenges. The nurses felt their work sometimes became monotonous because of a lack of variety.
Workload
Nurses usually have a considerable workload and must determine their priorities to handle various care challenges. Inadequate nurse-patient ratios, turnover of patients and nurses, workloads, job dissatisfaction, and administrative tasks contribute to creating a non-manageable workload.
The proportion of nurses to patients is not fair…. I provide care for many patients. So I work fast, hard, and sometimes lose my concentration…patient safety is endangered. (N9)
There should be enough nurses so I have time to perform my responsibilities correctly and perfectly and have a bit of time to deal with things that belong to me (N1).
Lack of Appropriate Protocols
Nurses indicated that the availability of a current protocol helps guide nurses to determine the best practice care for the patients. In addition, having a clear understanding of the VTE protocol is requisite and not just imposed by the head of the department.
Although training is beneficial, having a current protocol is necessary for the units. (N5)
A protocol will guide all healthcare professionals, not only nurses, to provide suitable care. (N8)
Unfavorable Supervision
Supervision is a keystone for performance refinement. Helps ensure that tasks are performed accurately. Most participants noted that the supervisor should have adequate supervision for those who work under his / her supervision to eliminate work conditions challenges.
The head nurse often does not take our requests into consideration while preparing the duty schedule…. It is also very difficult for her to reschedule due to the nurse shortage. (N10)
Positive interactions with a manager are necessary for team support and good manageability.
I’m a novice nurse, have very few clinical skills, and am hesitant to ask questions related to some skills. I can’t, “It challenges me”. (N8)
To achieve the benefits of the patient care process, the healthcare system needs appropriate communication between team members. (N7)
Safety Concerns
Participants agreed that quality of care is initial competency and credentialing. Negative perception and poor attitude among nurses toward VTE mechanical prophylaxis can reduce the continuity of this practice. The participating nurses experienced numerous challenges when performing mechanical prophylaxis, such as uncertainty, anxiety, fear, and patients’ refusal.
VTE mechanical prophylaxis constitutes challenging because I am afraid skin breakdown will worsen for patients. (N8)
I can’t take the correct fit for some patients due to obesity and complications such as extremity with a fracture, line access, and burns. (N6)
Resistance from Patients
Refusal by the Patients
The patients refused to use a VTE prophylaxis device, “I’m tired”, no energy. “I don’t want to apply the device.” “We cannot force the patient to apply the device if they don’t like it.” The nurses were eager to help the patient, but some resorted to accepting the patient’s decision.
Lack of strong communication with the patient creates an obstacle in terms of applying VTE precautions. The cooperation of the patient is very important, especially in the mobilization phase. (N2)
When we say to some of our patients, let’s mobilize, they may say you go; I’ll get up and walk by myself. After that, when we leave the room and go back to them, unfortunately, we can find the patient sitting on the bed or sleeping. (N4)
Discussion
VTE prevention is the most effective way to positively affect patient outcomes, reduce prolonged hospitalizations, and reduce VTE recurrence. Nurses play a significant part in translating VTE prophylaxis guidelines into practice.31 This study aimed to explore the nursing practices provided to VTE patients and nurses’ experiences with barriers to VTE prevention in surgical units.
From the participants’ perspectives, leg elevation, early mobilization, teaching foot-leg exercises, pain control, and providing VTE mechanical prophylaxis devices were the most frequent nursing care practices to prevent VTE. According to the NICE guideline, these practices are highly recommended in VTE prevention guidelines.15 Previous studies showed that foot exercise, leg elevation, and early mobilization contributed to increased blood flow velocity among VTE patients.32,33 These most daily frequent practices were similar to national study practices,22 and international studies.23,34 One possible explanation is that the nurses engaged in these practices because they may not require additional effort and time.
Lack of professional competence was one major barrier to efficient VTE prevention, evidenced by a lack of knowledge and professional skills. In-service training did not address this barrier, and participants stated that they did not receive theoretical or practical VTE-related training. The lack of knowledge related to VTE knowledge and practice was reported in different studies.20,35 The lack of knowledge of deep vein thrombosis prophylaxis was a significant barrier among nurses.25 The use of nurses who lack this knowledge threatens patients’ safety and health.36
The participants identified the lack of in-service training as a barrier to VTE prevention. A study in Northern Cyprus also reported that nurses receive inadequate training about VTE.37 Although participants had performed some basic VTE nursing practices such as foot exercises, leg elevation, and early mobilization, they mentioned that they lacked knowledge about VTE mechanical prophylaxis practices. Silva et al, reported lower priority for VTE mechanical device practices.23 Another study showed that only half of the nurses performed standardized roles when applying graduated compression stockings.21 Shah et al, study found that only one-third of nurses used graduated compression stockings correctly.37 The correct application of mechanical prophylaxis is necessary because the incorrect use may lead to a negative care result.23 The lack of translation of VTE mechanical prophylaxis correctly is attributable to low self-efficacy among nurses and a lack of VTE knowledge.38 Published literature shows that nurses’ adherence to prophylaxis increases dramatically through education programs and continuous follow-ups.39
Work conditions are another barrier and include subcategories such as workload, lack of appropriate protocols, unfavorable supervision, and safety concerns. In line with our findings related to workload, the evidence suggests that workload and inadequate nurse-patient ratios inhibit nurses from performing patient care effectively and cause severe difficulty in VTE mechanical prophylaxis.8,37 An increased workload was the second concern of nurses related to venous thromboembolism prophylaxis.35 The availability of enough nurses on the units is critical to cope with the workload and enhance their decision-making skills.40,41 Conversely, a staff shortage results in an increase in a nurse’s shifts, leading to burnout, fatigue, and negative outcomes for nurses and healthcare organizations.24,42
In the present study, the participants referred to negative supervision as one of the most significant barriers to VTE prevention. Having well-established managerial supervision to support nurses and other healthcare professionals is critical. Consistent with these findings, a study reported that nursing supervisors had limited knowledge and competence to supervise.43 Another study showed that nursing managers are not sufficiently empowered to implement their supportive roles, leadership, and managerial skills.36 The nursing managers should support nurses while performing VTE mechanical prophylaxis to restore a patient’s body function.
Our participants felt that the VTE protocol was not well implemented into daily routine nursing care. The reason behind this was protocol needs to be revised according to up-to-date VTE evidence-based practice to be implemented, and lack of training. A recent study found that more than half of the participants reported a lack of clear indications and guidelines for VTE prophylaxis.43 Nurses showed high compliance and VTE prophylaxis practices after adhering to clear guidelines.20,34 Hospitals and units should be encouraged to draft their own VTE guidelines and upgrade nurses’ awareness to translate them into their daily practices.
Patient safety is a source of great concern for nurses when discussing barriers to VTE mechanical prophylaxis.19 Our nurses perceived VTE mechanical prophylaxis as a challenge to patient safety and would prefer not to endanger the patients. The fear of patient complications, skin breakdown, and bleeding deters nurses from applying mechanical prophylaxis devices to their patients.24,44 Existing studies have shown that nurses perceived VTE mechanical prophylaxis as a risk outweighing benefits and stated that it was not relevant to their setup.45 Such perception reflects an erroneous belief related to the benefits of VTE mechanical prophylaxis.
At times, nurses experienced patients’ refusal to apply VTE mechanical prophylaxis devices and sometimes were unable to persuade them. Patients’ lack of response may also be associated with their negative beliefs and harmful mindsets. Haut et al, reported that the main reason for not adhering to VTE prophylaxis was patients’ refusal.46 Implementing guidelines that consider patient preferences may enhance patient satisfaction with and promote adherence to VTE prophylaxis and different diseases.47,48
Limitations
The participants of this study were recruited from a single surgical unit of a hospital, so the transferability and generalizability of the findings can be problematic. Using remote online meetings could have caused a limited view of participants’ body language, and technical problems may have resulted in participants giving short interpretations. The findings may not be generalized to all surgical nurses because all participants were female and from one hospital.
Conclusion
This study is thought to be the first to present nursing care and barriers to preventing venous thromboembolism in total knee and hip arthroplasty patients on surgical nurses. This study captured the contemplation of nursing care and barriers surgical nurses have faced when deciding to use VTE mechanical prophylaxis for their patients. Findings indicate that these barriers are varied and complex, which comprise a wide range of overlapping personal, organizational and environmental barriers. Nursing managers need adequate facilities and develop VTE guidelines to improve their professional competencies. Future studies in different nursing units and hospitals exploring the barriers to VTE mechanical prophylaxis are recommended.
Acknowledgment
The authors extend their appreciation to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
The research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention 2016. Venous thromboembolism (Blood Clots); 2019. Available from: http://www.cdc.gov/ncbddd/dvt/facts.html.
2. Lockwood R, Kable A, Hunter S. Evaluation of a nurse-led intervention to improve adherence to recommended guidelines for prevention of venous thromboembolism for Hip and knee arthroplasty patients: a Quasi-experimental study. J Clin Nurs. 2018;27(5–6):1048–1060. doi:10.1111/jocn.14141
3. Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016;118(9):1340–1347. doi:10.1161/CIRCRESAHA.115.306841
4. Lee WS, Kim KI, Lee HJ, Kyung HS, Seo SS. The incidence of pulmonary embolism and deep vein thrombosis after knee arthroplasty in Asians remains low: a meta-analysis knee. Clin Orthop Relat Res. 2013;471:1523e32. doi:10.1007/s11999-012-2758-9
5. Zhang Z, Song K, Yao Y, et al. Incidence and risk factors for post-thrombotic syndrome in patients with deep vein thrombosis following total knee and Hip arthroplasty. J Arthroplasty. 2019;34(3):560–563. doi:10.1016/j.arth.2018.10.013
6. Yeo DX, Junnarkar S, Balasubramaniam S, et al. Incidence of venous thromboembolism and its pharmacological prophylaxis in Asian general surgery patients: a systematic review. World J Surg. 2015;39(1):150–157. doi:10.1007/s00268-014-2763-0
7. Nakamura M, Yamada N, Ito M. Current management of venous thromboembolism in Japan: current epidemiology and advances in anticoagulant therapy. J Cardiol. 2015;66(6):451–459. doi:10.1016/j.jjcc.2015.03.012
8. Heit JA, Ashrani A, Crusan DJ, et al. Reasons for the persistent incidence of venous thromboembolism. Thromb Haemost. 2017;117:390–400. doi:10.1160/TH16-07-0509
9. Di Nisio M, van Es N, Buller HR. Deep vein thrombosis and pulmonary embolism. Lancet. 2016;388(10063):3060–3073. doi:10.1016/S0140-6736(16)30514-1
10. Dawoud DM, Wonderling D, Glen J, et al. Cost-utility analysis of venous thromboembolism prophylaxis strategies for people undergoing elective total hip and total knee replacement surgeries in the English national health service. Front Pharmacol. 2018;9:1370. doi:10.3389/fphar.2018.01370
11. Ruppert A, Steinle T, Lees M. Economic burden of venous thromboembolism: a systematic review. J Med Econ. 2011;14:65e74. doi:10.3111/13696998.2010.546465
12. Warren JA, Sundaram K, Anis HK, et al. Have venous thromboembolism rates decreased in total hip and knee arthroplasty? J Arthroplasty. 2019;2019:1–6.
13. Kim S, Ahn H, Shin SA, Park JH, Won CW. Trends of thromboprophylaxis and complications after major lower limb orthopaedic surgeries in Korea: national health insurance claim data. Thromb Res. 2017;155:48–52. doi:10.1016/j.thromres.2017.04.023
14. Shahi A, Bradbury TL, Guild GN, et al. What are the incidence and risk factors of in-hospital mortality after venous thromboembolism events in total Hip and knee arthroplasty patients? Arthroplast Today. 2018;4:343–347. doi:10.1016/j.artd.2018.02.014
15. National Institute for Health and Clinical Excellence. Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism; 2018. Available from https://www.nice.org.uk/guidance/ng89.
16. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis: ACCP Evidence-based clinical practice guidelines. Chest J. 2012;141:419–496.
17. Al‐Mugheed K, Bayraktar N. Effectiveness of a venous thromboembolism course using flipped classroom with nursing students: a randomized controlled trial. Nurs Forum. 2021;2021:1–7.
18. Al‐Mugheed K, Bayraktar N. Effectiveness of flipped classroom among nursing students on venous thromboembolism (VTE). Niger J Clin Prac. 2021;24:1463–1470. doi:10.4103/njcp.njcp_129_20
19. Lee JA, Grochow D, Drake D, Johnson L, Reed P, Servellen G. Evaluation of hospital nurses’ perceived knowledge and practices of venous thromboembolism assessment and prevention. J Vasc Nurs. 2014;32(1):18–24. doi:10.1016/j.jvn.2013.06.001
20. Oh H, Boo S, Lee J. Clinical nurses’ knowledge and practice of venous thromboembolism risk assessment and prevention in South Korea: a cross-sectional survey. J Clin Nurs. 2016;26:427–435. doi:10.1111/jocn.13424
21. Xu Y, Wang W, Zhao J, Wang J, Zhao T. Knowledge, attitude, and practice of healthcare professionals toward clinically applying graduated compression stockings: results of a Chinese web-based survey. J Thromb Thrombolysis. 2019;47:102–108. doi:10.1007/s11239-018-1749-4
22. Al‐Mugheed K, Bayraktar N. Knowledge and practices of nurses on deep vein thrombosis risks and prophylaxis: a descriptive cross sectional study. J Vasc Nurs. 2021;36(2):71–80. doi:10.1016/j.jvn.2018.02.001
23. Silva JS, Lee J, Grisante DL, et al. Nurses’ knowledge, risk assessment, and self-efficacy regarding venous thromboembolism. Acta Paul Enferm. 2020;33:20190125. doi:10.37689/acta-ape/2020AO0125
24. Elder S, Hobson DB, Rand CS, et al. Hidden barriers to delivery of pharmacological venous thromboembolism prophylaxis: the role of nursing beliefs and practice. J Patient Saf. 2016;12(2):63–68. doi:10.1097/PTS.0000000000000086
25. Lloyd NS, Douketis JD, Cheng J, et al. Barriers and potential solutions toward optimal prophylaxis against deep vein thrombosis for hospitalized medical patients: a survey of healthcare professionals. J Hosp Med. 2012;7(1):28–34. doi:10.1002/jhm.929
26. Colaizzi PF. Psychological Research as the Phenomenologist Views It. Oxford University Press; 1978.
27. Brannen J, Corm T. How many qualitative interviews is enough? In: Baker SE, Edwards R, editors. National Centre for Research Methods: Economic and Social Research Council. NCRM; 2005.
28. Saunders M, Lewis P, Thornhill A. Research Methods for Business Students. Harlow: Pearson Education Ltd; 2012.
29. Saarijarvi M, Bratt EL. When face-to-face interviews are not possible: tips and tricks for video, telephone, online chat, and email interviews in qualitative research. Euro J Cardiovasc Nurs. 2021;20(4):392–396. doi:10.1093/eurjcn/zvab038
30. Lincoln YS, Guba E. Naturalistic Inquiry. Thousand Oaks: SAGE; 1985.
31. AL-Mugheed K, Bayraktar N, Abdulqadir NJ, et al. Compliance of non-pharmacological preventive practice of venous thromboembolism among Jordanian nurses. Medicine. 2022;101(44):e31189. doi:10.1097/MD.0000000000031189
32. Albsoul-Younes A, Gharaibeh L, Younes N. Evaluation of venous thromboembolism prophylaxis after the introduction of an institutional guideline: extent of application and implementation of its recommendations. J Vasc Nurs. 2015;33(2):72–78. doi:10.1016/j.jvn.2014.11.002
33. Hanison E, Corbett K. Non-pharmacological interventions for the prevention of venous thromboembolism: a literature review. Nurs Stand. 2016;31(8):48–57. doi:10.7748/ns.2016.e10473
34. Ma Y, Xu Y, Ya P, et al. Nurses’ objective knowledge regarding venous thromboembolism prophylaxis: a national survey study. Medicine. 2018;97(14):0338.
35. Yan T, He W, Hang C, et al. Nurses’ knowledge, attitudes, and behaviors toward venous thromboembolism prophylaxis: how to do better. Vascular. 2020;1(1):1–7.
36. Kim C, Lee Y. Effects of compassion competence on missed nursing care, professional quality of life and quality of life among Korean nurses. J Nurs Manag. 2020;28:2118–2127. doi:10.1111/jonm.13004
37. Shah SS, Abdi A, O¨zcem B, et al. The rational use of thromboprophylaxis therapy in hospitalized patients and the perspectives of health care providers in Northern Cyprus. PLoS One. 2020;15(7):e0235495. doi:10.1371/journal.pone.0235495
38. Songwathana P, Promlek K, Naka K. Evaluation of a clinical nursing practice guideline for preventing deep vein thrombosis in critically ill trauma patients. Aust Emerg Nurs J. 2011;14:232–239. doi:10.1016/j.aenj.2011.09.002
39. Gaston S, White S. Venous thromboembolism (VTE) risk assessment: rural nurses’ knowledge and use in a rural acute care hospital. Int J Nurs Pract. 2013;19:60–64. doi:10.1111/ijn.12028
40. Rababa M, Bani-Hamad D, Hayajneh AA, Al Mugheed K. Nurses’ knowledge, attitudes, practice, and decision-making skills related to sepsis assessment and management. Electron J Gen Med. 2022;19(6):em420. doi:10.29333/ejgm/12556
41. Al‐Mugheed K, Bayraktar N. Patient safety attitudes among critical care nurses: a case study in North Cyprus. Int J Health Plann Manage. 2020;35(4):910–921. doi:10.1002/hpm.2976
42. AL-Mugheed K, Bayraktar N, Al-Bsheish M, et al. Patient safety attitudes among doctors and nurses: associations with workload, adverse events, experience. Healthcare. 2022;10:631. doi:10.3390/healthcare10040631
43. Janatolmakan M, Khatony A. Explaining the experience of nurses on missed nursing care: a qualitative descriptive study in Iran. Appl Nurs Res. 2022;63:151542. doi:10.1016/j.apnr.2021.151542
44. Kiflie AM, Mersha AT, Workie MM, Admass BA, Ferede YA, Bizuneh YB. Assessment of knowledge, attitude, practice and associated factors of venous thromboembolism prophylaxis among health professionals. A cross sectional study. Int J Surg Open. 2022;39:100436. doi:10.1016/j.ijso.2021.100436
45. Bhatti AM, Ahsin S, Salim B, Mansoor J. Knowledge, attitude and practices of healthcare providers towards deep vein thrombosis prophylaxis in five teaching hospitals of Rawalpindi. J Ayub Med Coll Abbottabad. 2012;24(2):136–139.
46. Haut ER, Aboagye JK, Shaffer DL, Wang J. Effect of real-time patient-centered education bundle on administration of venous thromboembolism prevention in hospitalized patients. JAMA Network Open. 2018;1(7):e184741. doi:10.1001/jamanetworkopen.2018.4741
47. Haac BE, O’Hara NN, Mullins D, et al. Patient preferences for venous thromboembolism prophylaxis after injury: a discrete choice experiment. BMJ Open. 2017;7:e016676. doi:10.1136/bmjopen-2017-016676
48. Rasha EA, Bdair IA, AL-Mugheed K, et al. Empowering self-efficacy by using patient empowerment among chronic obstructive pulmonary disease: pre–post-test study. Healthcare. 2023;1(11):430.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.