Back to Archived Journals » Reports in Medical Imaging » Volume 15
Nurses’ Roles in Managing Patient Anxiety Before MRI Scans Using Informative Video
Authors Alghamdi A ![]() , Algamdi MM
, Algamdi MM ![]() , Alatawi K
, Alatawi K ![]() , Alghamdi B, Alanazi H, Alamri S, Alamri S, Albishi Z
, Alghamdi B, Alanazi H, Alamri S, Alamri S, Albishi Z
Received 28 December 2021
Accepted for publication 14 March 2022
Published 24 March 2022 Volume 2022:15 Pages 9—19
DOI https://doi.org/10.2147/RMI.S353700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tarik Massoud
Ali Alghamdi,1 Maaidah Algamdi,2 Khaledah Alatawi,2 Basmah Alghamdi,2 Hana Alanazi,2 Shumukh Alamri,2 Somiah Alamri,2 Zahra Albishi2
1Department of Radiological Sciences, Faculty of Applied Medical Sciences, University of Tabuk, Tabuk, Saudi Arabia; 2Department of Nursing, Faculty of Applied Medical Sciences, University of Tabuk, Tabuk, Saudi Arabia
Correspondence: Ali Alghamdi, Department of Radiological Science, Faculty of Applied Medical Sciences, University of Tabuk, Tabuk, 47512, Saudi Arabia, Tel +966561587982, Email [email protected]
Background: Magnetic resonance imaging (MRI) has become one of the most essential diagnostic medical imaging techniques. The most common disadvantage of MRI is that patients may feel anxious before the examination, which can negatively affect them, prevent them from attending or completing the examinations, and cause patient movement during the examination, which accordingly results in misinterpretation issues. Recently, several methods have been suggested to reduce MRI anxiety. Our study aimed to examine nurses’ roles in reducing the levels of patient anxiety during pre-MRI scans by using informative video.
Methods: A cross-sectional and interventional study was conducted among MRI patients in Tabuk City. A convenience sample of 16 patients as the case group and 28 patients as the control group was included. A 2-minute informative video clip containing comprehensive instructions about MRI was recorded by the research team in the MRI room and introduced to patients 30 minutes before the scan in the waiting area. An Arabic version questionnaire (State-Trait Anxiety Inventory) was used to measure the pre-MRI-related anxiety of patients in the case and control groups. State-trait anxiety scores were analyzed and compared between groups. Median pulse, oxygen saturation, and blood pressure were also compared between the cases and control groups using a p-value of 0.05.
Results: The state anxiety score was significantly higher in cases compared to controls. However, the trait anxiety score was not significantly different between cases and controls. Females showed significantly higher state anxiety scores in the cases than in the controls. Based on the previous MRI experience, the cases group who had undergone a previous MRI had significantly higher state anxiety scores than those in the control group. Based on the educational degree, cases with bachelor’s degree had higher state anxiety scores than their counterparts in the control group.
Conclusion: The present study showed that the self-made visual tool used by nurses 30 minutes before MRI scan did not reduce the level of anxiety significantly in patients. However, state anxiety scores increased in females, patients with previous MRI experience, and patients with a higher educational degree. Healthcare professionals may need to consider the negative effect of informative video before MRI.
Keywords: magnetic resonance imaging, MRI, anxiety, nurses’ role, informative video, patient, interventions, STAI-Y
Introduction
Magnetic resonance imaging (MRI) has become one of the most essential diagnostic imaging methods in healthcare; it is used for evaluating a wide range of disorders, including cancer, stroke, bleeding, and other diagnoses; MRI examination is non-invasive and does not use ionizing radiations such as x-ray and CT scan.1–3 Furthermore, it is considered biologically safe and painless.4 The number of MRI scans is increasing worldwide and has reached more than 80 million.5 Radiation exposure can be a concern for pregnant women, and multiple factors can be considered, including the timing of exposure, exposure to low or high doses, type of radiation, and the route; however, compared with other imaging modalities, along with ultrasound, MRI is preferable in pregnancy, and no evidence indicates that MRI can harm the fetus.6–8
Regardless of the benefits of an MRI, it is contraindicated for patients with internal ferromagnetic objects.9 One of the contraindications for an MRI examination is the presence of a cardiovascular implantable electronic device (CIED); however, by following the safety protocol, an MRI can be performed safely in a patient with a modern CIED.10 In addition, one of the most common disadvantages of MRI is that people who undergo MRI may feel anxious before and during the examination, which may negatively affect image quality. Patients’ experiences of anxiety may prevent them from attending or completing MRI examinations. In a previous study, the estimated average number of patients who did not attend their appointments was 11.2%.11 Patient anxiety can be a cause of patient movement, which spends attentional resources, as it reduces the patient’s ability to stay still, causing the MRI examination to be repeated; therefore, the examination time increases, and expensive resources are consumed.12
Patient anxiety is induced by multiple factors concerning the nature of MRI, such as loud machine noise, closed tunnel, and long examination time, and by patient-related factors, such as fear of pain, the possible findings, and of losing control.13 The patient may get false information transmitted from family or friends who had a negative experience with an MRI scan, making them more nervous.14
Several studies have suggested different methods to overcome MRI-related anxiety. Anxiolytics have been recently used to reduce anxiety-related reactions in MRI examinations. The utilization of anxiolytics in adult outpatient MRI units has been evaluated.15 It was found that radiologists prescribed just over half of anxiolytics, in which these radiologists are commonly not involved in formal pharmacology training programs during residency.16 This results in about 40% of MRI patients being scanned too early before the peak effect of anxiolytics prescribed.15 In addition, the use of anxiolytics raises the need for monitoring patients’ vital functions to prevent any complications during MRI.17 Therefore, to avoid medications, several alternatives have been proposed to reduce the anxiety during MRI.18–20 One such method is audio-guided self- hypnosis. A recent study reported a significant reduction in claustrophobia in high-risk MRI patients using audio-guided self-hypnosis techniques.21 However, our study did not use any anxiolytic or audio-guided self-hypnosis techniques to reduce patients’ anxiety before MRI.
According to Grey et al,22 anxiety can also be reduced by simple interventions, such as providing accurate information about MRI machines and the procedures, listening to recorded audios of the MRI machine, and visiting the control room before scanning. An advisable practice is to prepare and assess patients for MRI scanning before the examination. The study estimated that patients experience less anxiety when they get more written and sensory information before being examined.22 The acoustic commotion resulting from an MRI machine is a remarkable factor that influences a patient’s inclination; during MRI assessments, the scanner produces different boisterous sounds, which are like a progression of rambunctious thumping, ringing, or noisy tweeting; the safety of a patient during the MRI evaluation can be significantly enhanced by reducing noise levels.23 The noise levels generated by MRI scanners have been reduced by 97% in new technology, leading to reduced patient anxiety.24
Although modern MRI machines also emit noise, this modification has remarkably affected the patient experience.23 A group of subjects whose sensory stimulation was evaluated during an MRI scan using olfactory stimuli intended to have a sedative effect reported an improvement in their subjective experience scores even though it did not affect their movement during an MRI.25 Anxiety helps keep the patient still throughout the examination process. Another common problem with MRI is claustrophobia, which is the excessive fear of tight spaces. A patient who experiences claustrophobia may not fear the enclosed place itself, as much as what can happen to them in this place.23 Other studies reported that claustrophobia might cause fear of an inability to control their anxiety or a fear that the scanner has radiation that could cause harm to them.26 The claustrophobic reaction incidence that results in failure or premature termination of an MRI examination is between 0.5% and 14.5%.27
Using 5-min event recall tasks (happiness and anger recall) and a 5-min Stroop Color-Word Test (SCWT) it was found that positive and negative moods are related to heart rate changes.28 Breathing characteristics are essential predictors of anxiety.29 One study that used Spielberger State and Trait Anxiety Inventory30 and MRI Fear Survey Schedule (MRI FSS)31 to measure anxiety level found that the highest level of anxiety among patients who underwent the examination was initially for both anxious and non-anxious patients and decreased over time, as indicated by their heart rate.32 According to Oxon,33 all healthcare providers must understand patients’ physical and psychological needs to help them provide the best care. An important role of an MRI practitioner is to loosen up patients and cause them to have a sense of security before the MRI scan; the ideal method of accomplishing this is by giving them detailed information about how the examination is done, what the exact checking time is, the insights that will be gained from the MRI results and what the assessment needs from them.34 According to Grossman,35 the patient must be taught before the assessment and be offered time for responding to any potential inquiries and to cause him to feel comfortable and safe. Nursing is increasingly becoming more prevalent in radiology settings, and radiology nurses must be proactive patient-centered and willing to collaborate with a diverse group of people; often, radiology nurses are pioneering new methods. Patients with more complex healthcare problems and the growing sophistication of procedures within the modalities necessitate motivated nursing practitioner skills.36
Evidence in many previous studies shows that patient anxiety can pose problems that can hinder the MRI test process, which may also have unfavorable effects on both patients and the healthcare organization, as it can cause economic losses to healthcare establishments. In Saudi Arabia, sedation strategies for MRI patients are feasible techniques that can alleviate anxiety.23 In a study in Finland, Földesa et al37 stated that anxiety reactions in MRI can cause unintended motion (movement artifact) and, accordingly, interpretation issues; moreover, they disagreed with using anesthesia and considered it unpreferable because it makes the method high-priced. Moreover, in the USA, nurses shared that anxiety interferes with the delivery of care (60.3%), and most respondents formally assessed it in their patients [61.7%].38
According to a UK study Tugwell et al,39 the routine arrangement letter did not contain sufficient data to fulfill most patients, which argues unequivocally for an improvement in current practice. According to a study in Turkey,2 MRI anxiety can be diminished by visual and written data and visual data might be more successful in reducing anxiety than written data. In the MRI evaluation of patients with acute stroke, Lin and Zhang40 found that high-quality nursing interventions have effects that can enhance reduce anxiety; therefore, increasing the completion rate of the test, shortening the length of the examination, and enhancing nursing satisfaction with a more substantial application is valuable. The combined intervention of information and communication was found to reduce anxiety prior to MRI scan.4 It was also reported that patient anxiety can be significantly reduced by listening to music during an MRI scan.37 In their study, State-Trait Anxiety Inventory (STAI) was used before the MRI scan to measure the anxiety level, whereas the STAI-State anxiety level, open-ended questions, Claustrophobia Questionnaire (CLQ) were measured after the scan.37
Studies that assess patient anxiety levels before MRI in Saudi Arabia are lacking. Moreover, the Arabic version of the state-trait anxiety inventory (STAI-Y) (Supplementary) questionnaire has never been used to measure MRI anxiety in Saudi Arabia or nurses’ roles to manage this type of anxiety. Also, insufficient studies have been conducted in Saudi Arabia to determine and focus on the effect of nurses’ roles to reduce patient anxiety during MRI scans. We assume that when nurses provide instructions about MRI before scans begin, they can influence and reduce patient anxiety compared with those who did not receive instructional information pre-MRI. Our work aimed to assess nurses’ roles through the dissemination of audio-visual instructional information pre-MRI scans in reducing MRI-related anxiety.
Theoretical Framework
The cognitive-behavioral theory is a branch of psychology that explains that behaviors and feelings are controlled by a person’s thoughts and control their actions. The cognitive theory indicates the reasons responsible for fear and anxiety: loss of control, such as unpredictable or uncontrollable events, can cause anxiety and/or depression; an inability to create a coping response to a threatening event; and state anxiety versus trait anxiety. State and trait anxiety means the personality traits of an individual. State anxiety is an emotional response that includes feelings of tension and fear; by contrast, trait anxiety is the probability of a person experiencing anxiety in stressful situations and is a characteristic of a person that can be used to explain the person’s behavioral consistencies.41 According to Rachman,42 people may see some natural signs that are life-threatening or dangerous caused by incorrect interpretation of these stimuli.
Methods
This is a cross-sectional and interventional study that was developed to identify nurses’ roles in reducing MRI-related anxiety in patients before MRI scans using informative video at two public hospitals in Tabuk City, Saudi Arabia. A convenience sample of 16 patients as the intervention group and 28 patients as the control group were included. Patients were divided into cases and control groups randomly in similar examination conditions. For example, on day one the first patient undergoes an MRI scan without watching the informative video. This patient was given STAI survey about 20 minutes before the scan and heartbeat, blood pressure, and oxygen level were measured during this period. The following patient watches the informative video in the waiting area about 30 minutes before the scan. Then, an SATI survey is provided to this patient about 20 minutes before the scan, and vital signs measured during this period in which this patient represents the case group.
We used the STAI to measure pre-MRI-related anxiety. It contains 40 items that consist of closed-ended questions, with two subscales (state and trait) with 20 items for each. The average time required to complete the survey was approximately 15 minutes.
Ethical Approval
The ethical approval was obtained from The Institutional Review Board (IRB), General Directorate of Health Affairs, Tabuk Region [Registration No. H-07-TU-077] on March 11, 2021. The guidelines outlined in the Declaration of Helsinki43 were followed. A consent form was distributed to all participating patients before the exam with full details about the study and they were informed that they have the right to withdraw at any time. Participated patients were also informed that all data are highly confidential.
Tool
The STAI-Y Arabic version (supplementary) of the questionnaire has high reliability and strong validity among Arabic speakers and has been tested among Saudi adult dental patients.44 Data were gathered from the control group in March 2021 through an online link.
STAI-Y was used, and participants’ blood pressure, oxygen saturation, and pulse rate were measured to compare the results between intervention and control groups with the nurses’ roles of providing an informative 2-minute video clip recorded by the research team in the same MRI room of the intervention group. An additional comparison was established among the participants’ gender, educational level, and previous MRI scan experience.
The video contains comprehensive information and instructions about the MRI being free from ionizing radiation, being safe for pregnant and lactating women, the device’s sounds, the tunnel’s size and potential weight, and the examination duration. The video also contained the importance of removing personal metal tools before the examination, remaining constant during the examination for the quality of results, and a radiologist’s presence to monitor the patient. The video emphasized the patient’s ability to stop the examination whenever he wishes. The informative video was spoken in Arabic with English subtitles as all patients were Arabic speakers.
Online informed consent from the control group and written informed consent from the intervention group were collected as the first part of the questionnaire. It included an explanation of the anxiety questionnaire before the MRI and the purpose of the study. It also emphasized that data are collected confidentially. The participants were free to agree or reject continuing.
Inclusion Criteria
• Adult, male, and female patients. • Agreement to participate.• Arabic speakers.
• Patients having MRI scans. • Conscious patients.
Exclusion Criteria
• Patients contraindicated from undergoing MRI scans:45
• patients under sedatives • Patients with severe diseases. • Younger than 18 y/o.
• Patients with mental disorders. • Refusal to participate. • Patients more than 150 kg.
Statistical Analysis
Data were checked for completeness, and errors were corrected. The reliability of the questionnaire was checked using a Cronbach’s alpha test (alpha value = 0.803). Categorical variables are presented as frequencies and percentages. All numerical variables were non-normally distributed according to the Shapiro–Wilk test, apart from age, which was normally distributed. These were presented as the median and interquartile range (IQR). The sociodemographic characteristics (gender, education level, marital status, and previous MRI experience) were compared between the cases and controls using chi-square tests. The median pulse, oxygen saturation, and blood pressure were compared between cases and controls using Mann–Whitney U-tests. The median values for all state anxiety and trait anxiety questions were presented and compared between cases and controls using the same test. The total state and trait anxiety scores were calculated by using the sum function and were compared between cases and controls by Mann–Whitney U-tests. The same test was done after classifying the dataset by gender.
The analysis was performed with a 95% confidence interval using the Statistical Package for Social Science (SPSS), version 23.0 (IBM, Armonk, NY, USA). Cronbach’s alpha tests for reliability analysis and comparison (Table 1) between cases and controls in terms of pulse, oxygen saturation, and blood pressure were conducted. Moreover, cases and controls were compared in terms of the median total state anxiety and trait anxiety scores. Cases and controls were also compared in terms of the median total state anxiety score split by gender, previous MRI experience, and level of education.
 |
Table 1 Cronbach's alpha test |
Results
This study included 16 cases and 28 controls. The gender distribution in the case group and the control group was equal (50% males and 50% females in both groups). The median (IQR) age of the intervention group was 37.5 years (27.3–45.0), while it was 31.5 years (26.3–38.8) for the control group. The age difference between the two groups was not statistically significant (p = 0.160). Similarly, there were no significant differences in other categorical demographic variables, including marital status and educational levels (Table 2). Among the cases and controls, 43.8% and 50% had previous MRI experience, respectively (OR = 1.286, p = 0.690) (Table 2).
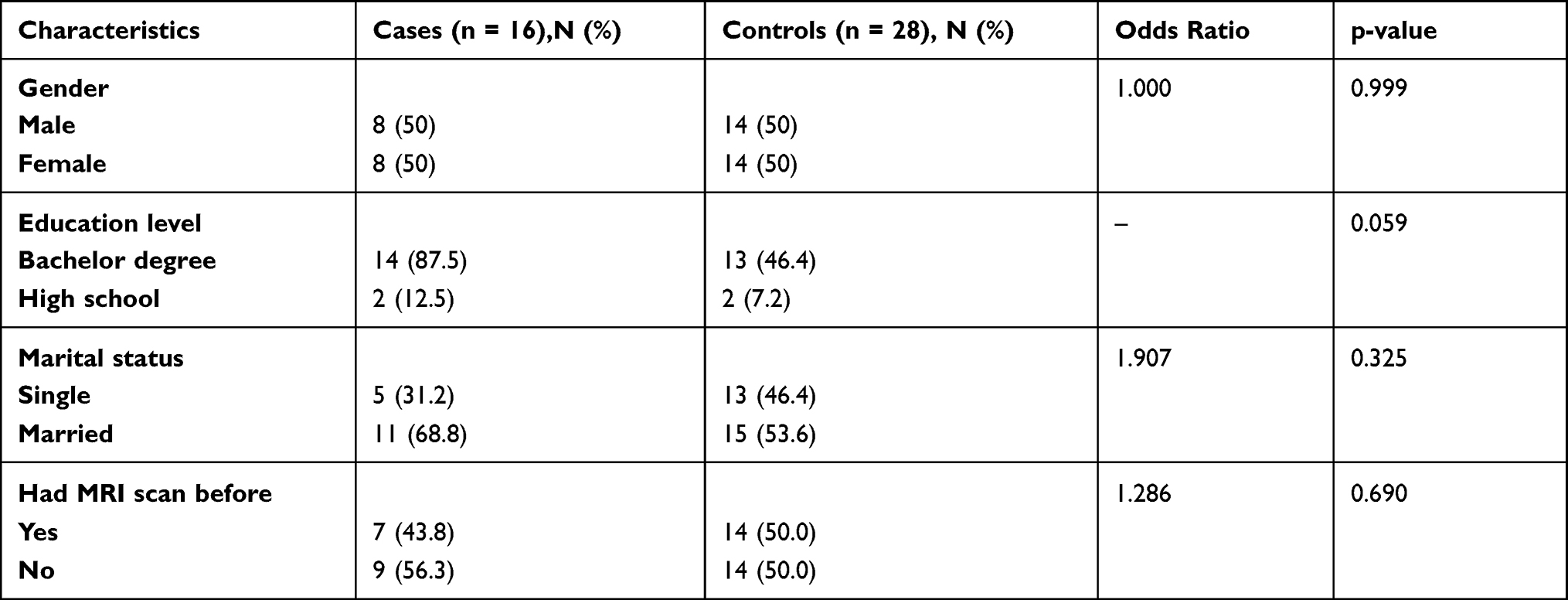 |
Table 2 Socio-Demographic Characteristics of Cases and Controls |
The difference between cases and controls in terms of vital signs (eg, pulse, oxygen saturation, systolic blood pressure, and diastolic blood pressure) was not statistically significant (all p-values > 0.050) (Table 3). The outcomes of state anxiety and trait anxiety questions for the cases and controls were presented in Tables 4 and 5. The cases group showed statistically significantly higher scores for item numbers 4, 6, and 17, with p-values of 0.015, 0.014, and 0.022, respectively. However, for other items and all trait anxiety and trait anxiety individual items, the differences between cases and controls were not statistically significant (all p-values > 0.050) (Tables 4 and 5).The median (IQR) state anxiety score in cases and controls were 52.5 (48.3–55.0) and 47.0 (43.3–50.0) (p-value = 0.010). Therefore, the cases had a significantly higher levels of state anxiety compared to the controls. In contrast, the Trait anxiety score was not significantly different between cases and controls (p-value = 0.508) (Table 6).
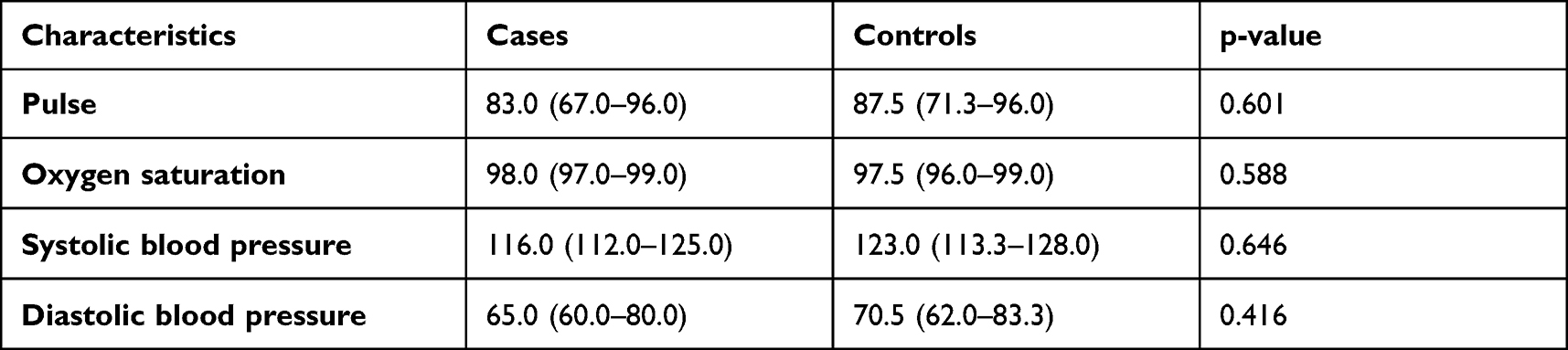 |
Table 3 Comparison Between Cases and Controls in Terms of Pulse, Oxygen Saturation, and Blood Pressure, Median (Interquartile Range) |
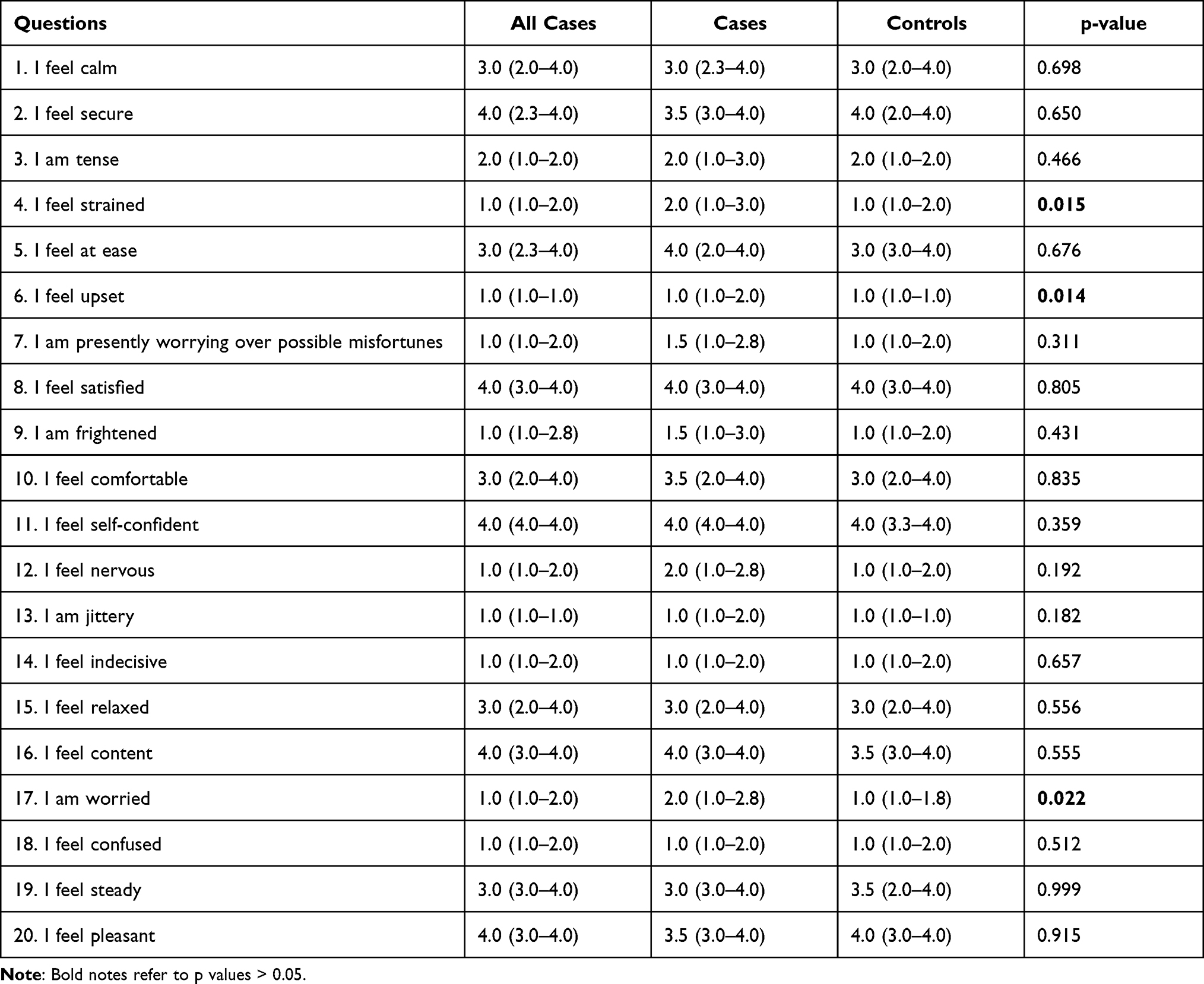 |
Table 4 State Anxiety Question Answers, Median (Interquartile Range) |
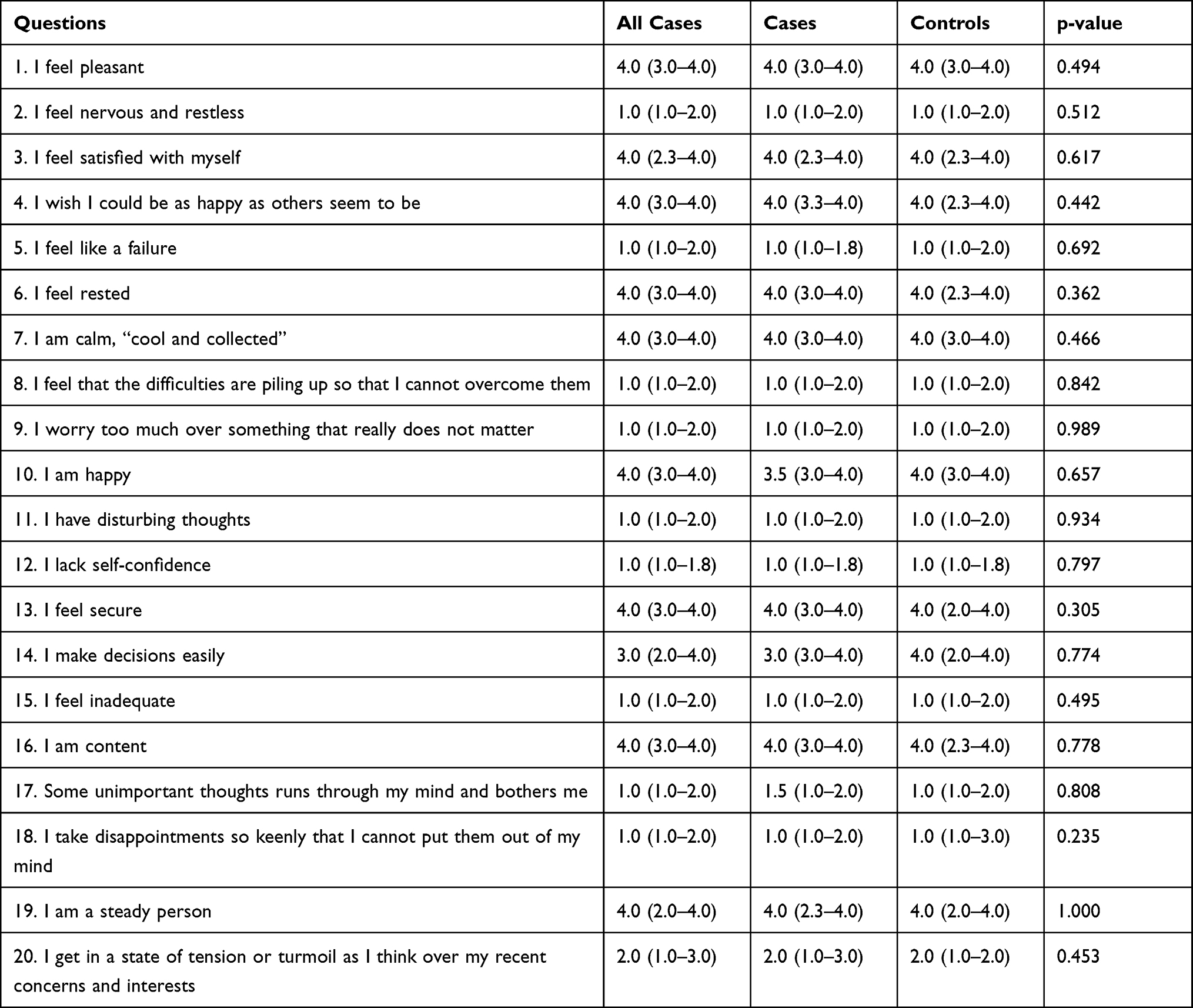 |
Table 5 Trait Anxiety Question Answers, Median (Interquartile Range) |
 |
Table 6 Comparison Between Cases and Controls in Terms of Median Total State Anxiety and Test Anxiety Scores |
In addition, a comparison was done after splitting the dataset by gender. Among the males, no difference in state anxiety and trait anxiety was found between the cases and controls (p-values = 0.131 and 0.864, respectively). However, among the females, state anxiety was found to be higher (median = 53.0, IQR = 48.3–55.0) in the cases than in the controls (median = 46.5, IQR = 42.5–50.0), with a p-value of 0.029. The trait anxiety was similar between the cases and controls in the female group (Table 7).
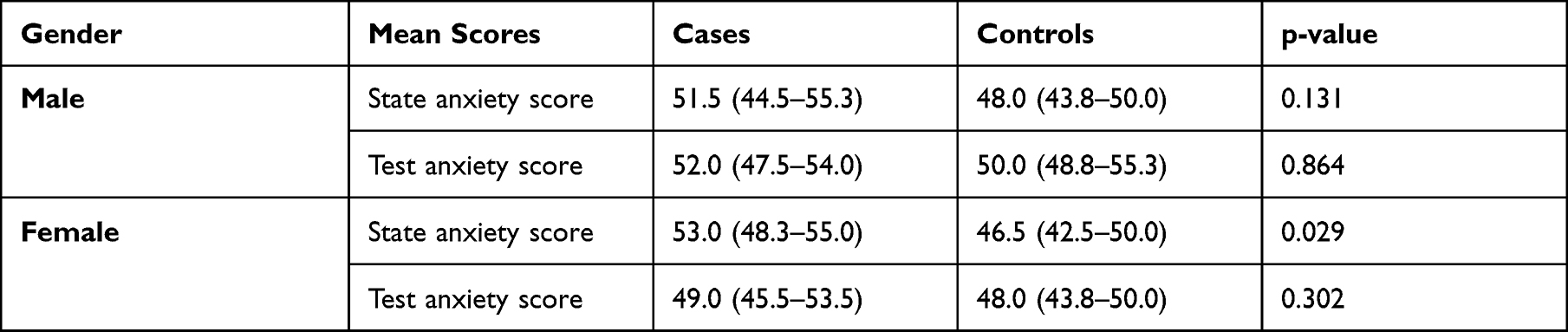 |
Table 7 Comparison Between Cases and Controls in Terms of Median Total State Anxiety Score Split by Gender |
The Trait anxiety was similar between cases and controls in the female group. (Table 7). Regarding participants’ stratification based on the previous MRI experience, results showed that the cases group who had undergone a previous MRI had significantly higher state anxiety scores (median = 55.0, IQR = 49.0–56.0) than those in the control group (median = 48.5, IQR = 43.0–50.0, p = 0.020 (Table 8). In addition, the state anxiety score differed significantly between cases and controls when the analysis split by educational level in which high academic degrees (median = 52.5, IQR = 48.8–55.0) in the case group and (median = 47.0, IQR = 41.0–49.5) in the controls group, p = 0.007 (Table 9).
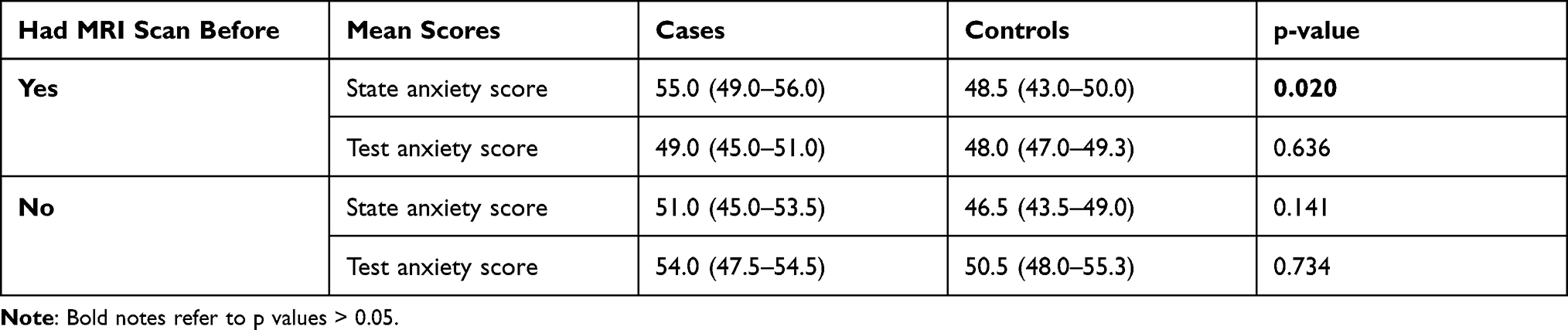 |
Table 8 Comparison Between Cases and Controls in Terms of Median Total State Anxiety Score Split by Previous MRI Experience |
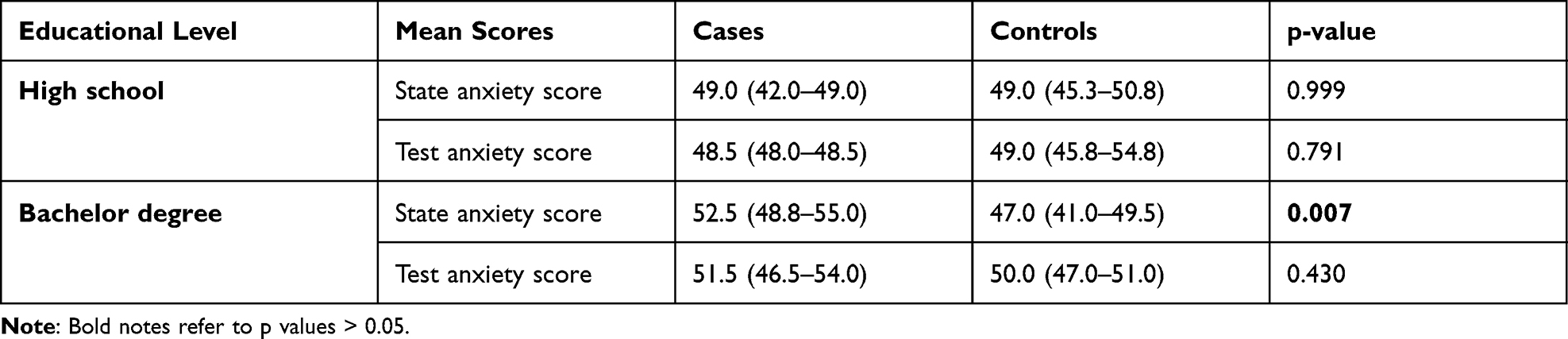 |
Table 9 Comparison Between Cases and Controls in Terms of Median Total State Anxiety Score Split by the Educational Level |
Discussion
This cross-sectional and interventional study was conducted to analyze nurses’ roles in alleviating the anxiety of MRI patients using a brief informative video. The anxiety levels of participants before MRI were measured using the STAI-Y. The video was displayed to a case group before answering the questionnaire, whereas the control group answered the questionnaire without watching the video. A comparison was made to assess the effect of the participants’ gender, previous MRI scan experience, and educational level, in addition to measuring and comparing pulse rate, blood pressure, and oxygen saturation. To our knowledge, this is the first interventional study of its type in Saudi Arabia.
In general, one of the most common drawbacks of MRI is the patient’s fear of the MRI environment. According to Grey et al22, this usually leads to an inability of the patient to stay still during the scan, which can lead to early termination of the examination and negatively affects the quality of the image.
Providing detailed information in different forms is expected to positively affect patients who are feeling fear of the unknown, which indirectly suggests that patients with the first MRI experience are likely to be anxious.39 This is clear in that patients with previous MRI experience proved to have lower levels of anxiety because they knew what to expect.46 A previous study showed that patients who reported receiving information about MRI or a DVD containing MRI clips or relaxation training before commencing the examination had lower anxiety levels than those who did not receive MRI information.47 Previous research suggests that visual data have more benefits and are more successful in reducing anxiety than other interventions.2 This is supported by several previous studies.48–51
However, contrary to our expectations, our study showed that STAI scores were significantly higher in patients who had seen the informative video clips. This is because the most significant outcomes that represented high levels of state anxiety were found in the case group’s answers for item numbers 4, 6, and 17, that is, “I feel strained,” “I feel upset,” and “I am worried,” with p-values of 0.015, 0.014, and 0.022, respectively. Why STAI scores increase in patients after receiving an informative video is unclear, suggesting that informative videos may negatively impact patient levels of anxiety. These results can be explained by the following. First, patients may think that health professionals provide information only in high-risk procedures, such as surgical operations and anesthesia, which may require further questioning to report their expectations after the video. Second, patients may have no idea about MRI, and visualizing MRI scanners in videos may provoke the level of anxiety, given that approximately 44% of the patients had no previous MRI experience. We also found that among females, higher State anxiety scores were observed in cases compared to controls (p = 0.029). This may indicate that females are more sensitive to informative video than males. This contradicts a previous study that measured the trait anxiety and state anxiety among three groups [visual information, written information, and control) to find the most effective method to reduce anxiety Yakar and Pirinçci2]. Although both visual and written information reduced the anxiety significantly, no significant differences between or within genders in trait anxiety scores were found.2 Our results also showed a significant increase in the state anxiety score in cases with bachelor’s degrees compared to controls (p= 0.007). This may indicate that informative video provokes expectations in the knowledgeable patients which increases the level of anxiety compared to controls. In addition, we found that patients who had previous MRI reported significantly higher state anxiety scores than those in the control group with p = 0.020 (Table 8). This raises the concern of whether previous MRI scans could provoke anxiety in some patients due to the bad experience. Further studies may be needed to investigate the association between past MRI experience and patient anxiety prior to the scan.
Our results also revealed no significant difference in using video intervention on vital signs. This indicates that the informative video used in our study had no profound effect that would change the biological signs of the patients. Our result contradicted that of a recent study reporting a significant decrease in oxygen saturation during MRI compared to the levels before and after MRI scans.52 The fact that no statistically significant variations in the vital signs between case and control groups in our results support the idea that our video did not considerably alleviate the level of anxiety in MRI patients. This is consistent with a previous study in which no difference in blood pressure was observed between the cases and control groups when informative video clips were used.53
Our findings have several limitations. The sample size used in this study was small, which caused difficulty in accurately identifying significant relationships from the data. Further studies with larger samples from different regions are required. Another limitation is the use of a long questionnaire (STAI-Y) consisting of 40 items, which may have led to a high rate of incomplete answers. In addition, anxiety levels and vital signs were not compared before and after the scan in the same patients. The source of anxiety and the MRI findings were not assessed in this study.
Recommendations
The findings in our study cannot be generalized because of the previously mentioned limitations. Therefore, we recommend including a larger sample size from different cities across the country to validate and generalize the current findings. For future research, we suggest using a questionnaire with a minimum number of questions to increase the response rate. We also recommend assessing the anxiety level and vital signs before and after MRI scans and investigating the sources of anxiety and the MRI findings.
Conclusions
Patients awaiting MRI examinations proved to have high levels of anxiety. This study tested the impact of informative video on MRI patients before scan. State anxiety scores were significantly higher in the cases compared to controls. Patients in the cases group who had undergone MRI scans previously had significantly higher state anxiety scores than those in the control group. Among the females, state anxiety was found to be significantly higher in the cases than in the controls. Patients with higher education in the case group had higher state anxiety than those in the control group. The self-made visual tool used by nurses in our study did not reduce the level of anxiety in MRI patients. Healthcare systems may need to consider the potential negative impact of informative video before MRI. Further studies with larger sample sizes may address this problem.
Acknowledgments
We want to thank all the patients who participated in this study and the radiologists at King Fahd Specialist Hospital and King Khalid Hospital. All appreciations were sent to the University of Tabuk for the continuous assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kasban H, El-Bendary MAM, Salama DH. A comparative study of Medical imaging techniques. Int J Inf Sci Intell Syst. 2015;4(2):37–58.
2. Yakar B, Pirinçci E. Investigation of the effect of written and visual information on anxiety measured before magnetic resonance imaging: which method is most effective? Medicina. 2020;56(3):136. doi:10.3390/medicina56030136
3. Yamaguchi‐Sekino S, Nakai T, Imai S, Izawa S, Okuno T. Occupational exposure levels of static magnetic field during routine MRI examination in 3 T MR system. Bioelectromagnetics. 2014;35(1):70–75. doi:10.1002/bem.21817
4. Tazegul G, Etcioglu E, Yildiz F, Yildiz R, Tuney D. Can MRI related patient anxiety be prevented? Magn Reson Imaging. 2015;33(1):180–183. doi:10.1016/j.mri.2014.08.024
5. Enders J, Zimmermann E, Rief M, et al. Reduction of claustrophobia during magnetic resonance imaging: methods and design of the “CLAUSTRO” randomized controlled trial. BMC Med Imaging. 2011;11(1):1–15. doi:10.1186/1471-2342-11-4
6. Bulas D, Egloff A. Benefits and risks of MRI in pregnancy. In: Seminars in Perinatology. Vol. 37. No. 5. WB Saunders; October, 2013:301–304.
7. Lum M, Tsiouris AJ. MRI safety considerations during pregnancy. Clin Imaging. 2020;62:69–75. doi:10.1016/j.clinimag.2020.02.007
8. Sreetharan S, Thome C, Tharmalingam S, et al. Ionizing radiation exposure during pregnancy: effects on postnatal development and life. Radiat Res. 2017;187(6):647–658. doi:10.1667/RR14657.1
9. Orchard LJ. Implementation of a ferromagnetic detection system in a clinical MRI setting. Radiography. 2015;21(3):248–253. doi:10.1016/j.radi.2014.12.007
10. Ipek EG, Nazarian S. Safety of implanted cardiac devices in an MRI environment. Curr Cardiol Rep. 2015;17(7):1–6. doi:10.1007/s11886-015-0605-9
11. Norbash A, Yucel K, Yuh W, et al. Effect of team training on improving MRI study completion rates and no‐show rates. J Magn Reson Imaging. 2016;44(4):1040–1047. doi:10.1002/jmri.25219
12. Klaming L, van Minde D, Weda H, Nielsen T, Duijm LE. The relation between anticipatory anxiety and movement during an MR examination. Acad Radiol. 2015;22(12):1571–1578. doi:10.1016/j.acra.2015.08.020
13. Brand J, Köpke S, Kasper J, et al. Magnetic resonance imaging in multiple sclerosis–patients’ experiences, information interests, and responses to an education programme. PLoS One. 2014;9(11):e113252. doi:10.1371/journal.pone.0113252
14. Rotunda TJ. Reducing occurrences of MR-related claustrophobia in patients with PTSD. Radiol Technol. 2017;89(1):97–99.
15. Middelkamp JE, Forster BB, Keogh C, Lennox P, Mayson K. Evaluation of adult outpatient magnetic resonance imaging sedation practices: are patients being sedated optimally? Can Assoc Radiol J. 2009;60(4):190–195. doi:10.1016/j.carj.2009.06.002
16. Mayson K, Lennox P, Anserimo M, Forster BB. Canadian radiology residents’ knowledge of sedation and analgesia: a Web-based survey. Can Assoc Radiol J. 2006;57(1):35.
17. Tith S, Lalwani K, Fu R. Complications of three deep sedation methods for magnetic resonance imaging. J Anaesthesiol Clin Pharmacol. 2012;28(2):178. doi:10.4103/0970-9185.94837
18. Munn Z, Jordan Z. Interventions to reduce anxiety, distress and the need for sedation in adult patients undergoing magnetic resonance imaging: a systematic review. Int J Evid Based Healthc. 2013;11(4):265–274. doi:10.1111/1744-1609.12045
19. Schupp CJ, Berbaum K, Berbaum M, Lang EV. Pain and anxiety during interventional radiologic procedures: effect of patients’ state anxiety at baseline and modulation by nonpharmacologic analgesia adjuncts. J Vasc Interv Radiol. 2005;16(12):1585–1592. doi:10.1097/01.RVI.0000185418.82287.72
20. Viggiano MP, Giganti F, Rossi A, et al. Impact of psychological interventions on reducing anxiety, fear and the need for sedation in children undergoing magnetic resonance imaging. Pediatr Rep. 2015;7(1):13–15. doi:10.4081/pr.2015.5682
21. Napp AE, Diekhoff T, Stoiber O, et al. Audio-guided self-hypnosis for reduction of claustrophobia during MR imaging: results of an observational 2-group study. Eur Radiol. 2021;31(7):4483–4491. doi:10.1007/s00330-021-07887-w
22. Grey SJ, Price G, Mathews A. Reduction of anxiety during MR imaging: a controlled trial. Magn Reson Imaging. 2000;18(3):351–355. doi:10.1016/S0730-725X(00)00112-0
23. Almutlaq ZM. Discussion of the causes, effect and potential methods of alleviating patient anxiety when undergoing magnetic resonance imaging (MRI). Egypt J Hosp Med. 2018;72(5):4473–4477. doi:10.21608/ejhm.2018.9515
24. Dewey M, Schink T, Dewey CF. Claustrophobia during magnetic resonance imaging: cohort study in over 55,000 patients. J Magn Reson Imaging. 2007;26(5):1322–1327. doi:10.1002/jmri.21147
25. Stanley E, Cradock A, Bisset J, McEntee C, O’Connell MJ. Impact of sensory design interventions on image quality, patient anxiety and overall patient experience at MRI. Br J Radiol. 2016;89(1067):20160389. doi:10.1259/bjr.20160389
26. Thorpe S, Salkovskis PM, Dittner A. Claustrophobia in MRI: the role of cognitions. Magn Reson Imaging. 2008;26(8):1081–1088. doi:10.1016/j.mri.2008.01.022
27. Eshed I, Althoff CE, Hamm B, Hermann KGA. Claustrophobia and premature termination of magnetic resonance imaging examinations. J Magn Reson Imaging. 2007;26(2):401–404. doi:10.1002/jmri.21012
28. Kop WJ, Synowski SJ, Newell ME, Schmidt LA, Waldstein SR, Fox NA. Autonomic nervous system reactivity to positive and negative mood induction: the role of acute psychological responses and frontal electrocortical activity. Biol Psychol. 2011;86(3):230–238. doi:10.1016/j.biopsycho.2010.12.003
29. Dziuda Ł, Zieliński P, Baran P, Krej M, Kopka L. A study of the relationship between the level of anxiety declared by MRI patients in the STAI questionnaire and their respiratory rate acquired by a fibre-optic sensor system. Sci Rep. 2019;9(1):1–11. doi:10.1038/s41598-019-40737-w
30. Spielberger CD, Gorsuch RL, Lushene RE, Vagg PR, Jacobs GA. State-Trait Anxiety Inventory. Palo Alto, CA: Mind Garden; 1983.
31. Lukins R, Davan IG, Drummond PD. A cognitive behavioural approach to preventing anxiety during magnetic resonance imaging. J Behav Ther Exp Psychiatry. 1997;28(2):97–104. doi:10.1016/S0005-7916(97)00006-2
32. Van Minde D, Klaming L, Weda H. Pinpointing moments of high anxiety during an MRI examination. Int J Behav Med. 2014;21(3):487–495. doi:10.1007/s12529-013-9339-5
33. Oxon P. An introduction to psychological care in nursing and the health professions. Midirs Midwifery Digest. 2012;22(4). https://www.taylorfrancis.com/books/mono/10.4324/9780203804865/introduction-psychological-care-nursing-health-professions-helena-priest
34. Stogiannos N. Reducing patient’s psychological stress. A guide for MR technologists. Hell J Radiol. 2019;4(1). doi:10.36162/hjr.v4i1.256
35. Grossman VA. Fast Facts for the Radiology Nurse: An Orientation and Nursing Care Guide in a Nutshell. Springer Publishing Company; 2014.
36. Donnelly LF, Dickerson JM, Goodfriend MA, Muething SE. Improving patient safety in radiology. Am J Roentgenol. 2010;194(5):1183–1187. doi:10.2214/AJR.09.3875
37. Földes Z, Ala-Ruona E, Burger B, Orsi G. Anxiety reduction with music and tempo synchronization on magnetic resonance imaging patients. Psychomusicology. 2017;27(4):343.
38. Musa A, Carpenter-Thompson R, Baron DA, et al. Attitudes of preprocedural patient anxiety: a 2019 cross-sectional study of radiology nurses. J Radiol Nurs. 2020;39(3):210–214. doi:10.1016/j.jradnu.2019.12.011
39. Tugwell JR, Goulden N, Mullins P. Alleviating anxiety in patients prior to MRI: a pilot single-centre single-blinded randomised controlled trial to compare video demonstration or telephone conversation with a radiographer versus routine intervention. Radiography. 2018;24(2):122–129. doi:10.1016/j.radi.2017.10.001
40. Lin WU, Zhang L. Effect of high-quality nursing on improvement of anxiety and depression of patients with acute stroke in MRI examination. Iran J Public Health. 2017;46(12):1646.
41. Kelvens C. Fear and Anxiety. Diundah dari; 1997.
42. Rachman S. A cognitive theory of obsessions: elaborations. Behav Res Ther. 1998;36(4):385–401. doi:10.1016/S0005-7967(97)10041-9
43. Goodyear MD, Krleza-Jeric K, Lemmens T. The declaration of Helsinki. BMJ. 2007;335(7621):624–625. doi:10.1136/bmj.39339.610000.BE
44. Bahammam MA. Validity and reliability of an Arabic version of the state-trait anxiety inventory in a Saudi dental setting. Saudi Med J. 2016;37(6):668–674. doi:10.15537/Smj.2016.6.13935
45. Ghadimi M, Sapra A. Magnetic resonance imaging contraindications. In: StatPearls [Internet]. StatPearls Publishing; 2020.
46. Watt L. Evaluating patient experience in magnetic resonance imaging (MRI).
47. Powell R, Ahmad M, Gilbert FJ, Brian D, Johnston M. Improving magnetic resonance imaging (MRI) examinations: development and evaluation of an intervention to reduce movement in scanners and facilitate scan completion. Br J Health Psychol. 2015;20(3):449–465. doi:10.1111/bjhp.12132
48. Jamshidi N, Abbaszadeh A, Kalyani MN, Sharif F. Effectiveness of video information on coronary angiography patients’ outcomes. Collegian. 2013;20(3):153–159. doi:10.1016/j.colegn.2012.06.001
49. Liszio S, Masuch M. Virtual reality MRI: playful reduction of children’s anxiety in MRI exams.
50. Papa L, Seaberg DC, Rees E, et al. Does a waiting room video about what to expect during an emergency department visit improve patient satisfaction? Can J Emerg Med. 2008;10(4):347–354. doi:10.1017/S1481803500010356
51. Schofield P, Jefford M, Carey M, et al. Preparing patients for threatening medical treatments: effects of a chemotherapy educational DVD on anxiety, unmet needs, and self-efficacy. Support Care Cancer. 2008;16(1):37–45. doi:10.1007/s00520-007-0273-4
52. Arda KN, Akay S, Yetkin S. Is there a relationship between oxygen saturation and MRI-induced anxiety? A prospective study. Clin Imaging. 2020;60(2):147–152. doi:10.1016/j.clinimag.2019.12.005
53. Yoon YH, Yoon HJ, Lee SK, Kim KH, Kwon GH. The effects of the communication accompanied with music therapy on the anxiety of the patients during the MRI examination. J Korea Acad. 2016;17(3):93–102. doi:10.5762/KAIS.2016.17.3.93
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.