Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Nurses’ and Physicians’ Experiences After Implementation of a Quality Improvement Project to Improve Sepsis Awareness in Hospitals
Authors Gustad LT ![]() , Bangstad IL
, Bangstad IL ![]() , Torsvik M
, Torsvik M ![]() , Rise MB
, Rise MB
Received 6 September 2023
Accepted for publication 27 November 2023
Published 4 January 2024 Volume 2024:17 Pages 29—41
DOI https://doi.org/10.2147/JMDH.S439017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lise Tuset Gustad,1,2,* Inger-Lise Bangstad,1,* Malvin Torsvik,1 Marit By Rise3
1Faculty of Nursing and Health Sciences, Nord University, Levanger, Norway; 2Nord-Trøndelag Hospital Trust, Department of Medicine, Levanger Hospital, Levanger, Norway; 3Regional Centre for Child and Youth Mental Health and Child Welfare (RKBU Central Norway), Department of Mental Health, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway
*These authors contributed equally to this work
Correspondence: Lise Tuset Gustad
Faculty of Nursing and Health Sciences, Nord University, Levanger, Norway
, Tel + 47 90 74 75 68
, Email [email protected]
Purpose: Previous research has explored nurses´ experience with the implementation of early detection alert systems, and nurses and physicians’ perceptions of sepsis management and use of sepsis triage. As one of the first, this study aims to investigate the perceived usefulness of an interdisciplinary quality improvement project including standardized sepsis patient pathway to improve the early identification and treatment of sepsis patients.
Participants and Methods: This study was a qualitative study that employed semi-structured interviews with thirteen ward nurses and five ward physicians recruited by convenience and respondent-driven sampling, respectively. The interviews explored the perceived usefulness of mutual training in sepsis care in medical hospital wards. We applied Systematic Text Condensation to analyze the experiences and knowledge of professional identification and cooperation in early identification of sepsis patients.
Results: The results revealed three main themes: Awareness of sepsis, collaboration between nurses and physicians, and clinical assessment and judgement. The findings highlighted the positive impact of the project in terms of raising awareness, improving communication, and enhancing the ability to detect and treat sepsis. The study also identified the importance of repetition and reminders to maintain awareness, the need for ongoing training for new healthcare professionals, and the challenges of collaboration and decision-making processes.
Conclusion: The sepsis intervention seemed successful in improving awareness of sepsis and enhancing interprofessional collaboration between nurses and physicians. Health professionals continued to rely on their clinical judgment but increased the use of objective measurements and communication of vital signs. Continuous repetition and education for new colleagues were identified as important factors for the sustainability of the intervention. Overall, the study highlights the importance of standardized protocols and training for early detection and management of sepsis in healthcare settings.
Keywords: qualitative study, sepsis, early identification, interprofessional training program
Introduction
Sepsis is a dynamic, rapid and life-threatening disease due to a dysregulated response to infection,1 affecting 48.9 million people worldwide every year.2 In 2020, 11 million sepsis-related deaths were reported.2 As there is no gold standard test, diagnosing sepsis can be challenging. Healthcare professionals must often rely on a combination of test results and clinical signs of organ failure (such as tachypnea, hypotension, tachycardia, oliguria, disorientation and icterus), as well as their knowledge of how these signs correlate with the likelihood of infection.3 All three Surviving Sepsis Consensuses (SSC) agree on early and timely identification and treatment in order to achieve good patient outcomes.1,4,5 As mortality increases with the development of organ failures6 and to identification and treatment initiation,7 the SSC has provided different guidelines including screening and early alert tools for sepsis.8
Although bedside nurses play a crucial role in identifying the early stages of sepsis,9–12 the SSC guidelines provide little information on their role in sepsis management.12 In the past, the SSC campaigns have mainly targeted the emergency departments and the intensive care units.13–17 However, two interventions that aimed to increase knowledge, competence and systems for early detection of sepsis on general wards among bedside nurses resulted in improved survival and shorter ICU stays.18,19 Nurses thus can become capable of identifying sepsis,3 but they rely on physicians to initiate adequate treatment. Thus, collaborative and effective communication, alert systems and response standards within and between these groups of healthcare professionals are crucial for optimal patient outcomes.9,18–25 Previous research has explored nurses´ experience with the implementation of early detection alert systems25 and nurses’ and physicians’ perceptions of sepsis management and use of sepsis triage.22,26,27 However, to the best of our knowledge, no studies have investigated how nurses and physicians perceive the usefulness of mutual training in communication, alert, and response standards in sepsis care. Therefore, the aim of this study was to explore the experiences of nurses and physicians following the implementation of a cross-disciplinary quality improvement project designed to enhance the early identification and treatment of sepsis patients.
Materials and Methods
This study was a qualitative study that employed semi-structured interviews with nurses and physicians in medical hospital wards. We applied Malterud’s phenomenological approach which is inspired by Giorgi,28,29 to explore the experiences and knowledge of professional identification and cooperation in early identification of sepsis patients. The phenomenological approach seeks to understand phenomena as they are naturally experienced by the individuals.28 The phenomenon at interest in this study was the health care professionals perception of their complex everyday work before and after the implementation of a cross-disciplinary intervention to early detection of sepsis.
Study Setting
A cross disciplinary intervention was performed on all medical, surgical and gynecological wards at a Norwegian hospital with around 200 confirmed sepsis patients per year.19 In 2010, the hospital employed process mapping30 to develop a standardized patient pathway tailored to each patient’s response to sepsis.19 Table 1 details the different aspects of the intervention previously described by Torsvik et al, which effectively reduced sepsis morbidity and mortality.19 The project with all interventions were collectively known as “Stop Sepsis Nurse” which were introduced for doctors and nurses in April 2011, and implemented in September 2011, with reinforcements in 2012 and 2013. The full Systemic Inflammatory Response Syndrome and Organ Failure (SOF)-triage, including red flag criteria can be found in Torsvik et al 2016,19 page 2. In brief The SOF-triage asks the nurse to measure SIRS signs (respiratory rate, pulse, temperature and oxygen or carbon dioxide amount in blood). If at least two of the SIRS signs are deviating the nurse are asked to do triage for organ failure (low systolic blood pressure or drop >40 mmHg in blood pressure, acute disorientation, low oxygen saturation in blood despite given oxygen, long capillary filling time, high serum-lactate, low thrombocytes, and low urinary output). The Stop Sepsis Nurse guideline was revised in line with the new Sepsis-3 definition in 2016.1 The change was not radical as the SOF-triage already included clinical assessment of organ failures.19 With the Sepsis-3 definition, The Norwegian health authorities invited to three national learning networks; early identification of deterioration (2016), early detection of sepsis in the emergency department (2017) and early detection of sepsis in general wards (2018). The first and second author of the present manuscript participated in all these networks. Two of the networks advocated the National Early Warning Score (NEWS2)31 as a good tool to identify deterioration in general and for sepsis. In addition, the quick SOFA score (q-SOFA)1 was advocated for sepsis detection in emergency departments. As the first author previously had done work suggesting poor performance of the q-SOFA,32 we did not want this tool as the stand-alone identification tool. Thus, we incorporated NEWS and q-SOFA into our triage system for sepsis, thus both a worsening in NEWS and a worsening of organ failure would trigger a sepsis alert.
 |
Table 1 Schematic Overview Over the Interventions in the Stop Sepsis Nurse Project |
Participants and Recruitment
The participants were recruited from the pool of 200 ward nurses and 50 physicians employed in the five medical wards from September 2015 to January 2016. Nurse managers were requested to identify nurses who had been employed since the start of the project and were able to provide comprehensive information. An e-mail was sent to all nurses that the nurse managers identified as recruitable. This is often referred to as criterion sampling, a variant of purposive sampling, that aims to select cases meeting predetermined criteria.33 The CEO of the clinic suggested physicians selected by criterion sampling, and these were invited via email and were asked to suggest additional colleagues. Such suggestions from peers are often called snowball sampling.33 In total 18 respondents were recruited. Of these 13 (72.2%) were nurses and five (28.8%) were physicians. The mean age were 45.2 years, with a range from 31 to 59, see Table 2 for further baseline characteristics.
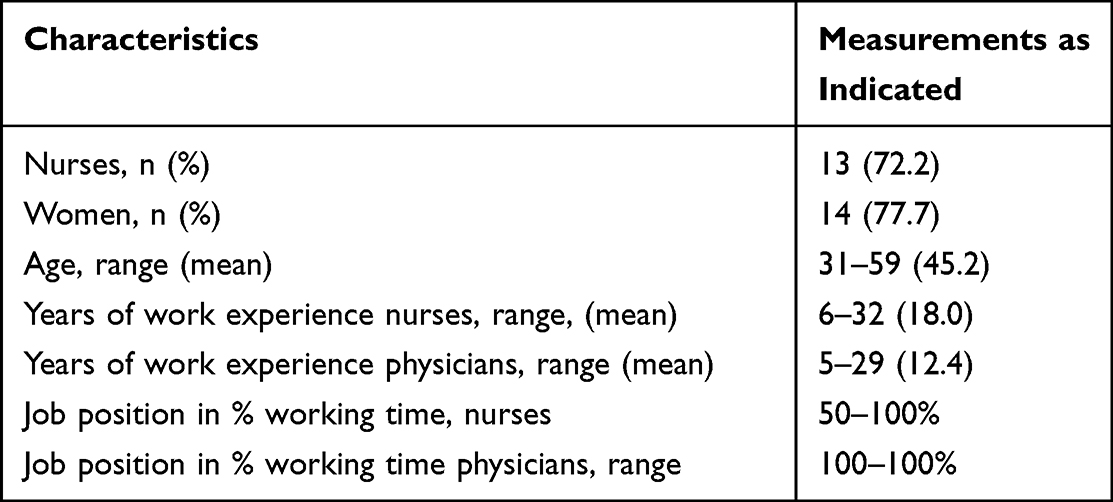 |
Table 2 Informants Baseline Characteristics, n=18 |
Data Collection and Analysis
Semi-structured individual interviews were conducted with the professionals to explore how they perceived the usefulness and experiences of the Stop Sepsis Nurse project. The interviews, which lasted between 20 to 50 minutes, were audio-recorded, and later transcribed verbatim. To analyze the data, we used the four analytic stages of Systematic Text Condensation (STC),29,34,35 a well-defined and structured method for qualitative data analysis. The first stage involved reading through the interviews several times to find initial themes while also bracketing the interviewers (ILB) preunderstanding.29 The second stage involved systematically reading the transcriptions line by line to identify units of meaning, which were sorted into preliminary themes, and adjusted as necessary. We used NVivo Pro 11, QSR international Pty LTD, to organize the units of meanings into the themes. In the third stage, the content of the units of meaning under each theme were abstracted and condensed. In the final stage, the material was re-contextualized to develop a comprehensive understanding of the data. Nuances under the themes were further categorized into subgroups and appropriate quotations from the material were chosen to illustrate the meaning of each theme and subgroup. The material was evaluated in several cycles between the four analytic stages during the process. An example of the analytical process is presented in Table 3.
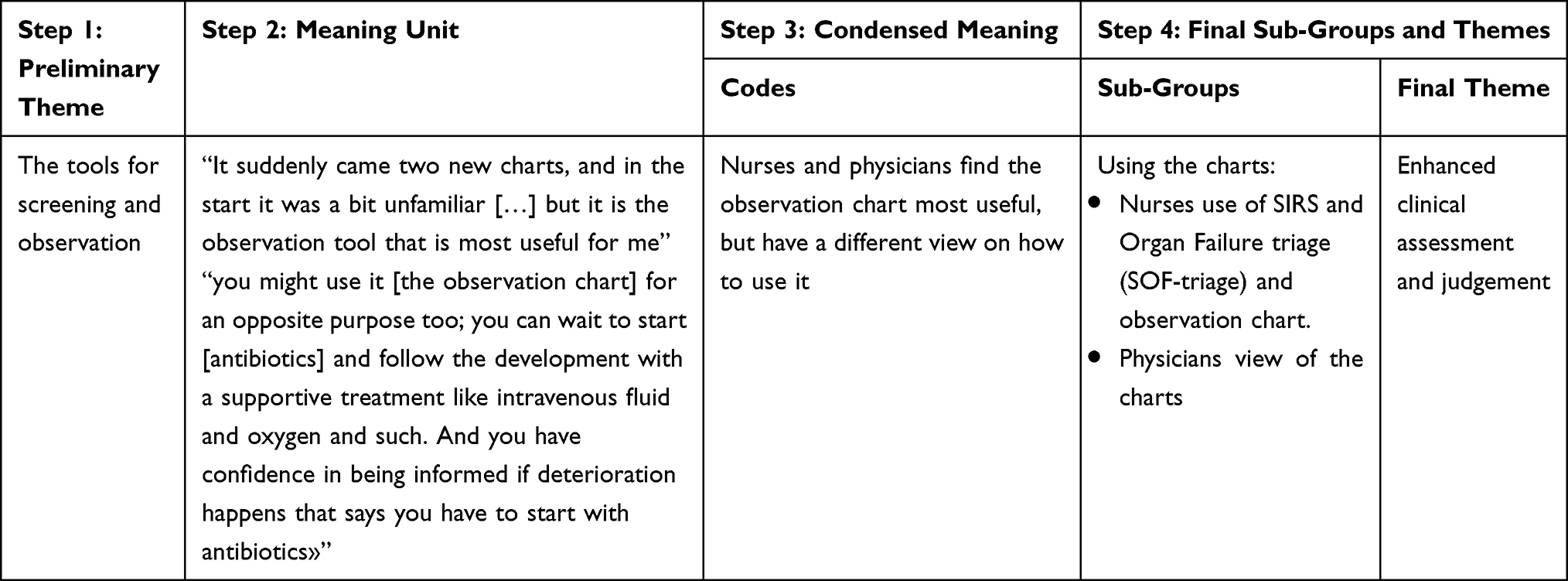 |
Table 3 Schematic Example of the Stepwise Analysing Process Using Systematic Text Condensation |
Results
Thirteen nurses (one male) and five physicians (three males) were interviewed. The participants ages ranged from 31 to 59 years, with a mean age of 45.2 years. The nurses had between 6 to 32 years (mean 18.0) professional experience and the physician’s had between 5 to 29 years (mean 12.4). All physicians had full-time positions at the hospital, while the nurses had positions ranging from 50% to 100%. All participants had been employed at the hospital prior to the stop sepsis nurse intervention, and six of the nurses had served as expert nurses during the intervention period.
During the interviews the professionals mainly discussed changes that took place in three specific areas after the intervention: Increased awareness of sepsis, improved collaboration between nurses and physicians, and enhanced clinical assessment and judgement. These three areas were identified as the main themes in the study’s result.
Main Theme #1. Increased Awareness of Sepsis
The nurses reported that the sepsis project had raised their awareness of sepsis, and the training sessions were particularly beneficial. In this main theme, the need of repetition and reminders was a sub-group. The training had provided them with knowledge about the rapid development of sepsis, and the importance of systematic observation for early identification and communication of deterioration. Consequently, the nurses felt their competence had increased, and they were better prepared to care for patients who were deteriorating into severe sepsis.
We focused a lot on it (…) the competence on the wards improved a lot, yes in all nurses (…) how much everyone knows, when we hear sepsis, it is like ringing a bell and then everyone immediately is alert. So, I feel that the knowledge is substantially increased after the training. (Nurse 7)
The physicians reported that the sepsis project had increased their awareness of the importance of early identification of sepsis. They also noted an increased focus on sepsis among ward nurses. The physicians observed that the nurses paid attention to the SIRS and organ failure triage (SOF-Triage) and used the vital signs belonging to the SOF-triage when communicating with the physician. In the past, the nurses had primarily reported only the patient’s blood pressure as a sign of deterioration.
We physicians quickly started to talk about an increased awareness on the wards. And not only on the medical wards, but also on the surgical wards. They [nurses] became more aware on sepsis and the SOF-triage criteria. [Physician 2]
The nurses stated that they believed the new awareness and focus resulted in earlier detection, enabling them to prevent patients from developing sepsis. Especially the patient case histories presented in the sepsis training program had made the nurses reflect upon previous patients, and how sepsis treatment could have been initiated earlier if they only had this knowledge previously.
I think that the increased knowledge of both nurses and physicians is leading to earlier initiation of treatment, resulting in patients becoming less ill and are being transferred to ICU less frequently. [Nurse 7]
The physicians, on the other hand, said they had discussed if the implementation of initiatives in the sepsis project would lead to fewer deaths.
Critical voices argued that the project would not improve survival, but I believe that it is always beneficial to focus on observation of our patients. This approach gives us all an increased awareness in the assessments and enable a quicker identification of patients who require a physician response. [Physician 4]
Sub-Group Main Theme 1: Repetition and Reminders
The nurses emphasized the significance of repeating the sepsis training, including frequent reminders to use the screening tools to avoid losing awareness. Sharing and discussing novel patient cases increased the awareness of sepsis. Furthermore, the nurses stressed the importance of ensuring that the sepsis training sessions also was given to new physicians and nurses to prevent unresponsiveness to patients deteriorating due to sepsis. They strongly felt that new nurses had to learn the detection of sepsis and new physicians had to be informed about the appropriate response and treatment algorithm.
It [training] needs to be continuously integrated, you know, even if you have had a project, because new nurses and new physicians are constantly starting. And as nurses, we can’t do much if the physicians are not informed about the project. It’s essential that they take it seriously when we call regarding a patient’s deterioration. They need to understand that they must prioritize these patients (]] Thus, we need to constantly repeat again and again [Nurse 12]
Main Theme #2. Collaboration Between Nurses and Physicians
Nurses perceived that the collaboration with the physicians had changed, mainly for the better, following the intervention period. The subgroups in this theme were changes in ways of communication, and physicians’ responses as experienced by nurses.
Changes in Ways of Communication
The nurses experienced that their communication had become more accurate and more focused on objective data, such as patients’ vital signs. They realized that they had previously reported the patients’ condition in more emotional and vague phrases.
It is much easier to call the physician now that we have these standardized criteria, because we now can report that the patient has two SIRS criteria, and it feels like we get a more specific response from the physician. It is easier to report objectively than to call and say, he’s [the patient] not feeling well. [Nurse 11]
The physicians also noticed changes in how nurses communicated about patient’s conditions, with a shift from diffuse terms to more reporting of vital parameters. Physicians reported that this made it easier to collaborate regarding patients and make decisions about the next step in treatments, ultimately saving time.
I think the communication is much more specific now. We are informed of the objective reason for being called; it could be due to a low blood pressure, anuria, or a patient with high fever and tachycardia, rather than just a vague statement like “I don’t like the patient’s condition”, as they used to communicate before.[Physician 4]
Physicians’ Response as Experienced by Nurses
Nurses felt the sepsis project had led to a better understanding between the professions. For example, nurses felt the response from the physicians had become much better. They were met with respect and their information were taken seriously.
It seems like the physicians I have been in contact with are well-informed about the SOF-triage, and I feel I get a good response to my observation. they come to the wards and assess the patient. [Nurse 3]
However, nurses expressed concerns that there were still challenges in the collaboration between the two professions. If the nurses sensed that a physician was unfamiliar with the SOF-triage algorithm, they used different methods to inform the physician about the sepsis-procedure.
If I sense that a physician is not informed about the SOF-triage, I tell them a little bit about it and almost try to put words into their mouth. Sometimes it is almost like giving an instruction. [Nurse 8]
The nurses also reported they had experienced that physicians were too busy to respond to the SOF-triage, and that after the intervention tried hard to get hold of other physicians if the first they called was too busy.
If the physician in charge is occupied, I try the next physician. Yes, I try the next (…). I do not give up on trying to reach someone. [Nurse 12]
Sometimes the nurses also disagreed with the physicians’ decision to just continue monitoring the patient and await sepsis treatment until further deterioration. This disagreement caused frustration in the nurses, as they would have preferred to start treatment immediately.
It is a frustration for nurses because, we have learned that we should intervene as soon as possible, and that every hour counts. I have learned this, and then the physician arrives and says “no, let’s wait a little and se. Just continue with observation”. Then we wait until we get a bacterial growth or something. [Nurse 12]
Main Theme #3. Clinical Assessment and Judgement
The participants talked about how the methods to assess the clinical situation had changed, both regarding technical assessment and use of measurements and charts, but also how the nurses’ clinical judgment influenced the assessment. The sub-groups in this theme were measurements of vital signs, using the charts, and clinical intuition (embodied know-how).
Measurements of Vital Signs
The nurses reported that the Stop Sepsis Nurse intervention increased their knowledge about importance of systematic measurement of vital signs when they suspected sepsis. It also helped them to put the measurements into a context to better understand the severity of the patient’s condition. They specifically mentioned that they were not aware of the importance of respiratory rate as a sepsis predictor before the intervention. However, they also experienced ambiguity between the patient’s need to sleep and the need for vital signs measurements, particularly during night-time.
At least I focus on counting respiratory frequency now, because at least I was not very good at doing that before. No. You just noticed they [the patients] breathed fast. [Nurse 5]
Using the Charts
Initially, nurses had hesitations about using the SOF-triage due to a concern about increased workload. However, once they had established the system of SOF-triage and followed the algorithm, they found that it actually saved them time. There were varying approaches to using the SOF-triage: some nurses filled it out and used it as evidence when communicating with physicians, while others used it as a checklist in order to ensure that all necessary measurements were taken. Some nurses integrated the SOF-triage into their thought process and no longer physically fill it out but used it as a mental checklist.
So we use the triage tool. Even if we don’t fill it in, we still have it at least as a template where we can consider how many of the areas of organ function are affected. This makes it much easier to communicate the information to others. [Nurse 9]
All the nurses found the observation chart very useful in providing an overview of the patient’s condition and response to treatment. This enabled the nurse-physician team to rapidly assess the patient’s condition and quickly decide on further treatment. Some nurses also used SOF-triage in conjunction with the observation chart. The observation chart documented their ongoing surveillance of the patient`s condition, while the SOF-triage supported rapid response from physicians.
I feel that we are good at using the observation chart, where we document all measurements, medications, and infusions (.). When that one is properly completed and used, it is really good tool that we always have laying on the patients nightstand). If you come to take over the patient during the shift change, then you can see the whole day’s record of blood pressures and O2 saturation. So you have it all there instead of speculating and then maybe understanding or maybe misunderstanding the situation. [Nurse 7]
The physicians said they rarely heard nurses used the word “triage” when referring to patients suspected of developing sepsis. Additionally, the physicians were not very familiar with the SOF-triage chart. However, like the nurses, all the physicians found the observation chart to be a useful tool in monitoring patients’ conditions and discussing further treatment and follow-up plans. The physicians also reported using the observation chart to determine the appropriate timing for antibiotic therapy in accordance with Norwegian guidelines for antibiotic therapy in sepsis treatment.
However, you might use it [the observation chart] for the opposite purpose as well. You can choose to delay the start-up [of antibiotics] and monitor the how patient’s condition develops with supportive treatment like intravenous fluid therapy and oxygen. You can trust that you will be informed [by the nurse] if there is any deterioration suggesting that antibiotics are necessary. […] In the beginning, we were confident in starting treatment very quickly for patients fulfilling the criteria. However, due to concerns about overuse and antibiotic resistance, there has been a shift towards using it [the observation chart] as a support to await too. [Physician 4]
Clinical Intuition (Embodied Know-How)
The nurses highlighted the importance of using both clinical intuition and objective data for a comprehensive patient assessment. Nurses defined clinical intuition as a subconscious feeling or a gut instinct that could indicate when the patient was getting sicker or had deteriorated, it could appear when they entered the patient’s room and noticed everything at and around the patient, a sense of “something is going on”.
After the Stop Sepsis Nurse intervention, the nurses reported that their clinical intuition prompted them to take additional vital signs measurements to confirm their initial impression. They emphasized that using their clinical intuition in combination with objective data helped them to make a more comprehensive assessment of the patient’s condition.
It’s obviously important during the first meeting when you come into the patient room, your clinical intuition may determine whether you choose to take measurements or not. [Nurse 12]
The physicians also relied on their clinical judgment to make decisions regarding the patients’ treatment. If they perceived that the patient’s condition was deteriorating, they had no hesitation in initiating intravenous treatment.
Discussion
The professionals’ experiences of the interdisciplinary quality improvement project Stop Sepsis Nurse were described in three main themes of importance: Awareness of sepsis, collaboration between nurses and physicians, and clinical assessment and judgement.
Awareness of Sepsis
The literature suggests that a lack of knowledge among ward nurses about acute deterioration in general and sepsis in particular has been a known issue.36–39 One important advancement in Stop Sepsis Nurse project is that the nurses experienced that their new competence in measuring vital signs and in using the sepsis triage was important in the early identification of sepsis. As they experienced, they identified sepsis earlier than before they wished they had gained this knowledge earlier. Their subjective experience of being better at identifying sepsis was later confirmed in quantifiable effects of the nurse-led sepsis screening, with decreased morbidity, shortened ICU stay and increased survival.19 In short, the group after the intervention (comprising 409 individuals) showed significant improvements. They had a 2.7 times higher likelihood of surviving 30 days (95% confidence interval: 1.6 to 4.6), a reduced chance of severe organ failure (0.7, 95% CI: 0.4 to 0.9), and a shorter average stay in intensive care by 3.7 days (95% CI: 1.5 to 5.9 days) compared to the pre-intervention group (consisting of 472 individuals). The success of the intervention among nurses can as such be understood in light of the normalization process theory (NPT), which suggests that the nurses experienced a sense of coherence with the intervention (ie their nursing effort became patient-relevant).40 In addition, the interventions initiated a cognitive process and reflexive monitoring of past and current practice, which enabled a collective skill set, and shared understanding of clinical actions among all nurses and doctors. This process has earlier been shown to making it easier to sustain the new practice.40–42
Previous studies have found that the nurses documented vital signs more frequently after implementing standardized triage and observation tools and an alert and treatment flow chart,19,43 and that such knowledge of guidelines helps to reduce sepsis mortality.19,44 Of importance to reduce sepsis mortality, the SOF-triage contains many measurements and cut-offs for identifying sepsis similar to the Sequential Organ Failure Assessment (SOFA) score, the quick-SOFA (qSOFA) score and red-flag responses for deterioration including physician response time similar to the National Early Warning Score II (NEWS II).45,46 However, several studies have also indicated a decline in adherence to new guidelines over time.47–49 In our study, the nurses expressed a need for continuous repetition and training of old and new members of the interprofessional team in order to maintain effective collaboration and good patient outcomes. The need for everyone to “be on board” calls for a good hospital quality system that includes continuous repetition and training of new staff, and this may be an important process indicator for maintaining competence.50
Collaboration Between Nurses and Physicians
Another important advancement in the Stop Sepsis nurse project is the that both doctors and nurses experienced more frequent use of objective and accurate communication, including the reporting of objective data or the use of medical terms by the nurses. Such systematic observation and objective communication is in a previous study shown to be more likely to trigger a physician response compared to subjective communication by the nurses.51 The Stop Sepsis Nurse project also identified more prompt and timely fluid resuscitation after the intervention,19 which is an objective measurement of the participants experience of improved collaboration between nurses and physicians. Another key factor is the emphasis on collective interprofessional coherence; trust in each other’s competence, need for unambiguous guidelines for the sepsis identification and treatment, which is previously also shown important for collaboration between health care professionals.22 The new intervention might have been beneficial due to a combination of factors, including improved communication, clearer roles and responsibilities for each profession, and the establishment of unambiguous guidelines for sepsis identification and treatment. All of the above elements are central in the NPT,41 which explain the experienced satisfaction with the Stop Sepsis Nurse among nurses and doctors.
Measurement of Vital Signs
The third advancement of the project was that both professions experienced that clinical assessment and judgement improved, nurses used the systematic measurement of vital signs in order to communicate effectively with the physicians.
The Use of Identification Tools
Previous research has identified the team’s perception of an intervention’s resource demand, usefulness, and user-friendliness as crucial success factors.41,42,52,53 The shift from skepticisms to acceptance of the new triage tool in our study was enabled through the positive experience of saving time, gaining professional control and improving cross-professional collaboration through its utilization. We argue that a key success factor for the project may therefore have been the iterative development of the tools through user pilots, with an emphasis on usability, usefulness, user experience and a sense of coherence.
Some of the nurses said that they used the SOF-triage as a check list in order to remember all the objective signs of SIRS and organ failure. Previous studies have shown that sepsis-related observations increase with the use of check lists.13,19 However, some nurses had also stopped using the SOF-triage because they felt they had internalized it as a part of their professional knowledge. This is in line with studies where senior nurses used clinical judgement in conjunction with NEWS II.54 This sense of mastering and internalizing procedural knowledge may explain why compliance with check lists often is found to decrease with time,55 and may be viewed as a natural process in the nurses’ development towards expert in the field as described by Benner (2009),56 rather than a negative development.
In previous studies, nurses often experienced frustration when they did not get appropriate physician responses when communicating patient deterioration.23,57 In our study, the nurses experienced frustration because physicians had a different approach to the observational chart when the physicians used the chart to await the start of antibiotics or when new doctors were uninformed about the sepsis algorithm. We see this frustration as a communication mismatch in and a lack of common objectives,58 particularly in terms of the timing of starting antibiotic therapy. The physicians was more aware of antibiotic resistance, and they did not want to start antibiotics inappropriately. Further, the intervention enabled the physicians to trust the nurses to alert them according to the SOF-triage alert system in case of deterioration. Despite this mismatch, both professions experienced higher satisfaction with the collaboration on sepsis patients after the intervention. As our intervention used collaborative training on sepsis cases, this might have further improved collaboration, as also shown in a previous study.22
Clinical Intuition
Despite the standardization of the sepsis algorithm, nurses, and physicians in the study experienced that they still felt the need to additionally use their clinical intuition or judgement. Intuition is known to detect subtle changes in patient’s condition even before there is a deviation in vital signs.56,59 After the intervention, nurses experienced to use their intuition as a trigger tool, the feeling of that “something is wrong with the patient” urged the objective measurements of vital signs. This finding is consistent with previous research on intuition as a triggering tool, which emphasizes the need to confirm intuitive feelings with measurements of objective vital signs.51,60 However, some researchers have found that sometimes intuition is used as a replacement for objective measurements.59,61 For the nurses in our study, intuition was experienced as a necessary and embodied knowledge that provided an overall impression of the patient’s condition. Some triggering tools, such as the NEWS2, include “health professionals concern about the patient” as a trigger for assessment,62 which aligns with the health professionals view on their own practice and professional knowledge. We believe that one key factor to the success was that the intervention enabled nurses to experience that objective measures of vital signs are a valuable and important addition to their intuition of caring for a patient in deterioration.
Strengths and Limitations
Overall, the study design had both strengths and limitations.
The strategic recruitment of nurses was a strength since this is a technique that strives to get variation in age, experience and gender mix in the sample.29 The snowball recruitment of the physicians may have led to a skewed sample with limited variation,29 however it is a strength that this study sought the experience of both nurses and physicians. The inclusion of only those who had experienced previous to the intervention was necessary to answer the study aim, however it limits the generalizability regarding usefulness of such interventions for those who start in a hospital with such a system in place.
The use of semi-structured interviews allowed for in-depth exploration of the participants’ experiences and perspectives, providing rich data. The interviewer (ILB) was both involved in the project Stop Sepsis Nurse and conducted the interviews. This could lead to a bias towards more positive expressions from the informants. However, ILB’s involvement in the intervention may also have helped to generate more relevant questions during the interviews and to facilitate a more open and honest dialogue with the participants. Prior to conducting the interviews ILB made an effort to acknowledge her preconception and biases, as recommended by Malterud.35
The participants were also informed that the interviews were not a test with right or wrong answers and were encouraged to provide their honest impressions of the intervention. Finally, the possibility of social desirability bias, where participants may provide responses that they perceive as desirable, cannot be ruled out.
Conclusion
Based on the results of the study, the Stop sepsis nurse intervention revealed several important experienced outcomes. First, both nurses and physicians experienced increased awareness of sepsis. The training sessions provided knowledge and increased competence in identifying and managing sepsis, which was proven to improved outcome for patients. Secondly, interprofessional collaboration between nurses and physicians was experienced improved following the intervention. Communication became more accurate and focused on objective data, which facilitated better decision making and saved time. Lastly, the study highlighted changes in clinical assessment and judgement. Nurses reported using systematic measurements and the observation chart to assess patient’s condition, and this enabled a quicker and more appropriate physicians treatment response. However, both nurses and physicians experienced that clinical intuition was still a crucial skill. Overall, this study contribute to the academic advancement in the field of sepsis management, as it highlights the importance of standardized protocols and interprofessional training for early detection and appropriate patient treatment.
Abbreviations
SOF-triage, Systemic Inflammatory Response Syndrome and Organ Failure (SOF)-triage; SIRS, Systemic Inflammatory Response Syndrome.
Data Sharing Statement
The transcriptions of the interviews can be shared upon reasonable request.
Ethics Approval and Informed Consent
The Regional Ethical medical committee (REK) deemed this project to be a quality improvement study and thus outside the scope of REK (ref no REK 2015/821/REK midt). The Norwegian Social Science Data services (NSD)/ SIKT (https://sikt.no/en/home) and the Data Protection Officer thus approved the project on behalf of the Institutional Review Board (IRB) (ref no 43538/3/LMR). All participants were informed about the study, that it was voluntary to participate and at all times possible to withdraw. The participants gave written consent to participate and to the publication of anonymized responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
All authors declare no financial competing interests nor non-financial competing interests for this work.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–211. doi:10.1016/s0140-6736(19)32989-7
3. Vincent JL. The challenge of early identification of the hospital patient at risk of septic complications. Ann Transl Med. 2017;5(3):56. doi:10.21037/atm.2017.01.49
4. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–1655. doi:10.1378/chest.101.6.1644
5. Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit Care Med. 2003;31(4):1250–1256. doi:10.1097/01.Ccm.0000050454.01978.3b
6. Knoop ST, Skrede S, Langeland N, Flaatten HK, Brakenridge S. Epidemiology and impact on all-cause mortality of sepsis in Norwegian hospitals: a national retrospective study. PLoS One. 2017;12(11):e0187990. doi:10.1371/journal.pone.0187990
7. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. doi:10.1097/01.Ccm.0000217961.75225.E9
8. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
9. Schorr C, Odden A, Evans L, et al. Implementation of a multicenter performance improvement program for early detection and treatment of severe sepsis in general medical-surgical wards. J Hosp Med. 2016;11(Suppl 1):S32–S39. doi:10.1002/jhm.2656
10. Kleinpell R. Promoting early identification of sepsis in hospitalized patients with nurse-led protocols. Crit Care. 2017;21(1):10. doi:10.1186/s13054-016-1590-0
11. Gyang E, Shieh L, Forsey L, Maggio P. A nurse-driven screening tool for the early identification of sepsis in an intermediate care unit setting. J Hosp Med. 2015;10(2):97–103. doi:10.1002/jhm.2291
12. Aitken LM, Williams G, Harvey M, et al. Nursing considerations to complement the surviving sepsis Campaign guidelines. Crit Care Med. 2011;39(7):1800–1818. doi:10.1097/CCM.0b013e31821867cc
13. Tromp M, Hulscher M, Bleeker-Rovers CP, et al. The role of nurses in the recognition and treatment of patients with sepsis in the emergency department: a prospective before-and-after intervention study. Int J Nurs Stud. 2010;47(12):1464–1473. doi:10.1016/j.ijnurstu.2010.04.007
14. Funk D, Sebat F, Kumar A. A systems approach to the early recognition and rapid administration of best practice therapy in sepsis and septic shock. Curr Opin Crit Care. 2009;15(4):301–307. doi:10.1097/MCC.0b013e32832e3825
15. Varpula M, Karlsson S, Parviainen I, Ruokonen E, Pettilä V. Community-acquired septic shock: early management and outcome in a nationwide study in Finland. Acta Anaesthesiol Scand. 2007;51(10):1320–1326. doi:10.1111/j.1399-6576.2007.01439.x
16. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi:10.1097/CCM.0b013e31827e83af
17. Levy MM, Rhodes A, Phillips GS, et al. Surviving sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Intensive Care Med. 2014;40(11):1623–1633. doi:10.1007/s00134-014-3496-0
18. Jones SL, Ashton CM, Kiehne L, et al. Reductions in sepsis mortality and costs after design and implementation of a nurse-based early recognition and response program. Jt Comm J Qual Patient Saf. 2015;41(11):483–491. doi:10.1016/s1553-7250(15)41063-3
19. Torsvik M, Gustad LT, Mehl A, et al. Early identification of sepsis in hospital inpatients by ward nurses increases 30-day survival. Crit Care. 2016;20(1):244. doi:10.1186/s13054-016-1423-1
20. Donohue LA, Endacott R. Track, trigger and teamwork: communication of deterioration in acute medical and surgical wards. Intensive Crit Care Nurs. 2010;26(1):10–17. doi:10.1016/j.iccn.2009.10.006
21. Martin JS, Ummenhofer W, Manser T, Spirig R. Interprofessional collaboration among nurses and physicians: making a difference in patient outcome. Swiss Med Wkly. 2010;140:w13062. doi:10.4414/smw.2010.13062
22. House S, Havens D. Nurses’ and physicians’ perceptions of nurse-physician collaboration: a systematic review. J Nurs Adm. 2017;47(3):165–171. doi:10.1097/nna.0000000000000460
23. Brier J, Carolyn M, Haverly M, et al. Knowing ‘something is not right’ is beyond intuition: development of a clinical algorithm to enhance surveillance and assist nurses to organise and communicate clinical findings. J Clin Nurs. 2015;24(5–6):832–843. doi:10.1111/jocn.12670
24. Wood C, Chaboyer W, Carr P. How do nurses use early warning scoring systems to detect and act on patient deterioration to ensure patient safety? A scoping review. Int J Nurs Stud. 2019;94:166–178. doi:10.1016/j.ijnurstu.2019.03.012
25. Smith DJ, Aitken LM. Use of a single parameter track and trigger chart and the perceived barriers and facilitators to escalation of a deteriorating ward patient: a mixed methods study. J Clin Nurs. 2016;25(1–2):175–185. doi:10.1111/jocn.13104
26. Rogan A, Lockett J, Peckler B, Robinson B, Raymond N. Exploring nursing and medical perceptions of sepsis management in a New Zealand emergency department: a qualitative study. Emerg Med Australas. 2022;34(3):417–427. doi:10.1111/1742-6723.13911
27. Kitto S, Marshall SD, McMillan SE, et al. Rapid response systems and collective (in)competence: an exploratory analysis of intraprofessional and interprofessional activation factors. J Interprof Care. 2015;29(4):340–346. doi:10.3109/13561820.2014.984021
28. Giorgi A. The phenomenological movement and research in the human sciences. Nurs Sci Q. 2005;18(1):75–82. doi:10.1177/0894318404272112
29. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40(8):795–805. doi:10.1177/1403494812465030
30. Antonacci G, Lennox L, Barlow J, Evans L, Reed J. Process mapping in healthcare: a systematic review. BMC Health Serv Res. 2021;21(1):342. doi:10.1186/s12913-021-06254-1
31. Royal College of Physicians. National Early Warning Score (NEWS) 2: standardising the assessment of acute-illness severity in the NHS. Updated report of a working party. London: RCP; 2017.
32. Askim Å, Moser F, Gustad LT, et al. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality - a prospective study of patients admitted with infection to the emergency department. Scand J Trauma Resusc Emerg Med. 2017;25(1):56. doi:10.1186/s13049-017-0399-4
33. Polit D, Beck C. Sampling in qualitative research. In: Nursing Research.
34. Malterud K. Shared understanding of the qualitative research process. Guidelines for the medical researcher. Fam Pract. 1993;10(2):201–206. doi:10.1093/fampra/10.2.201
35. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. doi:10.1016/s0140-6736(01)05627-6
36. Massey D, Aitken LM, Chaboyer W. What factors influence suboptimal ward care in the acutely ill ward patient? Intensive Crit Care Nurs. 2009;25(4):169–180. doi:10.1016/j.iccn.2009.03.005
37. Robson W, Beavis S, Spittle N. An audit of ward nurses’ knowledge of sepsis. Nurs Crit Care. 2007;12(2):86–92. doi:10.1111/j.1478-5153.2007.00210.x
38. Minton J, Clayton J, Sandoe J, Mc Gann H, Wilcox M. Improving early management of bloodstream infection: a quality improvement project. BMJ. 2008;336(7641):440–443. doi:10.1136/bmj.39454.634502.80
39. Turi SK, Von Ah D. Implementation of early goal-directed therapy for septic patients in the emergency department: a review of the literature. J Emerg Nurs. 2013;39(1):13–19. doi:10.1016/j.jen.2011.06.006
40. Murray E, Treweek S, Pope C, et al. Normalisation process theory: a framework for developing, evaluating and implementing complex interventions. BMC Med. 2010;8(1):63. doi:10.1186/1741-7015-8-63
41. McEvoy R, Ballini L, Maltoni S, O’Donnell CA, Mair FS, Macfarlane A. A qualitative systematic review of studies using the normalization process theory to research implementation processes. Implement Sci. 2014;9(1):2. doi:10.1186/1748-5908-9-2
42. May C, Sibley A, Hunt K. The nursing work of hospital-based clinical practice guideline implementation: an explanatory systematic review using normalisation process theory. Int J Nurs Stud. 2014;51(2):289–299. doi:10.1016/j.ijnurstu.2013.06.019
43. Daniels R, Nutbeam T, McNamara G, Galvin C. The sepsis six and the severe sepsis resuscitation bundle: a prospective observational cohort study. Emerg Med J. 2011;28(6):507–512. doi:10.1136/emj.2010.095067
44. Bleakley G, Cole M. Recognition and management of sepsis: the nurse’s role. Br J Nurs. 2020;29(21):1248–1251. doi:10.12968/bjon.2020.29.21.1248
45. Kangas C, Iverson L, Pierce D. Sepsis screening: combining early warning scores and SIRS criteria. Clin Nurs Res. 2021;30(1):42–49. doi:10.1177/1054773818823334
46. Karlsen EE, Rønsåsbjørg NA, Skrede S, Mosevoll KA. [Scoring systems for early detection of sepsis on the ward]. Skåringsverktøy for tidlig oppdagelse av sepsis på sengepost. Tidsskr Nor Laegeforen. 2023;143(2). Norwegian. doi:10.4045/tidsskr.21.0905
47. Plambech MZ, Lurie AI, Ipsen HL. Initial, successful implementation of sepsis guidelines in an emergency department. Dan Med J. 2012;59(12):1.
48. Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA. 2008;299(19):2294–2303. doi:10.1001/jama.299.19.2294
49. Steinmo SH, Michie S, Fuller C, Stanley S, Stapleton C, Stone SP. Bridging the gap between pragmatic intervention design and theory: using behavioural science tools to modify an existing quality improvement programme to implement “Sepsis Six”. Implement Sci. 2016;11:14. doi:10.1186/s13012-016-0376-8
50. World Health Organization. Improving the Quality of Health Services: Tools and Resources. Turning Recommendations into Practice. World Health Organization; 2018.
51. Odell M, Victor C, Oliver D. Nurses’ role in detecting deterioration in ward patients: systematic literature review. J Adv Nurs. 2009;65(10):1992–2006. doi:10.1111/j.1365-2648.2009.05109.x
52. Preece MH, Hill A, Horswill MS, Watson MO. Supporting the detection of patient deterioration: observation chart design affects the recognition of abnormal vital signs. Resuscitation. 2012;83(9):1111–1118. doi:10.1016/j.resuscitation.2012.02.009
53. Christofidis MJ, Hill A, Horswill MS, Watson MO. A human factors approach to observation chart design can trump health professionals’ prior chart experience. Resuscitation. 2013;84(5):657–665. doi:10.1016/j.resuscitation.2012.09.023
54. Lydon S, Byrne D, Offiah G, Gleeson L, O’Connor P. A mixed-methods investigation of health professionals’ perceptions of a physiological track and trigger system. BMJ Qual Saf. 2016;25(9):688–695. doi:10.1136/bmjqs-2015-004261
55. Ludikhuize J, de Jonge E, Goossens A. Measuring adherence among nurses one year after training in applying the modified early warning score and situation-background-assessment-recommendation instruments. Resuscitation. 2011;82(11):1428–1433. doi:10.1016/j.resuscitation.2011.05.026
56. Benner P. Expertise in Nursing Practice: Caring, Clinical Judgment and Ethics.
57. O’Neill SM, Clyne B, Bell M, et al. Why do healthcare professionals fail to escalate as per the early warning system (EWS) protocol? A qualitative evidence synthesis of the barriers and facilitators of escalation. BMC Emerg Med. 2021;21(1):15. doi:10.1186/s12873-021-00403-9
58. Muller-Juge V, Cullati S, Blondon KS, et al. Interprofessional collaboration between residents and nurses in general internal medicine: a qualitative study on behaviours enhancing teamwork quality. PLoS One. 2014;9(4):e96160. doi:10.1371/journal.pone.0096160
59. Douw G, Schoonhoven L, Holwerda T, et al. Nurses’ worry or concern and early recognition of deteriorating patients on general wards in acute care hospitals: a systematic review. Crit Care. 2015;19(1):230. doi:10.1186/s13054-015-0950-5
60. Cox H, James J, Hunt J. The experiences of trained nurses caring for critically ill patients within a general ward setting. Intensive Crit Care Nurs. 2006;22(5):283–293. doi:10.1016/j.iccn.2006.02.003
61. Williams DJ, Newman A, Jones C, Woodard B. Nurses’ perceptions of how rapid response teams affect the nurse, team, and system. J Nurs Care Qual. 2011;26(3):265–272. doi:10.1097/NCQ.0b013e318209f135
62. Welch J, Dean J, Hartin J. Using NEWS2: an essential component of reliable clinical assessment. Clin Med. 2022;22(6):509–513. doi:10.7861/clinmed.2022-0435
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.