Back to Journals » Journal of Pain Research » Volume 12
Nonpharmacological Interventions Addressing Pain, Sleep, and Quality of Life in Children and Adolescents with Primary Headache: A Systematic Review
Authors Klausen SH ![]() , Rønde G, Tornøe B
, Rønde G, Tornøe B ![]() , Bjerregaard L
, Bjerregaard L ![]()
Received 23 May 2019
Accepted for publication 12 September 2019
Published 23 December 2019 Volume 2019:12 Pages 3437—3459
DOI https://doi.org/10.2147/JPR.S216807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Susanne Hwiid Klausen,1 Gitte Rønde,1 Birte Tornøe,2 Lene Bjerregaard3
1Department of Pediatrics, Zealand University Hospital, Roskilde, Denmark; 2Department of Health Sciences, Lund University, Lund, Sweden; 3Open Patient Data Explorative Network (OPEN), University of Southern Denmark (SDU), Odense, Denmark
Correspondence: Susanne Hwiid Klausen
Department of Pediatrics, Zealand University Hospital, Køgevej 10, Roskilde 4000, Denmark
Tel +45 24416410
Email [email protected]
Purpose: Children and adolescents with primary headache are at risk of persistent somatic symptoms and reduced quality of life (Qol) due to pain and pain-related behaviors, such as avoiding school and activities. Sleep is essential to health, and children and adolescents with primary headaches have more sleep complaints than do healthy controls. A treatment approach that addresses multifactorial causes is likely important. Nonpharmacological interventions seem promising. However, knowledge about effective strategies is limited. The objective of this review is to assess the effect of nonpharmacological interventions in randomized controlled trials (RCTs) among children and adolescents with primary headache in order to identify useful strategies.
Patients and methods: Outcome measures are pain, sleep, Qol, and coping versus no intervention or control intervention. Medline, CINAHL, EMBASE, and PsycINFO were searched for eligible trials. ClinicalTrials.gov. was searched for ongoing trials. Initial searches yielded 2588 publications. After initial screening and subsequent full-text review and quality assessment, 13 RCTs reported in 15 articles were selected for review. All reviewers independently assessed study quality using the CONSORT criteria for nonpharmacological interventions.
Results: Cognitive behavioral therapy (CBT), including education on pain-related topics, sleep, coping, and stress management, is an effective strategy for reducing headache and pain within groups over time. Fifteen studies assessed pain, 3 studies assessed sleep, 6 studies assessed Qol, and 11 studies assessed coping.
Conclusion: Strategies identified as useful were parts of CBT interventions. However, it was not possible to identify a single effective intervention addressing pain, sleep, Qol, and coping in children and adolescents with headache, primarily because sleep was infrequently addressed. Various aspects of Qol and coping strategies were assessed, rendering comparison difficult. Strategies for future interventions should include descriptions of theory-driven CBT interventions, depending on clinical setting and based on local resources, to promote a solid evidence base for nonpharmacological interventions.
Keywords: tension-type headache, migraine, pain, sleep, quality of life, coping
Introduction
Despite advances in healthcare, pain from primary headache is one of the most frequently reported health problems globally among school-aged children and adolescents.1 The pathways leading to primary headache are complex and multifactorial.2 The prevalence of headache seems to increase with age. Before the age of 12 years, minor differences exist in the frequency of headache between genders, but girls report headache more frequently after puberty.3 Tension-type headache (TTH) and migraine are considered different disorders with separate pathomechanisms that often coexist in children.4 The prognosis appears better for boys; in one study, 23% were migraine-free before age 25 years.5 Long-term studies with 20–40 years of follow-up on headache are complex to conduct due to high drop-out rates.5,6 Yet existing studies conclude that 40–70% of children who suffer from primary headache in childhood also suffer from headache in adulthood.7 Remission to headache-free adulthood occurs in 20–25% of children and adolescents with TTH and 15% of those with migraine.8
Primary headache in children and adolescents is dominated by frequent or chronic TTH and/or migraine. They may co-occur in a single individual in varying relative importance over time, from predominant TTH to predominant migraine and vice versa.6,8 In chronic forms in which headache persists ≥15 days a month or consistently, pathophysiology is maintained by sensitization of the central nervous system in both TTH and migraine9–11 and further reinforced by lifestyle factors.
Sensitization of the nervous system is a pathomechanism from which it is very difficult to recover. Therefore, interdisciplinary educational interventions focus on health promotion and prevention to guide children and their families in paying attention to important lifestyle factors, such as sleep and coping.11
To reduce bias, accurate diagnosis is both possible with the International Classification of Headache Disorders (ICHD-I)-III12 and necessary before treatment and care. Headache as a pain condition can be treated by a team of interdisciplinary specialists, such as neuro-pediatricians, psychologists, physiotherapists, and specialist headache nurses.13 The team can facilitate thorough examinations, exercise planning, and education in pain mechanisms, coping strategies, and empowerment.14,15 Successful coping with stress contributes to positive headache remission,16 and cognitive behavioral therapy (CBT) and biofeedback seem to be effective.17 However, these nonpharmacological interventions are primarily available in specialists’ centers, restricting broad access. Many patients worry about the side effects of preventive medications. Complementary and alternative treatment strategies are needed.18 It is thus important to assess the effectiveness of nonpharmacological strategies accessible to patients.
Sleep is essential for health and quality of life.19 Youths with primary headaches have more sleep complaints than do healthy controls.20–25 However, a paucity of research explores the mediating and moderating effects of sleep on headache in children and adolescents.26 Overall, the literature suggests that the association between sleep and primary headache is bidirectional and that further studies are warranted.22,27 Because children with headache suffer from sleep impairment, it is important to investigate interventions addressing or assessing sleep in this population.28
Headache affects the quality of life (Qol) through impaired school, family, and emotional functioning.29,30 Headache is associated with lower academic performance.31 The family situation and daily routines play a major role in the child’s coping and, consequently, Qol.30,32 Reductions in Qol in children with headache were equivalent to or greater than other chronic or longer standing childhood illnesses, such as juvenile idiopathic arthritis and cancer.29 A child suffering from primary headache is at risk of long-term suffering in terms of lower Qol and reduced physical, social, and academic functioning.
Overall, the ability to cope influences pain, sleep, and Qol in children with headache. Lasting effects of coping in children with headache have been found after CBT, biofeedback, and relaxation therapies.33 Coping is concerned with efforts to manage adaptational demands and the emotions they generate.34 Coping has been described as a very broad concept, and no agreement exists about its conceptualization or measurement in children and adolescents.35 Coping is a highly relevant concept for interventions in children with headache.36,37 However, little is known about strategies, including effective and widely accessible interventions on pain, sleep, Qol, and coping in children and adolescents with primary headache. A systematic review is warranted.
Materials and Methods
The overall aims of this study are to systematically identify feasible and effective interventions for use in clinical practice and identify and evaluate the outcomes of nonpharmacological randomized interventions on 1) pain frequency, pain intensity, and pain duration; 2) sleep disturbances; 3) Qol; and 4) coping/activity limitations.
A systematic review of primary RCTs was conducted. The study was registered in the Prospero database, the international prospective register of systematic reviews (ID 104747).
Search Strategy and Study Selection
A detailed literature search of randomized trials was conducted in January 2017 and updated in August 2018. The search included Medical Subject Headings (MeSH) and subject terms or key words (Appendix 1). The full electronic search history is available in the Supplementary Material.
Reports published in 1990–2018 studying the effects of nonpharmacological interventions in children and young people with primary headache were identified in PubMed, CINAHL, PsycINFO, Cochrane, and SveMed Plus databases and supplemented by a snowball search technique. Reference lists were scrutinized, and unpublished literature was identified and retrieved by contacting authors of abstracts reported in conference proceedings and ClinicalTrials.gov searches. Reference lists of prior systematic reviews and other relevant papers were manually examined. The search was restricted to English language.
The following selection criteria were used for selection of the studies:
Studies
- Peer-reviewed original articles
- RCT published in full text
Participants
- Study populations comprised children and adolescents aged 7–18 years
- Participants were diagnosed with primary headache, tension-type headache (TTH) or migraine
Interventions
- Nonpharmacological interventions as standalone approaches or in combination with other treatments
Outcome measures
- Primary outcomes were headache and pain reduction; secondary outcomes were sleep, Qol, and coping.
Studies of mental illness, disability, and acute conditions, anxiety disorder, attention deficit hyperactivity disorder and other psychiatric diagnoses, pharmacology, melatonin and solely or primarily biofeedback were excluded, as were school-based studies (Appendix 2, PICO criteria).
The study selection process was guided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist.38 Search results were managed using COVIDENCE software, and duplicates were removed.39 Full text of relevant studies was retrieved and studies considered eligible for review were determined. Multiple reports from the same study were linked. A data extraction sheet was used in concordance with inclusion and exclusion criteria.
Quality Appraisal and Data Extraction
Validity, design characteristics, and research quality of included trials were evaluated by all authors according to the CONSORT checklist for nonpharmacological interventions,40,41 the extension suggested by Hoffmann42 and the International Classification of Headache Disorders (ICHD).12 For articles selected for full review, data were extracted on authors, title, purpose, study population, and sample size and outcome measures of pain, sleep, Qol, and coping. Interventions, results, and child/parent and health professionals’ satisfaction with an intervention were retrieved (Table 1). Finally, data on cost analysis, recruitment and retention, and other relevant information for health-care professionals were also retrieved.
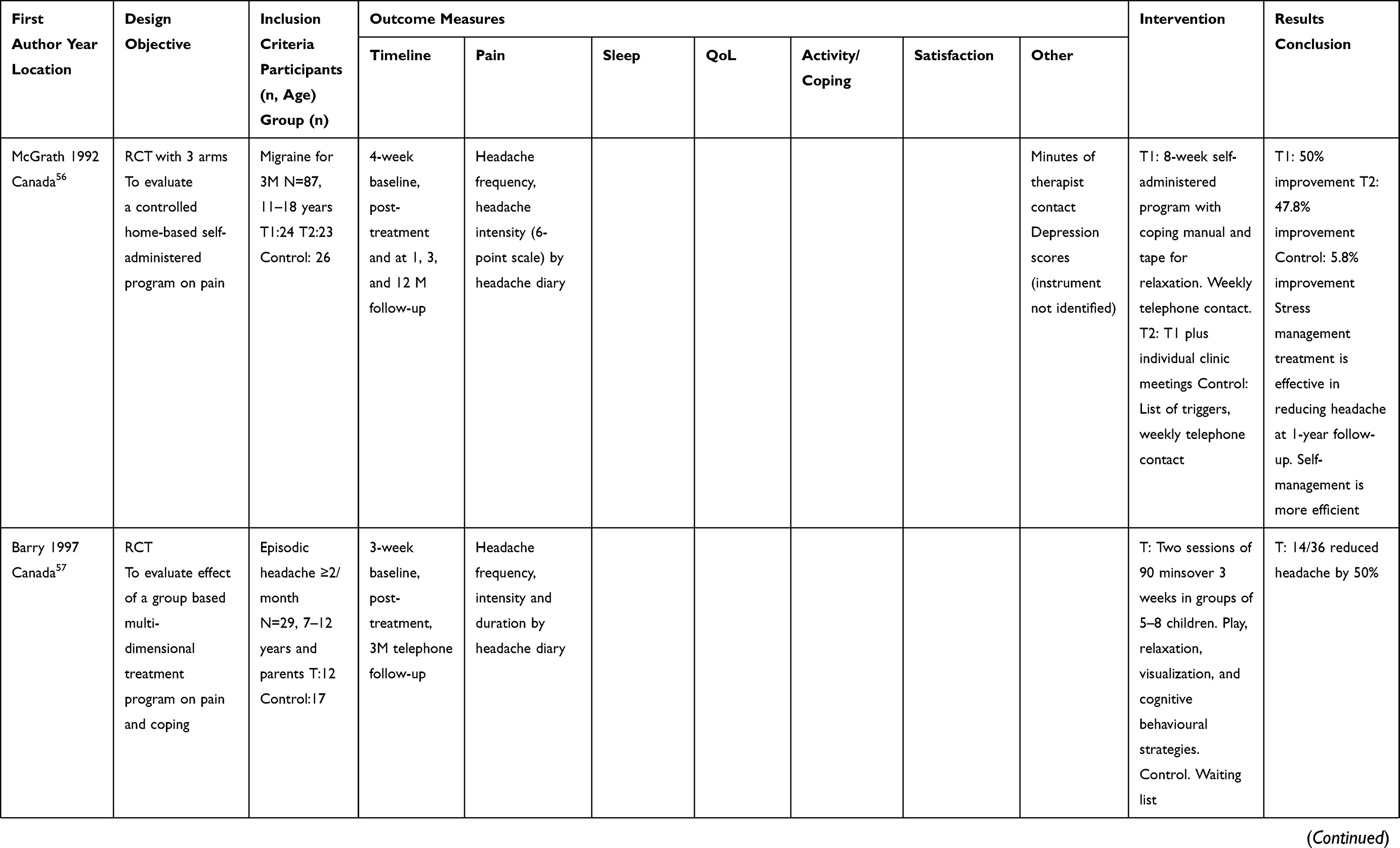 | 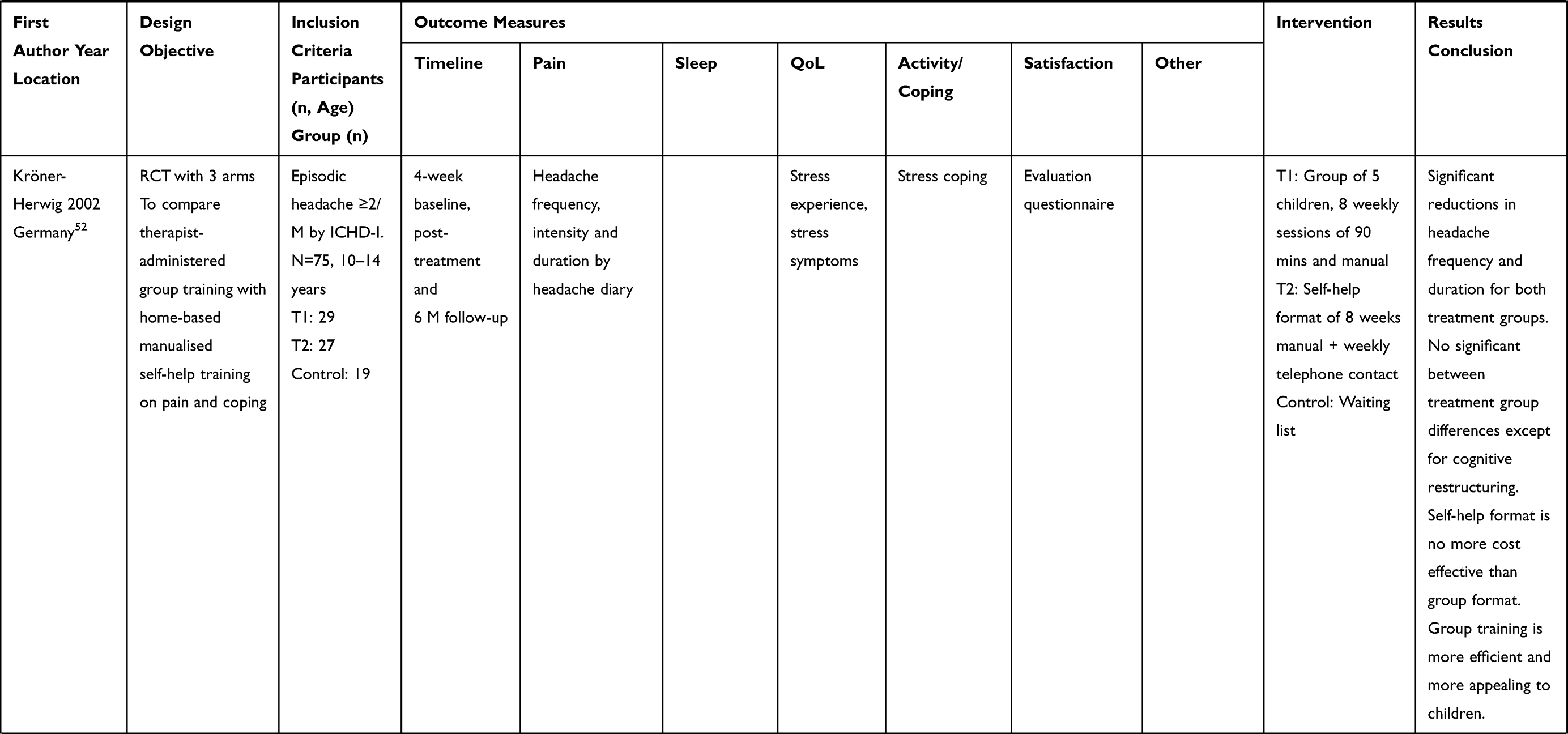 | 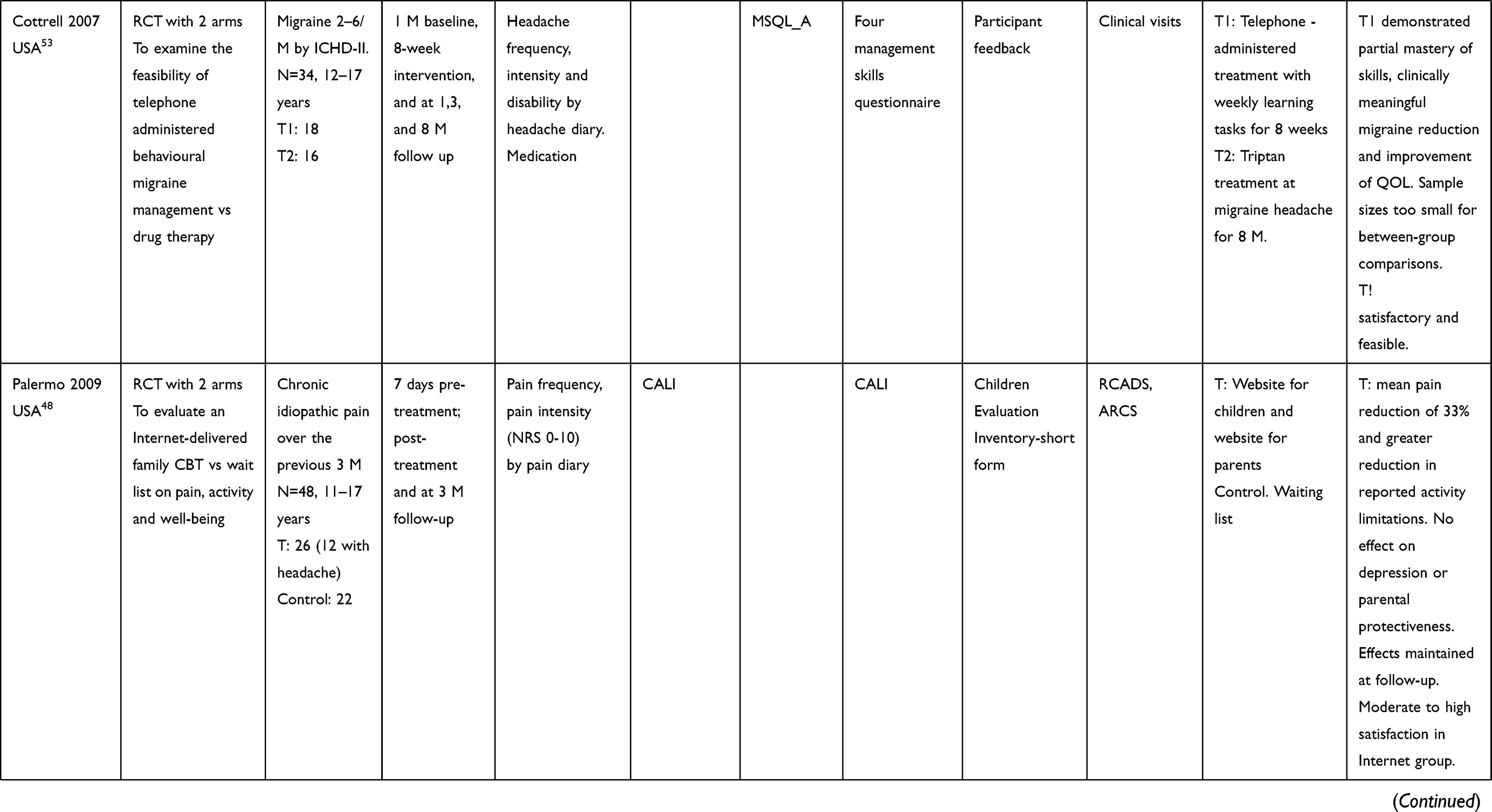 | 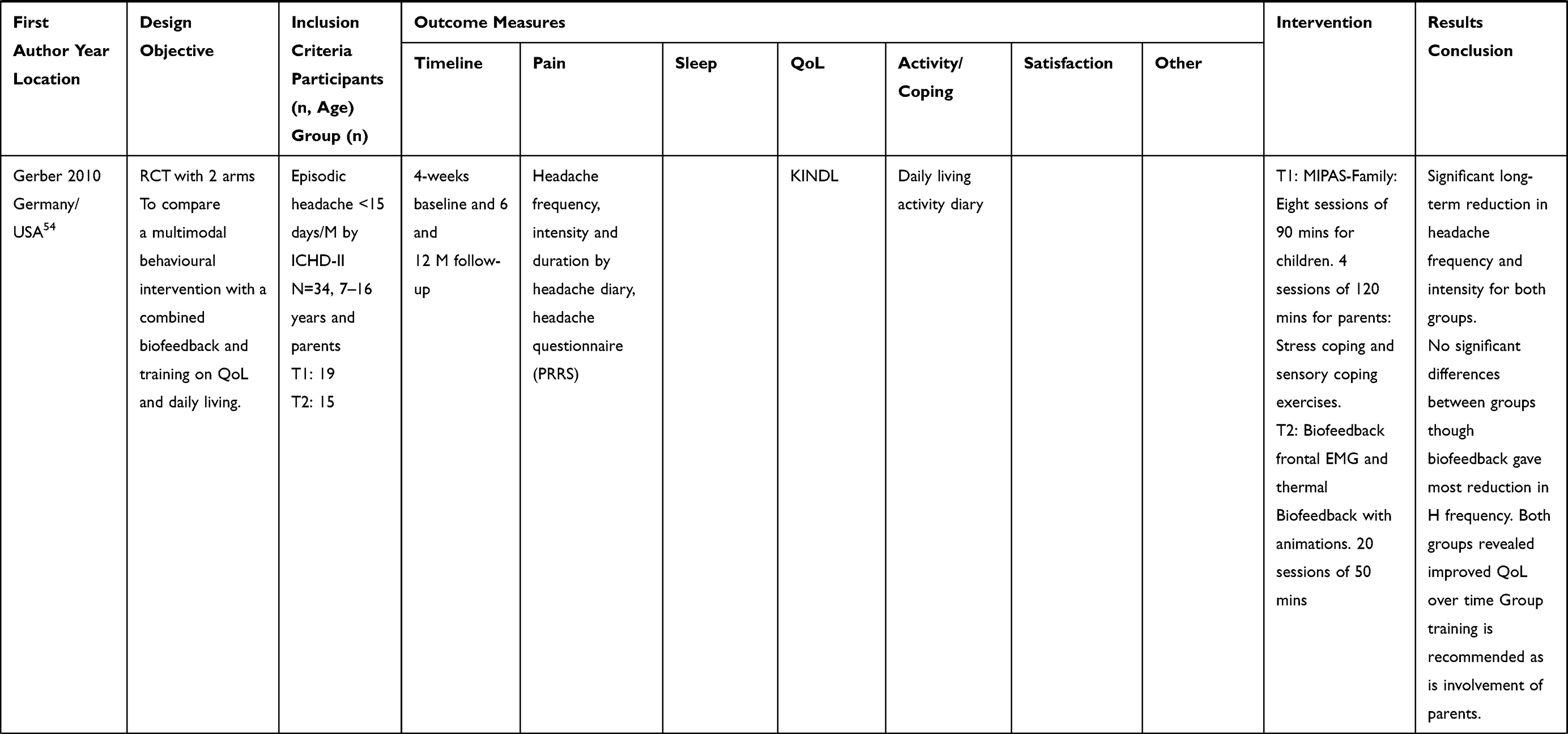 | 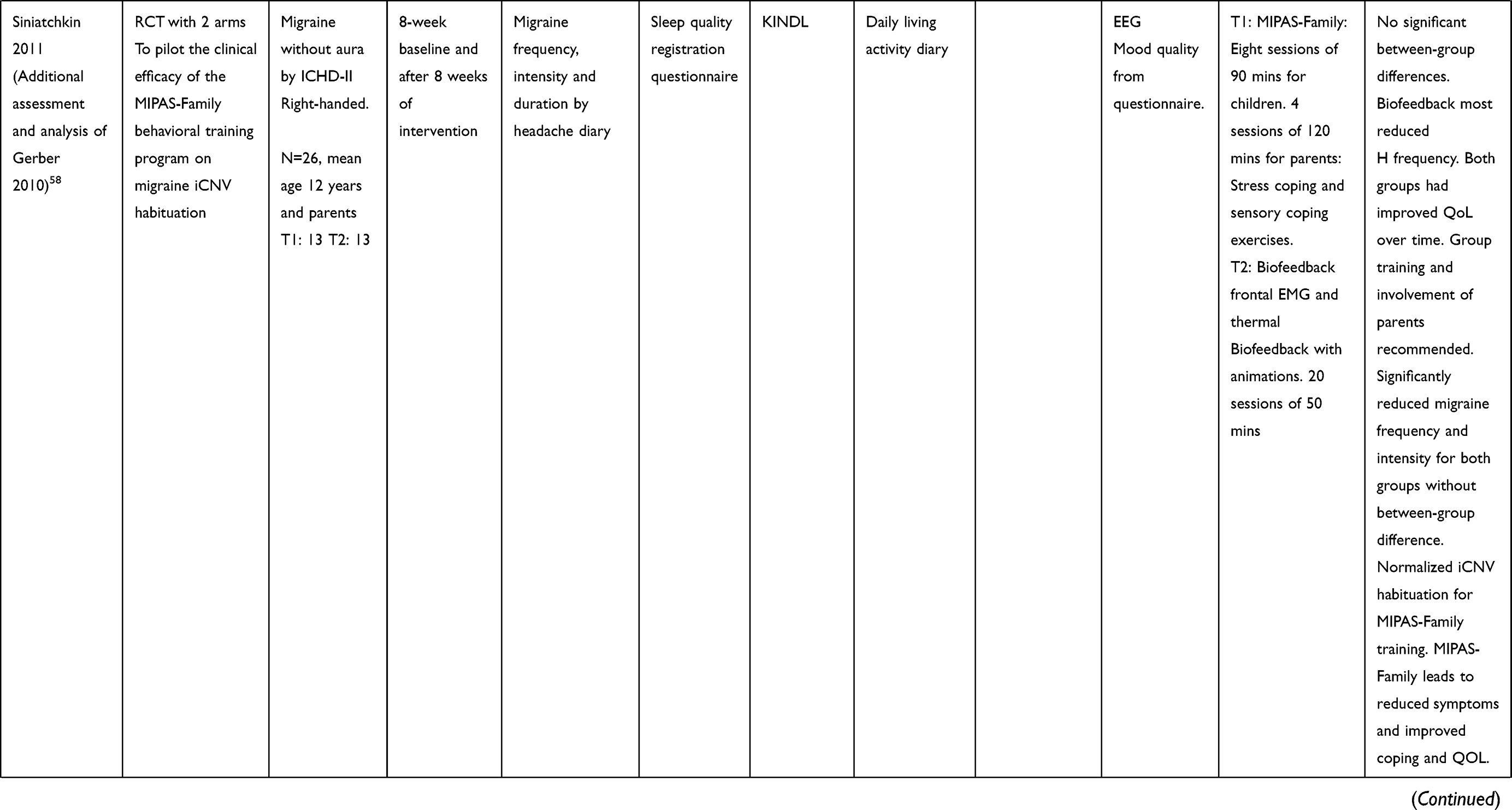 | 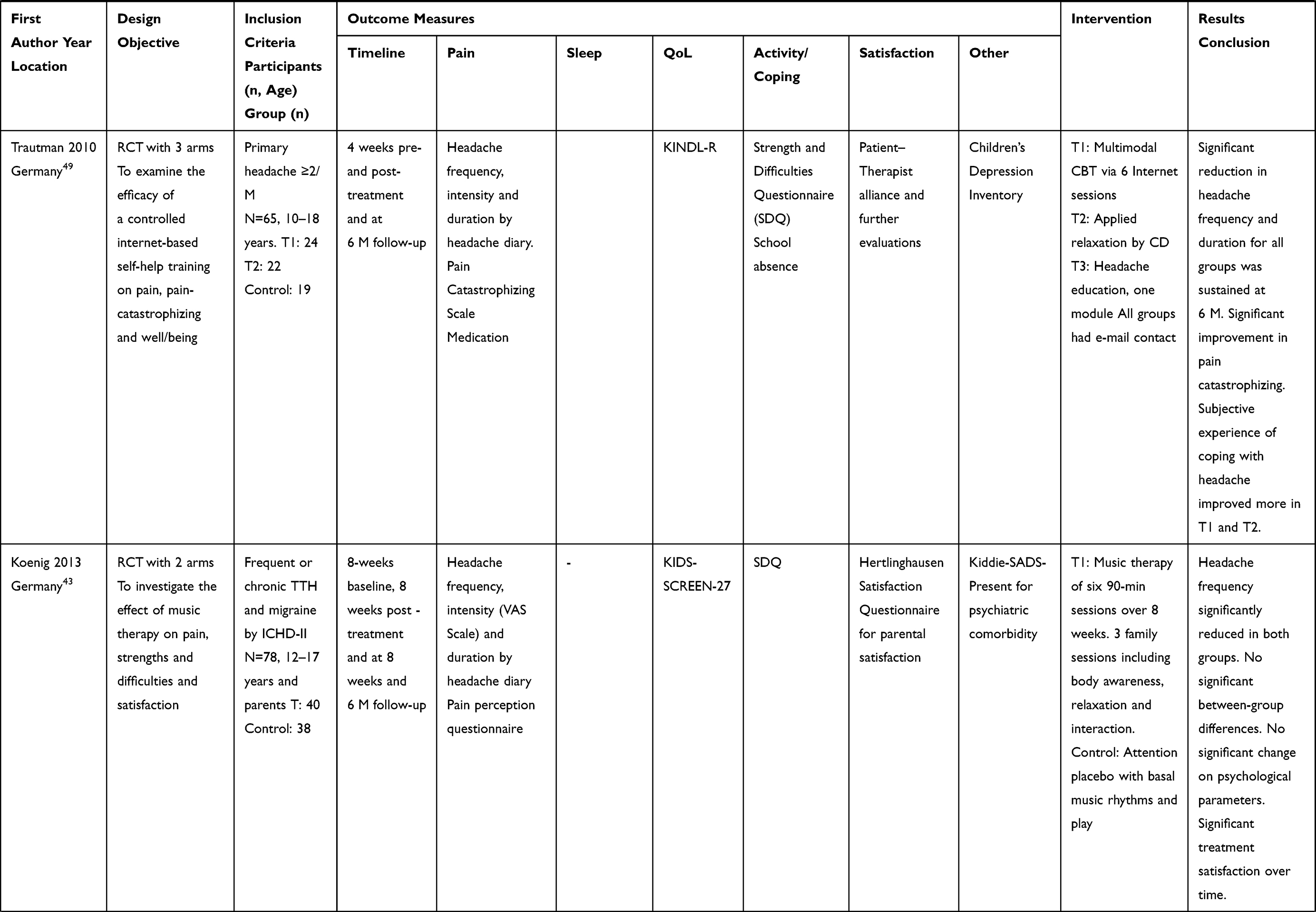 | 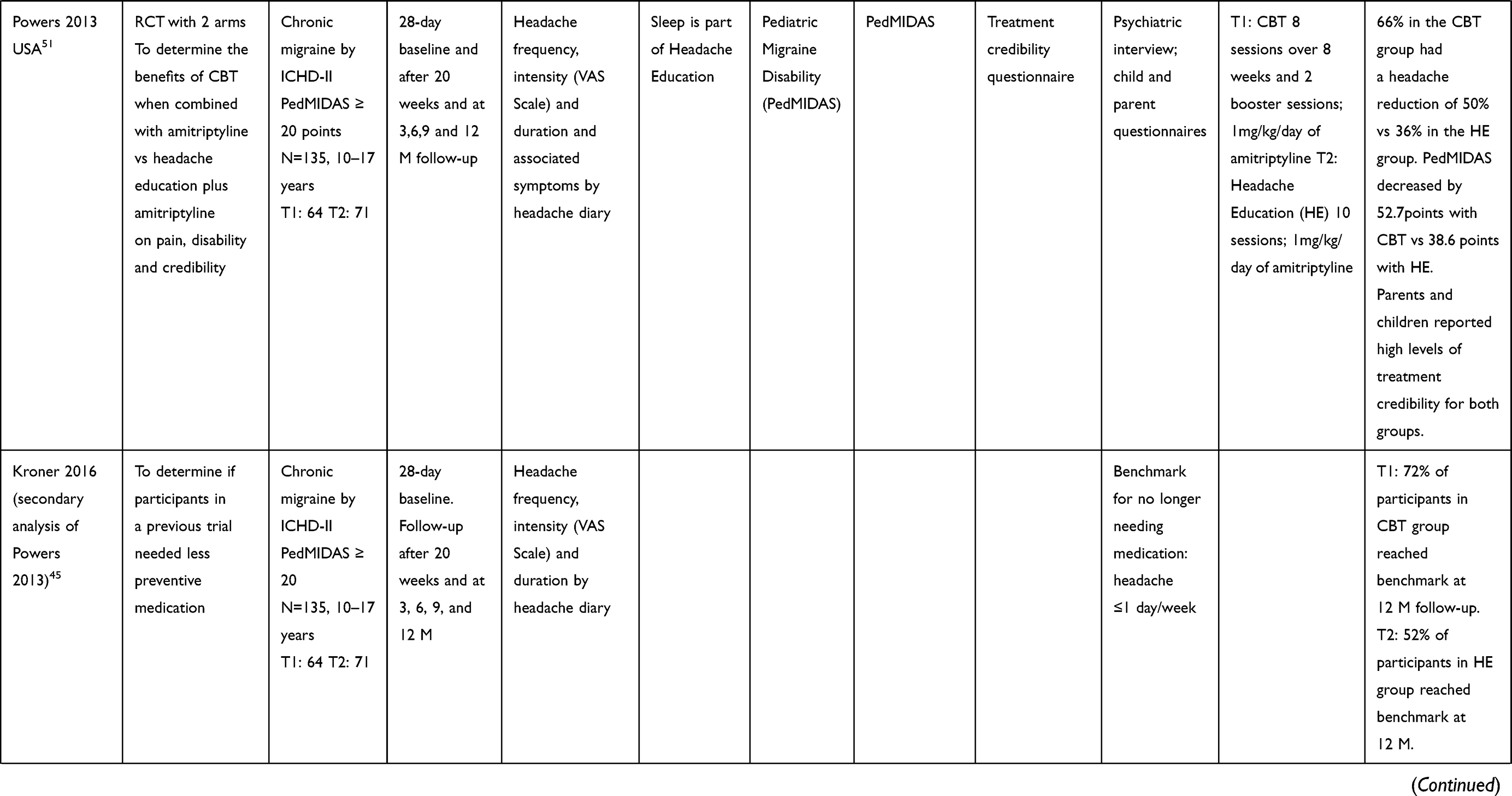 | 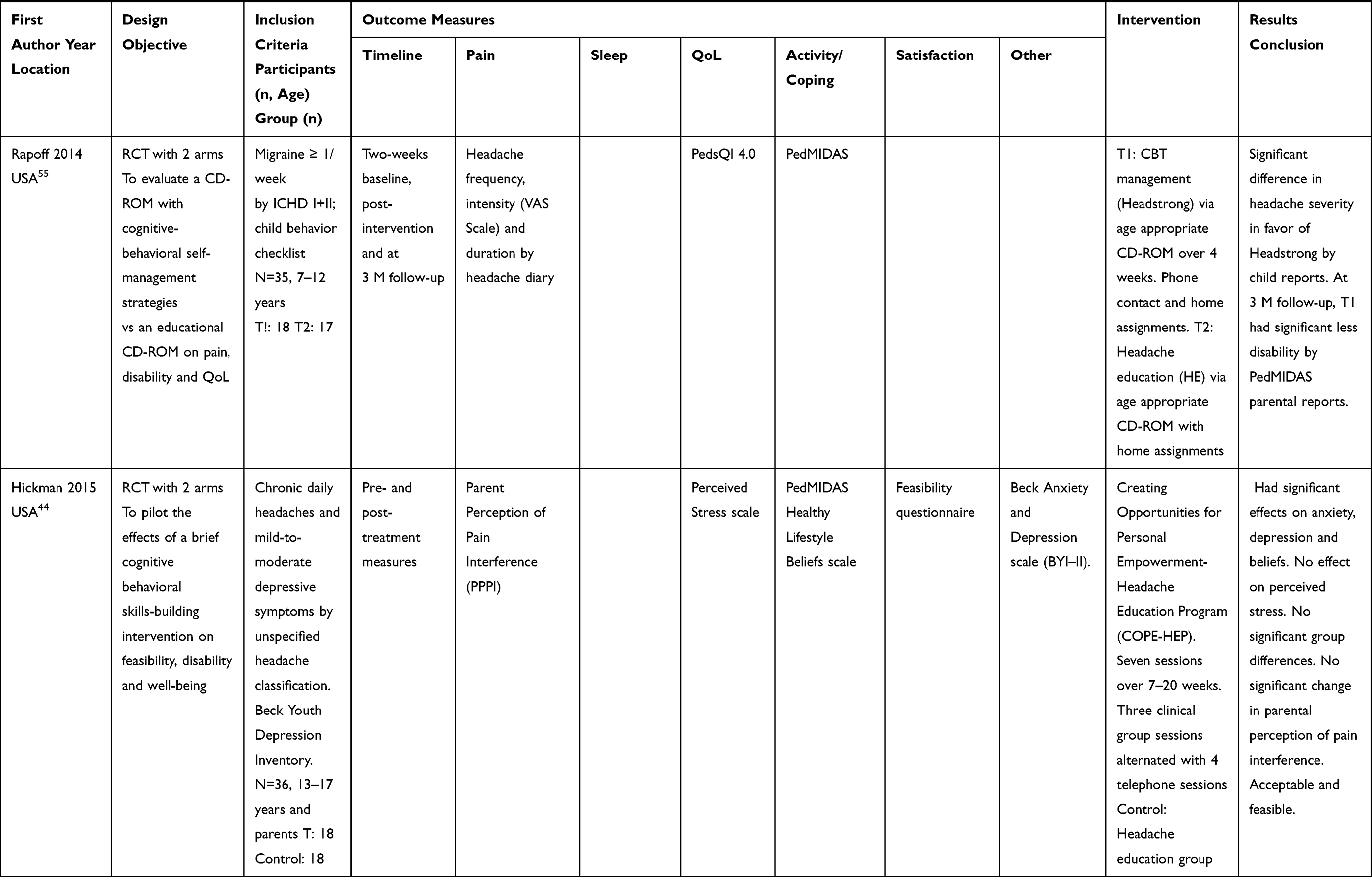 | 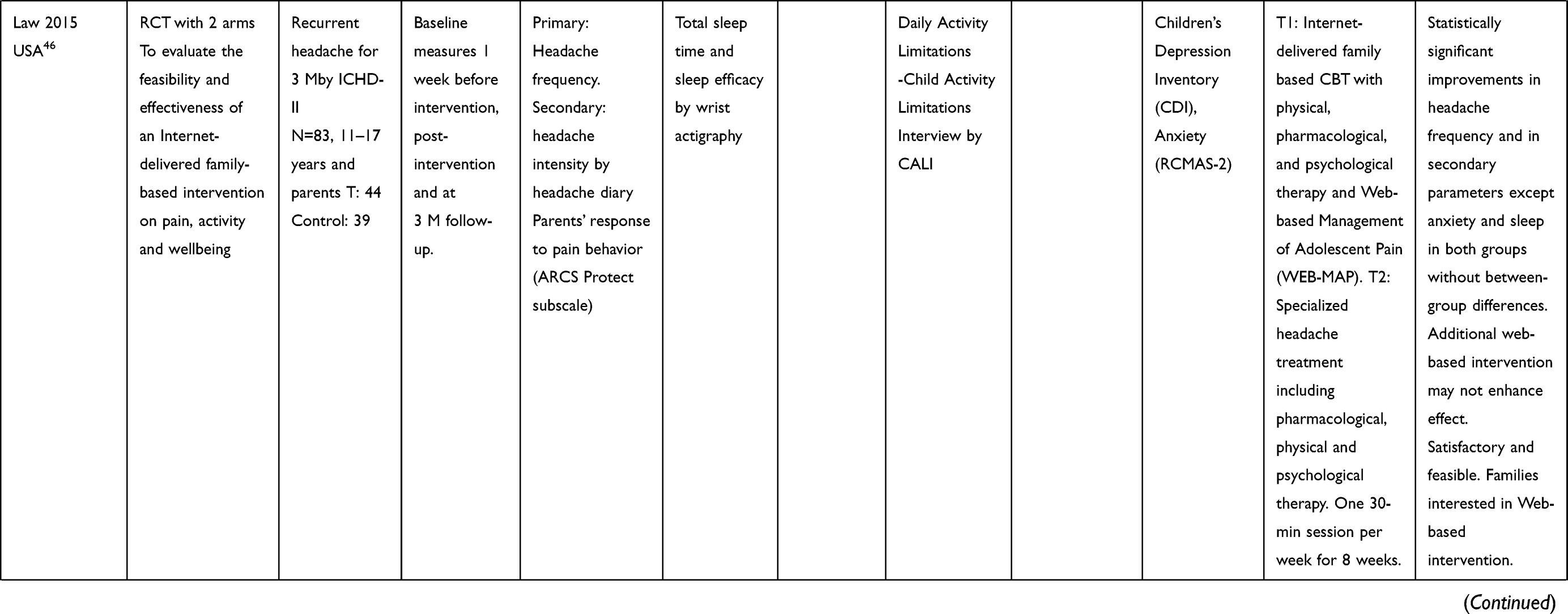 | 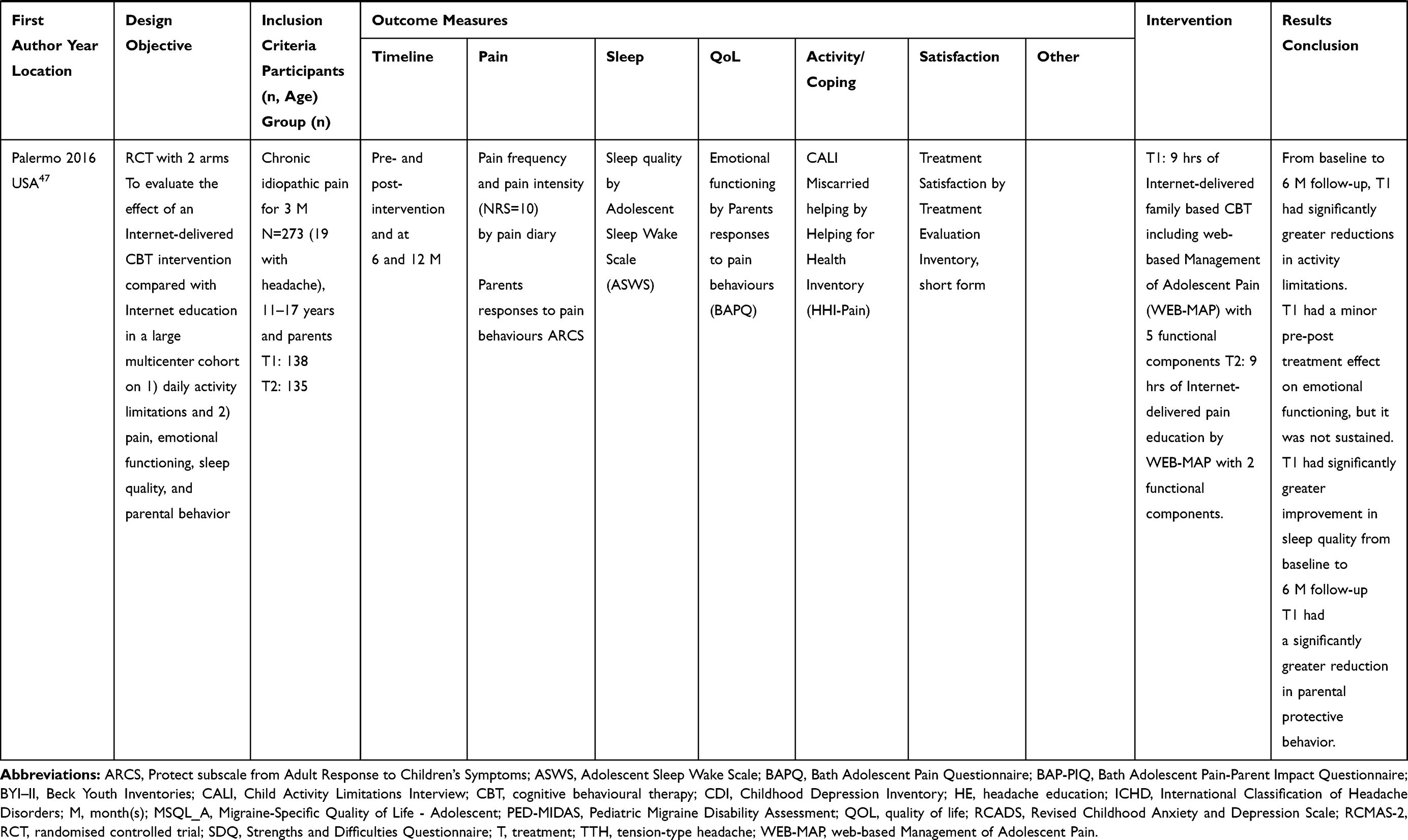 |
Table 1 Studies Included (N=13) |
Synthesis of Evidence
Three reviewers independently screened all titles and abstracts against inclusion and exclusion criteria. The three reviewers discussed disagreements and discrepancies, which were resolved by consensus and by a fourth reviewer. Evidence was synthesized by effect sizes and p values. We looked for complete descriptions of interventions that included setting, provider, procedure, and materials.
Results
A total of 2588 publications were identified. After removing duplicates and title and abstract screening, 247 full-text articles were assessed for eligibility. Thirteen RCTs reported in 15 articles were included (Figure 1).
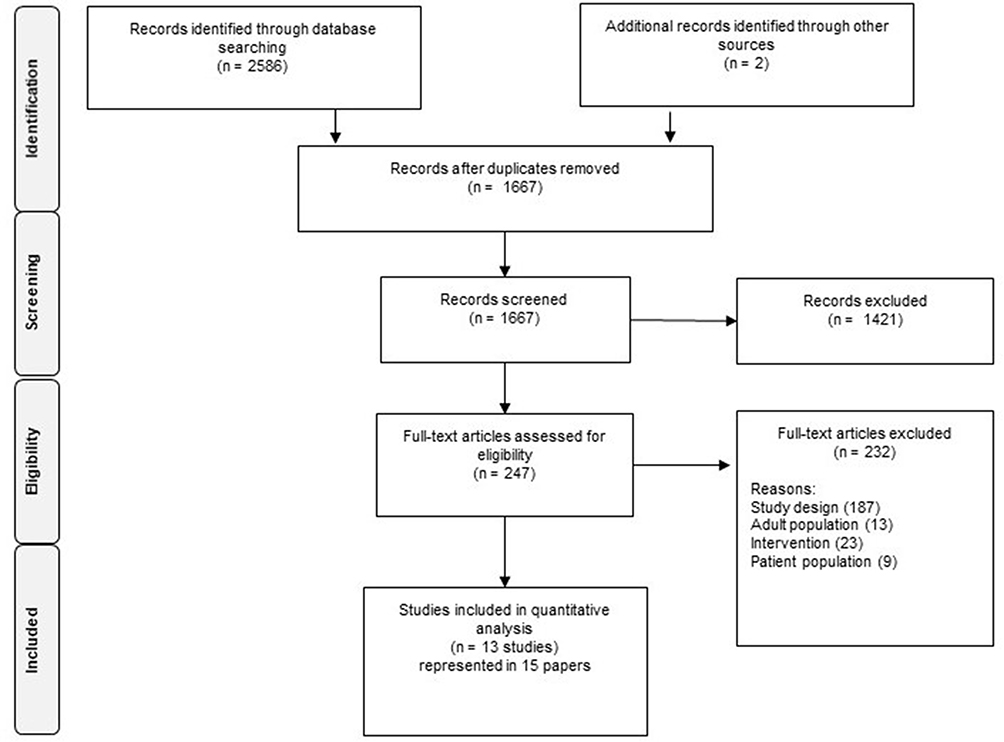 |
Figure 1 Flow chart of the search and selection process. |
Eight studies were conducted in the USA, two in Canada, and five in Germany (Table 1). Trials enrolled 26–135 participants aged 7–18 years. Eligibility was confirmed by ICHD-criteria I–II in seven studies and by neurologist assessment, parents, or unspecified in four studies.
Nine studies met the CONSORT criteria.40 No studies blinded researchers; one study blinded participants.43 Seven studies had low risk of bias related to randomization procedures.43–49 Findings were organized into the four outcomes of interest: pain, sleep, Qol, and coping. Figure 2 depicts assessment instruments used in included studies. Assessments were conducted 2–4 weeks before baseline and up to 12 months post intervention.
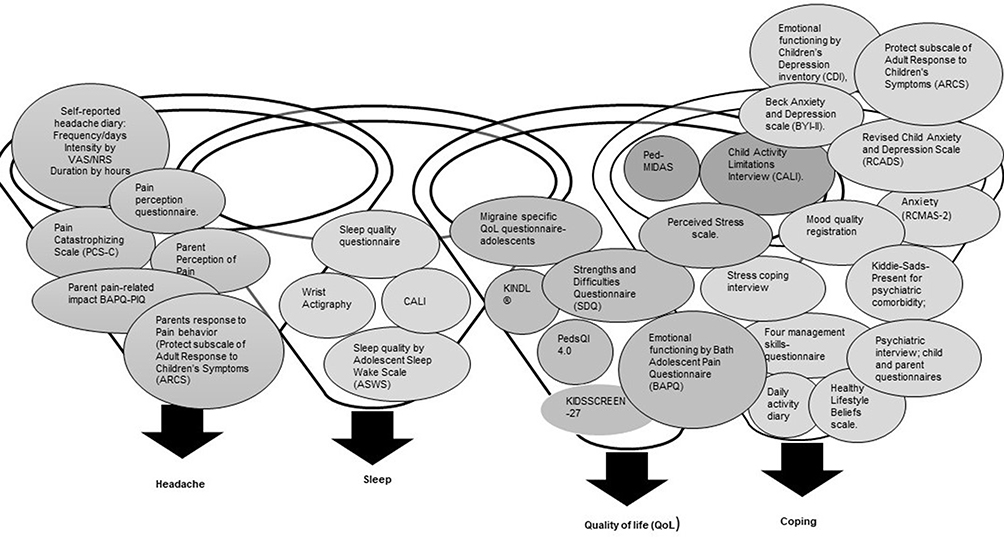 |
Figure 2 Identified assessment instruments. |
Strategies
Most treatment interventions were based on CBT and most control interventions were education. Table 2 identifies techniques contributing to effectiveness across interventions, inspired by Abraham and Michie’s taxonomy of behavior change techniques.50 Strategies to reduce pain were included in CBT, and educational interventions sought to influence children’s and parents’ perceptions of pain, as indicated by the assessments of outcomes on pain catastrophizing, pain perception, and parents’ response to pain behavior (Figure 2). Two studies described strategies aimed at improving sleep by education.46,51 Strategies directed at the ability to cope included education on coping with stress, images of self-concept,44,51,52 demonstration of relaxation skills,49,53 skills to reduce and manage stress48,54 and problem solving55 or were included in CBT.46,47 Figure 3 depicts effective components of CBT.
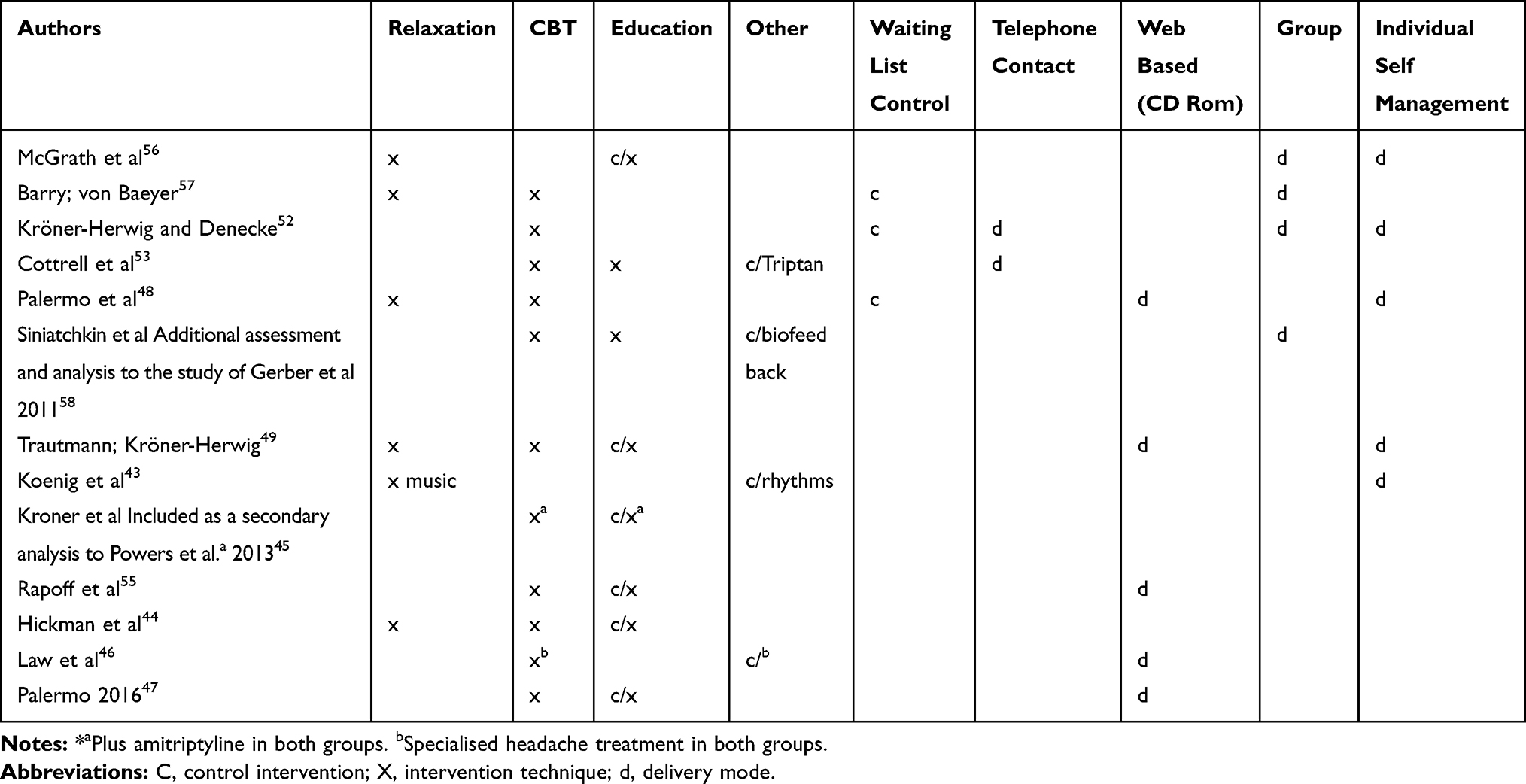 |
Table 2 Characteristics of Intervention Delivery Modes, Techniques, and Control Interventions |
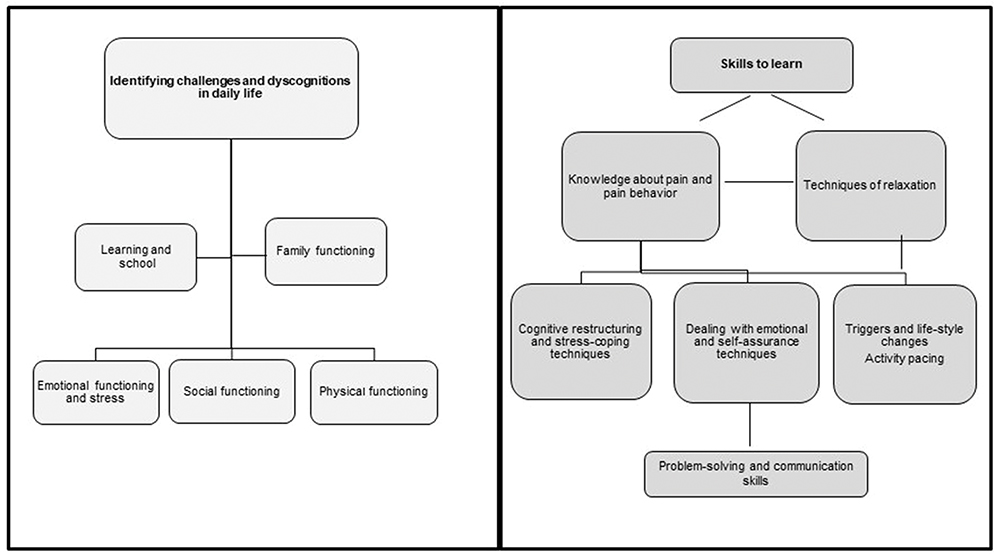 |
Figure 3 Components of effective cognitive behavioral theory. |
Pain Outcomes and Assessment Tools
Trautmann and Kröner-Herwig49 used data from a pain-catastrophizing scale, and the intervention was associated with significant reduction in pain catastrophizing. Koenig et al43 collected information from a pain perception questionnaire but found no significant change in psychological parameters. Hickmann et al44 found that parents’ perception of pain interference (PPPI) was unchanged. Law et al46 gathered information about parents’ responses to pain behavior and protectiveness (ARCS) and found statistically significant pre-post improvements in parent protective behaviors. Palermo et al47 also used the ARCS, as well as parents’ pain-related impact (BAPO-PIQ), and found a small-to-medium significant pre-post reduction in parent protective behavior (d=0.49). The authors also examined miscarried helping with the Helping for Health Inventory and found a small pre-post effect from CBT (d=−0.30).
Pain was assessed in 12 of 13 studies by daily self-reported headache or pain diaries to monitor headache frequency, intensity, and duration.43,45–49,51–58 Headache frequency was most frequently used as the primary self-reported outcome, as recommended by Andrasik et al and Penzien et al.59,60 McGrath et al56 used a 6-point Likert scale to assess headache intensity. Five studies measured intensity by a 0–10 visual analogue scale.43,49,51,54,55 Palermo et al used a 0–10 numeric rating scale to assess headache intensity.47,48
Ten studies reported statistically significant long-term within-group reductions in headache frequency and intensity or duration from interventions comprising CBT44,46,48,49,51–55,57,58 and, in one study, music therapy.43 None reported a statistically significant between-group difference.
Eight studies calculated effect sizes for primary outcomes, reported as Cohen’s d, mean effect size (ES) or ANCOVA (n): headache pre-post CBT, ES = 0.5;52 pre-post Internet treatment for migraines, d = 1.0;53 pre-post Internet treatment for activity limitations, n2 = 0.17;48 child report of headache frequency after a multi-modal behavioral training program (MIDAS), d = 0.88;54 headache frequency with CBT, ES = 0.24;49 headache severity post-Headstrong intervention, ES = 0.7;55 headache frequency pre-post Internet-delivered CBT, d = 0.40;46 and pre-post Internet-delivered CBT for activity limitations, d= −0.25.47 A single study49 calculated the number needed to treat (NNT) for  50% headache reduction; for the comparisons of CBT and education and of applied relaxation and education, respectively, it was 2.0 (95% confidence interval [CI], 1.3–4.7) and 5.2 (95% CI: 2.2- ∞), calculated by the Cook and Sackett method.61 Four studies reported results from intention-to-treat analyses (ITT).43,46,49,51 Five studies reported a preliminary power calculation.46–48,51,55
50% headache reduction; for the comparisons of CBT and education and of applied relaxation and education, respectively, it was 2.0 (95% confidence interval [CI], 1.3–4.7) and 5.2 (95% CI: 2.2- ∞), calculated by the Cook and Sackett method.61 Four studies reported results from intention-to-treat analyses (ITT).43,46,49,51 Five studies reported a preliminary power calculation.46–48,51,55
Medication
Cottrell et al53 used migraine medication as an active control group and found an effect size of d = 1.2 for migraines per month. Powers et al51 and Kroner et al45 used CBT plus amitriptyline as the primary intervention. Kroner et al45 collected data using a benchmark of headache ≤1 day/week indicating that preventive medication was no longer needed. In the CBT and headache education groups, respectively, 72% and 52% of participants reached the benchmark at 12 months of follow-up.
Sleep Outcomes and Assessment Tools
Two of the included studies examined the association between primary headache and sleep. Outcome measures were the Adolescent Sleep Wake Scale (ASWS) which assesses adolescents’ perception of sleep quality47 and actigraphy.46 A third study assessed sleep habits as part of the headache education received by the control group.51 Ten studies did not assess or evaluate sleep.
Quality of Life Outcomes and Assessment Tools
Qol was assessed in 10 studies by stress instruments,44,52 emotional functioning,47 a migraine-specific instrument,53 KINDL,54,58 KINDL-R,49 KidsScreen,43 PedMidas,51 or PedsQl.55 Qol was described in terms of decreasing stress symptoms by Kröner-Herwig and Denecke45 and Hickman et al44 and increased emotional functioning by Palermo et al.47
Coping Outcomes and Assessment Tools
Interventions demonstrating an effect on coping were found in 10 studies.44–46,49,51–55 Coping was assessed in six studies by validated instruments. Three studies used PedMIDAS62 to assess disability and school absence.44,51,55 Three studies46–48 assessed the activity of daily living with CALI, a pain-specific instrument.63 Three studies did not address coping.45,56,57 In five studies, assessments of coping (and functional status, comorbidities, anxiety, and depression) were undertaken with various instruments.43,49,52–54,58 (Figure 3)
Discussion
Thirteen RCTs included in this review, reported in 15 articles, examined the effect of nonpharmacological treatment of primary headache (migraine or TTH) on pain as a primary outcome and changes in sleep, Qol, and coping as secondary outcomes in children and adolescents aged 7–18 years. The studies used different approaches to perform CBT and various control groups.
Ten of 13 studies showed a significant within-group reduction in pain (headache frequency and intensity or duration) over time but no between-group differences that would indicate a general treatment effect. None of the included studies examined all outcomes of interest, i.e., pain, sleep disturbance, changes in Qol, and coping. Therefore, no specific strategy can be identified as superior; the choice of strategy will depend on the clinical setting and patient characteristics.
Sleep was infrequently evaluated. Two of 13 studies incorporated sleep education into CBT. One found a small but significant effect on sleep quality at follow-up;47 the other did not.46 In addition to pain reduction, better functional outcomes in daily life are vital for children and adolescents with primary headache. In the included studies, different aspects of Qol and coping strategies were measured; in some studies, the concepts of Qol and coping overlapped, rendering comparison difficult. Clearly defined outcome measures of Qol and coping are required to compare CBT intervention studies. Despite these limitations, nonpharmacological interventions seem to be well accepted, and feasible and effective components and strategies can be identified.
Participants
Baseline characteristics of participants reflected variation in age (7 to 18 years), headache type, and comorbidities (e.g., anxiety and depression), as well as illness severity. Three studies stratified participants to tailor age- and gender-relevant interventions.55–57 These and other stratifications seem appropriate in this population to generate and implement evidence-based treatments in clinical practice. As stratification will reduce the statistical power in studies with small sample sizes, multi-site studies may be a solution. In addition, the total number of participants in the included studies, which were published in 1992–2016, was 723, and dropout rates were substantial. Thus, larger multicentre studies are needed to generate valid conclusions.
Although nine of the included studies adhered to the CONSORT criteria, none fully adhered to the guidelines.40 A recent systematic review by Bouhklied et al on RCTs on chronic pain in children supports this finding.64 This is consistent with previous findings from studies with adults.65 Blinding of participants to a nonpharmacological intervention is challenging. However, blinding of outcome evaluators is possible. Following CONSORT recommendations, as well as other recommendations for pediatric headache research,59,60 can improve research validity and reliability. In addition, recommendations from The Pediatric Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (Ped-IMMPACT) stress that core outcome domains should be considered when designing pain clinical trials for acute and recurrent/chronic pain.66
Strategies and Successful Operational Components of Feasible and Effective Interventions
The results in this review indicate that CBT can reduce headache and pain symptoms significantly within groups and reduce parental protective behavior to some degree. However, when considering between-group differences and the scale of symptom reductions, the effects of treatments are less clear. No interventions described in depth the theoretical framework, even though CBT and music therapy are theory-based interventions. However, most studies described the intervention techniques.
Primary headaches are due to multifactorial somatic and psychosocial causes in different headache groups and can change over time. The effects of interventions can also dampen over time. The ideal intervention should encompass all causal elements of primary headache. This review highlights the fact that biopsychosocial interventions targeting children and adolescents with primary headache are complex.
The paradoxical finding of no between-group differences for any interventions in the included reports but significant within-group differences could be because both treatment and control interventions included useful strategies and modalities. To identify effective interventions, future studies should adhere to an identified theoretical framework and compare the intervention with another established treatment. Mindfulness-based stress reduction may be effective in the treatment of headache but was not tested in any of the included studies.67
Outcomes
Pain
Penzien et al60 stress the importance of  % improvement to exceed a possible placebo effect that might reach levels of
% improvement to exceed a possible placebo effect that might reach levels of  30%.68 In the review reported here, a consensus existed on using 50% as a standard. However, the placebo effect may play a larger role in future research, since what works for patients is most important. None of the studies report between-group differences. Appropriate statistical power is essential to reporting statistically significant findings and effect sizes.69 A preliminary power calculation was reported by only 5 of 13 included studies.46–48,51,55 Statistical power and a consensus on how to compute effect sizes in neuro-psychological studies are important. One study49 calculated NNT for the 50% standard, which could also be a good way to calculate effects.69
30%.68 In the review reported here, a consensus existed on using 50% as a standard. However, the placebo effect may play a larger role in future research, since what works for patients is most important. None of the studies report between-group differences. Appropriate statistical power is essential to reporting statistically significant findings and effect sizes.69 A preliminary power calculation was reported by only 5 of 13 included studies.46–48,51,55 Statistical power and a consensus on how to compute effect sizes in neuro-psychological studies are important. One study49 calculated NNT for the 50% standard, which could also be a good way to calculate effects.69
Sleep
The American Academy of Sleep Medicine recommends amounts of sleep per 24 hrs that children and adolescents should have on a regular basis to promote optimal health outcomes.19 Children aged 1–2 years should sleep 11–14 hrs, children aged 3–5 years should sleep 10–13 hrs, children aged 6–12 years should sleep 9–12 hrs, and adolescents aged 13–18 years should sleep 8–10 hrs.19 None of the included studies reported the amount of sleep study participants obtained, except for Law et al,46 who reported that participants aged 11–18 years of age in both treatment groups had insufficient sleep, averaging about 6 hrs per night. To investigate the impact of sleep on primary headache, a sleep evaluation must be performed before any intervention.
In this review, sleep was only addressed in 3 of 13 studies, evaluated by questionnaire in one study,47 and by actigraphy in another.46 Two of three recent studies included a sleep intervention as part of the CBT program. One study among a mixed chronic pain group in which just 7% of participants had headache alone found slightly better sleep quality in the CBT group, compared to participants receiving an educational strategy.47 In another study evaluating sleep by actigraphy among patients with primary headache, no between-group changes in sleep quality were found.46 In fact, participants spent a substantial amount of time awake in bed at night, as assessed by pre-treatment actigraphy. Screen time was not evaluated in these studies. None of the studies reported associations between primary headache and sleep.
Primary headaches (migraine and TTH) have been associated with sleep disturbance in observational studies. The association is bidirectional, with primary headaches influencing sleep and disturbed sleep influencing primary headaches.70,71 Sleep disturbances have been reported in as many as 65–73% of pediatric patients with chronic headache.23,72
A recent retrospective clinical study assessing the prevalence and occurrence of possible migraine trigger factors in children and adolescents with migraine showed that stress was the most frequently reported trigger factor (75.5%), followed by lack of sleep (69.6%).73 The same influence of headache triggers (poor sleep and emotional distress) was shown in a non-clinical population of children and adolescents by Bruni et al.74
Few studies have investigated the relationship between sleep and headache using a longitudinal design. Elements of primary headache may cause or aggravate a disturbed sleep schedule, and disturbed sleep may interfere with resolution of or trigger a primary headache. Bruni et al75 randomly assigned migraineurs aged 5–14 years to two groups: one received sleep hygiene recommendations and the other did not. After 6 months of follow-up, the sleep hygiene group reported lower mean headache duration than did the control group, suggesting that better sleep quality led to altered migraine patterns. Although this study did not directly measure the effects of sleep disturbance on migraines, it supports the direction of the relationship (i.e., sleep disturbance can negatively influence migraine).
Heyer et al76 performed a longitudinal prospective study of 52 children aged 10–18 years with episodic migraine; some participants also had TTH. The authors compared the frequency and headache characteristics of headache days with sleep disturbance to headache days without sleep disturbance. Outcomes were measured with an Internet-based, 90-day headache diary, self-rated headache intensity and Ped-MIDAS score, and reports of sleep disturbances directly related to proximate headaches. Twenty-one percent of participants reported headaches, and 13.9% reported sleep disruptions directly related to a proximate headache. The higher the Ped-MIDAS scores, the more days with sleep disturbances related to headache. The maximum proportion of headache days that impacted sleep was 32%. Headache intensity (P = 0.009) and timing of headache onset (P < 0.001) predicted sleep disturbances.
Many studies investigating the relationship between primary headaches and sleep disturbances have applied either Internet-based headache diaries76 or questionnaires assessing sleep difficulties or trigger factors.20–25,72–74 Few have applied objective measurements such as actigraphy for monitoring sleep patterns.27,77 This is an important area for future study. Regular insufficient sleep is associated with attention, behaviour and learning problems,9 which may aggravate primary headache and influence Qol and coping strategies.
Qol
Health-related Qol is a multidimensional concept that reflects the impact of disease and treatment on the patient’s subjective evaluation of functioning and well-being.29 Studies included in this review used a variety of approaches to capture the impact of an intervention on family functioning and daily life for children and adolescents suffering from headache. Most reported significant headache reduction regardless of group allocation, suggesting that increased attention on the child suffering from headache can positively impact the child and family.52
Parents were included in five studies.43,44,47,54,58 The underlying assumption was that the efficacy of the therapeutic intervention would increase by integrating parents into treatment programs.43,44 Incorporating family daily activities into treatment programs would facilitate parents becoming trainers, helping children to use learned techniques at home between program sessions.47,54 No reported result supported this assumption. However, Sinitchkin et al58 found improved transfer of learned strategies into daily life in the MIPAS-Family group, improving the child’s ability to cope with stressful situations, adjust to aversive stimuli, and even prevent migraine attacks. Gerber et al54 found that parents were increasingly motivated to participate in training as training proceeded, but they also lacked relevant knowledge about the child’s headache. This lack of knowledge may lead to underestimating the child’s complaint or parental behavior that exacerbates the chronicity of the child’s condition, emphasizing the value of including parents in the treatment of children or adolescents.54
Organization of the interventions may also determine effectiveness. Kröner-Herwig and Denecke52 argue that therapist-conducted training is preferable to a self-help format because it is more efficient and appealing to children. However, they also report dropouts due to scheduling difficulties, indicating that the logistics of bringing children to appointments at the hospital is a barrier that may lead to noncompliance. Similarly, Palermo et al47 found that parents were better integrated in a web-based treatment program because interventions in a clinical setting were time-consuming and harder to integrate into daily family routines.
In terms of the feasibility of training migraine management skills in a group setting for adolescents, Cottrell et al53 demonstrated that a telephone-administered behavior treatment was associated with clinically significant improvements in migraine that did not reach statistical significance due to small study size and the lack of a control group. The potential value of low-intensity treatment modalities provided by telephone or web may be enhanced by their low cost and adaptability to the daily lives of adolescents and families.
Coping
Coping can be characterized as engagement or disengagement coping.78 The authors define engagement coping as “aimed at dealing with the stressors or the resulting distress emotions” and disengagement coping as “aimed at escaping from dealing with the stressors or the resulting distress emotions”.78 In this review, all effective interventions included components of engagement coping strategies, such as cognitive restructuring and stress coping, emotional and self-reassurance techniques, or problem-solving or communicative strategies (Figure 3). This finding indicates that numerous components of effective interventions promote coping. Therefore, the accessibility of local resources could guide the choice of engagement coping strategies in future interventions to treat headache in children.17
Headache in childhood can be viewed as a biopsychosocial condition because sleep and other stressors can contribute to it.79 A biopsychosocial perspective adheres to the idea that pain is a result of interactions between nociceptive, sociocultural, behavioral, and cognitive factors.80 All these domains should be incorporated when identifying relevant outcomes, rather than relying on pain as the primary outcome. Studies included in this review showed substantial variation in outcomes. In two studies, activity limitations,47,48 as assessed by CALI,81 were the primary outcome, rather than the impact of pain from headache. Validation of CALI found that children with headache had more limitations on routine activities, such as going to school, reading, schoolwork, watching TV, and eating regular meals, than did children with abdominal pain, back pain, musculoskeletal pain, or other pain diagnoses. This finding makes CALI useful for targeting interventions and measuring outcomes in future interventions in children with headache.
Parental Involvement
Five studies gathered additional information about phenomena associated with pain, such as pain catastrophizing, pain perception and interference, and parental pain behavior. Three studies included proxy assessments by parents: PPPI, parents’ response to pain behavior (ARCS protect subscale) or parents’ response to pain.44,46,47 Children and, to a lesser extent, adolescents generally depend on their parents for daily assessments of symptoms and treatment. Parents’ personal pain histories could confound a child’s pain outcome; cross-sectional studies find that headache in childhood can be associated with parents’ pain history.82 This argues for the inclusion of parents in future interventions.
Satisfaction and Feasibility
Patient perspectives on experience of and satisfaction with interventions were sought in several studies,43,46,48,49,51,53 indicating the importance of patient acceptability. Nonadherence to pediatric interventions has a negative impact on implementation of evidence-based interventions because studies with small sample sizes lack power. A recent review of theoretical frameworks in pediatric adherence-promoting interventions found that there is a need for theory-driven studies in pediatrics.83
Other
Three studies were web-based interventions46–48 and applied gamification techniques.84 Web-based interventions have the potential to reach many more children and adolescents, overcoming problems related to attrition. However, they may quickly become outdated. In addition, increased screen time may influence headache mediated by less sleep. In a cross-sectional study of 1004 Italian students aged 10–16 years, Cerutti et al found that “results highlighted the potential impact of excessive Internet and mobile use, which ranges from different types of headache to other somatic symptoms”.85 Further studies are needed to confirm these findings and to assess the need for promoting preventive health interventions, especially in school settings. Sleep was not assessed in this study. Screen time was not assessed in any study.
Primary headache is multifactorial. It not possible to identify a single feasible and effective intervention addressing pain, sleep, Qol, and coping in children and adolescents with headache, primarily because sleep is insufficiently addressed. We identified risk of bias in more than a third of the studies due to lack of specified randomization procedures, blinding, ITT analyses, power calculations and effect sizes, or adequate description. Varying aspects of Qol and different coping strategies were assessed, making an overall comparison difficult. However, effective components and strategies were identified. CBT, including education on pain-related topics, sleep, coping, and stress management, is effective at reducing headache and pain within groups over time.
Future interventions should elaborate on detailed descriptions of theory-driven cognitive-based therapies to promote a solid evidence base for nonpharmacological interventions. Sleep examination and perspective of patients and families were identified as important components in future evaluations of primary headache interventions.
This review was conducted according to PRISMA guidelines and the protocol was published. Three independent reviewers validated the inclusion and exclusion process. Limitations include the exclusion criteria and restriction to English language-only studies.
Conclusion
Useful strategies that improve pain, sleep, Qol, and coping in children and adolescents with primary headache have been identified. None of the studies incorporated examination of all aspects of pain, sleep disturbance, changes in Qol, and coping. Therefore, no specific strategy can be identified as superior; the choice of intervention will depend on clinical setting and patient characteristics. In clinical practice, interventions should be based on local resources. Developing and testing new types of interventions should include the perspectives of patients and their families. Future research should adhere to rigorous methods and meaningful standardized patient outcomes.
Acknowledgments
This study was supported by a grant from Rosalie Petersens Fond. The authors thanks Rasmus Sand Bach, (Biomedical Research Librarian, University College South) and Susie Rimborg (Research Librarian Susie Rimborg, Royal Danish Library).
Disclosure
Dr Gitte Rønde reports grants from The Rosalie Petersens Foundation, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Currie C, Zanotti C, Morgan A, et al, editors. Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Health Policy for Children and Adolescents, No. 6. Copenhagen: WHO Regional Office for Europe; 2012.
2. Hershey AD. Current approaches to the diagnosis and management of paediatric migraine. Lancet Neurol. 2010;9(2):190–204. doi:10.1016/S1474-4422(09)70303-5
3. Abu-Arafeh I, Razak S, Sivaraman B, Graham C. Prevalence of headache and migraine in children and adolescents: a systematic review of population-based studies. Dev Med Child Neurol. 2010;52(12):1088–1097. doi:10.1111/j.1469-8749.2010.03793.x
4. Genizi J, Matar A, Schertz M, Zelnik N, Srugo I. Pediatric mixed headache. The relationship between migraine, tension-type headache and learning disabilities in a clinic-based sample. J Headache Pain. 2016;17:42. doi:10.1186/s10194-016-0625-x
5. Bille A. A 40-year follow-up of school children with migraine. Cephalagia. 1997;17(4):488–491. doi:10.1046/j.1468-2982.1997.1704488.x
6. Dooley JM, Augustine HF, Brna PM, Digby AM. The prognosis of pediatric headaches—A 30-year follow-up study. Pediatr Neurol. 2014;51:85–87. doi:10.1016/j.pediatrneurol.2014.02.022
7. Antonaci F, Voiticovschi-Iosob C, Di Stefano AL, Galli F, Ozge A, Balottin U. The evolution of headache from childhood to adulthood: a review of the literature. J Headache Pain. 2014;15(1):15. doi:10.1186/1129-2377-15-15
8. Gassmann J, Morris L, Heinrich M, Kroners-Herwig B. One-year course of paediatric headache in children and adolescents aged 8–15 years. Cephalalgia. 2008;28:1154–1162. doi:10.1111/j.1468-2982.2008.01657.x
9. de Tommaso M, Sciruicchio V, Delussi M, et al. Symptoms of central sensitization and comorbidity for juvenile fibromyalgia in childhood migraine: an observational study in a tertiary headache center. J Headache Pain. 2017;18(1):59. doi:10.1186/s10194-017-0764-8
10. Soee A-BL, Thomsen LL, Kreiner S, Tornoe B, Skov L. Altered pain perception in children with chronic tension-type headache: is this a sign of central sensitisation? Cephalalgia. 2013;33(7):454–462. doi:10.1177/0333102413476371
11. Tornøe B. Children and adolescents with primary tension-type headaches: research and practice perspectives for non-pharmacological interdisciplinary headache service. Current Perspectives on Less-Known Aspects of Headache. 2017. [Internet]. Available from https://www.intechopen.com/books/current-perspectives-on-less-known-aspects-of-headache. Available from.
12. Arnold M. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
13. Gaul C, van Doorn C, Webering N, et al. Clinical outcome of a headache-specific multidisciplinary treatment program and adherence to treatment recommendations in a tertiary headache center: an observational study. J Headache Pain. 2011;12(4):475–483. doi:10.1007/s10194-011-0348-y
14. Gaul C, Visscher CM, Bhola R, et al. Team players against headache: multidisciplinary treatment of primary headaches and medication overuse headache. J Headache Pain. 2011;12(5):511–519. doi:10.1007/s10194-011-0364-y
15. Soee A-BL, Skov L, Skovgaard LT, Thomsen LL. Headache in children: effectiveness of multidisciplinary treatment in a tertiary paediatric headache clinic. Cephalalgia. 2013;33(15):1218–1228. doi:10.1177/0333102413490349
16. Carasco M, Kröner-Herwig B. Psychological predictors of headache remission in children and adolescents. Adolesc Health Med Ther. 2016;7:59–66. doi:10.2147/AHMT.S97925
17. Faedda N, Cerutti R, Verdecchia P, Migliorini D, Arruda M, Guidetti V. Behavioral management of headache in children and adolescents. J Headache Pain. 2016;17(1):80. doi:10.1186/s10194-016-0671-4
18. Minen MT, Anglin C, Boubour A, Squires A, Herrmann L. Meta-synthesis on migraine management. Headache. 2018;58(1):22–44. doi:10.1111/head.13212
19. Paruthi S, Brooks LJ, D’Ambrosio C, et al. Consensus statement of the American Academy of Sleep Medicine on the recommended amount of sleep for healthy children: methodology and discussion. J Clin Sleep Med. 2016;12(11):1549–1561. doi:10.5664/jcsm.6288
20. Bruni O, Fabrizi P, Ottaviano S, Cortesi F, Giannotti F, Guidetti V. Prevalence of sleep disorders in childhood and adolescence with headache: a case-control study. Cephalalgia. 1997;17(4):492–498. doi:10.1046/j.1468-2982.1997.1704492.x
21. Miller VA, Palermo TM, Powers SW, Scher MS, Hershey AD. Migraine headaches and sleep disturbances in children. Headache. 2003;43(4):362–368. doi:10.1046/j.1526-4610.2003.03071.x
22. Heng K, Wirrell E. Sleep disturbances in children with migraine. J Child Neurol. 2006;21(9):761–766. doi:10.1177/08830738060210092201
23. Gilman DK, Palermo TM, Kabbouche MA, Hershey AD, Powers SW. Primary headache and sleep disturbances in adolescents. Headache. 2007;47(8):1189–1194. doi:10.1111/j.1526-4610.2007.00885.x
24. Isik U, Ersu RH, Ay P, et al. Prevalence of headache and its association with sleep disorders in children. Pediatr Neurol. 2007;36(3):146–151. doi:10.1016/j.pediatrneurol.2006.11.006
25. Pakalnis A, Splaingard M, Splaingard D, Kring D, Colvin A. Serotonin effects on sleep and emotional disorders in adolescent migraine. Headache. 2009;49(10):1486–1492. doi:10.1111/j.1526-4610.2009.01392.x
26. Fallone G, Owens JA, Deane J. Sleepiness in children and adolescents: clinical implications. Sleep Med Rev. 2002;6(4):287–306. doi:10.1053/smrv.2001.0192
27. Bursztein C, Steinberg T, Sadeh A. Sleep, sleepiness, and behaviour problems in children with headache. J Child Neurol. 2006;21:12. doi:10.1177/7010.2006.00239
28. Valrie CR, Bromberg MH, Palermo T, Schanberg LE. A systematic review of sleep in pediatric pain populations. J Dev Behav Pediatr. 2013;34(2):120–128. doi:10.1097/DBP.0b013e31827d5848
29. Powers SW, Patton SR, Hommel KA, Hershey AD. Quality of life in childhood migraines: clinical impact and comparison to other chronic illnesses. Pediatrics. 2003;112(1):e1–5. doi:10.1177/7010.2006.00239
30. Bruijn J, Arts WF, Duivenvoorden H, Dijkstra N, Raat H, Passchier J. Quality of life in children with primary headache in a general hospital. Cephalalgia. 2009;29(6):624–630. doi:10.1111/j.1468-2982.2008.01774.x
31. Rocha‐Filho PA, Santos PV. Headaches, quality of life, and academic performance in schoolchildren and adolescents. Headache. 2014;54(7):1194–1202. doi:10.1111/head.1239432
32. Frare M, Axia G, Battistella PA. Quality of life, coping strategies, and family routines in children with headache. Headache. 2002;42(10):953–962. doi:10.1046/j.1526-4610.2002.02224.x
33. Evidence-Based Child Health, Editorial Office. Clinical Answers: are nonpharmacological interventions for migraine effective in children and adolescents? Evid-Based Child Health. 2013;8(3):754–758. doi:10.1002/ebch.1918
34. Lazarus RS. Emotions and interpersonal relationships: toward a person-centered conceptualization of emotions and coping. J Pers. 2006;74(1):9–46. doi:10.1111/j.1467-6494.2005.00368.x
35. Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, Wadsworth ME. Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychol Bull. 2001;127(1):87–127. doi:10.1037/0033-2909.127.1.87
36. Landry BW, Fischer PR, Driscoll SW, et al. Managing chronic pain in children and adolescents: a clinical review. PM&R. 2015;7(11 Suppl):S295–315. doi:10.1016/j.pmrj.2015.09.006
37. Manworren RC, Stinson J. Pediatric pain measurement, assessment, and evaluation. Semin Pediatr Neurol. 2016;23(3):189–200. doi:10.1016/j.spen.2016
38. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–1012. doi:10.1016/j.jclinepi.2009.06.005
39. Covidence. Better systematic review management [Internet]. 2016. Available from: https://www.covidence.org/home.
40. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010;63(8):834–840. doi:10.1016/j.jclinepi.2010.03.004
41. Boutron I, Altman DG, Moher D, Schulz KF, Ravaud P, for the CONSORT NPT Group. CONSORT statement for randomized trials of nonpharmacologic treatments: a 2017 update and a CONSORT extension for nonpharmacologic trial abstracts. Ann Intern Med. 2017;167(1):40. doi:10.7326/M17-0046
42. Hoffman T, Glasziou P, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687. doi:10.1136/bmj.g1687
43. Koenig J, Oelkers-Ax R, Kaess M, et al. Specific music therapy techniques in the treatment of primary headache disorders in adolescents: a randomized attention-placebo-controlled trial. J Pain. 2013;14(10):1196–1207. doi:10.1016/j.jpain.2013.05.006
44. Hickman C, Jacobson D, Melnyk BM. Randomized controlled trial of the acceptability, feasibility, and preliminary effects of a cognitive behavioral skills building intervention in adolescents with chronic daily headaches: a pilot study. J Pediatr Health Care. 2015;29(1):5–16. doi:10.1016/j.pedhc.2014.05.001
45. Kroner JW, Hershey AD, Kashikar-Zuck SM, et al. Cognitive behavioral therapy plus amitriptyline for children and adolescents with chronic migraine reduces headache days to ≤4 per month. Headache. 2016;56(4):711–716. doi:10.1111/head.12795
46. Law EF, Beals-Erickson SE, Noel M, Claar R, Palermo TM. Pilot randomized controlled trial of internet-delivered cognitive-behavioral treatment for pediatric headache. Headache. 2015;55(10):1410–1425. doi:10.1111/head.12635
47. Palermo TM, Law EF, Bromberg M, Fales J, Eccleston C, Wilson AC. Problem solving skills training for parents of children with chronic pain: a pilot randomized controlled trial. Pain. 2016;157(6):1213–1223. doi:10.1097/j.pain.0000000000000508
48. Palermo TM, Wilson AC, Peters M, Lewandowski A, Somhegyi H. Randomized controlled trial of an internet-delivered family cognitive-behavioral therapy intervention for children and adolescents with chronic pain. Pain. 2009;146(1):205–213. doi:10.1016/j.pain.2009.07.034
49. Trautmann E, Kröner-Herwig B. A randomized controlled trial of internet-based self-help training for recurrent headache in childhood and adolescence. Behav Res Ther. 2010;48(1):28–37. doi:10.1016/j.brat.2009.09.004
50. Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27(3):379–387. doi:10.1037/0278-6133.27.3.379
51. Powers SW, Kashikar-Zuck SM, Allen JR, et al. Cognitive behavioral therapy plus amitriptyline for chronic migraine in children and adolescents: a randomized clinical trial. JAMA. 2013;310(24):2622. doi:10.1001/jama.2013.282533
52. Kröner-Herwig B, Denecke H. Cognitive–behavioral therapy of pediatric headache: are there differences in efficacy between a therapist-administered group training and a self-help format? J Psychosom Res. 2002;53(6):1107–1114. doi:10.1016/S0022-3999(02)00345-8
53. Cottrell C, Drew J, Gibson J, Holroyd K, O’Donnell F. Feasibility assessment of telephone-administered behavioral treatment for adolescent migraine. Headache. 2007;47(9):1293–1302. doi:10.1111/j.1526-4610.2007.00804.x
54. Gerber WD, Petermann F, Müller GG, et al. MIPAS-family—evaluation of a new multi-modal behavioral training program for pediatric headaches: clinical effects and the impact on quality of life. J Headache Pain. 2010;11(3):215–225. doi:10.1007/s10194-010-0192-5
55. Rapoff M, Conelly M, Bickel JL, et al. Headstrong intervention for pediatric migraine headache: a randomized clinical trial. J Headache Pain. 2014;15:12. doi:10.1186/1129-2377-15-12
56. McGrath PJ, Humphreys P, Keene D, et al. The efficacy and efficiency of a self-administered treatment for adolescent migraine. Pain. 1992;49(3):321–324. doi:10.1016/0304-3959(92)90238-7
57. Barry J, von Baeyer C. Brief cognitive-behavioral group treatment for children’s headache. Clin J Pain. 1997;13(3):215–220. doi:10.1097/00002508-199709000-00006
58. Siniatchkin M, Müller GG, Darabaneanu S, Petermann F, Stephani U, Gerber WD. Behavioural treatment programme contributes to normalization of contingent negative variation in children with migraine. Cephalalgia. 2011;31(5):562–572. doi:10.1177/0333102410388434
59. Andrasik F, Powers SW, McGrath PJ. Methodological considerations in research with special populations: children and adolescents. Headache. 2005;45(5):520–525. doi:10.1111/j.1526-4610.2005.05104.x
60. Penzien DB, Andrasik F, Freidenberg BM, et al. Guidelines for trials of behavioral treatments for recurrent headache, 1st edition. Headache. 2005;45:S110–S132. doi:10.1111/j.1526-4610.2005.4502004.x
61. Cook R, Sackett D. The number needed to treat - a clinically useful measure of treatment effect. BMJ. 1995;310(6977):452–454. doi:10.1136/bmj.310.6977.452
62. Hershey AD, Powers SW, Vockell AL, LeCates S, Kabbouche MA, Maynard MK. PedMIDAS development of a questionnaire to assess disability of migraines in children. Neurology. 2001;57(11):2034–2039. doi:10.1212/wnl.57.11.2034
63. Palermo TM, Witherspoon D, Valenzuela D, Drotar DD. CALI - child activity limitations interview [Internet]. 2008. Available from: https://eprovide.mapi-trust.org/instruments/child-activity-limitations-interview.
64. Boulkedid R, Abdou AY, Desselas E, et al. The research gap in chronic paediatric pain: a systematic review of randomised controlled trials. Eur J Pain. 2018;22(2):261–271. doi:10.1002/ejp.1137
65. Turner L, Shamseer L, Altman DG, Schulz KF, Moher D. Does use of the CONSORT statement impact the completeness of reporting of randomised controlled trials published in medical journals? A cochrane review. Syst Rev. 2012;1(1):60. doi:10.1186/2046-4053-1-60
66. McGrath PJ, Walco GA, Turk DC, et al. Core outcome domains and measures for pediatric acute and chronic/recurrent pain clinical trials: pedIMMPACT recommendations. J Pain. 2008;9(9):771–783. doi:10.1016/j.jpain.2008.04.007
67. Cathcart S, Galatis N, Immink M, Proeve M, Petkov J. Brief mindfulness-based therapy for chronic tension-type headache: a randomized controlled pilot study. Behav Cogn Psychother. 2014;42(1):1–15. doi:10.1017/S1352465813000234
68. Autret A, Valade D, Debiais S. Placebo and other psychological interactions in headache treatment. J Headache Pain. 2012;13(3):191–198. doi:10.1007/s10194-012-0422-0
69. Houle TT, Penzien DB, Houle CK. Statistical power and sample size estimation for headache research: an overview and power calculation tools. Headache. 2005;45(5):414–418. doi:10.1111/j.1526-4610.2005.05092.x
70. Rains JC, Davis RE, Smitherman TA. Tension-type headache and sleep. Curr Neurol Neurosci Rep. 2014;15(2):520. doi:10.1007/s11910-014-0520-2
71. Guidetti V, Dosi C, Bruni O. The relationship between sleep and headache in children: implications for treatment. Cephalalgia. 2014;34(10):767–776. doi:10.1177/0333102414541817
72. Zarowski M, Młodzikowska-Albrecht J, Steinborn B. The sleep habits and sleep disorders in children with headache. Adv Med Sci. 2007;52(Suppl 1):194–196.
73. Neut D, Fily A, Cuvellier JC, Vallee L. The prevalence of triggers in paediatric migraine: a questionnaire study in 102 children and adolescents. J Headache Pain. 2012;13(1):61–65. doi:10.1007/s10194-011-0397-2
74. Bruni O, Russo PM, Ferri R, Novelli L, Galli F, Guidetti V. Relationships between headache and sleep in a non-clinical population of children and adolescents. Sleep Med. 2008;9(5):542–548. doi:10.1016/j.sleep.2007.08.010
75. Bruni O, Galli F, Guidetti V. Sleep hygiene and migraine in children and adolescents. Cephalalgia. 1999;19:57. doi:10.1177/0333102499019S2516
76. Heyer GL, Rose SC, Merison K, Perkins SQ, Lee JE. Specific headache factors predict sleep disturbances among youth with migraine. Pediatr Neurol. 2014;51(4):489–493. doi:10.1016/j.pediatrneurol.2014.07.001
77. Bruni O, Russo P, Violani C, Guidetti V. Sleep and migraine: an actigraphic study. Cephalalgia. 2004;24(2):134–139. doi:10.1016/j.sleep.2007.08.010
78. Carver CS, Connor-Smith J. Personality and coping. Annu Rev Psychol. 2009;61(1):679–704. doi:10.1146/annurev.psych.093008.100352
79. Guidetti V, Faedda N, Siniatchkin M. Migraine in childhood: biobehavioural or psychosomatic disorder? J Headache Pain. 2016;17(1):82. doi:10.1186/s10194-016-0675
80. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
81. Palermo TM, Lewandowski AS, Long AC, Burant CJ. Validation of a self-report questionnaire version of the Child Activity Limitations Interview (CALI): the CALI-21. Pain. 2008;139(3):644–652. doi:10.1016/j.pain.2008.06.022
82. Zuckerman B, Stevenson J, Bailey V. Stomachaches and headaches in a community sample of preschool children. Pediatrics. 1987;79(5):677–682.
83. McGrady ME, Ryan JL, Gutiérrez‐Colina AM, Fredericks EM, Towner EK, Pai ALH. The impact of effective paediatric adherence promotion interventions: systematic review and meta-analysis. Child Care Health Dev. 2015;41(6):789–802. doi:10.1111/cch.12271
84. Hamari J, Koivisto J, Sarsa H. Does gamification work? – A literature review of empirical studies on gamification.
85. Cerutti R, Presaghi F, Spensieri V, Valastro C, Guidetti V. The potential impact of internet and mobile use on headache other somatic symptoms in adolescence. A population-based cross-sectional study. Headache. 2016;56(7):1161–1170. doi:10.1111/head.12840
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.