Back to Journals » Infection and Drug Resistance » Volume 16
Nonlinear Relationship Between Interleukin-6 and NT-proBNP at Admission in Hospitalized COVID-19 Patients
Received 14 July 2023
Accepted for publication 14 September 2023
Published 21 September 2023 Volume 2023:16 Pages 6259—6267
DOI https://doi.org/10.2147/IDR.S426470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Meijuan Zhang, Zhanquan Jiao
Department of Cardiology, Tianjin Institute of Respiratory Diseases, Tianjin Haihe Hospital, Tianjin University, Tianjin, People’s Republic of China
Correspondence: Zhanquan Jiao, Department of Cardiology, Tianjin Haihe Hospital, Jingu Road, Tianjin, 300350, People’s Republic of China, Tel +8613752370120, Email [email protected]
Purpose: Elevated levels of the inflammatory marker interleukin-6 (IL-6) and cardiac injury marker N-terminal pro-B-type natriuretic peptide (NT-proBNP) have been observed in patients with coronavirus disease 2019 (COVID-19). However, the relationship between IL-6 and NT-proBNP levels remains unclear. Therefore, we investigated the relationship between IL-6 and NT-proBNP levels in patients with COVID-19.
Patients and Methods: This was a cross-sectional study. Consecutive patients with COVID-19 were included herein. The independent and dependent target variables were the IL-6 and NT-proBNP levels, respectively, measured at baseline. Univariate and multivariate linear regression analyses and curve fitting were also performed.
Results: The average age of the 121 selected participants was 49.8 ± 15.8 years old, and 48.8% (59/121) were male. The estimated β value between Ln-transformed IL-6 and NT-proBNP was 0.28 (95% confidence interval [CI] 0.12– 0.44, P = 0.001) in univariate logistic regression analysis and 0.09 (95% CI − 0.04– 0.21, P = 0.176) in the fully adjusted model. This relationship was nonlinear, with a point of 2.7, and the β values (and CIs) for the left (< 2.7) and right (≥ 2.7) sides of the inflection point were − 0.06 (95% CI − 0.23– 0.12, P = 0.534) and 0.77 (95% CI 0.18– 1.37, P = 0.016) in the fully adjusted model, respectively.
Conclusion: Our results suggest a nonlinear association between IL-6 and NT-proBNP levels. Higher IL-6 levels are associated with NT-proBNP in patients with COVID-19.
Keywords: interleukin-6, NT-proBNP, COVID-19, nonlinear association
Introduction
In December 2019, pneumonia caused by a novel coronavirus broke out in Wuhan City, Hubei Province, China, and caused a global pandemic.1 Coronavirus disease 2019 (COVID-19) poses a significant threat to human health and was originally considered a respiratory disease. Heart injury is a common complication in patients with COVID-19. Myocardial injuries associated with COVID-19 have also been observed in several patients.2 Myocardial injury has been found to be significantly and independently associated with mortality.3,4
The N-terminal pro-B-type natriuretic peptide (NT-proBNP) is a commonly used biomarker of cardiac injury and has been used as an outcome indicator in study.5 NT-proBNP is an endogenous hormone secreted by ventricular myocytes after injury and has proven useful for risk stratification of heart failure.6 In a multicenter retrospective study of 3219 patients diagnosed with COVID-19, after adjusting for age, sex, and complications, an increase in NT-proBNP was significantly associated with 28-day mortality (HR 5.11, 95% confidence interval [CI] 3.50–7.47, P < 0.001).
Interleukin (IL)-6 is a pleiotropic inflammatory cytokine that affects mitochondrial activity, vascular disease, and innate and adaptive immunity7,8 and is a well-established cytokine storm indicator. Based on an analysis of 150 patients with COVID‑19 in Wuhan, China, an increase in IL-6 levels is a clinical predictor of death. Previous studies have shown that increased IL-6 levels in vivo mediate myocardial fibrosis, concentric hypertrophy, and diastolic dysfunction in rats.9 Elevated plasma IL-6 levels are frequently observed in patients with acute and chronic heart failure and are associated with poor clinical outcomes.10 However, contradictory conclusions have been drawn. Another study showed that IL-6 supplementation protects myocardial cells from oxidative stress during the early stages of lipopolysaccharide (LPS)-induced sepsis in rats.11 In addition, whether an increase in IL-6 levels is harmful or beneficial in COVID-19 remains controversial.12
Simultaneous elevation of IL-6 and NT-proBNP levels have been observed in patients with severe acute respiratory syndrome coronavirus 2 (SARS CoV-2) infection.13,14 However, the relationship between elevated IL-6 levels and NT-proBNP, which is used as a cardiac injury index, in patients with COVID-19 with still lacking evidence. Considering that both IL-6 and NT-proBNP are related to heart injury in patients with COVID-19 and that IL-6 may be a potential therapeutic target for cytokine storms, it is necessary to estimate IL-6 levels and explore its association with NT-proBNP. Therefore, we investigated whether IL-6 is independently related to NT-proBNP in patients with COVID-19.
Materials and Methods
Study Design and Participants/Study Population
Patients with COVID-19 were enrolled in this study from the infection department of Haihe Hospital, City, China, from January 21, 2020, to February 28, 2020, data were collected using the hospital's electronic medical record system. The target-independent variable was the IL-6 level, which was obtained at baseline. The NT-proBNP level was the dependent variable. All enrolled patients met the diagnostic criteria and clinical classification of the “Chinese Clinical Guidelines for COVID-19 Pneumonia Diagnosis and Treatment (sixth edition)”, published by the China National Health Commission.
Based on clinical symptoms, the severity of COVID-19 can be divided into the following four types: 1) mild, with mild clinical symptoms and no evidence of pneumonia; 2) moderate, with fever, respiratory symptoms, and confirmed pneumonia; 3) severe, any of the following: respiratory distress, respiratory rate (RR) >30 bpm, resting oxygen saturation <93%, or PaO2/FiO2 of <300 mmHg; and 4) critical, with any of the following: respiratory failure requiring mechanical ventilation, shock, or a combination of any other organ failure requiring intensive care.
We included only adult patients (aged ≥18 years). All participants were hospitalized. Patients with missing NT-proBNP and IL-6 data or a history of heart failure were excluded.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Tianjin Haihe Hospital (2023HHWZ-002). Owing to the retrospective design of this study and the utilization of anonymized data, the requirement for informed consent was waived.
Variables
NT-proBNP and IL-6 levels were first determined during hospital admission. Owing to skewness, the IL-6 and NT-proBNP levels were logarithmically transformed using the natural logarithm.
For the present analysis, we systematically identified patients with abnormal NT-proBNP levels according to the cutoff values recommended by the Heart Failure Association of the European Society of Cardiology: >450 pg/mL in patients aged <50 years, >900 pg/mL in patients aged 50–75 years, and >1800 pg/mL in patients aged >75 years.15 The routine upper normal limit of IL-6 as defined by the local laboratory was <10 pg/mL.
The following variables were included (1) demographic data; (2) variables that could affect IL-6 or NT-proBNP levels reported in literature; and (3) our clinical experience. Therefore, the following variables were used to construct the fully adjusted model: (1) continuous variables: age, onset time, white blood cell count, fasting blood glucose, hemoglobin, lymphocyte, creatinine, uric acid, aspartate aminotransferase, alanine aminotransferase, albumin, D-dimer, C-reactive protein, and CK-MB (obtained at baseline); and (2) categorical variables: sex, severity, smoking, drinking, and coronary heart disease (obtained at baseline).
Owing to the limited patient population in the mild and severe types, the participants were categorized into two groups: severe and non-severe. The non-severe group encompassed mild and moderate-type ones, whereas the severe group comprised patients with severe and critical type.
Statistical Analysis
Descriptive analyses were performed for all individuals. Categorical variables were expressed as numbers and percentages. Continuous variables were expressed as means and standard deviations thereof for normally distributed variables or medians and interquartile ranges for non-normally distributed variables.
Univariate and multivariate linear regression analyses were performed. We constructed three models: model I, adjusted for hemoglobin and albumin levels; model II, adjusted for variables in model I plus severity and coronary heart disease; and model III, adjusted for variables in model II plus age and sex.
A risk-adjusted restricted cubic spline (four nodes) was used to address the relationship between IL-6ln and NT-proBNPln. Any nonlinear relationship between IL-6ln and NT-proBNPln levels was evaluated using spline regression. The inflection point of IL-6ln was graphically represented to visualize the point at which NT-proBNPln began to increase. The influence point was moved along a predefined interval and detected to obtain the maximum likelihood of the model.
Because IL-6, C-reactive protein, and lymphocytes are indicators of inflammation, they were not included in the multifactor linear regression models.
All analyses were performed using the R statistical software package (http://www.R-project.org, The R Foundation) and Free Statistics software version 1.7. Two-tailed tests were performed, with P < 0.05.
Results
Baseline Characteristics of Selected Participants
A total of 121 participants were selected for final data analysis (see Figure 1 for a flowchart). The baseline characteristics of the study participants are shown in Table 1. The average age of the 121 selected participants was 49.8 ± 15.8 years old, and approximately 48.8% of them were male. The NT-proBNP and IL-6 levels were elevated in 7 and 50 of participants, respectively.
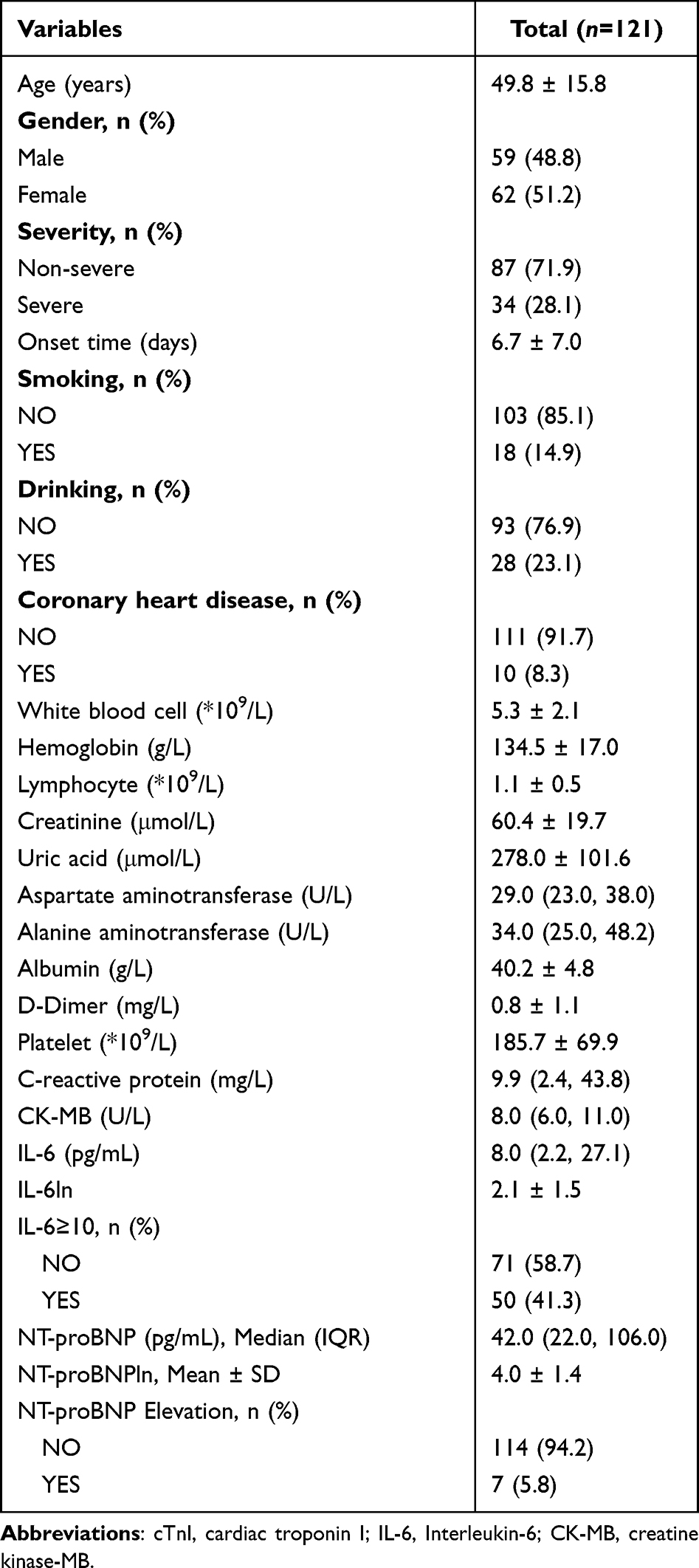 |
Table 1 Baseline Characteristics of Participants |
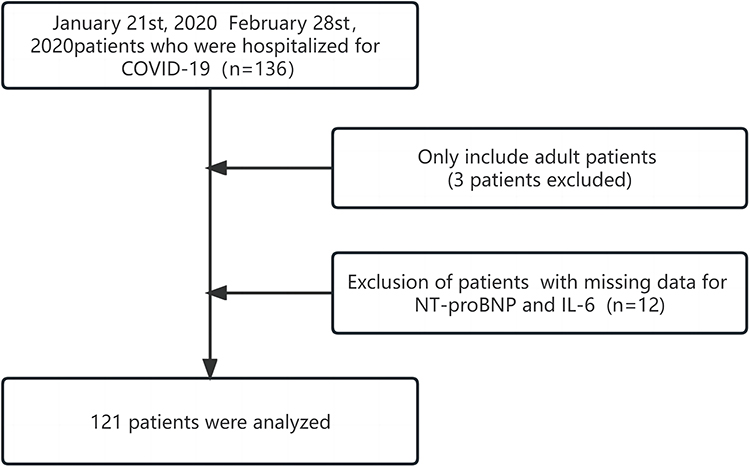 |
Figure 1 Flow chart describing the inclusion and exclusion criteria for study patients. |
Univariate Analysis
The univariate analysis results are presented in Table 2. Univariate binary logistic regression revealed that sex, creatinine, and CK-MB levels were not associated with NT-proBNP levels. Furthermore, lymphocyte, albumin, and hemoglobin levels were found to be negatively associated with NT-proBNP levels. In contrast, univariate analysis showed that age, severity, coronary heart disease, C-reactive protein level, and IL-6 level were positively correlated with NT-proBNP level.
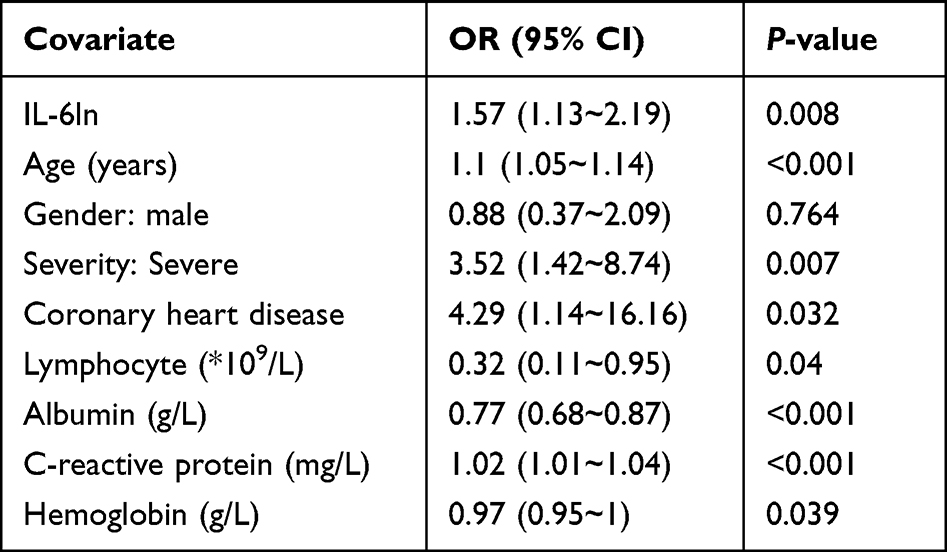 |
Table 2 Univariable Linear Regression Analyses of the Associations Between IL-6 and NT-proBNP Measured at Admission |
Results of Unadjusted and Adjusted Linear Regression
In this study, three models were constructed to analyze the independent effects of IL-6 on NT-proBNP levels (univariate and multivariate linear regressions). The effect sizes and 95% CIs are listed in Table 3. In the unadjusted model, high levels of IL-6ln at the baseline were significantly associated with NT-proBNPln (β = 0.28; 95% CI 0.12–0.44, P = 0.001).
 |
Table 3 Multivariable Linear Regression Analyses of the Associations Between IL-6 and NT-proBNP at Admission |
In the fully adjusted model (model 3), the estimated β value between IL-6ln and NT-proBNPln was 0.09 (95% CI −0.04–0.21, P = 0.176).
The Results of Nonlinearity of IL-6 and NT-proBNP
The smooth curve and results of the generalized additive model showed that the relationship between IL-6ln and NT-proBNPln was nonlinear after adjusting for age, sex, severity, coronary heart disease, and hemoglobin and albumin levels (Figure 2). The NT-proBNPln was relatively flat until the IL-6ln was approximately 2.7; thereafter, it increased (P for nonlinearity = 0.024).
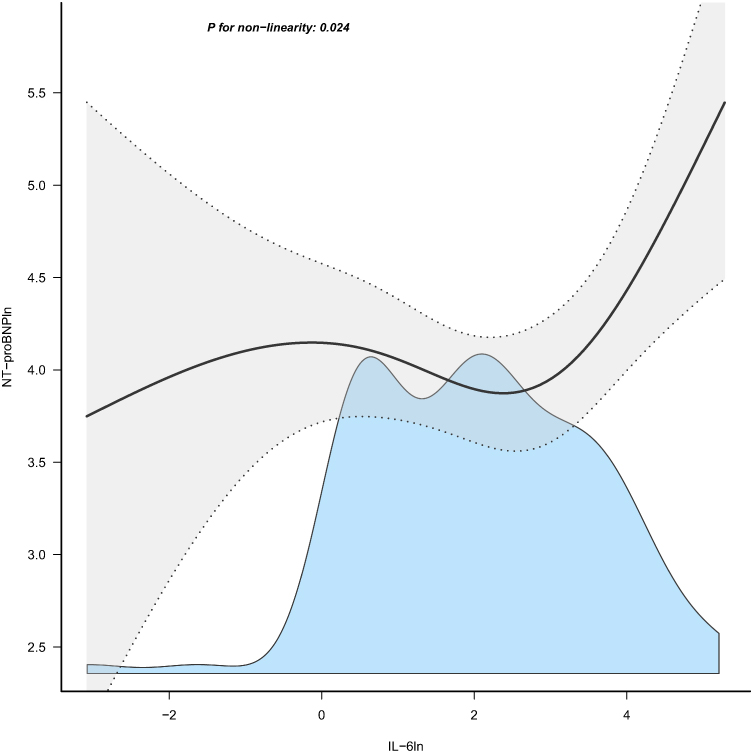 |
Figure 2 The fully adjusted model demonstrates the utilization of natural-penalized splines to determine the β values for NT-proBNP in relation to changes in IL-6, accompanied by 95% confidence intervals. |
Because the P for the log-likelihood ratio test was less than 0.05, we chose a two-piecewise linear regression to fit the association between IL-6ln and NT-proBNPln because it could accurately represent the relationship. On the left side of the inflection point (IL-6ln = 2.7), the effect size and 95% CI were −0.06 (−0.23–0.12, P = 0.534). On the right side of the inflection point, the effect size and 95% CI were 0.77 (0.18–1.37, P = 0.016) (Table 4).
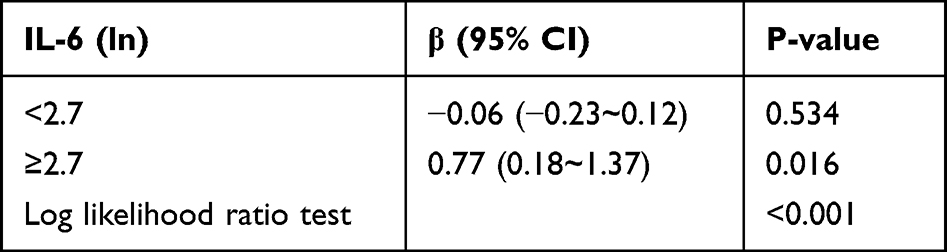 |
Table 4 Relationship Between IL-6ln and NT-proBNPln in Two-Piece-Wise Linear Regression Model |
Discussion
Our findings indicate that IL-6ln is positively associated with NT-proBNPln (β = 0.28, 95% CI 0.12–0.44, P = 0.001) in univariate logistic regression analysis, and the estimated β value was 0.09 (95% CI −0.04–0.21, P = 0.176) after adjusting for other covariates. Furthermore, we find that trend of the effect sizes on the left and right sides of the inflection point was inconsistent [left −0.06 (95% CI −0.23–0.12, P = 0.534); right 0.77 (95% CI 0.18–1.37, P = 0.016)]. This suggests a J-shaped association between IL-6 and NT-proBNP levels.
Sheth et al suggested that BNP levels were significantly higher in patients who died or were critically ill.16 Cardiac injury was independently associated with significantly increased odds of mortality. Similar findings have been reported by Qin et al17 and Shi et al.4 As a marker of cardiac injury, there was a 5.8% (7/121) prevalence of high NT-proBNP levels in patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in our study, which is lower than that reported in previous studies. Ruan et al reported that 7% patients with COVID-19 had myocardial damage,3 and Shi et al reported that 19.7% patients had cardiac injury in hospitalized patients with COVID-19.4 The definition of cardiac injury may have contributed to the discrepancy in results. In our study, elevated NT-proBNP was used to define cardiac injury in patients with COVID-19, whereas Ruan and Shi defined cardiac injury as blood levels of cardiac biomarkers (hs-TNI) above the 99th-percentile upper reference limit.3,4
The levels of the inflammatory biomarker IL-6 in COVID-19 are significantly increased in patients with severe disease and death.16,18 In another study, serum IL-6 has not been found to predict mortality in patients with COVID-19 in the ICU.19 There was a 41.3% prevalence of high IL-6 in patients with SARS-CoV-2 infection in our study. Giannitrapani et al observed higher IL-6 values in 16% non-critical and 53% critical patients.20
In a previous study, the dynamic evolution of IL-6 was shown to predict the 180-day all-cause mortality in patients with acute heart failure.21 In addition, acute and persistent elevations of IL-6 levels after ST-elevation myocardial infarction is associated with all-cause mortality.22 Siddiq et al infected human induced pluripotent stem cell-derived cardiomyocytes obtained from healthy human subjects with SARS CoV-2. Without increasing the degree of infection, IL-6 can cause dysfunctional myocardial cell contraction and decreased beating. However, whether an increase in IL-6 levels is harmful or beneficial in COVID-19 remains controversial.12 It is currently unclear whether elevated IL-6 levels are detrimental or beneficial to COVID-19. In an experimental model, IL-6 has been shown to suppress or facilitate viral replication.23
IL-6-deficient mice are more likely to die from influenza virus infection.24 Peng et al11 reported that IL-6 protects cardiomyocytes from oxidative stress during the early stages of LPS-induced sepsis.
In our study, we found a nonlinear relationship between IL-6 and NT-proBNP levels on the right side of the inflection point 2.7 (IL-6 = 14.8 pg/mL); IL-6 and NT-proBNP showed strong association. Low-dose IL-6 has been reported to play a beneficial role in cardiovascular diseases.11 IL-6 was administered at a rate of 2.5 μg·kg-1·hr-1 for 7 days, and adverse myocardial remodeling was mediated by elevated levels of IL-6.9 In addition, only the highest quartile of IL-6 level was associated with an increased risk of adverse clinical events and long-term all-cause mortality in patients with acute myocardial infarction.22 The concentration-dependent correlation between IL-6 and NT-proBNP levels may partly explain the discrepancy between the beneficial and harmful effects of IL-6 on the heart.
However, the potential mechanism by which IL-6 is associated with NT-proBNP levels in patients with COVID-19 remains unclear. The pathological anatomy of COVID-19 shows interstitial monocyte infiltration into myocardial tissue.25 The novel coronavirus invades human cells through the high affinity of the S protein for ACE2 of human cells.26 ACE2 is widely expressed in the cardiovascular system, and its related signaling pathways may play a role in heart injury. Hypoxemia and hypotension induced by pulmonary infections lead to insufficient oxygen and blood supply to the myocardium. Stretching the myocardium is known to elevate BNP levels and increase IL-6 production,27 and IL-6 induces the secretion of natriuretic peptides via IL-6 trans-signaling.28
The clinical value of this study is as follows: (1) to the best of our knowledge, this is the first study to observe a nonlinear association between IL-6 and NT-proBNP in patients with COVID-19; (2) the findings of this study should aid future research in the establishment of predictive models of NT-proBNP; and (3) in the case of IL-6 antagonists, it may be appropriate to perform a layered analysis based on the concentration of IL-6.
This study had the following limitations: 1, whenever a retrospective analysis was conducted, residual confounding may have occurred. To the best of our knowledge, this study adjusted for as many confounders as possible. 2, There was no causal relationship to establish as this was a cross-sectional study. 3, The participants of this study included patients who were positive for COVID-19. Therefore, there was a deficiency in the universality and extrapolation of this study. 4, Because we excluded patients with a history of heart failure, the findings of this study cannot be applied to these patients. 5, Due to the nature of our cross-sectional study on admission data, information regarding the utilization of angiotensin receptor blockers,29 which may affect NT-proBNP and mortality, is currently unavailable. However, we intend to delve deeper into this aspect through future investigations.
Conclusion
In this study, we addressed the nonlinearity between IL-6 and NT-proBNP levels in patients with COVID-19. This association warrants further extensive prospective cohort studies.
Acknowledgments
The authors thank all the staff members in our institution.
We thank Dr. Jie Liu of the Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital, for his statistical support and comments regarding the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lai -C-C, Shih T-P, W-C K, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924.
2. Topol EJ. COVID-19 can affect the heart. Science. 2020;370(6515):408–409. doi:10.1126/science.abe2813
3. Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46(5):846–848.
4. Shi S, Qin M, Shen B, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020;5(7):802–810. doi:10.1001/jamacardio.2020.0950
5. Ye L, Hu G, Yu H, Sun J, Yuan H. Metoprolol improves myocardial remodeling and cardiac function in patients with permanent pacemaker implantation. J Healthc Eng. 2022;2022:7340992. doi:10.1155/2022/7340992
6. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
7. McInnes IB, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol. 2007;7(6):429–442. doi:10.1038/nri2094
8. Rohleder N, Aringer M, Boentert M. Role of interleukin-6 in stress, sleep, and fatigue. Ann N Y Acad Sci. 2012;1261:88–96. doi:10.1111/j.1749-6632.2012.06634.x
9. Melendez GC, Mclarty JL, Levick SP, Du Y, Janicki JS, Brower GL. Interleukin 6 mediates myocardial fibrosis, concentric hypertrophy, and diastolic dysfunction in rats. Hypertension. 2010;56(2):225. doi:10.1161/HYPERTENSIONAHA.109.148635
10. Markousis-Mavrogenis G, Tromp J, Ouwerkerk W, et al. The clinical significance of interleukin-6 in heart failure: results from the BIOSTAT-CHF study. Eur J Heart Fail. 2019;21(8):965–973. doi:10.1002/ejhf.1482
11. Peng Y, Yang Q, Gao S, et al. IL-6 protects cardiomyocytes from oxidative stress at the early stage of LPS-induced sepsis. Biochem Biophys Res Commun. 2022;603:144–152. doi:10.1016/j.bbrc.2022.03.013
12. McGonagle D, Sharif K, O’Regan A, Bridgewood C. The role of cytokines including interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease. Autoimmun Rev. 2020;19(6):102537. doi:10.1016/j.autrev.2020.102537
13. Pilut CN, Citu C, Gorun F, et al. The utility of laboratory parameters for cardiac inflammation in heart failure patients hospitalized with SARS-CoV-2 infection. Diagnostics. 2022;12(4):824. doi:10.3390/diagnostics12040824
14. Caro-Codón J, Rey JR, Buño A, et al. Characterization of NT-proBNP in a large cohort of COVID-19 patients. Eur J Heart Fail. 2021;23(3):456–464. doi:10.1002/ejhf.2095
15. Mueller C, McDonald K, de Boer RA, et al. Heart failure association of the European society of cardiology practical guidance on the use of natriuretic peptide concentrations. Eur J Heart Fail. 2019;21(6):715–731. doi:10.1002/ejhf.1494
16. Sheth A, Modi M, Dawson D, Dominic P. Prognostic value of cardiac biomarkers in COVID-19 infection. Sci Rep. 2021;11(1):4930. doi:10.1038/s41598-021-84643-6
17. Qin -J-J, Cheng X, Zhou F, et al. Redefining cardiac biomarkers in predicting mortality of inpatients with COVID-19. Hypertension. 2020;76(4):1104–1112. doi:10.1161/HYPERTENSIONAHA.120.15528
18. Hara S, Sanatani T, Tachikawa N, et al. Comparison of the levels of neopterin, CRP, and IL-6 in patients infected with and without SARS-CoV-2. Heliyon. 2022;8(5):e09371. doi:10.1016/j.heliyon.2022.e09371
19. Talwar D, Kumar S, Acharya S, et al. Interleukin 6 and its correlation with COVID-19 in terms of outcomes in an intensive care unit of a rural hospital: a cross-sectional study. Indian J Crit Care Med. 2022;26(1):39–42. doi:10.5005/jp-journals-10071-24075
20. Giannitrapani L, Augello G, Mirarchi L, et al. Outcome predictors in SARS-CoV-2 disease (COVID-19): the prominent role of IL-6 levels and an IL-6 gene polymorphism in a western Sicilian population. J Infect. 2022;85:174–211. doi:10.1016/j.jinf.2022.04.043
21. Markousis-Mavrogenis G, Tromp J, Mentz RJ, et al. The additive prognostic value of serial plasma interleukin-6 levels over changes in brain natriuretic peptide in patients with acute heart failure. J Card Fail. 2021;27(7):808–811. doi:10.1016/j.cardfail.2021.01.008
22. Tøllefsen IM, Shetelig C, Seljeflot I, Eritsland J, Hoffmann P, Andersen G. High levels of interleukin-6 are associated with final infarct size and adverse clinical events in patients with STEMI. Open Heart. 2021;8(2):824. doi:10.1136/openhrt-2021-001869
23. Velazquez-Salinas L, Verdugo-Rodriguez A, Rodriguez LL, Borca MV. The Role of Interleukin 6 During Viral Infections. Front Microbiol. 2019;10:1057. doi:10.3389/fmicb.2019.01057
24. Yang M-L, Wang C-T, Yang S-J, et al. IL-6 ameliorates acute lung injury in influenza virus infection. Sci Rep. 2017;7:43829. doi:10.1038/srep43829
25. Xu Z, Shi L, Wang Y, Zhang J, Wang F. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respirat Medi. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
26. Donoghue M, Hsieh F, Baronas E, et al. A novel angiotensin-converting enzyme-related carboxypeptidase (ACE2) converts angiotensin I to angiotensin 1-9. Circ Res. 2000;87(5):E1–9. doi:10.1161/01.RES.87.5.e1
27. Nian M, Lee P, Khaper N, Liu P. Inflammatory cytokines and postmyocardial infarction remodeling. Circ Res. 2004;94(12):1543–1553. doi:10.1161/01.RES.0000130526.20854.fa
28. Szabo-Fresnais N, Lefebvre F, Germain A, Fischmeister R, Signalling MP. A new regulation of IL-6 production in adult cardiomyocytes by beta-adrenergic and IL-1 beta receptors and induction of cellular hypertrophy by IL-6 trans-signalling. Cell Signal. 2010;22(7):1143–1152. doi:10.1016/j.cellsig.2010.03.009
29. Acharya S, Kumar S, Kabra R, et al. Impact of angiotensin receptor blocker as antihypertensive in assessing mortality in patients of COVID-19: a single tertiary care center study. J Educ Health Promot. 2023;12:30. doi:10.4103/jehp.jehp_922_22
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.