")
Back to Journals » Clinical Epidemiology » Volume 15
Non-Selective Beta-Blockers and Risk of Sepsis in Patients with Cirrhosis and Ascites: Results from a Large Observational Study
Authors Jensen MD , Watson H , Vilstrup H, Jepsen P
Received 6 December 2022
Accepted for publication 22 May 2023
Published 21 June 2023 Volume 2023:15 Pages 775—783
DOI https://doi.org/10.2147/CLEP.S400399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Henrik Sørensen
Morten Daniel Jensen,1 Hugh Watson,1,2 Hendrik Vilstrup,1 Peter Jepsen1
1Department of Hepatology and Gastroenterology, Aarhus University Hospital, Aarhus, Denmark; 2Evotec ID (Lyon), Lyon, France
Correspondence: Morten Daniel Jensen, Department of Hepatology and Gastroenterology, Aarhus University Hospital, Entrance C, Plan 1, Intersection C116, Palle Juul-Jensens Boulevard 99, Aarhus N, 8200, Denmark, Tel +45 8949 3333, Email [email protected]
Background and Aims: Previous studies have not been able to determine whether non-selective beta-blockers (NSBB) reduce the risk of sepsis in cirrhosis. We aimed to examine this question with data from 1198 patients with cirrhosis and ascites included in clinical studies of satavaptan, a vasopressin receptor antagonist with no effect on infection risk.
Methods: Risk of sepsis was estimated for NSBB users vs nonusers. Patients were examined every four weeks, or in relation to hospitalization, for the one-year duration of the trials. We computed the cumulative risk of sepsis for patients who did vs did not use NSBB at baseline. We used Cox regression to compare hazard rates of sepsis between current users and nonusers, accounting for changes in NSBB use over time. We adjusted for patient sex and age, MELD-Na score, albumin, use of antibiotics, use of proton pump inhibitors, cirrhosis etiology, history of variceal bleeding or SBP, severity of ascites and HE, HCC, other cancers, and diabetes, while stratifying on geographical region.
Results: Of the 1198 patients, 54% used NSBB at some time. There were 56 sepsis episodes. The 1-year risk of sepsis was reduced to 5.7% (95% confidence interval [CI] 2.8– 8.6) in baseline NSBB users vs 11.6% (95% CI 7.0– 15.9) in baseline nonusers. The hazard ratio of sepsis for current NSBB users vs current nonusers was reduced to 0.5 (95% CI 0.3– 0.8) and after adjustment to 0.7 (95% CI 0.4– 1.3).
Conclusion: NSBB use may reduce the risk of sepsis in patients with cirrhosis and ascites, but the precision of the estimate was limited by the number of episodes of sepsis.
Keywords: non-selective beta-blockers, NSBB, infection, decompensated, time-dependent, treatment
Plain Language Summary
To help patients with cirrhosis of the liver, we examined if non-selective beta-blockers, a prescription drug used to prevent bleeding from varices of the oesophagus or the stomach, may help prevent sepsis, a severe manifestation of bacterial infection. We found that non-selective beta-blockers may have some protective effect against sepsis, though the effect could not be precisely estimated because only few patients had a sepsis episode.
Introduction
In patients with cirrhosis, infections are a leading cause of mortality,1 and sepsis is the most severe manifestation of infection. The barrier of the gut is important in keeping the potentially invasive microbes residing in the intestinal tract separated from the host. In cirrhosis, portal hypertension is found to increase gut permeability, making bacterial components able to translocate across the barrier.2–4 Translocation of gut bacteria to the portal blood is a likely route to sepsis in these patients, and reduction of portal pressure with non-selective beta-blockers (NSBB) reduces intestinal permeability and therefore possibly the risk of bacterial translocation and sepsis.5 This is the proposed mechanism behind a protective role of NSBB against sepsis. A small cross-sectional single-center study examined the effect of chronic NSBB use (ie, initiated 4 weeks or more) before hospitalization on the in-hospital sepsis risk and indicated a degree of protection. However, only hospitalized patients were included, follow-up was restricted by the length of their hospital stay, and the study may have underestimated the effects of NSBB use because it did not consider the possibility that patients could stop or start NSBB treatment during the follow-up.6
In light of the central prognostic importance of sepsis and the widespread use of NSBB in cirrhosis patients, we set out to study the effect of NSBB use on the risk of sepsis in a large, detailed database on cirrhosis patients with ascites. The study cohort comprised 1198 such patients prospectively recruited, and the database included comprehensive information on medications, potential confounders, and outcomes.
Materials and Methods
Data Sources
Three multicenter randomized controlled trials were conducted between 2006 and 2008 to examine the effect of satavaptan on ascites in patients with cirrhosis.7 The three trials were performed to a common design and examined patients with, respectively, diuretic-manageable ascites (N = 462), ascites managed by diuretics and occasional therapeutic paracentesis (N = 496), and diuretic-resistant ascites managed primarily by therapeutic paracentesis (N = 240). The primary outcomes were worsening of ascites in the first trial, and 12-week cumulative number of large volume paracenteses in the other two. The planned treatment duration was 52 weeks, but in all three trials some patients discontinued treatment earlier, and the second and third trials were stopped early due to expected poor risk–benefit ratio. All patients were followed for an additional week after their study medication was discontinued to assess drug safety, and patients experiencing an adverse event were followed until the event resolved or stabilized.7,8
Patients were excluded from participating in the trials if they had a functioning transjugular intrahepatic portosystemic shunt (TIPS), hepatic encephalopathy (HE) grade ≥2, variceal bleeding within 10 days prior to randomization, spontaneous bacterial peritonitis (SBP) within 10 days prior to randomization, serum creatinine >150 μmol/L, serum potassium >5.5 mmol/L, serum sodium >143 mmol/L, serum bilirubin >150 μmol/L, International Normalized Ratio (INR) >3.0, platelets <30,000/mm3, neutrophils <1000/mm3, hepatocellular carcinoma (HCC) beyond the Milan criteria (ie, 1 nodule >5 cm, 2 or 3 nodules with one or both >3 cm, or more than 3 nodules), used a potent modifier of the cytochrome P450 3A drug metabolism pathway, or used drugs with a risk of Q-T interval prolongation.7,8
Definitions
All diagnoses and medications were given by trained specialists in hepatology.
Follow-Up and Variable Update
Follow-up started on the date of randomization and ended one week after the study medication was discontinued, at which point surviving patients left the study.
At inclusion, investigators recorded cirrhosis etiology and whether patients had refractory ascites, a history of variceal bleeding, a history of HCC or other cancer, a history of diabetes mellitus (type 1 or type 2), or a history of SBP, as well as the patients’ sex and age; those variables were considered as constants in the analyses. Every four weeks, patients were seen in the outpatient clinic where clinical data and current medications were recorded, and blood samples were taken for serum biochemistry. Further, variables were updated at hospital contacts and during hospital admissions. Variables that were updated during the follow-up period were as follows: NSBB use, Model for End-stage Liver Disease Sodium (MELD-Na) score (according to United Network for Organ Sharing policy note 20159), serum albumin, antibiotics use, PPI use, and HE grade (grade 1–4).
Sepsis
Sepsis diagnoses were given according to guidelines at the treating hospitals. At the time, sepsis was defined in international literature according to the second revision of the sepsis criteria, ie, meeting at least two of the Systemic Inflammatory Response Syndrome (SIRS) criteria while having an infection.10,11 SIRS criteria, as defined by Bone et al: 1) Temperature >38°C/<36°C; 2) Heart rate >90 beats per minute; 3) Respiratory rate >20 breaths per minute/PaCO2 <32mm Hg; 4) White blood cell count >12,000 per mm3/<4000 per mm3/>10% immature (band) forms.11 The trial protocols did not instruct clinicians to specify the infection resulting in sepsis.
NSBB
Patients were considered NSBB users if they were prescribed either propranolol, carvedilol or nadolol. NSBB doses were evaluated in NSBB-type-dependent categories [annotated as propranolol/nadolol or carvedilol daily dose]: low: ≤40 or <12.5mg; medium: 41–80 or 12.5–24mg; high: >80 or ≥25mg.
Antibiotics
Antibiotics were defined as “any antibiotics except rifaximin or paromomycin” (which does not have systemic effects) and were considered prescribed simultaneously with (ie, against) sepsis if prescribed on the day of the sepsis diagnosis.
Statistical Analyses
NSBB treatment was instituted or discontinued at the attending physicians’ discretion as the trial protocols did not provide any instructions related to NSBB use. With respect to the effect of NSBB use, consequently, the trials were one large observational study.
We considered death as a censoring, not a competing, event, as a previous study of this same cohort found that NSBB use did not affect mortality.12 Satavaptan was not considered a confounding variable, as another study of this same cohort found that satavaptan use did not affect the risk of infections.7
Patient characteristics were compared using chi-square test for dichotomous variables, Wilcoxon Mann–Whitney rank sum test for comparing two medians, and Kruskal–Wallis test for comparing multiple medians.
Risk of Sepsis
Baseline NSBB Use
We used the cumulative incidence function to examine the cumulative risk of sepsis for patients who did or did not use NSBB at baseline. Cirrhosis severity was likely to influence the probability of discontinuing NSBB, since complications or adverse events from cirrhosis might result in premature termination of treatment. To correct the cumulative incidence estimate for such informative censoring, we used stabilized inverse probability of censoring weights (the method is described in detail in Supplementary Material 1).13–15
Current NSBB Use
Use of NSBB may change during the disease course, and to utilize this information we used Cox proportional hazards regression to estimate the hazard rate ratio (HR) of sepsis based on current NSBB use, treating NSBB use as a time-dependent variable. The effect of current NSBB use was adjusted for patient sex, baseline age, current MELD-Na score, current serum albumin, current and recent antibiotics use (ie, currently using or stopped within the previous 7 days) (yes/no), current PPI use (yes/no), cirrhosis etiology (categorical: “alcohol-related” as reference category), refractory ascites (yes/no), history of variceal bleedings (yes/no), history of HCC (yes/no), history of cancer (excluding HCC) (yes/no), history of diabetes mellitus type 1 or type 2 (yes/no), history of SBP (yes/no), and HE grade (grade 1–4) while stratifying on geographical region (to account for clustering, ie, differences in baseline mortality hazard across regions).
NSBB Dose
Only few patients used carvedilol or nadolol, so we could not compare the effects between the different types of NSBB. We did, however, examine the impact of NSBB dose.16 To examine the association between NSBB dose at inclusion and risk of sepsis, we repeated the analysis of cumulative risk in the three different categories of daily NSBB dose: low, medium and high. Then, we repeated the Cox proportional hazards regression analysis treating NSBB dose as a time-dependent categorical variable.
Antibiotics Use
The trial protocols did not define sepsis, so criteria may have differed between centers. To account for this possibility, we repeated the Cox proportional hazards regression, defining sepsis as a simultaneous diagnosis of sepsis and prescription of antibiotics.
Sepsis Type
NSBB use is believed to reduce the risk of sepsis by reducing the risk of bacterial translocation from the gastrointestinal tract. Although the origin of sepsis episodes can be elusive, we repeated the Cox regression analysis with increasingly narrow definitions of “sepsis possibly attributable to bacterial translocation from the gastrointestinal tract (GI)”. The definition was narrowed down by removing sepsis episodes no longer fitting the definition, however, note that this only removed the sepsis episode, not the patient. First, we left out sepsis episodes from sepsis types not compatible with bacterial translocation from the GI tract (definition 1). Secondly, we left out sepsis episodes with either a sepsis type or an underlying infection not compatible with bacterial translocation from the GI tract (definition 2). Third, sepsis was defined as sepsis episodes from sepsis types compatible with bacterial translocation from the GI tract (definition 3). Fourth, sepsis was defined as sepsis episodes from both a sepsis type and an underlying infection compatible with bacterial translocation from the GI tract (definition 4). Criteria are listed in Table S1.
Refractory Ascites
Use of NSBB in patients with refractory ascites has been debated. Therefore, we repeated the Cox regression analysis in the 595 patients with refractory ascites.
Mortality
Patients with Sepsis, After Sepsis Episode
Mortality for patients who developed sepsis was estimated from the date of sepsis diagnosis, using the Kaplan–Meier estimator. We used Cox regression to estimate the effect of NSBB use on the mortality hazard, and here we adjusted for the same confounders as in our analysis of sepsis risk.
Results
Our 1198 patients had a median follow-up time of 246 days and a total follow-up time of 779 person-years. The median age was 57 years, and the proportion of females was 30% in both groups at inclusion. At baseline, 47% used NSBB, and 54% used NSBB at some point during the follow-up. Only one user discontinued NSBB during the 1-week period before a sepsis episode, so discontinuation had no impact on our findings. At inclusion, more NSBB users than nonusers had a history of variceal bleeding. Of the NSBB users, 65% used ≤40mg propranolol/nadolol or <12.5mg carvedilol daily (Table 1).
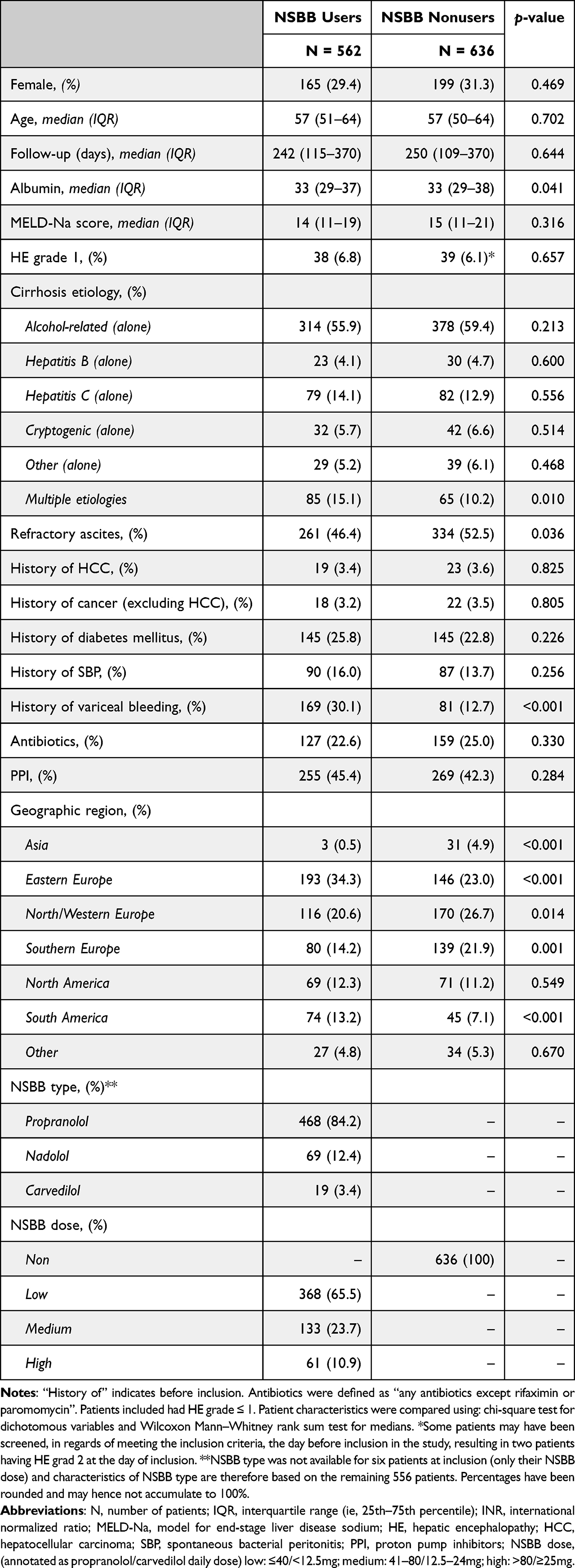 |
Table 1 Characteristics of the 1198 Patients from the Satavaptan Trials at Inclusion Based on Use of Non-Selective Beta-Blockers (NSBB) at Inclusion |
Risk of Sepsis
Overall, 56 sepsis episodes were registered during the follow-up period. Half of the sepsis patients had a recorded infection at the time of the sepsis episode (Table S1 gives information on types of infections). Thirty-seven of the sepsis patients (66%) received antibiotics on the day of the diagnosis, and an additional 11 received antibiotics within the following two days, reaching 86% of all sepsis patients. The pathogen of the sepsis episodes was unrecorded in 46 cases (82%), 8 were bacterial, and 2 were fungal. Baseline patient characteristics for the subset who later developed sepsis are presented in Table S2. Biochemistry from the time of sepsis diagnosis was not available.
Baseline NSBB Use
Patients using NSBB at the baseline of the study had a 1-year risk of sepsis of 5.7% (95% confidence interval [CI] 2.8–8.6) and those who did not had a risk of 11.6% (95% CI 7.0–15.9) (Figure 1).
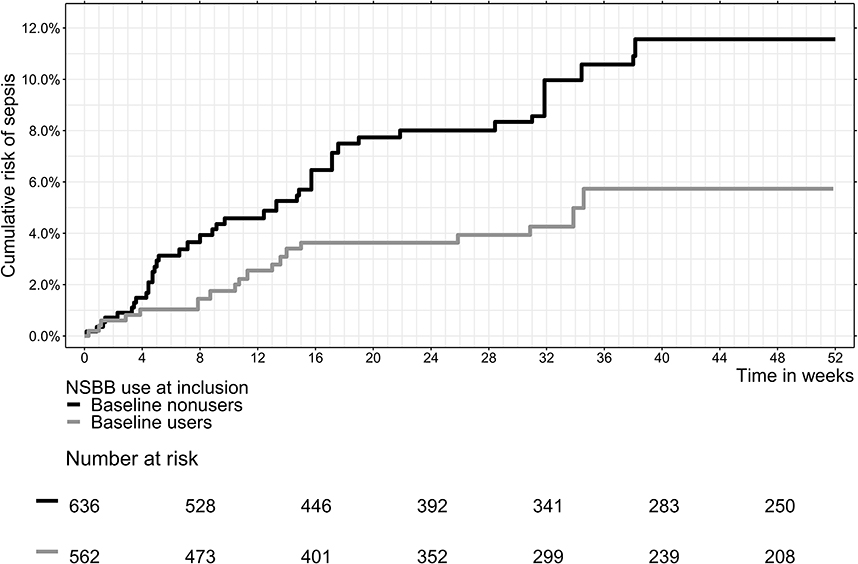 |
Figure 1 Cumulative risk of sepsis based on use of non-selective beta-blocker (NSBB) at the beginning of the study while applying inverse probability of censoring weights. |
Current NSBB Use
The crude HR of sepsis for current NSBB users vs current nonusers was 0.5 (95% CI 0.3–0.8), and the adjusted HR was 0.7 (95% CI 0.4–1.3).
NSBB Dose
We found no dose–response relationship between NSBB dose and development of sepsis. Patient characteristics by NSBB dose are presented in Table S3.
Antibiotics Use
With sepsis defined as both a sepsis diagnosis and initiation of antibiotics on the same day, 52 patients experienced a sepsis episode. Using this definition, the crude and adjusted HR’s for current NSBB users vs current nonusers were 0.5 (95% CI 0.3–0.9) and 0.8 (95% CI 0.4–1.5), respectively, essentially the same as in the primary analysis.
Sepsis Type
When using an increasingly narrow definition of sepsis, we found that the point estimate indicated a protective effect of NSBB use against sepsis, however, estimates grew very imprecise. Adjusted HRs of sepsis for current NSBB users vs current nonusers were, in the respective groups: definition 1 (53 sepsis episodes): HR 0.6 (95% CI 0.3–1.3); definition 2 (39 sepsis episodes): HR 0.5 (95% CI 0.2–1.2); definition 3 (14 sepsis episodes): HR 0.8 (95% CI 0.2–3.0); definition 4 (3 sepsis episodes): HR 0.2 (95% CI 0.002–21.3).
Refractory Ascites
Among the 595 patients with refractory ascites, comparing current NSBB users vs current nonusers yielded an adjusted HR for sepsis of 0.8 (95% CI 0.3–1.8), which is comparable to the estimate in the primary analysis.
Mortality
Patients with Sepsis, After Sepsis Episode
The sepsis patients had a 30-day mortality from onset of sepsis of 55.4% (95% CI 43.0–68.6). We could not determine the effect of NSBB use on this mortality because of the small number of patients.
Discussion
In this study, based on 1198 well-characterized trial participants with cirrhosis and ascites, we found that those who used NSBBs had a lower risk of sepsis. It must be noted, however, that there were a limited number of sepsis episodes and many relevant factors to adjust for. As a consequence, the adjusted estimate was not statistically significant. The point-estimate of relative risk, ie, the effect most compatible with the data, indicated a protective effect, a 30% relative risk reduction. The data were also reasonably compatible with an even larger relative risk reduction or even a risk increase, ie, the 95% confidence interval included strong protective effects and weak detrimental effects.
This is the first large multicenter study of its kind, and its results are in accordance with previous smaller studies. A cross-sectional study of 400 hospitalized cirrhosis patients found that patients on NSBB treatment for the previous 4 weeks had half as many sepsis episodes as those not on NSBB.6 Our study expands previous findings by showing that the protective effect may be present in established as well as newly initiated NSBB treatment. The latter observation supports the notion that a protective effect of NSSBs is indeed related to the drug and not to other unknown circumstances present at the study start.
We describe the sepsis-protective effect of NSBB under standard-of-care conditions, which is a strength in the sense that it promotes clinical generalizability of the effect. The effect is further supported by our access to comprehensive data on potential confounders updated during the study period. We found that the risk estimate for the effect measure of anytime NSBB use (HR), was most compatible with a protective effect, and that the risk estimate remained robust to extensive confounder adjustment, with an expected loss of precision. Further, some registered NSBB users may in fact not have taken their NSBB which would lead to underestimation of the benefit of NSBB. Additionally, when using increasingly narrow definitions of sepsis to reflect “sepsis possibly attributable to bacterial translocation from the GI tract”, the association remained with an anticipated loss of precision. We did not find a dose–response relationship between NSBB dose and sepsis risk, which was expected, as the NSBB effect on portal pressure is reported to not be dose-dependent.17 However, when analyzing associations between sepsis and NSBB dose, we were not able to assess titration of NSBB. Consequently, we cannot disentangle if NSBB dosage reflects different treatment intensities or simply differences in concentration needed to obtain a similar response. Therefore, while we did not find a dose–response relationship dependent on absolute dose of NSBB, a relationship may still exist based on treatment response. History of infections and of immune deficiencies are potential confounders that we could not adjust for, but there is no reason to expect that these conditions were skewed between the groups.
Some limitations of the current study warrant mentioning. The study protocol did not specify a sepsis definition, therefore, sepsis was diagnosed according to usual clinical practice. Further, we did not have data to calculate the Sequential Organ Failure Assessment score (SOFA-score). However, all diagnoses were given by trained specialists, we stratified our regression analyses on geographical region, and the estimates were unaffected in our sensitivity analysis after applying a stricter sepsis definition (sepsis diagnosis and antibiotic prescription). Even so, we cannot rule out that geographical variation in guidelines or clinical practice may have influenced our estimates.
The proposed mechanism for a protective effect of NSBB against sepsis should apply equally to SBP, as has been suggested.18 Further support of the proposed mechanism can therefore be found in a case–control study of 2165 patients with cirrhosis, which found that patients not using NSBB had higher rate of hospitalization for SBP (odds ratio: 4.2 [95% CI 1.6–11.0]).19
Use of NSBB in patients with refractory ascites has been heavily debated, and we found that estimates on current NSBB use and sepsis were comparable with those of the entire cohort.
The suggested mode of action of NSBBs on sepsis risk is via their effect in lowering the portal pressure, but up to 59% of cirrhosis patients are hemodynamic non-responders to NSBB.20 It is likely that the effect of NSBBs on preventing sepsis is even stronger in those identified as hemodynamic responders to NSBBs. Further, because the proposed pharmacodynamic mechanism is still the same today, it does not undermine the validity of our findings that data were collected more than a decade ago.
Clinical trials of NSBBs to prevent cirrhotic decompensation in patients with clinically significant portal hypertension showed that NSBBs reduce the risk of decompensation and that the effect is mainly mediated through an effect on portal hypertension;21,22 our findings may provide further arguments in favor of NSBB treatment in patients with cirrhosis and ascites.
Conclusions
In conclusion, NSBB treatment on clinical indication seems to provide a meaningful reduction in the risk of sepsis among patients with cirrhosis and ascites. While the risk estimate did not maintain statistical significance, it remained most compatible with a protective effect of NSBB use after extensive confounder adjustment and in multiple sensitivity analyses. We take this to mean that the protective effect was truly present while its estimate became less precise by the analyses. However, to obtain more precise estimates, studies with more patients or longer follow-up are needed.
Abbreviations
NSBB, non-selective beta-blocker; SBP, spontaneous bacterial peritonitis; TIPS, transjugular intrahepatic portosystemic shunt; HE, hepatic encephalopathy; INR, international normalized ratio; HCC, hepatocellular carcinoma; MELD, model for end-stage liver disease; PPI, proton pump inhibitor; HR, hazard rate ratio; GI, gastrointestinal; SOFA-score, Sequential Organ Failure Assessment score; HVPG, hepatic venous pressure gradient.
Data Sharing Statement
Data are available upon reasonable request.
Ethics and Consent Statement
This project, where data from an ethical committee-approved project were used, did not require a new approval from an ethics committee, according to Danish law. All data used complied with relevant data protection and privacy regulations.
Acknowledgment
The abstract of this paper was presented as an oral presentation at ‘AASLD: The Liver Meeting 2020’ with interim findings and was included in ‘The Best of The Liver Meeting’. The abstract was published in ‘Oral Abstracts’ in ‘Hepatology’: https://doi.org/10.1002/hep.31578.
Funding
The funding sources had no involvement in the writing of the article.
Disclosure
Hugh Watson is an employee of Evotec and holds shares in Sanofi. No other conflicts of interest to declare.
References
1. Arvaniti V, D’Amico G, Fede G, et al. Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology. 2010;139(4):1246. doi:10.1053/j.gastro.2010.06.019
2. Assimakopoulos SF, Tsamandas AC, Tsiaoussis GI, et al. Altered intestinal tight junctions’ expression in patients with liver cirrhosis: a pathogenetic mechanism of intestinal hyperpermeability. Eur J Clin Invest. 2012;42(4):439–446. doi:10.1111/j.1365-2362.2011.02609.x
3. Xu WH, Wu XJ, Li JS. Influence of portal pressure change on intestinal permeability in patients with portal hypertension. Hepatobiliary Pancreat Dis Int. 2002;1:510–514.
4. Madsen BS, Havelund T, Krag A. Targeting the gut–liver axis in cirrhosis: antibiotics and non-selective β-blockers. Adv Ther. 2013;30:659–670. doi:10.1007/s12325-013-0044-1
5. Reiberger T, Ferlitsch A, Payer BA, et al. Non-selective betablocker therapy decreases intestinal permeability and serum levels of LBP and IL-6 in patients with cirrhosis. J Hepatol. 2013;58(5):911–921. doi:10.1016/j.jhep.2012.12.011
6. Merli M, Lucidi C, Di Gregorio V, et al. The chronic use of beta-blockers and proton pump inhibitors may affect the rate of bacterial infections in cirrhosis. Liver Int. 2015;35(2):362–369. doi:10.1111/liv.12593
7. Wong F, Watson H, Gerbes A, et al. Satavaptan for the management of ascites in cirrhosis: efficacy and safety across the spectrum of ascites severity. Gut. 2012;61(1):108–116. doi:10.1136/gutjnl-2011-300157
8. Jepsen P, Watson H, Andersen PK, Vilstrup H. Diabetes as a risk factor for hepatic encephalopathy in cirrhosis patients. J Hepatol. 2015;63(5):1133–1138. doi:10.1016/j.jhep.2015.07.007
9. United_Network_for_Organ_Sharing. Changes to OPTN bylaws and policies from actions at OPTN/UNOS executive committee meetings July 2015-November 2015; 2015.
10. Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit Care Med. 2003;31(4):1250–1256. doi:10.1097/01.CCM.0000050454.01978.3B
11. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:1644–1655. doi:10.1378/chest.101.6.1644
12. Bossen L, Krag A, Vilstrup H, Watson H, Jepsen P. Nonselective β-blockers do not affect mortality in cirrhosis patients with ascites: post Hoc analysis of three randomized controlled trials with 1198 patients. Hepatology. 2016;63(6):1968–1976. doi:10.1002/hep.28352
13. Datta S, Satten GA. Estimation of integrated transition hazards and stage occupation probabilities for non‐Markov systems under dependent censoring. Biometrics. 2002;58:792–802. doi:10.1111/j.0006-341X.2002.00792.x
14. Sanne JW. Willems PDAWvdV. inverse probability censoring weights for routine outcome monitoring data; 2014.
15. Chesnaye NC, Stel VS, Tripepi G, et al. An introduction to inverse probability of treatment weighting in observational research. Clin Kidney J. 2021;15:14–20. doi:10.1093/ckj/sfab158
16. Mookerjee RP, Pavesi M, Thomsen KL, et al. Treatment with non-selective beta blockers is associated with reduced severity of systemic inflammation and improved survival of patients with acute-on-chronic liver failure. J Hepatol. 2016;64:574–582. doi:10.1016/j.jhep.2015.10.018
17. Rodrigues SG, Mendoza YP, Bosch J. Beta-blockers in cirrhosis: evidence-based indications and limitations. JHEP Rep. 2020;2:100063. doi:10.1016/j.jhepr.2019.12.001
18. Sundaram V, Manne V, Al-Osaimi AM. Ascites and spontaneous bacterial peritonitis: recommendations from two United States centers. Saudi J Gastroenterol. 2014;20:279–287. doi:10.4103/1319-3767.141686
19. Sasso R, Rockey DC. Non-selective beta-blocker use in cirrhotic patients is associated with a reduced likelihood of hospitalisation for infection. Aliment Pharmacol Ther. 2021;53:418–425. doi:10.1111/apt.16156
20. Heebøll S, Villadsen GE, Aagaard NK, Grønbæk H, Vilstrup H, Keiding S. Propranolol treatment of portal hypertension in cirrhosis patients is better the higher the untreated pressure: a single-centre prospective experience. Scand J Gastroenterol. 2013;48:969–973. doi:10.3109/00365521.2013.805811
21. Villanueva C, Albillos A, Genescà J, et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2019;393(10181):1597–1608. doi:10.1016/S0140-6736(18)31875-0
22. Villanueva C, Torres F, Sarin SK, et al. Carvedilol reduces the risk of decompensation and mortality in patients with compensated cirrhosis in a competing-risk meta-analysis. J Hepatol. 2022;77(4):1014–1025. doi:10.1016/j.jhep.2022.05.021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.