Back to Journals » International Journal of General Medicine » Volume 17
Nomogram to Predict Outcomes After Staged Revascularization in ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
Received 29 December 2023
Accepted for publication 20 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1713—1722
DOI https://doi.org/10.2147/IJGM.S457236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Redoy Ranjan
Huaigen Wang,1 Aiqun Ma,1,2 Tingzhong Wang1,2
1Department of Cardiovascular Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Shaanxi Key Laboratory of Molecular Cardiology (Xi’an Jiaotong University), Xi’an, Shaanxi, People’s Republic of China
Correspondence: Aiqun Ma; Tingzhong Wang, Email [email protected]; [email protected]
Objective: Approximately 50% of ST-segment elevation myocardial infarction (STEMI) patients have multivessel coronary artery disease (MVD). The management strategy for these patients remains controversial. This study aimed to develop predictive models and nomogram of outcomes in STEMI patients with MVD for better identification and classification.
Methods: The least absolute shrinkage and selection operator (LASSO) method was used to select the features most significantly associated with the outcomes. A Cox regression model was built using the selected variables. One nomogram was computed from each model, and individual risk scores were obtained by applying the nomograms to the cohort. After regrouping patients based on nomogram risk scores into low- and high-risk groups, we used the Kaplan–Meier method to perform survival analysis.
Results: The C-index of the major adverse cardiovascular event (MACE)-free survival model was 0· 68 (95% CI 0· 62– 0· 74) and 0· 65 [0· 62– 0· 68]) at internal validation, and that of the overall survival model was 0· 75 (95% CI 0· 66– 0· 84) and (0· 73 [0· 65– 0· 81]). The predictions of both models correlated with the observed outcomes. Low-risk patients had significantly lower probabilities of 1-year or 3-year MACEs (4% versus 11%, P= 0.003; 7% versus 15%, P=0.01, respectively) and 1-year or 3-year all-cause death (1% versus 3%, P=0.048; 2% versus 7%, respectively, P=0.001) than high-risk patients.
Conclusion: Our nomograms can be used to predict STEMI and MVD outcomes in a simple and practical way for patients who undergo primary PCI for culprit vessels and staged PCI for non-culprit vessels.
Keywords: ST-segment elevation myocardial infarction, multivessel coronary artery disease, percutaneous coronary intervention, major adverse cardiovascular events, all-cause death
Introduction
Acute coronary syndrome (ACS) is a common critical cardiovascular disease and a leading cause of death worldwide.1,2 ST-segment elevation myocardial infarction (STEMI) accounts for ~36% of ACS cases.3 STEMI is defined as a combination of persistent ST-segment elevation on electrocardiogram and the subsequent release of biomarkers of myocardial necrosis.4 Previous studies have shown that approximately half of STEMI patients have multivessel coronary artery disease (MVD). MVD increases the risk of recurrence and short-term death after percutaneous coronary intervention (PCI) and is an important cause of poor prognosis in STEMI patients.5,6
The first-line treatment for STEMI patients is timely primary PCI (PPCI) for culprit vessels.4 However, the presence of non-culprit vessels makes the treatment more complicated for patients with MVD. The management strategy and its impact on patient prognosis for non-culprit vessels are still controversial. The COMPLETE trial confirmed that complete revascularization was superior to culprit-lesion-only PCI in patients with STEMI and MVD.7 However, intervention strategies for non-culprit vessels, such as the optimal timing of intervention, are not very consistent. Previous retrospective studies reported inconsistent results due to the enrollment of different populations and different sample sizes.8–10 This suggests that this population is highly heterogeneous, and further assessment and classification are needed.
Therefore, this study aimed to develop predictive models of major adverse cardiovascular events (MACEs) and all-cause mortality in patients with STEMI combined with MVD to better identify and classify these patients.
Methods
Study Design and Participants
We conducted a retrospective investigation. Nomograms were developed to predict outcomes after staged revascularization (SR) in acute STEMI and MVD patients using data from the First Affiliated Hospital of Xi’an Jiaotong University. All patients met the diagnostic criteria for acute STEMI. They all underwent PPCI for culprit vessels and staged PCI for non-culprit vessels. The exclusion criteria were as follows: (1) STEMI without PPCI or staged PCI and (2) acute non-STEMI or unstable angina. This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of First Affiliated Hospital of Xi’an Jiaotong University. The informed consent was gained from the patients and their families.
Data Collection
General data (age, sex, body mass index (BMI), and smoking), medical history (including coronary heart disease, history of hypertension, type 2 diabetes mellitus, myocardial infarction, and coronary intervention), vital signs at admission (body temperature, pulse, respiratory rate, blood pressure), auxiliary examinations (white blood cell count, neutrophil count, red blood cell count, hemoglobin, platelet count, serum creatinine, uric acid, cholesterol, triglycerides (TG), low-density lipoprotein (LDL-C), high-density lipoprotein (HDL-C), creatine kinase (CK) and creatine kinase MB (CK-MB) peak, N-terminal pro b-type natriuretic peptide (NT-proBNP), left ventricular end-diastolic diameter (LDVd) and left ventricular ejection fraction (LVEF)), and estimated glomerular filtration rate (eGFR) calculated using the Modification of Diet in Renal Disease (MDRD) formula were recorded. Chest pain data, interventions (culprit vessels, location, diameter, length, number of vessels with lesions, treatment of non-culprit vessels or not, preoperative Thrombolysis in Myocardial Infarction (TIMI) flow, grading of postoperative TIMI flow, and intra-aortic balloon pump (IABP)), stents (most of the stents used in this study were drug-coated stents), medications (β-blocker, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB), aldosterone, diuretic, calcium channel blocker or no medication during the three months before admission), and administration of the above medications after admission were also collected from the medical charts.
Definitions
In-hospital mortality was defined as all-cause mortality during hospitalization. Chest pain data included symptom-to-door time and first medical contact time. The time of chest pain onset was obtained by asking the patient and consulting the family accompanying the patient. After admission, ECG and blood sampling were performed within 10 minutes. The self-reported chest pain onset time was validated according to the presence or absence of a Q wave, the dynamic evolution of ST-T, and whether blood myoglobin and CK-MB levels were elevated. MACEs were defined as cardiac death, recurrent myocardial infarction, revascularization or stroke.11
Statistical Analysis
The sample size was derived based on the available data, and no power calculation for sample size was performed upfront. Descriptive statistics are reported as frequencies and proportions for categorical variables and as medians (IQRs) or means (SDs) for continuous variables.
The least absolute shrinkage and selection operator (LASSO) method was used to select the features that were most significantly associated with the outcomes (MACEs and all-cause mortality). Then, Cox regression models were built using the selected variables.12,13 Cox regression analyses were applied to estimate the hazard ratios (HRs) or odds ratios and their 95% CIs or P values. The prediction accuracy of overall survival and MACE-free survival models was evaluated using two methods. First, discrimination was measured by Harrell’s concordance index (C-index) and its 95% CI. Second, model calibration was evaluated by calibration plots predicting the survival probability at 1 and 3 years versus the observed probability. One nomogram was computed from each model, and individual risk scores were obtained by applying the nomograms to the cohort. Then, the median of the nomogram-computed individual risk scores was taken as the cutoff point to stratify patients into low-risk or high-risk groups. Differences in overall survival and MACE-free survival between the low-risk and high-risk cohorts were determined using the Log rank test. The Kaplan–Meier (K-M) method was used for survival analysis. The distribution of putative variables between the low-risk and high-risk cohorts was compared using the Wilcoxon Mann–Whitney test (for continuous variables) or Fisher’s exact test (for categorical variables).
Internal validation of the model was performed using a bootstrap resampling process to provide an unbiased estimate of model performance (validate.cph package in R) as the C-index and its 95% CI. All statistical analyses were performed using R version 4.1.1(Vienna, Austria).
Results
Baseline Clinical Characteristics of the Two Groups
Between January 1, 2015, and December 31, 2020, 3256 patients were retrospectively screened, and 496 (15%) of them met the eligibility criteria. A total of 2760 (85%) patients were excluded: 1189 (37%) did not undergo primary PCI, 692 (21%) had single-vessel disease, 795 (29%) did not undergo staged revascularization for non-culprit vessels within 30 days after PPCI, 21 (0.6%) died during hospitalization or had cancer, and 42 (1.3%) were lost to follow-up (Figure 1). The median follow-up time was 39 (IQR 21, 59) months. Baseline characteristic data were well balanced between the two groups except for sex, age, BMI, history of smoking and hypertension, SR time, NT-proBNP and eGFR (Table 1). During the follow-up, MACEs occurred in 68 (14%) patients, and 34 (7%) patients died in the total study cohort. Postdischarge medication use was similar between the high-risk and low-risk groups (Table 2).
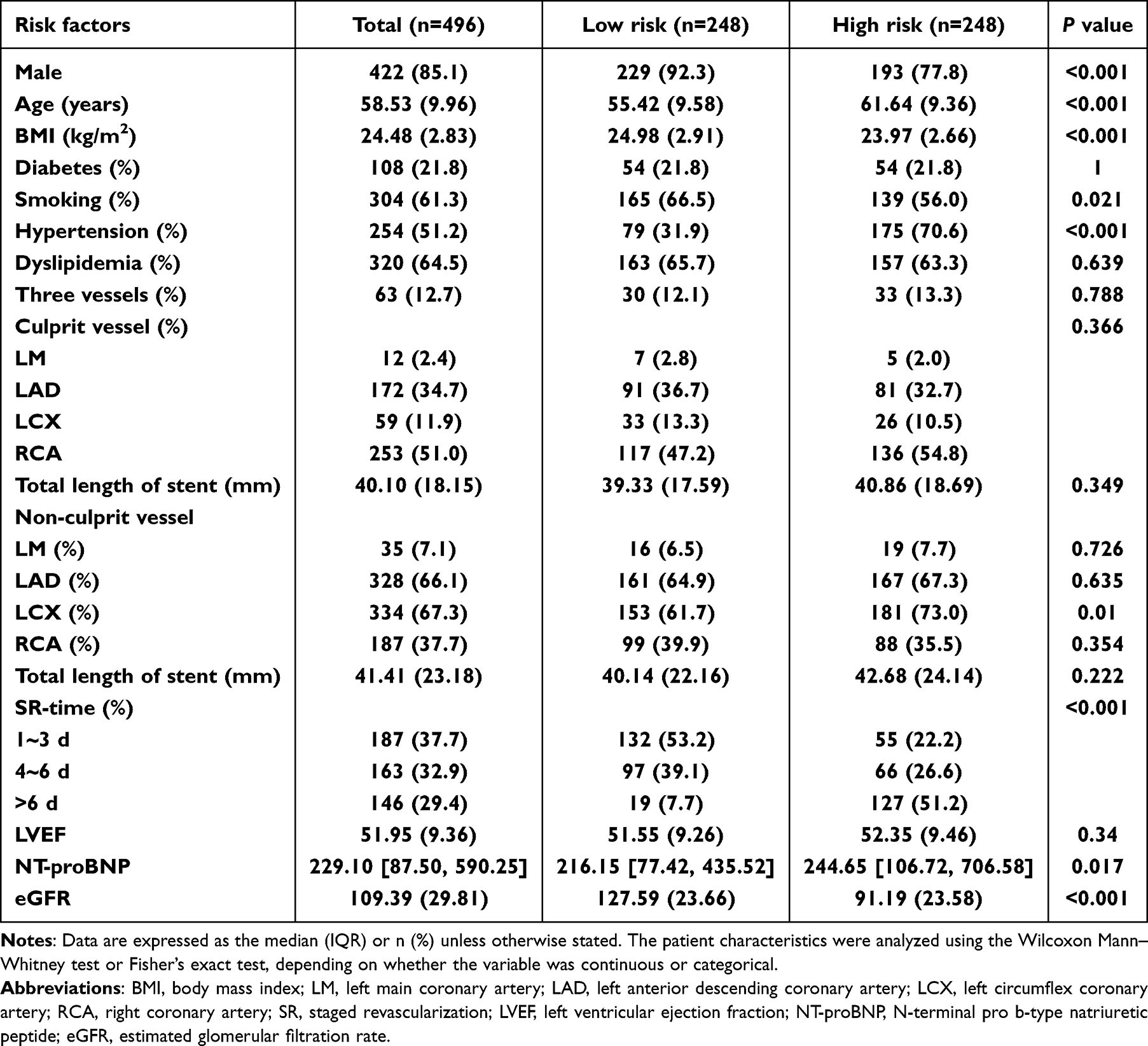 |
Table 1 Baseline Characteristics of the Study Cohort |
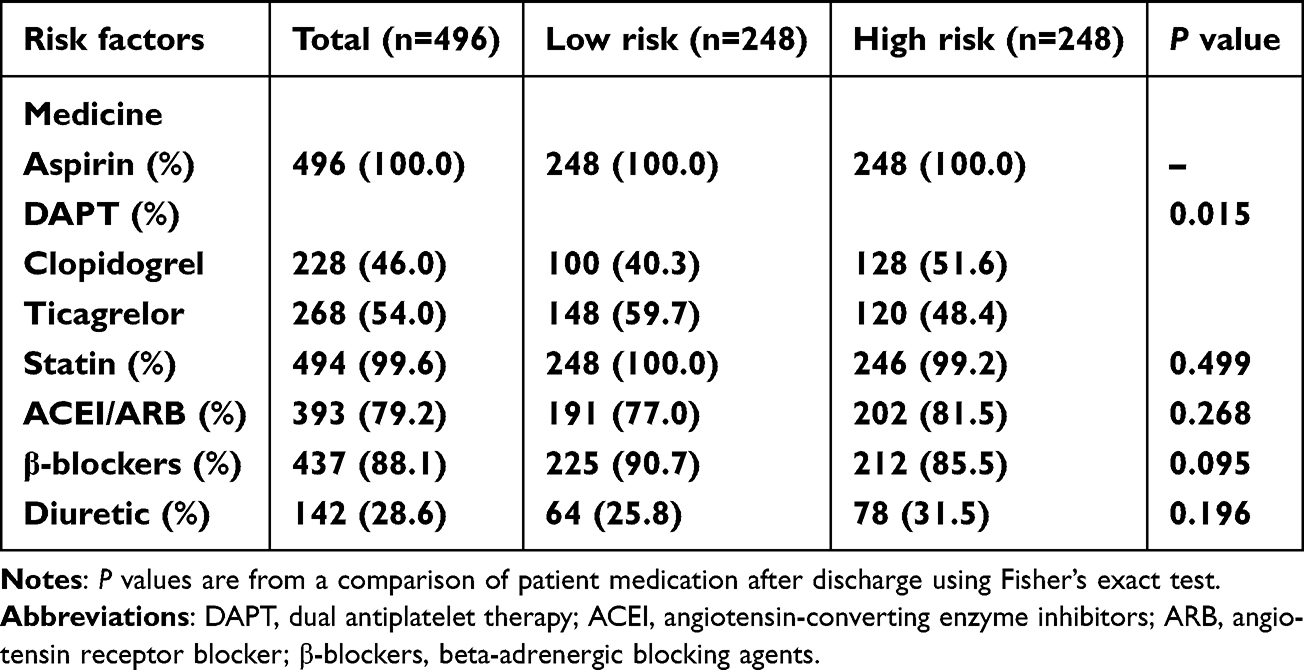 |
Table 2 Medication After Discharge |
 |
Figure 1 Study population flow chart. Abbreviations: STEMI, ST-segment elevation myocardial infarction; MVD, multivessel coronary artery disease; PCI, percutaneous coronary intervention; SCR, staged complete revascularization. |
Cox Regression Analysis of MACEs and All-Cause Death
Based on the LASSO analysis, eGFR, age, history of hypertension and SR time were selected as predictors for the MACE risk prediction model (Table 3). eGFR, age and chronic total occlusion (CTO) were selected as predictors for the MACE risk prediction model (Table 4).
 |
Table 3 The Characteristics of the Variables in the MACE Prediction Model |
 |
Table 4 The Characteristics of the Variables in the All-Death Prediction Model |
Development and Validation of Nomograms for Predicting MACE Risk and All-Cause Death Risk
The C-index of the MACE-free survival model was 0·68 (95% CI 0·62–0·74) and 0·65 [0·62–0·68] at internal validation. The nomogram was built based on the MACE-free survival model (Figure 2C). On the calibration plots, the model’s predicted probabilities were close to the observed probabilities (Figure 2A and B).
 |
Figure 2 MACE-free survival probabilities. Calibration plots of MACE-free survival probabilities at 1 year (A) and 3 years (B). Nomogram-predicted MACE-free survival is plotted on the x-axis, with observed MACE-free survival on the y-axis. Dashed lines along the diagonal line through the origin point represent the perfect calibration models in which the predicted probabilities are identical to the observed probabilities. (C) Nomogram for predicting the probability of MACE-free survival at 1 year and 3 years. The presence or absence of each clinical characteristic indicates a certain number of points. The number of points for each clinical characteristic is in the top row. For each characteristic, absence is assigned 0 points. The presence of characteristics is associated with a number of points generated using the nomogram function rms package in R based on the results of LASSO analysis. The points for each characteristic are summed to generate a total-points score. The total points correspond to the respective 1-year and 3-year MACE-free survival probabilities. Abbreviations: MACE, major adverse cardiovascular event; eGFR, estimated glomerular filtration rate; SR, staged revascularization. |
The C-index of the overall survival model was 0·75 (95% CI 0·66–0·84). Similar C-index was achieved at internal validation (0·73 [0·65–0·81]). The nomogram was built based on the overall survival model (Figure 3C). On the calibration plots, the model’s predicted probabilities were close to the observed probabilities (Figure 3A and B).
 |
Figure 3 Total survival probabilities. Calibration plots of total survival probabilities at 1 year (A) and 3 years (B). Nomogram-predicted total survival is plotted on the x-axis, with observed total survival on the y-axis. Dashed lines along the diagonal line through the origin point represent the perfect calibration models in which the predicted probabilities are identical to the observed probabilities. (C) Nomogram for predicting the probability of total survival at 1 year and 3 years. The presence or absence of each clinical characteristic indicates a certain number of points. The number of points for each clinical characteristic is in the top row. For each characteristic, absence is assigned 0 points. The presence of characteristics is associated with a number of points generated using the nomogram function rms package in R based on the results of LASSO analysis. The points for each characteristic are summed to generate a total-points score. The total points correspond to the respective 1-year and 3-year total survival probabilities. Abbreviations: eGFR, estimated glomerular filtration rate; CTO, chronic total occlusion. |
K-M Analysis
In the first model, the MACEs probability in the low-risk group was lower than that in the high-risk group (P<0.001). The 1-year MACEs probability for low-risk patients versus high-risk patients was 4% versus 11% (P= 0.003), and the 3-year MACEs probability was 6% versus 15% (P=0.01) (Figure 4A).
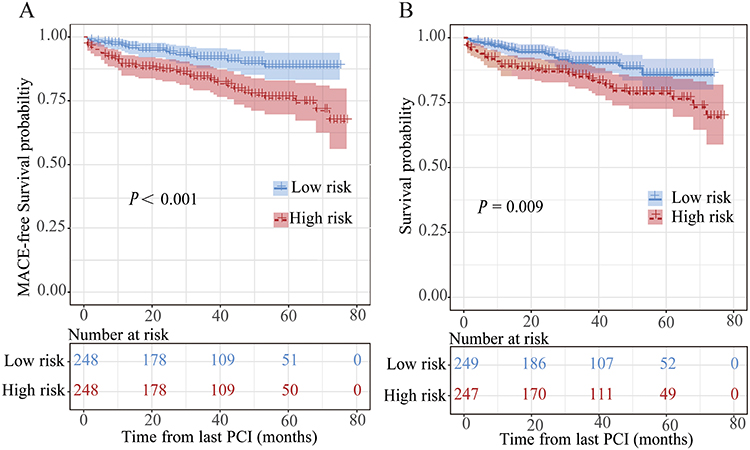 |
Figure 4 Survival curves by different risk groups. MACE-free survival curves (A) and overall survival curves (B), stratified into low-risk and high-risk groups by the median of the risk scores from the nomograms above. Abbreviations: MACE, major adverse cardiovascular event; PCI, percutaneous coronary intervention. |
In the second model, the all-cause death probability in the low-risk group was also lower than that in the high-risk group (P=0.009). The 1-year all-cause mortality for low-risk patients versus high-risk patients was 1% versus 3% (P=0.048), and the 3-year death probability was 2% versus 7% (P=0.001) (Figure 4B).
Discussion
It is a widely accepted fact that STEMI patients with MVD are at high risk. Management strategies for these patients, especially regarding intervention time in non-culprit vessels, remain controversial.14 We developed prediction models for MACEs and all-cause mortality based on several clinical indicators with promising accuracy (the C-index values were 0.68 and 0.75), allowing easier classification of such patients and identification of those at high risk.
Several previous studies have established nomograms for predicting different outcomes in patients with ACS undergoing PCI.15–17 However, these models are relatively complex, and there is currently no prediction model specifically tailored for STEMI patients with MVD. Our nomograms for MACE-free and overall survival combine traditional clinical prognostic variables (ie, age, history of hypertension), laboratory test results, characteristics of coronary vascular disease (CTO) and treatment strategy (SR time). Both nomograms support previous studies and suggest that eGFR is an independent predictor of outcomes in STEMI patients with or without MVD treated with PCI.18,19 Go AS et al found that the risk of all-cause mortality from cardiovascular adverse events (coronary heart disease, acute myocardial infarction, heart failure, and stroke) increased with the interval decrease in eGFR in a large-scale epidemiological study.20 Most patients with STEMI and MVD require multiple PCI procedures with more contrast agents, implying a higher risk of contrast-induced nephropathy. Clinically, we should be more vigilant and closely monitor renal function.
Complete revascularization of non-culprit vessels can significantly improve the prognosis of STEMI in MVD patients,7,21,22 although strategies for intervention in non-culprit vessels are still under investigation. Prior research indicates that utilizing fractional flow reserve (FFR) and intravascular imaging to guide interventions in non-culprit vessels may benefit such patients.23–25 A randomized clinical study by Lee et al found that compared to the traditional strategy of PCI based on angiographic diameter stenosis, a selective PCI strategy guided by FFR decision-making reduced the risk of death, myocardial infarction, or repeat revascularization in patients with AMI and MVD.25 In addition to preventive revascularization, comprehensive management approaches including adequate antiplatelet therapy, and the use of plaque-stabilizing medications (such as PCSK9 inhibitors and statins) are essential to further improve the prognosis of these patients.
The optimum timing of the revascularization strategy for non-culprit vessels in STEMI and MVD remains unclear. The results of previous studies investigating the optimum strategy for non-culprit vessels are also inconsistent due to differences in sample size, selection criteria, research methods, intervention timing, and intervention criteria. However, most of them suggest that early intervention (the best time point obtained by each study is different) of non-culprit vessels may benefit such patients’ prognosis.8,26 Our nomograms show that delayed intervention in non-culprit vessels may be detrimental to the prognosis of patients, but the optimal timing and strategy require further study in well-designed randomized controlled clinical trials. In patients with STEMI, the prevalence of CTO in a non–infarct-related artery (non-IRA) is 8% to 15%, with 2-fold greater morbidity and mortality than in those with single-vessel disease.27,28 We also found that CTO was a predictor of all-cause mortality.
This study has important clinical implications. STEMI and MVD patients experienced more MACEs and higher mortality than STEMI patients with single-vessel lesions.29,30 MVD is an essential factor in the poor prognosis of these patients and can significantly increase recurrence of myocardial infarction and short-term mortality after PCI.6,31 The COMPLETE trial demonstrated that, on a background of optimal medical therapy, compared with a culprit lesion-only revascularization strategy, a complete revascularization strategy can significantly reduce the risk of cardiovascular death or myocardial infarction, as well as the risk of cardiovascular death, myocardial infarction, or ischemia-driven revascularization.7 However, even complete revascularization has been performed, these patients still have a high rate of mortality and MACEs. This may be partly because most of these patients have comorbidities, such as advanced age, diabetes, hypertension and chronic kidney disease.32 Early identification and classification of those at risk among them and individualized management may improve the prognosis of this group of patients, but there is a lack of rapid and straightforward clinical methods for identifying and classifying these patients. Our study provides a preliminary tool to help clinicians make decisions and manage these patients in their clinical work.
The major limitations of this study are the small size of the cohort and the absence of a prospective external validation of the models. Although the recommended number of at least ten events per predictor variable was followed,33 validation of the models in larger patient populations is warranted. Second, this study was a single-center, retrospective, observational study with selection bias to adequately assess the impact of confounding factors on the study results. The prognostic discrimination (C-index: 0·68 for the MACE-free survival model and 0·75 for the overall survival model) was not ideal. The addition of other parameters to a larger patient population might increase the prognostic discrimination. Last, we did not adequately assess the severity of patients’ coronary lesions, such as applying the Gensini score or SYNTAX score to evaluate the severity of coronary artery lesions. The Gensini score and SYNTAX score are significantly associated with the prognosis of patients.
In summary, our study established two predictive nomograms based on four or three variables with promising discrimination to help clinicians predict the risk of MACEs and all-cause death in STEMI patients with MVD who underwent primary PCI for culprit vessels and staged PCI for non-culprit vessels. Use of the nomograms helps to manage these patients more precisely and personalize their treatment in the clinic.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. We thank AJE language editing services for English language editing.
Funding
This work was supported by the National Key Research and Development Program (2017YFC1308302) and the Science and Technology Program for Public Wellbeing of China (2012GS610101) and the Fundamental Research Funds for the Central Universities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sanchis-Gomar F, Perez-Quilis C, Leischik R, et al. Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 2016;4(13):256. doi:10.21037/atm.2016.06.33
2. Zhao D, Liu J, Wang M, et al. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16(4):203–212. doi:10.1038/s41569-018-0119-4
3. Steg PG, Goldberg RJ, Gore JM, et al. Baseline characteristics, management practices, and in-hospital outcomes of patients hospitalized with acute coronary syndromes in the Global Registry of Acute Coronary Events (GRACE). Am J Cardiol. 2002;90(4):358–363. doi:10.1016/s0002-9149(02)02489-x
4. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
5. Park D-W, Clare RM, Schulte PJ, et al. Extent, location, and clinical significance of non–infarct-related coronary artery disease among patients with ST-elevation myocardial infarction. JAMA. 2014;312(19):2019–2027. doi:10.1001/jama.2014.15095
6. Jang J-S, Spertus JA, Arnold SV, et al. Impact of multivessel revascularization on health status outcomes in patients with ST-segment elevation myocardial infarction and multivessel coronary artery disease. J Am Coll Cardiol. 2015;66(19):2104–2113. doi:10.1016/j.jacc.2015.08.873
7. Mehta SR, Wood DA, Storey RF, et al. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381(15):1411–1421. doi:10.1056/NEJMoa1907775
8. Hannan EL, Samadashvili Z, Walford G, et al. Culprit vessel percutaneous coronary intervention versus multivessel and staged percutaneous coronary intervention for ST-segment elevation myocardial infarction patients with multivessel disease. JACC: Cardiovasc Interv. 2010;3(1):22–31. doi:10.1016/j.jcin.2009.10.017
9. Lee W-C, Wu B-J, Fang C-Y, et al. Timing of staged percutaneous coronary intervention for a non-culprit lesion in patients with anterior wall ST segment elevation myocardial infarction with multiple vessel disease. Int Heart J. 2016:15–402. doi:10.1536/ihj.15-402
10. Zhao XD, Zhao GQ, Wang X, et al. Optimal timing of staged percutaneous coronary intervention in ST-segment elevation myocardial infarction patients with multivessel disease. J Geriatr Cardiol. 2018;15(5):356. doi:10.11909/j.issn.1671-5411.2018.05.005
11. Kip Kevin E, Hollabaugh K, Marroquin Oscar C, et al. The problem with composite end points in cardiovascular studies. J Am Coll Cardiol. 2008;51(7):701–707. doi:10.1016/j.jacc.2007.10.034
12. Zhang HH, Lu W. Adaptive Lasso for Cox’s proportional hazards model. Biometrika. 2007;94(3):691–703. doi:10.1093/biomet/asm037
13. Tibshirani R. The lasso method for variable selection in the Cox model. Stat Med. 1997;16(4):385–395. doi:10.1002/(sici)1097-0258(19970228)16:4<385::aid-sim380>3.0.co;2-3
14. D’Amico G, Basile M, Tarantini G, et al. Revascularization strategies in STEMI with multivessel disease: when and how. Minerva Cardioangiol. 2018;66(4):429–441. doi:10.23736/s0026-4725.18.04646-7
15. Xiao S, Zhang L, Wu Q, et al. Development and validation of a risk nomogram model for predicting revascularization after percutaneous coronary intervention in patients with acute coronary syndrome. Clin Interv Aging. 2021;16:1541–1553. doi:10.2147/cia.S325385
16. He W, Xu C, Wang X, et al. Development and validation of a risk prediction nomogram for in-stent restenosis in patients undergoing percutaneous coronary intervention. BMC Cardiovasc Disord. 2021;21(1):435. doi:10.1186/s12872-021-02255-4
17. Gao N, Qi X, Dang Y, et al. Establishment and validation of a risk model for prediction of in-hospital mortality in patients with acute ST-elevation myocardial infarction after primary PCI. BMC Cardiovasc Disord. 2020;20(1):513. doi:10.1186/s12872-020-01804-7
18. Polanska-Skrzypczyk M, Karcz M, Bekta P, et al. Prognostic value of renal function in STEMI patients treated with primary PCI: ANIN Registry. Br J Cardiol. 2013;20(65). doi:10.5837/bjc.2013.17
19. Han X, Bai L, Jeong MH, et al. Long-term clinical outcome according to changes of glomerular filtration rate in AMI patients with multivessel disease after percutaneous coronary intervention. Chonnam Med J. 2020;56(2):121. doi:10.4068/cmj.2020.56.2.121
20. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. doi:10.1056/NEJMoa041031
21. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med. 2013;369(12):1115–1123. doi:10.1056/NEJMoa1305520
22. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol. 2015;65(10):963–972. doi:10.1016/j.jacc.2014.12.038
23. Choi KH, Song YB, Lee JM, et al. Impact of intravascular ultrasound-guided percutaneous coronary intervention on long-term clinical outcomes in patients undergoing complex procedures. JACC: Cardiovasc Interv. 2019;12(7):607–620. doi:10.1016/j.jcin.2019.01.227
24. Yamamoto K, Shiomi H, Morimoto T, et al. Single-session versus staged multivessel optimal IVUS-Guided PCI in patients with CCS or NSTE-ACS. JACC Asia. 2023;3(4):649–661. doi:10.1016/j.jacasi.2023.03.013
25. Lee JM, Kim HK, Park KH, et al. Fractional flow reserve versus angiography-guided strategy in acute myocardial infarction with multivessel disease: a randomized trial. Eur Heart J. 2023;44(6):473–484. doi:10.1093/eurheartj/ehac763
26. Arnold JH, Bental T, Greenberg G, et al. Timing of nonculprit percutaneous coronary Intervention after ST-elevation myocardial infarction. Cardiology. 2021;146(5):556–565. doi:10.1159/000517295
27. Claessen BE, Dangas GD, Weisz G, et al. Prognostic impact of a chronic total occlusion in a non-infarct-related artery in patients with ST-segment elevation myocardial infarction: 3-year results from the HORIZONS-AMI trial. Eur Heart J. 2012;33(6):768–775. doi:10.1093/eurheartj/ehr471
28. Allahwala UK, Jolly SS, Dzavik V, et al. The presence of a CTO in a non-infarct-related artery during a STEMI treated with contemporary primary PCI is associated with increased rates of early and late cardiovascular morbidity and mortality the CTO-TOTAL substudy. Letter. JACC: Cardiovasc Interv. 2018;11(7):709–711. doi:10.1016/j.jcin.2017.12.005
29. Entezarjou A, Mohammad MA, Andell P, et al. Culprit vessel: impact on short-term and long-term prognosis in patients with ST-elevation myocardial infarction. Open Heart. 2018;5(2):e000852–e000852. doi:10.1136/openhrt-2018-000852
30. Baumann AAW, Mishra A, Worthley MI, et al. Management of multivessel coronary artery disease in patients with non-ST-elevation myocardial infarction: a complex path to precision medicine. Ther Adv Chronic Dis. 2020;11:2040622320938527. doi:10.1177/2040622320938527
31. Ryu KS, Bae JW, Jeong MH, Cho MC, Ryu KH. Risk scoring system for prognosis estimation of multivessel disease among patients with ST-segment elevation myocardial infarction. Int Heart J. 2019;60(3):708–714. doi:10.1536/ihj.17-337
32. Burgess S, Juergens CP, Yang W, et al. Cardiac mortality, diabetes mellitus, and multivessel disease in ST elevation myocardial infarction. Int J Cardiol. 2021;323:13–18. doi:10.1016/j.ijcard.2020.08.021
33. Peduzzi P, Concato J, Feinstein AR, et al. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48(12):1503–1510. doi:10.1016/0895-4356(95)00048-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preprocedural SII Combined with High-Sensitivity C-Reactive Protein Predicts the Risk of Contrast-Induced Acute Kidney Injury in STEMI Patients Undergoing Percutaneous Coronary Intervention
Ma K, Qiu H, Zhu Y, Lu Y, Li W
Journal of Inflammation Research 2022, 15:3677-3687
Published Date: 25 June 2022
Relation of Red Cell Distribution Width to Glucose Metabolism and Adverse Long-Term Prognosis in Patients with Acute Coronary Syndrome
Xiong K, Xu C, Shou X, Dong M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:61-70
Published Date: 11 January 2023
A Predictive Model for Contrast-Induced Acute Kidney Injury After Percutaneous Coronary Intervention in Elderly Patients with ST-Segment Elevation Myocardial Infarction
Qiu H, Zhu Y, Shen G, Wang Z, Li W
Clinical Interventions in Aging 2023, 18:453-465
Published Date: 22 March 2023
Development and Validation of Nomogram for the Prediction of Malignant Ventricular Arrhythmia Including Circulating Inflammatory Cells in Patients with Acute ST-Segment Elevation Myocardial Infarction
Wang L, Yang L, Li T, Geng S
Journal of Inflammation Research 2023, 16:3185-3196
Published Date: 27 July 2023
Association of Systemic Inflammatory Response Index and Pan-Immune-Inflammation-Value with Long-Term Adverse Cardiovascular Events in ST-Segment Elevation Myocardial Infarction Patients After Primary Percutaneous Coronary Intervention
Liu Y, Liu J, Liu L, Cao S, Jin T, Chen L, Wu G, Zong G
Journal of Inflammation Research 2023, 16:3437-3454
Published Date: 14 August 2023