Back to Journals » International Journal of General Medicine » Volume 16
Nomogram to Predict Cognitive Impairment in Patients with Asymptomatic Middle Cerebral Artery Stenosis
Authors Li J, Wang S, Li J, Fang Y, Wang Y, Zhang Y
Received 8 February 2023
Accepted for publication 29 March 2023
Published 15 April 2023 Volume 2023:16 Pages 1333—1343
DOI https://doi.org/10.2147/IJGM.S407728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jiayang Li, Shaoshuai Wang, Jun Li, Yalan Fang, Ying Wang, Yuanyuan Zhang
Department of Neurology, First Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China
Correspondence: Yuanyuan Zhang, Shanxi Medical University, No. 56 South Xinjian Road, Yingze District, Taiyuan, Shanxi Province, 03000, People’s Republic of China, Tel +8619834516348, Fax +863414867027, Email [email protected]
Purpose: This study aims to investigate the characteristics and influencing factors of cognitive impairment in patients with asymptomatic middle cerebral artery stenosis (aMCAS) and to construct a nomogram to predict the risk of cognitive impairment in patients with aMCAS.
Patients and Methods: We collected 54 patients with aMCAS and 35 healthy controls to investigate the impaired cognitive domains and pathogenesis in patients with aMCAS. All patients underwent a cranial MRI, CT perfusion, transcranial Doppler ultrasound, blood tests, and a comprehensive neuropsychological evaluation. According to the MoCA score, patients were divided into cognitively normal and cognitively impaired groups. To construct the nomogram, we conducted univariate and multivariate logistic regression analyses to identify factors that affect cognitive function. And the performance of nomogram was evaluated by ROC curves, calibration curves, decision curve analysis (DCA), and clinical impact curve (CIC).
Results: In 54 patients with aMCAS, 24 patients presented with cognitive normal, and 30 patients presented with cognitive impairment. The results of multivariate logistic regression suggested that perfusion decompensation, middle cerebral artery mean flow velocity, and LDL-cholesterol levels were independent influencing factors of cognitive impairment. In the following step, a nomogram was constructed. The AUC of the nomogram is 0.862. Calibrating curves show good agreement between nomogram predictions and actual observations, while DCA and CIC show great clinical usefulness.
Conclusion: Patients with aMCAS have cognitive impairment in multiple cognitive domains, and impaired executive function was observed during the perfusion compensation period. Furthermore, a nomogram was constructed and validated to predict the risk of cognitive impairment in patients with aMCAS, which can help clinicians to identify at an early stage and improve the management of patients.
Keywords: cognitive impairment, asymptomatic middle cerebral artery stenosis, nomogram, predictive model
Introduction
Intracranial atherosclerotic stenosis (ICAS) is one of the most common causes of stroke worldwide as well as a significant contributor to the risk of cognitive impairment.1,2 With the development of noninvasive imaging techniques, more and more patients can be diagnosed with asymptomatic ICAS before stroke or transient ischemic attack (TIA) occurs. Research has shown that the incidence of aICAS ranges from 5.9% to 24.5%. Moderate or above aICAS is associated with cognitive impairment, which affects the daily life and behavior of patients.3
Current research on aICAS is mainly focused on the carotid artery. Asymptomatic carotid artery stenosis (aCAS) is an independent risk factor for cognitive impairment,4 mainly manifested as impairment in visuospatial ability, processing speed, short-delay recall, long-delay recall, executive function, attention, and language.5–8 As an important branch of the carotid artery, the middle cerebral artery (MCA) mainly supplies blood to the front 2/3 of the dorsolateral of the cerebral hemisphere, including the frontal, parietal, temporal, and insular lobes. MCA stenosis may cause dysfunction in these brain areas and impair cognitive function. Current studies of cognitive impairment in patients with asymptomatic middle cerebral artery stenosis (aMCAS) focus on the impaired cognitive domains. However, fewer studies have investigated the mechanisms of cognitive impairment, and the model to predict cognitive impairment in patients with aMCAS has not been constructed.
Therefore, this study used the 60-min protocol recommended in vascular cognitive impairment harmonization criteria9 to comprehensively assess the cognitive function of patients with aMCAS. Additionally, CT perfusion (CTP) was used to assess the cerebral perfusion of patients, and transcranial Doppler ultrasound (TCD) was used to measure the blood flow velocity of MCA. We aimed to investigate the impaired cognitive domains and pathogenesis in patients with aMCAS, and constructed a nomogram for early recognition of cognitive impairment.
Materials and Methods
Participants
We collected 54 patients diagnosed with aMCAS admitted to the Department of Neurology of Shanxi Medical University First Hospital between July 2021 and November 2022. The inclusion criteria were: (1) patients with unilateral MCA stenosis of 50% or more as diagnosed by computed tomography angiography (CTA) or digital subtraction angiography (DSA), (2) stenosis caused by atherosclerosis and (3) patients can complete cognitive function tests independently. The exclusion criteria were: (1) stroke or TIA diagnosed by clinical and MRI, (2) stenosis of 50% or more in other large intracranial arteries (internal carotid artery, anterior cerebral artery, posterior cerebral artery, basilar artery, and vertebral artery), (3) intracranial vascular stenosis caused by other reasons (such as moyamoya disease, arteriovenous malformations, central nervous system (CNS) vasculitis, arterial dissection, cardiogenic embolism caused by atrial fibrillation, etc.), (4) cognitive impairment with other identifiable etiologies (such as Alzheimer’s disease, epilepsy, Parkinson’s disease, intracranial infections, mental illness, etc.), and (5) patient without cranial MRI, cranial CTP, TCD, and other blood tests. In addition, we also included 35 healthy controls to assess cognitive function as a comparison. This study was approved by the Ethics Committee of the First Hospital of Shanxi Medical University and followed the declaration of Helsinki. All patients and controls have signed informed consents.
Data Collection
Data collection included baseline assessments, imaging evaluations, and blood tests. Baseline assessments include sex, age, education, hypertension, diabetes, smoking history and drinking history. Imaging evaluations included the following parameters: (1) cranial CTA or DSA, including the degree of stenosis, the side of the stenosis and types of collateral compensation; (2) cranial MRI, including T1W1, T2W1, Flair, DWI, and then assessed the severity of white matter lesions using the revised Fazekas standard; (3) CTP, including time to peak (TTP), transit time (MTT), cerebral blood flow (CBF), and cerebral blood volume (CBV), (4) TCD, including peak systolic velocity, end diastolic velocity and mean flow velocity (MFV) of MCA, and then calculated pulsatility index (PI). Blood tests included kidney function, coagulation, serum lipids, homocysteine, folic acid, vitamin B12, and thyroid function, which were completed in all patients on the first day after admission. Based on the CTP results, patients were further divided into normal, compensation, and decompensation subgroups according to their perfusion period. CTP normal patients had complete blood perfusion. In the CTP compensation group, cerebrovascular function was retained (delayed TTP and MTT, normal or increased CBF and CBV), while in the CTP decompensation group, hypoperfusion was evident and cerebrovascular function was diminished (decreased CBF, normal or decreased CBV).
Neuropsychological Assessment
All patients underwent a standard neuropsychological evaluation by a specialized neurologist. The Montreal cognitive assessment scale (MoCA) assesses overall cognitive function. The auditory verb learn test-Huashan version (AVLT-H) was used to measure memory functions, including short-delay recall, long-delay recall, cued recall, and recognition. Executive function, including working memory, attention, dominance inhibition, set shifting, and fluency, was assessed with digit span test (DST), Symbol-digit Modalities Test (SDMT), Stroop color-word task (SCWT), trail making test (TMT), and verbal fluency test (VFT), respectively. The modified Boston naming test (mBNT) was used to measure language function and the Rey-Osterrieth complex figure test (RCFT) was used to measure visuospatial function. Patients were divided into cognitive normal (CN) group and cognitive impairment (CI) group according to MoCA score.
Statistical Analysis
SPSS 26.0 and R software were used for statistical analysis. The Kolmogorov–Smirnov test was used to analyze whether the data were normally distributed. For the data that passed the normality test, we used the two-sample independent t-test or analysis of variance, whereas for the data that failed it, we used the Mann–Whitney test or Kruskal–Wallis test. Chi-square test or Fisher’s exact test was used to compare qualitative variables. Univariate logistic regression analysis was used to screen predictors of cognitive impairment in patients with aMCAS. Factors with P<0.1 were included in the multivariate logistic regression analysis, and a backward conditional method was used to determine the best model. Based on the predictors of cognitive impairment identified in the final model, a nomogram was constructed and internally validated using bootstrap method with 1000 resamples. Receiver operating characteristic (ROC) curves were used to evaluate discrimination. Calibration curves were used to test the consistency between predicted probability and observed probability. Decision curve analysis (DCA) and clinical impact curve (CIC) were employed to evaluate the clinical applicability.
Results
General Clinical Characteristics
According to the inclusion and exclusion criteria, 54 patients with aMCAS were finally included in the study. Among them, 30 patients were cognitively impaired and 24 patients were cognitively normal. The general clinical characteristics of the two groups of aMCAS patients are shown in Table 1. The CI group included 14 patients with MCA occlusions and 16 patients with severe MCA stenosis; the CN group included 6 patients with MCA occlusions, 16 patients with severe MCA stenosis and 2 patients with moderate MCA stenosis. In addition, in the CI group, the number of patients in the CTP normal, CTP compensated, and CTP decompensated groups were 3, 11, and 16, respectively. In the CN group, the number of patients in the CTP normal, CTP compensated, and CTP decompensated groups were 6, 15, and 3, respectively. According to univariate analysis, there was a statistically significant difference between the two groups in terms of perfusion, MCA MFV, total cholesterol levels and LDL-c (P<0.05).
 |
Table 1 Characteristics of All Patients in the CN and CI Groups |
Comparison of Cognitive Function in Patients with aMCAS Under Different Perfusion Conditions
After grouping according to different perfusion periods, we compared the cognitive function of each group. There was no significant difference between the groups in VFT, mBNT, DSF, and RCFT (P > 0.05), while there was a significant difference in MoCA scores, AVLT-H, DSB, SDMT, TMT, and SCWT (P < 0.05). Compared with healthy controls, the CTP normal group had no significant difference in all cognitive tests, whereas the CTP compensation group had a significant difference in cued recall and executive function. The CTP decompensation group had significant differences in MoCA score, memory function, and executive function. In comparison among subgroups with different perfusion periods, patients in the CTP compensation group and decompensation group showed a significant decrease in attention, set shifting and dominance inhibition compared with the CTP normal group (P<0.05). And as the degree of hypoperfusion increased, the patients’ overall cognitive function and long-delayed recall ability gradually decreased (Table 2).
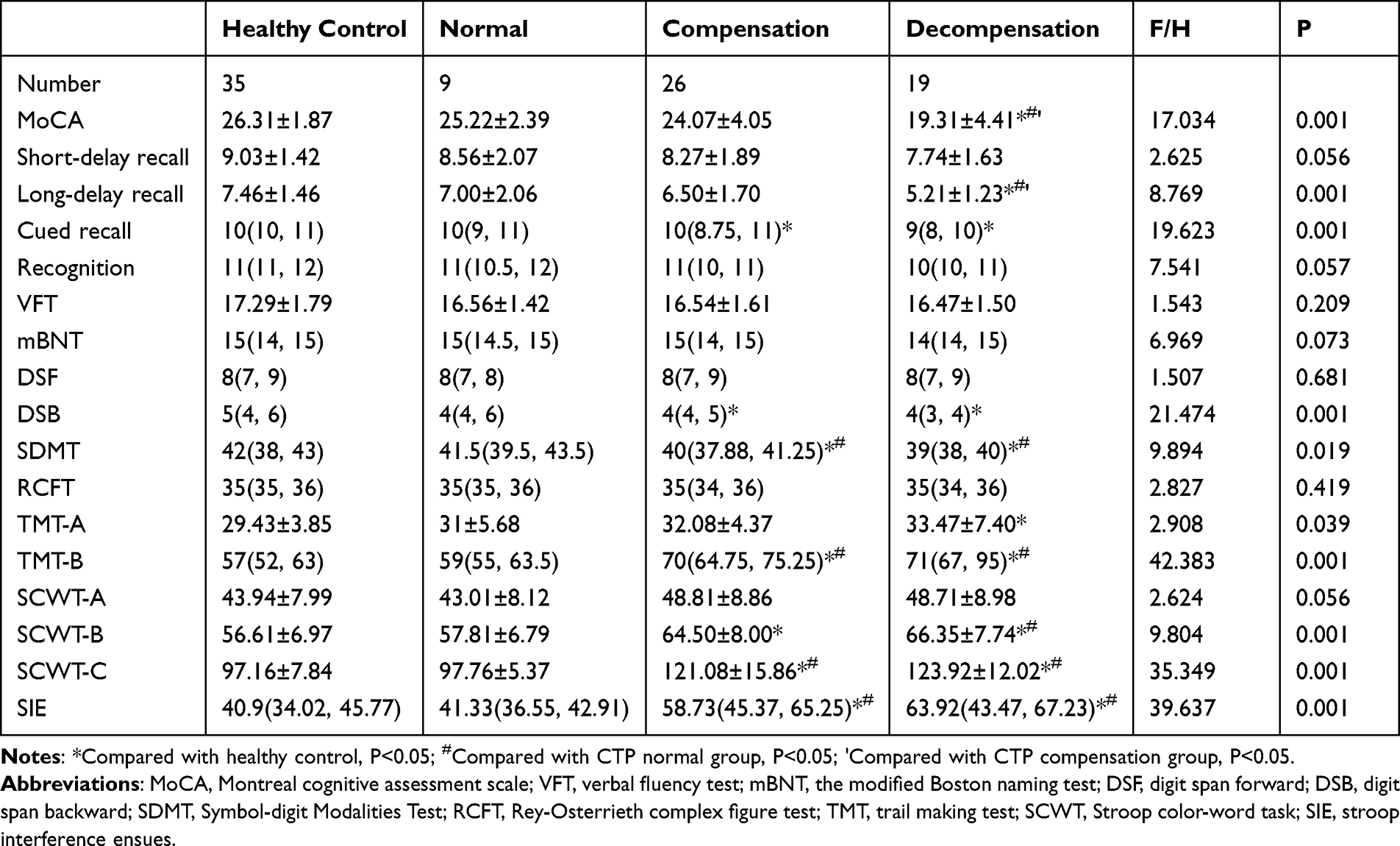 |
Table 2 Comparison of Cognitive Function in Patients with aMCAS Under Different Perfusion Periods |
Screening of Predictors and Construction of Prediction Model
Univariate logistic regression was used to screen predictors with a screening criterion of P<0.1. The results showed that CTP decompensation (OR=10.667, 95% CI 1.669–68.183), MCA MFV (OR=0.354, 95% CI 0.174–0.722), TC (OR=1.879, 95% CI 1.03–3.43), TG (OR=2.215, 95% CI 1.121–4.378), LDL-c (OR=2.239, 95% CI 1.178–4.257), FA (OR=1.748, 95% CI 0.933–3.275) and Fazekas grade 3 (OR=5, 95% CI 0.821–30.461) were included in further analysis. As a result of multivariate logistic regression, CTP decompensation (OR=15.220, 95% CI 1.461–158.606, P=0.023), MCA MFV (OR=0.412, 95% CI 0.191–0.893, P=0.025), and LDL-c (OR=2.409, 95% CI 1.11–5.228, P=0.026) were independent influencing factors of cognitive impairment in patients with aMCAS, which were included in the final model (Table 3).
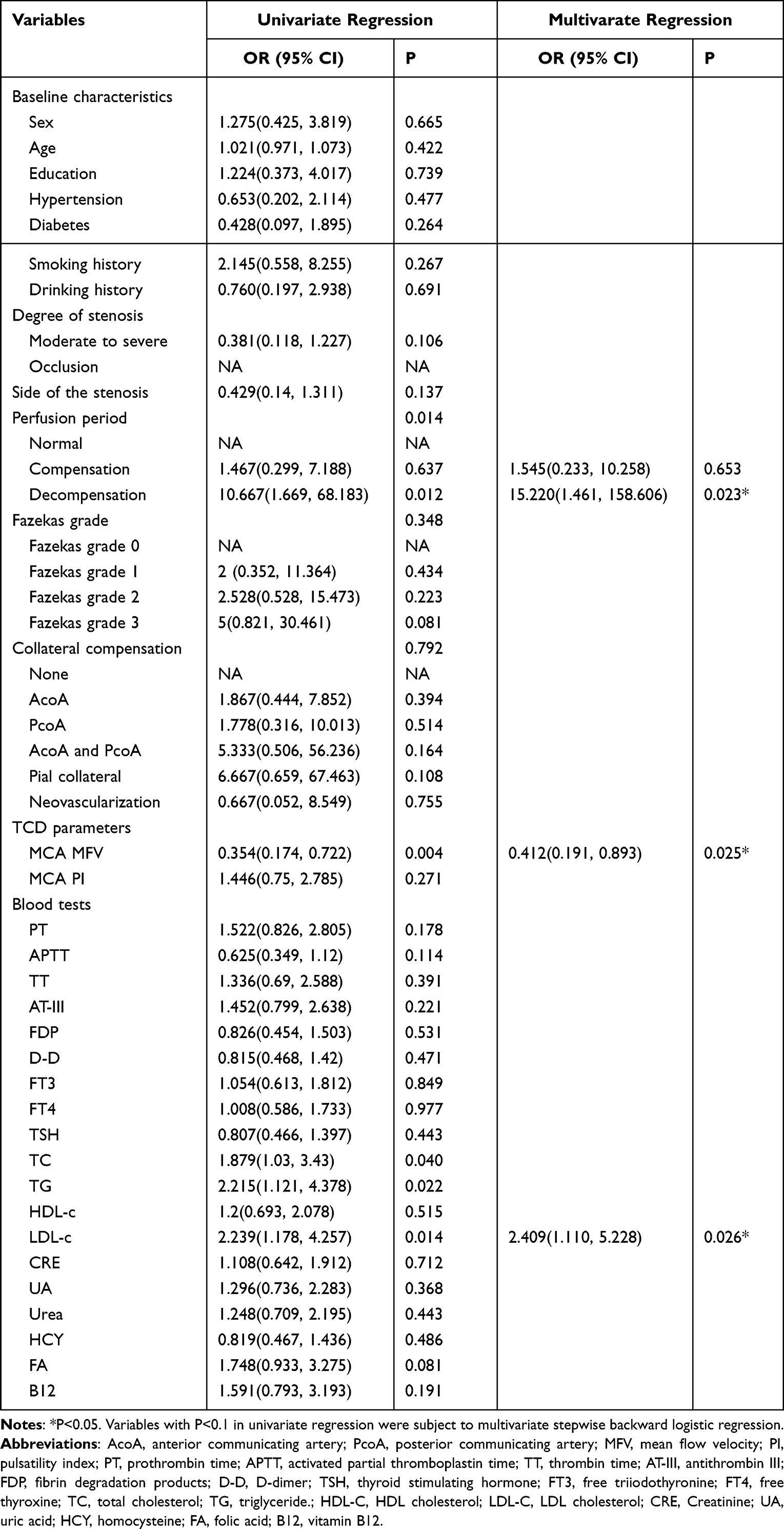 |
Table 3 Univariate and Multifactor Logistic Regression Results of Cognitive Impairment in Patients with aMCAS |
Construction of a Nomogram for Predicting Cognitive Impairment in Patients with aMCAS
Nomogram was plotted in R software based on the independent influences shown in the results of multivariate logistic regression (Figure 1). To validate the performance of the nomogram, the ROC curve was used to evaluate the ability of the predictive model and its components to discriminate cognitive impairment. The results showed that the AUC of perfusion period was 0.719 (sensitivity53.3%, specificity=87.5%, P<0.05), the AUC of MFV was 0.739 (sensitivity=90%, specificity=50%, P<0.05), and the AUC of LDL-c was 0.712 (sensitivity=63.3%, specificity=75%, P<0.05). The AUC for combined perfusion period, MFV, and LDL-c was 0.862 (sensitivity=73.3%, specificity=87.5%, P<0.05), which confirmed the good discriminatory ability of the nomogram (Figure 2A).
 |
Figure 1 Nomogram for predicting cognitive impairment in patients with aMCAS. |
 |
Figure 2 ROC curves (A), calibration curves (B), DCA curve (C) and CIC (D) of the nomogram. |
Validation of the Nomogram
The bootstrap method was used to internally validate the constructed model. Calibration curves for the nomogram showed good agreement between prediction and observation (Figure 2B). In addition, the DCA showed that the nomogram has great clinical applicability (Figure 2C). To more intuitively evaluate the clinical effect of the model, CIC was plotted on the basis of DCA (Figure 2D). The red curve represents the number of people classified as high risk by the nomogram at each threshold probability, and the blue dotted line represents the number of true positives at each threshold probability. With risk thresholds exceeding 60%, people at high risk of cognitive impairment judged by the nomogram were highly matched to people actually experiencing cognitive impairment.
Discussion
Vascular cognitive impairment is the second commonest type of dementia after Alzheimer’s disease. Most risk factors for vascular stenosis can be controlled, early diagnosis and effective treatment can delay the deterioration of cognitive function. Cognitive functions are jointly performed by multiple brain structures, and the frontal lobe is the key node of memory function.10 Executive functions depend on neural networks including structures such as the frontal lobe, parietal lobe, and basal ganglia,11 which are closely associated with the MCA. This study showed that aMCAS could impair multiple cognitive domains, including overall cognitive function, memory function and executive function. It is basically consistent with the results of previous studies.12,13 In addition, both the CTP compensation group and the CTP decompensation group showed significant impairment in subdomains of executive function and cued recall. This suggested that cognitive impairment existed even in the early stages of aMCAS when blood flow was able to maintain perfusion through collateral substitution. It further demonstrates the importance of early diagnosis.
Recently, there has been a focus on predicting patients’ risk of cognitive impairment and personalised treatment. Previous studies typically focused on analyzing the relationship between a single risk factor and cognitive impairment, overlooking the complex interplay of multiple risk factors. In this study, we analyzed various factors including baseline characteristics, vascular conditions, haemodynamic characteristics, and vascular risk factors in patients. Our study is the first to combine these factors and the results showed that CTP loss of compensation, MCA-MFV, and LDL-c levels were independent risk factors for cognitive impairment. And the nomogram was subsequently developed to assess the risk of cognitive impairment in patients, which has good discrimination, calibration and clinical applicability. Our study is the first to construct a predictive model to predict the risk probability of cognitive impairment in patients with aMCAS. The model serves as a tool to predict the risk probability of cognitive impairment in patients, enabling clinicians to identify and apply interventions early on.
Previous study found that patients with poor and moderate collateral circulation in aMCAS had worse cognitive function than patients with good collateral circulation,13 which suggested that cognitive impairment in patients with aMCAS may be associated with hypoperfusion. This was further confirmed in this study that perfusion decompensation was an independent risk factor for cognitive impairment in patients with aMCAS. Severe hypoperfusion can lead to irreversible atrophy and death,14 deposition of neurotoxic substances and exacerbation of neuronal dysfunction.15 In addition, hypoperfusion can also induce white matter damage and lead to cognitive impairment.16 However, in our study white matter lesions were associated with cognitive impairment, but logistic regression showed that it was not an independent influencing factor of cognitive impairment. This may be because our study mainly includes asymptomatic patients, but a variety of symptoms may develop as white matter lesions progress. As a result, most patients have a low level of white matter lesions, which may affect the results of the study. Apart from directly affecting brain structures dominated by MCA, research has shown that MCA occlusion can lead to delayed death of hippocampal neurons.17 This may be because the gap junction communication action of astrocytes propagates neurotoxic molecules or damage signals produced in the ischemic area to the hippocampus, expanding the ischemic damage.18 In summary, hypoperfusion can impair cognitive function through multiple pathways, and our study confirms for the first time that perfusion decompensation is an independent risk factor for cognitive function in patients with aMCAS. Therefore, identifying the perfusion period of patients with aMCAS is necessary for predicting cognitive impairment in patients.
In addition, we found that decreased MCA MFV was an independent risk factor for cognitive impairment in patients with aMCAS. When vascular stenosis occurs, the flow velocity of the artery is inversely proportional to the diameter, but the reduction in cerebral perfusion leads to a decrease in blood flow velocity at a certain degree of stenosis. Decreased MCA MFV was found strongly associated with cognitive impairment in patients with asymptomatic carotid stenosis and mild cognitive impairment.19,20 It is basically consistent with our results. Apart from MFV, PI is also one of the important parameters of TCD, which reflects cerebrovascular resistance and compliance. However, there was no significant correlation between PI and cognitive impairment in our study. The reason for this may be that in addition to cerebral blood flow resistance, PI can also be affected by arterial blood pressure, cerebral arterial elastic resistance, heart rate, and other factors.21 A community-based follow-up study also found no significant association between MCA-PI and cognitive decline.22 Therefore, monitoring MCA MFV in patients with aMCAS is important for assessing changes in cognitive function.
Apart from perfusion period and MCA MFV, LDL-c is also an independent risk factor for cognitive function in patients with aMCAS. As an important part of the neuron, cholesterol is essential for maintaining neuronal function.23 However, low LDL levels in the periphery do not affect normal brain function because the cholesterol required by the CNS is resynthesized in brain cells.24 Studies have shown that low LDL levels are associated with a slowed rate of cognitive decline.25–27 Peripheral cholesterol can enter the CNS as 27-hydroxycholesterol (27-OHC), which can accelerate Aβ accumulation, increase hyperphosphorylated tau levels, decrease brain antioxidant enzyme activity, involve in inflammatory responses to promote neurodegeneration and reduce brain glucose uptake.28 There is a close relationship between circulating cholesterol and 27-OHC levels, and high plasma cholesterol can lead to increased plasma levels of 27-OHC.29 Therefore, reduced peripheral blood cholesterol levels may be beneficial to improving cognitive function. The development of PCSK9 inhibitors has made it possible to lower LDL-c to very low levels without causing adverse neurocognitive events.30 Our findings provide evidence that low levels of LDL-c are beneficial for cognitive function. Therefore, early intervention to lower LDL-c is crucial in preventing and delaying cognitive function deterioration in patients with aMCAS.
Although our findings suggest that hypoperfusion and decreased mean middle cerebral artery flow velocity are independent risk factors for patients with aMCAS, it is controversial whether cognitive function can be improved after revascularization by surgery to relieve stenosis. Neuronal damage is permanent under conditions of chronic occlusion and long-term chronic ischemia may be irreversible.31 Recent studies have shown that endovascular therapy may not improve cognitive function or decrease the 1-year risk of stroke and death in patients with aMCAS.32–34 Therefore, drug therapy alone is a critical treatment for patients with aMCAS. This further emphasizes the importance of early diagnosis and treatment. Using nomogram for individualized assessment of aMCAS patients can help clinicians better evaluate patients’ conditions and develop more accurate treatment plans.
The limitations of this study are as follows: (1) This study had a relatively small sample size, which may have influenced the results. (2) This study was a cross-sectional study and did not longitudinally follow up the change in cognitive function of the patients. (3) Since this study included inpatients mainly with more than severe stenosis, our findings may not be generalized to patients with mild degrees of aMCAS.
Conclusion
This study showed that CTP decompensation, MCA-MFV, and LDL-c were independent risk factors for cognitive impairment in patients with aMCAS. Afterwards, a nomogram was constructed with good discrimination, calibration, and clinical validity for predicting cognitive impairments. It can help clinicians to identify patients with cognitive impairment as early as possible to delay or even stop the deterioration of cognitive function in patients with aMCAS.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Arenillas JF. Intracranial atherosclerosis: current concepts. Stroke. 2011;42(1 Suppl):S20–S23. doi:10.1161/STROKEAHA.110.597278
2. Dearborn JL, Zhang Y, Qiao Y, et al. Intracranial atherosclerosis and dementia: the Atherosclerosis Risk in Communities (ARIC) Study. Neurology. 2017;88(16):1556–1563. doi:10.1212/WNL.0000000000003837
3. Suri MFK, Zhou J, Qiao Y, et al. Cognitive impairment and intracranial atherosclerotic stenosis in general population. Neurology. 2018;90(14):e1240–e1247. doi:10.1212/WNL.0000000000005250
4. Viticchi G, Falsetti L, Potente E, Bartolini M, Silvestrini M. Impact of carotid stenosis on cerebral hemodynamic failure and cognitive impairment progression: a narrative review. Ann Transl Med. 2021;9(14):1209. doi:10.21037/atm-20-7226
5. Romero JR, Beiser A, Seshadri S, et al. Carotid artery atherosclerosis, MRI indices of brain ischemia, aging, and cognitive impairment: the Framingham study. Stroke. 2009;40(5):1590–1596. doi:10.1161/STROKEAHA.108.535245
6. Mathiesen EB, Waterloo K, Joakimsen O, Bakke SJ, Jacobsen EA, Bonaa KH. Reduced neuropsychological test performance in asymptomatic carotid stenosis: the Tromso Study. Neurology. 2004;62(5):695–701. doi:10.1212/01.WNL.0000113759.80877.1F
7. Martinić-Popović I, Lovrenčić-Huzjan A, Demarin V. Assessment of subtle cognitive impairment in stroke-free patients with carotid disease. Acta Clin Croat. 2009;48(3):231–240.
8. He S, Duan R, Liu Z, et al. Altered functional connectivity is related to impaired cognition in left unilateral asymptomatic carotid artery stenosis patients. BMC Neurol. 2021;21(1):350. doi:10.1186/s12883-021-02385-4
9. Hachinski V, Iadecola C, Petersen RC, et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke. 2006;37(9):2220–2241. doi:10.1161/01.STR.0000237236.88823.47
10. Pergola G, Suchan B. Associative learning beyond the medial temporal lobe: many actors on the memory stage. Front Behav Neurosci. 2013;7:162. doi:10.3389/fnbeh.2013.00162
11. Barnes JJ, Dean AJ, Nandam LS, O’Connell RG, Bellgrove MA. The molecular genetics of executive function: role of monoamine system genes. Biol Psychiatry. 2011;69(12):e127–e143. doi:10.1016/j.biopsych.2010.12.040
12. Kimura S, Ogata T, Watanabe J, Inoue T, Tsuboi Y. Does cerebral large-artery disease contribute to cognitive impairment? eNeurologicalSci. 2017;8:5–8. doi:10.1016/j.ensci.2017.06.003
13. Meng Y, Yu K, Zhang L, Liu Y. Cognitive decline in asymptomatic middle cerebral artery stenosis patients with moderate and poor collaterals: a 2-year follow-up study. Med Sci Monit. 2019;25:4051–4058. doi:10.12659/MSM.913797
14. Cechetti F, Pagnussat AS, Worm PV, et al. Chronic brain hypoperfusion causes early glial activation and neuronal death, and subsequent long-term memory impairment. Brain Res Bull. 2012;87(1):109–116. doi:10.1016/j.brainresbull.2011.10.006
15. Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci. 2011;12(12):723–738. doi:10.1038/nrn3114
16. Duncombe J, Kitamura A, Hase Y, Ihara M, Kalaria RN, Horsburgh K. Chronic cerebral hypoperfusion: a key mechanism leading to vascular cognitive impairment and dementia. Closing the translational gap between rodent models and human vascular cognitive impairment and dementia. Clin Sci. 2017;131(19):2451–2468. doi:10.1042/CS20160727
17. Wang W, Redecker C, Bidmon HJ, Witte OW. Delayed neuronal death and damage of GDNF family receptors in CA1 following focal cerebral ischemia. Brain Res. 2004;1023(1):92–101. doi:10.1016/j.brainres.2004.07.034
18. Xie M, Yi C, Luo X, et al. Glial gap junctional communication involvement in hippocampal damage after middle cerebral artery occlusion. Ann Neurol. 2011;70(1):121–132. doi:10.1002/ana.22386
19. Sun ZW, Zhu YX, Liu HY, et al. Decreased cerebral blood flow velocity in apolipoprotein E epsilon4 allele carriers with mild cognitive impairment. Eur J Neurol. 2007;14(2):150–155. doi:10.1111/j.1468-1331.2006.01579.x
20. Marshall RS, Pavol MA, Cheung YK, Asllani I, Lazar RM. Cognitive impairment correlates linearly with mean flow velocity by transcranial Doppler below a definable threshold. Cerebrovasc Dis Extra. 2020;10(1):21–27. doi:10.1159/000506924
21. de Riva N, Budohoski KP, Smielewski P, et al. Transcranial Doppler Pulsatility Index: what it is and what it isn’t. Neurocrit Care. 2012;17(1):58–66. doi:10.1007/s12028-012-9672-6
22. Xiao Z, Ren X, Zhao Q, et al. Relation of middle cerebral artery flow velocity and risk of cognitive decline: a prospective community-based study. J Clin Neurosci. 2022;97:56–61. doi:10.1016/j.jocn.2021.12.028
23. Pfrieger FW. Cholesterol homeostasis and function in neurons of the central nervous system. Cell Mol Life Sci. 2003;60(6):1158–1171. doi:10.1007/s00018-003-3018-7
24. Bjorkhem I, Meaney S. Brain cholesterol: long secret life behind a barrier. Arterioscler Thromb Vasc Biol. 2004;24(5):806–815. doi:10.1161/01.ATV.0000120374.59826.1b
25. Hua R, Ma Y, Li C, Zhong B, Xie W. Low levels of low-density lipoprotein cholesterol and cognitive decline. Sci Bull. 2021;66(16):1684–1690. doi:10.1016/j.scib.2021.02.018
26. Power MC, Rawlings A, Sharrett AR, et al. Association of midlife lipids with 20-year cognitive change: a cohort study. Alzheimers Dement. 2018;14(2):167–177. doi:10.1016/j.jalz.2017.07.757
27. An Y, Zhang X, Wang Y, et al. Longitudinal and nonlinear relations of dietary and Serum cholesterol in midlife with cognitive decline: results from EMCOA study. Mol Neurodegener. 2019;14(1):51. doi:10.1186/s13024-019-0353-1
28. Wu M, Zhai Y, Liang X, et al. Connecting the dots between Hypercholesterolemia and Alzheimer’s disease: a potential mechanism based on 27-hydroxycholesterol. Front Neurosci. 2022;16:842814. doi:10.3389/fnins.2022.842814
29. Babiker A, Dzeletovic S, Wiklund B, et al. Patients with atherosclerosis may have increased circulating levels of 27‐hydroxycholesterol and cholestenoic acid. Scand J Clin Lab Invest. 2009;65(5):365–376. doi:10.1080/00365510510025746
30. Olsson AG, Angelin B, Assmann G, et al. Can LDL cholesterol be too low? Possible risks of extremely low levels. J Intern Med. 2017;281(6):534–553. doi:10.1111/joim.12614
31. de la Torre JC, Fortin T, Park GAS, Pappas BA, Richard MT. Brain blood flow restoration ‘rescues’ chronically damaged rat CA1 neurons. Brain Res. 1993;623(1):6–15. doi:10.1016/0006-8993(93)90003-6
32. Bossema ER, Brand N, Moll FL, Ackerstaff RG, van Doornen LJ. Does carotid endarterectomy improve cognitive functioning? J Vasc Surg. 2005;41(5):775–781; discussion 781. doi:10.1016/j.jvs.2004.12.057
33. Kwon JY, Han YS, Kim JY, et al. Intracranial artery stenting may not improve cognitive function: a preliminary study. J Stroke. 2016;18(2):227–229. doi:10.5853/jos.2015.01641
34. Gao P, Wang T, Wang D, et al. Effect of stenting plus medical therapy vs medical therapy alone on risk of stroke and death in patients with symptomatic intracranial stenosis: the CASSISS randomized clinical trial. JAMA. 2022;328(6):534–542. doi:10.1001/jama.2022.12000
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
Establishment and Validation of a Predictive Nomogram for Hallux Valgus with Pain Under the Second Metatarsal
Bai Z, Cao X, Yang Y, Sun X, Dong Y, Wen J, Sun W
Journal of Pain Research 2022, 15:3523-3536
Published Date: 7 November 2022
Establishment and Validation of a Model for Disease-Free Survival Rate Prediction Using the Combination of microRNA-381 and Clinical Indicators in Patients with Breast Cancer
Shen J, Wang M, Li F, Yan H, Wang R, Zhou J
Breast Cancer: Targets and Therapy 2022, 14:375-389
Published Date: 30 November 2022
A Visualized Mortality Prediction Score Model in Hematological Malignancies Patients with Carbapenem-Resistant Organisms Bloodstream Infection
Qian C, Wu Q, Ruan Z, Liu F, Li W, Shi W, Ma L, Peng D, Yin H, Yao L, Li Z, Hong M, Xia L
Infection and Drug Resistance 2023, 16:201-215
Published Date: 7 January 2023
Establishment and Validation of a Predictive Model for Post-Treatment Anxiety Based on Patient Attributes and Pre-Treatment Anxiety Scores
Sun W, Shen J, Sun R, Zhou D, Li H
Psychology Research and Behavior Management 2023, 16:3883-3894
Published Date: 19 September 2023