")
Back to Journals » Clinical Interventions in Aging » Volume 17
Nomogram for Persistent Post-Stroke Depression and Decision Curve Analysis
Authors Lan Y , Pan C , Qiu X, Miao J, Sun W, Li G, Zhao X, Zhu Z, Zhu S
Received 25 January 2022
Accepted for publication 30 March 2022
Published 5 April 2022 Volume 2022:17 Pages 393—403
DOI https://doi.org/10.2147/CIA.S357639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yan Lan, Chensheng Pan, Xiuli Qiu, Jinfeng Miao, Wenzhe Sun, Guo Li, Xin Zhao, Zhou Zhu, Suiqiang Zhu
Department of Neurology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Zhou Zhu; Suiqiang Zhu, Tel +86-18171081029 ; +86-13035101141, Email [email protected]; [email protected]
Purpose: Previous studies have shown that persistent post-stroke depression (PSD) was associated with unfavorable prognosis. The aim of this multicenter prospective study was to investigate the predictors associated with persistent PSD, develop a nomogram and validate its clinical usefulness by decision curve analysis (DCA).
Patients and Methods: A total of 875 acute ischemic stroke patients from four hospitals were consecutively recruited and completed 1-year follow-ups. Sociodemographic indicators, vascular risk factors, clinical information, serum biochemical indicators and cytokines were collected on admission. The functional outcome was assessed at 1 year after stroke. Persistent depression was defined as having a presentation of depression at each follow-up points and the depressive symptoms occurring persistently since the diagnosis of depression.
Results: There were 513 patients who experienced PSD during the 1-year follow-up, the cumulative incidence of PSD within 1 year was 58.6%. Persistent PSD was recorded in 289 patients, of which 59 (20.4%) result in unfavorable outcomes. The risk factors of persistent PSD in 1 year after stroke were the Hamilton Depression Scale-17 items (HAMD-17) score at admission, serum direct bilirubin and free serum thyroxine (FT4) level and activated partial thromboplastin time (APTT). Nomogram conducted based on these factors has a C-index (± standard deviation) of 0.655 ± 0.039, and the DCA demonstrated that the nomogram had a favorable clinical utility.
Conclusion: We found that persistent depression after stroke in the first-year time course after stroke was associated with HAMD-17 score at admission, lower serum direct bilirubin and FT4 level, and APTT. A nomogram was developed with advisable clinical usefulness in our study.
Keywords: persistent post-stroke depression, nomogram, decision curve analysis
Introduction
Stroke is a leading disease not only endangering physical health outcome but also causing emotional disturbance. Post-stroke depression (PSD) is a common complication after stroke, which contributes to an increasing disability and lower quality of life.1–4 The incidence of PSD at different time course after stroke was reported to be as high as 18.8–41.8%,5–8 early onset PSD could happen in 1 month after stroke, while later onset PSD occurs in the subsequent follow-up visits after stroke.9,10 PRIOD study had indicated that the PSD can be transient, persistent, or maybe recurrent.5,11 Among the patients with depression after stroke, those who developed persistent depression were reported to be more disabled and have more severe depressive symptoms. Previous studies have shown that persistent PSD was associated with unfavorable prognosis measured by modified Rankin Scale (mRS) and quality of life (QoL).5,12,13 A multicenter study including 56 hospitals in mainland China showed that patients with persistent depression after stroke were 7.6 times higher than others in the risk of poor 1-year prognosis.5 However, there are few studies researching on the risk factors related to persistent depression after stroke.
The aim of this multicenter prospective study was to investigate the predictors associated with persistent PSD, develop a nomogram that contributes to risk prediction for patients, and validate its clinical usefulness by decision curve analysis (DCA).
Methods
Study Design and Participants
This is a multicenter prospective cohort study conducted in four large 3A hospitals: Wuhan Tongji Hospital, Wuhan First Hospital, Wuhan Central Hospital and Fujian Provincial Hospital (Registration number: ChiCTR-ROC-17013993). A total of 1027 stroke patients treated in the above hospitals were recruited into the study from May 2018 to October 2019. Written informed consent was given from all the participants in accordance with the Declaration of Helsinki. And the research was approved by the Ethics Committee of Tongji Medical College of Huazhong University of Science and Technology (ID:TJ-IRB20171108).
Inclusion criteria for this study were as follows: 1) age ≥18 years; 2) admitted to hospital within 7 days of first stroke onset; 3) acute ischemic stroke diagnosed by computed tomography (CT) or magnetic resonance imaging (MRI) scans, with clinical presentations according to the World Health Organization (WHO) criteria for stroke.14 And patients with any of the following conditions were excluded from the study: 1) brain dysfunction was caused by non-vascular causes such as traumatic brain injury, brain tumor or metastatic brain tumor; 2) history of depression or antidepressant use, dementia, or other mental illness; 3) unable to cooperate to the assessment as aphasia, dysarthria, blindness, deafness, or cognitive dysfunction (Mini-mental State Examination (MMSE) score <19 points, and illiterate patients <17 points); 4) diagnosed as transient ischemic attack (TIA) or hemorrhagic stroke; 5) unable to conduct the follow-up. At last, 857 patients were included in the final study.
Information Acquisition
The standard case report forms (CRF) were used to collect sociodemographic indicators, vascular risk factors and clinical information of patients during the first 24 hours of admission. Sociodemographic indicators included gender, age, body mass index (BMI), educational level and marital status. Vascular risk factors covered smoking, drinking, coronary heart disease (CHD), hypertension, diabetes and hyperlipidemia. Clinical information such as National Institutes of Health Stroke Scale (NIHSS) score, Mini-Mental State Examination (MMSE), Center for Epidemiologic Studies Depression Scale (CES-D), neuroticism assessed by Eysenck Personality Questionnaire (EPQ), mental resilience assessed by Connor–Davidson resilience scale (CD-RISC), Social Support Rating Scale (SSRS) and the Hamilton Depression Scale-17 items (HAMD-17) were also obtained at admission by trained neurologists. Moreover, serum samples for assay of biochemical indicators and cytokines were sampled at 6 a.m. the day after admission.
The PSD diagnosis was established according to the DSM-V at the follow-up. At the same time, HAMD-17 was assessed for depression severity at 2 weeks, 3 and 6 months, and 1 year (day 14 ± 2, day 84 ± 7, day 182 ±7, day 360 ± 7, respectively) after stroke onset. The mRS score was obtained to determine functional outcome at 1 year. The follow-up at each center was conducted by systematically trained neurologists by outpatient visit or video telephone. None of these physicians knew the baseline information of patients. All raters were blinded to the baseline information of patients.
Persistent depression was defined as having a presentation of depression at each follow-up points and the depressive symptoms occurring persistently since the diagnosis of depression. Recurrent depression was defined as depression at non-consecutive follow-up time points. Transient depression was defined as depressive symptoms showed only at one time point or at 2–3 consecutive follow-up points without recurrence.5,6,12 The unfavorable prognosis of 1 year after stroke was considered mRS score ≥2.15
Statistical Analysis
Statistical analyses were performed using Statistical Package for the Social Sciences version 22.0 (SPSS, Chicago, IL) and R version 3.5.2 (http://www.r-project.org). Categorical data were presented as frequencies and proportions, and the variables were compared using chi-square test and Fisher’s exact test in univariate analysis. Continuous data were expressed as medians and interquartile ranges, and Mann–Whitney U-test was used for comparing these variables. To get the best possible result, variables with P < 0.10 in univariate analysis results should be subjected to stepwise backward multivariable logistic regression analysis. A two-tailed P value less than 0.05 (P<0.05) was identified as statistical significance. The adjusted odds ratio (aOR) and 95% confidence intervals (CIs) for the risk factors were obtained by multivariate-adjusted binary logistic regression.
On this basis, a nomogram of persistent PSD during 1 year was formulated by predictors in multivariable logistic regression analysis by using the package “rms”. Internal validation of the nomogram was conducted by a resampling method, reflected in the concordance index and the calibration curves. Moreover, the clinical usefulness of the nomogram was evaluated by decision curve analysis (DCA), which was conducted by calculating the net benefit at different threshold risk of the model using the package “rmda”. DCA was founded in 2006 by Dr Andrew J Vickers,16,17 the method was based on a probability threshold to express the relative harms of false positives and false negatives, it was a rising method for evaluating clinical predictive models these years.
Results
Baseline Characteristics of Patients
The study included a total of 875 acute ischemic stroke patients after evaluation (mean age, 59.06±10.48) (Figure 1), with 513 patients experienced PSD during the 1-year follow-up. The cumulative incidence of PSD within 1 year was 58.6% (Table 1). Of those 513 patients, there were 119 females and 394 males. There were 338 patients (65.8%) from Tongji Hospital, 130 patients (25.3%) from Wuhan First Hospital, 32 patients (6.2%) from Wuhan Central Hospital and 13 patients (2.5%) from Fujian provincial hospital. Among those patients who experienced PSD, there were 289 patients with persistent PSD, 181 patients with transient PSD, and 43 patients with recurrent PSD, the cumulative incidence of persistent PSD in the first year after stroke was 33.0%. For patients with persistent PSD, unfavorable outcomes were recorded in 59 (20.4%) patient. Neither transient PSD nor recurrent PSD has significant association with 1-year prognosis after stroke (P = 0.302, 0.950). In the multivariable logistic regression analysis adjusting for confounding factors, we found that persistent PSD was an independent risk factor for unfavorable prognosis (adjusted odds ratio [aOR] = 3.389; 95% confidence interval [CI], 2.171–5.291; P < 0.001).
 |
Table 1 Incidence of Depression in Stroke Patients |
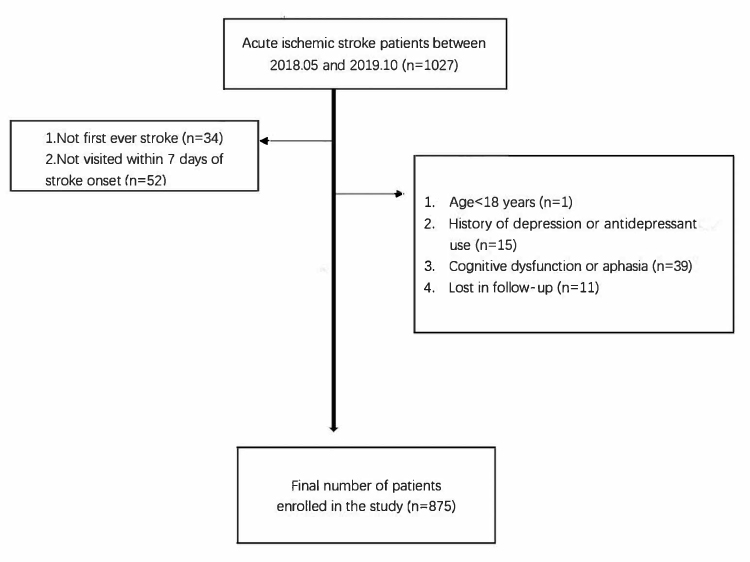 |
Figure 1 Flow chart of the research. |
Compared with others, patients with persistent depression after stroke were more likely to be married, had significantly higher NIHSS scores at admission, tended to get higher scores in CES-D scale and HAMD-17 scale, were more likely to be neurotic and get less score in MMSE scale. Moreover, patients with persistent PSD were more likely to have lower serum direct bilirubin level, free serum thyroxine level (FT4), IL-18 level, BDNF level, longer activated partial thromboplastin time (APTT), and higher serum fibrinogen level (Table 2).
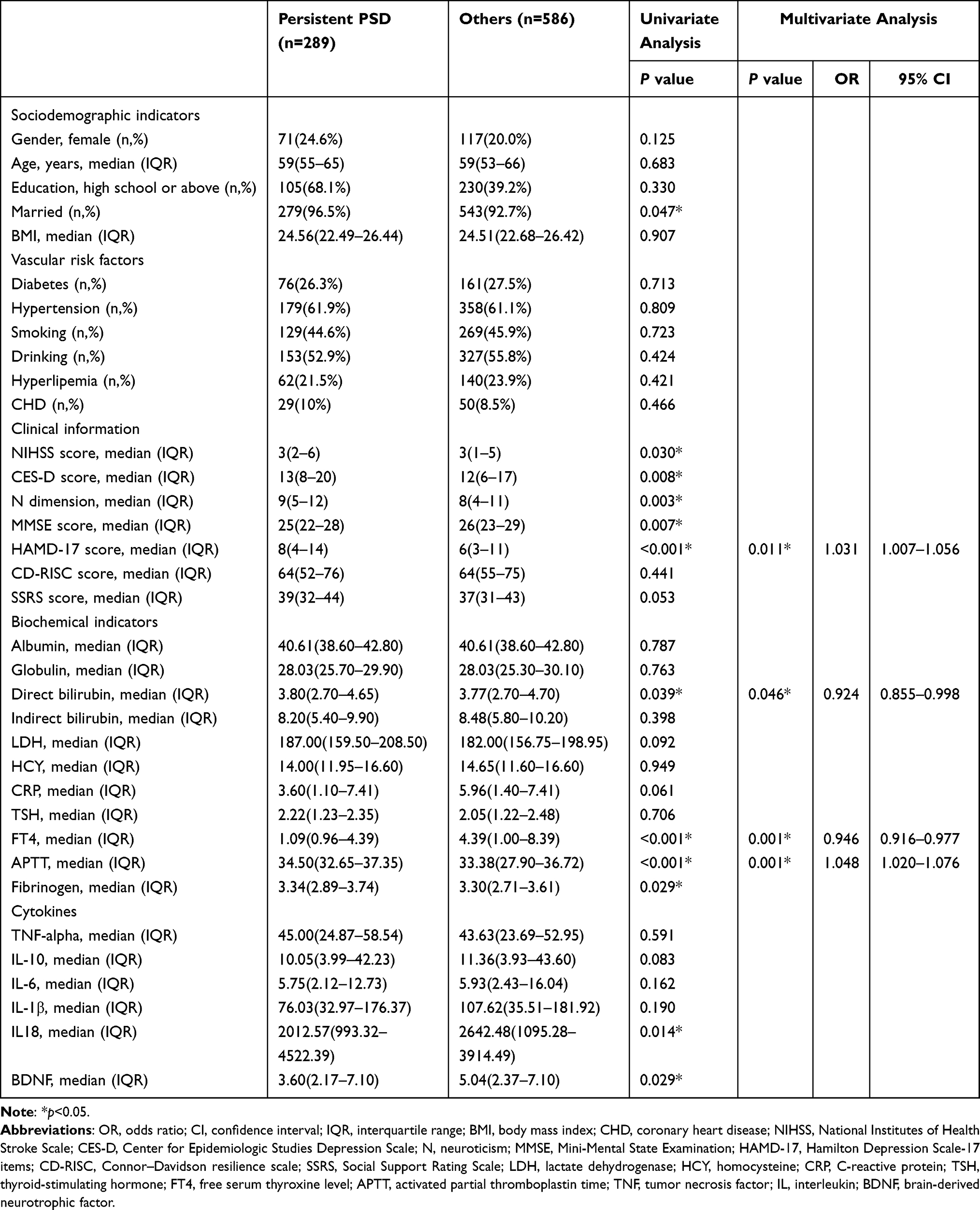 |
Table 2 Comparison of Baseline Characteristics Between Persistent PSD and Others |
Risk Factors of Persistent PSD
As showed in Table 2, the risk factors of persistent PSD in 1 year after stroke were HAMD-17 score at admission ([aOR], 1.031; [CI], 1.007–1.056, P=0.011), serum direct bilirubin ([aOR], 0.924; [CI], 0.855–0.998, P=0.046) and FT4 level ([aOR], 0.946; [CI], 0.916–0.977, P<0.001) and APTT ([aOR],1.048; [CI], 1.020–1.076, P<0.001). These variables were independently associated with persistent PSD even after adjusting for confounding factors like age, gender, marriage, education level, BMI, vascular risk factors and NIHSS score on admission.
Predictive Model of Persistent PSD and Model Evaluation
All the variables identified in the multivariate logistic regression analysis of persistent PSD were involved in constructing the nomogram (Figure 2). A risk of persistent PSD could be obtained by calculating the total points of each predictors. Calibration curves were plotted to measure the calibration of the nomogram, accompanied with the Hosmer–Lemeshow test and 1000 bootstrap resamples.18 The Harrell’s C-index (±standard deviation) was 0.655±0.039 and the calibration curves for this model demonstrated a moderate agreement between the predicted risk and actual observations (Figure 3).
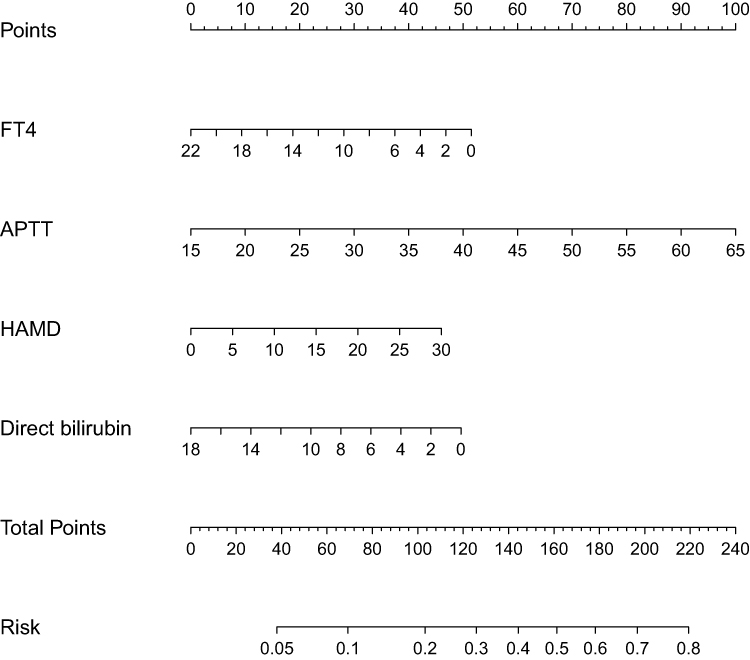 |
Figure 2 Nomogram predicting persistent depression in 1-year time course after stroke. Abbreviations: FT4, free serum thyroxine level; APTT, activated partial thromboplastin time; HAMD, Hamilton Depression Scale-17 items. |
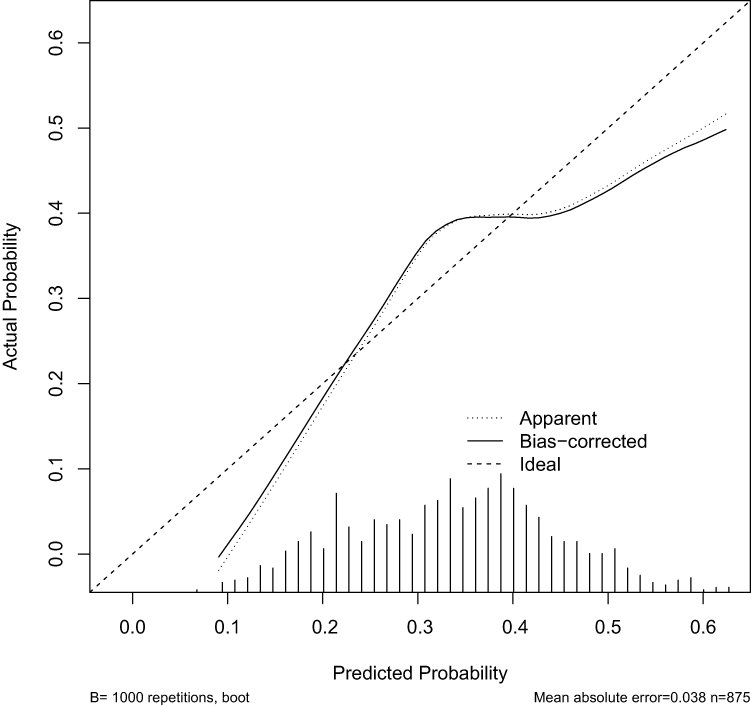 |
Figure 3 Calibration plots of the nomogram. |
The DCA for persistent PSD nomogram is presented in Figure 4. It showed that if the risk threshold of a patient is between 12% and 70%, there will be more net benefit than either treating all patients or treating none by using the nomogram to decide whether or not to conduct treatment. The decision curve demonstrated that the nomogram had a favorable clinical utility.
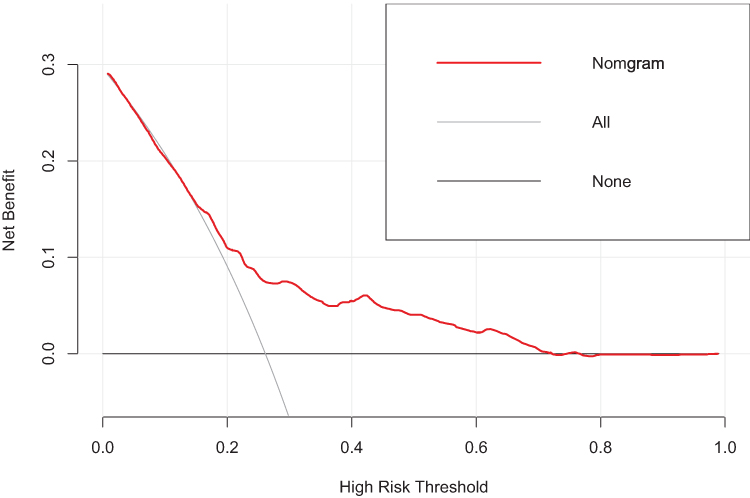 |
Figure 4 Decision curve analysis of the model. |
Discussion
This is a multicentric prospective cohort study on PSD with 1-year follow-up in first-ever acute ischemic stroke patients. The cumulative incidence of PSD was 58.6%, more than half of these patients with PSD were diagnosed in the first month after stroke onset, the incidence of newly occurring PSD was continuously declining in the first-year time course of stroke. In 56.3% of PSD patients depression was persistent during 1-year time course after stroke. The study demonstrated that persistent depression after stroke was an independent predictor of unfavorable functional outcome at 1 year, which was consistent with previous studies.5,12,13,19
PSD is a critical complication after stroke, which can occur in different phases in the course of stroke. Previous studies indicated that persistent PSD was linked with poor prognosis and the relief of PSD could be associated with the improvement of quality of life.20–22 In view of the cumulative incidence of PSD and persistent depression reported in this study was higher than previous studies, determining predictors of persistent depression after stroke is of essence. We have identified HAMD-17 score, APTT, serum direct bilirubin and FT4 at admission, related to the occurrence of persistent PSD in the first-year time course, and developed a nomogram to facilitate the individualized risk prediction of persistent PSD. To the best of our knowledge, it is the first research to construct a nomogram for the prediction of persistent PSD.
HAMD-17 score at admission may represent the depression condition of patients in the baseline. We found that high HAMD-17 scores were associated with persistent PSD. A patient would be more likely to develop persistent depression in the first-year course after stroke if he/she was diagnosed with depression at the admission just after the stroke onset. Patients who had experienced more severe stroke tended to have higher psychological stress, which always manifests as depressive symptoms and scores in scale assessing.23–26 On univariate analysis in our study, stroke severity represented by NIHSS score was associated with persistent depression. Hence, the link between HAMD-17 score at admission and persistent depression might be explained by stroke severity.
There were hardly any researches going into the link between serum FT4 and persistent PSD. FT4 is a sensitive indicator of thyroid function, which can reflect thyroid function directly even in the circumstances of concentration and binding force of plasma thyroid binding protein changing under physiological and pathological conditions. Interaction of the thyroid and serotonin system was suggested to be a potential underlying mechanism of the association between FT4 and PSD. Thyroxine has modulatory effects on the brain serotonin system, and previous studies have demonstrated that reduced levels of thyroxine could slow serotonergic transmission and decrease 5-HT responsiveness in the brains nervous system, which contributed to depression and suicidal behaviors.27–29 In addition, thyroid hormones are used as an effective adjunct antidepressant treatment over the decades, and exogenous thyroid hormones may increase 5-HT2 receptor sensitivity, desensitize 5-HT1A raphe autoreceptors, and increase 5-HT release in cortical and hippocampal.27,30,31 Patients with lower serum FT4 level tend to develop more depressive symptoms and respond slower to antidepressant treatment compared with others.32–35 Besides, lower FT4 may perform weakly in neuroprotective effect when removing glutamate in the reperfusion phase after ischemic stroke.36 However, in a research with small sample size, FT4 was found to have no significant association with PSD.33 It is indispensable to make further research to the relationship between FT4 and persistent PSD.
Bilirubin is a useful antioxidant in our body, and the relationship of a low serum direct bilirubin level with persistent PSD was observed in the study. Very few of previous studies had researched the relationship between serum direct bilirubin level and PSD, and the evidence is controversial. A prospective cohort of 635 participants conducted in Hong Kong demonstrated that high serum bilirubin could predict PSD at 3 months after stroke.37 Another study found that lower levels of serum bilirubin on admission was associated with PSD between 3 and 6 months post-stroke.38 The potential explanations of the relation we could infer were as follows. Numerous studies have found that acute ischemic stroke could generate strong oxidative stress and free radicals, which is an important pathogenesis of post-stroke depression.39–42 There is now growing evidence that serum bilirubin plays a beneficial role in antioxidant, anti-inflammatory and cellular protection in the body, especially the human brain.43–46 Serum direct bilirubin, as an important antioxidant in central nervous system, has a powerful antioxidant protective effect against free radical damage after acute stroke.38,44,45 The imbalance between antioxidants and oxidant activity in patients with low serum direct bilirubin would be not conductive to the antioxidant capacity that protect body from ischemic injury. Moreover, Gao et al believe that lower levels of serum bilirubin were related to greater stroke severity, which induces stronger oxidative stress.38 Further studies about the relationship between serum bilirubin and PSD will be required.
The APTT represents the time of intrinsic coagulation. The APTT test reflects the activities of coagulation factors like factor XII, XI, IX, and VIII in the intrinsic procoagulant pathway.47 Different from previous studies, we had found that prolonged APTT played a role in persistent depression after stroke. However, APTT was considered having no significant relationship with depression in a research of blood coagulation and major depression.48 Another research about the patients with CHD found that shorter APTT represented higher perception of stress, which could worsen the cardiovascular prognosis.49 Similarly, researchers had demonstrated that shortened APTT was associated with stroke severity and functional outcome,50 while in the group of persistent depression after stroke in our study, patients were found to have prolonged APTT, more severe stroke and unfavorable prognosis. Despite this, we speculated that the correlation between prolonged APTT and persistent PSD observed in our study may be explained by increasing hemorrhagic transformation. Prolongation of APTT was reported to be associated with the risk of hemorrhagic transformation in ischemic stroke patients after thrombolysis, which could aggravate the stroke severity and worsen functional outcome.51 While on the contrary, in the research of stroke patients who did not receive thrombolysis, APTT was not significant in relation to hemorrhagic transformation.52 Thus, the mechanisms are still not well understood and need further study.
To the best of our knowledge, this is the first multicenter prospective cohort study to research the predictors of persistent depression in the first-year time course after stroke with a relatively large sample size. We discovered several predictive factors associated with persistent PSD, and developed a nomogram for the prediction realization. Moreover, we demonstrated the clinical applicability of the nomogram by decision curve analysis. However, several limitations of this study need to be addressed. First, several patients were excluded from our study for the reason of dementia or aphasia at admission, and yet these patients may had experienced more severe strokes. Thus, patients included in our study may have a relatively mild stroke attack with a mean NIHSS score of 4, and the NIHSS score was 0–21. This might explain why there was no significant association between NIHSS score and persistent PSD in the multivariate analysis in our study to some extent. Second, no comparison of the baseline characteristics was made between the patients lost at follow-up and those be included in the analysis. Third, the study failed to record and analyze the relationship between antidepressant therapy and the type of depression or functional prognosis after stroke. Last, though the C-index of nomogram was not that desirable which only reached 0.655±0.039, the decision curve analysis demonstrated that the model was of satisfactory clinical use.
Conclusions
We found that persistent depression after stroke in the first-year time course after stroke was associated with HAMD-17 score at admission, lower serum direct bilirubin and FT4 level, and APTT. A nomogram was developed with advisable clinical usefulness in our study. However, further investigations either in basic science or in clinical research are required to confirm these findings.
Data Sharing Statement
The data and R codes that was used to generate the results can be made available upon request from corresponding authors.
Ethics Approval and Informed Consent
The research was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (ID: TJ-IRB20171108). Written informed consent was obtained from all subjects or their caregivers.
Author Contributions
All authors met the following conditions:
- Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
- Drafted or wrote, or substantially revised or critically reviewed, the article.
- Agreed on the journal to which the article will be submitted.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Funding
This work was financially supported by the National Key Research & Development Program of China [grant number 2017YFC1310000], Hubei Technological Innovation Special Fund [grant number 2019ACA132], National Natural Science Fund of China [grant numbers 82101605, 82001218, 82171465]. The funders had no role in study design, data collection and analysis, decision to publish.
Disclosure
All authors declare no competing interests in the work.
References
1. Hadidi N, Treat-Jacobson DJ, Lindquist R. Poststroke depression and functional outcome: a critical review of literature. Heart Lung. 2009;38(2):151–162. doi:10.1016/j.hrtlng.2008.05.002
2. Aström M, Adolfsson R, Asplund K. Major depression in stroke patients A 3-year longitudinal study. Stroke. 1993;24(7):976–982.
3. Feigin VL, Krishnamurthi RV, Parmar P, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990–2013: the GBD 2013 study. Neuroepidemiology. 2015;45(3):161–176. doi:10.1159/000441085
4. Angelelli P, Paolucci S, Bivona U, et al. Development of neuropsychiatric symptoms in poststroke patients: a cross-sectional study. Acta Psychiat Scand. 2004;110(1):55–63. doi:10.1111/j.1600-0447.2004.00297.x
5. Zhang N, Wang C-X, Wang A-X, et al. Time course of depression and one-year prognosis of patients with stroke in mainland China. CNS Neurosci Ther. 2012;18(6):475–481. doi:10.1111/j.1755-5949.2012.00312.x
6. Bour A, Rasquin S, Aben I, Boreas A, Limburg M, Verhey F. A one-year follow-up study into the course of depression after stroke. J Nutr Health Aging. 2010;14(6):488–493. doi:10.1007/s12603-010-0033-x
7. Aben I, Verhey F, Strik J, Lousberg R, Lodder J, Honig A. A comparative study into the one year cumulative incidence of depression after stroke and myocardial infarction. J Neurol Neurosurg Psychiatry. 2003;74(5):581–585. doi:10.1136/jnnp.74.5.581
8. Kouwenhoven SE, Kirkevold M, Engedal K, Kim HS. Depression in acute stroke: prevalence, dominant symptoms and associated factors. A systematic literature review. Disabil Rehabil. 2011;33(7):539–556. doi:10.3109/09638288.2010.505997
9. Zeng YY, Wu MX, Geng DD, et al. Early-onset depression in stroke patients: effects on unfavorable outcome 5 years post-stroke. Front Psychiatry. 2021;12:556981. doi:10.3389/fpsyt.2021.556981
10. Gaete JM, Bogousslavsky J. Post-stroke depression. Expert Rev Neurother. 2008;8(1):75–92. doi:10.1586/14737175.8.1.75
11. Whyte EM, Mulsant BH, Vanderbilt J, Dodge HH, Ganguli M. Depression after stroke: a prospective epidemiological study. J Am Geriatr Soc. 2004;52(5):774–778. doi:10.1111/j.1532-5415.2004.52217.x
12. Li LJ, Yao XM, Guan BY, Chen Q, Zhang N, Wang CX. Persistent depression is a predictor of quality of life in stroke survivors: results from a 5-year follow-up study of a Chinese cohort. Chin Med J. 2019;132(18):2206–2212. doi:10.1097/CM9.0000000000000400
13. Shi YZ, Xiang YT, Wu SL, et al. The relationship between frontal lobe lesions, course of post-stroke depression, and 1-year prognosis in patients with first-ever ischemic stroke. PLoS One. 2014;9(7):e100456.
14. Kunitz SC, Gross CR, Heyman A, et al. The pilot stroke data bank: definition, design, and data. Stroke. 1984;15(4):740–746. doi:10.1161/01.STR.15.4.740
15. Uyttenboogaart M, Stewart RE, Vroomen PC, De Keyser J, Luijckx GJ. Optimizing cutoff scores for the Barthel index and the modified rankin scale for defining outcome in acute stroke trials. Stroke. 2005;36(9):1984–1987. doi:10.1161/01.STR.0000177872.87960.61
16. Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006;26(6):565–574. doi:10.1177/0272989X06295361
17. Vickers AJ, Cronin AM, Elkin EB, Gonen M. Extensions to decision curve analysis, a novel method for evaluating diagnostic tests, prediction models and molecular markers. BMC Med Inform Decis Mak. 2008;8(1):53. doi:10.1186/1472-6947-8-53
18. Kramer AA, Zimmerman JE. Assessing the calibration of mortality benchmarks in critical care: the Hosmer-Lemeshow test revisited. Crit Care Med. 2007;35(9):2052–2056. doi:10.1097/01.CCM.0000275267.64078.B0
19. Oni OD, Olagunju AT, Olisah VO, Aina OF, Ojini FI. Post-stroke depression: prevalence, associated factors and impact on quality of life among outpatients in a Nigerian hospital. Sajp-S Afr J Psychi. 2018;24. doi:10.4102/sajpsychiatry.v24i0.1058
20. Shi YZ, Xiang YT, Yang Y, et al. Depression after minor stroke: the association with disability and quality of life - a 1-year follow-up study. Int J Geriatr Psych. 2016;31(4):425–431. doi:10.1002/gps.4353
21. Berg A, Psych L, Palomaki H, et al. Poststroke depression - An 18-month follow-up. Stroke. 2003;34(1):138–143. doi:10.1161/01.STR.0000048149.84268.07
22. Kim ES, Kim JW, Kang HJ, et al. Longitudinal impact of depression on quality of life in stroke patients. Psychiat Invest. 2018;15(2):141–146. doi:10.30773/pi.2017.10.11
23. Ferro JM, Caeiro L, Figueira ML. Neuropsychiatric sequelae of stroke. Nat Rev Neurol. 2016;12(5):269–U48. doi:10.1038/nrneurol.2016.46
24. Hackett ML, Yapa C, Parag V, Anderson CS. Frequency of depression after stroke - A systematic review of observational studies. Stroke. 2005;36(6):1330–1340. doi:10.1161/01.STR.0000165928.19135.35
25. Medeiros GC, Roy D, Kontos N, Beach SR. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiat. 2020;66:70–80. doi:10.1016/j.genhosppsych.2020.06.011
26. Kutlubaev MA, Hackett ML, Part II. predictors of depression after stroke and impact of depression on stroke outcome: an updated systematic review of observational studies. Int J Stroke. 2014;9(8):1026–1036. doi:10.1111/ijs.12356
27. Bauer M, Heinz A, Whybrow PC. Thyroid hormones, serotonin and mood: of synergy and significance in the adult brain. Mol Psychiatry. 2002;7(2):140–156. doi:10.1038/sj.mp.4000963
28. Saravanan P, Visser TJ, Dayan CM. Psychological well-being correlates with free thyroxine but not free 3,5,3’-triiodothyronine levels in patients on thyroid hormone replacement. J Clin Endocrinol Metab. 2006;91(9):3389–3393. doi:10.1210/jc.2006-0414
29. Peng R, Dai W, Li Y. Low serum free thyroxine level is correlated with lipid profile in depressive patients with suicide attempt. Psychiatry Res. 2018;266:111–115. doi:10.1016/j.psychres.2018.05.059
30. Altshuler LL, Bauer M, Frye MA, et al. Does thyroid supplementation accelerate tricyclic antidepressant response? A review and meta-analysis of the literature. Am J Psychiatry. 2001;158(10):1617–1622. doi:10.1176/appi.ajp.158.10.1617
31. Gur E, Lerer B, Newman ME. Chronic clomipramine and triiodothyronine increase serotonin levels in rat frontal cortex in vivo: relationship to serotonin autoreceptor activity. J Pharmacol Exp Ther. 1999;288(1):81–87.
32. Hage MP, Azar ST. The link between thyroid function and depression. J Thyroid Res. 2012;2012:590648. doi:10.1155/2012/590648
33. Taroza S, Rastenytė D, Burkauskas J, Podlipskytė A, Mickuvienė N. Lower serum free triiodothyronine levels are associated with symptoms of depression after ischemic stroke. J Psychosom Res. 2019;122:29–35. doi:10.1016/j.jpsychores.2019.04.018
34. Abulseoud O, Sane N, Cozzolino A, et al. Free T4 index and clinical outcome in patients with depression. J Affect Disorders. 2007;100(1–3):271–277. doi:10.1016/j.jad.2006.10.012
35. Cole DP, Thase ME, Mallinger AG, et al. Slower treatment response in bipolar depression predicted by lower pretreatment thyroid function. Am J Psychiatry. 2002;159(1):116–121. doi:10.1176/appi.ajp.159.1.116
36. You J, Feng L, Xin M, Ma D, Feng J. Cerebral ischemic postconditioning plays a neuroprotective role through regulation of central and peripheral glutamate. Biomed Res Int. 2018;2018:6316059. doi:10.1155/2018/6316059
37. Tang WK, Liang HJ, Chu WCW, Mok V, Ungvari GS, Wong KS. Association between high serum total bilirubin and post-stroke depression. Psychiat Clin Neuros. 2013;67(4):259–264. doi:10.1111/pcn.12051
38. Gao J, Xu W, Han K, Zhu L, Gao LL, Shang XL. Changes of serum uric acid and total bilirubin in elderly patients with major postischemic stroke depression. Neuropsych Dis Treat. 2018;14:83–93. doi:10.2147/NDT.S149712
39. Nanetti L, Raffaelli F, Vignini A, et al. Oxidative stress in ischaemic stroke. Eur J Clin Invest. 2011;41(12):1318–1322.
40. Palta P, Samuel LJ, Miller ER, Szanton SL. Depression and oxidative stress: results from a meta-analysis of observational studies. Psychosom Med. 2014;76(1):12–19. doi:10.1097/PSY.0000000000000009
41. Miyaoka T, Yasukawa R, Yasuda H, et al. Urinary excretion of biopyrrins, oxidative metabolites of bilirubin, increases in patients with psychiatric disorders. Eur Neuropsychopharmacol. 2005;15(3):249–252. doi:10.1016/j.euroneuro.2004.11.002
42. Maes M, Galecki P, Chang YS, Berk M. A review on the oxidative and nitrosative stress (O&NS) pathways in major depression and their possible contribution to the (neuro) degenerative processes in that illness. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(3):676–692. doi:10.1016/j.pnpbp.2010.05.004
43. Thakkar M, Edelenbos J, Bilirubin DS. Ischemic stroke: rendering the current paradigm to better understand the protective effects of bilirubin. Mol Neurobiol. 2019;56(8):5483–5496. doi:10.1007/s12035-018-1440-y
44. Wang X, Wu D, Zhong P. Serum bilirubin and ischaemic stroke: a review of literature. Stroke Vasc Neurol. 2020;5(2):198–204. doi:10.1136/svn-2019-000289
45. Zhong P, Wu D, Ye X, et al. Association of circulating total bilirubin level with ischemic stroke: a systemic review and meta-analysis of observational evidence. Ann Transl Med. 2019;7(14):335. doi:10.21037/atm.2019.06.71
46. Vasavda C, Kothari R, Malla AP, et al. Bilirubin links heme metabolism to neuroprotection by scavenging superoxide. Cell Chem Biol. 2019;26(10):1450–60 e7. doi:10.1016/j.chembiol.2019.07.006
47. White GC
48. Maes M, Van der Planken M, Van Gastel A, Desnyder R. Blood coagulation and platelet aggregation in major depression. J Affect Disord. 1996;40(1–2):35–40. doi:10.1016/0165-0327(96)00044-4
49. Yin H, Cheng X, Liang Y, et al. High perceived stress may shorten activated partial thromboplastin time and lead to worse clinical outcomes in patients with coronary heart disease. Front Cardiovasc Med. 2021;8:769857. doi:10.3389/fcvm.2021.769857
50. Lin CH, Kuo YW, Kuo CY, et al. Shortened activated partial thromboplastin time is associated with acute ischemic stroke, stroke severity, and neurological worsening. J Stroke Cerebrovasc Dis. 2015;24(10):2270–2276. doi:10.1016/j.jstrokecerebrovasdis.2015.06.008
51. Wang R, Zeng J, Wang F, Zhuang X, Chen X, Miao J. Risk factors of hemorrhagic transformation after intravenous thrombolysis with rt-PA in acute cerebral infarction. QJM. 2019;112(5):323–326. doi:10.1093/qjmed/hcy292
52. Ye C, Wang Y, Song Q, Liu J, Wei C, Liu M. Association between coagulation function and spontaneous hemorrhagic transformation in acute ischemic stroke. Curr Neurovasc Res. 2020;17(4):344–353. doi:10.2174/1567202617666200514114258
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.