Back to Journals » Journal of Inflammation Research » Volume 16
Nomogram Based on Hemoglobin, Albumin, Lymphocyte and Platelet Score to Predict Overall Survival in Patients with T3-4N0-1 Nasopharyngeal Carcinoma
Authors Zhao R ![]() , Liang Z, Chen K, Zhu X
, Liang Z, Chen K, Zhu X ![]()
Received 20 March 2023
Accepted for publication 28 April 2023
Published 9 May 2023 Volume 2023:16 Pages 1995—2006
DOI https://doi.org/10.2147/JIR.S411194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Rong Zhao,1 Zhongguo Liang,1 Kaihua Chen,1 Xiaodong Zhu1– 3
1Department of Radiation Oncology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, People’s Republic of China; 2Affiliated Wu-Ming Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 3Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor (Guangxi Medical University), Ministry of Education/Guangxi Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Nanning, Guangxi, People’s Republic of China
Correspondence: Xiaodong Zhu, Email [email protected]
Purpose: There is still uncertainty regarding the prognosis of nasopharyngeal carcinoma (NPC) based on hemoglobin, albumin, lymphocytes, and platelets (HALP) score. The aim of this study was to build and verify a nomogram using HALP score to investigate the prognostic value of NPC and identify low-risk patients in T3-4N0-1 NPC to guide treatment options.
Patients and methods: A total of 568 NPC patients with stage T3-4N0-1M0 were recruited in the study, who were given either concurrent chemoradiotherapy (CCRT) or induction chemotherapy (IC) plus CCRT. The prognostic factors of overall survival (OS) were picked by Cox proportional hazards regression analysis to generate a nomogram, which appraised by discrimination, calibration and clinical utility. Patients were stratified according to risk scores calculated by the nomogram, and compared to the 8th TNM staging system using the Kaplan–Meier methods.
Results: Multivariate analysis showed that TNM stage, Epstein–Barr virus DNA (EBV DNA), HALP score, lactate dehydrogenase-to-albumin ratio (LAR) and systemic inflammatory response index (SIRI) were independent prognostic indicators for OS, and these factors contained in the nomogram. The nomogram demonstrated a significant enhancement over the 8th TNM staging system in terms of assessing OS (C-index, 0.744 vs 0.615 in the training cohort, P < 0.001; 0.757 vs 0.646 in the validation cohort, P = 0.002). Calibration curves displayed good agreement and the stratification in high-risk and low-risk groups resulted in a significant divergence of Kaplan–Meier curves for OS (P < 0.001). In addition, the decision analysis (DCA) curves confirmed satisfactory discriminability and clinical utility.
Conclusion: The HALP score was an independent prognostic factor for NPC. The prognostic function of the nomogram for T3-4N0-1 NPC patients was more accurate compared to the 8th TNM system, facilitating personalized treatment planning.
Keywords: Epstein–Barr virus, induction chemotherapy, concurrent chemoradiotherapy, locoregional extension patterns, immunoinflammatory marker
Introduction
Nasopharyngeal carcinoma (NPC), a type of the malignant tumor in head and neck, is characterized by unique, unbalanced, endemic distribution, predominantly in southeast Asia.1 It is presumed that there were 133354 new patients of NPC worldwide in 2020, and in excess of 70% of them were classified as locoregionally advanced NPC (LA-NPC), with a 5-year overall survival (OS) of 68.9–78.6%.2–4 In the National Comprehensive Cancer Network (NCCN) guidelines, concurrent chemoradiotherapy (CCRT) is essential for the treatment of patients with LA-NPC, adding induction chemotherapy (IC) or adjuvant chemotherapy (AC) to CCRT is imperative for certain high-risk groups, particularly for patients with bulky or extensive lymph node who have higher metastatic probability.5 Moreover, according to the 2021 CSCO (Chinese Society of Clinical Oncology) Guidelines for NPC,6 CCRT is recommended for grade I treatment in T3N0 patients, which means most of T3N0 patients are low-risk LA-NPC who do not have to receive IC. Hence, it is significant to explore ways to distinguish high- and low-risk patients and to give more rational treatment. In terms of the regional extension patterns (LEPs), LA-NPC can be categorized into three types with distinct clinical differences in biological behavior, the ascending type (T3-4N0-1, or type A), descending type (T1–2N2-3, or type D), and the mixed type (T3-4N2-3, or type AD). The ascending type of NPC showed superior local recurrence free survival (LRFS) and distant metastasis free survival (DMFS) than the descending and mixed types, at 90.7% and 89.9%, respectively, according to a retrospective study involving 7227 patients.7 Considering the early stage of lymph node metastasis in T3-4N0-1 patients, it is reasonable to assume that low-risk patients are more likely to be present in T3-4N0-1 patients. We established the nomogram in T3-4N0-1 patients to more accurately identify low-risk patients and exempt them from IC and its adverse effects and financial burden.
Inflammation is a major component of tumor microenvironment that substantially contributes to proliferation of tumor cells, metastasis, stimulation of angiogenesis, subvert immunity, and resistance to chemotherapy.8,9 Previous studies have shown that inflammatory factors are related to tumor prognosis. For example, systemic immune inflammation index (SII) and systemic inflammatory response index (SIRI) have been confirmed to be related to poor OS and progression free survival (PFS) in patients with NPC.10,11 In addition, nutritional status is closely associated with treatment-related prognosis, therapeutic responses and complications in various cancer types.12 Serum albumin (ALB) is a classical nutritional status assessment indicator, which can reliably evaluate the nutritional status of cancer patients. The reduction of ALB level predicts poor prognosis of various cancers.13 Furthermore, there exist a complex and dynamic interaction between immune environment and tumor cell, and immune biomarkers reveal prognosis of cancer.14 Lymphocytes, a crucial type of immune cell, take part in immune monitoring of the proliferation, invasion and metastasis of tumor cells.15 Lymphocyte count decrease is a sign of poor prognosis for cancer.16,17 Low hemoglobin levels reflect tumor hypoxia, which can reduce the efficacy of radiotherapy.18 Platelet is associated with metastasis, which can defend cancer cells from immune assault.19 The hemoglobin, albumin, lymphocyte and platelet (HALP) scores, a combination of inflammatory, nutritional and immune status, have been demonstrated to be a useful prognostic indicator for several malignancies, such as bladder cancer, gastrointestinal stromal tumor, esophageal squamous cell carcinoma and so on.20–22 However, it remains unclear that the prognostic value of the HALP score in NPC patients and the clinical value of HALP scores in conjunction with other prognostic factors.
Hence, the objective of this study was to explore whether the HALP scores could be a parameter to predict the prognosis of NPC. In addition, we set up and verify a nomogram based on HALP scores and other immunoinflammatory indicators to predict OS and stratified de novo T3-4N0-1 NPC patients prior to therapy initiation and identify potential beneficiaries receiving CCRT alone.
Methods
Patients
We conducted a retrospective review of NPC patients who received CCRT with or without IC between 2011 and 2019. Patients were recruited in terms of the following criteria: (a) age from 18 to 65 years at the time of diagnosis; (b) histopathology substantiated NPC; (c) defined as T3-4N0-1M0 according to the 8th TNM staging system; (d) treatment regimens were CCRT with or without IC. Patients were excluded based on the following criteria: (a) previous history of tumor or concurrent diagnosis of double or multiple cancers; (b) absence of values in relevant indicators or survival data. Eventually, a total of 568 patients met criteria for analysis. This study was endorsed by the Ethics Committee of Guangxi Medical University Cancer Hospital (IRB approval number: LW2023048), and was not required informed consent as a consequence of retrospective nature. Data was anonymized for protecting the privacy of the participants. It was conducted in compliance with the principles of Declaration of Helsinki.
Treatment
A thorough history taking and physical examination were essential prior to treatment, and the general condition was assessed by blood tests. Besides, the pathology was clarified by obtaining tissue through nasopharyngoscopy, and the extent of tumor invasion was ascertained by magnetic resonance imaging (MRI) of the head and neck, eliminated distant metastases by chest and abdominal computed tomography (CT), skeletal emission computed tomography (ECT), or 18Ffluorodeoxyglucose positron emission tomography-CT (PET/CT). The TNM stage of patients were reclassified according to the 8th edition by three radiologists with more than 10 years of experience independently. The ascending NPC is described as patients with predominantly advanced localised lesions (T3-4) but early cervical lymphadenopathy in the neck (N0-1).
All patients underwent IMRT. The target volumes were demarcated in reference to the International Commission on Radiation Units and Measurements Reports 50 and 62. The prescribed radiation dose was 70~75.9 Gary for the primary nasopharyngeal tumor and 60~73.6 Gary for the cervical metastatic lymph node in 30–32 fractions. The IC regimens consisted of GP (cisplatin 80 mg/m2, 1st day; gemcitabine 1000 mg/m2, 1st and 8th days), and TPF (docetaxel 60 mg/m2, 1st day; cisplatin 60 mg/m2 1st day; 5-fluorouracil 600 mg/m2, day one to day five) repeated every 3 weeks for a total of two or three cycles. The regimen for concurrent chemotherapy was cisplatin (100 mg/m2) delivered for 2–3 cycles, every 3 weeks during radiation therapy.23,24
Immunoinflammatory Markers
Hematology samples were collected within 1 week prior to treatment. The Epstein–Barr virus deoxyribonucleic acid (EBV DNA) was assayed by a real-time quantitative polymerase chain-reaction assay. The calculation formula of immunoinflammatory biomarkers are as described below:
HALP (hemoglobin, albumin, lymphocyte and platelet) score = hemoglobin (g/L) × serum albumin (g/L) × lymphocyte count (109/L)/platelet count (109 /L);
SIRI (systemic inflammatory response index) = monocyte count (109/L) × neutrophil count (109/L)/lymphocyte count (109/L);
SII (systemic immune inflammation index) = platelet count (109/L) × neutrophil count (109/L)/lymphocyte count (109/L);
LAR (lactate dehydrogenase-to-albumin ratio) = lactate dehydrogenase (U/L)/serum albumin (g/L).
Survival Data
The primary endpoint was overall survival (OS), measured from the diagnosis to death or last visit. After completing radiotherapy, patients were followed up at least every 3 months for first 3 years, every 6 months for 3 to 5 years, and then annually thereafter until death, which included a physical examination, indirect nasopharyngoscopy and relevant imaging.
Statistical Analysis
The patients were stochastically assigned into training cohort and validation cohort in a proportion of nearly 7:3 (caret, version 6.0–90). Categorical variables were compared with the chi-square test, and the Mann Whitney U-test was applied to compare continuous variables. The cut-off level of pre-treatment EBV DNA was based on a value 5000 copies/mL, which was specified by the laboratory in the hospital. In addition, receiver operation characteristic (ROC) curve analysis (pROC, version 1.18.0) was utilized to discern the cut-off value of continuous variables for OS in training cohort, and then continuous variables converted to binary variables in the whole population depending on these cut-off values (Supplementary Figure 1). Univariate cox regression analysis was employed to evaluate the association between variables and OS. Factors with P < 0.1 in the univariate cox analysis were fed into the multivariate analysis, and the independent prognostic variables with a final P < 0.05 were employed to create the nomogram (rms, version 6.2–0).25,26 Prognostic performance of the proposed model and TNM stage were assessed by Harrell’s concordance index (C-index). The calibration curves were plotted to estimate the agreement in the observed survival with the nomogram-predicted survival. Furthermore, decision curve analysis (DCA) was utilized to appraise the value of the nomogram for clinical application (ggDCA, version 1.2). The total risk scores were acquired via the nomogram, and patients were separated into high-risk and low-risk groups depending on the cut-off value of the risk scores obtained in ROC curve. Survival curves were developed on the basis of Kaplan–Meier (KM) method. The p-value of hazard ratio (HR) estimate was derived with the Log rank test. R software (version 4.0.3) was carried out to conduct statistical analysis. A two-sided p < 0.05 indicating that the corresponding estimate reaches significant difference.
Results
Clinical Features
A total of 568 patients with ascending type NPC were ascertained (Table 1 and Supplementary Table 1), consisting of 400 patients in the training cohort and 168 patients in the validation cohort. There was no difference observed between the training and validation groups, aside from EBV DNA. Median follow-up was 50 months (range 2–126), and the 3-year and 5-year OS was 90.6%, 79.7%, respectively.
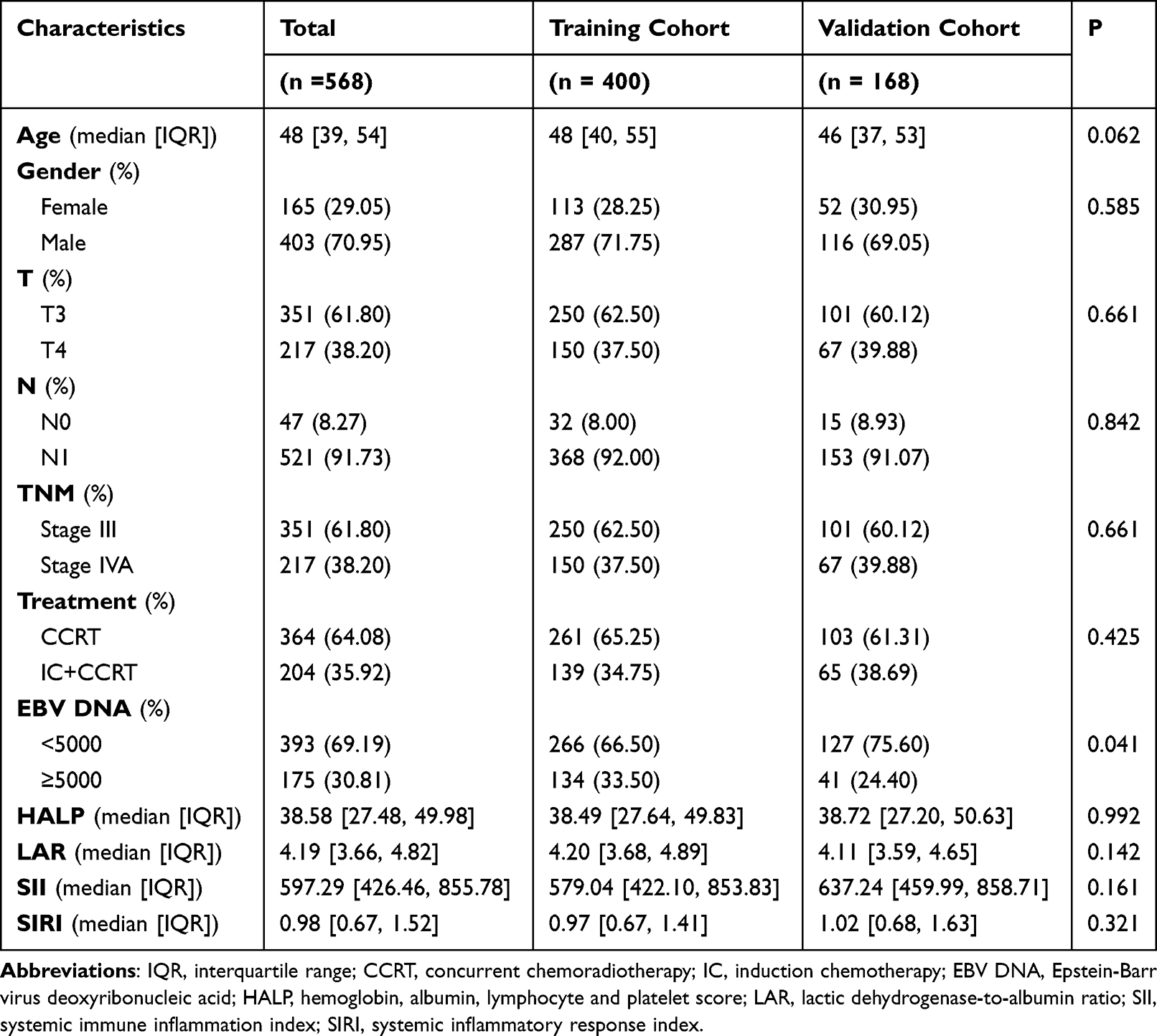 |
Table 1 Clinical Characteristics of Patients in the Training and Validation Cohorts |
Survival Analysis in Training Cohort
The univariate analysis revealed that older age, stage IVA, detectable pre-treatment EBV DNA, high HALP, high LAR and high SIRI were correlated with poorer OS (Table 2). The multivariate analysis demonstrated that patient TNM stage (stage III or IVA), pre-treatment EBV DNA (<5000 or ≥5000 copies/mL), HALP (<46.61 or ≥46.61), LAR (<4.52 or ≥4.52) and SIRI (<2.06 or ≥2.06) remained the significant prognostic factors.
 |
Table 2 Risk Factors for OS in the Training Cohort |
Construction, Validation and Comparison of the Models
All independent prognostic factors were integrated into our nomogram (Figure 1). In the training cohort, the C-index was 0.744 (95% CI: 0.681–0.806) for the nomogram, and 0.615 (95% CI: 0.554–0.676) for the 8th TNM system (P < 0.001, Supplementary Table 2). In the validation cohort, the C-index reached 0.757 (95% CI: 0.673–0.840) for our nomogram, and 0.646 (95% CI: 0.560–0.731) for the TNM system (P = 0.002). The calibration curves, measured by bootstrap verification with 1000 resamples, presented an acceptable agreement between the nomogram-predicted value and actual value for 3- and 5-year OS in the training cohort and validation cohort (Figure 2). The DCA curve suggested a higher net benefit for the nomogram than the TNM staging system which indicated that the nomogram had superior clinical utility (Figure 3).
 |
Figure 1 OS Nomogram in the Training Cohort. Abbreviations: OS, overall survival; EBV DNA, Epstein-Barr virus deoxyribonucleic acid; HALP, hemoglobin, albumin, lymphocyte and platelet score; LAR, lactic dehydrogenase-to-albumin ratio; SIRI, systemic inflammatory response index. Notes: The line segment corresponding to each variable is marked with a scale, which represents the range of possible values of the variable and draws a vertical line upward to get the corresponding score. Add all the variables to get the total score and draw a vertical line downward to get the probability of survival of OS at 3 or 5 years. |
 |
Figure 2 Calibration Curve Graphs for Nomogram of OS. Abbreviation: OS, overall survival. Notes: Calibration curve graphs to predict the 3 and 5-year OS of the nomogram in the training cohort (A and C) and validation cohort (B and D). Nomogram-estimated OS were drawn on the abscissa; the observed OS were drawn on the ordinate. The diagonal representing the predicted probability was equal to the actual probability. The closer the nomogram curve is to the diagonal line, the more closely the predicted probability matches the actual probability. |
 |
Figure 3 Decision Curves of Nomogram and 8th TNM Staging System. Notes: Decision curves to predict the 3 and 5-year overall survival in the training cohort (A and C) and validation cohort (B and D). The x-axis was determined by the threshold probability, at which the harm of false-positive intervention exceeded the harm of a false-negative non-intervention, and thus an intervention was triggered. The y-axis was a net benefit, which was the relative benefit derived from the proportion of true-positive results subtracted from the proportion of false-positive results weighted by a ratio of threshold probabilities. Under the same probability, the clinical usefulness was better when the net benefit was higher. |
Risk Stratification
Patients were classified into high-risk group (≥153 scores) and low-risk group (<153 scores) according to risk scores (Supplementary Table 3). Significant discrimination in OS between the low-risk and high-risk groups was apparent in the training (P < 0.001) and validation cohort (P < 0.001, Figure 4), which means risk stratification can effectively identify patients at a high risk of death from NPC. Moreover, the KM curves displayed a greater difference in risk stratification for nomogram compared to the TNM system.
 |
Figure 4 Kaplan–Meier Curves Demonstrating OS in T3-4N0-1 of Nasopharyngeal Carcinoma Patients. Abbreviation: OS, overall survival. Notes: Kaplan–Meier survival curves for OS of the training cohort (A and B) and validation cohort (C and D) in different models. The nomogram was divided into a high-risk group and a low-risk group comparison (B and D); AJCC/UICC 8th staging system was divided into stage III and stage IVA comparisons (A and C). |
Discussion
The role of IC in LA-NPC is still controversial. Several clinical trails showed there was no significant difference in OS, DMFS and disease-free survival (DFS) between CCRT and IC+CCRT in LA-NPC.27–29 Nevertheless, when target population of the clinical trails covered all LA-NPC except for T3N0–1 or T3–4N0 subgroups, it was found that IC+CCRT achieved higher OS or DFS than CCRT alone, which suggested that there was a subset of LA-NPC patients regarded as low-risk group and additional IC to CCRT may be futile for these patients.23,24,30 Patients with the ascending type, whose primary failure mode was local recurrence rather than distant metastasis, had a significantly better prognosis than those with descending type and the mixed type among LA-NPC.31,32 In addition, some studies indicated that the incorporation of IC into CCRT in NPC patients with stage T3-4N0-1 did not significantly enhance OS, LRFS, DMFS and PFS.32–34 It is currently unknown which T3-4N0-1 patients require IC. Hence, we created a nomogram to predict OS for T3-4N0-1 patients and then stratified patients at risk to provide evidences for the choices of IC.
Systemic inflammatory responses can forecast survival in cancer patients as they are engaged in crucial steps of tumor formation.35 It is illustrated that inflammatory cells interact with cancer to facilitate neo-vascular formation, extracellular matrix remodeling and a sustained inflammatory microenvironment to stimulate metastasis.36 Inflammatory status can be estimated by different clinical hematological variables, responding the dynamic balance between the tumor function and the immune system. It demonstrated that SIRI was significantly associated with PFS and OS in patients with NPC.37,38
Moreover, LAR is the ratio of lactate dehydrogenase to albumin. LDH is an indicator of tumor load, and the larger the LDH, the higher the risk of metastasis.39 Albumin can assess the nutritional status of NPC patients, and low albumin predicts poor survival.40 When patients have high LDH and low albumin, namely large LAR, it indicates a high tumor load, poor nutritional status and poor prognosis. Previous researches showed that LAR was significantly related to a relatively short OS and PFS in NPC.41,42 These findings illustrated the adverse effects of nutritional deficiencies on survival of patients with NPC and the importance of nutritional interventions.
Furthermore, HALP scores, combination of hemoglobin, albumin, lymphocyte and platelet, reflect inflammatory status and the anti-tumor function of the immune system. Low HALP predicts worse survival in many cancers.43,44 A meta-analysis comprising 13,038 patients showed that a low HALP score was associated with decreased OS in patients with solid tumors.45 The prognostic value of HALP on OS was observed across different stages and types of tumors. In hematologic tumors, low HALP is associated with adverse clinicopathological features of diffuse large B-cell lymphoma and appears to be an independent adverse prognostic factor for International Prognostic Index.46 Besides, HALP score is a valuable prognostic marker for patients with multiple myeloma.47 A retrospective study with 319 pharyngeal cancer patients including nasopharyngeal carcinoma, oropharyngeal carcinoma and hypopharyngeal carcinoma indicated that HALP score was an independent factor for OS.48 However, the number of patients included in the article was small and each type of tumor was not analyzed separately. In the present study, more patients were included. It demonstrated that HALP may be a new prognostic factor for NPC, and low HALP predicts worse OS. Additionally, the prognostic performance of HALP was better than that of the four components alone or combined.
EBV DNA analysis has proven useful for early detection, monitoring of treatment response, prognostication, and even guiding treatment decisions for NPC.49,50 A recursive partitioning analysis-based TNM staging system and EBV DNA status may promote clinical trial designs and prognostic stratification.51 In this study, EBV DNA combined with TNM stage and immunoinflammatory index model greatly improved performance and allowed for good identification of high-risk patients.
The inadequacy of the study is as follows. First, the prognostic value of HALP needs to be validated in more prospective studies. In addition, this nomogram is only validated internally and requires extensive multi-center or prospective external validation. Besides, this study concentrated on the first diagnosis and treatment of T3-4N0-1 NPC and failed to explore the influence of its salvage treatment on OS.
Conclusion
In summary, our study first demonstrated that HALP is a promising predictor of survival outcome in NPC. Moreover, we created and verified a nomogram to predict OS in T3-4N0-1 NPC patients, which involved TNM stage, pre-EBV-DNA, HALP, LAR and SIRI. The nomogram showed outstanding consistent and discriminatory to categorize NPC patients into high-risk and low-risk groups, which can offer useful clues for doctors to recognize the high-risk NPC patients and in opting for IC treatments.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Key Research and Development Program Project of Guangxi Zhuang Autonomous Region (Grant No.GuikeAB18221007), Guangxi Colleges and Universities Young and Middle-aged Teachers Research Basic Ability Improvement Project (2022KY0087) and the Independent Project of Key Laboratory of Early Prevention & Treatment for Regional High-Incidence-Tumor (GKE-ZZ202224), the Project of Guangxi Medical and Health Appropriate Technology Development and Extension Application (No. S2018001), Guangxi Natural Science Foundation (No. 2020GXNSFBA159002), the Health Commission of Guangxi Zhuang Autonomous Region (No.Z20200333, NO.Z20191054).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Chen YP, Chan ATC, YS PB, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/S0140-6736(19)30956-0
2. Zhang MX, Li J, Shen GP, et al. Intensity-modulated radiotherapy prolongs the survival of patients with nasopharyngeal carcinoma compared with conventional two-dimensional radiotherapy: a 10-year experience with a large cohort and long follow-up. Eur J Cancer. 2015;51(17):2587–2595. doi:10.1016/j.ejca.2015.08.006
3. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
4. Tang LL, Chen YP, Mao YP, et al. Validation of the 8th Edition of the UICC/AJCC staging system for nasopharyngeal carcinoma from endemic areas in the intensity-modulated radiotherapy era. J Natl Compr Canc Netw. 2017;15(7):913–919. doi:10.6004/jnccn.2017.0121
5. Caudell JJ, Gillison ML, Maghami E, et al. NCCN guidelines(R) insights: head and neck cancers, version 1.2022. J Natl Compr Canc Netw. 2022;20(3):224–234. doi:10.6004/jnccn.2022.0016
6. Tang LL, Chen YP, Chen CB, et al. The Chinese Society of Clinical Oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma. Cancer Commun. 2021;41(11):1195–1227. doi:10.1002/cac2.12218
7. Zhang LL, Huang MY, Fei X, et al. Risk stratification for nasopharyngeal carcinoma: a real-world study based on locoregional extension patterns and Epstein-Barr virus DNA load. Ther Adv Med Oncol. 2020;12:1758835920932052. doi:10.1177/1758835920932052
8. Candido J, Hagemann T. Cancer-related inflammation. J Clin Immunol. 2013;33:S79–84. doi:10.1007/s10875-012-9847-0
9. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
10. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (Siri) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
11. Xiong Y, Shi LL, Zhu LS, Ding Q, Ba L, Peng G. Prognostic efficacy of the combination of the pretreatment systemic immune-inflammation index and Epstein-Barr virus DNA status in locally advanced nasopharyngeal carcinoma patients. J Cancer. 2021;12(8):2275–2284. doi:10.7150/jca.52539
12. Mayne ST, Playdon MC, Rock CL. Diet, nutrition, and cancer: past, present and future. Nat Rev Clin Oncol. 2016;13(8):504–515. doi:10.1038/nrclinonc.2016.24
13. Wei YH, Wang Y, Li H, et al. A nomogram to predict survival in patients with locoregional recurrent nasopharyngeal carcinoma receiving comprehensive treatment. Front Oncol. 2022;12:892510. doi:10.3389/fonc.2022.892510
14. Bruni D, Angell HK, Galon J. The immune contexture and immunoscore in cancer prognosis and therapeutic efficacy. Nat Rev Cancer. 2020;20(11):662–680. doi:10.1038/s41568-020-0285-7
15. Shinko D, Diakos CI, Clarke SJ, Charles KA. Cancer-related systemic inflammation: the challenges and therapeutic opportunities for personalized medicine. Clin Pharmacol Ther. 2017;102(4):599–610. doi:10.1002/cpt.789
16. Jimbo H, Horimoto Y, Ishizuka Y, et al. Absolute lymphocyte count decreases with disease progression and is a potential prognostic marker for metastatic breast cancer. Breast Cancer Res Treat. 2022;196(2):291–298. doi:10.1007/s10549-022-06748-4
17. Park SJ, Lee J, Kim H, et al. Association between absolute lymphocyte count and overall mortality in patients with surgically resected gastric cancer. Korean J Intern Med. 2021;36(3):679–688. doi:10.3904/kjim.2019.358
18. Graham K, Unger E. Overcoming tumor hypoxia as a barrier to radiotherapy, chemotherapy and immunotherapy in cancer treatment. Int J Nanomedicine. 2018;13:6049–6058. doi:10.2147/IJN.S140462
19. Zhang GM, Zhu Y, Luo L, et al. Preoperative lymphocyte-monocyte and platelet-lymphocyte ratios as predictors of overall survival in patients with bladder cancer undergoing radical cystectomy. Tumour Biol. 2015;36(11):8537–8543. doi:10.1007/s13277-015-3613-x
20. Peng D, Zhang CJ, Gong YQ, et al. Prognostic significance of halp (hemoglobin, albumin, lymphocyte and platelet) in patients with bladder cancer after radical cystectomy. Sci Rep. 2018;8(1):794. doi:10.1038/s41598-018-19146-y
21. Zhao Z, Yin XN, Wang J, Chen X, Cai ZL, Zhang B. Prognostic significance of hemoglobin, albumin, lymphocyte, platelet in gastrointestinal stromal tumors: a propensity matched retrospective cohort study. World J Gastroenterol. 2022;28(27):3476–3487. doi:10.3748/wjg.v28.i27.3476
22. Cong L, Hu L. The value of the combination of hemoglobin, albumin, lymphocyte and platelet in predicting platinum-based chemoradiotherapy response in male patients with esophageal squamous cell carcinoma. Int Immunopharmacol. 2017;46:75–79. doi:10.1016/j.intimp.2017.02.027
23. Sun Y, Li W-F, Chen N-Y, et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016;17(11):1509–1520. doi:10.1016/s1470-2045(16)30410-7
24. Zhang Y, Chen L, Hu G-Q, et al. Gemcitabine and cisplatin induction chemotherapy in nasopharyngeal carcinoma. New England J Med. 2019;381(12):1124–1135. doi:10.1056/nejmoa1905287
25. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–80. doi:10.1016/S1470-2045(14)71116-7
26. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
27. Xu T, Zhu G, He X, Ying H, Hu C, Phase III A. Randomized study comparing neoadjuvant chemotherapy with concurrent chemotherapy combined with radiotherapy for locoregionally advanced nasopharyngeal carcinoma: updated long-term survival outcomes. Oral Oncol. 2014;50(2):71–76. doi:10.1016/j.oraloncology.2013.11.002
28. Tan T, Lim WT, Fong KW, et al. Concurrent chemo-radiation with or without induction gemcitabine, carboplatin, and paclitaxel: a randomized, phase 2/3 trial in locally advanced nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2015;91(5):952–960. doi:10.1016/j.ijrobp.2015.01.002
29. Frikha M, Auperin A, Tao Y, et al. A randomized trial of induction docetaxel-cisplatin-5fu followed by concomitant cisplatin-Rt versus concomitant cisplatin-Rt in nasopharyngeal carcinoma (Gortec 2006-02). Ann Oncol. 2018;29(3):731–736. doi:10.1093/annonc/mdx770
30. Cao SM, Yang Q, Guo L, et al. Neoadjuvant chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase iii multicentre randomised controlled trial. Eur J Cancer. 2017;75:14–23. doi:10.1016/j.ejca.2016.12.039
31. Fan Y, Guan W, Huang R, et al. Clinical characteristics and survival outcomes of ascending, descending and mixed types of nasopharyngeal carcinoma in the non-endemic areas of China: a propensity score matching analysis. Cancer Med. 2020;9(24):9315–9325. doi:10.1002/cam4.3537
32. Yao JJ, Qi ZY, Liu ZG, et al. Clinical features and survival outcomes between ascending and descending types of nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: a big-data intelligence platform-based analysis. Radiother Oncol. 2019;137:137–144. doi:10.1016/j.radonc.2019.04.025
33. Lan XW, Xiao Y, Zou XB, Zhang XM, OuYang PY, Xie FY. Outcomes of adding induction chemotherapy to concurrent chemoradiotherapy for stage T3n0-1 Nasopharyngeal carcinoma: a propensity-matched study. Onco Targets Ther. 2017;10:3853–3860. doi:10.2147/OTT.S133917
34. Gabani P, Barnes J, Lin AJ, et al. Induction chemotherapy in the treatment of nasopharyngeal carcinoma: clinical outcomes and patterns of care. Cancer Med. 2018;7(8):3592–3603. doi:10.1002/cam4.1626
35. Hussain SP, Harris CC. Inflammation and cancer: an ancient link with novel potentials. Int J Cancer. 2007;121(11):2373–2380. doi:10.1002/ijc.23173
36. Philip M, Rowley DA, Schreiber H. Inflammation as a tumor promoter in cancer induction. Semin Cancer Biol. 2004;14(6):433–439. doi:10.1016/j.semcancer.2004.06.006
37. Feng Y, Zhang N, Wang S, et al. Systemic inflammation response index is a predictor of poor survival in locally advanced nasopharyngeal carcinoma: a propensity score matching study. Front Oncol. 2020;10:575417. doi:10.3389/fonc.2020.575417
38. Zeng X, Liu G, Pan Y, Li Y. Development and validation of immune inflammation-based index for predicting the clinical outcome in patients with nasopharyngeal carcinoma. J Cell Mol Med. 2020;24(15):8326–8349. doi:10.1111/jcmm.15097
39. Long G, Tang W, Fu X, et al. Pre-treatment serum lactate dehydrogenase predicts distant metastasis and poor survival in nasopharyngeal carcinoma. J Cancer. 2019;10(16):3657–3664. doi:10.7150/jca.32716
40. Oei RW, Ye L, Huang J, et al. Prognostic value of nutritional markers in nasopharyngeal carcinoma patients receiving intensity-modulated radiotherapy: a propensity score matching study. Onco Targets Ther. 2018;11:4857–4868. doi:10.2147/OTT.S165133
41. Peng RR, Liang ZG, Chen KH, Li L, Qu S, Zhu XD. Nomogram based on lactate dehydrogenase-to-albumin ratio (Lar) and Platelet-to-Lymphocyte Ratio (Plr) for predicting survival in nasopharyngeal carcinoma. J Inflamm Res. 2021;14:4019–4033. doi:10.2147/JIR.S322475
42. Miao S, Lei H, Li X, et al. Development and validation of a risk prediction model for overall survival in patients with nasopharyngeal carcinoma: a prospective cohort study in China. Cancer Cell Int. 2022;22(1):360. doi:10.1186/s12935-022-02776-8
43. Jiang P, Kong W, Gong C, et al. Predicting the recurrence of operable cervical cancer patients based on hemoglobin, albumin, lymphocyte, and platelet (Halp) score and classical clinicopathological parameters. J Inflamm Res. 2022;15:5265–5281. doi:10.2147/JIR.S383742
44. Guc ZG, Alacacioglu A, Kalender ME, et al. Halp score and gnri: simple and easily accessible indexes for predicting prognosis in advanced stage NSCLC patients. the izmir oncology group (Izog) study. Front Nutr. 2022;9:905292. doi:10.3389/fnut.2022.905292
45. Xu H, Zheng X, Ai J, Yang L. Hemoglobin, albumin, lymphocyte, and platelet (Halp) score and cancer prognosis: a systematic review and meta-analysis of 13,110 patients. Int Immunopharmacol. 2023;114:109496. doi:10.1016/j.intimp.2022.109496
46. Vlatka P, Marko L, Stefan M, Dorian L. The hemoglobin, albumin, lymphocyte, and platelet (Halp) score is a novel prognostic factor for patients with diffuse large B-cell lymphoma. J Cancer Res Ther. 2022;18(3):725–732. doi:10.4103/jcrt.jcrt_174_21
47. Solmaz S, Uzun O, Sevindik OG, et al. The effect of haemoglobin, albumin, lymphocyte and platelet score on the prognosis in patients with multiple myeloma. Int J Lab Hematol. 2023;45(1):13–19. doi:10.1111/ijlh.13958
48. Wu CY, Lin YH, Lo WC, et al. Nutritional status at diagnosis is prognostic for pharyngeal cancer patients: a retrospective study. Eur Arch Otorhinolaryngol. 2022;279(7):3671–3678. doi:10.1007/s00405-021-07222-5
49. Chan ATC, Hui EP, Ngan RKC, et al. Analysis of plasma Epstein-Barr virus DNA in nasopharyngeal cancer after chemoradiation to identify high-risk patients for adjuvant chemotherapy: a randomized controlled trial. J Clin Oncol. 2018;36(31):3091–3100. doi:10.1200/jco.2018.77.7847
50. Chen FP, Luo YS, Chen K, et al. Circulating Epstein-Barr virus DNA level post induction chemotherapy contributes to prognostication in advanced-stage nasopharyngeal carcinoma. Eur J Cancer. 2021;151:63–71. doi:10.1016/j.ejca.2021.03.052
51. Li W-Z, Wu H-J, Lv S-H, et al. Assessment of survival model performance following inclusion of Epstein-Barr virus DNA status in conventional TNM staging groups in Epstein-Barr virus–related nasopharyngeal carcinoma. JAMA Network Open. 2021;4(9):e2124721. doi:10.1001/jamanetworkopen.2021.24721
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.