Back to Journals » International Journal of General Medicine » Volume 14
No Independent Influence of Statins on the Chronic Obstructive Pulmonary Disease Exacerbation Rate: A Cohort Observation Study Over 10 Years
Authors Yayan J ![]() , Bald M, Franke KJ
, Bald M, Franke KJ
Received 5 March 2021
Accepted for publication 10 June 2021
Published 28 June 2021 Volume 2021:14 Pages 2883—2892
DOI https://doi.org/10.2147/IJGM.S309647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Josef Yayan,1,2 Markus Bald,2 Karl-Josef Franke1,2
1Witten/Herdecke University, Witten, Germany; 2Department of Internal Medicine, Pulmonary Division, Internal Intensive Care Medicine, Infectiology, and Sleep Medicine, Märkische Clinics Health Holding Ltd, Clinic Lüdenscheid, Lüdenscheid, Germany
Correspondence: Josef Yayan
Department of Internal Medicine, Pulmonary Division, Internal Intensive Care Medicine, Infectiology, and Sleep Medicine, Märkische Clinics Health Holding Ltd, Clinic Lüdenscheid, Witten/Herdecke University, Paulmannshöher Str. 14, Lüdenscheid, 58515, Germany
Tel +49 02351 46-3360
Fax +49 02351 46-3366
Email [email protected]
Purpose: Some previously published primarily retrospective studies have shown that statins could reduce the rate and severity of exacerbations, the length of hospital stays, and mortality in patients with chronic obstructive pulmonary disease (COPD), but retrospective data needs to be reviewed regarding this connection since statins are cholesterol-lowering drugs. Therefore, the aim of this study was to investigate the independent influence of statins on the exacerbation rate in COPD patients.
Methods: An observational retrospective study was conducted to assess the independent influence of statins on the COPD exacerbation rate at the Department of Internal Medicine, Pulmonary Division, Internal Intensive Care Medicine, Infectiology, and Sleep Medicine, Märkische Clinics Health Holding Ltd, Clinic Lüdenscheid, Witten/Herdecke University from January 1, 2010 to December 31, 2020. This study enrolled patients with COPD in 2010 and documented their exacerbation rate over a further 10 years. The number of exacerbations in COPD patients was compared between statin users and non-users.
Results: Of the total of 295 [176 male (59.7%)] COPD patients, 105 (35.6%, CI 30.3– 41.2%) patients with COPD were treated with statins, and 190 (64.4%, CI 58.8– 69.7%) were treated without statins. The mean exacerbation rate in the COPD patients who received statin did not differ from that in the COPD patients who did not receive statin (p = 0.175). Also, the mortality rates did not differ between the statin-treated and non-statin-treated COPD patients (p = 0.271).
Conclusion: Statins have no effect on the exacerbation rate or mortality in COPD patients.
Keywords: chronic obstructive pulmonary disease, statins, exacerbation, infection prophylaxis, death
Introduction
Statins are a group of active agents that inhibit endogenous cholesterol synthesis.1 These drugs are used to treat hypercholesterolemia to prevent cardiovascular diseases, such as stroke, heart attack, and vascular diseases.2 The different types of statins include the following: atorvastatin, cerivastatin, fluvastatin, lovastatin, mevastatin, pravastatin, and simvastatin.3 These substances influence lipid metabolism in various ways: via the competitive inhibition of the key enzyme in cholesterol synthesis, 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMG-CoA reductase); by reducing cholesterol biosynthesis in the liver; by increasing the concentration of low-density lipoprotein receptors in the liver cells; and through the modification of lipoproteins.1 Statins have a major influence on the composition of serum lipids, including a strong lowering effect of the low-density lipoprotein cholesterol concentration and a slight increase in the high-density lipoprotein concentration.4 There are also some potential pleiotropic effects of statins, such as improvements in endothelial dysfunction, the stabilization of atherosclerotic plaques, anti-inflammatory effects, and the reduction and stabilization of the lipid core.5 The reduction of the large lipid core and the decrease in inflammatory activity are probably of the greatest importance in this case.6 The anti-inflammatory and antioxidant effects of statins can also help chronic obstructive pulmonary disease (COPD) patients at risk of exacerbation.7,8 In practice, however, the benefits of statins in lowering the rate of exacerbations have been shown to be limited.7,8 According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD), COPD is a preventable and treatable disease of the airways that is associated with a restriction in airflow.9 The disease is progressive and associated with a chronic inflammatory response of the lungs to harmful particles or gases.9 There have been different study results published in the medical literature thus far. According to an analysis published in the New England Journal of Medicine, statins have no effect on the exacerbation rate of COPD.10 In contrast, retrospective analyzes have shown a connection between the use of statins and the frequency and severity of COPD exacerbations.11–14 Based on these different study results, to date, it is not yet clear whether patients with COPD can benefit from the anti-inflammatory effects of statins. Therefore, the aim of this study was to investigate the independent influence of statins on the COPD exacerbation rate over a period of ten years.
Materials and Methods
Study Design, Setting, and Data Collection
This observational cohort study retrospectively observed the number of exacerbations in COPD patients receiving and not receiving statin treatment. The study made use of hospital-chart data from the Department of Internal Medicine, Pulmonary Division, Internal Intensive Care Medicine, Infectiology, and Sleep Medicine, Märkische Clinics Health Holding Ltd, Clinic Lüdenscheid, Witten/Herdecke University from 2010 to 2020. Moreover, the study monitored 295 patients with COPD treated at this hospital in 2010, documenting the number of exacerbations between January 1, 2010 and December 31, 2020.
Patients
For this study, all COPD patients were placed into one of two matched cohorts: in cohort 1, all COPD patients received statin treatment, and, in cohort 2, no COPD patients received statin treatment. All patients were reviewed for sex; mean, and median age; as well as length of hospital stay. The number of deaths during hospitalization was recorded in each of the two cohorts. The study participants were mixed in terms of age in both cohorts—with the exception of adolescents younger than 18 years of age and children.
Inclusion and Exclusion Criteria for This Study
The inclusion criteria for participation in this study was COPD patients with a history of exacerbations or other acute illnesses with a reason for admission to this hospital who had been examined via body plethysmography. The study excluded COPD patients who had not undergone a lung function test.
Diagnosis of Chronic Obstructive Pulmonary Disease
The patient’s COPD is classified according to its severity based on the classification of certain lung function parameters according to the guidelines in the 2017 version of the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) I−IV.15–18 In addition, there is a further division of each stage (GOLD A−D) into groups A−D, which is based on the severity of symptoms, including shortness of breath as well as exacerbation degree and exacerbation frequency.19 The overall COPD classification system therefore extends from GOLD I A to GOLD IV D.19 The most common values of spirometry for each study participant, such as forced expiratory volume in one second and the ratio forced expiratory volume in one second to forced vital capacity, were compared as an expression of a mean value between the two cohorts. After collecting the data, the severity of airflow limitation according to GOLD classification stages I A – IV D in patients with chronic obstructive pulmonary disease was compared between the two cohorts. The stage-appropriate COPD therapy was investigated according to the recommendations of the guidelines.20 The drug therapy of COPD is done in the earlier stages I–II according to the clinical symptoms. Asymptomatic patients do not need long-term drug therapy in these stages I–II. In stages III–IV, patients benefit from long-term therapy with inhaled corticosteroids, ideally in combination with long-acting bronchodilators.20 The classification of COPD was carried out in each case in this study according to the latest edition of the International Classification of Diseases (ICD J44.0−J44.9).21
Definition of Exacerbation of Chronic Pulmonary Disease
The signs of an acute exacerbation in the present study groups were defined as sudden, significant worsening of the symptoms of an existing COPD, such as breathlessness, more frequent severe coughing, an increase in coughed up mucus, increased thick mucus, a different mucus color (yellow-green), tiredness, fatigue, or fever.22,23 The individual symptoms of COPD are not examined in detail in this study. They are only used for diagnosis of COPD.
Definition, Effects, Representatives of Statins
Statins are a group of drugs that cause a decrease in the serum concentration of cholesterol through the competitive inhibition of the enzyme HMG-CoA reductase.24 The active agents in the group of statins included in this study were simvastatin, atorvastatin, fluvastatin, and pravastatin.
Comorbidities
A comorbidity is defined as a disease that exists in a study patient in addition to the underlying disease that is in the foreground of the therapy.25 In this study, the number of comorbidities was taken into account if the number was more than nine for each group. However, if the number of comorbidities in one cohort was less than 10, this was taken into account for comparison purposes if, in the other cohort, the number of comorbidities was more than 10.
Inflammatory Laboratory Markers
After sampling in lithium heparin SARSTEDT Monovette® 4.7 mL (orange cap), C-reactive protein (normal value is < 0.6 mg/dL) was measured in human serum and plasma using a standard immunoturbidometric assay on the Atellica® Solution analyzer (Siemens Healthcare Diagnostics, Erlangen, Germany).
The blood leukocyte count (normal range 3600−10,500/µL) was determined after removal in EDTA Monovette® 2.7 mL after cluster analysis in the basophil channel on ADVIA® 2120i hematology system with autoslide (Siemens Healthcare Diagnostics, Erlangen, Germany).
The inflammation values of the blood laboratory were recorded as a mean and median value after taking into account all exacerbations for each study participant.
Statistical Analysis
The different data values were expressed as percent (%) and after the 95% confidence interval (CI) in percent,26 while the continuous numbers were specified as both the median and the range numbers from minimum to maximum as well as the mean and standard deviation (SD).27 The Mann–Whitney U-test for unpaired data was used to calculate age differences, hospital stay length, forced expiratory volume in one second, the ratio of forced expiratory volume in one second to forced vital capacity, inflammation values, the number of study participants with inhaler and steroid treatment, the number of study participants with stage-appropriate COPD therapy, and the number of COPD exacerbations between the two cohorts,28 while a chi-square analysis for the association between two categorical variables was used to calculate the gender differences, the number of severe COPD cases as defined by the GOLD classification system, indication of statin therapy, and the number of comorbidities between the two cohorts.29 The probability of survival was calculated using the Kaplan–Meier method.30 All statistical calculations were carried out as two-tailed, and a p-value of < 0.05 was deemed statistically significant.
Results
This study examined a total of 295 [176 male (59.7%, CI 54.0−65.1%); 119 female (40.3%, CI 34.9−46.0%)] patients with COPD who were treated at the Department of Internal Medicine, Pulmonary Division, Internal Intensive Care Medicine, Infectiology, and Sleep Medicine, Märkische Clinics Health Holding Ltd, Clinic Lüdenscheid, Witten/Herdecke University from January 1, 2010 to December 31, 2020. Of these, 105 (35.6%, CI 30.3−41.2%) patients with COPD were treated with statins (cohort 1), and 190 (64.4%, CI 58.8−69.7%) patients with COPD were treated without statins (cohort 2). The initiation of statin therapy in cohort 1 was mainly in 93 (88.6%, CI 81.8−93.3%) patients with COPD for vascular disease with statistical significance (p = 0.0169); followed by 12 (11.4%, CI 6.7−18.9%) for hypercholesterolemia. In cohort 2, however, treatment was discontinued in 32 (16.8%, CI 12.2−22.8%) patients with COPD due to vascular disease; and statin treatment was not necessary in 13 (6.8%, CI 4.0−11.4%) patients with hypercholesterolemia. There were no significant differences based on gender between the two groups (p = 0.863) (Table 1). There was also no difference in the mean age of the study participants when comparing the two cohorts (p = 0.311) (Table 1). In addition, the mean hospital stay length did not differ significantly between the two cohorts (p = 0.192) (Table 1). The majority of the study participants (81.4%, CI 76.5−85.4%) compared to those who were overweight had a normal weight with statistical significance (p = 0.005) (Table 1). Almost half of the study participants in both cohorts were still smokers with no statistical significance (p = 0.888) (Table 1).
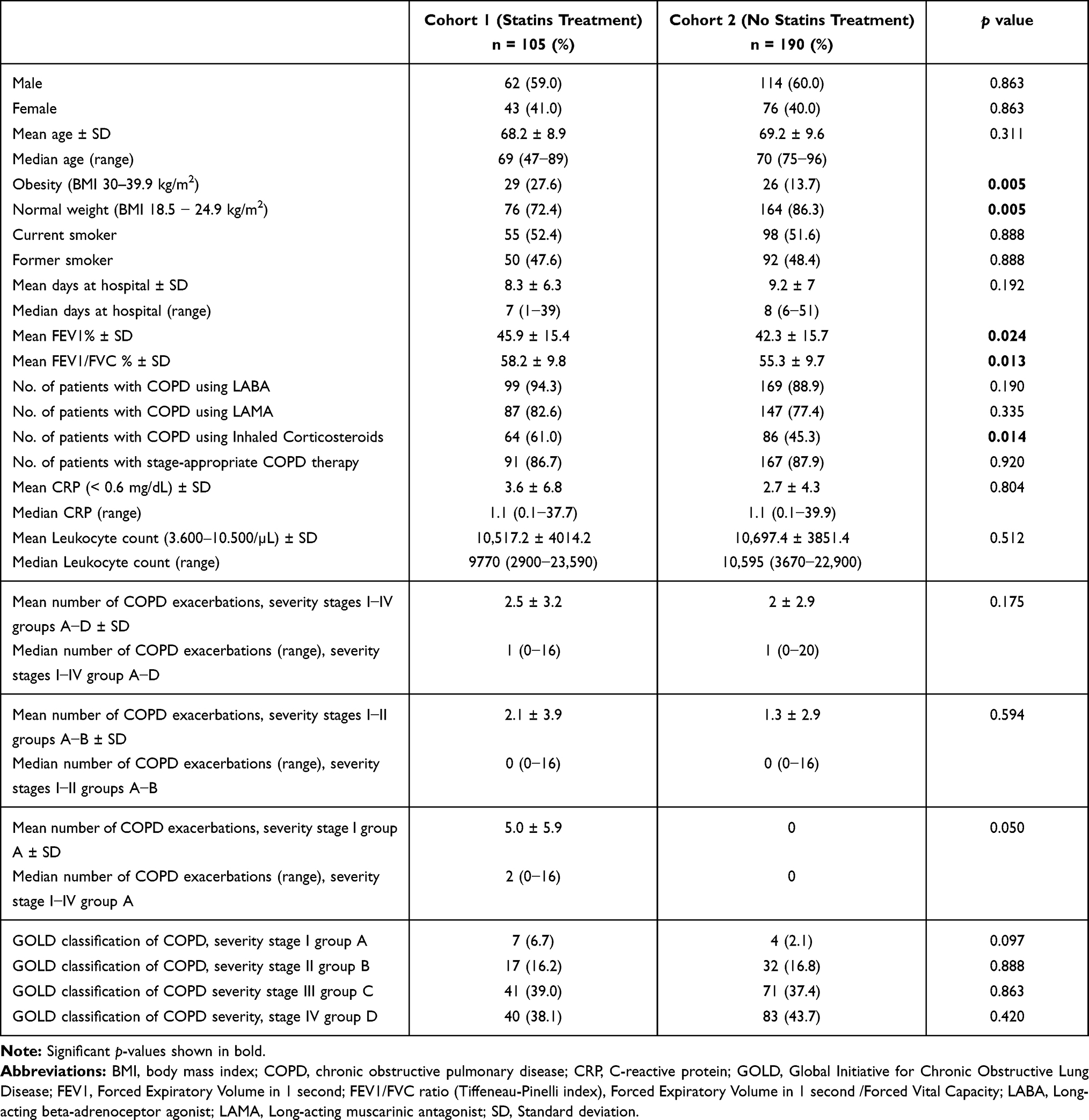 |
Table 1 Demographic Data, Duration of Hospitalization, Severity of Airflow Limitation After GOLD Classification Stage I−IV for Chronic Obstructive Pulmonary Disease Patients with (Cohort 1) and without (Cohort 2) Statin Treatment |
Most of the study participants in cohort 1 were, according to the GOLD classification system, classified as severity III group C, while those in cohort 2 were mainly classified as severity IV group D (Table 1). There was no statistically significant difference between the cohorts in terms of the number of study participants classified with GOLD grades I−IV groups A−D (Table 1). A comparison of those classified in COPD stages I−II groups A−B between the two cohorts also showed no statistically significant differences (p = 0.594) (Table 1). Likewise, the exacerbation rates at the initial stage GOLD I of COPD showed no statistically significant differences when comparing the two cohorts (p = 0.050) (Table 1). However, the two cohorts showed statistical differences in spirometric parameters, forced expiratory volume in one second (p = 0.024), and the ratio of forced expiratory volume in one second to forced vital capacity (p = 0.013) (Table 1).
Each study participant from both cohorts was observed for their number of COPD exacerbations from January 1, 2010 to December 31, 2020, and this parameter was not found to be statistically significantly different between the cohorts (p = 0.175) (Table 1, Figure 1).
 |
Figure 1 Comparison of chronic obstructive pulmonary disease exacerbation rates between patients with (cohort 1) and without (cohort 2) statin treatment. Each study participant from both cohorts was observed for their number of COPD exacerbations from January 1, 2010 to December 31, 2020. The mean number of COPD exacerbations, severity stages I−IV groups A−D was 2.5 ± 3.2 in cohort 1 and 2 ± 2.9 in cohort 2. The median number of COPD exacerbations (range), severity stages I−IV group A−D was 1 (0−16) in cohort 1 and 1 (0−20) in cohort 2. This parameter was not found to be statistically significantly different between the cohorts (p = 0.175). |
The inhalation treatment did not differ in the comparison of the two cohorts in the COPD patients receiving long-acting beta-adrenoceptor agonists (p = 0.190) and long-acting muscarinic antagonists (p = 0.335) (Table 1). Only inhalation therapy with steroids differed between the cohorts; more patients in cohort 1 used steroid therapy with statistical significance (p = 0.014) (Table 1). Most COPD patients in both cohorts received stage-appropriate treatment with no statistical difference (Table 1). The inflammation values in the blood laboratory also did not vary when the two cohorts were compared (Table 1).
The most frequently prescribed statins in cohort 1 in terms of the number of COPD study patients, who received them as treatment were the following: simvastatin (94) (89.5%, CI 82.2−94.1%), atorvastatin (6) (5.7%, CI 2.6−11.9%), fluvastatin (3) (2.9%, CI 1.0−8.1%), and pravastatin (2) (1.9%, CI 0.5−6.7%). When the two cohorts were compared with regard to the number of comorbidities of the study participants, statistically significant differences were found with the majority of diseases in cohort 1: cardiac decompensation (p = 0.017); coronary artery disease (p <0.0001); heart failure (p = 0.002); peripheral arterial disease (p = 0.005); status after heart attack (p = 0.0004); and status after stroke (p <0.0001) (Table 2). A total of 38 (12.9%, CI 9.5−17.8%) study participants died in both cohorts, with more in cohort 2, but this was not a statistically significant difference (p = 0.271) (Table 2). So, the probability of survival for all COPD patients with and without statin treatment was 87.1% (CI 83.0−91.2%) according to the Kaplan Meier method.
 |
Table 2 Comparison of Comorbidities (in Alphabetical Order) Between Chronic Obstructive Pulmonary Disease Patients with (Cohort 1) and without (Cohort 2) Statin Treatment |
Discussion
This study examined the independent effects of statins on exacerbations in COPD patients over a long observation period of 10 years. This study not only included the long-term outcomes which involving the number of mortality but also included the GOLD (I−IV) classification, the different active agents in the group of statins, spirometry values, inflammatory laboratory markers, stage-appropriate COPD therapy, smoking status, and comorbidities which provide evidence for the clinical treatment. According to the results of this current study, statins did not reduce the rate of exacerbations in COPD patients. The mean exacerbation rates in this study were similar in the cohorts receiving and not receiving statin treatment. Similarly, in the early stages of COPD, the statins did not reduce the exacerbation rates in COPD patients in this study. The most common indication for statin therapy was a vascular disease in this study. However, statin therapy was discontinued in a small proportion of the patients without further investigating the reasons, as this was outside the scope of this study.
A study conducted by the COPD Clinical Research Network came to the same conclusion that statins have no effect on the COPD exacerbation rate, according to an analysis published in the New England Journal of Medicine in 2014.10 This prospective randomized placebo-controlled trial of simvastatin for the prevention of COPD exacerbations included 885 patients with moderate to severe COPD who were treated with 40 mg simvastatin or a placebo daily for almost two years.10 In this earlier study, the exacerbation rates were almost the same in both study arms, namely 1.36 exacerbations in the simvastatin group and 1.39 exacerbations in the placebo group.10 Although there were more study participants in the previous study compared to in the present study, the study duration of two years in the previous study was much shorter compared to the current study period of 10 years. The median amount of time until the first exacerbation was observed in each patient (223 days with statin vs 231 days with placebo), the number of serious side effects (0.63 events with simvastatin and 0.62 events with placebo), and the number of deaths (28 with statin vs 30 with placebo) did not differ between the two treatment groups in this earlier study.10 Only patients with a history of exacerbations were included in the New England Journal of Medicine work. We compared the number of exacerbations per COPD patient in this study over ten years. Overall, we see a low exacerbation rate over 10 years in our study! However, it should be emphasized that only visits to the hospital were severe exacerbations in this study, and the minor exacerbations were not recorded. However, the statin treatment not only had no significant effect in this early study or the present study but there was not even a trend in favor of statin treatment for any endpoint, such as exacerbation and mortality rates, in this earlier study.10 Quite apart from the fact that prospective studies have a clear methodology and a clear statement, so prospective studies have more of an advantage. The authors of this earlier study concluded that simvastatin administered at 40 mg per day in COPD patients at a high risk of exacerbation did not affect the exacerbation rate or the amount of time until the presence of a first exacerbation.10 In the present study, however, different types and concentrations of the statins were examined, which was in contrast to the previous study, which only used 40 mg simvastatin. However, a comparison between another observational study might have been more appropriate in this case. Nevertheless, this comparison of this current study with the previous study by Criner et al was carried out because the prospective randomized double-blind placebo-controlled study represents the gold standard when it comes to testing the effectiveness of therapeutic interventions.10 In this context, gold standard means the highest quality of scientific primary studies with particularly high evidence. The previous study had some limitations, including the fact that the patients were already receiving the maximum standard medication.10 Another flaw in the above-mentioned previous study was that it excluded those study participants with cardiovascular disease that would benefit from statin therapy.10 The present study also had some limitations, which are listed in the section “Study Limitations” below.
A second randomized controlled trial, with rosuvastatin treatment in stable chronic obstructive pulmonary disease (RODEO), investigated the benefit of HMG-CoA reductase inhibitors in the COPD population and found no benefit in terms of exacerbation rates.31 These results were reflected in the clinical practice guidelines, which did not support the use of HMG-CoA reductase inhibitors to reduce COPD exacerbations.32
The same result came from a similar observational study carried out earlier than the present study with nearly the same number of examination patients and the same examination duration as used in the current study.33 This earlier observational study showed no causal relationship between statin use and the prevention of COPD exacerbations.33
In contrast to that finding, some previous COPD observational studies suggested that statin use was associated with reduced morbidity and mortality.34 It is possible that a subgroup of COPD patients with cardiovascular indications for statin and systemic inflammation may gain a clinical benefit from statin treatment.34 Moreover, understanding the immunomodulatory effects of statins in COPD can lead to the development of new targeted interventions.34 However, this immunomodulatory effect as an indirect expression of reduction in exacerbation rate was not seen in the current study.
A previous retrospective nested case-control study by Wang et al in patients with frequent COPD exacerbations examined the association between statin use and the risk of a COPD exacerbation at this previous study’s hospital.11 The conclusions of this previous study were that statin use was associated with a reduced risk of COPD exacerbation.11 A further reduction in the risk of exacerbation due to statin treatment took place when the statins were prescribed more recently or at high doses.11 Like any drug, the statins have a dose-dependent, but the cholesterol-lowering drugs could not reduce the exacerbation rates of COPD patients in this study, however.
Another previous study examined the effect of statin use on the decline in lung function in elderly patients and whether smoking could alter this effect.35 The results showed that statin consumption moderated the decline in lung function in the elderly patients, with the size of this positive effect changing with the smoking status of the individual patients.35 The estimated annual decline in lung function in the study by Alexeeff et al for statin non-users was 23.9 mL compared to 10.9 mL for statin users. Almost half of the study participants in this current study were still smokers.
This study compared both the number of patients and the number of exacerbations per patient according to the severity of COPD according to the GOLD classification I−V between the two cohorts with and without statin treatment. In the present study, we could not observe an improvement in lung function as an expression of the severity of the GOLD classification. However, the spirometric values differed significantly between the two cohorts in this present study.
Another study looked at the association between statin use and mortality in patients with peripheral arterial disease with and without COPD.36 In summary, statin use was associated with improved short- and long-term survival in patients with peripheral arterial disease both with and without COPD.36 Patients with COPD should be treated with an increased statin dose to achieve an optimal effect in both the short- and long-term, as a recommendation from the last study mentioned.36 In this study, an increased number of COPD patients had peripheral arterial disease following statin treatment, and this showed statistical significance. However, we could not determine a difference in the mortality of the study population of the two groups in the present study.
A systematic review of studies reporting the effects of statin treatment in COPD was performed.37 Eight studies met the selection criteria.13,36,38–43 Outcomes associated with statin treatment included decreased all-cause mortality and mortality, the incidence of emergency respiratory care, fewer COPD exacerbations, fewer intubations for COPD exacerbations, and mitigated decreases in lung function.13,36,38–43 Despite the fact that although this study did not all perform the same research compared to the systemic review. The present study was unable to achieve the key messages as this systemic review.
Study Limitations
This study only examined patients with COPD in the internal medicine department of the hospital. It also did not collect data regarding this study population’s treatment for exacerbations received from other hospitals. The indication for the use of statins in cohort 1 could have changed during the 10-year observation period of this study. Also, this study did not thoroughly review the possible reasons for COPD patients discontinuing statin use after their decision or by their treating physician during this study period. Patients classified as non-statin users could have received statin medication from their primary care doctor outside of the hospital or from other medical departments of the hospital. Patients identified as not exhibiting a COPD exacerbation may have experienced an exacerbation either in primary care settings outside the hospital, at another hospital, or in other medical departments within the present hospital. Moreover, important confounding factors were not measured, which could lead to an incorrectly observed association. This study only examined the basic relationship between statins and the risk of exacerbation without taking into account other important confounding factors, such as co-medications that could be significant in terms of exacerbation. Different statin substances, mainly simvastatin, were also used in this study population, which could possibly lead to a bias of the results.
Conclusions
This study failed to demonstrate the anti-inflammatory effects of statins in the prevention of exacerbations in COPD patients. An improvement in mortality in patients receiving or not receiving statin treatment could also not be ascertained through the use of statins in this study.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The Ethics Committee of the Westphalia-Lippe Medical Association and the Medical Faculty of the Westfälische Wilhelms-University Münster, Gartenstrasse 210-214, 48147 Münster, Germany, approved the ethics application for this study, with the file number 2020-825-f-S. All methods were carried out in accordance with relevant guidelines and regulations. Informed consent to hospital treatment was obtained from all subjects. No further permissions were necessary to collect the data in this study. This manuscript was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Prof. Dr. Karl-Josef Franke report personal fees from Boehringer Ingelheim, personal fees from Glaxo Smith Kline, personal fees from Berlin Chemie, outside the submitted work. The authors confirm no other conflicts of interests in this work.
References
1. Weingärtner O, Lütjohann D, Böhm M, Laufs U. Cholesterinhomöostase und kardiovaskuläres Risiko [Cholesterol homeostasis and cardiovascular risk]. Dtsch Med Wochenschr. 2011;136(1–2):34–38. doi:10.1055/s-0030-1269438
2. Cherepanov D, Bentley TGK, Hsiao W, et al. Real-world cardiovascular disease burden in patients with atherosclerotic cardiovascular disease: a comprehensive systematic literature review. Curr Med Res Opin. 2018;34(3):459–473. doi:10.1080/03007995.2017.1401529
3. Shen H, Rui L, Yan R, et al. Adjunctive therapy with statins in schizophrenia patients: a meta-analysis and implications. Psychiatry Res. 2018;262:84–93. doi:10.1016/j.psychres.2018.02.018
4. Noseda G, Darioli R, Keller U, et al. Prüfung der Wirksamkeit und Verträglichkeit von Atorvastatin bei Hyperlipidämie unter Praxisbedingungen (SWITCH-Studie) [Evaluating the efficacy and tolerance of atorvastatin in hyperlipidemia in general practice (SWITCH Study)]. Schweiz Med Wochenschr. 2000;130(23):889–895.
5. de Souza Zago VH, Tanus-Santos JE, Gardin Danelon MR, et al. Chemical modification of high density lipoprotein subfractions - HDL2 and HDL3 - after use of atorvastatin. Int J Clin Pharmacol Ther. 2014;52(04):277–283. doi:10.5414/CP201742
6. Capurso A. Le promesse delle statine [The promise of statins]. Ital Heart J Suppl. 2000;2(3):224–229.
7. Bargon J. Statine: stumpfes Schwert gegen COPD-Exazerbationen. MMW Fortschr Med. 2020;162(12):26–27. doi:10.1007/s15006-020-0604-7
8. Lin CM, Yang TM, Yang YH, et al. Statin use and the risk of subsequent hospitalized exacerbations in COPD patients with frequent exacerbations. Int J Chron Obstruct Pulmon Dis. 2020;15:289–299. doi:10.2147/COPD.S229047
9. Narsingam S, Bozarth AL, Abdeljalil A. Updates in the management of stable chronic obstructive pulmonary disease. Postgrad Med. 2015;127(7):758–770. doi:10.1080/00325481.2015.1084212
10. Criner GJ, Connett JE, Aaron SD, et al. COPD Clinical Research Network; Canadian Institutes of Health Research. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N Engl J Med. 2014;370(23):2201–2210. doi:10.1056/NEJMoa1403086
11. Wang MT, Lo YW, Tsai CL, et al. Statin use and risk of COPD exacerbation requiring hospitalization. Am J Med. 2013;126(7):598–606.e2. doi:10.1016/j.amjmed.2013.01.036
12. Huang CC, Chan WL, Chen YC, et al. Statin use and hospitalization in patients with chronic obstructive pulmonary disease: a nationwide population-based cohort study in Taiwan. Clin Ther. 2011;33(10):1365–1370. doi:10.1016/j.clinthera.2011.08.010
13. Blamoun AI, Batty GN, DeBari VA, et al. Statins may reduce episodes of exacerbation and the requirement for intubation in patients with COPD: evidence from a retrospective cohort study. Int J Clin Pract. 2008;62(9):1373–1378. doi:10.1111/j.1742-1241.2008.01731.x
14. Ingebrigtsen TS, Marott JL, Nordestgaard BG, Lange P, Hallas J, Vestbo J. Statin use and exacerbations in individuals with chronic obstructive pulmonary disease. Thorax. 2015;70(1):33–40. doi:10.1136/thoraxjnl-2014-205795
15. Johnson JD, Theurer WM. A stepwise approach to the interpretation of pulmonary function tests. Am Fam Physician. 2014;89(5):359–366.
16. Milne S, Jetmalani K, Chapman DG, et al. Respiratory system reactance reflects communicating lung volume in chronic obstructive pulmonary disease. J Appl Physiol. 2019;126(5):1223–1231. doi:10.1152/japplphysiol.00503.2018
17. Bernabeu-Mora R, Sánchez-Martínez MP, Montilla-Herrador J, et al. GOLD Stages of COPD: transitions, predictor factors and comparison with 2017 GOLD stages. Int J Chron Obstruct Pulmon Dis. 2011;2020(15):1519–1527.
18. Soriano JB, Hahsler M, Soriano C, et al. CHAIN investigators. Temporal transitions in COPD severity stages within the GOLD 2017 classification system. Respir Med. 2018;142:81–85. doi:10.1016/j.rmed.2018.07.019
19. Kobayashi S, Hanagama M, Ishida M, et al. Clinical characteristics and outcomes in Japanese patients with COPD according to the 2017 GOLD classification: the Ishinomaki COPD network registry. Int J Chron Obstruct Pulmon Dis. 2018;13:3947–3955. doi:10.2147/COPD.S182905
20. van Haarst A, McGarvey L, Paglialunga S. Review of drug development guidance to treat chronic obstructive pulmonary disease: US and EU perspectives. Clin Pharmacol Ther. 2019;106(6):1222–1235. doi:10.1002/cpt.1540
21. World Health Organisation. International statistical classification of diseases and related health problems. 10th revision, 5th ed, 2016; 2016. Available from: file:///C:/Users/J/AppData/Local/Temp/9789241549165-V1-eng-2.pdf.
22. Leidy NK, Wilcox TK, Jones PW, et al. EXACT-PRO Study Group. Development of the EXAcerbations of Chronic Obstructive Pulmonary Disease Tool (EXACT): a patient-reported outcome (PRO) measure. Value Health. 2010;13(8):965–975. doi:10.1111/j.1524-4733.2010.00772.x
23. Gayle A, Dickinson S, Morris K, Poole C, Mathioudakis AG, Vestbo J. What is the impact of GOLD 2017 recommendations in primary care? - a descriptive study of patient classifications, treatment burden and costs. Int J Chron Obstruct Pulmon Dis. 2018;13:3485–3492. doi:10.2147/COPD.S173664
24. Yamakuchi M, Greer JJ, Cameron SJ, et al. HMG-CoA reductase inhibitors inhibit endothelial exocytosis and decrease myocardial infarct size. Circ Res. 2005;96(11):1185–1192. doi:10.1161/01.RES.0000170229.49776.81
25. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357–363. doi:10.1370/afm.983
26. Lowry R. Confidence Interval of a Proportion; 2020. Available from: http://vassarstats.net/prop1.html.
27. Kummer J. Statistics Calculator. Calculator for producing statistics about a dataset. averages and other statistical measures; 2020. Available from: https://jumk.de/statistik-rechner/.
28. Navendu Vasavada Statistics. Mann Whitney test for unpaired data, two sample; 2016. Available from: http://astatsa.com/WilcoxonTest/.
29. Lowry R. Contingency table—VassarStats; 2020. Available from: http://vassarstats.net/newcs.html.
30. Huchon DJR. Calculator for survival probabilities (Kaplan-Meier Method). Available from: http://www.hutchon.net/Kaplan-Meier.htm. Accessed December 31, 2020.
31. Neukamm A, Høiseth AD, Einvik G, et al. Rosuvastatin treatment in stable chronic obstructive pulmonary disease (RODEO): a randomized controlled trial. J Intern Med. 2015;278(1):59–67. doi:10.1111/joim.12337
32. Carlson AA, Smith EA, Reid DJ. The stats are in: an update on statin use in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:2277–2284. doi:10.2147/COPD.S78875
33. Yayan J. No significant detectable anti-infection effects of aspirin and statins in chronic obstructive pulmonary disease. Int J Med Sci. 2015;12(3):280–287. doi:10.7150/ijms.11054
34. Thomson NC. Clinical studies of statins in asthma and COPD. Curr Mol Pharmacol. 2017;10(1):60–71. doi:10.2174/1874467209666160112125911
35. Alexeeff SE, Litonjua AA, Sparrow D, Vokonas PS, Schwartz J. Statin use reduces decline in lung function: VA normative aging study. Am J Respir Crit Care Med. 2007;176(8):742–747. doi:10.1164/rccm.200705-656OC
36. van Gestel YR, Hoeks SE, Sin DD, et al. Effect of statin therapy on mortality in patients with peripheral arterial disease and comparison of those with versus without associated chronic obstructive pulmonary disease. Am J Cardiol. 2008;102(2):192–196. doi:10.1016/j.amjcard.2008.03.038
37. Dobler CC, Wong KK, Marks GB. Associations between statins and COPD: a systematic review. BMC Pulm Med. 2009;9(1):32. doi:10.1186/1471-2466-9-32
38. Lee TM, Lin MS, Chang NC. Usefulness of C-reactive protein and interleukin-6 as predictors of outcomes in patients with chronic obstructive pulmonary disease receiving pravastatin. Am J Cardiol. 2008;101(4):530–535. doi:10.1016/j.amjcard.2007.09.102
39. Frost FJ, Petersen H, Tollestrup K, Skipper B. Influenza and COPD mortality protection as pleiotropic, dose-dependent effects of statins. Chest. 2007;131(4):1006–1012. doi:10.1378/chest.06-1997
40. Soyseth V, Brekke PH, Smith P, Omland T. Statin use is associated with reduced mortality in COPD. Eur Respir J. 2007;29(2):279–283. doi:10.1183/09031936.00106406
41. Ishida W, Kajiwara T, Ishii M, et al. Decrease in mortality rate of chronic obstructive pulmonary disease (COPD) with statin use: a population-based analysis in Japan. Tohoku J Exp Med. 2007;212(3):265–273. doi:10.1620/tjem.212.265
42. Mancini GB, Etminan M, Zhang B, Levesque LE, FitzGerald JM, Brophy JM. Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J Am Coll Cardiol. 2006;47(12):2554–2560. doi:10.1016/j.jacc.2006.04.039
43. Keddissi JI, Younis WG, Chbeir EA, Daher NN, Dernaika TA, Kinasewitz GT. The use of statins and lung function in current and former smokers. Chest. 2007;132(6):1764–1771. doi:10.1378/chest.07-0298
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.