Back to Journals » Journal of Pain Research » Volume 13
No Differences in the Prevalence and Intensity of Chronic Postsurgical Pain Between Laparoscopic Hysterectomy and Abdominal Hysterectomy: A Prospective Study
Authors Jin J, Min S, Peng L, Du X, Zhang D, Ren L
Received 29 July 2019
Accepted for publication 24 December 2019
Published 7 January 2020 Volume 2020:13 Pages 1—9
DOI https://doi.org/10.2147/JPR.S225230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Juying Jin, Su Min, Lihua Peng, Xunsong Du, Dong Zhang, Li Ren
Department of Anesthesiology, The First Affiliated Hospital of Chongqing Medical University, Chongqing 400016, People’s Republic of China
Correspondence: Juying Jin
Department of Anesthesiology, The First Affiliated Hospital of Chongqing Medical University, 1 Youyi Road, Chongqing 400016, People’s Republic of China
Email [email protected]
Objective: To compare the prevalence and characteristics of chronic postsurgical pain (CPSP) between laparoscopic hysterectomy (LH) and abdominal hysterectomy (AH) groups 3, 6, and 12 months after surgery, and to assess the impact of pain on the activities of daily living (ADL) of patients.
Methods: The demographic characteristics, intraoperative clinical factors, and postoperative pain score were collected prospectively in patients scheduled for elective LH or AH for benign disease at our institution from July 2014 to June 2015. Patients were interviewed by telephone and followed up for pain assessment 3, 6, and 12 months after surgery. The prevalence, intensity, and specific locations of pain, as well as analgesic administration and impact on the ADL, were included in the questionnaire.
Results: The results from 406 patients (225 patients in the LH group and 181 patients in the AH group) were obtained. Three months after surgery, the prevalence of CPSP was 20.9% in the LH group and 20.4% in the AH group. At 6 months, the prevalence of pain declined to 11.6% in the LH group and 9.4% in the AH group. At 12 months after surgery, only 13 (5.8%) patients in the LH group and 11 (6.1%) patients in the AH group complained about persistent pain. The prevalence of CPSP, as well as the average numerical rating scale pain scores at rest and during movement, during 12 months after surgery were not significantly different between the groups. CPSP after hysterectomy exhibited a negative impact on the ADL.
Conclusion: The prevalence and intensity of CPSP were not significantly different between patients undergoing LH or AH within 12 months after surgery. A tendency towards a reduction in chronic pain over time was documented. Chronic post-hysterectomy pain exhibited a negative impact on the ADL.
Keywords: chronic post-surgical pain, laparoscopic hysterectomy, abdominal hysterectomy
Introduction
In spite of numerous postoperative analgesic strategies, pain may persist after a surgical procedure, resulting in the unrecognized complication of chronic postsurgical pain (CPSP). According to the International Association for the Study of Pain, CPSP is considered to be persistent or intermittent for ≥3 months following surgery.1 CPSP can impair daily activities and reduce the health-related quality of life, and can occur in 10–65% of postoperative patients depending on the type of surgery, with 2–10% of these patients suffering from severe chronic pain.2–5 Persistent pain has been described after limb surgery,6 hernia operation,7 cesarean section,8 sternotomy,9 breast surgery,10 and thoracotomy.11
Although hysterectomy is one of the most common surgical options worldwide, few studies have focused on chronic pain after hysterectomy.12 As even a low prevalence of CPSP following hysterectomy may result in significant public-health problems, close attention must be paid to these consequences.
Laparoscopic hysterectomy (LH) is becoming more common and has been used to replace conventional surgical procedures. This surgical approach is associated with a lower prevalence of perioperative morbidity and faster return to normal activities when compared with conventional open surgery. Laparoscopy has been considered a type of minimally invasive surgery for patients undergoing hysterectomy.13,14 Between 2005 and 2013, the percentage of abdominal hysterectomy (AH) for benign indications has declined from 59% to 22%.15 Although minimally invasive surgery can reduce the prevalence of CPSP after inguinal hernia repair and axillary dissection,5,16 there is far less information available regarding the prevalence of CPSP in patients receiving LH in comparison with those receiving AH.
We aimed to compare the prevalence and characteristics of chronic pain between LH and AH groups 3, 6, and 12 months after surgery, and to assess the impact of pain on the activities of daily living (ADL) in these patients.
Methods
Ethical Approval of the Study Protocol
Ethical approval (registration number: 2013–61) was obtained from the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (Chongqing, China). This study was conducted according to guidelines set in the Declaration of Helsinki. All participants provided written informed consent before study enrolment.
Inclusion and Exclusion Criteria
The inclusion criteria were age >18 years and the ability to communicate in Mandarin. The exclusion criteria were an inability to provide informed consent, a malignant indication for hysterectomy, mental illness, and an inability to attend telephone or personal interviews.
Study Design and Participants
This prospective cohort study was carried out between July 2014 and June 2015. We enrolled patients scheduled for elective LH or elective AH from the hospital ward at our institution 1 day before or on the day of the surgical procedure. Patients were interviewed in-person by a trained investigator preoperatively and 24-h postoperatively. Follow-ups were carried out through telephone interviews 3, 6, and 12 months after surgery. The intraoperative data of each patient were acquired from her medical record.
Preoperative Questionnaire
Patients were administered questionnaires focusing on demographic and medical variables after gynecological admission. Questions regarding, age, marital status, education level, employment status, number of pregnancies, previous abdominal/pelvic surgery, vaginal/cesarean delivery, preoperative pelvic pain, pain in other body regions, and indication for hysterectomy were included. Marital (married/unmarried) and employment (employed/unemployed/retired) statuses were dichotomized. Education level was divided into three groups (high school diploma or below; professional diploma; university/postgraduate degree). The height and weight measured during surgical admission were used to calculate the body mass index.
Surgical Variables
Based on the type of surgical procedure scheduled, patients were categorized into LH group and AH group. The type of hysterectomy was selected by the attending gynecologist according to international recommendations.17
AH was carried out through a transverse incision (except for patients with a prior vertical incision). The procedure was undertaken using an extrafascial technique with clamps and suture ligation. After uterus removal, the vaginal cuff was closed continuously with an absorbable suture. For LH, a three-port technique was applied. Pneumoperitoneum was established by insufflation of CO2 with the pressure limited to 12 mmHg. Both relations of the uterus and vaginal complex were cut by bipolar electrocautery. The specimen was removed through the vagina. The procedure was completed with closing the vaginal cuff by a laparoscopic intracorporeal approach. Intraoperative variables (duration of the procedure, blood loss, and uterus weight) were acquired from the operating-room record.
Anesthesia Variables
General anesthesia was performed in accordance with the protocol used routinely in our department. Premedication was not given. In the operating room, routine monitoring (electrocardiography, noninvasive monitoring of blood pressure, pulse oximetry) was undertaken for all patients. General anesthesia was induced along with endotracheal intubation by intravenous injection of propofol (2 mg/kg), sufentanil (0.2–0.4 μg/kg) and rocuronium (0.6–0.9 mg/kg). Anesthesia was maintained through inhalation of sevoflurane in 40% O2. Mechanical ventilation was undertaken to establish an end-tidal CO2 of 35–45 mmHg. Sufentanil and rocuronium were injected intermittently if needed. A body temperature of >36°C was maintained in the two groups during the surgical procedure. All patients received parecoxib sodium (40 mg, i.v.) and ondansetron (4 mg, i.v.) 30 min before the end of the surgical procedure. According to standard criteria, patients were extubated in the operating room and then transferred to the post-anesthesia care unit (PACU). Upon arrival at the PACU, patient-controlled analgesia (tramadol, i.v.) was administered through an infusion pump (Rythmic™ Evolution; Micrel, Athens, Greece) to relieve postoperative pain. Patients were monitored every 6 h for 24 h for pain management, tramadol administration, and related adverse effects.
Assessment of Acute Pain
Patients were visited at 24 h after surgery. The pain intensity of patients was evaluated with regard to average pain at rest and during movement within 24 h using the numerical rating scale (NRS). Specifically, 0 points indicated “no pain” and 10 points indicated “the worst pain imaginable”.
Definition of Chronic Pain
Chronic pain was characterized by pain that had persisted beyond the regular healing time (3 months), along with a NRS value of >0 at rest and/or during movement. The number of patients who reported chronic pain in the week before the survey was used to define point prevalence.
Assessment of Chronic Pain
At 3, 6, and 12 months after the surgical procedure, patients were followed up with a telephone interview lasting ≤15 min. CPSP was determined by the short-form Brief Pain Inventory (BPI), a self-reporting questionnaire for describing postoperative pain experiences in adults after a major surgical procedure.18,19 This questionnaire contains four questions on pain severity and seven questions on pain interference with the ADL.
The items of pain severity were represented by the NRS. Pain experiences at rest and during movement were rated in the week before the survey. The sub-scales of pain severity were classified as 0 (“no pain”), 1–3 (“mild”), 4–6 (“moderate”), and 7–10 (“severe”). Besides, the frequency and specific locations of pain as well as analgesic administration were asked for each patient. The seven items relating to pain interference with the ADL were calculated by NRS values, where 0 points indicated “no interference” and 10 points indicated “complete interference”. Specifically, these seven items were general activity, mood, walking, work, relationships with others, sleep, and enjoyment of life.
Statistical Analysis
Based on previous findings that CPSP develops after approximately 25% of AH procedures,20,21 we determined that we would need to enroll 167 patients in each group to detect a 12% difference between the groups with 0.80 power at an alpha level of 0.05. With an estimated dropout rate of 20%, 209 patients in each group were needed.
The data were tested for normality before analyses. Continuous variables with a normal distribution are presented as the mean ± standard deviation, and were tested by the independent samples t-test. Other continuous data are expressed as median (range) and were analyzed using the Mann–Whitney U-test. Categorical data are presented as the number of patients and percentages. Differences between categorical variables were compared using chi-square and Fisher’s exact tests. P < 0.05 was considered significant. Statistical analyses were conducted using SPSS v18.0 (IBM, Armonk, NY, USA).
Results
From July 2014 to June 2015, 520 patients scheduled for LH or AH were screened for eligibility. Twenty-one patients declined participation and 28 surgical procedures were canceled. Thus, 259 patients who underwent LH and 212 patients who underwent AH were included. Between the first follow-up visit and 12-month telephone interview, 65 patients dropped out. As a result, data from 406 patients (225 patients in the LH group and 181 patients in the AH group) were included for assessment. Figure 1 shows patient flow starting from recruitment until 12-month assessment.
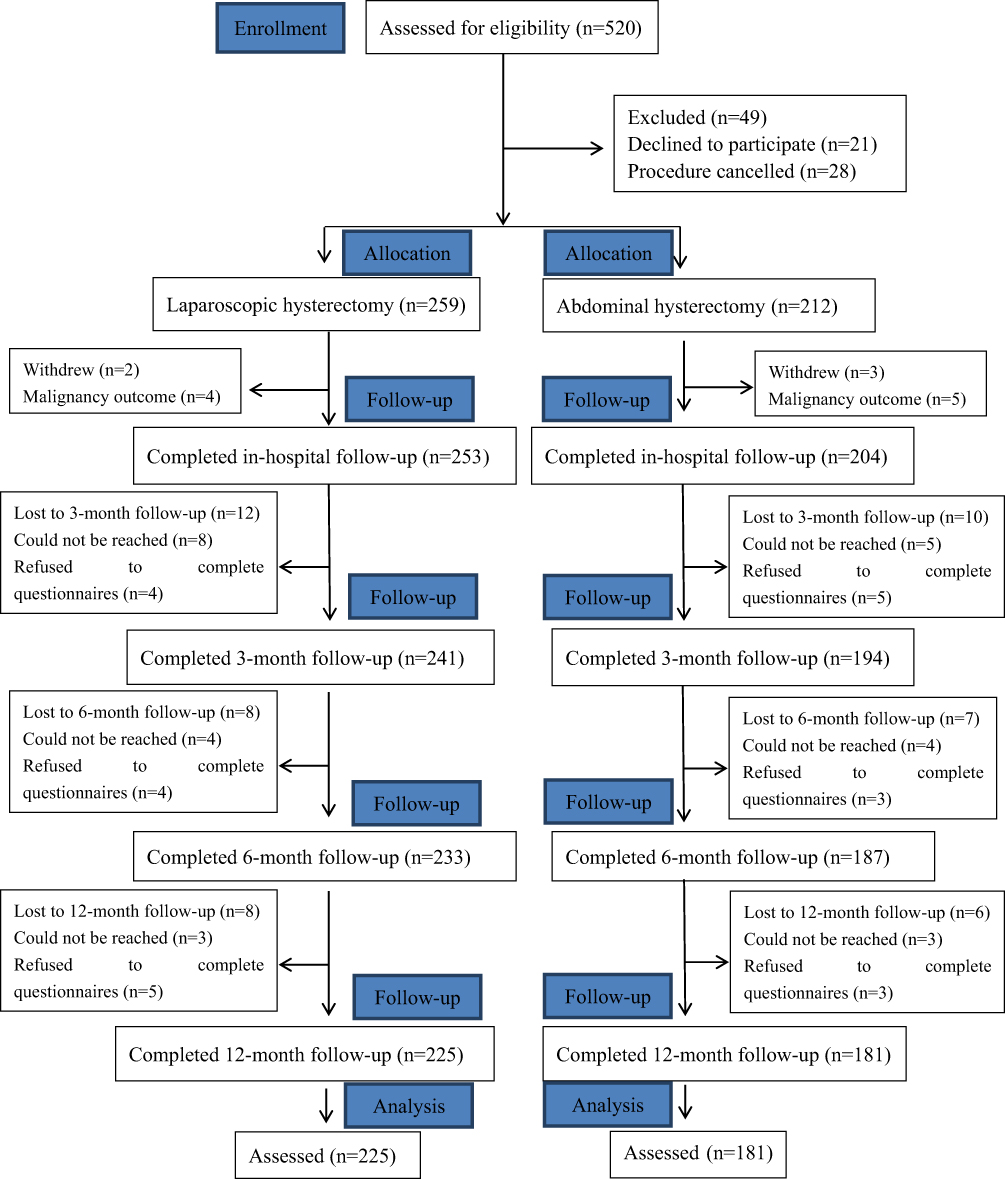 |
Figure 1 Flowchart of participants throughout the study. |
Table 1 summarizes the demographic characteristics, along with information on the surgical procedure, analgesia and postoperative pain control. The indications for hysterectomy were not significantly different between the two groups. Based on the definition in our study, 47 (20.9%) patients in the LH group and 37 (20.4%) patients in the AH group exhibited the features of CPSP 3 months after the surgical procedure. At 6 months after surgery, the prevalence of pain decreased to 11.6% (26 out of 225) in the LH group and 9.4% (17 out of 181) in the AH group. At 12-month follow-up, only 13 (5.8%) patients in the LH group and 11 (6.1%) patients in the AH group complained about persistent postoperative pain. The prevalence of CPSP 12 months after surgery was not significantly different between the two groups (Table 1).
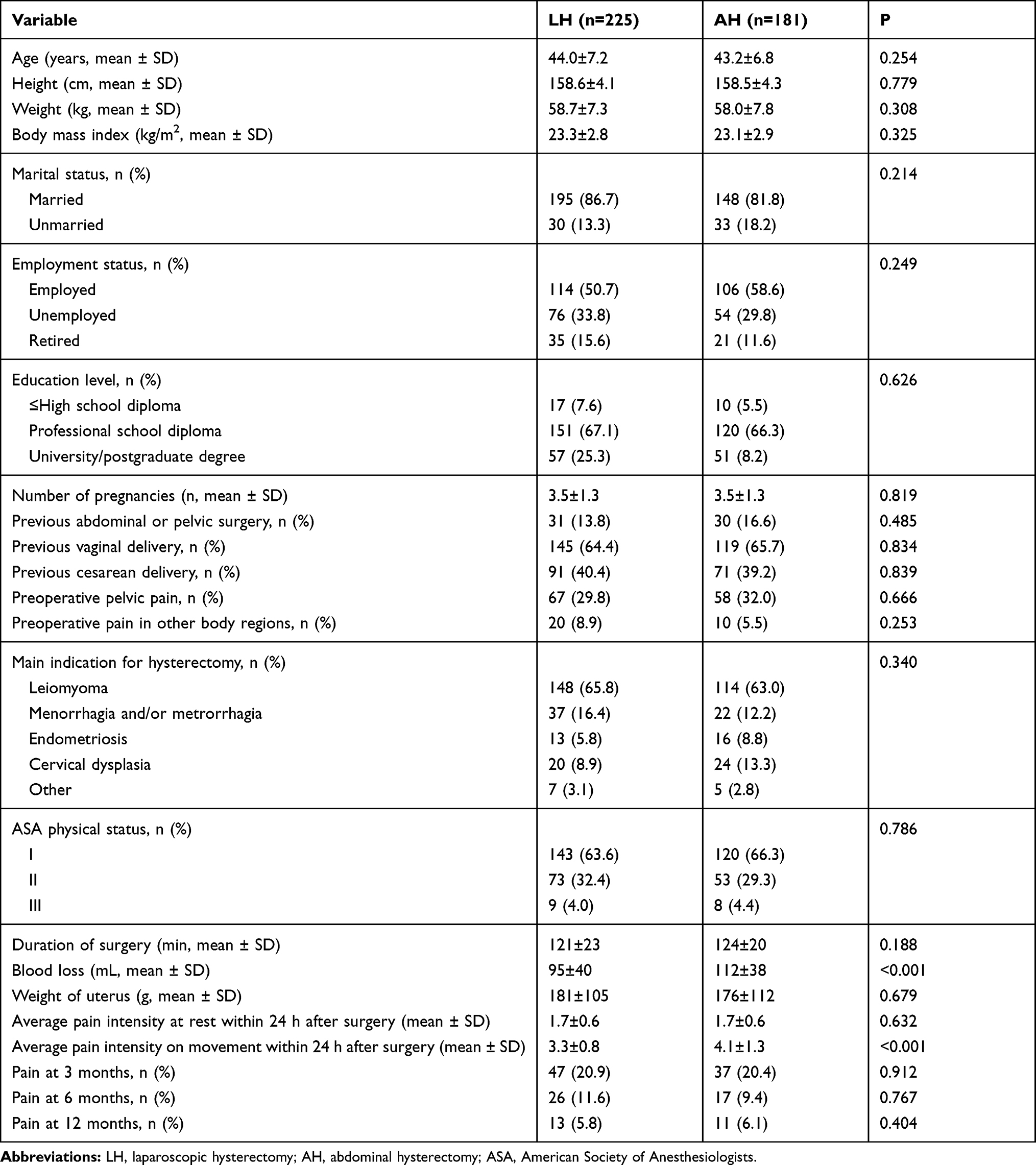 |
Table 1 Perioperative Variables of LH vs AH Groups |
The severity and frequency of CPSP are presented in Table 2. Notably, mild pain at rest was observed among most patients with CPSP in the two groups 12 months after surgery. At 3 months after surgery, approximately 50% of those with persistent pain in the two groups exhibited moderate-to-severe pain during movement. No patient in either group experienced severe persistent pain 12 months after surgery. Moreover, the average NRS pain score at rest and during movement was not significantly different between the two groups 3, 6, or 12 months after surgery. Among patients with CPSP, the prevalence of analgesic administration was not significantly different between the two groups 3, 6, or 12 months after surgery. In both groups, pain occurred several times a week or even every day in most patients with CPSP 3 months after surgery. At 6 months after surgery, pain occurred once or several times a week in ~60% of patients with CPSP in the two groups. At 12 months after surgery, approximately two-thirds patients of patients with CPSP in the LH group and one-third of patients with CPSP in the AH group reported pain occurring once a week and less than once a week, respectively. The two most common sites of CPSP in the two groups were the pelvis and incision site, followed by lower back, vagina and groin (Table 2).
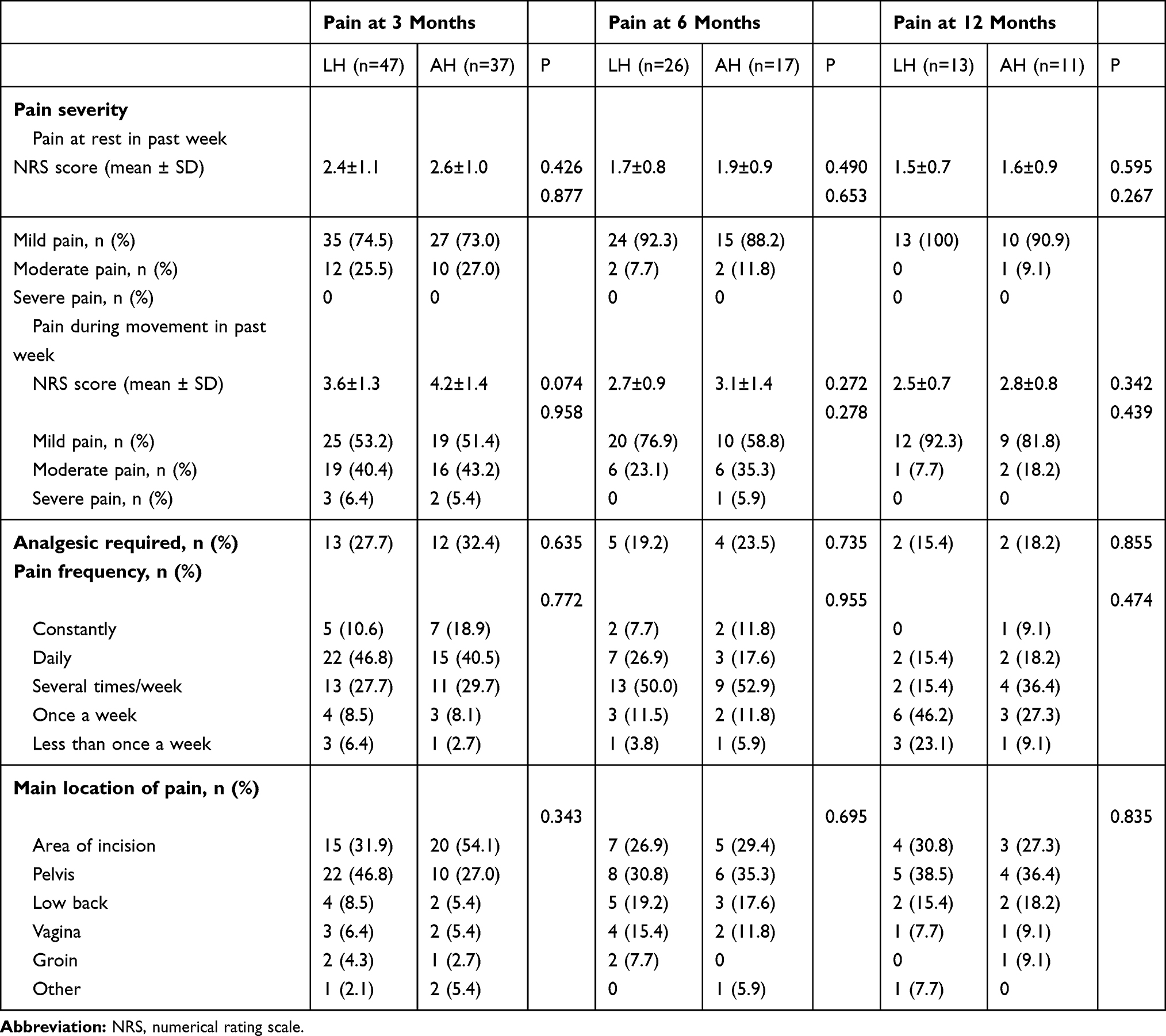 |
Table 2 Characteristics of Pain 3, 6 and 12 Months After Surgery |
Among the patients with CPSP in the two groups, mood and life enjoyment were the domains most affected by pain 3 months after surgery. At 6 months after surgery, the most crucial interference of pain was mood and relationships with other people in patients with CPSP in the two groups. At 12 months after surgery, the impact of pain on normal work, mood and social relationships was obvious among patients with CPSP in the LH group, whereas social relationships and life enjoyment were the domains most affected by CPSP in the AH group (Table 3).
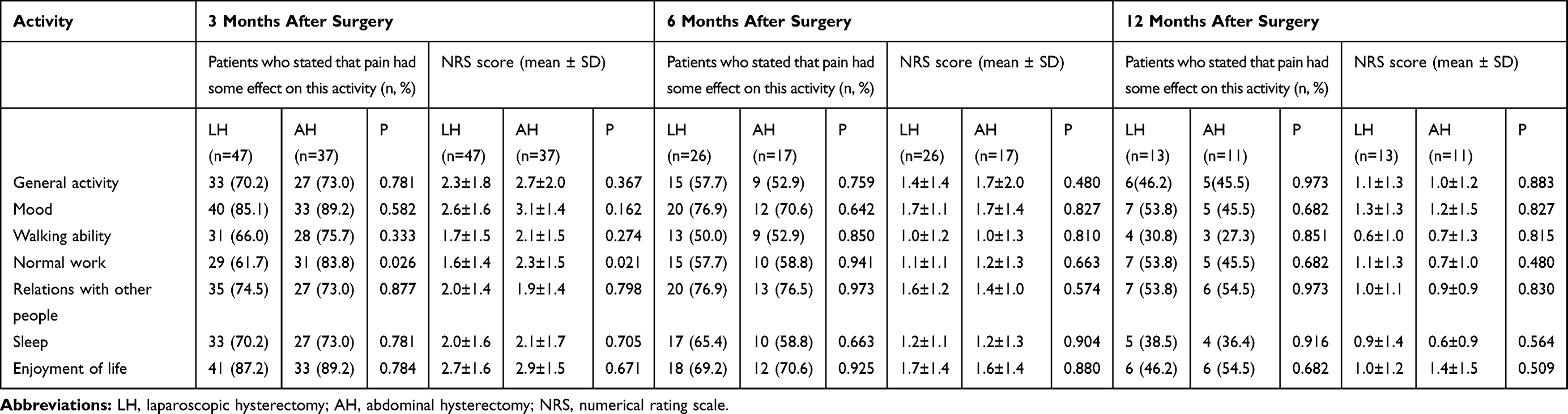 |
Table 3 The Activities of Daily Living Affected by Chronic Pain, and the Extent of the Perceived Interference |
Discussion
We found that the prevalence and intensity of chronic pain did not differ in patients who underwent AH or LH during 12 months after surgery, despite the obvious difference between a laparoscopic and abdominal procedure. Whether a laparoscopic procedure can reduce the risk of CPSP following hysterectomy or inguinal hernia repair,22 cholecystectomy,23 nephrectomy,24 or thoracotomy25 is not known. A possible explanation for such discrepancies is that nerve injury has an essential role in CPSP pathophysiology after breast surgery and inguinal herniorrhaphy, whereas a visceral component (instead of nerve injury) may lead to CPSP following intra-abdominal and intrathoracic procedures, regardless of the type of surgery.3,24–26
On the other hand, the average pain intensity measured by the NRS during movement within 24 h after surgery was markedly lower in patients who underwent LH compared with those who underwent AH. This difference may have been due to self-administration of analgesics to control pain. Through patient-controlled analgesia, the pain during movement remained an important barrier. Several studies have compared laparoscopic surgery for treatment of gynecologic diseases with abdominal or vaginal procedures, and their results support our findings.27–29 The differences in the pain scores may have been due to two main reasons. First, laparoscopic surgery involves electrosurgical instruments for coagulation and dissection, whereas abdominal procedures involve clamps, scissors, and tying knots. Therefore, similar to other open procedures, AH can induce a wide variety of inflammatory reactions.30,31 Second, a conventional incision is subject to greater tension forces, which may result in more severe acute pain.32
The pathogenic mechanisms underlying the transition from acute pain to chronic pain after surgery are largely unknown. The nervous system is sensitized in response to noxious stimuli, but this response returns to normal after healing. In certain cases, the sensitization persists, and this may result in chronic pain.3 Yarnitsky et al33 suggested that a low efficiency of diffuse noxious inhibitory control is related to chronic post-thoracotomy pain, reflecting individual differences in the endogenous analgesic system.
We found that the prevalence of chronic pain after hysterectomy was about 20%, 10%, and 6% at 3, 6, and 12 months after surgery. The prevalence of chronic pain reduced over time in patients who underwent LH or AH, data that are consistent with the findings of other scholars.34,35 One could speculate that spontaneous remission of chronic pain is natural because only two cases in each group were administered an analgesic for CPSP 12 months after surgery. On the other hand, pelvic pain is common among fertile women and, thus, post-hysterectomy pain may indicate pain in the general population.36 The prevalence of chronic pelvic pain among females aged 18 years to 49 years have has been reported to be 24.0% in the UK population37 and 14.7% in the US population.38
Only a small proportion of patients with CPSP suffered severe pain at rest. Moderate and severe pain during movement was found in nearly 50% of patients with CPSP 3 months after LH or AH, and this percentage was reduced at 6 months and 12 months after surgery. The values for pain severity observed in our study are similar to those of other studies.34,35,39,40 In view of the different methods used for pain assessment, our data should be interpreted with caution.
We discovered that CPSP exerted a negative impact on the ADL in patients who underwent AH or LH. Notably, chronic pain displayed predominant effects on general activity, mood and enjoyment of life, which may lead to impaired health-related quality of life among these patients. Besides, a psychic component may have been involved in the repercussion of chronic pain.
The strengths of our study were its prospective study design, consecutive sampling, and use of a validated measurement tool for pain assessment. Unlike other retrospective studies, which are dependent on a patient’s recall of events occurring months (or even years) after surgery, the patients in our study were requested to assess pain during their interview, but not recall previous pain experiences. Besides, randomization of the surgical procedures would not be ethical in these patients because the time taken to recover from laparoscopy may be more rapid. Hence, the type of surgical procedure was chosen based on the preference of the patient or surgeon.
Our study had three main limitations. First, the study cohort was restricted to people with non-malignant disease, so our findings may not reflect all patients who underwent hysterectomy. However, we chose this group to exclude patients with cancer-related pain. Second, our analysis was dependent upon self-reporting by patients, and quantitative sensory testing and physical examination were not taken into account. Finally, the follow-up period was limited to the first 12 months after surgery, so a more valid conclusion on long-term pain outcomes could not be drawn according to the definition of CPSP.
Conclusion
This prospective study demonstrated that the prevalence and pain intensity of CPSP were not significantly different between patients who underwent LH or AH throughout the 12 months after surgery. There was a tendency towards a reduction in chronic pain over time, and only a small percentage of patients exhibited CPSP 12 months after surgery. Our findings reveal that chronic pain after hysterectomy can have negative effects on the ADL of patients.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Macrae WA, Davies HTO. Chronic postsurgical pain. In: Crombie IKLS, Croft P, Von Korff M, LeResche L, editors. Epidemiology of Pain. Seattle: IASP Press; 1999:125–142.
2. Macrae WA. Chronic pain after surgery. Br J Anaesth. 2001;87(1):88–98. doi:10.1093/bja/87.1.88
3. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
4. Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77–86. doi:10.1093/bja/aen099
5. Perkins FM, Kehlet H. Chronic pain as an outcome of surgery. A review of predictive factors. Anesthesiology. 2000;93(4):1123–1133. doi:10.1097/00000542-200010000-00038
6. Jensen TS, Krebs B, Nielsen J, Rasmussen P. Phantom limb, phantom pain and stump pain in amputees during the first 6 months following limb amputation. Pain. 1983;17(3):243–256. doi:10.1016/0304-3959(83)90097-0
7. Aasvang E, Kehlet H. Chronic postoperative pain: the case of inguinal herniorrhaphy. Br J Anaesth. 2005;95(1):69–76. doi:10.1093/bja/aei019
8. Jin J, Peng L, Chen Q, et al. Prevalence and risk factors for chronic pain following cesarean section: a prospective study. BMC Anesthesiol. 2016;16(1):99. doi:10.1186/s12871-016-0270-6
9. Kalso E, Mennander S, Tasmuth T, Nilsson E. Chronic post-sternotomy pain. Acta Anaesthesiol Scand. 2001;45(8):935–939. doi:10.1034/j.1399-6576.2001.450803.x
10. Kroner K, Knudsen UB, Lundby L, Hvid H. Long-term phantom breast syndrome after mastectomy. Clin J Pain. 1992;8(4):346–350. doi:10.1097/00002508-199212000-00009
11. Perttunen K, Tasmuth T, Kalso E. Chronic pain after thoracic surgery: a follow-up study. Acta Anaesthesiol Scand. 1999;43(5):563–567. doi:10.1034/j.1399-6576.1999.430513.x
12. Brandsborg B. Pain following hysterectomy: epidemiological and clinical aspects. Dan Med J. 2012;59(1):B4374.
13. Olsson JH, Ellstrom M, Hahlin M. A randomised prospective trial comparing laparoscopic and abdominal hysterectomy. Br J Obstet Gynaecol. 1996;103(4):345–350. doi:10.1111/j.1471-0528.1996.tb09740.x
14. Munro MG, Deprest J. Laparoscopic hysterectomy: does it work?: a bicontinental review of the literature and clinical commentary. Clin Obstet Gynecol. 1995;38(2):401–425. doi:10.1097/00003081-199506000-00024
15. Lim PC, Crane JT, English EJ, et al. Multicenter analysis comparing robotic, open, laparoscopic, and vaginal hysterectomies performed by high-volume surgeons for benign indications. Int J Gynaecol Obstet. 2016;133(3):359–364. doi:10.1016/j.ijgo.2015.11.010
16. Grant AM, Scott NW, O’Dwyer PJ, Group MRCLGHT. Five-year follow-up of a randomized trial to assess pain and numbness after laparoscopic or open repair of groin hernia. Br J Surg. 2004;91(12):1570–1574. doi:10.1002/bjs.4799
17. ACOG. Committee Opinion No. 444: choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009;114(5):1156–1158. doi:10.1097/AOG.0b013e3181c33c72.
18. Cleeland CS, Ryan KM. Pain assessment: global use of the brief pain inventory. Ann Acad Med Singapore. 1994;23(2):129–138.
19. Mendoza TR, Chen C, Brugger A, et al. The utility and validity of the modified brief pain inventory in a multiple-dose postoperative analgesic trial. Clin J Pain. 2004;20(5):357–362. doi:10.1097/00002508-200409000-00011
20. Hillis SD, Marchbanks PA, Peterson HB. The effectiveness of hysterectomy for chronic pelvic pain. Obstet Gynecol. 1995;86(6):941–945. doi:10.1016/0029-7844(95)00304-A
21. Gimbel H, Zobbe V, Andersen BM, Filtenborg T, Gluud C, Tabor A. Randomised controlled trial of total compared with subtotal hysterectomy with one-year follow up results. BJOG. 2003;110(12):1088–1098. doi:10.1111/bjo.2003.110.issue-12
22. Aasvang EK, Gmaehle E, Hansen JB, et al. Predictive risk factors for persistent postherniotomy pain. Anesthesiology. 2010;112(4):957–969. doi:10.1097/ALN.0b013e3181d31ff8
23. Bisgaard T, Rosenberg J, Kehlet H. From acute to chronic pain after laparoscopic cholecystectomy: a prospective follow-up analysis. Scand J Gastroenterol. 2005;40(11):1358–1364. doi:10.1080/00365520510023675
24. Gerbershagen HJ, Dagtekin O, Rothe T, et al. Risk factors for acute and chronic postoperative pain in patients with benign and malignant renal disease after nephrectomy. Eur J Pain. 2009;13(8):853–860. doi:10.1016/j.ejpain.2008.10.001
25. Searle RD, Simpson MP, Simpson KH, Milton R, Bennett MI. Can chronic neuropathic pain following thoracic surgery be predicted during the postoperative period? Interact Cardiovasc Thorac Surg. 2009;9(6):999–1002. doi:10.1510/icvts.2009.216887
26. Brandsborg B, Nikolajsen L, Hansen CT, Kehlet H, Jensen TS. Risk factors for chronic pain after hysterectomy: a nationwide questionnaire and database study. Anesthesiology. 2007;106(5):1003–1012. doi:10.1097/01.anes.0000265161.39932.e8
27. Ghezzi F, Uccella S, Cromi A, et al. Postoperative pain after laparoscopic and vaginal hysterectomy for benign gynecologic disease: a randomized trial. Am J Obstet Gynecol. 2010;203(2):118 e111–118. doi:10.1016/j.ajog.2010.04.026
28. Campos LS, Limberger LF, Stein AT, Kalil AN. Postoperative pain and perioperative outcomes after laparoscopic radical hysterectomy and abdominal radical hysterectomy in patients with early cervical cancer: a randomised controlled trial. Trials. 2013;14:293. doi:10.1186/1745-6215-14-293
29. Medeiros LR, Stein AT, Fachel J, Garry R, Furness S. Laparoscopy versus laparotomy for benign ovarian tumor: a systematic review and meta-analysis. Int J Gynecol Cancer. 2008;18(3):387–399. doi:10.1111/j.1525-1438.2007.01045.x
30. Veenhof AA, Sietses C, von Blomberg BM, et al. The surgical stress response and postoperative immune function after laparoscopic or conventional total mesorectal excision in rectal cancer: a randomized trial. Int J Colorectal Dis. 2011;26(1):53–59. doi:10.1007/s00384-010-1056-9
31. de Carvalho GL, Cavazzola LT. Can mathematic formulas help us with our patients? Surg Endosc. 2011;25(1):336–337. doi:10.1007/s00464-010-1065-3
32. Nieboer TE, Johnson N, Lethaby A, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2009;(3):CD003677.
33. Yarnitsky D, Crispel Y, Eisenberg E, et al. Prediction of chronic post-operative pain: pre-operative DNIC testing identifies patients at risk. Pain. 2008;138(1):22–28. doi:10.1016/j.pain.2007.10.033
34. Montes A, Roca G, Sabate S, et al. Genetic and clinical factors associated with chronic postsurgical pain after hernia repair, hysterectomy, and thoracotomy: a two-year multicenter cohort study. Anesthesiology. 2015;122(5):1123–1141. doi:10.1097/ALN.0000000000000611
35. Theunissen M, Peters ML, Schepers J, et al. Recovery 3 and 12 months after hysterectomy: epidemiology and predictors of chronic pain, physical functioning, and global surgical recovery. Medicine (Baltimore). 2016;95(26):e3980. doi:10.1097/MD.0000000000003980
36. Latthe P, Mignini L, Gray R, Hills R, Khan K. Factors predisposing women to chronic pelvic pain: systematic review. BMJ. 2006;332(7544):749–755. doi:10.1136/bmj.38748.697465.55
37. Zondervan KT, Yudkin PL, Vessey MP, et al. The community prevalence of chronic pelvic pain in women and associated illness behaviour. Br J Gen Pract. 2001;51(468):541–547.
38. Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF. Chronic pelvic pain: prevalence, health-related quality of life, and economic correlates. Obstet Gynecol. 1996;87(3):321–327. doi:10.1016/0029-7844(95)00458-0
39. Brandsborg B, Dueholm M, Nikolajsen L, Kehlet H, Jensen TS. A prospective study of risk factors for pain persisting 4 months after hysterectomy. Clin J Pain. 2009;25(4):263–268. doi:10.1097/AJP.0b013e31819655ca
40. VanDenKerkhof EG, Hopman WM, Goldstein DH, et al. Impact of perioperative pain intensity, pain qualities, and opioid use on chronic pain after surgery: a prospective cohort study. Reg Anesth Pain Med. 2012;37(1):19–27. doi:10.1097/AAP.0b013e318237516e
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.