Back to Journals » Nature and Science of Sleep » Volume 14
Nightmare Distress as a Risk Factor for Suicide Among Adolescents with Major Depressive Disorder
Authors Song TH, Wang TT ![]() , Zhuang YY
, Zhuang YY ![]() , Zhang H, Feng JH, Luo TR, Zhou SJ
, Zhang H, Feng JH, Luo TR, Zhou SJ ![]() , Chen JX
, Chen JX ![]()
Received 22 February 2022
Accepted for publication 1 September 2022
Published 22 September 2022 Volume 2022:14 Pages 1687—1697
DOI https://doi.org/10.2147/NSS.S362999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Tian-He Song,1,2,* Ting-Ting Wang,2,3,* Yun-Yue Zhuang,1,2 Hua Zhang,4 Jun-Hui Feng,5 Tang-Ren Luo,6 Shuang-Jiang Zhou,2 Jing-Xu Chen2
1Department of Psychology, Chengde Medical University, Chengde, Hebei, People’s Republic of China; 2Beijing HuiLongGuan Hospital, Peking University HuiLongGuan Clinical Medical School, Beijing, People’s Republic of China; 3School of Mental Health, Bengbu Medical College, Bengbu, Anhui, People’s Republic of China; 4Dongying People’s Hospital, Dongying, Shandong, People’s Republic of China; 5Jining Psychiatric Hospital, Jining, Shandong, People’s Republic of China; 6The Third Hospital of Longyan, Longyan, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuang-Jiang Zhou; Jing-Xu Chen, Beijing HuiLongGuan Hospital, Peking University HuiLongGuan Clinical Medical School, Beijing, 10096, People’s Republic of China, Tel +86 13466401377 ; +86 13681394260, Email [email protected]; [email protected]
Purpose: Nightmare is common and is also independently implicated in suicide risk among the adolescent population. Adolescents with major depressive disorder (MDD) are at an increased risk of suicide. Therefore, comorbid nightmares may amplify suicide risk among this clinical population. This study aimed to explore the effects of nightmares on suicide risk among adolescents with MDD.
Patients and Methods: Subjects were 499 outpatients aged 12– 18 in four large psychiatric hospitals clinic of China, from January 1 to October 31, 2021. Simultaneously, we matched 499 healthy controls according to gender and age. All participants underwent affective state (depressive and anxiety symptoms) and sleep variable (nightmare frequency/distress, insomnia symptoms, and daytime sleepiness) evaluation as well as MDD diagnoses and determination of suicide risk by a fully structured diagnostic clinical interview.
Results: Adolescents with MDD reported a higher incidence of frequent nightmares (at least one night per week) and level of nightmare distress than healthy controls (22.0% vs 6.1%; 28.85 ± 11.92 vs 17.30 ± 5.61). Over half of the patients with suicide risk (51.6%) experienced frequent nightmares compared with approximately one-third of those at a risk for suicide (30.7%). Patients with suicide risk scored scientifically higher on sleep variables, depressive and anxiety symptoms than those without the risk. Further logistic regression analysis indicated that female gender, junior grade, recurrent depressive episode, severe nightmare distress and severe depressive symptoms were independently and significantly associated with suicide risk.
Conclusion: Our study provided evidence that adolescents with MDD experienced a higher prevalence of frequent nightmares and suffered more nightmare distress. Nightmare distress is an independent risk factor for suicide risk.
Keywords: major depressive disorder, sleep problems, nightmare, suicide risk, adolescent
Introduction
Major depressive disorder (MDD) is a significant public health concern worldwide; approximately 264 million individuals are affected by MDD.1 Adolescents are a population group at a high risk of experiencing MDD, and the prevalence is increasing.2,3 A meta-analysis suggests that the global prevalence of any depressive disorder is 2.6% and 1.3% major depression.4 There is strong evidence on the relationship between MDD and severe consequences, including suicide, which is the third leading cause of death among adolescents.5 Therefore, it is critical to identify the risk factors related to increased suicide risk among adolescents with MDD to develop effective interventions accordingly.
Sleep is a physiological phenomenon that occupies up to one-third of the human lifespan and is believed to be a pivotal operating state of the central nervous system.6 Adequate sleep among adolescents is essential owing to its significant effects on the development of vital psychophysiological functions.7 The findings of several previous studies in the adolescent population, which showed that sleep problems, such as insomnia, are closely linked to depression and other psychiatric disorders and are major risk factors for developing suicidal thoughts and behaviors, supported this notion.8–10 Sleep problems are common among patients with MDD and have been formerly regarded as the core secondary symptoms of a depressive episode.11–13 Furthermore, patients with sleep problems are often implicated with adverse outcomes, including elevated symptom severity, increased suicide risk,14 and greater recurrence risk.15,16 Therefore, sleep problems warrant attention as a public health concern. It is a particularly important step to prevent and identify these problems as accurately as possible and develop effective strategies of sleep improvement interventions to reduce suicide risk.8,9
Nightmare is one of the most common and specific types of sleep problems, typically characterized by dysphoric, frightening, or disturbing dreams that cause extreme irritability and often lead to awakening.17,18 According to several epidemiological studies on the general adolescent population, nightmares are prevalent.17,19,20 For example, Liu et al reported that 45.2% of the participants experience at least one nightmare episode per month, and 8% experience frequent nightmares (at least one episode per week).19 Nightmares have been linked to a variety of mental health consequences, such as insomnia, daytime sleepiness, anxiety and depressive symptoms, post-traumatic stress disorder, behavioral problems, and impaired psychosocial function.19,21,22 Furthermore, studies have demonstrated that nightmares are associated with an increased risk of suicide risk in the past few years.17,21,23
However, several issues have been left open by the previous literature, which warrant to be addressed in the current study. First, in adult psychiatric patients with MDD, bipolar disorders, and schizophrenia, nightmares occur at a higher rate than in the general population, ranging from 29.9% to 62.3%.18,24,25 However, to date, no evidence for the prevalence of nightmares among adolescent patients with MDD exists. Second, although a growing number of studies have focused on the sleep–suicide relationship, only two studies have specifically been designed to examine this issue using adolescent samples with MDD.26,27 Moreover, sleep variables in these studies only include insomnia and sleepiness, but not nightmares. Third, no studies have attempted to identify which specific sleep problems are associated with suicide risk independently from other sleep variables since they are probably highly correlated or overlap. For example, nightmares frequently lead to insomnia and excessive daytime sleepiness.
Therefore, using valid measures of a wide range of different sleep disturbances and suicide risk in adolescent patients with MDD, we mainly sought to investigate the following research questions: (1) determine the prevalence of nightmares among the clinical population and whether it is higher than in healthy controls and (2) whether nightmares are associated with suicide risk after controlling for demographics, psychopathology (eg, anxiety and depressive symptoms), and other sleep variables.
Methods
Participants
This study was conducted at the outpatient clinics of four large psychiatric hospitals in China between January 1 and October 31, 2021. The following were the inclusion criteria: participants 12–18 years old, those who met the diagnostic criteria of MDD according to the DSM-IV, and those not receiving any treatment during the current depressive episode (The participants include first episode and recurrence of depression). The DSM-IV diagnosis of MDD was established by a trained psychiatrist using a face-to-face structured clinical interview using the Mini-International Neuropsychiatric Interview (MINI) Version 5.0.28 Patients with any of the following conditions were excluded from this study: significant physical illnesses, such as cardiovascular disease and organic brain disorder; another mental illness, such as Post traumatic stress disorder (PTSD) and bipolar depression; pregnant or lactating; alcohol, drug and cigarette dependence or abuse and mental retardation; and those who have undergone treatment with electroconvulsive therapy within the last month.
Gender and age matched controls were also included as controls in this study. The following were the inclusion criteria: participants 12–18 years old, those without a personal or family history of mental illness. They also received a face-to-face clinical interview to determine that they without a personal or family history of mental illness. Other exclusion criteria were the same as those in the experimental group. There were recruited from volunteers in the community near the hospital between January 1 and October 31, 2021. All participants and their guardians provided written informed consent to indicate their willingness to participate.
Measures
Insomina
Insomnia symptoms were measured using the Chinese version of the Insomnia Severity Index (ISI), a brief self-reported questionnaire with seven items.29 A five-point Likert scale was used (total score range: 0–28). The severity level is divided into four grades (normal, 0–7; subthreshold [mild], 8–14; moderate, 15–21; and severe, ≥22).30 In one adolescent validation study, reliability was strong (Cronbach's α=0.83), and test-retest reliability was acceptable (r=0.79).31
Daytime Sleepiness
Daytime sleepiness was assessed using the Chinese Adolescent Daytime Sleepiness Scale (CADSS).32 The CADSS consists of seven items, and all items are rated using a five-point scale, with a total score ranging from 7 to 35. Higher scores indicated more daytime sleepiness. The scale has better reliability and validity than other scales among Chinese adolescents, with a Cronbach's alpha coefficient of 0.89.32
Nightmare Frequency
Nightmare frequency was measured by the first question from the Nightmare Disorder Index,33 “How many nights a week did you have nightmares in the past 1 month (ie, disturbing, extended, and well-remembered dreams)?” Participants were offered a range of five response options, from “0 nights per week” to “7 nights per week”.
Nightmare Distress
Nightmare distress was measured using the Nightmare Distress Questionnaire-Chinese version (NDQ-CV).20 The questionnaire consists of 14 items, and each item is rated using a five-point scale, with a total score ranging from 14 to 70. The higher the score obtained from the NDQ-CV, the higher the degree of nightmare distress. This scale has good reliability and validity among Chinese adolescents, with a Cronbach's alpha coefficient of 0.88.20
Depression Severity
The 17-item Hamilton Rating Scale (HAMD-17) was used to assess the depression severity. The total HAMD-17 score ranges from 0 to 52 and is divided into four grades (normal, 0–7; mild, 8–16; moderate, 17–23; and severe, ≥24).34 In this study, the raters from each clinical site were trained, and the average between-rater intraclass correlation coefficient was 0.87.
Anxiety Severity
Anxiety severity was measured using the seven-item Generalized Anxiety Disorder (GAD-7). GAD-7 is a seven-item self-report scale with a four-point Likert scale (from 0 to 3), and the total score ranges from 0 to 21. The severity level is categorized as none (0–4 points), mild (5–9 points), moderate (10–14 points), and severe (≥15 points).35 This scale has good reliability and validity among Chinese adolescents, with a Cronbach's alpha coefficient of 0.90–0.92.36
Suicide Risk
Suicide risk was evaluated using the suicidal module of the MINI.28 The suicidal module consists of six screening questions, with a total score ranging from 0 to 33. The suicide risk is divided into four groups: none (0), low (1–5), moderate (6–9), and high (≥10) risk. Based on previous studies, we stratified all participants into two groups: absence (low or none) or presence of suicide risk (moderate or high).8,37
Statistical Analyses
Statistical analyses were performed using SPSS 25.0 (IBM SPSS, IBM Corp., Armonk, NY). Continuous variables were expressed as means and standard deviations and categorical variables as raw numbers and percentages (%). The t-test was employed for parametric continuous variables and the Mann–Whitney U-test for continuous nonparametric variables. The Chi-square test was used for categorical variable analyses. Correlation analysis among the scores of each scale was performed by determining the Pearson correlation coefficients with Bonferroni correction. Binary multivariate logistic regression analyses were used to explore the association between the predictors of suicide risk. Suicide risk (no = 0; yes = 1) was used as a dependent variable. Gender, grade, depressive episode, insomnia symptoms, daytime sleepiness, frequency of nightmare distress, and anxiety and depressive symptoms were the independent variables. Backward stepwise binary logistic regression analysis was performed to determine the factors providing independent prediction of suicide risk. P values <0.05 (two-sided) were considered statistically significant.
Results
A total of 523 outpatients with MDD participated in this survey, and 24 patients were excluded from the analysis owing to missing data that precluded assessment. No significant differences in age, gender, and grade between outpatients (n = 499) and healthy participants were noted (n = 499) (p > 0.05). The demographic and clinical characteristics of the participants are outlined in Table 1. In the participants with MDD, the proportion of insomnia and suicide risk was higher than in the healthy ones (all p < 0.001). Patients with MDD showed higher total ISI, CADSS, and NDQ-CV scores than healthy controls (all p < 0.001). Moreover, patients with MDD reported more nightmare frequency than healthy controls (p < 0.001). Up to 67.5% (339/499) of the patients had experienced nightmares in the past month, and 38.7% (193/499) reported frequency nightmare at least once a week, and 28.7% (143/499) and 6.0% (30/499), respectively, among the controls. Significant differences in the abovementioned two indexes between patients and controls were noted (all p < 0.001).
 |
Table 1 Demographic and Clinical Characteristics of All Participants |
Of all adolescents with MDD, 190 (38.1%) presented a risk of suicide (Table 2). Between patients with or without suicide risk, significant differences were observed in terms of gender, grade, and insomnia prevalence (all p < 0.001). One in two patients with suicide risk (51.6%) experienced frequency nightmares, which was significantly higher than those without suicide risk (30.7%). Moreover, patients with recurrence were at a higher risk of suicide than those with first episodes (p < 0.001). To compare the effects of different degrees of daytime sleepiness and nightmare distress on patients, the total scores of CADSS and NDQ-CV were categorized into three levels (“low”, “medium”, and “severe”) using terciles as cutoff points. A significant difference in the severity of insomnia symptoms, daytime sleepiness, nightmare distress, and anxiety and depressive symptoms between patients with and without suicide risk was noted (all p < 0.05). Notably, the percentage of severe nightmare distress among patients with suicide risk was 54.2%, whereas that without suicide risk was 24.3%.
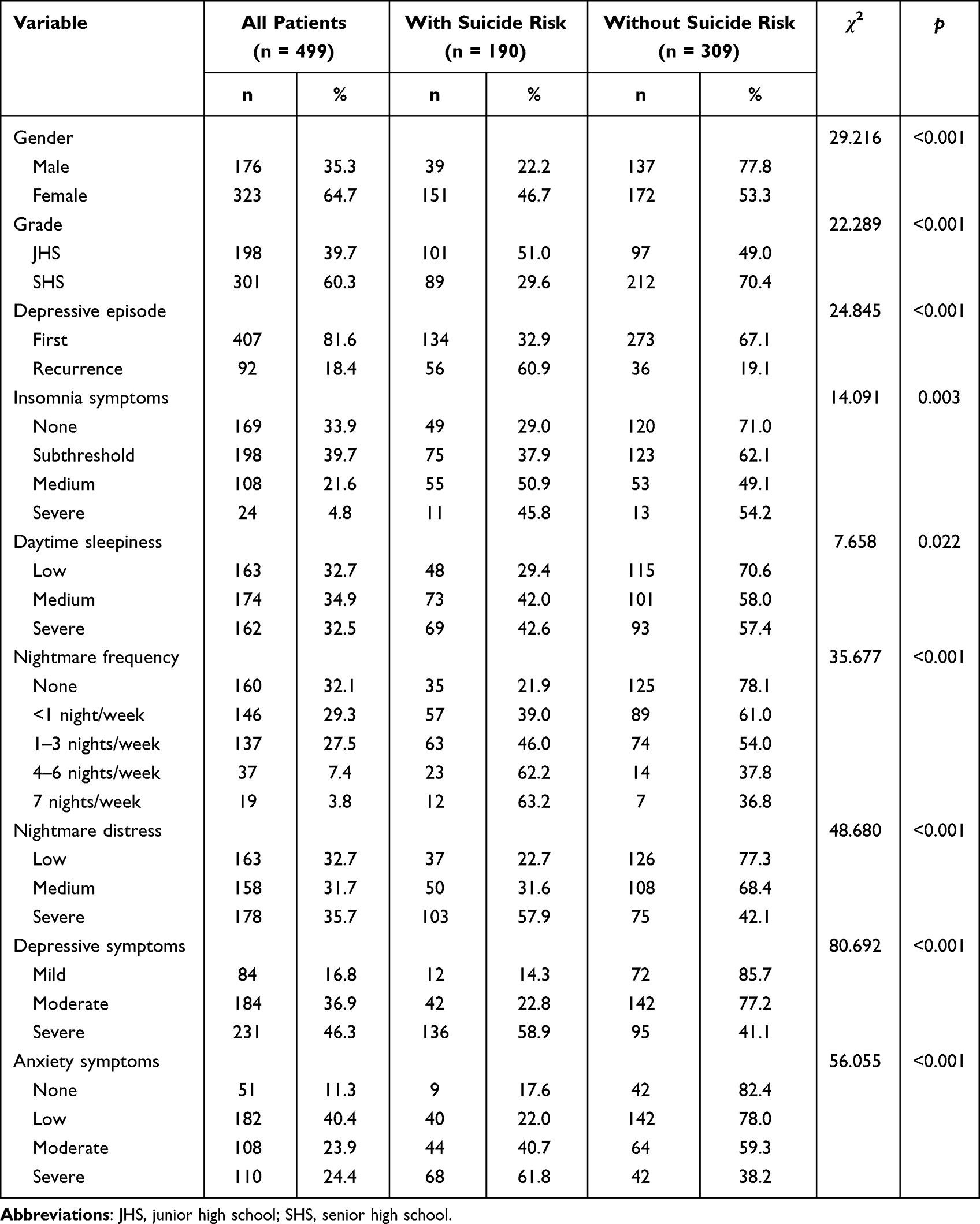 |
Table 2 Demographic and Clinical Characteristics of Participants with Depression in Relation to Suicide Risk |
The results of correlation analysis are shown in Table 3 and Figure 1. Positive Correlations among suicide risk, nightmare frequency NDQ-CV, CADSS, ISI and PHQ-9 scores ranged from r = 0.141 to 0.669 and all of their coefficients were significantly correlated (P < 0.001).
 |
Table 3 Correlations Among Suicide Risk, Sleep Disorders, and Depressive Symptoms in Participants with MDD |
 |
Figure 1 Pearson rho correlation coefficients. |
Binary logistic regression analyses were conducted to explore the relationships between suicide risk and demographic and clinical characteristics significant in univariable analyses (Table 4). Female gender (odds ratio [OR] = 2.722, 95% confidence interval [CI]: 1.64–4.52), junior grade (OR =2.758, 95% CI: 1.73–4.41), recurrent depressive episode (OR = 2.525, 95% CI: 1.73–4.71), severe nightmare distress (OR= 2429, 95% CI: 1.38–4.29) and severe depressive symptoms (OR = 7.065, 95% CI: 3.36–14.86) were independently and significantly associated with suicide risk.
 |
Table 4 Logistic Regression of Demographic and Clinical Characteristics of Depressive Patients and Suicide Risk in Participants with MDD |
Discussion
Most of the previous studies on nightmares and suicide risk were conducted in schools. We have extended the current knowledge about the impact of nightmares on the risk of suicidality in this particular population. This large-scale, cross-sectional investigation has shown that nightmares are frequent among adolescents with MDD: 67.5% and 38.7% of the patients reported at least one nightmare episode per month and at least one nightmare episode per week, respectively, both were observed to be higher than those of controls (27.7% and 8.0%). Furthermore, the prevalence of frequent nightmares in our patient group (51.6%) was significantly higher than those of previous studies (8.9%).38 The results were compatible with other studies.39,40 Consistent with the higher nightmare frequency among adolescents with MDD, these patients experienced more severe nightmare distress than healthy ones. Moreover, compared with normal individuals, adolescents with MDD may be predisposed to insomnia symptoms, daytime drowsiness, and suicide risk, which were concordant with several previous studies.41–43
This study represents one of the exploring sleep disorders associated with suicide risk in a sample of adolescents with MDD. Consistent with most previous studies,9,44,45 our results indicated significant correlations between suicide risk and multiple sleep disorders, including nightmare frequency, nightmare distress, insomnia symptoms, and daytime sleepiness. Considering that the pairwise comparisons of sleep disorders were significantly correlated, it would be important to examine the shared and specific effects of sleep disorders on suicide risk. However, we performed a logistic regression analysis and demonstrated that only nightmare distress was an independent risk factor for increased suicide risk after adjusting for grade, gender, emotional symptoms, and other sleep variables. Such information may help us to better understand the role of sleep problems in the pathogenesis of suicide and design effective prevention and intervention strategies for suicide by improving nightmare distress.
Over the past decades, several researchers investigating nightmares have long been interested in nightmare frequency and have provided some evidence to support it as an independent risk factor for suicide.19,23,46 Notably, most individuals who experienced nightmares may have only mild negative effects on psychosocial functioning, and distress caused by nightmares is the most important clinical indicator of nightmare severity because it is more highly correlated with psychological disturbances.20 In this context, the study of nightmares needs to include frequency and distress, which can be potentially overlapping and interconnected. A recent prospective longitudinal survey with a large general population of adolescents found that both nightmare frequency and distress significantly increased suicidal thoughts, plans, and attempts.17 In our study on adolescents with MDD, we identified and validated that more than half of the patients with suicide risk were accompanied by frequent nightmares and severe nightmare distress. However, it is not the frequency of nightmares but the self-reported distress related to the nightmare experience that may be the critical variable in predicting suicide risk.
Several studies have investigated the psychological mechanisms underlying the association between nightmares and suicide; however, the association remains unclear. The promising preliminary evidence suggests that difficulties with affect/emotion regulation and negative cognitive appraisals may play a pivotal role in nightmares leading to suicide.47 For example, Littlewood et al48 found that the experience of nightmares initially resulted in defeat, which in turn leads to perceptions of entrapment and hopelessness, and ultimately suicidal behaviors. Neuroimaging argue that nightmare severity was associated with reduced activity in the limbic-prefrontal emotion regulation network, particularly the right medial prefrontal cortex and bilateral anterior cingulate cortex, and these areas are believed to play a significant role in suicide.49 In addition, nightmares may cause sleep disruption and nighttime wakefulness, thereby increasing the likelihood of suicidal ideations.50
Several studies in various countries have suggested that females with MDD were more likely to be affected by the occurrence of suicidal ideation.51,52 Similarly, we found that adolescent patients with MDD had a relative risk that was 2.67 times higher than male patients, possibly owing to gender differences in neuroendocrine responses under stress53 and different emotional responses during adolescence.54 In the general adolescent population, suicide risk increases with age.55 However, our study on MDD showed that junior students had a higher suicide risk than senior ones. There are similar results in some domestic studies, and the suicide risk of adolescents is negatively correlated with age.56 Some studies show that suicidal behavior is related to impulse control.57 The reason for the high suicide risk of junior high school students may be related to their younger age and relatively insufficient ability to control impulsive behavior. The brain function of patients with relatively young age is relatively weak, so the risk of suicide is relatively high.58,59
We found that patients with severe depressive episodes had a seven-fold increased risk of suicide compared with those with mild depressive episodes. A strong and robust relationship between depressive symptom severity and suicide has been confirmed by several cross-sectional and longitudinal studies.60,61 The possible cause may be related to depressed mood, hopelessness, self-blame, and feelings of worthlessness that could influence patients to commit suicide to end their suffering.62–64 Furthermore, consistent with some previous studies,65,66 the present study indicated that suicide risk in patients with recurrent episodes was significantly higher than that in patients with first-episode MDD. Anxiety is one of the most common psychological comorbidities among patients with MDD. Of the overall depressive adolescents, the majority with suicide risk had moderate to severe anxiety symptoms, which were significantly higher than those without suicide risk. However, further analysis found that the coexistence of anxiety was not an independent predictor of suicide risk. This result is consistent with that of a recent study, which showed no statistically significant correlation between MDD with comorbid anxiety and suicidal behavior.67
Although the results of our study add to the understanding of suicide risk in adolescent patients with MDD, several limitations need to be considered. First, the data were collected using a cross-sectional study design, making it impossible to determine the direction of a causal relationship between nightmare stress and suicide risk. Further study with a longitudinal or retrospective cohort design should be employed to establish the relationships among these variables. Second, sleep variables were measured by self-report questionnaires, which may have led to biased reporting of the sleep variables. Therefore, studies must include personal interviews and appropriate objective measures, such as electroencephalography and actigraphy, to overcome the limitations from exclusive use of self-report data. Third, Some studies have shown that the age of onset, life stress, and previous suicide risk of MDD patients are risk factors for their current suicide risk.68,69 However, these variables were not included them in the analysis. Future studies of the relationship between nightmares and suicide will need to include more possible factors influencing suicide risk.
Conclusion
In conclusion, the current study, which included a large clinical population, provides evidence that nightmares occur frequently among adolescent patients with MDD. Furthermore, the results of this study demonstrate that nightmare distress is independently associated with an increased risk of suicide. These findings may have important implications for further research on night-suicide mechanisms and for identifying individuals who are at a risk of suicide by asking about nightmare distress. Since nightmares are potentially modifiable, and the clinical efficacy of psychotherapy is well documented, intervention programs aimed at addressing nightmare-related distress may play an important role in preventing suicide among adolescents with MDD.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Formal approval for the study was obtained from the Ethics Committees of the four participating hospitals (ie, Peking University HuiLongGuan Clinical Medical School, Dongying People’s Hospital, Jining Psychiatric Hospital, and The Third Hospital of Longyan). All participants and their guardians provided written informed consent to indicate their willingness to participate. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2008.
Acknowledgments
The authors would like to thank all the subjects who participated in this study. The authors thank all the researchers and scientific advisors for their contribution to the design of this study. Tian-He Song and Ting-Ting Wang are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Capital Foundation of Medicine the National Key Research and Development Program of China (2021YFC2501504) and Beijing Hospitals Authority Clinical Medicine Development of special funding (XMLX202150).
Disclosure
The authors report no conflicts of interest in this work.
References
1. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858.
2. Mojtabai R, Olfson M, Han B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics. 2016;138(6). doi:10.1542/peds.2016-1878
3. Catalan A, Salazar de Pablo G, Vaquerizo Serrano J, et al. Annual research review: prevention of psychosis in adolescents - systematic review and meta-analysis of advances in detection, prognosis and intervention. J Child Psychol Psychiatry. 2021;62(5):657–673. doi:10.1111/jcpp.13322
4. Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015;56(3):345–365. doi:10.1111/jcpp.12381
5. Belfer ML. Child and adolescent mental disorders: the magnitude of the problem across the globe. J Child Psychol Psychiatry. 2008;49(3):226–236. doi:10.1111/j.1469-7610.2007.01855.x
6. Morales-Munoz I, Broome MR, Marwaha S. Association of parent-reported sleep problems in early childhood with psychotic and borderline personality disorder symptoms in adolescence. JAMA Psychiatry. 2020;77(12):1256–1265. doi:10.1001/jamapsychiatry.2020.1875
7. Tokiya M, Itani O, Otsuka Y, Kaneita Y. Relationship between internet addiction and sleep disturbance in high school students: a cross-sectional study. BMC Pediatr. 2020;20(1):379. doi:10.1186/s12887-020-02275-7
8. Blake MJ, Allen NB. Prevention of internalizing disorders and suicide via adolescent sleep interventions. Curr Opin Psychol. 2020;34:37–42. doi:10.1016/j.copsyc.2019.08.027
9. Kearns JC, Coppersmith DDL, Santee AC, Insel C, Pigeon WR, Glenn CR. Sleep problems and suicide risk in youth: a systematic review, developmental framework, and implications for hospital treatment. Gen Hosp Psychiatry. 2020;63:141–151. doi:10.1016/j.genhosppsych.2018.09.011
10. de Zambotti M, Goldstone A, Colrain IM, Baker FC. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12–24. doi:10.1016/j.smrv.2017.06.009
11. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
12. Hutka P, Krivosova M, Muchova Z, et al. Association of sleep architecture and physiology with depressive disorder and antidepressants treatment. Int J Mol Sci. 2021;22(3):1333. doi:10.3390/ijms22031333
13. Goldstone A, Javitz HS, Claudatos SA, et al. Sleep disturbance predicts depression symptoms in early adolescence: initial findings from the adolescent brain cognitive development study. J Adolesc Health. 2020;66(5):567–574. doi:10.1016/j.jadohealth.2019.12.005
14. Li SX, Lam SP, Yu MWM, Zhang J, Wing YK. Nocturnal sleep disturbances as a predictor of suicide attempts among psychiatric outpatients: a clinical, epidemiologic, prospective study. J Clin Psychiatry. 2010;71(11):1440. doi:10.4088/JCP.09m05661gry
15. Zhao J, Liu H, Wu Z, et al. Clinical features of the patients with major depressive disorder co-occurring insomnia and hypersomnia symptoms: a report of NSSD study. Sleep Med. 2021;81:375–381. doi:10.1016/j.sleep.2021.03.005
16. Chan JW, Lam SP, Li SX, et al. Eveningness and insomnia: independent risk factors of nonremission in major depressive disorder. Sleep. 2014;37(5):911–917. doi:10.5665/sleep.3658
17. Liu X, Yang Y, Liu ZZ, Jia CX. Longitudinal associations of nightmare frequency and nightmare distress with suicidal behavior in adolescents: mediating role of depressive symptoms. Sleep. 2021;44(1). doi:10.1093/sleep/zsaa130
18. Akkaoui MA, Lejoyeux M, d’Ortho MP, Geoffroy PA. Nightmares in patients with major depressive disorder, bipolar disorder, and psychotic disorders: a systematic review. J Clin Med. 2020;9(12):3990. doi:10.3390/jcm9123990
19. Liu X, Liu ZZ, Liu BP, Jia CX. Nightmare frequency and psychopathological problems in a large sample of Chinese adolescents. Soc Psychiatry Psychiatr Epidemiol. 2022;57(4):805–816. doi:10.1007/s00127-022-02224-y
20. Liu X, Liu L, Yang Y, Liu ZZ, Jia CX. Psychometric properties of the Chinese version of nightmare distress questionnaire (NDQ-CV) in adolescents. Sleep Med. 2021;79:94–100. doi:10.1016/j.sleep.2021.01.001
21. Liu X, Liu ZZ, Chen RH, et al. Nightmares are associated with future suicide attempt and non-suicidal self-injury in adolescents. J Clin Psychiatry. 2019;80(4). doi:10.4088/JCP.18m12181
22. Kammerer MK, Bub K, Lincoln TM. The relationship between nightmares and psychotic experiences in young adults. Sleep Med. 2021;77:315–322. doi:10.1016/j.sleep.2020.08.014
23. Stanley IH, Hom MA, Luby JL, et al. Comorbid sleep disorders and suicide risk among children and adolescents with bipolar disorder. J Psychiatr Res. 2017;95:54–59. doi:10.1016/j.jpsychires.2017.07.027
24. van Schagen A, Lancee J, Swart M, Spoormaker V, van den Bout J. Nightmare disorder, psychopathology levels, and coping in a diverse psychiatric sample. J Clin Psychol. 2017;73(1):65–75. doi:10.1002/jclp.22315
25. Swart ML, van Schagen AM, Lancee J, van den Bout J. Prevalence of nightmare disorder in psychiatric outpatients. Psychother Psychosom. 2013;82(4):267–268. doi:10.1159/000343590
26. Eikelenboom M, Beekman ATF, Penninx B, Smit JH. A 6-year longitudinal study of predictors for suicide attempts in major depressive disorder. Psychol Med. 2019;49(6):911–921. doi:10.1017/S0033291718001423
27. Lopes MC, Boronat AC, Wang YP, Fu IL. Sleep complaints as risk factor for suicidal behavior in severely depressed children and adolescents. CNS Neurosci Ther. 2016;22(11):915–920. doi:10.1111/cns.12597
28. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim PA, Dunbar GCL. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33.
29. Chung KF, Kan KK, Yeung WF. Assessing insomnia in adolescents: comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep Med. 2011;12(5):463–470. doi:10.1016/j.sleep.2010.09.019
30. Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
31. Li SH, Graham BM, Werner-Seidler A. Gender differences in adolescent sleep disturbance and treatment response to smartphone app-delivered cognitive behavioral therapy for insomnia: exploratory study. JMIR Form Res. 2021;5(3):e22498. doi:10.2196/22498
32. Liu X, Yang Y, Liu -Z-Z, Chen H, Fan F, Jia C-X. Psychometric assessment of the Chinese adolescent daytime sleepiness scale (CADSS). Sleep Biol Rhythms. 2017;15(3):207–216. doi:10.1007/s41105-017-0106-x
33. Dietch JR, Taylor DJ, Pruiksma K, et al. The nightmare disorder index: development and initial validation in a sample of nurses. Sleep. 2021;44(5). doi:10.1093/sleep/zsaa254
34. Xiong N, Liu Q, Lv X, et al. Demographic and psychosocial variables could predict the occurrence of major depressive disorder, but not the severity of depression in patients with first-episode major depressive disorder in China. J Affect Disord. 2020;274:103–111. doi:10.1016/j.jad.2020.05.065
35. Qi M, Zhou SJ, Guo ZC, et al. The effect of social support on mental health in Chinese adolescents during the outbreak of COVID-19. J Adolesc Health. 2020;67(4):514–518. doi:10.1016/j.jadohealth.2020.07.001
36. Zhou SJ, Wang LL, Yang R, et al. Sleep problems among Chinese adolescents and young adults during the coronavirus-2019 pandemic. Sleep Med. 2020;74:39–47. doi:10.1016/j.sleep.2020.06.001
37. Chen JX, Feng JH, Zhang LG, et al. Association of serum uric acid levels with suicide risk in female patients with major depressive disorder: a comparative cross-sectional study. BMC Psychiatry. 2020;20(1):477. doi:10.1186/s12888-020-02891-8
38. Zzla B, Jyt B, Cxj A, Xl C. Depression as a mediator between frequent nightmares and non-suicidal self-injury among adolescents: a 3-wave longitudinal model - ScienceDirect. Sleep Med. 2020;77:29–34.
39. Li SX, Yu MW, Lam SP, et al. Frequent nightmares in children: familial aggregation and associations with parent-reported behavioral and mood problems. Sleep. 2011;1:487–493. doi:10.1093/sleep/34.4.487
40. Li SX, Zhang B, Li AM, et al. Prevalence and correlates of frequent nightmares: a community-based 2-phase study. Sleep. 2010;33(6):774–780. doi:10.1093/sleep/33.6.774
41. Sba B, Pvac D, Sg A, et al. A systematic review of suicide and suicide attempts in adolescents with psychotic disorders. Schizophr Res. 2021;235:80–90. doi:10.1016/j.schres.2021.07.029
42. Urrila AS, Kiviruusu O, Haravuori H, et al. Sleep symptoms and long-term outcome in adolescents with major depressive disorder: a naturalistic follow-up study. Eur Child Adolesc Psychiatry. 2020;29(5):595–603. doi:10.1007/s00787-019-01436-z
43. Boz S, Lanquart JP, Mungo A, Delhaye M, Loas G, Hein M. Risk of excessive daytime sleepiness associated to major depression in adolescents. Psychiatr Q. 2021;92(4):1473–1488. doi:10.1007/s11126-021-09922-x
44. Geoffroy PA, Oquendo MA, Courtet P, et al. Sleep complaints are associated with increased suicide risk independently of psychiatric disorders: results from a national 3-year prospective study. Mol Psychiatry. 2021;26(6):2126–2136. doi:10.1038/s41380-020-0735-3
45. Russell K, Rasmussen S, Hunter SC. Insomnia and nightmares as markers of risk for suicidal ideation in young people: investigating the role of defeat and entrapment. J Clin Sleep Med. 2018;14(5):775–784. doi:10.5664/jcsm.7104
46. Lamis DA, Innamorati M, Erbuto D, et al. Nightmares and suicide risk in psychiatric patients: the roles of hopelessness and male depressive symptoms. Psychiatry Res. 2018;264:20–25. doi:10.1016/j.psychres.2018.03.053
47. Andrews S, Hanna P. Investigating the psychological mechanisms underlying the relationship between nightmares, suicide and self-harm. Sleep Med Rev. 2020;54:101352. doi:10.1016/j.smrv.2020.101352
48. Littlewood DL, Gooding PA, Panagioti M, Kyle SD. Nightmares and suicide in posttraumatic stress disorder: the mediating role of defeat, entrapment, and hopelessness. J Clin Sleep Med. 2016;12(3):393–399. doi:10.5664/jcsm.5592
49. Marquis LP, Julien SH, Baril AA, et al. Nightmare severity is inversely related to frontal brain activity during waking state picture viewing. J Clin Sleep Med. 2019;15(2):253–264. doi:10.5664/jcsm.7628
50. Tubbs AS, Fernandez FX, Perlis ML, et al. Suicidal ideation is associated with nighttime wakefulness in a community sample. Sleep. 2021;44(1). doi:10.1093/sleep/zsaa128
51. Tang F, Byrne M, Qin P. Psychological distress and risk for suicidal behavior among university students in contemporary China. J Affect Disord. 2018;228:101–108. doi:10.1016/j.jad.2017.12.005
52. Erausquin JT, McCoy TP, Bartlett R, Park E. Trajectories of suicide ideation and attempts from early adolescence to mid-adulthood: associations with race/ethnicity. J Youth Adolesc. 2019;48(9):1796–1805. doi:10.1007/s10964-019-01074-3
53. Rhodes AE, Boyle MH, Bridge JA, et al. Antecedents and sex/gender differences in youth suicidal behavior. World J Psychiatry. 2014;4(4):120–132. doi:10.5498/wjp.v4.i4.120
54. Miranda-Mendizabal A, Castellvi P, Pares-Badell O, et al. Gender differences in suicidal behavior in adolescents and young adults: systematic review and meta-analysis of longitudinal studies. Int J Public Health. 2019;64(2):265–283. doi:10.1007/s00038-018-1196-1
55. Liu X, Yang Y, Liu ZZ, Jia CX. Longitudinal associations of nightmare frequency and nightmare distress with suicidal behavior in adolescents: mediating role of depressive symptoms. Sleep. 2020;44(1):1.
56. Yuan XP. Analysis of risk factors of depressive disorder in adolescents with high risk of suicide. Anhui Medical University; 2022.
57. Kwak CW, Ickovics JR. Adolescent suicide in South Korea: risk factors and proposed multi-dimensional solution. Asian J Psychiatr. 2019;43:150–153. doi:10.1016/j.ajp.2019.05.027
58. Minzenberg MJ, Lesh TA, Niendam TA, et al. Control-related frontal-striatal function is associated with past suicidal ideation and behavior in patients with recent-onset psychotic major mood disorders. J Affect Disord. 2015;188:202–209. doi:10.1016/j.jad.2015.08.049
59. Stanley B, Michel CA, Galfalvy HC, et al. Suicidal subtypes, stress responsivity and impulsive aggression. Psychiatry Res. 2019;280:112486. doi:10.1016/j.psychres.2019.112486
60. Melhem NM, Porta G, Oquendo MA, et al. Severity and variability of depression symptoms predicting suicide attempt in high-risk individuals. JAMA Psychiatry. 2019;76(6):603–613. doi:10.1001/jamapsychiatry.2018.4513
61. Moller CI, Cotton SM, Badcock PB, et al. Relationships between different dimensions of social support and suicidal ideation in young people with major depressive disorder. J Affect Disord. 2021;281:714–720. doi:10.1016/j.jad.2020.11.085
62. Fang X, Zhang C, Wu Z, et al. Prevalence, risk factors and clinical characteristics of suicidal ideation in Chinese patients with depression. J Affect Disord. 2018;235:135–141. doi:10.1016/j.jad.2018.04.027
63. Kang C, Zheng Y, Yang L, et al. Prevalence, risk factors and clinical correlates of suicidal ideation in adolescent patients with depression in a large sample of Chinese. J Affect Disord. 2021;290:272–278. doi:10.1016/j.jad.2021.04.073
64. Horwitz AG, Czyz EK, Berona J, King CA. Prospective associations of coping styles with depression and suicide risk among psychiatric emergency patients. Behav Ther. 2018;49(2):225–236. doi:10.1016/j.beth.2017.07.010
65. Barbuti M, Mazzarini L, Vieta E, et al. Relationships between recurrence and polarity in major depressive disorders: pooled analysis of the BRIDGE and BRIDGE-II-MIX cohorts. J Affect Disord. 2019;256:250–258. doi:10.1016/j.jad.2019.06.005
66. Oquendo MA, Currier D, Mann JJ. Prospective studies of suicidal behavior in major depressive and bipolar disorders: what is the evidence for predictive risk factors? Acta Psychiatr Scand. 2006;114(3):151–158. doi:10.1111/j.1600-0447.2006.00829.x
67. Mathialagan K, Ceren Amuk O, Eskander N, Patel RS. Comorbid anxiety and suicidal behaviors in American adolescents with major depression. Cureus. 2020;12(6):e8598. doi:10.7759/cureus.8598
68. Zhou Y, Ren W, Sun Q, et al. The association of clinical correlates, metabolic parameters, and thyroid hormones with suicide attempts in first-episode and drug-naive patients with major depressive disorder comorbid with anxiety: a large-scale cross-sectional study. Transl Psychiatry. 2021;11(1):97. doi:10.1038/s41398-021-01234-9
69. Lin J, Su Y, Lv X, et al. Perceived stressfulness mediates the effects of subjective social support and negative coping style on suicide risk in Chinese patients with major depressive disorder. J Affect Disord. 2020;265:32–38. doi:10.1016/j.jad.2020.01.026
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.