")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
“NEWS2” as an Objective Assessment of Hospitalised COPD Exacerbation Severity
Authors Stone PW , Minelli C, Feary J, Roberts CM, Quint JK , Hurst JR
Received 19 January 2022
Accepted for publication 12 March 2022
Published 8 April 2022 Volume 2022:17 Pages 763—772
DOI https://doi.org/10.2147/COPD.S359123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Philip W Stone,1 Cosetta Minelli,1 Johanna Feary,1 C Michael Roberts,2 Jennifer K Quint,1,2,* John R Hurst2,3,*
1National Heart and Lung Institute, Imperial College London, London, UK; 2National Asthma and COPD Audit Programme, Royal College of Physicians of London, London, UK; 3UCL Respiratory, University College London, London, UK
*These authors contributed equally to this work
Correspondence: John R Hurst, UCL Respiratory, University College London, London, UK, Email [email protected]
Introduction: There is currently no accepted way to risk-stratify hospitalised exacerbations of chronic obstructive pulmonary disease (COPD). We hypothesised that the revised UK National Early Warning Score (NEWS2) calculated at admission would predict inpatient mortality, need for non-invasive ventilation (NIV) and length-of-stay.
Methods: We included data from 52,284 admissions for exacerbation of COPD. Data were divided into development and validation cohorts. Logistic regression was used to examine relationships between admission NEWS2 and outcome measures. Predictive ability of NEWS2 was assessed using area under receiver operating characteristic curves (AUC). We assessed the benefit of including other baseline data in the prediction models and assessed whether these variables themselves predicted admission NEWS2.
Results: 53% of admissions had low risk, 24% medium risk and 23% a high risk NEWS2 in the development cohort. The proportions dying as an inpatient were 2.2%, 3.6% and 6.5% by NEWS2 risk category, respectively. The proportions needing NIV were 4.4%, 9.2% and 18.0%, respectively. NEWS2 was poorly predictive of length-of-stay (AUC: 0.59[0.57– 0.61]). In the external validation cohort, the AUC (95% CI) for NEWS2 to predict inpatient death and need for NIV were 0.72 (0.68– 0.77) and 0.70 (0.67– 0.73). Inclusion of patient demographic factors, co-morbidity and COPD severity improved model performance. However, only 1.34% of the variation in admission NEWS2 was explained by these baseline variables.
Conclusion: The generic NEWS2 risk assessment tool, readily calculated from simple physiological data, predicts inpatient mortality and need for NIV (but not length-of-stay) at exacerbations of COPD. NEWS2 therefore provides a classification of hospitalised COPD exacerbation severity.
Keywords: COPD, exacerbation, hospital, NEWS2, severity
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a prevalent long-term condition and exacerbations of COPD are a major challenge for global health services.1 In the UK, one in eight emergency admissions to hospital is for exacerbation of COPD, making it the second commonest cause of emergency admission with more than 130,000 cases per year.2 In the most recent data from the UK national COPD audit of 82,268 exacerbation admissions, the inpatient mortality was 3.6% and 10.2% needed support with non-invasive ventilation (NIV).3 Patients who require NIV during admission are more than three and a half times more likely to die within 30 days (AOR: 3.55 [95% CI: 3.23–3.90]) and are a particularly high-risk group to identify and manage. 4
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) classifies COPD exacerbations as mild when needing only a change in inhaled bronchodilators, moderate as requiring oral antibiotics and/or corticosteroids, and severe as those resulting in hospitalisation or visit to an emergency room.1 A recent consensus paper has attempted to provide an objective assessment of exacerbation severity but this “Rome” proposal requires validation.5 Despite clear clinical need to better guide monitoring and treatment decisions, there is no accepted way to further risk-stratify hospitalised COPD exacerbations. Complicating any such assessment, the acuity of an exacerbation presentation represents a composite of the severity of the underlying COPD, the severity of the exacerbation insult, and the presence and severity of any co-morbidities.
A recent systematic review examining risk scoring in COPD concluded no studies at low risk of bias had been designed to risk-stratify COPD exacerbations.6 Whilst offering acceptable prediction of outcomes, the “DECAF” score (comprising dyspnea, eosinopenia, radiographic consolidation, acidemia and atrial fibrillation7) requires blood count, blood gas, chest radiograph and clinical assessment of heart rhythm to score. In addition, DECAF has only been validated in patients with an established, pre-admission spirometric diagnosis of COPD8 (which does not represent clinical reality), and many clinicians consider the presence of radiographic consolidation – a component of DECAF - to represent a diagnosis of pneumonia in COPD, rather than a COPD exacerbation.9
A generic risk prediction tool suitable for use across acute presentations and requiring only simple data would have clear implementation benefits in clinical practice over “DECAF” and “Rome”. One such generic acuity score is the revised UK National Early Warning Score (NEWS2),10 already widely used following endorsement by the UK National Health Service (NHS) as an initial assessment and monitoring tool.11 NEWS2 is readily calculated from routine physiological parameters including respiratory rate, oxygen saturation (noting the presence or absence of oxygen supplementation), systolic blood pressure, pulse rate, level of consciousness and temperature without the need for biochemical or radiological assessment. Established risk-thresholds are employed.10
We hypothesised that NEWS2 would predict clinically important outcomes in hospitalised exacerbations of COPD, including inpatient mortality, the need for NIV and length of stay and these were the primary outcomes of the study. Secondary outcomes were to examine if NEWS2 was predicted by baseline patient factors including COPD disease severity and co-morbidity, and therefore investigate whether NEWS2 was more representative of the patient at baseline than the exacerbation insult.
Methods
Dataset
The National Asthma and COPD Audit Programme (NACAP) supports continuous prospective audit and quality improvement of the care received by patients admitted to hospitals in England, Scotland, and Wales for exacerbations of COPD.12 The over-arching aim is that all patients admitted to hospital and managed as an exacerbation of COPD have data entered into the audit. A limited clinical dataset is entered into an online data collection tool. This analysis uses the 2018–2019 cut of audit data, representing admissions between 01/10/2018 and 30/09/2019. Further details on the 2018–2019 NACAP COPD clinical audit can be found in the published reports.3,4 NACAP is covered by UK National Health Service Section 251 approval from the Confidentiality Advisory Group (CAG) of the Health Research Authority (HRA) and individual patient consent for data collection is not required. The approval reference number is CAG-8-06(b)/2013.
Explanatory and Outcome Variables
We examined the association between NEWS2 and inpatient death, need for acute treatment with NIV at any point during the admission and length of stay for those surviving to discharge. Length of stay had a very skewed distribution and was analysed as a binary outcome, coded as ≤ and > the median length of stay of four days.
NEWS2 was calculated on arrival to hospital in the Emergency Room as previously described10 and was available in 89% of cases. A NEWS2 score of 0–4 is defined as low risk, 5 or 6 as medium risk, and 7 or more as high risk.10
We examined the following potential predictors of outcomes and NEWS2: gender, index of multiple deprivation, COPD severity, smoking status (current, ex-, never), history of cardiovascular disease, and history of mental illness. Definitions of these terms are provided in the published reports,3,4 with COPD severity assessed using the GOLD stage based on the recorded forced expiratory volume in 1 second (FEV1) % predicted.1 Where more than 5% of values for a variable were missing, an additional “not recorded” category was added.
Statistical Analysis
Data management and analyses were performed using Stata 16. English hospitals were randomly split 50:50 to provide separate development and internal validation cohorts for the prediction models. Patients admitted to Welsh hospitals were used as an external validation cohort. Baseline characteristics of the cohorts were summarised using proportions or means and standard deviation (SD) as appropriate. Sensitivity analyses were performed including only those participants who had evidence of COPD on spirometry (most recent FEV1/FVC <0.7).
Univariable Association Between NEWS2 and Exacerbation Outcomes
Logistic regression was used to model the relationship between NEWS2 and the three exacerbation outcomes. The Akaike information criterion (AIC) was used to determine if NEWS2 should be analysed as a categorical (low, medium, or high risk) or continuous variable. All models provided a better fit when using NEWS2 as a continuous variable (lower AIC). Therefore, NEWS2 was included in the models as a continuous variable. Discrimination of NEWS2 in predicting inpatient mortality, requirement for NIV and length of stay was assessed using area under receiver operating characteristic curves (AUC). The optimal NEWS2 value for outcome prediction was chosen based on Youden’s index. Calibration of the NEWS2 models was assessed using calibration plots with deciles of predicted risk plotted against observed risk.
Multivariable Analysis of All Potential Predictors of Exacerbation Outcomes
NEWS2 and other potential predictors were included in logistic regression models for each of the three outcomes to form adjusted models. Age was included in the models as a categorical variable (quintiles). As above, discrimination was assessed using AUC and calibration was assessed using calibration plots.
Predictors of NEWS2
Predictors of NEWS2 were assessed by including all potential predictors in a multiple linear regression model. As with the previous models, calibration was assessed using calibration plots.
Results
The development cohort consisted of 26,776 patients from 83 hospitals and the internal validation cohort consisted of 29,244 patients from 84 hospitals. A total of 2537 patients admitted to 16 Welsh hospitals were used as an external validation cohort. However, as 2595 (9.69%), 3656 (12.50%), and 22 (0.87%) of admissions did not have an available NEWS2 score in the development, validation, and external validation cohorts, respectively, the final numbers of patients available for use in the cohorts were 24,181 (development), 25,588 (internal validation), and 2515 (external validation), Figure 1. Admissions without a NEWS2 recorded did not differ substantially in outcome measures from admissions with NEWS2, with the exception of length of stay in the external validation cohort (Supplementary Tables 1–3).
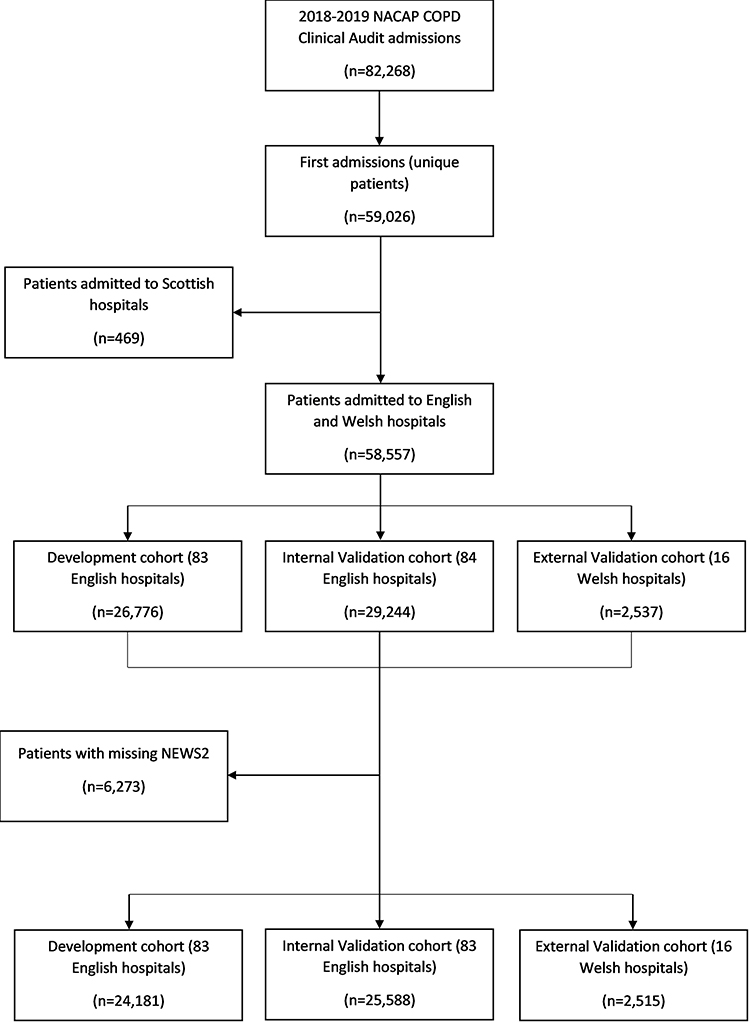 |
Figure 1 Patient flow-chart. |
The patient characteristics and three outcome measures in the three cohorts are reported in Table 1. In the development cohort, the overall inpatient mortality was 3.5%, 8.7% required treatment with NIV and 41.6% had a length of stay greater than the median of four days. Regarding admission NEWS2, 52.7%, 24.0% and 23.3% were in the low, medium and high risk NEWS2 groups, respectively. Outcomes were similar in the internal validation cohort, but inpatient mortality, need for NIV and length of stay appeared higher in the external validation cohort compared with the development cohort (Table 1).
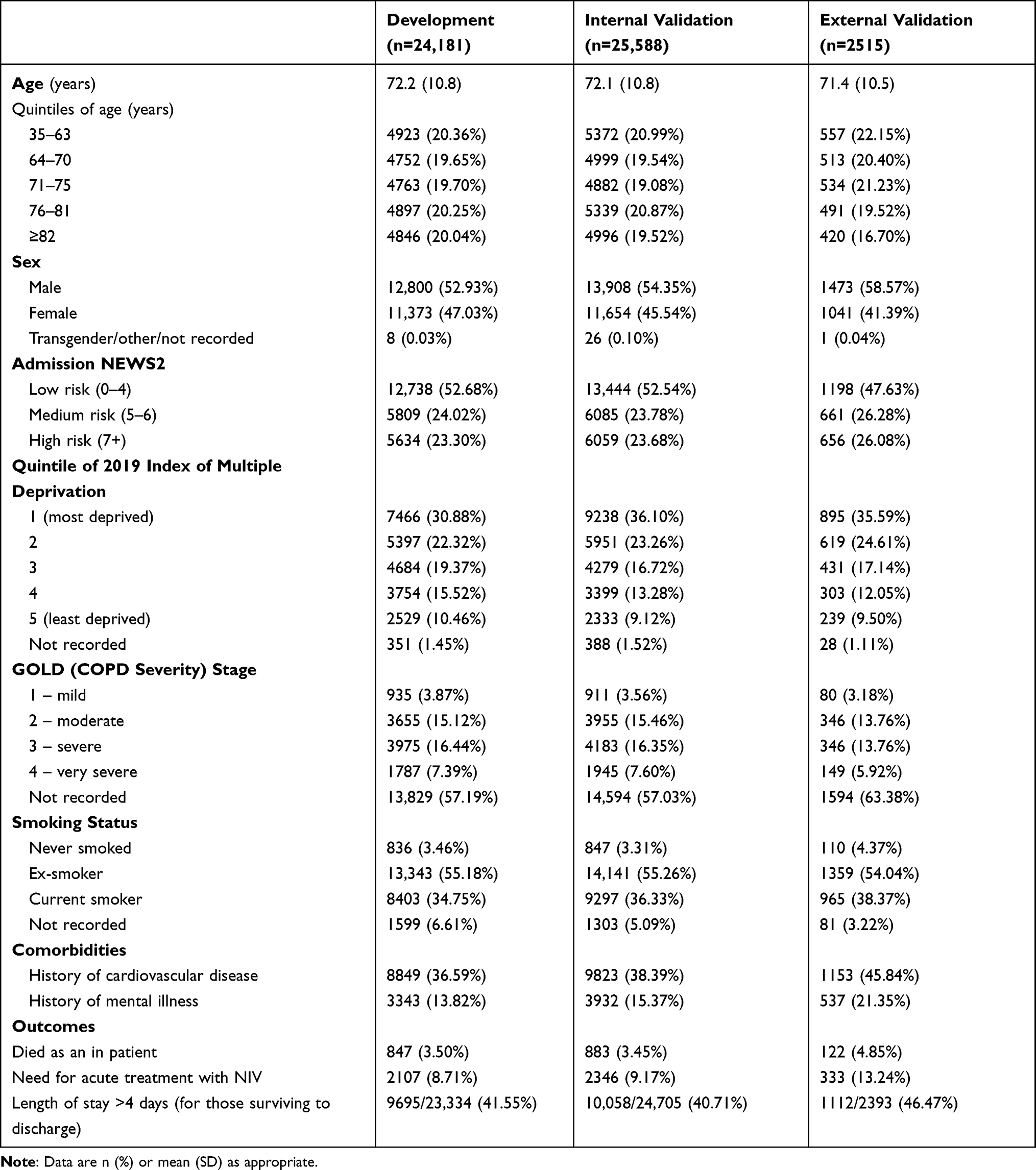 |
Table 1 Characteristics of Patients Included in the Development, Internal Validation, and External Validation Cohorts |
NEWS2 as a Univariable Predictor of Exacerbation Outcomes
In the development cohort, inpatient mortality was 2.2%, 3.6% and 6.5%, respectively, for low, medium and high risk NEWS2. The proportion needing NIV were, respectively, 4.4%, 9.2% and 18.0%. The discriminatory ability of NEWS2 to predict inpatient mortality, need for acute NIV, and hospital stay longer than the median is summarised in Table 2, with the ROC curves illustrated in Supplementary Figure 1. The external validation cohort demonstrates acceptable utility for NEWS2 in predicting inpatient mortality (AUC = 0.72) and need for NIV (AUC = 0.70), but not length of stay (AUC = 0.59).
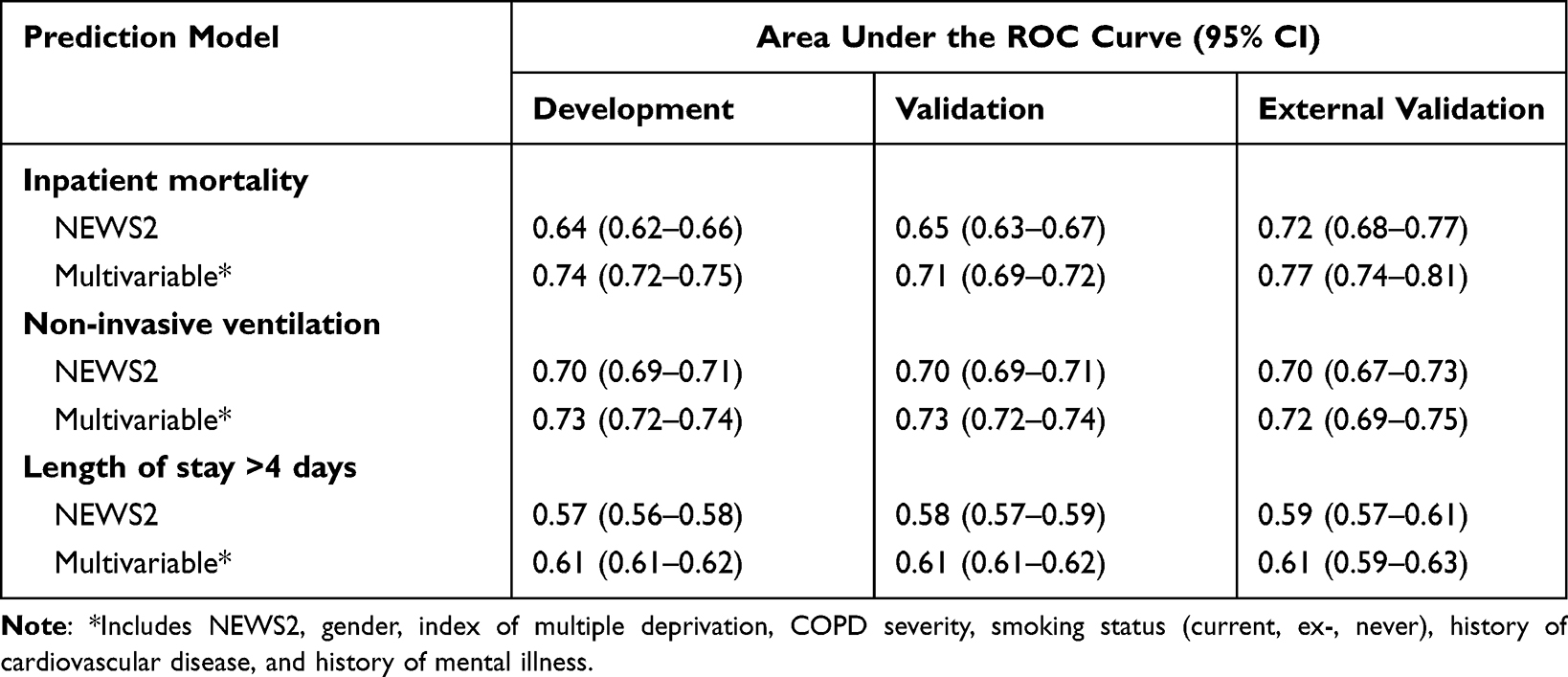 |
Table 2 Area Under the ROC Curve (and 95% CI) for the Univariable NEWS2 and Multivariable Predictive Models |
The performance of individual NEWS2 cut points is provided in Supplementary Tables 4–6 and summarised below in Table 3 for medium and high risk cut points (internal validation cohort). Youden’s index indicated that a NEWS2 of 6 would provide optimal prediction compared to the standard thresholds (Supplementary Table 7). The sensitivity and specificity for inpatient mortality was 55.5% and 65.8%, respectively; 62.5% and 67.8% for predicting the need for acute NIV.
 |
Table 3 NEWS2 Category and Outcome Prediction in the Internal Validation Cohort |
The coefficients for NEWS2 to predict inpatient mortality, need for acute NIV, and a length of stay greater than four days are reported in Supplementary Table 8. For each one-point increase in NEWS2, the odds of inpatient death increased by 20% (OR: 1.20 [95% CI: 1.17–1.23]), odds of needing acute NIV during admission increased by 30% (OR: 1.30 [95% CI: 1.28–1.33]), and the odds of having a hospital stay of more than 4 days increased by 10% (OR: 1.10 [95% CI: 1.09–1.11]). Supplementary Figure 2 shows good calibration in the internal validation cohort, less so in the external validation cohort where there is under-estimation of risk at the highest NEWS2.
Multivariable Predictors of Exacerbation Outcomes
Results from the multivariable analysis for the association of all predictors with inpatient mortality, need for acute NIV and length of stay in the development cohort are reported in Table 4, with model discrimination in comparison to NEWS2 reported in Table 2. Lung function, which was used to calculate GOLD (COPD severity) stage was poorly recorded with 57% of admissions missing this information in the development cohort (Table 1). ROC curves for the NEWS2 and multivariable prediction models for each of the three outcomes in each cohort are presented in Supplementary Figure 1.
 |
Table 4 Results from the Multivariable Analysis for the Association of All Predictors with Inpatient Mortality, Requirement for NIV, and a Length of Stay Greater Than the Median of 4 Days in the Development Cohort |
Adding all potential predictors (including age, deprivation, GOLD stage, smoking status, and history of cardiovascular disease) in the mortality prediction model produced a 7% improvement in AUC to 0.77 (95% CI: 0.74–0.81) in the external validation cohort, compared to 0.72 (95% CI 0.68–0.77) for NEWS2 alone (Table 2).
Adding all potential predictors (including age, deprivation, GOLD stage, smoking status, and history of cardiovascular disease) in the NIV prediction model produced a 3% improvement in AUC to 0.72 (95% CI: 0.69–0.75) in the external validation cohort, compared to 0.70 (95% CI 0.67–0.73) for NEWS2 alone (Table 2).
Adding all potential predictors (including age, deprivation, GOLD stage, smoking status, and history of cardiovascular disease) in the length of stay prediction model produced a 3% improvement in AUC to 0.61 (95% CI: 0.59–0.63) in the external validation cohort, compared to 0.59 (95% CI 0.57–0.61) for NEWS2 alone (Table 2).
Calibration of the multivariable models for each outcome appeared good in the internal validation cohort (Supplementary Figure 2).
Sensitivity analyses restricted to include only those subjects with confirmatory spirometry did not materially affect the results (data not shown).
Multivariable Predictors of NEWS2
Coefficients for the variables included in the NEWS2 prediction model are reported in Supplementary Table 9. Only 1.3% of the variation in admission NEWS2 was explained by age, gender, deprivation, GOLD stage, smoking status, history of cardiovascular disease, and history of mental illness. Calibration of the model to predict NEWS2 was reasonable in the internal validation cohort but less so in the external validation cohort (Supplementary Figure 3).
Discussion
Using data from three cohorts totaling 52,284 admissions to hospital with exacerbations of COPD, we show that a generic risk assessment score (NEWS2), readily calculated at admission from routine clinical variables, is predictive of inpatient mortality and the need for acute NIV, but not length of stay.
For the 23% of patients in the highest risk NEWS2 category, the risk of inpatient death was more than three times higher than the low risk group, and the risk of needing NIV was more than four times higher, with 19.0% needing NIV. Whilst the accuracy is high (number of correct assessments/all assessments), the PPV is lower reflecting that inpatient death and the need for NIV are, fortunately, outcomes seen in only a minority of admissions. Admission NEWS2 is therefore a simple to use and acceptable predictor of important short-term outcomes during a hospital admission for exacerbation of COPD, identifying patients at higher risk of poor outcomes for enhanced early triage, monitoring and treatment and with performance characteristics that we have now precisely defined. In acute settings where there is not yet a risk prediction score in use, NEWS2 has the clear advantage that is generic, not disease specific, and therefore informs on risk in unselected acute medical admissions.
The UK National Early Warning Score (NEWS) was first developed by the Royal College of Physicians of London in 2012.13,14 NEWS was designed to improve the detection of, and response to presentation severity and changes in acuity in patients with unselected acute illness. NEWS was criticised for not accounting for risks associated with over-oxygenation in patients with or at risk of hypercapneic (Type 2) respiratory failure (T2RF; including those with COPD), causing excessive alerts and overuse of oxygen treatment in this vulnerable group. A revised “NEWS2” score was published in 2017 which included a separate oxygenation scale for those with or at risk of T2RF (strictly defined as confirmed T2RF on blood gas analysis at this or a prior admission). NEWS2 was also optimised for better detection of sepsis and delirium.10 NEWS2 is now mandated for use by NHS England11 such that understanding its real-world performance for COPD exacerbation risk-stratification is important,15 whilst utility in predicting short-term outcomes would support the use of NEWS2 in other health-care settings. NEWS2 comprises only simple physiological measures: respiratory rate, peripheral oxygen saturation (noting if breathing air or supplemental oxygen), systolic blood pressure, pulse rate, and temperature together with level of consciousness such that it is readily calculated across emergency health-care settings without the need for laboratory or radiographic investigations. Such variables can readily be incorporated in electronic recording systems, facilitating the wide implementation of NEWS2.
There is the need to better risk stratify hospitalised exacerbations of COPD. A recent systematic review reported on 155 risk prediction models for patients with COPD,6 all of which were considered to be at risk of bias. There is thus no standardised clinical risk prediction tool for hospitalised exacerbations of COPD. There are, in addition, clear advantages of using a generic acuity tool for emergency admissions rather than multiple disease-specific scores, which had been the original stimulus to develop NEWS. It is not clear how NEWS2 performs in COPD compared to unselected acute admissions as studies have generally examined the ability of NEWS2 (and NEWS14) to predict outcomes such as death, cardiac arrest or need for intensive care support over a 24-hour period from the point of observation.
There is some evidence that NEWS2 may provide better risk prediction than the original iteration of NEWS in patients with COPD,16 although this has been controversial17 and may be dependent on how use of the separate oxygen scale for patients at risk of T2RF has been interpreted.18 NEWS2 has also been compared against the disease-specific DECAF score.16 DECAF was designed to predict mortality and inform decisions on need for hospital admission at exacerbation of COPD.7,8 However, DECAF has not been widely implemented, being disease specific and requiring assessment of blood eosinophils, radiographic consolidation, arterial blood pH and cardiac rhythm. Moreover, the DECAF derivation and validation cohorts7,8,16 all consisted of patients with documented pre-existing airflow obstruction (spirometry was not available in more than half of the real-life admissions included in the present analysis, which we addressed through sensitivity analyses as described further below). The DECAF studies also included patients with radiographic consolidation which remains a controversial area in COPD and may be best considered as pneumonia in a patient with underlying COPD.9 Patients with COPD and a primary diagnosis of pneumonia should not have data entered into the national audit. There are existing, alternative risk-prediction tools available for community-acquired pneumonia such as CURB-65.19
We report that variation in NEWS2 was poorly explained by baseline patient demographics, the presence of cardiac co-morbidity20 and COPD disease severity as measured by the degree of airflow obstruction (GOLD stage). As the acuity of an exacerbation presentation represents a composite of the severity of the underlying COPD, the severity of the exacerbation insult, and the presence and severity of co-morbidities, this suggests that NEWS2 may provide an assessment of the severity of the exacerbation insult itself. This is novel, and potentially important because it can facilitate different treatment strategies guided by the severity of the exacerbation insult, independent of impairment due to the underlying COPD, co-morbidity and demographics. There is no current way to define the severity of a hospitalised COPD exacerbation. The current COPD exacerbation severity classification groups all exacerbations requiring hospital admission or emergency room assessment as “severe”.1 This is unsatisfactory given the need to identify those at greatest risk of the poorest outcomes such as the need for NIV and death. Whilst there has been a recent proposal to provide an objective classification of COPD exacerbation severity,5 this requires validation and it is likely that a large proportion of hospitalised events would fall into the “moderate” category.
The UK national COPD audit has assisted transformation of COPD care.12 However, unexplained variations in care persist which may be due to differences in case-mix. The demonstration that NEWS2 associates with important outcomes at exacerbation of COPD suggests that NEWS2 may have utility as a method to adjust for case-mix in clinical audit.
More than 50% of patients admitted to hospital with a COPD exacerbation were in the lowest risk of NEWS2 score. Further studies should be conducted to determine whether NEWS2 can be used to guide decisions about supporting earlier discharge. Further research should also study use of NEWS2 as an acuity score for COPD exacerbations treated in the community. NEWS2 is designed not only to measure acuity but to track acuity over time, aiding detection and management of the deteriorating patient.10 Further research might also explore the utility of examining changes in NEWS2 during COPD exacerbation admissions and how these relate to outcome measures.
There are strengths and weaknesses to our analysis. The strengths include the very large sample size enabling us to examine risk prediction in development and two separate validation datasets. We pragmatically included all first cases presenting to hospital and being managed as COPD exacerbations, as is common in clinical practice, such that not all patients have confirmatory spirometry. Sensitivity analyses restricted to include only those subjects with confirmatory spirometry did not materially affect the results. The most recent data on audit case ascertainment suggest that around 55% of the total number of eligible cases are entered.12 Thus, whilst our sample size is large, we cannot be certain that the admissions included in the audit are truly reflective of all COPD admissions. Our definition of requirement for NIV was based on those receiving NIV. We have not identified any other significant sources of bias or confounding.
In conclusion, we report that the generic NEWS2 risk-assessment tool, readily calculated from routine physiological variables at presentation to hospital with a clinical diagnosis of COPD exacerbation, provides improved prediction of inpatient mortality and the need for acute NIV, but not length of stay. As a measure of exacerbation acuity, distinct from underlying COPD, patient demographics and co-morbidity, NEWS2 can also facilitate better classification of COPD exacerbation severity assessment for the purposes of clinical care, research and audit.
Data Sharing Statement
Data may be obtained from a third party and are not publicly available. Data collected on behalf of HQIP by all NCAPOP projects are routinely reported and these reports are available in the “Resources” section of the HQIP website (https://www.hqip.org.uk/resources/). The reported data are also placed on the data.gov.uk website. Data are also placed upon MyNHS and NHS Choices. For details of how to apply for data that is not in the public domain, please see HQIP’s data access webpages (https://www.hqip.org.uk/national-programmes/accessing-ncapop-data/).
Ethics Approval
The audit operates under Section 251 approval from the Confidentiality Advisory Group of the Health Research Authority. The reference number is CAG-8-06(b)/2013.
Acknowledgments
We thank all contributors to the National Asthma and COPD Audit Programme.
Disclosure
Professor John R Hurst reports personal fees, and non-financial support from pharmaceutical companies that make medicines to treat respiratory disease, outside the submitted work. Mr Philip W Stone and Professor Jennifer K Quint report grants from Royal College of Physicians, during the conduct of the study. Professor C Michael Roberts reports grants from Healthcare Quality Improvement Partnership, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2021. Available from: https://goldcopd.org/2021-gold-reports/.
2. Chronic obstructive pulmonary disease (COPD) update. UK national institute for health and care excellence; 2015. Available from: https://www.nice.org.uk/guidance/qs10/documents/briefing-paper.
3. National COPD audit report. Available from: https://www.nacap.org.uk/nacap/welcome.nsf/vwFiles/NACAP-COPD-SC-202007/$File/NACAP_COPD_SC_Clinical_National_Report_2018_19_060720.pdf?openelement.
4. National COPD audit report. Available from: https://www.nacap.org.uk/nacap/welcome.nsf/vwFiles/NACAP-COPD-SC-202007a/$File/NACAP_COPD_SC_Outcomes_2017-18_Report_290620.pdf?openelement.
5. Celli BR, Fabbri LM, Aaron SD, et al. An updated definition and severity classification of COPD exacerbations: the Rome proposal. Am J Respir Crit Care Med. 2021;27. PMID: 34570991. doi:10.1164/rccm.202108-1819PP
6. Bellou V, Belbasis L, Konstantinidis AK, Tzoulaki I, Evangelou E. Prognostic models for outcome prediction in patients with chronic obstructive pulmonary disease: systematic review and critical appraisal. BMJ. 2019;367:l5358. doi:10.1136/bmj.l5358
7. Steer J, Gibson J, Bourke SC. The DECAF score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax. 2012;67(11):970–976. PMID: 22895999. doi:10.1136/thoraxjnl-2012-202103
8. Echevarria C, Steer J, Heslop-Marshall K, et al. Validation of the DECAF score to predict hospital mortality in acute exacerbations of COPD. Thorax. 2016;71(2):133–140. doi:10.1136/thoraxjnl-2015-207775
9. Hurst JR. Consolidation and Exacerbation of COPD. Med Sci. 2018;6(2):44. PMID: 29865214; PMCID: PMC6024675. doi:10.3390/medsci6020044
10. Royal College of Physicians. National early warning score (NEWS) 2 standardising the assessment of acute-illness severity in the NHS; 2017. Available from: https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-score-news-2.
11. NHS England, Royal College of Physicians. NHS Improvement Patient Safety Alert: Resources to Support the Safe Adoption of the Revised National Early Warning Score (NEWS2). NHS; 2018.
12. Hurst JR, Quint JK, Stone RA, Silove Y, Youde J, Roberts CM. National clinical audit for hospitalised exacerbations of COPD. ERJ Open Res. 2020;6(3):00208–2020. PMID: 32984418; PMCID: PMC7502696. doi:10.1183/23120541.00208-2020
13. Royal College of Physicians of London. National early warning score (NEWS): standardising the assessment of acute-illness severity in the NHS—report of a working party; 2012. Available from: www.rcplondon.ac.uk/resources/national-early-warning-score-news.
14. Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation. 2013;84:465–470. PMID: 23295778. doi:10.1016/j.resuscitation.2012.12.016
15. Smith GB, Redfern OC, Pimentel MA, et al. The National Early Warning Score 2 (NEWS2). Clin Med. 2019;19(3):260. doi:10.7861/clinmedicine.19-3-260
16. Echevarria C, Steer J, Bourke SC. Comparison of early warning scores in patients with COPD exacerbation: DECAF and NEWS score. Thorax. 2019;74(10):941–946. doi:10.1136/thoraxjnl-2019-213470
17. Hodgson LE, Congleton J, Venn R, Forni LG, Roderick PJ. NEWS 2 - too little evidence to implement? Clin Med. 2018;18(5):371–373. doi:10.7861/clinmedicine.18-5-371
18. Williams B. The National Early Warning Score 2 (NEWS2) in patients with hypercapnic respiratory failure. Clin Med. 2019;19:94–95. doi:10.7861/clinmedicine.19-1-94
19. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382. doi:10.1136/thorax.58.5.377
20. Roberts CM, Stone RA, Lowe D, Pursey NA, Buckingham RJ. Co-morbidities and 90-day outcomes in hospitalized COPD exacerbations. COPD. 2011;8(5):354–361. PMID: 21864116. doi:10.3109/15412555.2011.600362
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.