Back to Journals » Infection and Drug Resistance » Volume 19
Neutrophil-to-Lymphocyte Ratio and Systemic Inflammatory Response Index as Predictors of In-Hospital Mortality in Ventilator-Associated Pneumonia Patients
Authors Turbawaty DK ![]() , Dewa A, Indrati AR
, Dewa A, Indrati AR ![]() , Rostini T
, Rostini T
Received 10 November 2025
Accepted for publication 20 February 2026
Published 8 March 2026 Volume 2026:19 572622
DOI https://doi.org/10.2147/IDR.S572622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Dewi Kartika Turbawaty, Ananda Dewa, Agnes Rengga Indrati, Tiene Rostini
Department of Clinical Pathology, Faculty of Medicine Universitas Padjadjaran/Hasan Sadikin General Hospital, Bandung, West Java, Indonesia
Correspondence: Dewi Kartika Turbawaty, Department of Clinical Pathology, Faculty of Medicine Universitas Padjadjaran/Hasan Sadikin General Hospital, Jl. Pasteur No. 38, Bandung, West Java, 40161, Indonesia, Tel +628122150145, Email [email protected]
Purpose: Ventilator-associated pneumonia (VAP) is a common complication in intensive care units (ICUs) with high mortality rates. Early risk stratification is often limited by the lack of availability of complex prognostic scoring and microbiology turnaround time. This study aimed to assess the neutrophil-to-lymphocyte ratio (NLR) and systemic inflammatory response index (SIRI) on the day of VAP diagnosis as predictors of in-hospital mortality.
Patients and Methods: We conducted a retrospective cohort study using secondary data from mechanically ventilated adult patients with VAP admitted to Hasan Sadikin General Hospital (a tertiary referral hospital in Bandung, Indonesia) from January 1, 2021 to December 31, 2022. VAP was confirmed by chart review using standard clinical and radiologic criteria occurring ≥ 48 hours after the start of mechanical ventilation, with endotracheal aspirate culture when available. The primary outcome was all-cause in-hospital mortality (death before hospital discharge). NLR and SIRI were calculated from the first complete blood count on the day of VAP diagnosis. Optimal cut-offs were determined using ROC analysis (Youden index). Survival was analyzed from VAP diagnosis until death or discharge.
Results: Among 87 patients, 68 died in hospital and 19 survived to discharge. NLR had excellent discriminatory power for in-hospital mortality (AUC 0.981); a cut-off > 11 had 100% sensitivity and 89.5% specificity. SIRI had good discriminatory power (AUC 0.860); a cut-off > 16 had 64.7% sensitivity and 100% specificity. In univariable Cox models, NLR > 11 was associated with increased mortality risk (HR 29.07; 95% CI 2.24– 376.92), whereas SIRI > 16 showed a non-significant trend (HR 1.55; 95% CI 0.93– 2.57).
Conclusion: NLR and SIRI obtained on the day of VAP diagnosis are simple, non-invasive laboratory markers that could aid in early risk stratification for in-hospital mortality in VAP. These markers should not replace but rather complement established clinical severity assessment and treatment decisions.
Keywords: ventilator-associated pneumonia, neutrophil-to-lymphocyte ratio, systemic inflammatory response index, mortality, NLR, SIRI
Introduction
Ventilator-Associated Pneumonia (VAP) is the most common nosocomial infection in intensive care units, particularly among patients on mechanical ventilation. VAP is a potentially life-threatening complication for patients in the Intensive Care Unit (ICU) and has a high mortality rate.1
One of the difficulties in the infection management process is the lack of a gold standard diagnostic test. As a result, the present diagnostic criteria include clinical manifestations (fever above 38°C, purulent tracheobronchial secretions, and leukocytosis), which have a low sensitivity and specificity of 69% and 75%, respectively. This results in a high rate of both under- and overdiagnosis, resulting in inappropriate medical therapy.1–3
In Indonesia, VAP is often complicated by multidrug-resistant (MDR) Gram-negative bacteria, carbapenem-resistant Acinetobacter baumannii (CRAB), and the availability of new anti-MDR drugs may be inconstant in hospitals. In these situations, the use of inexpensive and readily available prognostic tests from routine complete blood counts may assist in early prioritization of care escalation and discussions about patient prognosis while waiting for microbiology and clinical outcomes.
Although prognostic scoring systems like APACHE II and SOFA are commonly used in ICU populations, they require multiple physiologic variables and may not be readily available or recalculated quickly in resource-limited settings.4,5 Inflammatory variables like NLR and SIRI, which are simple and readily available, may therefore provide complementary risk stratification information at the bedside.
Several variables have been investigated to predict outcomes in VAP, including in-hospital mortality, to facilitate earlier therapeutic decisions. Several studies have identified neutrophil-to-lymphocyte ratio (NLR) and systemic inflammatory response index (SIRI) as readily available variables that reflect systemic inflammation.6
NLR is determined by absolute neutrophil and lymphocyte counts, while SIRI includes neutrophils, monocytes, and lymphocytes. In severe bacterial infection and sepsis-like physiology in VAP, innate immune activation (such as IL-6, TNF-α) leads to neutrophilia and monocytosis, while lymphopenia may occur due to stress-related redistribution and apoptosis (including anti-inflammatory cytokine signaling such as IL-10). Because these processes can occur early, values determined by the first complete blood count at the time of VAP diagnosis may reflect early inflammatory burden.7,8 Therefore, this study sought to assess NLR and SIRI values on the day of VAP diagnosis as predictors of in-hospital mortality in VAP patients.
Materials and Methods
Study Design and Population
This retrospective observational study evaluated whether NLR and SIRI values measured on the day of VAP diagnosis can predict in-hospital mortality. Adult ICU inpatients undergoing invasive mechanical ventilation at Hasan Sadikin General Hospital from January 2021 to December 2022 were identified through ICU ventilation data and diagnostic codes, and VAP was validated through chart review. VAP was identified as pneumonia occurring ≥48 hours after the start of invasive mechanical ventilation for an underlying condition, with new or progressive pulmonary infiltrates and at least two of the following: fever or hypothermia, leukocytosis or leukopenia, purulent respiratory secretions, or evidence of worsening oxygenation. Patients ventilated for pneumonia at admission were eligible only if they met these criteria ≥48 hours after ventilation, indicating a new VAP episode rather than persistence of the index pneumonia. Ethical approval was granted by the Ethics Committee of Hasan Sadikin General Hospital, Bandung (LB.02.01/X.6.5/270/2023).
Inclusion criteria were adults (≥18 years) with confirmed VAP and a complete blood count (CBC) performed on the day of VAP diagnosis (day 0). Exclusion criteria included malignancy, aplastic anemia, COVID-19, chemotherapy or radiotherapy within four months prior to VAP diagnosis, HIV infection, and the use of systemic corticosteroids or other anti-inflammatory therapies at or near the time of VAP diagnosis (Figure 1).
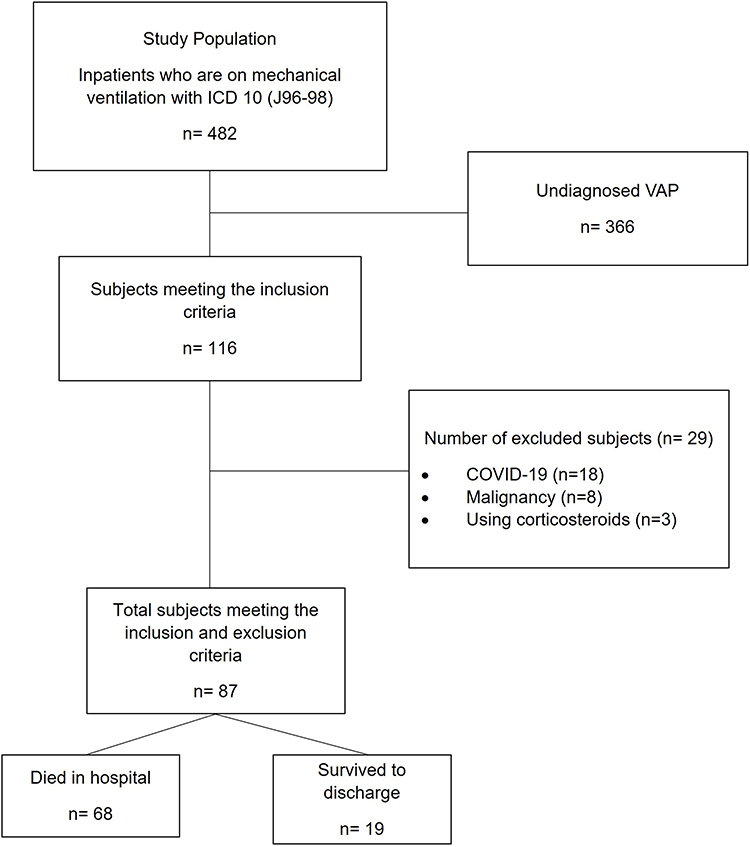 |
Figure 1 Flowchart of Subject Selection. Abbreviations: COVID-19, coronavirus disease 2019; ICD, International Classification of Diseases; n, number of patients; VAP, ventilator-associated pneumonia. |
Data were extracted from medical records and the Laboratory Information System (LIS). Collected variables included age, sex, admission diagnosis, CBC parameters on day 0, endotracheal aspirate culture results, and length of hospital stay. NLR was calculated as the absolute neutrophil count divided by the absolute lymphocyte count, while SIRI was calculated as (absolute neutrophil count × absolute monocyte count) divided by the absolute lymphocyte count. The primary outcome was all-cause in-hospital mortality, defined as death before hospital discharge. Patients discharged alive were classified as survivors to discharge based on documentation of clinical stabilization and discharge disposition. Time-to-event analyses used day 0 as the starting point and followed patients until death or hospital discharge.
Statistical analyses were conducted using SPSS software version 25. Categorical variables were presented as frequencies and percentages and compared using the Chi-square test or Fisher’s exact test, as appropriate. Continuous variables were expressed as medians (range) and compared using the Mann–Whitney U-test. The discriminatory performance of NLR and SIRI for predicting in-hospital mortality was evaluated using receiver operating characteristic (ROC) curve analysis, with optimal cut-off values determined by the Youden index.9 Survival from day 0 to death was analyzed using univariable Cox proportional hazards models, with discharge alive treated as a censoring event. Due to the limited sample size and the risk of model instability, multivariable analyses were not performed and are acknowledged as a study limitation.
Results
The baseline characteristics are summarized in Table 1. The median age was higher among patients who died in hospital compared with those who survived to discharge (61 [21–87] vs 42 [19–76] years; p=0.013). Median NLR and SIRI values on day 0 were also significantly higher in non-survivors than in survivors (NLR 23.5 vs 8.8; SIRI 19.3 vs 6.7; both p<0.001).
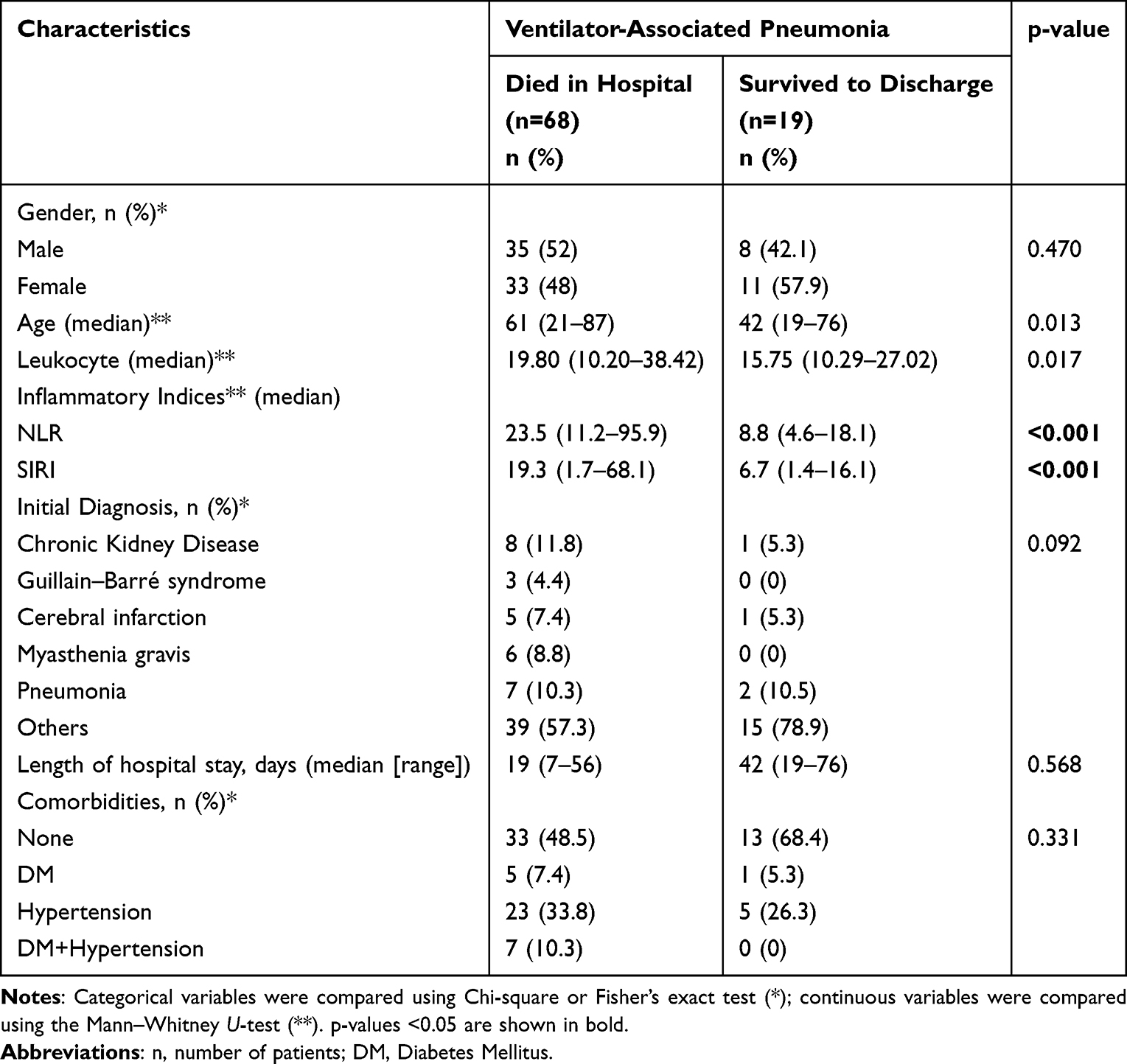 |
Table 1 Basic Characteristics of Subjects by In-Hospital Outcome |
Receiver operating characteristic (ROC) analysis (Table 2 and Figure 2) demonstrated that the optimal cut-off value for NLR in predicting in-hospital mortality was >11, with an AUC of 0.981, sensitivity of 100%, and specificity of 89.5%. For SIRI, the optimal cut-off value was >16, yielding an AUC of 0.860, sensitivity of 64.7%, and specificity of 100%.
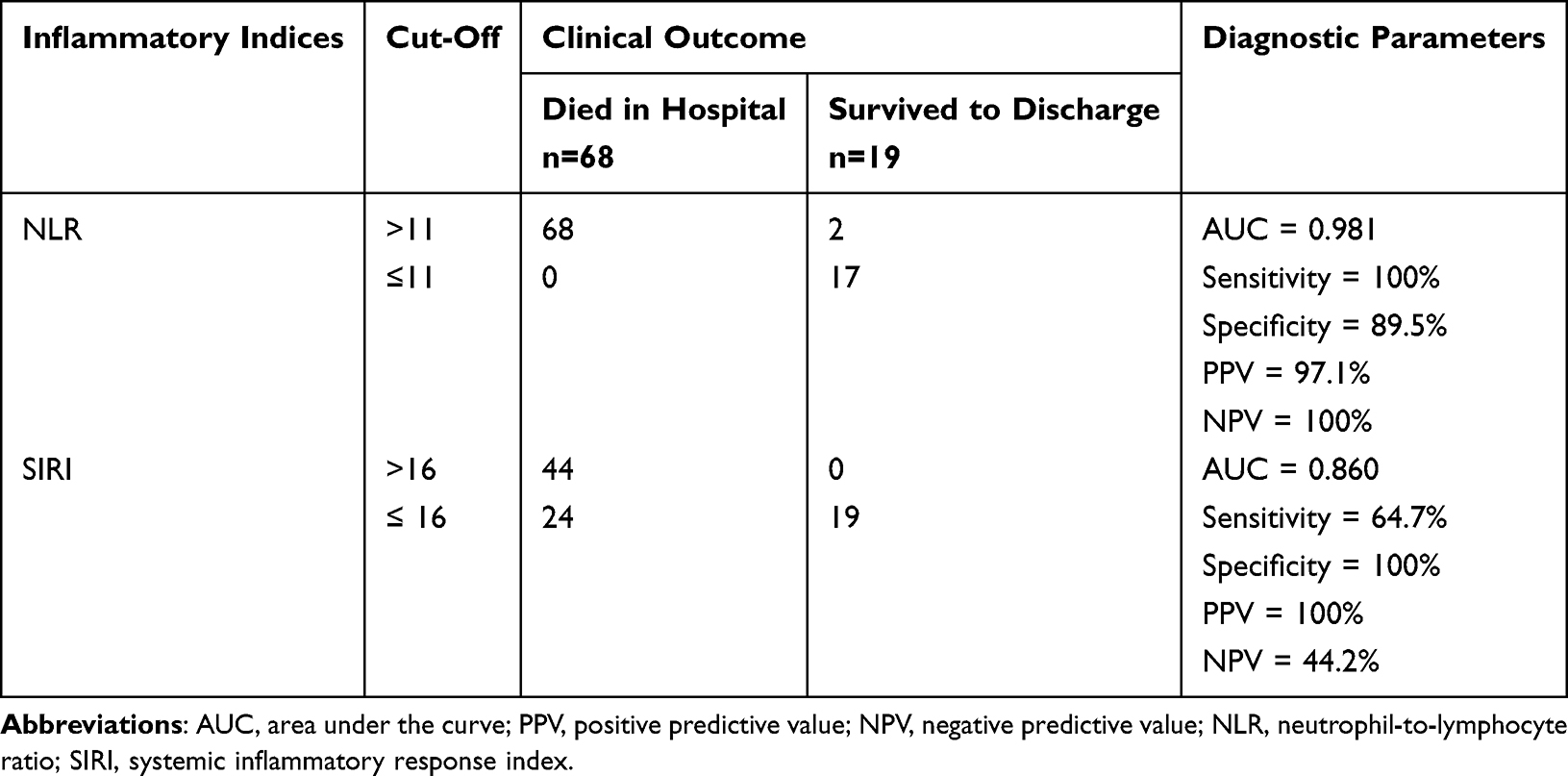 |
Table 2 Diagnostic Performance of NLR and SIRI on Day 0 for Predicting In-Hospital Mortality |
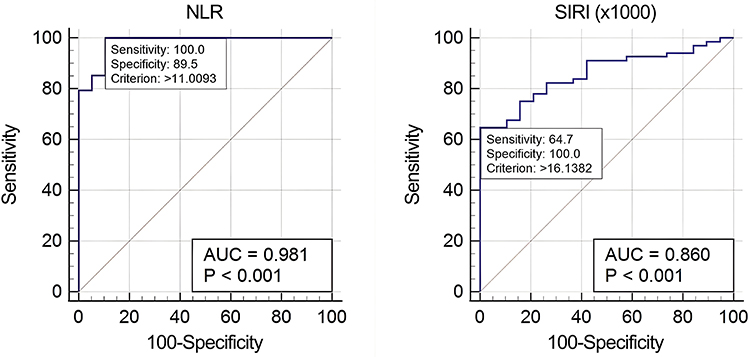 |
Figure 2 Receiver Operating Characteristic (ROC) Curves of NLR and SIRI for Predicting In-Hospital Mortality in Ventilator-Associated Pneumonia (VAP). Abbreviations: AUC, Area Under Curve; P, p-value; NLR, Neutrophil to Lymphocyte Ratio; SIRI, Systemic Inflammatory Response Index. |
Diagnostic performance was further evaluated using 2×2 contingency tables, and AUC, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated (Table 2). At the cut-off point of >11, NLR showed a PPV of 97.1% and an NPV of 100%. For SIRI, using a cut-off point of >16, the PPV was 100% and the NPV was 44.2%.
Mortality risk analysis in VAP patients with outcomes of death or survival to discharge was performed using hazard ratios (HR) and Kaplan–Meier survival curves (Table 3 and Figure 3). Patients with NLR >11 had a markedly increased risk of mortality (HR 29.07; 95% CI: 2.24–376.92), whereas SIRI >16 was associated with a non-significant increase in mortality risk (HR 1.55; 95% CI: 0.93–2.57).
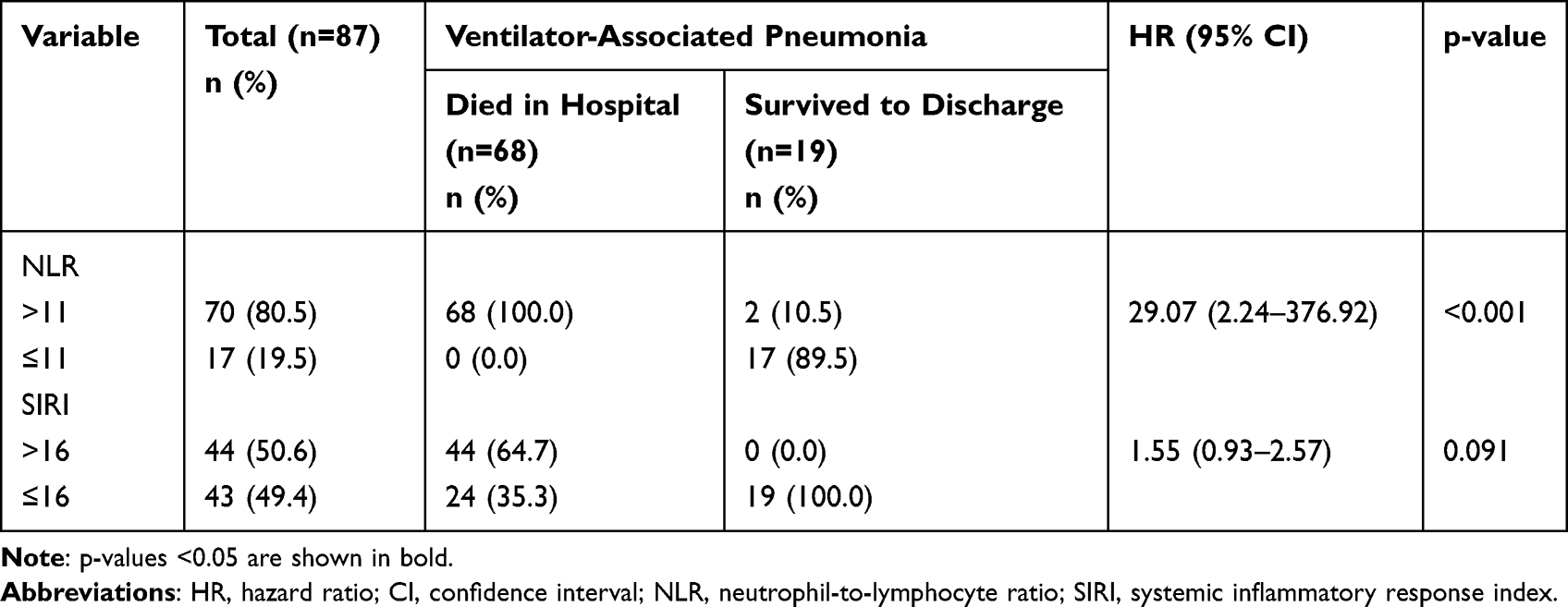 |
Table 3 Univariable Cox Analysis of NLR and SIRI for Time to In-Hospital Death (Time Origin: VAP Diagnosis) |
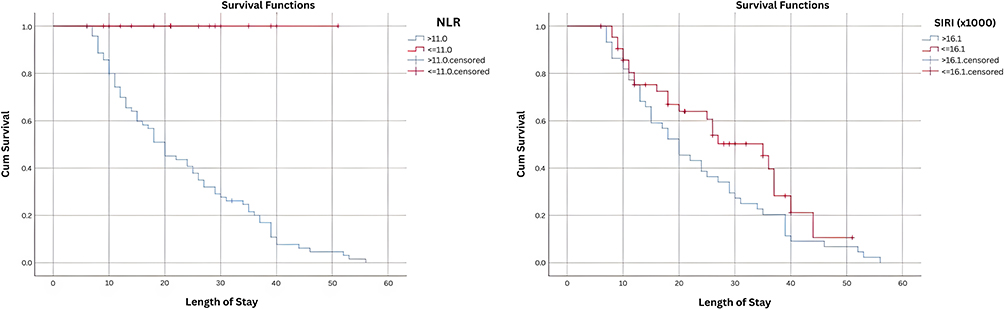 |
Figure 3 Kaplan-Meier Curve of SIRI Inflammatory Index as a Predictor of In-Hospital Mortality in Ventilator-Associated Pneumonia (VAP). Abbreviations: NLR, Neutrophil to Lymphocyte Ratio; SIRI, Systemic Inflammatory Response Index. |
Several bacterial pathogens were identified from endotracheal aspirate sputum cultures. As shown in Table 4, 19 patients (21.8%) had no bacterial growth in culture. Acinetobacter baumannii was the most frequently isolated organism, identified in 32 cases (47%) among patients who died and in 5 cases (26.4%) among those who survived to discharge. Of the 32 A. baumannii isolates in the mortality group, 31 (45.6%) were carbapenem-resistant.
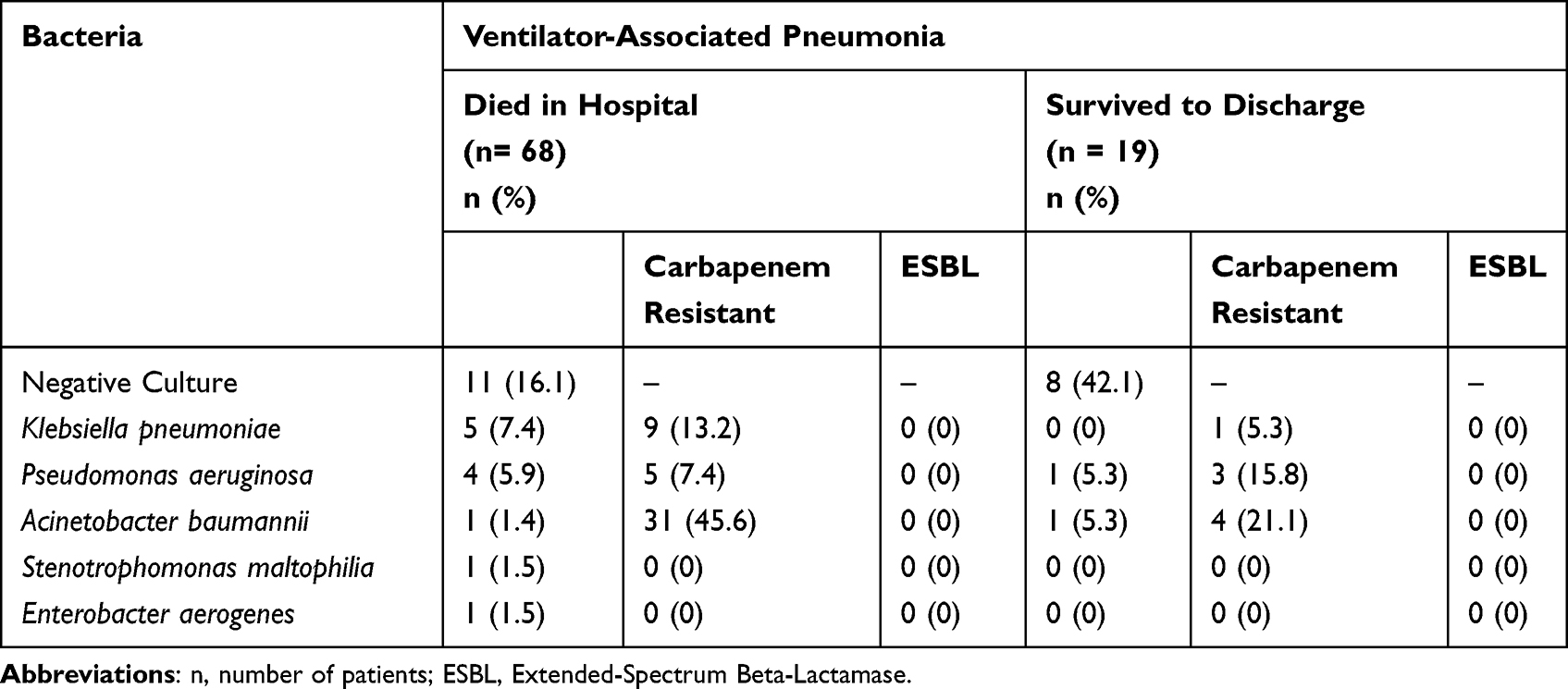 |
Table 4 Endotracheal Aspirate Culture Results in Ventilator-Associated Pneumonia Patients |
Discussion
Our key result is that NLR measured on the day of VAP diagnosis showed excellent discrimination for in-hospital mortality (AUC 0.981) and was strongly associated with time to death in univariable survival analysis. SIRI also demonstrated good discriminatory ability, with perfect specificity at the selected cut-off, but had lower sensitivity and did not show a statistically significant association with mortality risk in the Cox regression model.
Patients who died were older than those who survived, highlighting the heterogeneity of VAP populations and the importance of baseline host factors in determining outcomes. Advanced age has consistently been linked to poorer outcomes in VAP and other critical illnesses, likely reflecting the combined effects of immunosenescence and a higher burden of comorbidities.10–12
The identified NLR threshold (>11) is comparable to cut-off values reported in previous pneumonia and ICU studies and supports the concept that early neutrophilia accompanied by lymphopenia reflects a heightened systemic inflammatory response and physiologic stress.13 In severe infections, pro-inflammatory cytokines such as IL-6 and TNF-α promote neutrophil recruitment, while stress-related responses and apoptosis contribute to lymphopenia, together resulting in an elevated NLR.14,15
SIRI incorporates monocytes in addition to neutrophils and lymphocytes. Although monocytes play a key role in antimicrobial defense and cytokine signaling, their levels may vary depending on the timing of measurement, prior antimicrobial exposure, and the balance between pro- and anti-inflammatory pathways.16–18 These factors may help explain why SIRI showed high specificity but lower sensitivity in this cohort and why its association with mortality did not reach statistical significance.
In Indonesia and other settings with a high prevalence of multidrug-resistant Gram-negative VAP, particularly CRAB, early risk stratification may be clinically valuable to prioritize closer monitoring, prompt escalation of supportive care, and timely optimization of antimicrobial therapy while awaiting culture and susceptibility results.19,20 However, because NLR and SIRI were not used to guide treatment decisions in this retrospective study, it cannot be concluded that awareness of these biomarkers improves outcomes. Rather, they should be considered complementary tools alongside established severity scoring systems, such as APACHE II and SOFA, and antimicrobial stewardship practices.4,5
Several limitations should be acknowledged. First, this was a single-center retrospective study with an imbalanced outcome distribution and a small number of survivors, which may have inflated performance estimates and contributed to the wide confidence interval observed for the NLR hazard ratio, indicating statistical uncertainty. Second, detailed data on antimicrobial therapy (including empiric selection, timing, and de-escalation) and physiologic ventilation parameters (such as the PaO2/FiO2 ratio) were not consistently available, limiting adjustment for treatment effects and disease severity. Third, outcome assessment was limited to in-hospital discharge status, and post-discharge outcomes were not captured. Future prospective studies should assess serial measurements, integrate NLR and SIRI with established severity scores, and evaluate whether biomarker-guided strategies can improve patient-centered outcomes.
Conclusion
NLR and SIRI values derived from a routine complete blood count on the day of VAP diagnosis were associated with in-hospital outcomes in this cohort. An NLR cut-off of >11 demonstrated excellent discrimination for in-hospital mortality, while a SIRI cut-off of >16 showed high specificity but lower sensitivity.
In clinical practice, these simple and inexpensive indices may aid early bedside risk stratification by helping clinicians identify patients who could benefit from closer monitoring, early escalation of supportive care, and timely reassessment of antimicrobial therapy while awaiting microbiological results. However, given the retrospective design and limited sample size of this study, prospective validation and integration with established severity scoring systems are necessary before fixed cut-off values can be adopted for routine clinical decision-making.
Ethical Considerations
This research was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of Hasan Sadikin General Hospital (LB.02.01/X.6.5/270/2023). The requirement for informed consent was waived by the Ethics Committee due to the retrospective design of the study and the use of data obtained from hospital and laboratory information systems. All collected data were anonymized to protect patient privacy and confidentiality.
Acknowledgments
The authors would like to thank Evan Susandi for his role as a statistical consultant, Sapta for assistance as a medical record manager in obtaining patient medical records, Dr. Delita Prihatni, Dr. SpPK(K), Head of the Laboratory Installation at Hasan Sadikin Hospital Bandung, and Dr. dr. Jimmy Panelewen, SpB-KBD, Director of Hasan Sadikin Hospital. This study was supported by an internal grant from Universitas Padjadjaran, Bandung, West Java, Indonesia.
Disclosure
The authors declare no relevant financial disclosures or conflicts of interest.
References
1. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clinl Infect Dis. 2016;63(5):e61–8. doi:10.1093/cid/ciw353
2. Kumar A, Lodha R. Biomarkers for diagnosing ventilator associated pneumonia: is that the way forward? Indian J Pediatr. 2018;85:411–412. doi:10.1007/s12098-018-2672-6
3. Kollef MH. Ventilator-associated pneumonia: the role of emerging therapies and diagnostics. Chest. 2015;147(6):1448–1450. doi:10.1378/chest.14-2745
4. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
5. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
6. Abers M, Musher D. Clinical prediction rules in community-acquired pneumonia: lies, damn lies and statistics. QJM. 2014;107(7):595–596. doi:10.1093/qjmed/hcu096
7. Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
8. Biyik M, Biyik Z, Asil M, Keskin M. Systemic inflammation response index and systemic immune inflammation index are associated with clinical outcomes in patients with acute pancreatitis? J Invest Surg. 2022;35(8):1613–1620. doi:10.1080/08941939.2022.2084187
9. Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3(1):32–35. doi:10.1002/1097-0142(1950)3:1<32::AID-CNCR2820030106>3.0.CO;2-3
10. Ariel Núñez S, Roveda G, Soledad Zárate M, Emmerich M, Teresa Verón M. Ventilator-associated pneumonia in patients on prolonged mechanical ventilation: description, risk factors for mortality, and performance of the SOFA score. J Bras Pneumol. 2021;e20200569. doi:10.36416/1806-3756/e20200569
11. Tuon FF, Graf ME, Merlini A, et al. Risk factors for mortality in patients with ventilator-associated pneumonia caused by carbapenem-resistant Enterobacteriaceae. Braz J Infect Dis. 2017;21(1):1–6. doi:10.1016/j.bjid.2016.09.008
12. Koulenti D, Blot S, Dimopoulos G, et al. 107: ventilator-associated pneumonia in middle-aged, old, and very-old icu patients. Crit Care Med. 2012;40(12):1. doi:10.1097/01.ccm.0000424327.87141.47
13. Kuikel S, Pathak N, Poudel S, et al. Neutrophil–lymphocyte ratio as a predictor of adverse outcome in patients with community‐acquired pneumonia: a systematic review. Health Sci Rep. 2022;5(3):e630. doi:10.1002/hsr2.630
14. Kido T, Tamagawa E, Bai N, et al. Particulate matter induces translocation of IL-6 from the lung to the systemic circulation. Am J Respir Cell Mol Biol. 2011;44(2):197–204. doi:10.1165/rcmb.2009-0427OC
15. Hiraiwa K, van Eeden SF, Hiraiwa K, van Eeden SF. Nature and consequences of the systemic inflammatory response induced by lung inflammation. In: Lung Inflammation. IntechOpen; 2014.
16. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
17. Xu L, Yu S, Zhuang L, et al. Systemic inflammation response index (SIRI) predicts prognosis in hepatocellular carcinoma patients. Oncotarget. 2017;8(21):34954. doi:10.18632/oncotarget.16865
18. Li YT, Wang YC, Lee HL, Tsao SC, Lu MC, Yang SF. Monocyte chemoattractant protein-1, a possible biomarker of multiorgan failure and mortality in ventilator-associated pneumonia. Int J Mol Sci. 2019;20(9):2218. doi:10.3390/ijms20092218
19. Yin Y, Zhao C, Li H, et al. Clinical and microbiological characteristics of adults with hospital-acquired pneumonia: a 10-year prospective observational study in China. Eur J Clin Microbiol Infect Dis. 2021;40:683–690. doi:10.1007/s10096-020-04046-9
20. Kyriakidis I, Vasileiou E, Pana ZD, Tragiannidis A. Acinetobacter baumannii antibiotic resistance mechanisms. Pathogens. 2021;10(3):373. doi:10.3390/pathogens10030373
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Significance of Admission-Day Blood Routine-Derived Indices for 30-Day Mortality Risk in Elderly Patients with Bacterial Pneumonia
Huang X, Huang L, Zhao S, Yuan L, Wang X, Tang G, Yuan K, Xiao M
International Journal of General Medicine 2025, 18:1295-1309
Published Date: 5 March 2025
Diagnostic Significance of Hematological Parameters and Ratios in the Context of Mycobacterium Avium Complex Pulmonary Disease Across Various Age Groups

Long X, Li Q, Wang H, Wang S, Ren Z, Wang X, Gao Y
Infection and Drug Resistance 2025, 18:4847-4862
Published Date: 13 September 2025