Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Neurologists’ Openness to Evidence-Based Innovation in Multiple Sclerosis Care: Individual and Structural Determinants
Authors Monreal E, Gómez-Ballesteros R ![]() , Meca-Lallana V, Caminero AB, Meca-Lallana JE
, Meca-Lallana V, Caminero AB, Meca-Lallana JE ![]() , Martínez-Yélamos S, Landete L, García-Domínguez JM
, Martínez-Yélamos S, Landete L, García-Domínguez JM ![]() , Agüera E, García-Arcelay E, Medrano N, Villar LM, Maurino J
, Agüera E, García-Arcelay E, Medrano N, Villar LM, Maurino J ![]()
Received 23 February 2025
Accepted for publication 14 July 2025
Published 29 July 2025 Volume 2025:21 Pages 1523—1531
DOI https://doi.org/10.2147/NDT.S524459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Enric Monreal,1 Rocío Gómez-Ballesteros,2 Virginia Meca-Lallana,3 Ana B Caminero,4 Jose E Meca-Lallana,5 Sergio Martínez-Yélamos,6 Lamberto Landete,7 Jose M García-Domínguez,8 Eduardo Agüera,9 Elena García-Arcelay,2 Nicolas Medrano,2 Luisa M Villar,10 Jorge Maurino2
1Department of Neurology, Hospital Universitario Ramón y Cajal, Madrid, Spain; 2Medical Department, Roche Farma, Madrid, Spain; 3Department of Neurology, Hospital Universitario La Princesa, Madrid, Spain; 4Department of Neurology, Complejo Asistencial de Ávila, Ávila, Spain; 5Department of Neurology, Hospital Clinico Universitario Virgen de la Arrixaca, Murcia, Spain; 6Department of Neurology, Hospital Universitari de Bellvitge, Barcelona, Spain; 7Department of Neurology, Hospital Universitario Dr. Peset, Valencia, Spain; 8Department of Neurology, Hospital Universitario Gregorio Marañón, Madrid, Spain; 9Department of Neurology, Hospital Universitario Reina Sofía, Córdoba, Spain; 10Department of Immunology, Hospital Universitario Ramón y Cajal, Madrid, Spain
Correspondence: Jorge Maurino, Medical Department, Roche Farma, Ribera del Loira 50 (28042), Madrid, Spain, Tel +34 91 324 8100, Email [email protected]
Purpose: Integration of evidence-based innovations, such as serum neurofilament light chain (sNfL) measurement into routine practice represents a pivotal opportunity to advance personalized care in multiple sclerosis (MS) management. This study assessed neurologists’ openness to adopting healthcare innovations (sNfL testing), focusing on individual characteristics and structural factors like workplace environment and resources.
Methods: An observational, cross-sectional study was conducted in partnership with the Spanish Society of Neurology. Neurologists caring for patients with MS completed an e-survey assessing openness to innovation using the Openness subscale of the Evidence-Based Practice Attitude Scale (EBPAS), alongside measures of empathy, healthcare-related regret, risk preferences, burnout, and workplace communication. Logistic and linear regression models were conducted to identify predictors of openness to innovation.
Results: One hundred and sixteen neurologists were studied. Mean age (SD) was 41.9 (10.1) years, 53.4% were male. Mean experience as neurologists was 16.0 (9.2) years and 96.6% worked in an academic hospital. Median (IQR) EBPAS-Openness score was 3.0 (2.5– 3.5), with 54.3% (n=63) of participants demonstrating openness to innovation. Participants fully dedicated to MS care, managing higher patient volumes, engaged in research publications, with access to serum neurofilament light chain testing, and a greater propensity for risk-taking, were more open to adopting innovations than their counterparts. Multivariate logistic regression analysis showed that access to sNfL testing and higher empathy levels were significant predictors of openness (OR=3.52, CI 95%: 1.3– 10.3; p=0.016 and OR=1.09, CI 95%: 1.0– 1.2; p=0.005, respectively). Complementary linear regression reinforced the significant positive association between higher EBPAS-Openness scores and empathy (estimate=0.024, p=0.001).
Conclusion: Neurologists exhibited a varied openness to innovation. Implementing initial innovative strategies in clinical practice should prioritize neurologists with specific profiles to support the integration of emerging tools and personalized healthcare approaches in MS care.
Keywords: innovation, multiple sclerosis, decision-making, neurofilament light chain, personalized medicine
Introduction
A cornerstone of modern healthcare, particularly in the era of personalized medicine, is the integration of evidence-based advancements into clinical practice.1 Such innovation can be defined as the judicious integration of the best available research evidence with clinical expertise and patient values to guide healthcare decisions and the adoption of novel practices, tools, or treatments.2,3 This approach ensures that new developments are not merely novel but are also supported by robust scientific evidence and align with the practical realities and ethical considerations of patient care.
Advances in diagnostic tools, biomarkers, and treatment modalities hold the potential to transform patient care. However, their successful integration into practice relies not only on the strength of the supporting evidence but also on the perspectives and behaviors of the healthcare professionals responsible for their implementation.2–5 The primary barriers to innovation within healthcare institutions include insufficient access to information, psychological unpreparedness, entrenched routines and resistance to change, apprehension about potential failure, and the influence of prior negative experiences.5
Different medical specialties tend to embrace innovation in distinct ways.6 While surgeons and oncologists often focus on the introduction of novel therapeutic interventions, general practitioners tend to conceptualize innovation primarily in terms of operational improvements and service efficiency.6 This suggests that some specialties may be more readily inclined towards emerging treatments. Currently, neurology stands at the forefront of healthcare innovation, with significant progress in areas such as advanced diagnostic and monitoring techniques.7 Innovative technologies, such as fluid Alzheimer’s disease biomarkers and serum neurofilament light chain (sNfL) measurement, offer exciting opportunities for the early diagnosis, prognosis, and monitoring of various neurological disorders, including Alzheimer’s disease and multiple sclerosis (MS).8–10
Providing adequate care for MS requires making complex medical decisions that consider both short- and long-term factors. Despite these challenges, care decisions are traditionally based on clinical and radiological assessments, often lacking the sensitivity to detect underlying disease activity.11 In this context, sNfL measurement has emerged as a promising innovation in MS management.9,10,12,13 sNfL levels serve as a valuable biomarker of active neuroaxonal damage, offering the ability to predict disease activity and progression, and evaluate the efficacy of disease-modifying therapies.12–14 However, despite its clinical potential, the adoption of this innovation varies significantly among neurologists.15
While previous research on healthcare innovation adoption has primarily focused on system-level factors, such as institutional resources, financial incentives, and regulatory frameworks, clinician-specific factors have received comparatively less attention.4 These include cognitive and behavioral characteristics, which are pivotal in determining the uptake of new practices.11,16–19 Identifying these factors can yield critical information for designing strategies to promote evidence-based practice and facilitate the implementation of personalized approaches in neurological care. The aim of this study was to assess how neurologists’ individual characteristics, professional background, and access to novel tools shape their openness to adopting healthcare innovations in MS care.
Methods
We conducted an observational, cross-sectional study in partnership with the Spanish Society of Neurology (SEN) as part of the NewFeeLs-MS initiative.20 This study aimed to explore neurologists’ perspectives on the role of sNfL testing in guiding treatment decisions in MS care. The present analysis focuses on evaluating neurologists’ attitudes toward innovation and identifying the factors associated with their openness to adopting new evidence-based practices.
Neurologists actively involved in the care of patients with MS were invited by the SEN to join the study via Email and completed an electronic survey with standardized questions on their demographic profile, professional background, clinical practice setting, and behavioral characteristics. These included healthcare-related regret, empathy, risk preferences, workplace communication, and occupational burnout. The study was approved by the ethical review board of Hospital Universitario Clínico San Carlos, Madrid, Spain (reference 23/471-E). All participants provided written informed consent.
Outcome Measures
The Openness subscale of the Evidence-Based Practice Attitude Scale (EBPAS) is a validated tool to assess healthcare professionals’ receptiveness to adopting new treatments, practices, or interventions voluntarily, without external mandates.21 It consists of four items, each rated on a five-point Likert scale, ranging from 0 (“not at all”) to 4 (“to a very great extent”). The total score, calculated as the average of item responses, ranges from 0 to 4, with higher scores indicating greater openness to adopting new and innovative practices. Participants were classified as willing to adopt innovations based on the median score.
Empathy with patients was assessed by the Jefferson Scale of Empathy-Health Professionals (JSE-HP).22 It consists of 20 items rated on a seven-point Likert scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). The total score ranges from 20 to 140, with higher scores indicating greater degree of empathy. Low empathy is defined by cutoff scores of ≤95 for males and ≤100 for females. Healthcare-related regret was measured using the Regret Intensity Scale (RIS-10), a 10-item tool that captured the intensity of regret experienced in past patient care situations.23 Each item was scored on a five-point scale from 1 (“not at all”) to 5 (“totally”). The total score ranges from 1 to 5, with higher scores reflecting greater regret intensity. The German Socio-Economic Panel is a validated instrument used to assess willingness to take risks across various life domains, such as financial matters, health, driving, and work.24 Participants were asked: “How would you rate your willingness to take risks at your work?” Responses were recorded on a scale from 0 (“not at all willing”) to 10 (“very willing”). Higher scores indicate a greater propensity to take risks. Open workplace communication was assessed with a single item from the Thriving from Work Questionnaire (TfWQ), which asked participants to rate their agreement with the statement: “I can express my concerns or make suggestions at work without fear of getting into trouble”.25 Response options range from 1 (“never”) to 6 (“always”). Scores of 4 or higher are indicative of a workplace environment where employees feel a strong sense of psychological safety. Occupational burnout at work was assessed using a non-proprietary single-item measure from the Physician Work Life Study.26 This item is scored on a five-point ordinal scale, with response options ranging from 1 (“I enjoy my work. I have no symptoms of burnout”) to 5 (“I feel completely burned out and often wonder if I can go on”). Scores of 3 or higher are indicative of burnout.
Statistical Analysis
Descriptive statistics were calculated for all variables. Continuous variables were summarized using measures of central tendency (mean and median) and variability/dispersion (standard deviation [SD] and interquartile range [IQR]). Categorical variables were described using absolute and relative frequencies (percentages).
Multivariate logistic regression was used to identify predictors of openness, treating the EBPAS-Openness score as a dichotomous variable based on its median split. Additionally, to provide a complementary analysis and a more nuanced understanding of the factors influencing the degree of openness, a linear regression model was performed using the EBPAS-Openness total score as a continuous dependent variable. The explanatory variables included in both models were predefined based on conceptual and clinical relevance, ensuring a balance between empirical and conceptual justification: age, sex, years of professional practice, years managing MS patients, practice setting (academic vs non-academic), full or partial dedication to MS care, number of MS patients seen weekly, access to sNfL testing, participation in MS clinical trials (yes or no), co-authorship of peer-reviewed manuscripts (yes or no), open workplace communication (yes or no), burnout (yes or no), empathy (JSE-HP score), care-related regret (RIS-10 score), and risk attitude at work (yes or no). All variables were included simultaneously in the multivariable models to assess their independent associations. Responses were mandatory, resulting in no missing data. P<0.05 values were considered significant. As this was an exploratory study, no formal power calculation was conducted.
Results
One hundred and sixteen neurologists were studied. The mean age (SD) was 41.9 (10.1) years, and 53.4% were male. Seventy-eight were neurologists fully dedicated to the care of demyelinating disorders (67.2%) and treated a mean of 18.5 (13.6) MS patients per week. Thirty-three (28.4%) participants reported experiencing burnout at work. Table 1 shows participants´ characteristics.
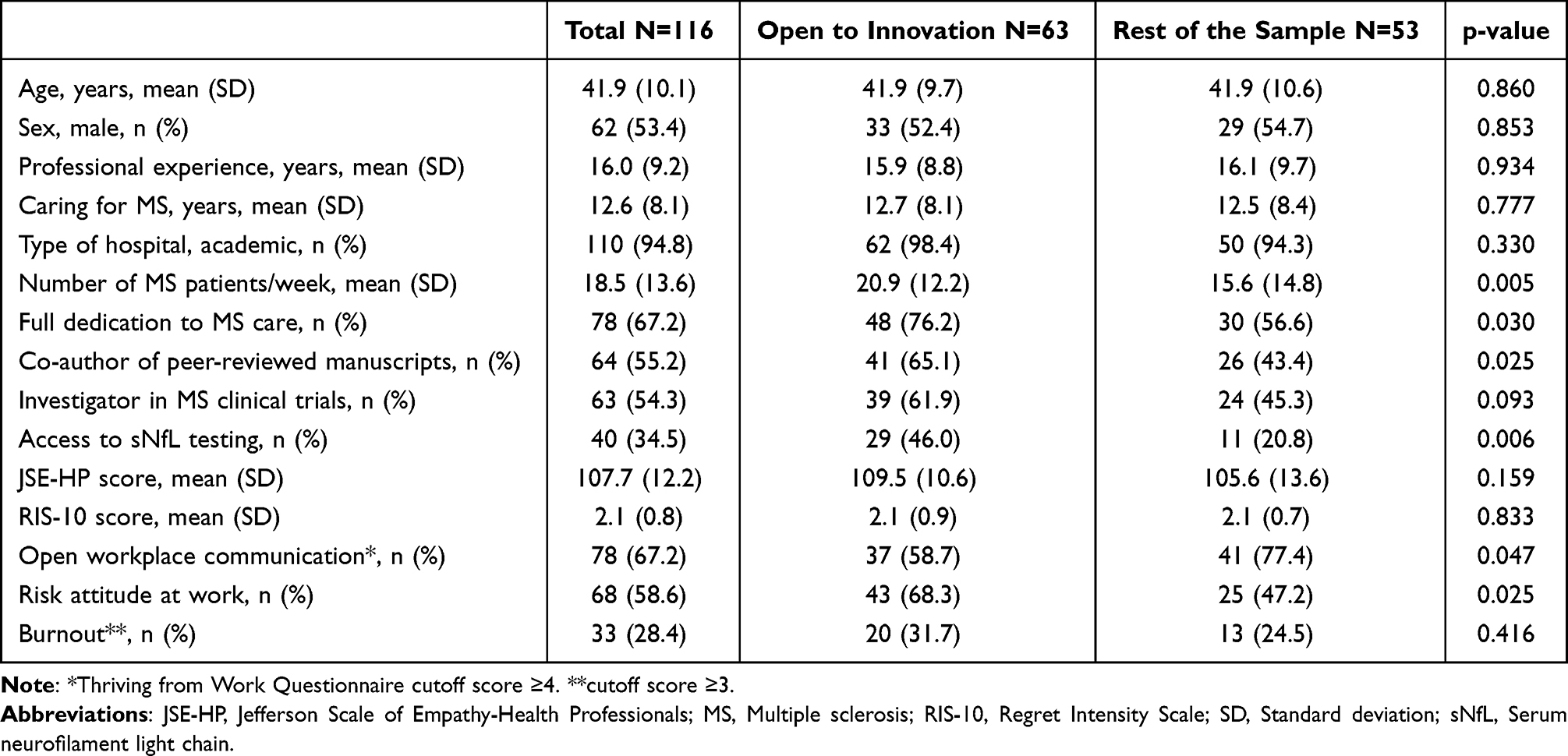 |
Table 1 Demographic, Professional, and Behavioral Characteristics of Participants |
The median EBPAS-Openness score was 3.0 (interquartile range 2.5–3.5), with 54.3% (n=63) of participants demonstrating openness to innovation. Bivariate analyses showed that innovative participants were predominantly fully dedicated to MS management (p=0.030), saw more patients per week (p=0.005), published more frequently (p=0.025), had greater access to sNfL testing (p=0.006), were more inclined to take risks at work (p=0.025), and were less likely to feel they could express concerns at work without fear of trouble (p= 0.047) compared to their counterparts (Table 1).
Multivariate logistic regression analysis identified access to sNfL testing (OR=3.52, CI 95%: 1.3 −10.3, p=0.016) and greater empathy for patients (OR=1.09, CI 95%: 1.0–1.2, p=0.005) as significant predictors of an open attitude toward innovation (Table 2). Further elucidating these relationships, a complementary linear regression model showed that higher EBPAS-Openness scores were also significantly associated with the JSE-HP score (estimate=0.024, p=0.001).
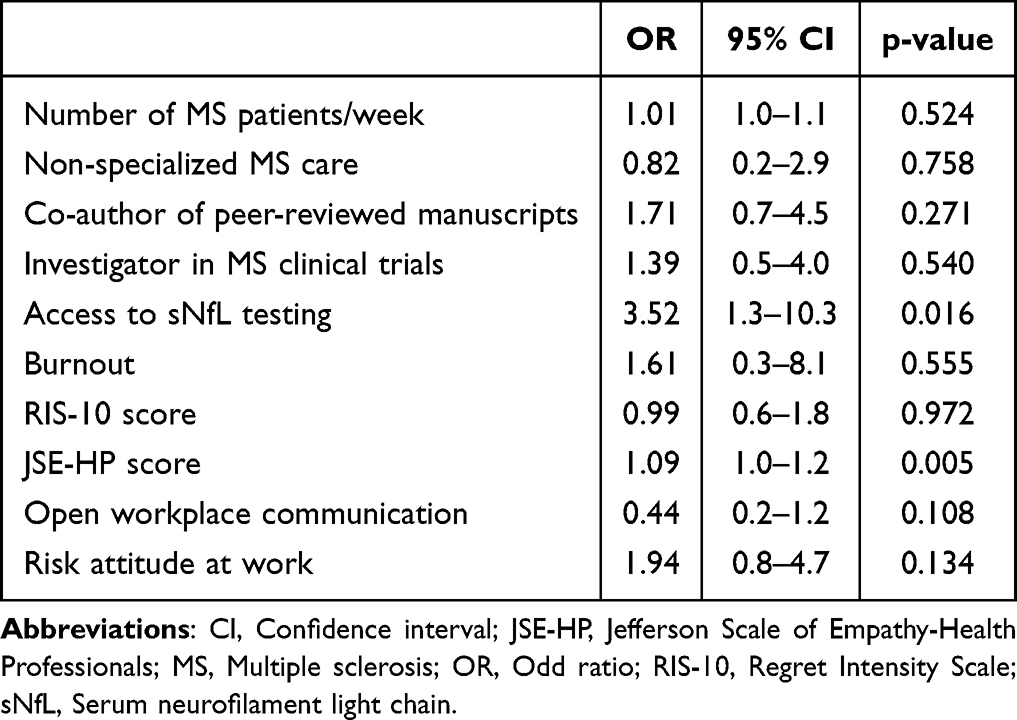 |
Table 2 Multivariate Logistic Regression Analysis |
Discussion
MS represents an ideal setting for studying the adoption of innovation by healthcare professionals. Over the past two decades, neurologists specializing in MS care have witnessed significant advancements, including the development of advanced diagnostic and monitoring techniques and the introduction of highly effective disease-modifying therapies.27,28 Among these innovations, biomarkers such as sNfL and glial fibrillary acidic protein have emerged as reliable, non-invasive tools to better understand disease prognosis and assess treatment responses.12–14 sNfL testing offers the potential to address unmet needs in MS care by providing more sensitive measures of neuroaxonal damage and disease activity, complementing traditional clinical and radiological assessments.13,14 As such, their integration into routine practice marks a pivotal step toward personalized and evidence-based MS management, making MS an exemplary model for exploring the factors that influence the adoption of novel healthcare innovations.14
Our study found that over half of the participating neurologists demonstrated openness to adopting an evidence-based innovation. Access to resources like sNfL testing and higher empathy levels were identified as significant predictors of openness to innovation. These findings highlight the importance of both structural factors, such as the availability of advanced biomarker tools, and personal traits, like the ability to empathize with patients, in shaping neurologists’ attitudes toward adopting new evidence-based practices.
Empathy, the ability of physicians to understand and share the emotions of patients regarding their health conditions, is fundamental to the physician-patient relationship and plays a crucial role in delivering high-quality, patient-centered care.29–31 However, the decline in empathy is an increasingly recognized challenge in modern medical practice.32 Our study found overall high empathy levels, with only 14.5% of males and 18.5% of females scoring below the low-empathy thresholds. This finding aligns with previous research indicating that empathetic clinicians are more attuned to patients’ needs and focused on achieving better outcomes.30,31 Neurologists with a greater capacity to understand and relate to their patients’ experiences may be more inclined to adopt innovations that enhance personalized care and improve patient outcomes.
This study employed both logistic and linear regression models to comprehensively evaluate determinants of neurologists’ openness to innovation. While our initial logistic regression highlighted access to sNfL testing and higher empathy as significant predictors of demonstrating openness, the complementary linear regression, treating openness as a continuous variable, allowed for a more nuanced exploration of these relationships. The linear model strongly reinforced the pivotal role of empathy, demonstrating a significant positive association with the degree of openness to innovation. This consistent finding across both analytical approaches emphasizes empathy’s fundamental importance in fostering an adaptive and patient-centered approach to MS care. In a comparative study conducted in Italy with MS patients, participants evaluated alternative responses to four frequently asked health-related questions, which were formulated by both ChatGPT and neurologists.33 ChatGPT demonstrated significantly higher empathy scores than neurologists. This finding suggests that empathy may serve as a key driver of behavior change, aligning with broader efforts to prioritize patient-centered approaches in healthcare.2,3,29
Other key study findings were the role of access to innovations in fostering openness to new practices. Participant neurologists who reported greater access to sNfL were more likely to exhibit openness to evidence-based practices. A recent study conducted in a neuroimmunology unit in the Netherlands described a substantial influence of sNfL testing on clinical decision-making.18 Neurologists demonstrated moderate to high motivation to access sNfL data, emphasizing the growing interest in incorporating this biomarker into routine patient management. The availability of sNfL results, particularly when elevated levels were identified, influenced clinical decisions, notably in evaluating new symptoms, refining differential diagnoses, and monitoring treatment efficacy. This result underscores the importance of creating enabling environments where clinicians have the opportunity to engage with and experience new technologies. Institutions and healthcare systems should prioritize the provision of access to emerging diagnostic and therapeutic advances as part of continuing professional development initiatives and on-site clinical training.34,35 By ensuring neurologists have hands-on experience with innovations like sNfL testing, healthcare organizations may accelerate the adoption process and facilitate evidence-based decision-making.4,34,35
In our study, neurologists who were more open to adopting innovations demonstrated higher levels of clinical engagement, including full dedication to MS care, higher patient volumes, and more frequent involvement in research publications. These findings are consistent with previous research suggesting that clinicians actively participating in research and specialized care are more likely to embrace evidence-based practices.36
Interestingly, we found that significantly fewer innovator participants felt safe expressing concerns or making suggestions at work compared to non-innovators. This may be because innovators often encounter greater resistance or barriers when presenting unconventional ideas or challenging established norms.37 While innovators are typically willing to take risks as seen in our study and advocate for change, they may perceive the workplace as less supportive when open communication or novel ideas are not fully embraced. In contrast, non-innovators, who are more aligned with established practices, might experience less resistance and, consequently, a greater sense of psychological safety. It is notable that 28.4% of participants reported feeling burned out, although burnout was not found to be significantly associated with openness to innovation in this study. While burnout has been linked to decreased engagement and reduced motivation to change in other healthcare settings, its lack of association here may be related to the specific context of neurological care or the characteristics of the sample.38–40 Future research should explore the potential moderating effects of burnout on openness to innovation, as it remains a critical factor in healthcare workforce well-being and performance.
Despite the promising clinical potential of sNfL testing in MS care, its adoption remains inconsistent, reflecting a broader trend observed in the uptake of healthcare innovations. Barriers such as limited access to testing, uncertainty about its utility in routine practice, and varying levels of institutional support may account for this variability.15,20,41
These findings have important implications for promoting the integration of evidence-based innovations in neurology. Interventions to increase openness to innovation should address structural and individual-level determinants. At the structural level, healthcare institutions should invest in expanding access to advanced diagnostic tools, such as sNfL testing, by integrating them into clinical workflows, developing centralized testing platforms, and securing reimbursement pathways.5,15 At the individual level, fostering neurologist traits associated with openness can be supported through structured professional development programs.42–44 These may include simulation-based training in patient-centered communication, workshops on behavioral flexibility and adaptive decision-making, and mentoring initiatives that pair clinicians with innovation champions or early adopters. Incorporating innovation-related competencies into continuing medical education and leadership development pathways may also accelerate cultural change toward greater receptivity to evidence-based advances in practice.
This study has some limitations. The cross-sectional design does not allow for causal inferences, and the findings are specific to neurologists involved in MS care within Spain, which may limit generalizability to other specialties and regions. Moreover, self-reported measures are subject to potential response bias. Although our analysis identified access to sNfL testing as a significant predictor of openness to innovation, it is important to acknowledge that detailed classification of institutional characteristics beyond the academic versus non-academic setting was not collected. Therefore, access to sNfL may also reflect broader institutional factors such as research infrastructure, availability of specialized resources, or engagement in innovation-focused initiatives. Future research could employ longitudinal designs to assess changes in openness over time and explore how targeted interventions influence this critical attitude.
In conclusion, this study identified key factors that influence neurologists’ openness to evidence-based innovations. Access to innovations and empathy for patients emerge as critical drivers of openness. These findings offer valuable guidance for healthcare institutions, policymakers, and educators seeking to accelerate the implementation of evidence-based advances in neurological care. By addressing these determinants, stakeholders can create supportive environments that facilitate the timely integration of emerging tools and personalized healthcare approaches, ultimately improving patient outcomes.
Abbreviations
EBPAS, Evidence-Based Practice Attitude Scale; JSE-HP, Jefferson Scale of Empathy-Health Professionals; IQR, Interquartile range; MS, Multiple sclerosis; OR, Odds ratio; RIS-10, Regret Intensity Scale; SD, Standard deviation; sNfL, Serum neurofilament light chain; SEN, Spanish Society of Neurology; TfWQ, Thriving from Work Questionnaire.
Data Sharing Statement
The datasets generated during the analysis of the study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Hospital Universitario Clínico San Carlos in Madrid, Spain (protocol code: 23/471-E). All participants provided written informed consent.
Acknowledgments
The authors extend their sincere appreciation to all the neurologists who contributed to the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Roche Farma Spain. The funding source had no role in the design, analysis and interpretation of the data, review or approval of the manuscript, or decision to submit for publication.
Disclosure
JMG-D received honoraria as speaker, advisor and researcher from Almirall, Bristol Myers Squibb, Biogen, Janssen, Merck, Novartis, Roche, Teva, and Sanofi. JEM-L received honoraria as a consultant, chairman and lecturer in meetings and participated in clinical trials and other research projects promoted by Alexion, Biogen, Bristol Myers Squibb, Janssen, Merck, Novartis, Roche, and Sanofi. EM reported receiving research grants, travel support, or honoraria for speaking engagements from Almirall, Merck, Roche, Sanofi, Bristol Myers Squibb, Biogen, Janssen, and Novartis. LL received honoraria for participating in advisory boards and scientific and educational activities from Almirall, Bayer, Biogen, Bristol Myers Squibb, Sanofi, Merck, Novartis, UCB, Roche, and Teva. VM-L received consulting and speaking fees from Almirall, Biogen, Genzyme, Janssen, Merck, Novartis, Roche, Terumo, Sanofi, Teva, and Bristol Myers Squibb. LQ received speaker honoraria from Merck, Sanofi, Roche, Biogen, Grifols and CSL Behring; provided expert testimony for Grifols, Johnson & Johnson, Annexon Pharmaceuticals, Sanofi, Novartis, Takeda, and CSL-Behring; and received research funds from Roche, UCB, and Grifols. EA received speaking honoraria from Roche, Novartis, Merck, Sanofi, and Biogen. SM-Y received honoraria for participating on advisory boards and for collaborations as consultant and scientific communications; they also received research support as well as funding for travel and congress expenses from Amgen, Celgene, Janssen, Kern Pharma, Lilly, Merck, Pfizer, Neuraxpharm, Sandoz, Roche, Biogen Idec, Novartis, TEVA, Merck, Genzyme, Sanofi, Bayer, Almirall, and Bristol Myers Squibb. LMV reported receiving research grants and personal fees from Merck, Roche, Sanofi, Bristol Myers Squibb, Biogen, and Novartis. ABC received courses and honoraria for her participation as speaker/meeting moderator/symposia organizer from Alter, Almirall, Bayer, Bial, Biogen, Bristol Myers Squibb, Lilly, Merck, Mylan, Novartis, Roche, Sanofi-Genzyme, Teva, and UCB; and support to attend scientific meetings from Biogen, Bial, Merck-Serono, Novartis, Roche, Sanofi, and Teva. RG-B, EG-A, NM, and JM are employees of Roche Farma Spain. The authors report no other conflicts of interest in this work.
References
1. International Consortium for Personalised Medicine and Working Group ‘Personalised Medicine in Healthcare’ (WG2); Cinti C, Trivella MG, Joulie M, et al. The roadmap toward personalized medicine: challenges and opportunities. J Pers Med. 2024;14(6):546. doi:10.3390/jpm14060546
2. Santesson AHE, Holmberg R, Bäckströ M, et al. Clinician attitudes towards adoption of evidence-based practice: a nationwide multiprofessional cross-sectional study of child and adolescent mental health services in Sweden. BMC Health Serv Res. 2024;24(1):1432. doi:10.1186/s12913-024-11934-9
3. Safi S, Thiessen T, Schmailzl KJ. Acceptance and resistance of new digital technologies in medicine: qualitative study. JMIR Res Protoc. 2018;7(12):e11072. doi:10.2196/11072
4. Stefanicka-Wojtas D, Kurpas D. Barriers and facilitators to the implementation of personalised medicine across Europe. J Pers Med. 2023;13(2):203. doi:10.3390/jpm13020203
5. Drejeris R, Drejeriene E. Novel approach to the actions for causes elimination of staff resistance to innovative change. J Multidiscip Healthc. 2022;15:1011–1022. doi:10.2147/JMDH.S354329
6. Elliott T, Miola J, Samanta A, et al. Fears and fallacies: doctors’ perceptions of the barriers to medical innovation. Clin Ethics. 2019;14(4):155–164. doi:10.1177/1477750919886090
7. Hampel H, Gao P, Cummings J, et al. The foundation and architecture of precision medicine in neurology and psychiatry. Trends Neurosci. 2023;46(3):176–198. doi:10.1016/j.tins.2022.12.004
8. VandeVrede L, Schindler SE. Clinical use of biomarkers in the era of Alzheimer’s disease treatments. Alzheimers Dement. 2024. doi:10.1002/alz.14201
9. Khalil M, Teunissen CE, Lehmann S, et al. Neurofilaments as biomarkers in neurological disorders - towards clinical application. Nat Rev Neurol. 2024;20(5):269–287. doi:10.1038/s41582-024-00955-x
10. Cai L, Huang J. Neurofilament light chain as a biological marker for multiple sclerosis: a meta-analysis study. Neuropsychiatr Dis Treat. 2018;14:2241–2254. doi:10.2147/NDT.S173280
11. Saposnik G, Montalban X. Therapeutic inertia in the new landscape of multiple sclerosis care. Front Neurol. 2018;9:174. doi:10.3389/fneur.2018.00174
12. Di Filippo M, Gaetani L, Centonze D, et al. Fluid biomarkers in multiple sclerosis: from current to future applications. Lancet Reg Health Eur. 2024;44:101009. doi:10.1016/j.lanepe.2024.101009
13. Monreal E, Ruiz PD, San Román IL, et al. Value contribution of blood-based neurofilament light chain as a biomarker in multiple sclerosis using multi-criteria decision analysis. Front Public Health. 2024;12:1397845. doi:10.3389/fpubh.2024.1397845
14. Freedman MS, Abdelhak A, Bhutani MK, et al. The role of serum neurofilament light (sNfL) as a biomarker in multiple sclerosis: insights from a systematic review. J Neurol. 2025;272(6):400. doi:10.1007/s00415-025-13093-1
15. Moccia M, Terracciano D, Brescia Morra V, et al. Neurofilament in clinical practice: is the multiple sclerosis community ready? Mult Scler. 2024;30(6):643–645. doi:10.1177/13524585241246536
16. Sedney C, Kurowski-Burt A, Smith M, et al. Therapeutic nihilism of neurological diseases: a comparative qualitative study. J Clin Neurosci. 2019;69:124–131. doi:10.1016/j.jocn.2019.08.013
17. Fortea J, García-Arcelay E, Terrancle Á, et al. Attitudes of neurologists toward the use of biomarkers in the diagnosis of early Alzheimer’s disease. J Alzheimers Dis. 2023;93(1):275–282. doi:10.3233/JAD-221160
18. van Lierop ZY, Wessels MH, Lekranty WM, et al. Impact of serum neurofilament light on clinical decisions in a tertiary multiple sclerosis clinic. Mult Scler. 2024;30(13):1620–1629. doi:10.1177/13524585241277044
19. Téllez-Lara N, Gómez-Ballesteros R, Sepúlveda M, et al. Preferences for neuromyelitis optica spectrum disorder treatments: a conjoint analysis with neurologists in Spain. Mult Scler Relat Disord. 2024;88:105732. doi:10.1016/j.msard.2024.105732
20. Saposnik G, Monreal E, Medrano N, et al. Does serum neurofilament light chain measurement influence therapeutic decisions in multiple sclerosis? Mult Scler Relat Disord. 2024;90:105838. doi:10.1016/j.msard.2024.105838
21. Melas CD, Zampetakis LA, Dimopoulou A, et al. Evaluating the properties of the Evidence-Based Practice Attitude Scale (EBPAS) in health care. Psychol Assess. 2012;24(4):867–876. doi:10.1037/a0027445
22. Hojat M, DeSantis J, Shannon SC, et al. The Jefferson scale of empathy: a nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Adv Health Sci Educ Theory Pract. 2018;23(5):899–920. doi:10.1007/s10459-018-9839-9
23. Saposnik G, Bueno-Gil G, Sempere ÁP, et al. Regret and therapeutic decisions in multiple sclerosis care: literature review and research protocol. Front Neurol. 2021;12:675520. doi:10.3389/fneur.2021.675520
24. Dohmen T, Falk A, Huffman D, et al. Individual risk attitudes: measurement, determinants, and behavioral consequences. J Eur Econ Assoc. 2011;9:522–550. doi:10.1111/j.1542-4774.2011.01015.x
25. Peters SE, Gundersen DA, Katz JN, et al. Thriving from work questionnaire: dimensionality, reliability, and validity of the long and short form questionnaires. Am J Ind Med. 2023;66(4):281–296. doi:10.1002/ajim.23465
26. Dolan ED, Mohr D, Lempa M, et al. Using a single item to measure burnout in primary care staff: a psychometric evaluation. J Gen Intern Med. 2015;30(5):582–587. doi:10.1007/s11606-014-3112-6
27. Oreja-Guevara C, Martínez-Yélamos S, Eichau S, et al. Beyond lines of treatment: embracing early high-efficacy disease-modifying treatments for multiple sclerosis management. Ther Adv Neurol Disord. 2024;17:17562864241284372. doi:10.1177/17562864241284372
28. Rocca MA, Preziosa P, Barkhof F, et al. Current and future role of MRI in the diagnosis and prognosis of multiple sclerosis. Lancet Reg Health Eur. 2024;44:100978. doi:10.1016/j.lanepe.2024.100978
29. Decety J. Empathy in medicine: what it is, and how much we really need it. Am J Med. 2020;133(5):561–566. doi:10.1016/j.amjmed.2019.12.012
30. Howick J, Moscrop A, Mebius A, et al. Effects of empathic and positive communication in healthcare consultations: a systematic review and meta-analysis. J R Soc Med. 2018;111(7):240–252. doi:10.1177/0141076818769477
31. Moya-Salazar J, Goicochea-Palomino EA, Porras-Guillermo J, et al. Assessing empathy in healthcare services: a systematic review of South American healthcare workers’ and patients’ perceptions. Front Psychiatry. 2023;14:1249620. doi:10.3389/fpsyt.2023.1249620
32. Mangione S. The empathy gap. Am J Med. 2024;137(3):290–291. doi:10.1016/j.amjmed.2023.12.008
33. Digital Technologies, Web, Social Media Study Group of the Italian Society of Neurology (SIN); Maida E, Moccia M, Palladino R, et al. ChatGPT vs. neurologists: a cross-sectional study investigating preference, satisfaction ratings and perceived empathy in responses among people living with multiple sclerosis. J Neurol. 2024;271(7):4057–4066. doi:10.1007/s00415-024-12328-x
34. Sapci AH, Sapci HA. The effectiveness of hands-on health informatics skills exercises in the multidisciplinary smart home healthcare and health informatics training laboratories. Appl Clin Inform. 2017;8(4):1184–1196. doi:10.4338/ACI-2017-08-RA-0136
35. Altmiller G, Pepe LH. Influence of technology in supporting quality and safety in nursing education. Nurs Clin North Am. 2022;57(4):551–562. doi:10.1016/j.cnur.2022.06.005
36. Saposnik G, Maurino J, Sempere AP, Terzaghi MA, Amato MP, Montalban X. Does attendance at the ECTRIMS congress impact on therapeutic decisions in multiple sclerosis care? Mult Scler J Exp Transl Clin. 2019;5(1):2055217319835226. doi:10.1177/2055217319835226
37. Daly JA, Sætre AS. The consequences of face-threatening feedback on innovators’ psychological safety, affect, and willingness to engage in future innovation projects. Front Psychol. 2023;14:1060617. doi:10.3389/fpsyg.2023.1060617
38. Weiss EM, Canazei M, Perchtold-Stefan CM, et al. Different facets of creativity in employees covering non-clinical to clinical manifestations of burnout. J Intell. 2022;10(4):105. doi:10.3390/jintelligence10040105
39. Budd J. Burnout related to electronic health record use in primary care. J Prim Care Commun Health. 2023;14:21501319231166921. doi:10.1177/21501319231166921
40. Guo J, Gokcebel S, Grewal P, et al. Burnout in practicing neurologists: a systematic review and meta-analysis. Neurol Clin Pract. 2025;15(1):e200422. doi:10.1212/CPJ.0000000000200422
41. Lycke J, Fox RJ. Using serum neurofilament-light in clinical practice: growing enthusiasm that may need bridling. Mult Scler. 2024;30(13):1575–1577. doi:10.1177/13524585241291452
42. Sulena S, Kapoor A, Kulkarni A, et al. Curriculum innovation: integrating case-based learning with seminar and journal club to enhance critical thinking skills in residency program. Neurol Educ. 2025;4(2):e200213. doi:10.1212/NE9.0000000000200213
43. Edwards Roger A, White Bobbie AA, Findyartini A. Editorial: innovations in teaching and learning for health professions educators. Front Med. 2025;12:1611578. doi:10.3389/fmed.2025.1611578
44. Yang F, Lei F, Li Y, et al. Qualitative insights into empathy in medical education: perspectives from students, doctors, and educators. BMC Med Educ. 2025;25(1):473. doi:10.1186/s12909-025-06882-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Shared Decision-Making in the Treatment of Multiple Sclerosis: Results of a Cross-Sectional, Real-World Survey in Europe and the United States
Keenan A, Le HH, Gandhi K, Adedokun L, Jones E, Unsworth M, Pike J, Trenholm E
Patient Preference and Adherence 2024, 18:137-149
Published Date: 16 January 2024