Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Neurofibromatosis Type 1 (NF1): Addressing the Transition from Pediatric to Adult Care
Authors Radtke HB ![]() , Berger A, Skelton T, Goetsch Weisman A
, Berger A, Skelton T, Goetsch Weisman A
Received 4 October 2022
Accepted for publication 19 January 2023
Published 9 February 2023 Volume 2023:14 Pages 19—32
DOI https://doi.org/10.2147/PHMT.S362679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Heather B Radtke,1,2,* Angela Berger,3 Tammi Skelton,4 Allison Goetsch Weisman3,5,*
1Medical College of Wisconsin, Milwaukee, WI, USA; 2Children’s Tumor Foundation, New York, NY, USA; 3Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, USA; 4UAB Heersink School of Medicine, Birmingham, AL, USA; 5Northwestern University, Chicago, IL, USA
*These authors contributed equally to this work
Correspondence: Heather B Radtke, Email [email protected]
Abstract: Health care transition, or HCT, is the process of adolescents and young adults moving from a child/family-centered model of health care to an adult/patient-centered model of health care. Healthcare providers have an essential role in this process which can be especially challenging for individuals with medical or special healthcare needs. Neurofibromatosis type 1 (NF1) is a complex multisystem disorder requiring lifelong medical surveillance, education, and psychosocial support. This review highlights the transition needs of NF1 patients and provides resources for both clinicians and families to facilitate HCT in this population. The authors propose a framework for the development of an effective NF1 transition program by using the Six Core Elements model of the Got Transition program, reviewing existing literature, and incorporating author experiences in the care and transition of NF1 patients.
Keywords: adolescents, young adults, neurofibromatosis, transition, healthcare
Introduction
Healthcare Transition
Healthcare transition (HCT) is defined as the purposeful, planned movement of adolescents and young adults (AYA) from child-centered care to an adult-oriented care system.1
This process often, but not always, involves a physical transition to a new healthcare system and/or medical provider(s) and may be complicated by the differences between pediatric and adult healthcare models of care (Table 1). Successful HCT strategies are designed to build healthcare independence2 and can be characterized by individual and health-related outcomes, such as improved quality of life, decreased hospitalization, and decreased disease morbidity.3,4 It is widely accepted that HCT for AYA with special healthcare needs, including those with genetic conditions, is more complex than generally healthy peers.1 AYA with special healthcare needs encounter a variety of challenges, some due to the normal developmental stage that they are in and some from the stresses of their chronic medical conditions on the transition to adult healthcare and life.
 |
Table 1 Comparison of Pediatric and Adult Health Care Models |
Research has shown that the HCT process among AYA with special healthcare needs has been disorganized and at times results in a lack of appropriate insurance coverage and decreased access to adequate healthcare.6–11 Further, underdeveloped health-related self-management skills have been observed in association with a decline in health, as well as poorer outcomes compared to the general population regarding education, employment, and socioeconomic status.11 Improvements in HCT for AYA with special healthcare needs are needed to eliminate gaps in medical care and improve health outcomes, as well as general quality of life.12–15
Similar to other conditions with special healthcare needs, effective HCT in neurofibromatosis type 1 (NF1) is often deficient because of poor access to care and limited disease knowledge, and may be further complicated by psychiatric diagnoses, cognitive impairment, and executive function deficits.16,17 This review focuses on the important aspects of HCT in NF1 and provides information about resources available to clinicians and families to promote successful HCT.
Neurofibromatosis Type 1 and Healthcare Transition
Neurofibromatosis Type 1
Neurofibromatosis type 1 (NF1) is a relatively common genetic condition that affects approximately 1 in 2500–3000 people.18,19 NF1 is caused by a heterozygous pathogenic variant in the NF1 gene (NF1). NF1 is highly variable within and between families and has complete penetrance. It is characterized by the presence of multiple café-au-lait macules (CALM), intertriginous freckling, cutaneous and subcutaneous neurofibromas, plexiform neurofibromas, bone abnormalities, Lisch nodules, and optic pathway gliomas. Additional complications may include malignancies, other central nervous system neoplasms, chronic pain, vasculopathy, hypertension, delayed or early puberty, learning disabilities, attention deficit with or without hyperactivity, and psychological disorders. Psychological concerns include impaired socialization, low self-esteem, poor interpretation of social cues, anxiety, and depression.20 Complications of NF1 may cause serious disease morbidity, and in some cases, mortality. While pediatric and adult medical care guidelines and a genetic counseling practice resource exist for the care of individuals with NF1,21–23 limited information has been published to date about the deficiencies, needs, and strategies specific to provide HCT for AYA with NF1.
Healthcare Transition Readiness and Perceptions of Adolescents and Young Adults with NF1
Few studies have addressed transition preparation and perspectives in the NF1 population. A quantitative HCT study utilizing the validated Transition Readiness Assessment Questionnaire (TRAQ) in the NF1 population was published by Goetsch Weisman et al.24 Transition readiness was found to be significantly lower for AYA with NF1 than in healthy peers, consistent with the HCT literature assessing transition readiness for AYA with special healthcare needs. In addition, the authors used the TRAQ as a model to develop an NF1-specific readiness questionnaire (NF1-TRAQ) and demonstrated a high correlation between TRAQ scores and NF1-TRAQ scores, indicating that increased transition readiness correlated with greater self-reported knowledge of NF1 and associated NF1 specific HCT skills. Overall, participants reported adequate knowledge of NF1 and comfort talking to medical providers, but discomfort with appointment keeping, insurance-related tasks, addressing NF1 medical emergencies, and discussing their diagnosis with other (non-NF1) medical providers and peers. The study also found that both TRAQ and NF1-TRAQ scores were lower in individuals who reported that their NF1 diagnosis had an impact on their education, career, and relationships, suggesting that decreased transition readiness is associated with a negative impact on young adult life. The results of this study emphasize the crucial need for education and mentoring throughout adolescence.
A qualitative study by Davidson25 evaluated parent perspectives of adolescents with NF1. Consistent with HCT research for AYA with special healthcare needs, parents of adolescents with NF1 had considerable concern about adolescent ability to take responsibility for medical needs and independently manage their healthcare. Importantly, the study found a positive correlation between parent perspectives of a young adult’s knowledge of NF1, involvement with healthcare management, and independence with self-management tasks. Similarly, Rietman et al26 completed a qualitative assessment of the worries and needs of young adults and parents of young adults with NF1. Findings indicated that young adults with NF1 desire more information about their diagnosis and medical needs, access to and improved communication with NF1 expert clinicians, daily living support, mental health services, and socioeconomic participation. Parents also stressed the concern that they often remain in a coordination role for their adult child due to their child’s lack of understanding and health-related self-management skills. Parents reported significant stress and concerns about the time they spend assisting their child with factors of young adult life, including medical management. Results of these studies emphasize the importance of parent participation in a patient’s HCT, and that this partnership may include working together to make medical and life decisions.
The importance of continued follow-up and education after the transition period was emphasized in a study by Oates et al16 in Australia, which revealed that many young adults with NF1 have poor access to healthcare, limited disease knowledge, and high NF1 complication rates. The authors found that for many young adults, the lack of ongoing healthcare and complication surveillance might explain the large number of new medical complications they identified, and suggests that lack of knowledge of associated risks and complications, cognitive deficits, and no identified NF1 care provider likely contributes to poor health surveillance and management.
Quality of Life and Mental Health Issues in Adolescents and Young Adults with NF1
It is well established that NF1 can have a profound effect on quality of life (QoL) across all domains, including general physical health, bodily pain, mental health, activities of daily living, independence, and social functioning and relationships.27–33 An important goal of HCT is to manage factors that may decrease QoL by increasing knowledge and building independence, as well as ensuring AYA have appropriate support in all facets of their lives.
Medical worries expressed by young adults with NF1 often relate to the unpredictable nature of the disease.26,34 This includes fear of potential loss of function, future surgeries, aesthetic problems, malignancy risk, pain, and the visibility of their disease (Table 2).26 Studies have consistently shown that visibility of disease is a major predictor of poor QoL and poor mental health among adults with NF1.27,30,35–37
 |
Table 2 Potential Health Risks in Adults with Neurofibromatosis Type 1 |
Children and adolescents with NF1 experience more psychosocial problems and mental health issues compared to their healthy peers, such as anxiety, depression, inattention and impulsivity, internalization and externalization of problems, difficulties socializing, and poor adaptive behavior.38,39 Similarly, adults with NF1 have high levels of depression, anxiety, and stress.30,33,34,40,41 It has been theorized that adults with NF1 may experience these mental health concerns due to social withdrawal and isolation,36 as well as a lack of coping skills necessary to avoid sustained heightened emotional distress.33 Psychosocial interventions to address distress have been designed for individuals with NF1, and preliminary results show improvements in both QoL and pain interference.42–44
NF1 can significantly impact social roles and relationships. Rietman et al26 surveyed young adults with NF1 and found that participants commonly reported loneliness and trouble initiating and maintaining social and romantic relationships. Adults with NF1, particularly women, report greater insecurity and lower self-esteem and body image than their peers.26,45 Kodra et al28 found that approximately 40% of participants with NF1 in their study reported feeling embarrassed about their skin and Smith et al46 found that 67% of women with NF1 in their study expressed an NF1-related appearance concern. Additionally, women with NF1 often report feeling less attractive and confident, more self-conscious about their bodies, and more dissatisfied sexually secondary to these feelings.45–47 These concerns should be considered by healthcare providers when caring for adolescents and adults with NF1. The University of Alabama created a resource for providers and patients regarding intimacy in NF148 which may be useful for AYA as they struggle through these insecurities.
Achieving independence with regard to education, employment, and social interactions can be a significant challenge for some young adults with NF1, particularly those with learning disabilities and/or cognitive dysfunction.26,27,36,49–51 The AYA’s perceptions about themselves, their familial and community support, and their access to mental health services may contribute to these challenges. In a review of data from the National Longitudinal Study of Adolescent Health, individuals with chronic illness were more likely to be unemployed, receive public benefits, and have a generally lower income than their peers without chronic illness.52 This was similarly seen by Gregory et al51 in an assessment of adults with NF1 in the Pacific Northwest region of the United States, in which participants were less likely than age-matched healthy peers to have private insurance, be employed, and have children. Thus, individuals with NF1 may require more support at school and in the workplace. Connecting AYA with NF1 to assistance programs, including disability service offices and vocational rehabilitation, can allow individuals to receive appropriate accommodations in educational and work environments. This may potentially increase labor force participation and decrease barriers to successful employment.50
NF1 is an autosomal dominant condition with a 50% risk of transition to offspring which can significantly impact family planning decisions. While most individuals with NF1 report being interested in having biological children without NF1, young adults generally want more information and education about genetics and reproduction, including alternative family planning options.24,26 A practice resource by the National Society of Genetic Counselors provides guidance to clinicians regarding family planning discussions, as well as general psychosocial topics that may affect QoL in individuals with NF1.23
Although there are few studies linking the two, the potential negative impact of NF1 on QoL and mental health among AYA highlights the importance of a structured HCT program, with multidisciplinary expert care before, during, and after the formal HCT.26 HCT strategies can be designed to address these concerns, including facilitation of the development of health and non-health related self-management skills, psychosocial support and referrals, connection with resources to obtain accommodations at school and work, and access to genetic counseling for family planning.
Components of a Healthcare Transition Program and Associated Challenges
Healthcare Transition Models
Best practices for transition have been established, and several HCT models exist.53–55 Regardless of the model utilized to implement a formal HCT program, a structured transition intervention results in more positive outcomes.56,57
The most widely used model is available through Got Transition (GT),5 a federally funded resource center with an aim to improve the transition from pediatric to adult healthcare. GT provides several tools and resources for providers, patients, and families. The Six Core Elements of Transition58 were created for clinicians to guide transition programs and interventions. These Core Elements align with approaches used by numerous professional organizations including the American Academy of Pediatrics (AAP), with the endorsement of the American Academy of Family Physicians (AAFP) and the American College of Physicians (ACP).55
Often, healthcare providers consider transition as a discrete event, such as the actual transfer of care. The concept of the Six Core Elements presents transition as a process, starting in early adolescence and continuing into young adulthood. There are three separate guides provided by GT that are specific to the type of practice facilitating the transition, including whether the AYA changes clinicians, continues to follow with the same provider but transitions to an adult model of care, or integrates into adult health care. The elements of transition highlighted below focus on transitioning AYA to a new adult healthcare provider and provides a framework to apply these strategies to NF1 patients.
The first Core Element of Got Transition’s Six Core Elements is Transition and Care Policy/Guide. If a transition guide is not already established, the policy ideally should be crafted with input from patients and families, and be written at an appropriate literacy level. Policies often provide patients and families with helpful anticipatory guidance and indicate how the practitioner will support the patient and their family during the transition process. A transition policy often includes age ranges that can allow an early introduction of the concept of transition to patients and their families, ideally around 12–14 years of age. Once developed, the transition policy can be communicated to families in different ways such as: during a clinic visit, a mailing, or posted on a program’s website. The policy can be reviewed yearly with patients and families. The policy should also be clearly communicated to program staff. Several examples of transition guides are available on the GT website and can be easily modified for NF1 and the specific clinic setting.
The second Core Element is Tracking and Monitoring. This involves defining criteria to identify youth requiring HCT assistance and tracking the receipt of the HCT program. This is also applicable to AYA with NF1 with tracking and receipt of a structured HCT program to support the best outcomes and patient/family support and communication. It is not unusual to have multiple specialties involved in caring for NF1 patients. A shared HCT tracking system allows each clinician to monitor the patient as they progress through transition. Electronic Medical Record (EMR) systems often have customizable ways to track and monitor patient history, and can be applied to HCT. Other databases can also be helpful in tracking and monitoring transition progress.
The third Core Element is Transition Readiness. This can be evaluated by regular assessments using the validated TRAQ or other readiness measures such as the NF1-TRAQ, which is specific to NF1 transition readiness.11,24 The tools should be used at regular intervals to monitor transition readiness over time,2 as the information can guide the clinician’s approach to the education, anticipatory guidance, and counseling of AYA with NF1. This is an important component of the HCT process leading to positive perceptions of readiness and future success.9,59 Lemke et al60 found that AYA with chronic illnesses who received care coordination support through an HCT program were more than two times as likely to report receiving the care they thought they needed and to speak to their providers about future care than those who did not receive care coordination support.
The fourth Core Element is Transition Planning. This includes readying the patient and family for the eventual shift to adult models of care, including education about the differences in the culture between pediatric care and adult care, timing of the transfer of care, identification of adult providers, and discussion of a patient’s goals and priorities. During this planning stage, clinicians should develop a medical history summary and emergency care plan for the patient. Additionally, healthcare providers might provide a release of medical information, legal documents for guardianship if applicable, and insurance options and resources. Individuals with NF1 should be well informed of these important aspects of transition planning.
The fifth Core Element is Transfer of Care to an adult counterpart. Introducing the concept of HCT early prepares patients and families for their eventual transition to an adult provider or model of health care. It is important to develop relationships with adult providers and be willing to serve as a continued resource should an adult colleague need consultation. A “warm handoff” between providers either by phone, electronic message, or joint telehealth visit, are all ways to facilitate this transfer. Assistance locating an NF provider is available on NF organization websites,61,62 however, there may not be an identified clinic in the area that provides comprehensive care for adults with NF1. In this case, it is advisable for the pediatric provider to identify and educate a local provider or subspecialist, such as a neurologist or neuro-oncologist, to ensure appropriate care for adults with NF1. This often includes forwarding existing NF1 resources, guidelines and practice resources.22,23
The sixth and final Core Element is Transfer Completion. This involves communication with both the patient/caregiver and adult providers, as well as between the pediatric and adult providers, to be sure the transfer has been successfully executed. Although this step can be time intensive, it is especially important for NF1 patients who may not feel comfortable with navigating a new healthcare model and either request to return to the pediatric clinic, or are lost to follow-up and therefore not receiving the comprehensive medical care and support needed.
In addition to NF1-specific HCT, the transition program needs to consider and address other life transitions common in the AYA period, including the transition to higher education and career, social and romantic relationships, and family planning. Transition readiness and anticipatory guidance are critical to consider as individuals are guided to prepare to take care of themselves and live independently.
There are several additional considerations of the transition process including recognition of barriers to successful HCT, identification of high-risk individuals, patient and provider education of HCT and NF1, and billing and reimbursement for transition services.
Barriers to Successful NF1 Healthcare Transition
Many of the challenges of an effective NF1 HCT are the same as barriers in the general transition process. In order to start and maintain a successful HCT program, identification and acknowledgment of potential barriers are necessary. Several barriers to effective HCT have been identified (Table 3) and include limited or lack of insurance coverage, income/financial concerns, lack of service coordination, lack of support from ancillary staff (eg nursing, social work, and case management), healthcare culture differences, work involved in transferring and accessing medical records, difficulty obtaining reimbursement for extended clinic appointments, lack of provider knowledge and comfort caring for individuals with special healthcare needs, poor communication between the healthcare provider and family, lack of communication and anticipatory guidance about the HCT process, and family stress and comfort with medical complexities.2,3,26,63,64
 |
Table 3 Barriers to Effective Healthcare Transition |
Notably, Gray et al65 found that a prominent barrier to HCT reported by patients and families is relationships. Patients are often reluctant to leave their pediatric care team and have difficulty accessing knowledgeable adult providers whom they trust with their concerns. Further, HCT requires committed parental involvement. In a review of parent experiences with HCT, Ellison et al66 found that barriers to parental facilitation of HCT include concerns surrounding relationship loss, loss of parental role, lack of knowledge and/or skills, and concerns related to the healthcare system in general. Similarly, Rietman et al26 found that parents of young adults with NF1 reported significant stress regarding their now adult child’s medical care. Participants reported that providers do not acknowledge the worries of parents, expressed confusion about their parental role, and felt a decrease in the quality of their parent-child relationship.
Of additional importance, for individuals with NF1 and an intellectual disability, there may be limitations in autonomy and self-management. This typically requires an assessment of decision-making abilities to determine the capacity for self-advocacy.67 In these situations, parents or guardians play a significant role in the transition process and may continue as the primary caregiver.
Identification of High-Risk Patients
Individuals at increased risk to have challenges with the HCT process may need additional support and services before, during, and after the transition to adult healthcare. The National Survey of Children’s Health data details that AYA with special healthcare needs are more likely to live in poverty, be non-Hispanic Black, and have public insurance than their generally healthy peers.68,69 And, while it has generally been shown that AYA with special healthcare needs are not receiving HCT counseling at high rates, it is worse for minority patients, with reports of Hispanic children, younger teens, and non-Hispanic Black children being counseled at lower rates.70 In addition to receiving less counseling, there are significant disparities with regard to race, age, and disability and the availability of transition services.71 Although providers may self-report no bias against people with disabilities, an overwhelming majority had implicit biases in a study by VanPuymbrouck et al.72 Low health literacy has also been linked to increased emergency department (ED) utilization and lower levels of transition readiness on the TRAQ.73 Especially concerning for individuals with NF1, patients who receive care based solely during ED visits typically do not receive the comprehensive and knowledgeable care that an experienced clinician in a typical healthcare setting can provide. This can lead to medical mismanagement, lack of a consistent medical plan with poor adherence to health maintenance screenings, deficiencies in patient education and counseling, and higher healthcare costs. HCT for those with low health literacy and NF1 may be further complicated by associated diagnoses of associated psychiatric diagnoses, cognitive impairment, and executive function deficits.16,17,38,39 Autism spectrum disorder in particular has been found to be associated with the lowest levels of transition readiness compared to other chronic conditions,74 an important consideration given the increased incidence of autism among individuals with NF1.
Lausdahl et al17 from Denmark surveyed individuals with NF1 and found that those who self-reported the most difficulty with the HCT process had psychiatric diagnoses, executive function deficits, and/or special educational needs, emphasizing the importance of multidisciplinary collaboration and support to facilitate the effective transition for these individuals. Specialists involved in the HCT process for AYA with NF1 may need to include medical providers, neuropsychologists, mental health providers, social workers, therapists, and education liaisons.
Access to medical insurance that will ensure continued care is yet another challenge that AYA with special healthcare needs experience. Medicaid expansion and the Affordable Care Act have greatly benefitted youth with disabilities,75,76 including those with NF1, however, concerns remain that there may be delayed care or forgoing of care completely because of changes in the usual provision of healthcare leading to poor health outcomes into adulthood.77 Disabled youth with chronic medical conditions were also shown to be at increased risk of losing health insurance, both public and private, than their non-disabled peers.78 Thus, as part of the HCT program, providers should identify those NF1 patients who may be at greater risk to have challenges with the HCT process, including lack of appropriate insurance coverage, and need for additional support and guidance.
NF1 Patient Education
Healthcare transition programs should address the changing medical needs through adulthood and provide applicable resources to the family. In a study assessing worries and needs of adults and parents of adults with NF1, Rietman et al26 found a common false expectation among participants that care needs decrease in adulthood. However, NF1 is a progressive condition with significant risk for disease morbidity in adulthood (Table 2). Education about adult health risks and the importance of medical care management and screenings is a vital component of an NF1 HCT plan, with particular attention to cancer risk and surveillance, cardiovascular complications, bone health, pain management, neurologic complications, neurocognitive functioning, mental health, and reproductive risks and options.22,23,79,80 Table 4 and Table 5 provide several patient resources about the HCT process and information about NF1 for providers to share with their patients for ongoing education and support. Additional priorities of patient education should address medication management, appointment keeping, tracking health issues, identifying medical emergencies, understanding the insurance system, and talking with providers; all of which can be assessed using the validated TRAQ.11
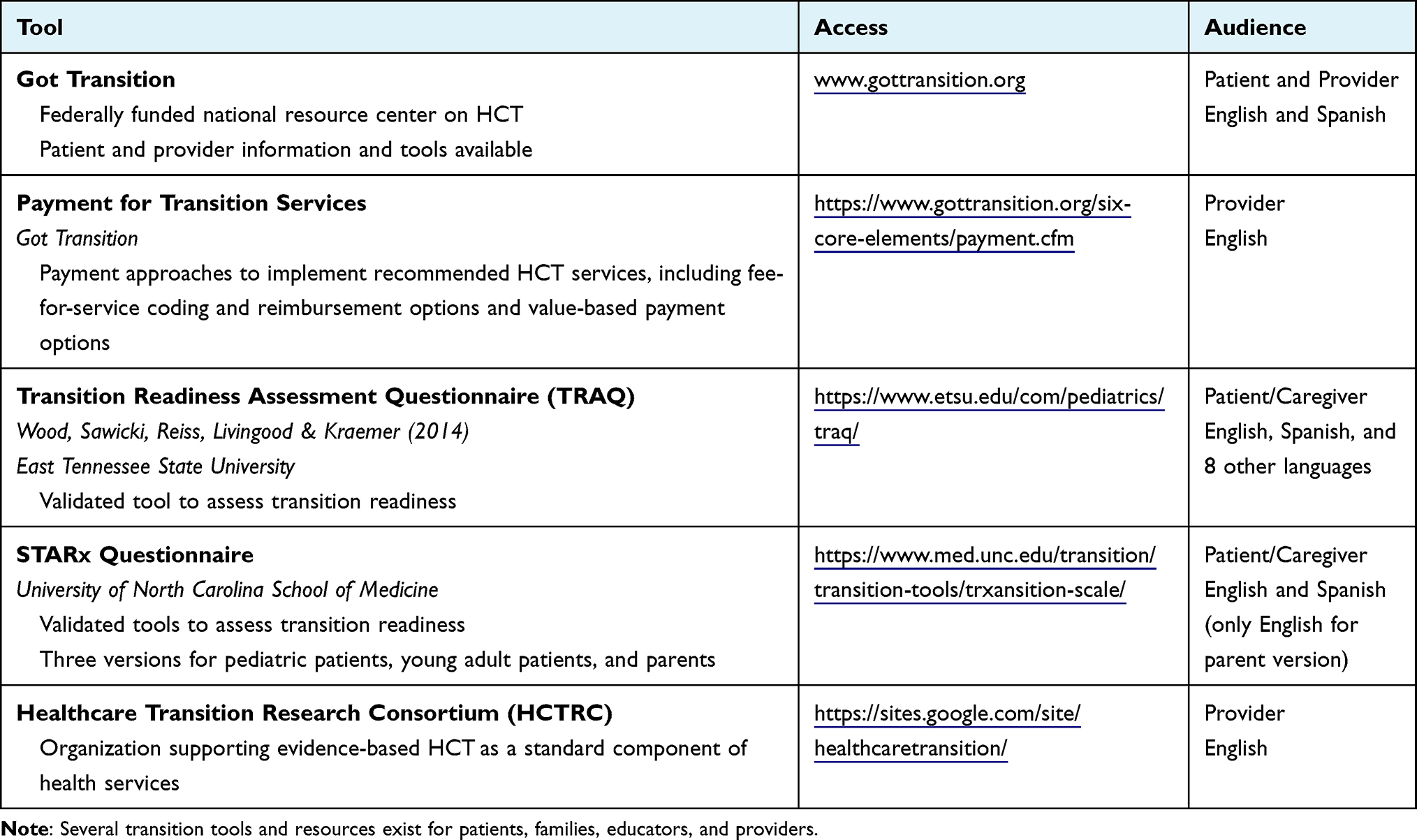 |
Table 4 General Transition Tools and Resources |
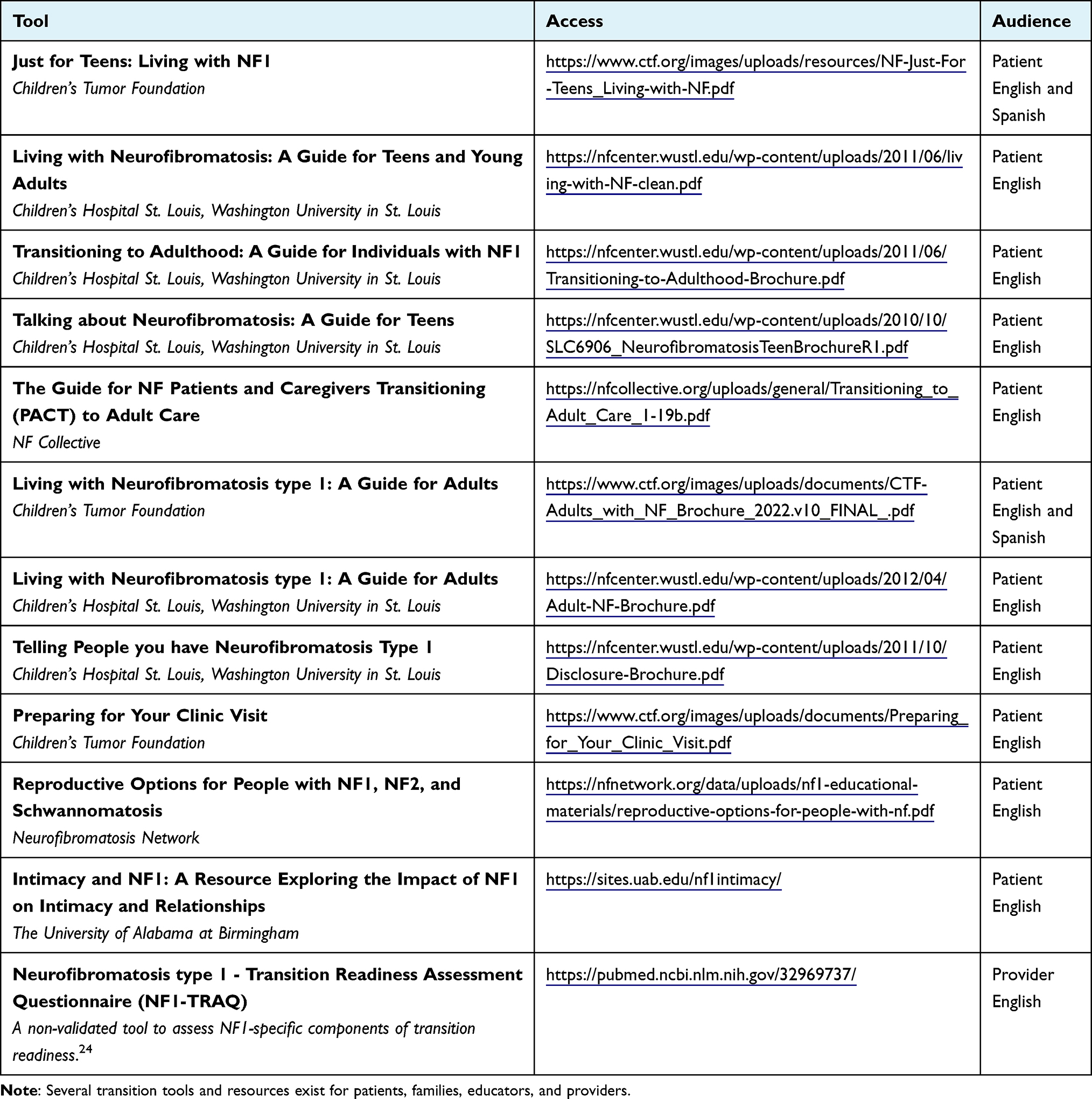 |
Table 5 NF1-Specific Transition Tools and Resources |
Information about the genetic etiology of NF1 and risks to offspring is another important educational component of NF1 HCT. While most individuals with NF1 report being interested in having biological children without NF1, young adults generally want more information and education about genetics and reproduction, including alternative family planning options.23,24,26
Provider Knowledge of the Healthcare Transition Process and NF1
Healthcare providers are tasked with helping patients and families navigate and address barriers of the HCT process.55,81 However, multiple studies have demonstrated that the majority of practicing providers do not feel prepared to help AYA patients through HCT or to provide adult care to these patients.82–85 Adult primary care doctors who are comfortable caring for complex patients are also in short supply, and these physicians report needing more support and training to care for this population.86,87 A survey by Patel et al87 compared comfort in the transfer of patients with chronic childhood disease to adult-oriented health care between internal medicine and pediatric residents. The authors reported a higher level of comfort among the pediatric trainees and suggested that training should be included in internal medicine programs. Becoming familiar with the HCT process as well as gaining knowledge and experience with NF1 can help build confidence in the HCT of AYA with NF1.
Billing and Reimbursement
The lack of reimbursement for the billing and care of AYA with special healthcare needs is a hurdle faced by healthcare providers.55 GT has numerous resources and research on reimbursement for providers to use and consider along with recommendations and the argument for value-based payment models.88 Healthcare providers should consider contacting their internal billing department to review the process of billing for services such as care coordination and readiness assessment so that transition services can be appropriately reimbursed.
Healthcare Transition and NF1 Resources and Support
Many tools and resources to facilitate effective transition are available; some apply to general healthcare transition (Table 4), while others are NF1-specific (Table 5). Formal transition programs which are often part of large pediatric medical centers are also excellent referral sites for transitioning patients.
In addition, several organizations exist that provide support and education to patients and families impacted by NF1, advocate for NF1 awareness and improvement in care, and promote NF1 research and clinical trials (Table 6). The organizations also provide a list of NF1 providers throughout the US and Canada,61,62 including many comprehensive clinics that are part of the Children’s Tumor Foundation NF Clinic Network, a network established in 2007 to improve clinical care and support best practices for those living with NF1.89
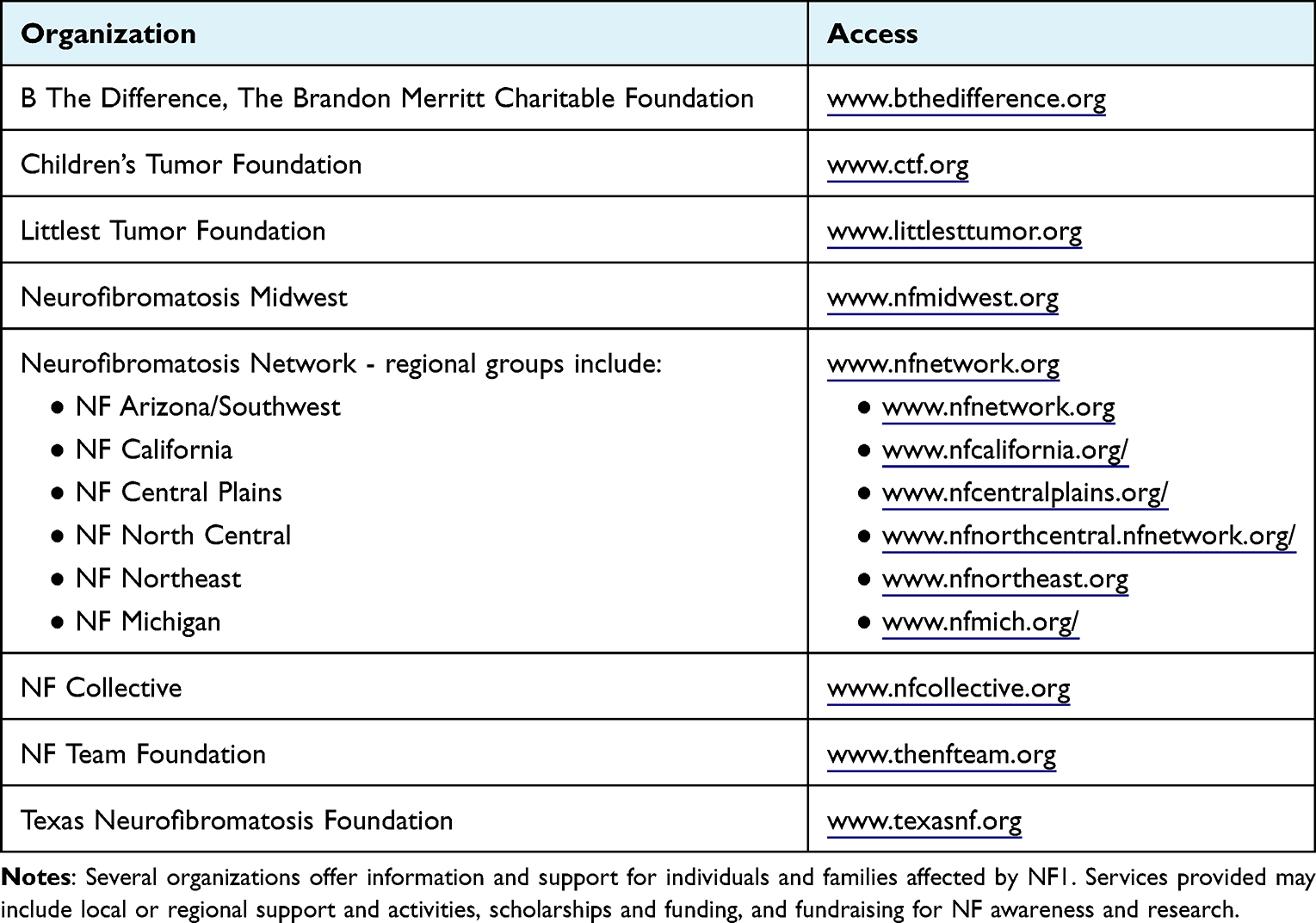 |
Table 6 Support and Advocacy Organizations for Neurofibromatosis Type 1 (NF1) |
Conclusion
NF1 is a complex multisystemic disorder with a variety of manifestations including a predisposition to tumor development, potential for disease-associated morbidity, and in some cases, cognitive or mental health impairments. A misconception among AYA individuals with NF1 is that their NF1-related health concerns may decrease as they age, rather than NF1 being a progressive condition with additional risks of adult medical complications. A committed clinician and a structured HCT program are necessary to effectively transition AYA with NF1 from a pediatric to an adult care model with the goal of building independence, improving quality of life, and decreasing associated medical complications. This review aimed to introduce clinicians to the concept of formal HCT programming for AYA with NF1 and provide valuable resources for program implementation and patient and provider education.
Future Directions
Although the need for effective HCT programs and interventions is well recognized, there is a lack of rigorous evidence-based longitudinal studies evaluating interventions, especially in AYA with special healthcare needs. There is a national research agenda currently proposed by Okumura et al90 that addresses three key areas of interest including the optimal development and implementation of HCT service models, evaluation and outcome measures for HCT, and fiscal policies to incentivize the HCT process and continuity of care. Further research is needed in these areas which can be used as a model for the care of AYA with NF1 in order to best implement HCT services in this population.
Acknowledgments
The authors would like to thank Dr. Parag Shah for his insightful comments and suggestions in the review of this manuscript.
Disclosure
Ms Heather B Radtke is an employee of the Children’s Tumor Foundation, one of the NF organizations mentioned in the manuscript. The authors report no other conflicts of interest in this work.
References
1. Blum RW, Garell D, Hodgman CH, et al. Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine. J Adolesc Health. 1993;14(7):570–576. doi:10.1016/1054-139x(93)90143-d
2. Sandquist M, Davenport T, Monaco J, et al. The transition to adulthood for youth living with rare diseases. Children. 2022;9(5):710. doi:10.3390/children9050710
3. Berens JC, Jan S, Szalda D, Hanna CM. Young adults with chronic illness: how can we improve transitions to adult care? Pediatrics. 2017;139(5). doi:10.1542/peds.2017-0410
4. Fair C, Cuttance J, Sharma N, et al. International and interdisciplinary identification of health care transition outcomes. JAMA Pediatr. 2016;170(3):205–211. doi:10.1001/jamapediatrics.2015.3168
5. White P, Schmidt A, Shorr J, Ilango S, Beck D, McManus M Six Core Elements of Health Care Transition™ Vol. 3.0. Washington, DC: Got Transition®, The National Alliance to Advance Adolescent Health; July 2020.
6. Callahan ST, Cooper WO. Continuity of health insurance coverage among young adults with disabilities. Pediatrics. 2007;119(6):1175–1180. doi:10.1542/peds.2006-1881
7. Lotstein DS, Seid M, Klingensmith G, et al. Transition from pediatric to adult care for youth diagnosed with type 1 diabetes in adolescence. Pediatrics. 2013;131:e1062–e1070. doi:10.1542/peds.2012-1450
8. Rosen DS, Blum RW, Britto M, Sawyer SM, Siegel DM. Transition to adult health care for adolescents and young adults with chronic conditions. J Adolesc Health. 2003;33(4):309–311. doi:10.1016/S1054-139X(03)00208-8
9. Sawicki GS, Whitworth R, Gunn L, Butterfield R, Lukens-Bull K, Wood D. Receipt of health care transition counseling in the national survey of adult transition and health. Pediatrics. 2011;128(3):e521–e529. doi:10.1542/peds.2010-3017
10. Quinn CT, Rogers ZR, McCavit TL, Buchanan GR. Improved survival of children and adolescents with sickle cell disease. Blood. 2010;115(17):3447–3452. doi:10.1182/blood-2009-07-233700
11. Wood DL, Sawicki GS, Miller MD, et al. The Transition Readiness Assessment Questionnaire (TRAQ): its factor structure, reliability, and validity. Acad Pediatr. 2014;14(4):415–422. doi:10.1016/j.acap.2014.03.008
12. Biggs EE, Carter EW. Quality of life for transition-age youth with autism or intellectual disability. J Autism Dev Disord. 2016;46(1):190–204. doi:10.1007/s10803-015-2563-x
13. Cotts TB. Transition of care in congenital disease: allaying fears for patients and specialists. Prog Cardiovasc Dis. 2018;61(3–4):282–286. doi:10.1016/j.pcad.2018.07.016
14. Essaddam L, Kallali W, Jemel M, et al. Implementation of effective transition from pediatric to adult diabetes care: epidemiological and clinical characteristics-A pioneering experience in North Africa. Acta Diabetol. 2018;55(11):1163–1169. doi:10.1007/s00592-018-1196-x
15. Walter M, Kamphuis S, van Pelt P, de Vroed A, Hazes JMW. Successful implementation of a clinical transition pathway for adolescents with juvenile-onset rheumatic and musculoskeletal diseases. Pediatr Rheumatol Online J. 2018;16(1):50. doi:10.1186/s12969-018-0268-3
16. Oates EC, Payne JM, Foster SL, Clarke NF, North KN. Young Australian adults with NF1 have poor access to health care, high complication rates, and limited disease knowledge. Am J Med Genet A. 2013;161A(4):659–666. doi:10.1002/ajmg.a.35840
17. Lausdahl S, Handrup MM, Rubak SL, Jensen MD, Ejerskov C. Transition to adult care of young patients with neurofibromatosis type 1 and cognitive deficits: a single-centre study. Orphanet J Rare Dis. 2022;17:208. doi:10.1186/s13023-022-02356-z
18. Evans DG, Howard E, Giblin C, et al. Birth incidence and prevalence of tumor-prone syndromes: estimates from a UK family genetic register service. Am J Med Genet Part A. 2010;152A:327–332. doi:10.1002/ajmg.a.33139
19. Lammert M, Friedman JM, Kluwe L, Mautner VF. Prevalence of neurofibromatosis 1 in German children at elementary school enrollment. Arch Dermatol. 2005;141(1):71–74. doi:10.1001/archderm.141.1.71
20. Lehtonen A, Howie E, Trump D, Huson SM. Behaviour in children with neurofibromatosis type 1: cognition, executive function, attention, emotion, and social competence. Dev Med Child Neurol. 2013;55(2):111–125. doi:10.1111/j.1469-8749.2012.04399.x
21. Miller DT, Freedenberg D, Schorry E, et al. Health supervision for children with neurofibromatosis type 1. Pediatrics. 2019;143(5):e20190660. doi:10.1542/peds.2019-0660
22. Stewart DR, Korf BR, Nathanson KL, Stevenson DA, Yohay K. Care of adults with neurofibromatosis type 1: a clinical practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2018;20(7):671–682. doi:10.1038/gim.2018.28
23. Radtke HB, Bergner AL, Goetsch AL, McGowan C, Panzer K, Cannon A. Genetic counseling for neurofibromatosis 1, neurofibromatosis 2, and schwannomatosis-practice resource of the national society of genetic counselors. J Genet Couns. 2020;29(5):692–714. doi:10.1002/jgc4.1303
24. Goetsch Weisman A, Haws T, Lee J, Lewis AM, Srdanovic N, Radtke HB. Transition readiness assessment in adolescents and young adults with neurofibromatosis type 1 (NF1). Compr Child Adolesc Nurs. 2020;1–17. doi:10.1080/24694193.2020.1806402
25. Davidson LA. Transition of Health Care for Adolescent Patients with Neurofibromatosis Type 1: Parent Perspectives [Unpublished master’s thesis]. University of South Carolina; 2010. Available from: https://scholarcommons.sc.edu/etd/165.
26. Rietman AB, van Helden H, Both PH, et al. Worries and needs of adults and parents of adults with neurofibromatosis type 1. Am J Med Genet A. 2018;176(5):1150–1160. doi:10.1002/ajmg.a.38680
27. Page PZ, Page GP, Ecosse E, Korf BR, Leplege A, Wolkenstein P. Impact of neurofibromatosis 1 on Quality of Life: a cross-sectional study of 176 American cases. Am J Med Genet A. 2006;140(18):1893–1898. doi:10.1002/ajmg.a.31422
28. Kodra Y, Giustini S, Divona L, et al. Health-related quality of life in patients with neurofibromatosis type 1. Dermatology. 2009;218:215–220. doi:10.1159/000187594
29. Wolkenstein P, Rodriguez D, Ferkal S, et al. Impact of neurofibromatosis 1 upon quality of life in childhood: a cross-sectional study of 79 cases. Br J Dermatol. 2009;160:844–848. doi:10.1111/j.1365-2133.2008.08949.x
30. Vranceanu AM, Merker VL, Park E, Plotkin SR. Quality of life among adult patients with neurofibromatosis 1, neurofibromatosis 2 and schwannomatosis: a systematic review of the literature. J Neurooncol. 2013;114(3):257–262. doi:10.1007/s11060-013-1195-2
31. Cohen JS, Levy HP, Sloan J, Dariotis J, Biesecker BB. Depression among adults with neurofibromatosis type 1: prevalence and impact on quality of life. Clin Genet. 2015;88(5):425–430. doi:10.1111/cge.12551
32. Cipolletta S, Spina G, Spoto A. Psychosocial functioning, self-image, and quality of life in children and adolescents with neurofibromatosis type 1. Child Care Health Dev. 2018;44(2):260–268. doi:10.1111/cch.12496
33. Fishbein NS, Vranceanu AM, Mace RA. Baseline characteristics of adults with neurofibromatosis enrolled on a psychosocial randomized controlled trial. J Neurooncol. 2022;159(3):637–646. doi:10.1007/s11060-022-04104-6
34. Wang DL, Smith KB, Esparza S, et al. Emotional functioning of patients with neurofibromatosis tumor suppressor syndrome. Genet Med. 2012;14(12):977–982. doi:10.1038/gim.2012.85
35. Merker VL, Bredella MA, Cai W, et al. Relationship between whole-body tumor burden, clinical phenotype, and quality of life in patients with neurofibromatosis. Am J Med Genet A. 2014;164A(6):1431–1437. doi:10.1002/ajmg.a.36466
36. Doser K, Andersen EW, Kenborg L, et al. Clinical characteristics and quality of life, depression, and anxiety in adults with neurofibromatosis type 1: a nationwide study. Am J Med Genet Part A. 2020;182A:1704–1715. doi:10.1002/ajmg.a.61627
37. Hamoy-Jimenez G, Kim R, Suppiah S, Zadeh G, Bril V, Barnett C. Quality of life in patients with neurofibromatosis type 1 and 2 in Canada. Neuro Oncol Adv. 2020;2(Suppl1):i141–i149. doi:10.1093/noajnl/vdaa003
38. Descheemaeker MJ, Ghesquière P, Symons H, Fryns JP, Legius E Behavioural, academic and neuropsychological profile of normally gifted Neurofibromatosis type 1 children. J Intellect Disabil Res. 2005;49(Pt1):33–46.
39. Graf A, Landolt MA, Mori AC, Boltshauser E. Quality of life and psychological adjustment in children and adolescents with neurofibromatosis type 1. J Pediatr. 2006;149(3):348–353. doi:10.1016/j.jpeds.2006.04.025
40. Vranceanu AM, Merker VL, Park ER, Plotkin SR. Quality of life among children and adolescents with neurofibromatosis 1: a systematic review of the literature. J Neurooncol. 2015;122(2):219–228. doi:10.1007/s11060-015-1725-1
41. Yoshida Y, Ehara Y, Koga M, Imafuku S. Health-related quality of life in patients with neurofibromatosis 1 in Japan: a questionnaire survey using EQ-5D-5L [published online ahead of print, 2022 Jul 3]. J Dermatol. 2022. doi:10.1111/1346-8138.16510
42. Vranceanu AM, Zale EL, Funes CJ, et al. Mind-body treatment for international english-speaking adults with neurofibromatosis via live video conferencing: protocol for a single-blind randomized controlled trial. JMIR Res Protoc. 2018;7(10):e11008. doi:10.2196/11008
43. Reichman M, Riklin E, Macklin E, Vranceanu AM. Virtual mind-body treatment for adolescents with neurofibromatosis: study protocol for a single-blind randomized controlled trial. Contemp Clin Trials. 2020;95:106078. doi:10.1016/j.cct.2020.106078
44. Martin S, Allen T, Toledo-Tamula MA, et al. Acceptance and commitment therapy for adolescents and adults with neurofibromatosis Type 1, plexiform neurofibromas, and chronic pain: results of a randomized controlled trial. J Contextual Behav Sci. 2021;22(93–101):93–101. doi:10.1016/j.jcbs.2021.10.003
45. Granström S, Langenbruch A, Augustin M, Mautner VF. Psychological burden in adult neurofibromatosis type 1 patients: impact of disease visibility on body image. Dermatology. 2012;224(2):160–167. doi:10.1159/000337548
46. Smith KB, Wang DL, Plotkin SR, Park ER. Appearance concerns among women with neurofibromatosis: examining sexual/bodily and social self-consciousness. Psycho-Oncology. 2013;22(12):2711–2719. doi:10.1002/pon.3350
47. Leidger A, Vosschulte M, Nieder TO, Mautner VF. Sexual self-esteem and psychological burden of adults with neurofibromatosis type 1. Front Psychol. 2022;13. doi:10.3389/fpsyg.2022.883019
48. The University of Alabama at Birmingham. Intimacy and NF1: a resource exploring the impact of NF1 on intimacy and relationships. Available from: https://sites.uab.edu/nf1intimacy/.
49. Hyman SL, Shores A, North KN. The nature and frequency of cognitive deficits in children with neurofibromatosis type 1. Neurology. 2005;65:1037–1044. doi:10.1212/01.wnl.0000179303.72345.ce
50. Buono FD, Sprong ME, Paul E, Martin S, Larkin K, Garakani A. The mediating effects of quality of life, depression, and generalized anxiety on perceived barriers to employment success for people diagnosed with Neurofibromatosis Type 1. Orphanet J Rare Dis. 2021;16:234. doi:10.1186/s13023-021-01866-6
51. Gregory TA, Molina P, Phillips GD, Henson JW. Impact of neurofibromatosis type 1 in an adult community population. Neuro Oncol Pract. 2022;9(3):229–235. doi:10.1093/nop/npac014
52. Maslow GR, Haydon AA, Ford CA, Halpern CT. Young adult outcomes of children growing up with chronic illness: an analysis of the national longitudinal study of adolescent health. Arch Pediatr Adolesc Med. 2011;165(3):256–261. doi:10.1001/archpediatrics.2010.287
53. Peron A, Canevini MP, Ghelma F, Di Marco F, Vignoli A. Healthcare transition from childhood to adulthood in Tuberous Sclerosis Complex. Am J Med Genet C Semin Med Genet. 2018;178(3):355–364. doi:10.1002/ajmg.c.31653
54. Ebel F, Greuter L, Guzman R, Soleman J. Transitional care in pediatric brain tumor patients: a systematic literature review. Children. 2022;9(4):501. doi:10.3390/children9040501
55. White PH, Cooley WC, Boudreau ADA, et al.; Transitions Clinical Report Authoring Group, American Academy of Pediatrics, American Academy of Family Physicians, & American College of Physicians. Supporting the health care transition from adolescence to adulthood in the Medical Home. Pediatrics. 2018;142(5):e20182587. doi:10.1542/peds.2018-2587
56. Gabriel P, McManus M, Rogers K, White P. Outcome Evidence for structured pediatric to adult health care transition interventions: a systematic review. J Pediatr. 2017;188:263–269.e15. doi:10.1016/j.jpeds.2017.05.066
57. Van Lierde A, Menni F, Bedeschi MF, et al. Healthcare transition in patients with rare genetic disorders with and without developmental disability: neurofibromatosis 1 and Williams-Beuren syndrome. Am J Med Genet A. 2013;161A(7):1666–1674. doi:10.1002/ajmg.a.35982
58. White P, Schmidt A, Shorr J, Ilango S, Beck D, McManus M. Six Core Elements of Health Care Transition™ 3.0. Washington, DC: Got Transition®, The National Alliance to Advance Adolescent Health; 2020.
59. Syverson EP, McCarter R, He J, D’Angelo L, Tuchman LK. Adolescents’ perceptions of transition importance, readiness, and likelihood of future success: the role of anticipatory guidance. Clin Pediatr. 2016;55(11):1020–1025. doi:10.1177/0009922816666882
60. Lemke M, Kappel R, McCarter R, D’Angelo L, Tuchman LK. Perceptions of health care transition care coordination in patients with chronic illness. Pediatrics. 2018;141:e20173168. doi:10.1542/peds.2017-3168
61. Children’s Tumor Foundation. Find a doctor. Available from: https://ctf.org/doctor.
62. NF Collective. Find a doctor. Available from: https://nfcollective.org/find-A-doctor.
63. Breneol S, Doucet S, McIsaac J-L, et al. Programmes to support transitions in community care for children with complex care needs: a scoping review. BMJ Open. 2022;12(7):e056799. doi:10.1136/bmjopen-2021-056799
64. Varshney K, Iriowen R, Morrell K, Pillay P, Fossi A, Stephens MM. Disparities and outcomes of patients living with Down Syndrome undergoing healthcare transitions from pediatric to adult care: a scoping review. Am J Med Genet A. 2022;188(8):2293–2302. doi:10.1002/ajmg.a.62854
65. Gray WN, Schaefer MR, Resmini-Rawlinson A, Wagoner ST. Barriers to transition from pediatric to adult care: a systematic review. J Pediatr Psychol. 2018;43(5):488–502. doi:10.1093/jpepsy/jsx142
66. Ellison JL, Brown RE, Ameringer S. Parents’ experiences with health care transition of their adolescents and young adults with medically complex conditions: a scoping review. J Pediatr Nurs. 2022;66(70–78):70–78. doi:10.1016/j.pedn.2022.04.018
67. Miller D, Felker M, Ciccarelli M. Transitioning ambulatory medicine from pediatrics to adult care for patients with epilepsy and intellectual disability. J Pediatr Epilep. 2020;09(04):172–176. doi:10.1055/s-0040-1717135
68. Health Resources & Services Administration (HRSA) Maternal & Child Health. Children and Youth with Special Health Care Needs (CYSHCN). Available from: https://mchb.hrsa.gov/programs-impact/focus-areas/children-youth-special-health-care-needs-cyshcn.
69. Data Resource Center for Child & Adolescent Health. The national survey of children’s health. Available from: https://www.childhealthdata.org/learn-about-The-nsch/NSCH.
70. Lotstein DS, McPherson M, Strickland B, Newacheck PW. Transition planning for youth with special health care needs: results from the national survey of children with special health care needs. Pediatrics. 2005;115(6):1562–1568. doi:10.1542/peds.2004-1262
71. Heron LM, Agarwal R, Greenup J, Maddux M, Attong N, Burke SL. Disparities in healthcare transition support received by adolescents with special healthcare needs. J Appl Res Intellect Disabil. 2020;33(2):180–192. doi:10.1111/jar.12658
72. Van Puymbrouck L, Friedman C, Feldner H Explicit and implicit disability attitudes of healthcare providers. Rehabil Psychol. 2020;65(2):101–112.
73. Chisolm DJ, Keedy HE, Hart LC, et al. Exploring health literacy, transition readiness, and healthcare utilization in medicaid chronically ill youth. J Adolesc Health. 2021;69(4):622–628. doi:10.1016/j.jadohealth.2021.03.023
74. Beal SJ, Riddle IK, Kichler JC, et al. The associations of chronic condition type and individual characteristics with transition readiness. Acad Pediatr. 2016;16(7):660–667. doi:10.1016/j.acap.2016.06.007
75. Huang J, Porterfield SL. Changes in health insurance coverage and health care access as teens with disabilities transition to adulthood. Disabil Health J. 2019;12(4):551–556. doi:10.1016/j.dhjo.2019.06.009
76. Feldman HM, Buysse CA, Hubner LM, Huffman LC, Loe IM. Patient Protection and Affordable Care Act of 2010 and children and youth with special health care needs. J Dev Behav Pediatr. 2015;36(3):207–217. doi:10.1097/DBP.0000000000000151
77. Okumura MJ, Hersh AO, Hilton JF, Lotstein DS. Change in health status and access to care in young adults with special health care needs: results from the 2007 national survey of adult transition and health. J Adolescent Health. 2013;52(4):413–418. doi:10.1016/j.jadohealth.2012.08.005
78. Wang G, Grembowski D, Watts C. Risk of losing insurance during the transition into adulthood among insured youth with disabilities. Matern Child Health J. 2010;14(1):67–74. doi:10.1007/s10995-009-0470-5
79. National Comprehensive Cancer Network. Genetic/familial high-risk assessment: breast, ovarian and pancreatic. Volume 2.2022. Available from: https://NCCN.org/guidelines/category_2.
80. Leppävirta J, Kallionpää RA, Uusitalo E, et al. The pregnancy in neurofibromatosis 1: a retrospective register-based total population study. Am J Med Genet A. 2017;173(10):2641–2648. doi:10.1002/ajmg.a.38372
81. Cooley WC, Sagerman PJ; American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians; Transitions Clinical Report Authoring Group. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. 2011;128(1):182–200. doi:10.1542/peds.2011-0969
82. Freed GL; Research Advisory Committee of the American Board of Pediatrics. Comparing perceptions of training for medicine-pediatrics and categorically trained physicians. Pediatrics. 2016;118(3):1104–1108. doi:10.1542/peds.2006-0042
83. Hunt S, Sharma N. Pediatric to adult-care transitions in childhood-onset chronic disease: hospitalist perspectives. J Hosp Med. 2013;8(11):627–630. doi:10.1002/jhm.2091
84. Okumura MJ, Heisler M, Davis MM, Cabana MD, Demonner S, Kerr EA. Comfort of general internists and general pediatricians in providing care for young adults with chronic illnesses of childhood. J General Intern Med. 2008;23(10):1621–1627. doi:10.1007/s11606-008-0716-8
85. Sadun RE, Chung RJ, Pollock MD, Maslow GR. Lost in transition: resident and fellow training and experience caring for young adults with chronic conditions in a large United States’ academic medical center. Med Educ Online. 2019;24(1):1605783. doi:10.1080/10872981.2019.1605783
86. McManus M, Fox H, O’Connor K, Chapman T, MacKinnon J. Pediatric perspectives and practices on transitioning adolescents with special needs to adult health care. Fact Sheet No. 6. The National Alliance to Advance Adolescent Health; 2008. Available from: https://www.thenationalalliance.org/publications/2017/7/9/pediatric-perspectives-and-practices-on-transitioning-adolescents-with-special-needs-to-adult-health-care.
87. Patel MS, O’Hare K. Residency training in transition of youth with childhood-onset chronic disease. Pediatrics. 2010;126(Suppl 3):S190–S193. doi:10.1542/peds.2010-1466P
88. Payment for Transition Services. Six core elements of health care transition. Available from: https://www.gottransition.org/six-core-elements/payment.cfm.
89. NF Clinic Network (NFCN). Children’s tumor foundation. Available from: https://ctf.org/research/nf-clinic-network.
90. Okumura MJ, Kuo DZ, Ware AN, Cyr MH, White PH. Improving health care transitions for children and youth with special health care needs. Acad Pediatr. 2022;22(2):S7–S13. doi:10.1016/j.acap.2021.03.014
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review and Content Analysis of Available Chronic Pain Education Programs and Resources for Children, Adolescents and Young Adults with Diverse Abilities
Smith MG, Schaly S, Berryman C, Khillan A, Ostojic K, Harvey A
Journal of Pain Research 2026, 19:601477
Published Date: 13 May 2026