")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Neural Correlates of Anhedonia in Major Depressive Disorder: Insights from Concurrent Analysis of Feedback-Related Negativity and Stimulus-Preceding Negativity
Authors Sun Y, Huang Z, Gao X , Chen L, Wang J, Zhou Z , Zhou H
Received 11 August 2023
Accepted for publication 16 November 2023
Published 23 November 2023 Volume 2023:19 Pages 2549—2560
DOI https://doi.org/10.2147/NDT.S435017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Yifan Sun,1 Zixuan Huang,2 Xuezheng Gao,1 Limin Chen,3 Jun Wang,1,3 Zhenhe Zhou,1,3 Hongliang Zhou4
1Department of Psychiatry, The Affiliated Wuxi Mental Health Center of Nanjing Medical University, Wuxi City, 214151, People’s Republic of China; 2Department of Music and Wellbeing, School of Music, University of Leeds, Leeds City, UK; 3Department of Psychiatry, The Affiliated Mental Health Center of Jiangnan University, Wuxi City, 214151, People’s Republic of China; 4Department of Psychology, The Affiliated Hospital of Jiangnan University, Wuxi City, 214151, People’s Republic of China
Correspondence: Jun Wang, Department of Clinical Psychology, The Affiliated Wuxi Mental Health Center of Nanjing Medical University, Wuxi City, 214151, People’s Republic of China, Tel +86 13358119628, Fax +86 51083219366, Email [email protected]; Zhenhe Zhou, Department of Psychiatry, The Affiliated Wuxi Mental Health Center of Nanjing Medical University, Wuxi City, 214151, People’s Republic of China, Tel +86 13358118986, Fax +86 51083219366, Email [email protected]
Purpose: Anhedonia, a core symptom of major depressive disorder (MDD), is explored in this study, focusing on the neural underpinnings through the examination of two event-related potential (ERP) components: feedback-related negativity (FRN) and stimulus-preceding negativity (SPN).
Patients and Methods: This cross-sectional study was conducted in China from March 2022 to March 2023. It involved 35 MDD patients and 31 healthy controls (HC) participating in a modified 2-door task with simultaneous EEG recordings. Depression severity and anhedonia were assessed using the Hamilton Depression Scale (HAMD) and the Temporal Experience of Pleasure Scale (TEPS-CV), respectively. FRN and SPN metrics, along with correlations with each other and clinical assessments, were examined.
Results: In comparison to the HC group, the MDD group exhibited significantly lower scores in TEPS-CV (t = 2.854, p = 0.006) and its subscales (t = − 3.596, p = 0.001 and t = 2.434, p = 0.018, respectively), along with consistently reduced amplitudes of FRN (F 1.64= 4.726, p = 0.033) and SPN (F 1.64= 4.195, p = 0.045) across all conditions. Limited correlations were observed between ERP metrics and clinical indicators, except for positive correlations between FRN amplitudes (loss minus win) and HAMD scores (r = 0.392, p = 0.020), and SPN amplitudes after losing (SPN-L) and TEPS-CV consumption subscale scores (r = 0.357, p = 0.035). Notably, while the HC group displayed no significant FRN-SPN correlations, the MDD group exhibited positive FRN-SPN correlations under distinct conditions (r = 0.376, p = 0.026 and r = 0.355, p = 0.037, respectively).
Conclusion: Our data reveal subjective and objective anhedonia in both consumption and anticipation, suggesting a shared impairment in reward feedback processing and anticipatory neural mechanisms in individuals with MDD. These findings deepen our understanding of anhedonia’s neural foundations and may guide targeted interventions for this core symptom.
Keywords: major depressive disorder, anhedonia, event-related potential, reward processing, feedback-related negativity, stimulus-preceding negativity
Introduction
Major depressive disorder (MDD) is a prevalent mental health condition affecting millions worldwide, characterized by persistent feelings of sadness, anhedonia, and a diminished capacity to experience pleasure from once-enjoyable activities. Anhedonia, in particular, plays a crucial role in the development and maintenance of depression, serving as a core symptom for current diagnostic criterion.1 The severity of anhedonia is usually associated with the overall severity of the depressive episode, and individuals with more pronounced anhedonia tend to be more treatment-resistant, and have overall poorer quality of life2,3 Despite its clinical significance, the underlying neurobiological mechanisms that give rise to anhedonia remain poorly understood.
In recent years, researchers have turned to the study of electrophysiological characteristics, such as event-related potentials (ERPs), to gain deeper insights into the neural processes underlying anhedonia in MDD patients. Anhedonia in consumption and anticipation are the most common subtypes of anhedonia, referring to the diminished ability to experience pleasure or enjoyment when engaging in consumer activities and the reduced sense of excitement, pleasure, or positive anticipation that individuals experience before engaging in a future consumer activity, respectively.1 Correspondingly, there are two specific ERP components that may reflect the neurobiological processes related to anhedonia in consumption and anticipation, namely, the Feedback-Related Negativity (FRN) and the Stimulus Preceding Negativity (SPN). In brief, the FRN is an ERP component elicited in response to feedback following the outcome of an action, reflecting the brain’s sensitivity to the valence of received feedback.4–6 On the other hand, the SPN is observed before the presentation of an upcoming stimulus and has been associated with anticipatory neural processes.7–9
In MDD, the FRN has been the subject of considerable research, particularly in the context of anhedonia and reward processing deficits.6 Multiple studies have indicated that individuals with depression, particularly those experiencing anhedonia, demonstrate decreased FRN amplitudes in response to positive feedback or rewards (also named reward positivity, RewP10,11) compared to healthy controls.12,13 Some studies have also reported significant differences in SPN amplitudes between individuals with depression and healthy controls.14 In general, these studies can offer valuable insights into the neurobiological mechanisms underlying anhedonia in MDD. Worth noting is that results of previous studies are not always consistent.15 For example, Christina Luckhardt et al discovered a correlation between MDD symptoms and smaller SPN,14 whereas another study identified an increased SPN in participants with high levels of depression.16 The inconsistencies may be due to differences in study methodologies, participant characteristics, and the specific nature of the tasks used to elicit the FRN and/or SPN response, which also illustrates the need to further explore the characteristics of FRN and SPN in patients with MDD.
More notably, previous studies have often studied the FRN and SPN in MDD separately, and sparse research exploring whether patients with MDD have concurrent deficits in both FRN and SPN, as well as the relationship between them, has yielded inconsistent results.17–20 Evidence has shown that FRN and SPN may have distinct but also overlapping neural circuits that reflect different neural processes in the brain.21 By investigating the concurrent deficits or alterations in these ERP components and unraveling the relationship between them in the same framework, we can gain deeper insights into the neural mechanisms underlying anhedonia and reward processing deficits in MDD. Ultimately, this research will provide important information for identifying reliable neural markers that may aid in diagnostic assessment and personalized treatment approaches.
Based on the above reasons, we undertook the current study with the aim of addressing the critical gaps in our current understanding of the characteristics of and relationship between the FRN and SPN in individuals with MDD within the same framework. We expect to replicate FRN and SPN deficits in individuals with MDD, particularly those with anhedonia, when compared to healthy controls. Moreover, we hypothesize that the abnormalities of FRN and SPN in MDD, while distinct in clinical correlations, would exhibit less independence than those observed in health controls, suggesting the altered anticipatory and feedback-related processes in MDD may be linked and influenced by shared neural mechanisms. This comprehensive investigation will not only contribute to the existing literature but also provide valuable information for gaining deeper insights into the interconnected neural mechanisms underlying anhedonia and related neuroprocessing deficits in MDD.
Materials and Methods
Time and Setting
This was a cross-sectional study conducted from March 2022 to March 2023 at the Wuxi Mental Health Center (WMHC), a university-affiliated psychiatric hospital in Wuxi city, Jiangsu province, China. Prior to commencement, the study received approval from the local Ethics Committee (WXMHCIRB2022LLky002), and it was conducted in accordance with the principles outlined in the Declaration of Helsinki. All participants in the study signed informed consent forms prior to their participation, indicating their voluntary agreement to take part in the research.
Participants
We recruited participants for the MDD group from both the outpatient and inpatient departments of the WMHC, prioritizing inpatients to minimize the risk of dropout. Researchers reached out to potentially eligible patients to provide information about the study, and those who expressed voluntary interest were subsequently assessed for eligibility using predefined criteria as follows. The inclusion criteria for this group included: (a) met the criteria of MDD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), (b) aged from 18 to 60 years at enrolment, and (c) Chinese Han, and have a minimum education level of primary school. The exclusion criteria included: (a) met the criteria of any other mental disorders according to DSM-5, (b) had undergone (modified) electroconvulsive therapy (ECT/MECT) during the past 6 months, (c) had substance abuse or dependence, such as nicotine, alcohol, morphine, (d) had significant physical or neurological illnesses, and (e) had difficulty to fulfil the required paradigm in this study.
Participants for the Healthy Control (HC) group were recruited by posting flyers in local communities. As with the MDD group, interested individuals received detailed information and were assessed for eligibility upon volunteering to participate. To be included, participants must not meet criteria of any psychotic disorders as determined by the Chinese version of MINI-International Neuropsychiatric Interview.22 They were also required to have no family history of mental disorders. Inclusion criteria (b) and (c), as well as the exclusion criteria for HC group were the same as the MDD group.
Sample size calculation for the planned mixed-design analysis of variance (ANOVA) (detailed in the Statistical Analysis section) was conducted using G*Power 3.1.9.2.23. Based on findings from a recent meta-analytic review involving FRN,6 we assumed there would be a medium effect size for the difference between the MDD and HC groups and therefore set a Cohen’s f of 0.25 (corresponding to a medium effect size). We set an alpha level of 0.05 and a power of 0.95 to detect at least this effect size. The analysis assumed a correlation among repeated measures of 0.5 and a nonsphericity correction ε of 1, and the number of measurements was set at 2. Given these parameters, G*Power estimated that a total sample size of 54 participants would be required to achieve adequate power for the primary outcome measures in the mixed-design ANOVA. Given a dropout and low data quality rate of 20%, a total of 68 participants should be enrolled to ensure we retain the required sample size, which means no less than 34 participants per group at a 1 to 1 ratio.
Clinical Assessments
In this study, the severity of depressive symptoms was assessed using the 17-item Chinese version of the Hamilton Depression Rating Scale (HAMD), which is known for its satisfactory internal consistency, reliability, and validity, and is one of the most commonly employed scales in evaluating depression severity.24–26 Total scores were categorized as follows: scores of <7 points indicated no depressive symptoms, 7–17 points indicated mild depressive symptoms, 18–24 points indicated moderate depressive symptoms, and scores >24 points indicated severe depressive symptoms.
For evaluating participants’ anhedonia characteristics and severities, the Chinese version of the Temporal Experience of Pleasure Scale (TEPS-CV) was used. As previously reported, the TEPS-CV has demonstrated good internal consistency and test-retest stability, and has been frequently used to study anhedonia in individuals with various conditions in China.27–30 TEPS-CV consists of 20 questions rated on a scale from 1 (very false) to 6 (very true), with lower scores indicating more severe anhedonia. By calculating the scores of subscales, the TEPS-CV can further classify anhedonia into anticipatory (ANT) and consummatory (CON) subtypes.27–30
Study Paradigm
Among the various paradigms for assessing anhedonia and reward processing deficits, the simple gambling task—also known as the “2-door task” or “Doors guessing task”—is a classic example that has been widely used and reported, especially when combined with neuroscience research technology6,29,31 In this study, this paradigm was adapted and programmed using E-Prime 3.0 (Psychology Software Tools Incorporated, Pittsburgh, United States). The sketch of the study procedure is depicted in Figure 1. In this task, participants were informed that they would be playing a guess-door game with the computer. They were required to press the left or right arrow on the keyboard to choose one of the two identical doors displayed on the screen within a time limit of 5000 milliseconds (ms) per trial. Although the odds of winning or losing were set at 50% to 50% in advance, participants were informed that if they chose the same door as the computer, they would receive a monetary reward; otherwise, they would lose money.
 |
Figure 1 Sketch of the 2-door task: Participants are required to select one of the two identical doors displayed on the screen within 5000ms. Following a 3000ms wait time with a fixation at the center of the screen, feedback indicating either a monetary win or loss will be presented for 2000ms. The inter-trial interval (ITI) is set at 1000ms. |
After making their choice, the doors disappeared, and a fixation cross “+” appeared at the center of the screen, lasting for 3000 ms, before the feedback was presented. The feedback consisted of an up arrow with the Chinese character “赢” (meaning “win” in English) or a down arrow with the Chinese character “输” (meaning “lose” in English) in the same colour and font size, representing either a win or a loss of money, respectively. The amounts of reward were manipulated as smaller (5 RMB) or bigger (55 RMB) at a 1:1 ratio for both winning and losing situations. The feedback remained on the screen for 2000 ms before the next trial started.
The task included a total of 160 trials, with each of the four feedback conditions (win 5, win 55, lose 5, and lose 55) equally allocated to different trials. Consequently, each condition appeared 40 times for each participant in a random sequence, regardless of which button the participant chose. To avoid fatigue, the 160 trials were equally divided into two blocks, with a 10-minute rest between the blocks. At the end of the first block, a motivational message appeared, stating “you have won 135 RMB, keep up and good luck!” to encourage participants to remain interested and engaged.
Before the formal task, a practice session was conducted to ensure that all participants were familiar with the test. After completing the entire experiment, each participant was compensated with a payment of 200 RMB (approximately 30 US dollars) for their time.
EEG Recording and Pre-Processing
Continuous EEG data was synchronously recorded while the participants were performing the 2-door task using a 64-channel EasyCap (Brain Products GmbH, Germany) and the BrainAmp Standard amplifier (Brain Products GmbH, Germany). The EEG signal was sampled at a rate of 500 Hz and filtered with a band-pass filter ranging between 0.1 and 100 hertz (Hz). An electrode placed on the forehead served as the reference, while the one on the left subclavian area served as the ground. To record signals of blinks and other types of eye movements, two horizon electrooculogram (HEOG) electrodes were positioned approximately 1cm behind the lateral angles of the eyes, and a vertical electrooculogram (VEOG) electrode was placed around 1cm below the center of the left eye. To ensure high-quality recordings, the impedance of all electrodes was carefully maintained below 5 kiloOhm (kΩ) throughout the entire recording process.
The software MATLAB 2020b (The MathWorks GmbH, Adalperostr. 45, München (Ismaning), 85737, Germany) and the EEGLAB 2021 (https://sccn.ucsd.edu/eeglab/index.php) were employed to pre-process the EEG data, following established methods reported by previous studies. The pre-processing steps included the following: Spherical spline interpolation method was used to interpolate bad channels, all EEG data were re-referenced to the average of bilateral mastoids, and was band-pass filtered from 0.1 to 30 Hz (0.1 to 20 Hz for SPN, and with a low-pass cutoff at 7 Hz for SPN figures17,32) with a notch filter at 50 Hz. Independent Component Analysis (ICA) was applied to identify and reject components related to eye movements and noise. For FRN analysis, segmentation was performed from −200ms prior to and 1000ms post-feedback stimuli, with a baseline correction using the time window from −200ms to 0ms. For SPN analysis, epochs were segmented based on participants’ response (pressing the left or right arrow), and baseline correction was done using the time window from 1000ms to 1200ms post-response, effectively excluding movement-related potentials. Epochs were then automatically rejected if their absolute amplitudes exceeded 70μV or if the absolute amplitude was less than 0.5μV for a duration of more than 100ms. After then, epochs of the same condition were averaged on the individual level.
For FRN, the indicators of interest were the peak amplitudes for each condition within the time window of 250ms to 350ms after feedback. As this component is typically maximum in the frontal-central region, we focused on the average amplitude of six electrodes (F1, Fz, F2, FC1, FCz, FC2) was selected for analysis, as has been done in many previous studies.33 Similarly, in line with the typical topographical features of SPN, our attention was directed towards the mean amplitude of the right frontal-central sites (F2, FC2) within the time frame of 200ms prior to the feedback presentation (equivalent to 2800~3000ms following the last keyboard response).
Statistical Analysis
The data analysis was performed using IBM SPSS Statistics version 22 (IBM Corp., Armonk, NY, United States). For continuous variables, independent sample t-tests were used to compare differences between the two groups, while the chi-square test was employed for categorical variables. To assess the group differences in FRN for both win and lose conditions, we conducted a 2 (Group: MDD vs HC) × 2 (Valence: win vs lose) mixed-design analysis of variance (ANOVA). Furthermore, we explored the impact of reward amount on FRN using a 2 (Group: MDD vs HC) × 2 (Valence: win vs lose) × 2 (Amount: big vs small) mixed-design ANOVA. Similarly, for SPN, a 2 (Group: MDD vs HC) × 2 (Valence: following win feedback vs following lose feedback) mixed-design ANOVA was utilized to compare the group differences in SPN amplitude following different conditions. To explore the impact of consecutive feedbacks (ie, win again or lose again) for SPN, we also performed a 2 (Group) × 2 (Valence) × 2 (Times: win/lose once vs win/lose again) mixed- design ANOVA. In cases where the sphericity assumption was violated, Greenhouse-Geisser correction was applied, and post hoc comparisons were adjusted using Bonferroni correction. Pearson’s correlation analysis was performed to investigate the relationships between FRN and SPN, as well as the ERP metrics and clinical indicators. A p-value of less than 0.05 (2-sided) was considered statistically significant.
Results
Flow of Participants Through the Study
A total of 41 MDD patients and 36 HCs participated in this study. Among them, 2 MDD patients and 2 HCs declined to complete all procedures due to fatigue or discomfort. Additionally, data from 4 MDD patients and 2 HCs were excluded due to poor data quality, and data from another 1 HC was excluded due to technical issues. Ultimately, data from 35 individuals with MDD (10 males and 25 females) and 31 HCs (8 males and 23 females) were included in the final analysis.
Demographic and Clinical Characteristics
Table 1 presents the demographic characteristics of the participants. There were no significant differences between the two groups in terms of age at enrolment, gender distribution, educational level, and handedness. This indicates that both groups were comparable in terms of these demographic factors. The total scores of HAMD were significantly higher in the MDD group than in the HC group (t = −7.921, p < 0.001). On the other hand, the MDD group had significantly lower total TEPS-CV scores (t = 2.854, p = 0.006), as well as significantly lower ANT subscale scores (t = −3.596, p = 0.001) and CON subscale scores (t = 2.434, p = 0.018). These findings collectively indicate the presence of anhedonia, both in terms of reduced anticipation and consumption of pleasurable activities, in this population with MDD.
 |
Table 1 Demographic Characteristics and Clinical Information of Two Groups |
ERP Metrics
For the ERP analysis, only EEG data following valid responses were included in the analysis. This means that trials in which participants failed to choose a door within 5 seconds were excluded. In total, the average number of valid responses in the MDD group was 157.60 ± 9.87, and in the HC group, it was 153.74 ± 10.14. Independent t-tests were conducted, and the results indicated that the valid responses for all conditions were comparable between both groups (t = −1.89~-0.62, all p > 0.05). These findings suggest that participants from both groups engaged similarly in the task, ensuring a valid basis for the subsequent ERP analysis.
Regarding the amplitude of FRN, the results of a 2 (Group) × 2 (Valence) mixed- design ANOVA revealed significant main effects for both Group (F 1.64= 4.726, p = 0.033, ηp2 = 0.069) and Valence (F 1.64= 22.096, p < 0.001, ηp2 = 0.257). Specifically, the MDD group exhibited a markedly lower (more negative) FRN amplitude compared to the HC group. Additionally, the amplitude of FRN following the Lose condition (FRN-L) was notably lower than that following the Win condition (FRN-W). The interaction effect of Group × Valence was found to be significant (F 1.64= 6.212, p = 0.015, ηp2 = 0.088). Further simple effect analysis revealed that the mean amplitude of FRN-W was significantly larger (less negative) than that of FRN-L in the HC group (F 1.64= 24.391, p < 0.001, ηp2 = 0.276), while such a pattern was not observed in the MDD group (F 1.64= 2.595, p = 0.112, ηp2 = 0.039). Additionally, in comparison to the MDD group, the amplitude of FRN-W was significantly larger (F 1.64= 6.268, p = 0.015, ηp2 = 0.089), and the amplitude of FRN-L was marginally larger in HC group (F 1.64= 3.206, p = 0.078, ηp2 = 0.048). An independent-sample t-test revealed that the difference wave of FRN (FRN-D, calculated as FRN-L minus FRN-W) was also significantly larger in the HC group compared to the MDD group. (t64 = −2.596, p = 0.012). These findings collectively highlight distinct FRN response patterns between the HC and MDD groups, particularly in the context of different win and lose conditions (Figure 2).
 |
Figure 2 (a) Grand averaged ERPs of the win condition in the HC group (solid green line), lose condition in the HC group (solid red line), win condition in the MDD group (dashed green line), and lose condition in the MDD group (dashed red line); the difference wave of the lose condition minus the win condition in the HC group (solid blue line) and in the MDD group (dashed blue line). The time window corresponding to FRN is indicated by the pink shaded area. (b) A topography map depicting the grand average amplitude of the difference wave within the 250ms-350ms timeframe for the HC group (upper) and the MDD group (lower). Electrodes of interest (F1, Fz, F2, FC1, FCz, FC2) are marked as red points. Abbreviations: HC, Healthy Control; MDD, Major Depressive Disorder; FRN, feedback-related negativity. |
We further explored the impact of reward amounts using a 2 (Group) × 2 (Valence) × 2 (Amount) mixed-design ANOVA. The main effect of amount was found to be significant (F 1.64= 13.631, p < 0.001, ηp2 = 0.176). However, the interaction effects involving amount, including Group × Valence × Amount (F 1.64= 3.265, p = 0.075, ηp2 = 0.049), Group × Amount (F 1.64= 0.891, p = 0.349, ηp2 = 0.014), as well as Valence × Amount (F 1.64= 1.710, p = 0.196, ηp2 = 0.026), were all found to be non-significant. The main effects of Valence (F 1.64= 22.058, p < 0.001, ηp2 = 0.256) and the interaction effect of Group × Valence (F 1.64= 6.127, p = 0.016, ηp2 = 0.087), which were significant in the 2 (Group) × 2 (Valence) mixed-design ANOVA, remained significant in this 3-way mixed model ANOVA, with minimal changes in the statistical outcomes.
Based on the outcomes of the independent sample t-test, when aggregating the combined SPNs (SPN-C) following both win feedback (SPN-W) and lose feedback (SPN-L) from the last trial, the mean amplitude of SPN-C in the HC group exhibited a significantly larger (more negative) value compared to the MDD group (t64 = −2.821, p = 0.006). Similar to the FRN analysis, we conducted a 2 (Group) × 2 (Valence) mixed-design ANOVA to further investigate differences within and between groups. The main effect of Group was found to be significant (F 1.64= 4.195, p = 0.045, ηp2 = 0.062), indicating that the HC group exhibited a much larger SPN amplitude compared to the MDD group. Moreover, the main effect of Valence was also significant (F 1.64= 5.733, p = 0.019, ηp2 = 0.083), revealing that the amplitude of SPN-W was larger than that of SPN-L. However, the interaction effect of Group × Valence was not significant (F 1.64= 0.370, p = 0.545, ηp2 = 0.006), suggesting that the difference in SPN amplitude between the HC and MDD groups was consistent across both win and lose conditions (Figure 3).
 |
Figure 3 (a) Grand averaged ERPs preceding feedbacks following the win condition in the HC group (solid green line) and MDD group (dashed green line), and the lose condition in the HC group (solid red line) and MDD group (dashed red line). The SPN time window is highlighted using a pink shadow. (b) Topography map of the grand average amplitude of SPN within its timeframe for HC group (up) and MDD group (down). The electrodes of interest (F2, FC2) are highlighted as red points. Abbreviations: HC, Healthy Control; MDD, Major Depressive Disorder; SPN, stimulus-preceding negativity. |
To explore whether participant adjust their anticipation levels based on consecutive feedbacks (ie, win again or lose again), we conducted further analysis to assess whether the occurrence of Win-again or Lose-again feedback would influence SPN amplitude. Results of a 2 (Group) × 2 (Valence) × 2 (Times) mixed-design ANOVA indicated that the main effect of Times (F 1.64 = 0.508, p = 0.479, ηp2 = 0.008) was not statistically significant. Similarly, none of the interaction effects involving the Again factor demonstrated significance, including Group × Valence × Times (F 1.64 = 0.309, p = 0.580, ηp2 = 0.005), Group × Times (F 1.64 = 2.413, p = 0.125, ηp2 = 0.036), and Valence × Times (F 1.64 = 0.873, p = 0.354, ηp2 = 0.013) interactions. It is worth noting that the previously mentioned main effects of Group (F 1.64 = 5.756, p = 0.019, ηp2 = 0.083) and Valence (F 1.64 = 10.804, p = 0.002, ηp2 = 0.144) remained statistically significant, albeit with minor variations in the results.
Correlations Among Variables
We conducted a Pearson correlation analysis to investigate potential correlations among the aforementioned factors, with a specific focus on the FRN and SPN metrics, within both the HC and MDD groups. As illustrated in Figure 4, moderate to high positive correlations were observed for both groups within three internal domains of variables, including TEPS-CV and its subscales, different subtypes of FRN, as well as various subtypes of SPN.
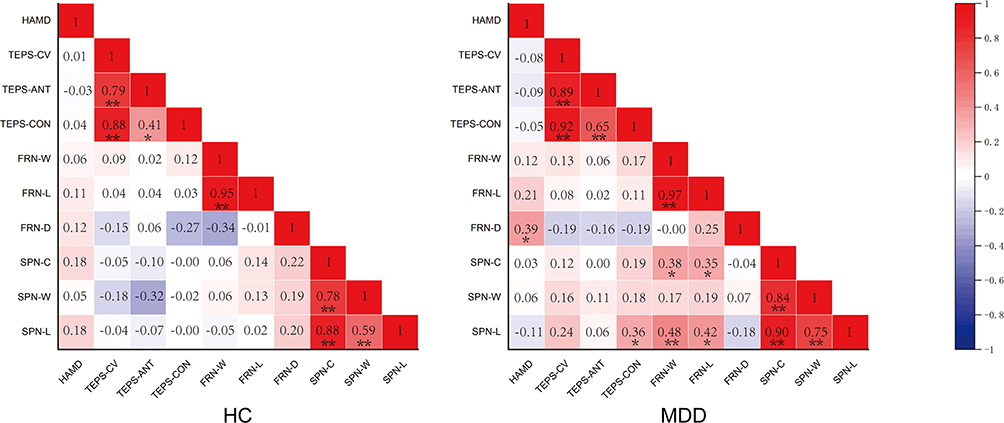 |
Figure 4 Heat map for correlations among variables in HC (left) and MDD (right) groups. Positive correlations are indicated in red, while negative correlations are marked in blue. Abbreviations: HC, Healthy Control; MDD, Major Depressive Disorder; HAMD, Hamilton Depression Scale; TEPS-CV, Temporal Experience of Pleasure Scale-Chinese Version; TEPS-ANT, TEPS anticipatory subscale; TEPS-CON, TEPS consummatory subscale; FRN, feedback-related negativity; FRN-W, FRN following the win feedback; FRN-L, FRN following the lose feedback; FRN-D, difference wave of FRN; SPN, stimulus-preceding negativity; SPN-C, combined SPN; SPN-W, SPN following the win feedback; SPN-L, SPN following the lose feedback. Notes: *Shows the significant difference p<0.05; **Shows the significant difference p<0.01. |
For HC group, no significant correlation across any domains was found (all p > 0.05). In MDD group, however, the FRN-D was positively related to HAMD scores (r = 0.392, p = 0.020), while SPN-L showed a positive correlation with the TEPS-CON score (r = 0.357, p = 0.035), suggesting a different clinical correlates for FRN and SPN. More importantly, the amplitude of SPN-C was positively correlated with both FRN-W (r = 0.376, p = 0.026) and FRN-L (r = 0.355, p = 0.037), and subtype analysis of SPN indicated that these correlations might be primarily influenced by SPN-L. Furthermore, although not reaching the threshold of significance, the correlation direction between SPN-L and FRN-D was opposite to that in the HC group (r = −0.18 vs r = 0.20).
Discussion
The significance of anhedonia in the context of MDD is indisputable, yet the intricate nature of its characteristics and underlying neural mechanisms remains enigmatic despite considerable research endeavors. By investigating the FRN and SPN within a same framework, in conjunction with the TEPS questionnaire, our study has yielded compelling evidence regarding the co-occurrence of anhedonia in both consumptive and anticipatory domains among those with MDD. Furthermore, our results indicated positive correlations between specific metrics of FRN and SPN exclusively within the MDD group. This correlation pattern was absent in the control group, potentially suggesting an impaired neural dissociation between reward feedback and anticipation mechanisms among individuals affected by MDD.
Compared to the healthy control group, our study revealed significantly lower scores within the MDD group in both the TEPS-CON and TEPS-ANT domains, along with reductions in the amplitudes of both the FRN and SPN. This convergence of findings lends support that individuals with MDD encompassing anhedonia in both consumption and anticipation.14 This could potentially hold clinical value, particularly in distinguishing MDD from conditions like schizophrenia, as prior research has indicated that individuals with schizophrenia predominantly manifest anhedonia during the anticipation phase.34,35 Interestingly, our data did not show evident correlations between the ERP metrics and any of the TEPS domains in either the HC or MDD groups. This suggests that the interplay between neural responses reflected by ERP components and the self-reported experiences of pleasure and anticipation, as captured by the TEPS questionnaire, may not follow a straightforward linear relationship. In conjunction with previously divergent findings in this area,36,37 our discovery underscores the intricate complexity of anhedonia. Longitudinal investigations are essential to elucidate the most predictive indicators for MDD occurrence, clinical response, risk of recurrence, or overall prognosis.
In contrast to the HC group, the MDD group exhibited more negative amplitudes for both FRN-L and FRN-W. Moreover, the amplitude of FRN-D positively correlated with the HAMD score, suggesting a potential connection between the severity of clinical symptoms and the degree of anhedonia impairment. These findings align with prior researches38–40 and the prevailing concept that the negative deflection of FRN is elicited by feedback stimuli linked to unfavorable outcomes, with its amplitude influenced by top-down processes such as interest and motivation levels.41 The monetary feedback amount did not appear to hold as much significance in our study as the valence of the feedback. This finding is consistent with previous research indicating that the amplitude of the FRN is primarily influenced by the valence of rewards and punishments, rather than their magnitudes.42 However, it should be note that there is also report suggesting that variations in rewards can impact the amplitude of the FRN.43 Difference in task designs, participant characteristics, or experimental conditions may contribute to the diverse findings across studies, highlighting a need for further investigation and replication to establish more robust conclusions. As for the SPN, our study revealed consistently lower amplitudes among individuals with MDD, regardless of whether they received a gain or loss feedback in the preceding trial. This finding is also in agreement with previous reports, reinforcing the notion of altered anticipatory neural processes in MDD.14,32,44 Of note, intriguingly, a preceding win feedback exhibited the ability to enhance the SPN in both groups, and this effect remained unaffected by consecutive gains. This implies that individuals with MDD may retain the capacity, to some extent, for heightened anticipatory neural processes. Furthermore, this finding may potentially unveil a novel avenue for interventions to enhance positive anticipation and alleviate anhedonic symptoms in MDD individuals.
The relationship between FRN and SPN continues to be a noteworthy area of investigation lacking a definitive consensus. Some of previous studies pertaining to healthy individuals suggested a negative correlation between them,17,18 while others failed to find any correlations.19,20 Significantly, our study yielded intriguing outcomes: no substantial correlation between FRN and SPN was found in the HC group, suggesting independence in the underlying neural processes or functioning. However, the MDD group exhibited positive correlations between these ERP components, particularly evident in the connections between FRN-W and FRN-L with SPN-L. Given that SPN and FRN are believed to capture distinct aspects of anhedonia and different stages of reward processing, this alteration suggests that the neural process or functional independence typically maintained in healthy individuals may be compromised in individuals with MDD. The heightened correlations between FRN and SPN in MDD may also indicate a shared impairment in both reward feedback processing and anticipatory neural mechanisms. Neuroimaging studies and source analysis have revealed distinct yet overlapping neural circuits involved in FRN and SPN. The FRN primarily involves the anterior cingulate cortex (ACC), a brain region associated with error detection, conflict monitoring, and emotional processing. Additionally, it is interconnected with other areas such as the ventral striatum (involved in reward processing) and the amygdala (associated with emotional responses).45,46 The major neural generator of the SPN is believed to be the anterior insula,7 which is functionally interconnected with the ACC. They often work together as part of the salience network. Additionally, both the FRN and SPN are influenced by the mesolimbic dopamine system,47 which plays a crucial role in reward processing and motivation. Accordingly, it is understandable that a functioning brain is capable of finely regulating two similar but not identical functions, whereas individuals with MDD are vulnerable to have simultaneous impairments.
Several limitations of this study should be acknowledgment. Firstly, the size of our participant sample and the range of severity among MDD patients were relatively modest. Expanding our study to encompass a broader spectrum of MDD subgroups could potentially enhance the generalizability and applicability of our findings to a wider population. Moreover, it’s important to recognize that the potential effects of medications and other treatments on the observed ERPs in MDD patients were not thoroughly examined in our current study. Investigating treatment-naïve individuals or exploring the specific impact of different treatment modalities on the ERP characteristics could yield a more comprehensive understanding of the neural mechanisms involved. Additionally, while the 2-door task has been widely utilized as a paradigm to investigate anhedonia and reward processing, it’s worth noting that several participants in our study reported finding it somewhat monotonous and challenging to engage with. Future refinements are needed to address this concern and better replicate real-world reward processing situations.
Conclusion
Despite its limitations, our study provides valuable insights into the abnormalities of anhedonia and underlying neural processing in MDD. The concurrent deficits in FRN and SPN, along with correlations across ERP components and between them and clinical factors—especially the distinct interplay pattern of FRN and SPN observed in MDD compared to the HC group—shed light on the intricate underlying neural mechanisms, and may inform the development of targeted interventions for addressing anhedonia and related deficits.
Acknowledgments
We are grateful to everyone who generously participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study is supported by the Medical Research Project of Jiangsu Province Health Commission (M2020078), Wuxi Municipal Health Commission Major Project (No. 202107) and the Key project of precision medicine of Wuxi Health Commission (J202008).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Der-avakian A, Markou A. The neurobiology of anhedonia and other reward-related deficits. Trends Neurosci. 2012;35(1):68–77.
2. Pizzagalli DA, Iosifescu D, Hallett LA, Ratner KG, Fava M. Reduced hedonic capacity in major depressive disorder: evidence from a probabilistic reward task. J Psychiatr Res. 2008;43(1):76–87. doi:10.1016/j.jpsychires.2008.03.001
3. Treadway MT, Buckholtz JW, Schwartzman AN, Lambert WE, Zald DH, García AV. Worth the ‘EEfRT’? The effort expenditure for rewards task as an objective measure of motivation and anhedonia. PLoS One. 2009;4(8):e6598. doi:10.1371/journal.pone.0006598
4. Mueller EM, Pechtel P, Cohen AL, Douglas SR, Pizzagalli DA. Potentiated processing of negative feedback in depression is attenuated by anhedonia. Depress Anxiety. 2015;32(4):296–305. doi:10.1002/da.22338
5. Miltner WH, Braun CH, Coles MG. Event-related brain potentials following incorrect feedback in a time-estimation task: evidence for a “generic” neural system for error detection. J Cogn Neurosci. 1997;9(6):788–798. doi:10.1162/jocn.1997.9.6.788
6. Keren H, O’Callaghan G, Vidal-Ribas P, et al. Reward processing in depression: a conceptual and meta-analytic review across fMRI and EEG studies. Am J Psychiatry. 2018;175(11):1111–1120. doi:10.1176/appi.ajp.2018.17101124
7. Chen Y, Xu J, Zhou L, Zheng Y. The time course of incentive processing in anticipatory and consummatory anhedonia. J Affect Disord. 2018;238:442–450. doi:10.1016/j.jad.2018.05.053
8. Van Boxtel GJM, Böcker KBE. Cortical measures of anticipation. J Psychophysiol. 2004;18(2/3):61–76. doi:10.1027/0269-8803.18.23.61
9. Brunia CH. Movement and stimulus preceding negativity. Biol Psychol. 1988;26(1–3):165–178. doi:10.1016/0301-0511(88)90018-X
10. Proudfit GH. The reward positivity: from basic research on reward to a biomarker for depression. Psychophysiology. 2015;52(4):449–459. doi:10.1111/psyp.12370
11. Holroyd CB, Pakzad-Vaezi KL, Krigolson OE. The feedback correct-related positivity: sensitivity of the event-related brain potential to unexpected positive feedback. Psychophysiology. 2008;45(5):688–697. doi:10.1111/j.1469-8986.2008.00668.x
12. Brush CJ, Ehmann PJ, Hajcak G, Selby EA, Alderman BL. Using multilevel modeling to examine blunted neural responses to reward in major depression. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3(12):1032–1039. doi:10.1016/j.bpsc.2018.04.003
13. Klawohn J, Burani K, Bruchnak A, Santopetro N, Hajcak G. Reduced neural response to reward and pleasant pictures independently relate to depression. Psychol Med. 2021;51(5):741–749. doi:10.1017/S0033291719003659
14. Luckhardt C, Mühlherr AM, Schütz M, et al. Reward processing in adolescents with social phobia and depression. Clin Neurophysiol. 2023;150:205–215. doi:10.1016/j.clinph.2023.03.356
15. Tucker DM, Luu P, Frishkoff G, Quiring J, Poulsen C. Frontolimbic response to negative feedback in clinical depression. J Abnorm Psychol. 2003;112(4):667–678. doi:10.1037/0021-843X.112.4.667
16. Umemoto A, Holroyd CB. Neural mechanisms of reward processing associated with depression-related personality traits. Clin Neurophysiol. 2017;128(7):1184–1196. doi:10.1016/j.clinph.2017.03.049
17. Zheng Y, Li Q, Zhang Y, et al. Reward processing in gain versus loss context: an ERP study. Psychophysiology. 2017;54(7):1040–1053. doi:10.1111/psyp.12855
18. Morís J, Luque D, Rodríguez-Fornells A. Learning-induced modulations of the stimulus-preceding negativity. Psychophysiology. 2013;50(9):931–939. doi:10.1111/psyp.12073
19. Novak BK, Novak KD, Lynam DR, Foti D. Individual differences in the time course of reward processing: stage-specific links with depression and impulsivity. Biol Psychol. 2016;119:79–90. doi:10.1016/j.biopsycho.2016.07.008
20. Fuentemilla L, Cucurell D, Marco-Pallarés J, Guitart-Masip M, Morís J, Rodríguez-Fornells A. Electrophysiological correlates of anticipating improbable but desired events. Neuroimage. 2013;78:135–144. doi:10.1016/j.neuroimage.2013.03.062
21. Abram SV, Roach BJ, Holroyd CB, et al. Reward processing electrophysiology in schizophrenia: effects of age and illness phase. Neuroimage Clin. 2020;28:102492. doi:10.1016/j.nicl.2020.102492
22. Si TM, Shu L, Dang WM, et al. Evaluation of the reliability and validity of Chinese version of the mini international neuropsychiatric interview in patients with mental disorders. Chin Ment Health J. 2009;23:493–503. Chinese.
23. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
24. Sun XY, Li YX, Yu CQ, Li LM. Reliability and validity of depression scales of Chinese version: a systematic review. Zhonghua Liu Xing Bing Xue Za Zhi. 2017;38(1):110–116. doi:10.3760/cma.j.issn.0254-6450.2017.01.021
25. Zheng YP, Zhao JP, Phillips M, et al. Validity and reliability of the Chinese Hamilton depression rating scale. Br J Psychiatry. 1988;152:660–664. doi:10.1192/bjp.152.5.660
26. Ma HY, Wang XM, Huang XJ, et al. Psychometric properties of the Chinese version of the clinically useful depression outcome scale for patients with major depressive disorder. Neuropsychiatr Dis Treat. 2021;17:2387–2395. doi:10.2147/NDT.S307662
27. Zhou H, Liu W, Fan J, Xia J, Zhu J, Zhu X. The Temporal Experience of Pleasure Scale (TEPS): measurement invariance across gender in Chinese university students. Front Psychol. 2019;10:2130. doi:10.3389/fpsyg.2019.02130
28. Chan RC, Shi YF, Lai MK, Wang YN, Wang Y, Kring AM. The Temporal Experience of Pleasure Scale (TEPS): exploration and confirmation of factor structure in a healthy Chinese sample. PLoS One. 2012;7(4):e35352. doi:10.1371/journal.pone.0035352
29. Wang X, Wu H, Huang J, et al. Reward mechanism of depressive episodes in bipolar disorder: enhanced theta power in feedback-related negativity. J Affect Disord. 2021;292:217–222. doi:10.1016/j.jad.2021.05.057
30. Yu L, Wu Z, Wang D, et al. Increased cortical structural covariance correlates with anhedonia in schizophrenia. Schizophrenia. 2023;9(1):19. doi:10.1038/s41537-023-00350-3
31. Balasubramani PP, Diaz-Delgado J, Grennan G, et al. Distinct neural activations correlate with maximization of reward magnitude versus frequency. Cereb Cortex. 2023;33(10):6038–6050. doi:10.1093/cercor/bhac482
32. Zheng Y, Li Q, Wang K, Wu H, Liu X. Contextual valence modulates the neural dynamics of risk processing. Psychophysiology. 2015;52(7):895–904. doi:10.1111/psyp.12415
33. Kamei M, Kotani Y, Sakuma H. Preparing for saliencies: emotional expectations under probabilistically and aversively salient situations. Psychophysiology. 2018;55(6):e13056. doi:10.1111/psyp.13056
34. Wolf DH. Anhedonia in schizophrenia. Curr Psychiatry Rep. 2006;8(4):322–328. doi:10.1007/s11920-006-0069-0
35. Kring AM, Moran EK. Emotional response deficits in schizophrenia: insights from affective science. Schizophr Bull. 2008;34(5):819–834. doi:10.1093/schbul/sbn071
36. Klumpp H, Bauer BW, Glazer J, et al. Neural responsiveness to reward and suicidal ideation in social anxiety and major depression before and after psychotherapy. Biol Psychol. 2023;178:108520. doi:10.1016/j.biopsycho.2023.108520
37. Liu WH, Wang LZ, Shang HR, et al. The influence of anhedonia on feedback negativity in major depressive disorder. Neuropsychologia. 2014;53:213–220. doi:10.1016/j.neuropsychologia.2013.11.023
38. O’Callaghan G, Stringaris A. Reward processing in adolescent depression across neuroimaging modalities. Z Kinder Jugendpsychiatr Psychother. 2019;47(6):535–541. doi:10.1024/1422-4917/a000663
39. Bress JN, Meyer A, Hajcak G. Differentiating anxiety and depression in children and adolescents: evidence from event-related brain potentials. J Clin Child Adolesc Psychol. 2015;44(2):238–249. doi:10.1080/15374416.2013.814544
40. Foti D, Hajcak G. Depression and reduced sensitivity to non-rewards versus rewards: evidence from event-related potentials. Biol Psychol. 2009;81(1):1–8. doi:10.1016/j.biopsycho.2008.12.004
41. Yeung N, Holroyd CB, Cohen JD. ERP correlates of feedback and reward processing in the presence and absence of response choice. Cereb Cortex. 2005;15(5):535–544. doi:10.1093/cercor/bhh153
42. Yeung N, Sanfey AG. Independent coding of reward magnitude and valence in the human brain. J Neurosci. 2004;24(28):6258–6264. doi:10.1523/JNEUROSCI.4537-03.2004
43. Zottoli TM, Grose-Fifer J. The feedback-related negativity (FRN) in adolescents. Psychophysiology. 2012;49(3):413–420. doi:10.1111/j.1469-8986.2011.01312.x
44. Ohgami Y, Kotani Y, Tsukamoto T, et al. Effects of monetary reward and punishment on stimulus-preceding negativity. Psychophysiology. 2006;43(3):227–236. doi:10.1111/j.1469-8986.2006.00396.x
45. Foti D, Weinberg A, Dien J, Hajcak G. Event-related potential activity in the basal ganglia differentiates rewards from nonrewards: temporospatial principal components analysis and source localization of the feedback negativity. Hum Brain Mapp. 2011;32(12):2207–2216. doi:10.1002/hbm.21182
46. Becker MP, Nitsch AM, Miltner WH, Straube T. A single-trial estimation of the feedback-related negativity and its relation to BOLD responses in a time-estimation task. J Neurosci. 2014;34(8):3005–3012. doi:10.1523/JNEUROSCI.3684-13.2014
47. Mattox ST, Valle-Inclán F, Hackley SA. Psychophysiological evidence for impaired reward anticipation in Parkinson’s disease. Clin Neurophysiol. 2006;117(10):2144–2153. doi:10.1016/j.clinph.2006.05.026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.