Back to Journals » International Journal of General Medicine » Volume 16
Neonatal Seizure Pattern, Outcome, and its Predictors Among Neonates Admitted to NICU of Ayder Comprehensive Specialized Hospital, Mekelle, Tigray, Ethiopia
Authors Weldegerima K, Gebremariam DS ![]() , Haftu H
, Haftu H ![]() , Berhe G
, Berhe G ![]() , Hadgu A, Mohammedamin MM
, Hadgu A, Mohammedamin MM
Received 29 May 2023
Accepted for publication 16 September 2023
Published 25 September 2023 Volume 2023:16 Pages 4343—4355
DOI https://doi.org/10.2147/IJGM.S414420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Kiros Weldegerima,1 Dawit Seyoum Gebremariam,1 Hansa Haftu,1 Gebretsadik Berhe,2 Amanuel Hadgu,1 Mohammed Mustefa Mohammedamin1
1Mekelle University, College of Health Sciences, School of Medicine, Department of Pediatrics and Child Health, Mekelle, Ethiopia; 2Mekelle University, College of Health Sciences, School of Public Health, Department of Epidemiology, Mekelle, Ethiopia
Correspondence: Dawit Seyoum Gebremariam, Mekelle University, College of Health Sciences, School of Medicine, Department of Pediatrics and Child Health, P.O.Box 1871, Mekelle, Ethiopia, Tel +251011731454, Email [email protected]
Background: Seizure is the most frequently observed symptom of neurological disorders and an important determinant of outcome during neonatal period. In clinical practice, it is prevalent and observed in neonates admitted to hospital in low-resources countries, but due to the paucity of studies in these regions, little is known about its pattern, clinical outcomes of hospitalization, and its predictors. Therefore, aims to evaluate seizure patterns, clinical outcomes, and its predictors among neonates admitted to the NICU of ACSH, Mekelle, and Tigray.
Methods: A hospital-based cross-sectional study design was conducted among neonates with neonatal seizures admitted to NICU of Ayder Comprehensive Specialized Hospital. Data collection was done from record reviews. SPSS Version 25 was used. Descriptive statistics and bivariate logistic regressions where a p-value of < 0.05 is considered statistically significant.
Results: Out of 1622 NICU admissions, 155 (9.6%) were cases of neonatal seizure. The most frequently observed types of seizure in this study were subtle 70 (45.1%) and tonic 49 (31.6%) respectively. At the end of hospitalization 70.3% of neonates were discharged improved, 21.3% of neonates died and 8.4% of neonates had severe neurologic deficits. Poorly controlled seizures (AOR 4.8, 95% CI 2.6– 9.2), prolonged duration of labor (AOR 4.3, 95% CI 2.2– 8.8) and seizure onset < 72 hours (AOR 3.7, 95% CI 1.6– 8.5), respectively, were found to be independent predictors of poor neonatal outcome.
Conclusion: Of all neonatal admissions, neonatal seizure was observed in close to 9.6%. The most frequently observed type of seizure was subtle. Of those admitted neonates, 30% had poor outcomes following the end of their hospitalization or when they leave against medical advice for lack of improvement). Poorly controlled seizures, prolonged duration of labor, and seizure onset < 72 hours were independent predictors of poor neonatal outcomes.
Keywords: neonatal seizure, pattern, outcome, predictors
Introduction
Of all neurological disorders, seizures are most common neonatal emergency and have specific clinical manifestations. Seizures can cause injury and compound existing brain damage.1,2 Neonatal physiological hyper-excitability and a connected vulnerability to seizure are explained by a high level of synaptogenesis and neural plasticity in new-borns.2,3 Neonatal seizures are usually an acute manifestation of disturbance of the developing brain and are common in the early weeks of life.4,5 Despite the prevalence of neonatal seizures admitted to hospitals in Africa, few studies have conducted about the patterns, outcomes of treatments, and their predictors.6 Neonatal encephalopathy, neonatal sepsis, and premature births in developing countries suggest that the burden may be much higher than the study conducted at a hospital in rural Kenya demonstrated; seizures were documented in 9% of neonatal admissions.6
Because of the arborization of axons and dendritic processes and incomplete myelination, generalized tonic-clonic convulsions do not occur in neonates. Thus, dissimilar to child and adult seizures, the most frequent seizures observed in neonates are focal, multifocal, clonic, tonic, myoclonic, and subtle seizure.3,4,7
Subtle seizure is more common in term babies, particularly with severe global insult, and the incidence range from 10% to 35%. The Clonic type comprises 50% of all neonatal seizures, it is more common in term babies and consciousness is usually preserved. The other is tonic seizure, which comprises 20% and is more common in pre-term babies. The myoclonic type comprises 5% of all neonatal seizures.8
A hospital-based descriptive study on the incidence and etiology of neonatal seizures conducted in Pakistan showed that the common type of seizures reported in the study were subtle (39.6%) and tonic (31.4%) subsequently clonic and myoclonic were 25.10% and 3.7% respectively.9 Another prospective study conducted in India on Clinico-etiological profile and outcome of neonatal seizure showed the most common type of neonatal seizure was subtle, 95 (63.33%) followed by generalized tonic, 29 (19.33%), and multifocal clonic, 15 (10%)10 A similar study done in Nigeria showed that 71.2% had both subtle and generalized seizure.11
Diagnosis of neonatal seizure is difficult due to lack of access to top-of-the-line diagnostic tools like video EEG. Where access is available, accuracy of results vary due to observer skills and training. Other diagnostic tools like computed tomography and magnetic resonance imaging (MRI) are not sufficiently accurate. Thus, clinician-based observation of the semiology of seizure remains the backbone of the diagnosis of neonatal seizure.10–13
Over the past 20 years, there have been medical advancements leading to an improved global medical health. However, neonatal seizure remains a frequent phenomenon. Neonatal seizures can lead to increased risk of neurological sequelae, i.e., developmental delay, epilepsy, and cognitive impairment as well as even mortality.13
A 4-year prospective cohort study on incidence, etiology, and outcome of neonatal seizures in Kenyan district hospitals showed out of 142 neonates with seizures the immediate outcomes while being discharged from the hospital were 96 (67.6%) neonates discharged with improvement, 32 (22.5%) of neonates died and 14 (9.8%) of neonates had an abnormal neurologic examination.6 Another hospital-based prospective observational cohort study conducted at University of Gondar Hospital, Ethiopia, on etiology, clinical features, and short-term outcome of seizures in new-borns reported that 19.7% mortality rate and a 10.6% neurologic sequelae out of 117 enrolled neonates. Among the surviving neonates, motor deficits, spasticity and decreased level of consciousness were observed at the time of discharge.14
Planning a robust and long-term health assistance for affected children can be supported through a mapping of risk factors which can facilitate the prediction of outcomes. As documented in Dongol et al, several prognostic factors for the adverse outcome of a seizure are well known, namely brain immaturity, abnormal cranial ultrasonography (US) findings, low Apgar score, early onset of a seizure, prolonged duration of seizure, the underlying etiology of the convulsion, response to treatment as well as the extent of cerebral insult. Early-onset seizures, asphyxia-induced, and poorly controlled seizures appear to have the worst prognosis.15
Many studies have been published in different countries. However, there is a dearth of papers in Ethiopia focusing in patterns, outcomes of hospitalization and predictors of poor outcomes in new-borns with seizures.
Methods
Study Area and Period
Ayder Comprehensive Specialized Hospital (ACSH) is a teaching referral hospital found in Mekelle city in Tigray region, Northern Ethiopia. ACSH Neonatal intensive care unit (NICU) gives intensive care services for inpatient neonates (intensive care and KMC) and outpatient services such as neonatal emergency OPD evaluations and follow-up clinic evaluation and monitoring for high-risk neonates. The study was conducted from March 2020 to July 2020 in the inpatient admitted neonates.
Study Design
A hospital-based cross-sectional study design was conducted in Ayder Comprehensive Specialized Hospital.
Study Population
The study population includes all neonates with seizures who were admitted to the neonatal intensive care unit of Ayder Comprehensive Specialized Hospital from September 1, 2018, to August 30, 2019.
Target Population
All neonates with seizures who were admitted to the neonatal intensive care unit of ACSH stayed for more than 24 hours.
Sample Size Determination
The sample size was calculated using the population proportion formula from the Mwaniki et al's study (9) done in a Kenyan district hospital which showed seizures were reported in 142 out of 1572 neonatal admissions, i.e., 9%, hence n = p (1-p) z2/d2, n = 126. Considering an increase in our sample size and for proper representations of our source population, all neonatal admissions with a seizure during the one-year study period, i.e., 155 neonates were included in the study.
Data Collection Tools and Procedures
Data Collection Methods
The data abstraction format was developed locally using the record review technique from patient chart reviews. The data was filled in by a trained data collector. The questionnaire was pretested for and modified before the actual data collection.
Sampling Procedure While Starting Data Collection
During the year 2018/2019, a total of 1694 neonatal admissions were found registered in the NICU registration log book, and 1622 charts were retrieved and reviewed. The remaining 72 charts were not found for different reasons. A total of 155 charts with a diagnosis of neonatal seizure were included in the study.
Data Quality Assurance
The authors undertook several steps to ensure the quality of data. Locally developed data abstraction instrument was prepared by record review technique. This data abstraction instrument was pretested in 5% of the retrieved charts. Furthermore, the principal investigator reviewed the questionnaires for completeness and to make sure the information collected makes sense.
Data Processing and Analysis
Data coding, cleaning, and editing were completed. IBM SPSS version 25 was used to perform descriptive and statistical analysis and bivariate logistic regression to determine neonatal seizure patterns, the short-term clinical outcomes of hospitalization, and its predictors for poor neonatal outcomes.
Results
Socio-Demographic Data Results
Out of 155 neonates with seizures enrolled in the study, 84 were male and 71 were females. The majority of study participants (80.6%) were term babies and the remaining 18.1 and 1.3% were pre-term and post-term deliveries respectively (Table 1).
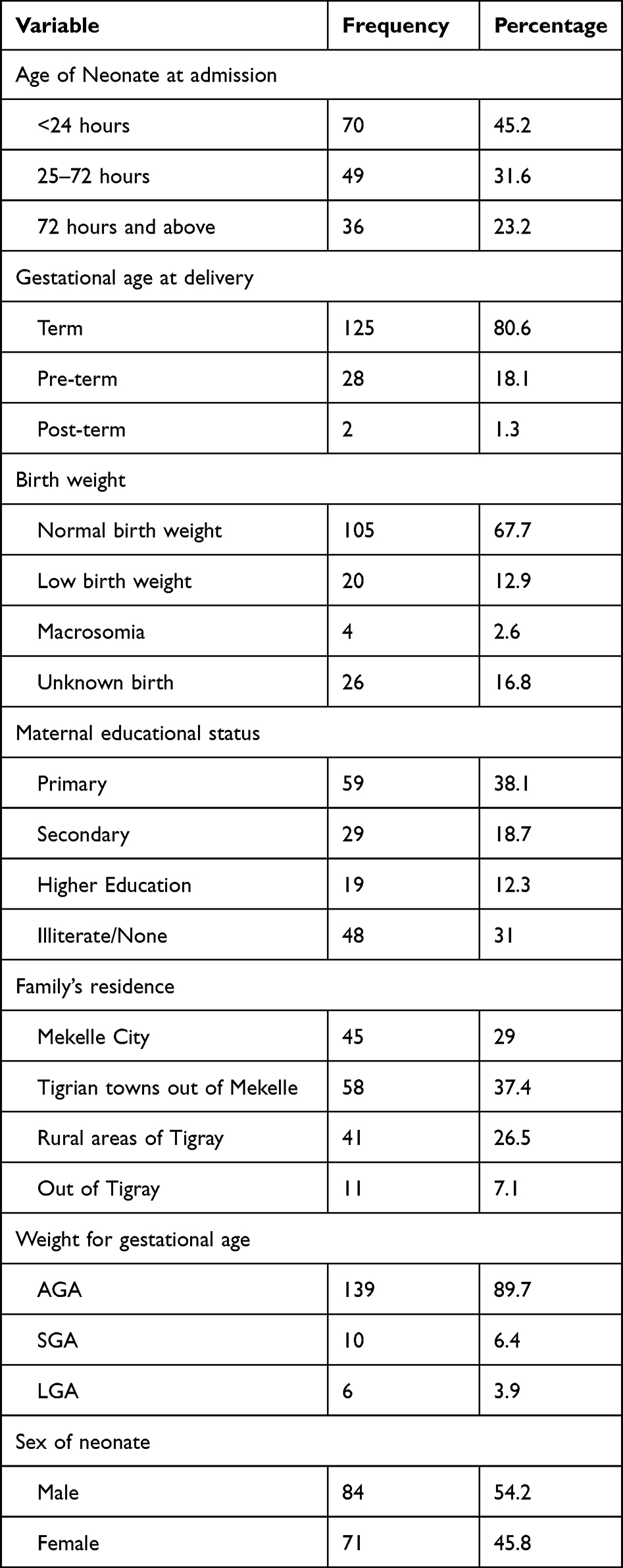 |
Table 1 Socio-Demographic Characteristics of Neonates with Seizure and Their Parents in ACSH, 2018/2019 |
Perinatal Conditions of Mothers and Neonates with Neonatal Seizure
The perinatal condition findings of this study revealed that 16 to 21% of neonates were delivered from mothers with morbidity during pregnancy, these include 21% of neonates delivered from mothers with pregnancy-induced hypertension, 19% of neonates delivered from mothers with fever and 16% of neonates were delivered from mothers with offensive vaginal discharge. Other perinatal conditions in this study include delayed cry after delivery, prolonged labor, low APGAR score, and neonatal jaundice were present in 42.6%, 35.5%, 34.9%, and 23.2%, respectively (Table 2).
 |
Table 2 Perinatal Characteristics of Neonates with Seizure and Their Mothers in ACSH, 2018/2019 |
Laboratory and Clinical Findings/Measurements in Neonates with Seizure
The common laboratory evaluations done in neonates with seizures include CSF analysis, brain imaging, CBC, random blood sugar, and serum electrolytes. Almost in all of them, CBC was done and the result shows normal in 59.4%, sepsis in 34.2%, and anemia in 6.5% of neonates. CSF analysis was performed in 86.5% of neonates and the results showed Normal in 102(65.8%), meningitis in 22 (14.2%), and traumatic in 10 (6.5%) of neonates. Brain scanning was done similarly in 86.5% of neonates with seizure and the commonest abnormality detected was intracranial hemorrhage (12.3%) followed by hydrocephalus and subdural effusions 15 (9.7%). Congenital CNS malformations were detected in 3(1.9%) neonates only. Hypoglycemia was detected in 13 (8.4%) of neonates only, in the majority of them (85.2%) the random blood sugar was within the normal range (Table 3).
 |
Table 3 Clinical and Laboratory Characteristics Findings of Neonates with Seizure |
Patterns of Neonatal Seizure
Out of 1622 NICU admissions, there were 155(9.6%) cases with neonatal seizure, Based on the time onset, 108 (69.7%) new-borns experienced their first seizure onset within 72 hours of birth, and 47 (30.3%) had seizure onset after 72 hours of age. The majority of neonates (116; 74.8%) had multiple episodes of seizures compared with those having single episodes (39; 25.2%). (Table 4)
 |
Table 4 Shows Patterns, Episodes of Attacks, Time Onset, Treatment and Outcome Related Findings of Neonatal Seizure in ACSH, 2018/2019 |
In this study the most frequently observed type of seizure was subtle (70; 45.1%), insuingly tonic seizure (49; 31.6%) and the least type of seizure is myoclonic. (Table 4)
Clinical Outcome of Neonates with a Seizure at the End of Hospitalization
The clinical outcomes of admitted neonates with a seizure at the end of their hospitalization were; 109 (70.3%) neonates discharged improved, 33 (21.3%) neonates died, 13 (8.4%) neonates were discharged with severe neurological deficits with palliative care to be continued at nearby health institutions and left against medical advice due to lack of improvement (Figure 1).
 |
Figure 1 Clinical outcome of neonates with a seizure at the end of hospitalization in ACSH, 2018/2019. |
In this study all neonates with seizures started anticonvulsant therapy. Phenobarbitone was the most common prescribed and used drug (106; 68.4%). The seizure was controlled with one, two, and three drugs in 86, 54, and 13 neonates respectively. Well controlled seizures were seen in 113 neonates and the rest (43) neonates were poorly controlled (Table 4).
Predictors of Poor Outcome in Neonates with Seizure
Predictors of poor neonatal outcomes among neonates with seizures admitted to NICU were identified by conducting binary logistic regression. Three (poorly controlled seizure, prolonged duration of labor, and the onset of seizure <72 hours) variables were identified as independent predictors of poor neonatal outcome. The odds of poor outcomes were 4.3 times higher among neonates with seizures delivered during a prolonged labor (>24 hours) compared to those with a normal duration of labor (<24 hours), with an adjusted odds ratio of 4.3 (95% CI 2.2–8.8) and a P value of 0.003. The odds of poor outcomes were 4.8 times higher among neonates whose seizures were poorly controlled or refractory compared to those similar neonates with well-controlled seizures after treatments, with an adjusted odds ratio of 4.8 (95% CI 2.6–9.2) and a P value of 0.001. The odds of poor outcome were also 3.7 times higher among neonates with early onset seizures (<72 hours) compared to those with late onset of seizure (>72 hours), with an adjusted odds ratio of 3.7 (95% CI 1.6–8.5) and a P value of 0.007 (Table 5).
 |
Table 5 Shows Predictors of Poor Neonatal Outcome Among Neonates with Seizure n = 155 |
Discussion
Our study found that the burden of neonatal seizures was 9.6% of neonatal admissions, which is comparable to the finding of Shah et al's study (9.95%)9 and Mwaniki et al's study (9%)6 but slightly lower than the results of Dongol Singh et al's study (12.26%)15 and Sudia et al's study (11.7%).16 This low incidence can be because we were only able to document clinically obvious seizures and we did not practice diagnostic EEG recording for neonates who are at risk of seizure which possibly subclinical seizures can be missed.
In our study we found that 80.6% of neonates with seizures were term babies, this was comparable with Amare et al's study (81%)17 and Alyasiri et al's study (91%).7 The most likely explanation for this is due to the most common comorbidity in the above studies being perinatal asphyxia which is usually most common in full terms babies, rather than pre-term. In our study it was also found that; 69.7% of new-borns had an early-onset seizure which occurs before 72 hours. This finding is comparable to the findings in the study by Shah et al,9 Rastogi et al's study (66.67%),4 Dongol Singh et al's study (70.9%),15 and Baudou et al's study (78%).18 The explanation is as perinatal asphyxia is the most common comorbidity in those studies and seizures in perinatal asphyxia are usually early onset.
In this study, subtle and tonic seizure were the two most common types of seizure which accounts 45.1% and 31.6%, respectively. Comparable results were reported by Shah et al's study which was 39.6% by subtle and 31.4% by tonic types seizure,9 Sudia et al's study was subtle (63.3%_, followed by tonic (19.3%),16 Alyasiri et al's study also showed subtle (37.3%), whereas tonic seizure account for 28.7%,7 and Lai et al's study was subtle (44%) followed by clonic (19.4%),14 but this was different from Nemati et al's study12 and Baudou et al's study18 that showed the clonic type of seizure was the most frequently observed type of seizure, 45.5% and 35%, respectively.
In our study the clinical outcomes of admitted neonates with a seizure at the end of their hospitalization were; 109 (70.3%) neonates improved and were discharged, 33 (21.3%) neonates died, and 13 (8.4%) neonates were discharged with severe neurological deficits. This was comparable to Mwaniki et al's study, a 4 year prospective cohort study on the incidence, etiology, and outcome of neonatal seizure in Kenyan district hospitals which showed out of 142 neonates with seizures, the immediate outcomes while being discharged from hospital were 96 (67.6%) neonates discharged with improvement, 32 (22.5%) of neonates died and 14 (9.8%) of neonates had an abnormal neurologic exam, but the follow-up surveillance which revealed another 16 neonates died and 23 developed epilepsy and developmental delay did not go with our study as our study has no follow-ups.6 Similarly the outcomes of neonates with seizure in other studies, like Amare et al, showed that 84 (71.8%) were alive with no sequelae, 23 (19.6%) were dead, and 10 (8.6%) had sequelae.17 Alyasiri et al's study showed that 69 (56.6%) of neonates were discharged with no complications, 32 (26.2%) had sequelae of nervous system, and 21 (17.2%) of them had died.9 Both of this studies were comparable to our study. But when our study is compared with Sudia et al's study, 80 (53.33%) neonates had completely recovered, 27.34% (41) and 19.33% (29) neonates were discharged with complications and expired respectively.16 The deaths are comparable at 21.3% vs. 19.33% while the neonates who were discharged improved higher in our study at 70.3% vs. 53.33% this might be likely due to the presence of follow-up conditions for 6 months after discharge and adding up those who developed complications later after discharge in the study by Sudia et al, compared to our retrospective study for which we do not have follow-ups after discharge. Similarly, those who were discharged with sequela were 13 (8.4%) in our study and 41 (27.34%) in Sudia et al's study, which is lower due to the later development of sequela in the follow-up time of 6 months after discharge which was present in Sudia et al's study, compared to our study that has no follow up time after discharge.
In our study, the predictors of adverse/poor neonatal outcomes were the presence of prolonged labor, jaundice, and early onset of seizures (<72 hours). Similar studies were described by Lai et al, Dongol Singh et al and Laurel et al regarding early onset seizure and prolonged labor as predictors of poor neonatal outcomes but jaundice was not found to be a predictor of poor outcome in those studies.15,17,19 This could be due to the number of patients with seizures who had also jaundice, in our study neonates with seizures who were also jaundiced at presentation were 36 (23.2%) of all neonates with seizures (Table 2), but in Dongol Singh et al and Hsuan lai et al studies, none of the neonates involved in the study had jaundice at presentation or during a hospital stay.
WHO guidelines on neonatal seizure treatment options (strongly) recommended phenobarbital as the preferred option of treatment of neonatal seizures.20 Our study and other similar studies, for example,Aggarwal et al,21 also shows phenobarbital is the most common used Anti-Epileptic Drug (AED) for treating neonatal seizure but Laurel et al described that phenobarbital and phenytoin were equally effective to control neonatal seizures.19
Recommendations
The major underlying etiologies with neonatal seizures and the deaths and neurological deficits ascribed are certainly preventable, hence exhaustive and efficient efforts are important to achieve optimal prenatal, natal and postnatal services, safe delivery to prevent birth asphyxia, and to address essential care and improve transportation of sick new-borns at different levels of care for early treatment and achievement of better outcomes. We recommend conducting a prospective study, and to assess their long-term neurodevelopmental outcome to devise effective further treatment plans.
Limitations of the Study
Since neonatal seizures are frequently subclinical, EEG recording of electrographic seizures in high-risk neonates is critical for the assessment of true seizures; our study did not perform EEG for high-risk neonates due to the study being retrospective.
Conclusion
Of all neonatal admissions, neonatal seizure was found in 9.6% and the frequent type of seizure observed is subtle type. Thirty percent of neonates with seizures admitted to the Neonatal Intensive Care Unit (NICU) had poor outcomes at the end of their hospitalization (death, severe neurologic deficit at discharge, or when they leave against medical advice for lack of improvement). Poorly controlled seizures, prolonged duration of labor, and seizure onset <72 hours were independent predictors of poor neonatal outcomes.
Operational Definitions
Clinical Seizure is defined as:-A sudden uncontrolled surge of electrical activity in the brain manifests as physical convulsion, autonomic changes, cognitive changes, or a combination of any of those symptoms diagnosed by a physician.
Poor outcome:- Neonates with a seizure that died or discharged/left against medical advice with severe neurologic deficit.
Incomplete documentation of history, physical examination, diagnosis, investigations, and treatments;- means missing any of the required history, physical examination, diagnosis, investigations, and treatments on the chart of a patient.
Birth asphyxia:- when a physician has diagnosed birth asphyxia and documented it or when there is documented history of evidence like low APGAR score or delayed cry after delivery, history of resuscitation, and presence of risk factors.
Bacterial meningitis:- when the neonate had documented diagnosis and treatment for meningitis by a physician with evidence from history, physical examination, and investigations with CSF analysis or imaging with Cranial US/MRI.
Low APGAR score;- when the immediate 1st minute of life evaluation condition of the neonate is less than 7 and requires resuscitation.
Poorly controlled seizure;-patients who have 2 or more seizure attack per week.
Abbreviations
ACSH, Ayder Comprehensive Specialized Hospital; NICU, Neonatal Intensive Care Unit; EEG, Electro Encephalo Gram; APGAR, Appearance, Pulse Grimace Activity Respiratory rate; CBC, Complete Blood Count; CSF, Cerebro Spinal Fluid; US, Ultra Sound; MRI, Magnetic Resonance Imaging; CT, Computed Tomography; KMC, kangaroo mother care; ICH, Intra Cranial Hemorrhage; SGA, small for gestational age; LGA, large for gestational age; AGA, appropriate for gestational age; HC, Head Circumference.
Data Sharing Statement
The data set can be made available based on the request to the corresponding author and Confidentiality of the data maintained safely.
Ethical Considerations
Ethical clearance was obtained from the Health Research Ethics Review Committee (HRERC) and Ethical Review Board of the College of Health Sciences of Mekelle University with MU-IRB reference number of 1640/2020. Permission from the dataset owner (Ayder Comprehensive Specialized Hospital clinical director’s offices) and a support letter from the chief clinical director were obtained before the commencement of the study. This study was conducted in line with “the Decleration of Helsinki”. Data were taken from patient records. Therefore, confidentiality of the data was kept safely and the data were only used for our current study. Patient consent was not needed for this retrospective chart review study as Mekelle University, College of Health Sciences: Ayder Comprehensive Specialized Hospital retains (right to own) the medical chart of the patients.
Acknowledgments
The authors are grateful to the authors, editors, and publishers of the articles that are cited and included in the references for this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pellegrin S, Munoz FM, Padula M, et al. Neonatal seizures: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Elsevier J Books. 2019;37. doi:10.1016/j.vaccine.2019.05.031
2. Kliegman RM, Geme JW. Nelson Textbook of Pediatrics.
3. Scher MS. Seizures in neonates. In: Martin RJ, Fanaroff AA, Walsh MC, editors. Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant.
4. Rostagi S, Lata Rai P, Prasad PL. Clinicoetiological profile of neonatal seizures in a tertiary care hospital. Indian J Child Health. 2017;4(4):587–590. doi:10.32677/IJCH.2017.v04.i04.029
5. Agrawal A. Neonatal Seizures review Indian. J Clin Pract. 2017;28:4.
6. Mwaniki M, Mathenge A, Gwer S, et al. Neonatal seizures in a rural Kenyan District Hospital: aetiology, Incidence and outcome of hospitalization. BMC Med. 2010;8(16). doi:10.1186/1741-7015-8-16
7. Alyasiri AA. Etiology and short outcome of neonatal seizures. Med Res Chron. 2015;2(1):30–40. doi:10.13140/RG.2.2.32000.84487
8. Fisher RS, Cross JH, D’Souza C, et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia. 2017;58(4):531–542. doi:10.1111/epi.13671
9. Shah FU, Jehanzeb M, Khan MA. Etiological study of seizures in neonates. Khyber Med Univ J. 2013;5(1):9–12.
10. Francisco P, Carlotta S. Neonatal seizure: a review of outcomes and outcome predictors. Neuropediatrcs. 2016;47:12–19.
11. Adebami OJ. Pattern of neonatal seizures in Osogbo south western Nigeria. SAJCH. 2010;4(2):46–49.
12. Nemati H, Karimzadeh P, Fallahi M. Causes and factors associated with neonatal seizure and its short-term outcome: a retrospective prognostic cohort study Iran. J Child Neurol. 2018;12(3):59–68. PMCID: PMC6045936.
13. Hashen AH, Ahmed I, Eslam EQ. Clinico-Etiological pattern of neonatal seizure. Al-azhar J ped. 2020. doi:10.21608/AZJP.2020.127064
14. Lai YH, Ho CH, Chui NC, Tsang CF, Huang YL. Prognostic factors of developmental outcome in neonatal seizure in terms infants. Pediatr Neonatol. 2013;166–172. doi:10.1016/j.pedneo.2013.01.001
15. Dongol Singh S, Shrestha RPB, Shrestha A. Etiological Profile and Neurodevelopment Outcome of Neonatal seizure. J Lumbini Med Coll. 2018;6(2). doi:10.22502/jlmc.v6i2.212
16. Sudia S, Berwal P, Nagaraj N, Jeavaji P, Swami S, Berwal A. Clinicoetiological profile and outcome of neonatal seizures. Int J Contemp Pediatr. 2015;2015:389–394. doi:10.36347/sjams.2020.v08i09.041
17. Amare HT, Amare AT. Etiology, clinical features, and short-term outcome of seizures in newborns admitted to the University of Gondar Hospital, Ethiopia. Pediatr Heal Med Ther. 2019;10:107–113. doi:10.2147/PHMT.S228241
18. Baudou E, Cances C, Dimeglio C, Hachon Lecamus C. Etiology of neonatal seizures and maintenance therapy use: a 10-year retrospective study at Toulouse Children’s hospital. BMC Pediatr. 2019;19:136. doi:10.1186/12887-019-1508-5
19. Laurel AS, Anup DP, Jonathan L. Pharmacological treatment of neonatal seizures: a systematic review. J Child Neurol. 2013;28(3):351–364. doi:10.1177/0883073812470734
20. World Health Organization. Guidelines on Neonatal Seizures. World Health Organization; 2011.
21. Aggarwal P, Chaudhari S, Bhave S, et al. Clinical predictors of outcome in hypoxic ischemic encephalopathy in term neonates. Ann Trop Paediatr. 1998;18:117–121. doi:10.1080/02724936.1998.11747937
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prediction of Long-Term Poor Clinical Outcomes in Cerebral Venous Thrombosis Using Neural Networks Model: The BEAST Study
Ranjan R, Ken-Dror G, Sharma P
International Journal of General Medicine 2024, 17:2919-2930
Published Date: 2 July 2024