Back to Journals » International Journal of Women's Health » Volume 18
Neoadjuvant Paclitaxel–Carboplatin Followed by Concurrent Chemoradiotherapy versus Concurrent Chemoradiotherapy Alone in Locally Advanced Cervical Cancer
Authors Homenta C, Kurniadi A ![]() , Winarno GNA
, Winarno GNA ![]() , Santiana L
, Santiana L ![]() , Utama MS
, Utama MS ![]()
Received 10 November 2025
Accepted for publication 9 March 2026
Published 13 March 2026 Volume 2026:18 580324
DOI https://doi.org/10.2147/IJWH.S580324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Christian Homenta,1 Andi Kurniadi,1 Gatot Nyarumenteng Adhipurnawan Winarno,1 Leni Santiana,2 Marhendra Satria Utama3
1Obstetrics and Gynecology Department, Universitas Padjadjaran/Hasan Sadikin Hospital, Bandung, Indonesia; 2Department of Radiology, Universitas Padjadjaran/Hasan Sadikin Hospital, Bandung, Indonesia; 3Department of Radiation Oncology, Universitas Padjadjaran/Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Christian Homenta, Obstetrics and Gynecology Department, Universitas Padjadjaran/Hasan Sadikin Hospital, Jl. Prof. Eyckman No. 38, Pasteur, Kec. Sukajadi, Kota Bandung, Jawa Barat, 40161, Indonesia, Email [email protected]
Background and Purpose: Concurrent chemoradiotherapy (CCRT) remains the standard of care for locally advanced cervical cancer, yet recurrence and treatment-related toxicity continue to limit outcomes. Neoadjuvant chemotherapy using a Paclitaxel-Carboplatin regimen followed by CCRT (NACT-CCRT) been proposed to improve therapeutic response while minimizing systemic toxicity. This study aimed to compare the efficacy and safety of NACT-CCRT versus CCRT alone in patients with locally advanced (FIGO IIA–IIIC) and metastatic (stage IVA) cervical cancer.
Patients and Methods: Prospective cohort study was conducted at Hasan Sadikin General Hospital, Bandung, between July 2024 and September 2025. Sixty-five eligible patients were enrolled using convenience sampling, comprising 32 in the NACT+CCRT group and 33 in the CCRT group. Treatment response was assessed according to RECIST 1.1 criteria, and tumour size reduction was measured using pelvic MRI before and after therapy. Statistical analysis included independent t-tests, Chi-square tests, and Repeated Measures ANOVA, with significance set at p< 0.05.
Results: Patients receiving NACT-CCRT achieved higher complete and overall response rates (100%) compared to those treated with CCRT alone. Tumour reduction exceeding 75% was observed in both groups, with the NACT+CCRT group show lower mortality rate. No significant increase in treatment-related toxicity was noted.
Conclusion: The combination of Paclitaxel Carboplatin-based neoadjuvant chemotherapy followed by chemoradiation appears to be an effective and well-tolerated approach for selected patients with locally advanced cervical cancer, particularly those with good performance status and large tumours. Nevertheless, larger randomized controlled trials and biomarker-driven studies are needed to validate these findings and identify subgroups that may achieve the most durable clinical benefit.
Keywords: cervical cancer, chemoradiotherapy, neoadjuvant chemotherapy, paclitaxel–carboplatin, treatment response, tumour reduction, toxicity, survival outcomes
Introduction
Cervical cancer remains one of the leading causes of cancer-related morbidity and mortality among women, accounting for about 17.2% of all malignancies and 19.1% of cancer deaths worldwide.1 Recent study have identified several signaling pathways and gene networks that contribute to tumor progression and aggressiveness, highlighting the complex nature of this malignancy.2 Despite advances in treatment, the overall survival rate drops markedly as the disease progresses, reaching only 25–50% in stages III–IV.3 These figures indicate that current therapeutic options, such as surgery, chemotherapy, radiotherapy, or their combination, have not yet achieved optimal outcomes.4
Concurrent chemoradiotherapy (CCRT) is widely accepted as the standard of care for locally advanced cervical cancer (LACC); however, it is still associated with high recurrence rates and notable systemic toxicity. In resource-limited settings, including many developing countries, restricted access to radiotherapy and treatment delays further worsen patient prognoses.4 To address these challenges, neoadjuvant chemotherapy (NACT) with agents such as Paclitaxel and Carboplatin administered before CCRT has been proposed as a potential strategy to improve tumour control and radiosensitivity. Paclitaxel induces G2/M phase cell-cycle arrest, a phase known to be highly radiosensitive, while platinum agents cause DNA cross-linking that enhances radiation-induced cytotoxicity. These mechanisms provide a biological rationale for using paclitaxel-carboplatin as induction chemotherapy prior to definitive chemoradiotherapy.5,6
Recent published INTERLACE trial demonstrated improved overall survival in patients with locally advanced cervical cancer who received induction chemotherapy followed by chemoradiotherapy, compared to those treated chemotherapy alone.7 However, evidence regarding treatment outcomes in resource-limited settings remains limited. Thus, the present study aims to compare the efficacy of NACT followed by CCRT versus CCRT alone in patients with locally advanced and metastatic cervical cancer, focusing on treatment response, recurrence, and toxicity. The results are expected to contribute to the refinement of multimodal therapeutic strategies and provide an evidence-based foundation for improving survival and quality of life among cervical cancer patients, particularly within the Indonesian healthcare context.
Materials and Methods
This investigation employed a prospective cohort design to compare therapeutic outcomes between patients treated with Neoadjuvant Chemotherapy (NACT) followed by Concurrent Chemoradiotherapy (CCRT) and those treated with CCRT alone in cases of locally advanced and metastatic cervical carcinoma. The study was conducted within the Department of Obstetrics and Gynecology and the Radiation Oncology Unit of Hasan Sadikin General Hospital, Bandung, from July 2024 to September 2025. Eligible participants were women diagnosed with locally advanced (FIGO 2018 stages IIA–IIIC) or metastatic (stage IVA) cervical cancer who provided written informed consent for inclusion in either treatment arm. Inclusion criteria comprised confirmed histopathological finding, nonrecurrent cervical malignancy, absence of previous hysterectomy or concomitant neoplasms, Eastern Cooperative Oncology Group (ECOG) performance status 0–1, and adequate hematologic, renal, and hepatic function. Patients who failed to complete therapy within 12 weeks, expired during treatment, or withdrew voluntarily were considered non-evaluable for response.
A total of 78 patients met eligibility criteria; 13 patients were not evaluable for response, eleven due to mortality before therapy completion and 2 due to voluntary discontinuation, resulting in 65 evaluable subjects (32 receiving NACT+CCRT and 33 receiving CCRT alone). The calculated sample size provided 80% statistical power at a 95% confidence level. Patients received neoadjuvant chemotherapy consisting of weekly paclitaxel 80 mg/m2 and carboplatin (AUC 2) for six cycles. This was followed by concurrent chemoradiotherapy according to the institutional protocol. External beam radiation therapy (EBRT) was delivered to the pelvic region at a dose of 50 Gy in 25 fractions, with weekly cisplatin 40 mg/m2 administered concurrently. After completion of EBRT, patients underwent intracavitary brachytherapy with a total dose of 28 Gy delivered in four fractions, resulting in an approximate cumulative radiation dose of 78 Gy. Collected variables included demographic characteristics (age at diagnosis), clinical parameters (FIGO stage, histopathological subtype, ECOG status), therapeutic protocol, and oncologic outcomes (pre- and post-treatment tumour dimensions, response rate, and adverse events). Tumour measurements were derived from pelvic magnetic resonance imaging (MRI), and treatment response was assessed per Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1.
Data were systematically recorded on standardized collection sheets. Statistical analyses incorporated both descriptive and inferential methods: intergroup comparisons of continuous variables utilized independent t-tests, whereas categorical variables were examined using Fisher’s exact tests. Repeated Measures ANOVA was applied to assess temporal changes in tumour size and interaction effects between treatment modalities. Statistical significance was set at α = 0.05 (p < 0.05) (Figure 1).
 |
Figure 1 Study Flowchart of NACT+CCRT vs. CCRT in Cervical Cancer. This diagram illustrates the recruitment of patients with locally advanced or metastatic cervical cancer via convenience sampling. Following pre-treatment MRI and randomization, the control group received standard concurrent chemoradiotherapy (CCRT), while the experimental group received neoadjuvant chemotherapy (NACT) prior to CCRT. Treatment response was assessed via MRI at 12 weeks post-completion. Statistical evaluation included descriptive metrics and inferential testing (Fisher’s Exact and independent t-tests). |
Ethical approval was granted by the Research Ethics Committee of Hasan Sadikin General Hospital (Approval Code: DP.04.03/D.XIV.6.5/386/2024). No generative artificial intelligence tools were employed in study design, data acquisition, or analysis beyond language refinement.
Results
A total of 78 patients diagnosed with locally advanced or metastatic cervical carcinoma were initially enrolled. Thirteen participants were not evaluable for response, eleven due to mortality before therapy completion and two due to voluntary discontinuation, yielding a final analytic cohort of 65 subjects. Thirty-two patients received Neoadjuvant Chemotherapy followed by Concurrent Chemoradiotherapy (NACT+CCRT), while thirty-three underwent CCRT alone. Baseline demographics and clinical characteristics were well balanced between the two cohorts. The mean age was comparable (46.9 ± 9.2 years in NACT+CCRT vs. 47.0 ± 9.9 years in CCRT; p = 0.968), with a shared median age of 44 years (IQR ± 13).
Clinical staging based on FIGO 2018 revealed predominance of stage IIB disease 18 patients (56.3%) in NACT+CCRT and 23 (69.7%) in CCRT followed by stage IIIB in 13 (40.6%) and 10 (30.3%) patients, respectively. Stage IVA was rare, present in one NACT+CCRT case and absent in CCRT. No statistically significant intergroup difference was observed (p = 0.366). Histopathological distribution was also similar: squamous cell carcinoma (SCC) was predominant (81.3% vs. 81.8%), followed by adenocarcinoma (12.5% vs. 9.1%) and adenosquamous carcinoma (6.3% vs. 9.1%) (p = 1.000). (Table 1).
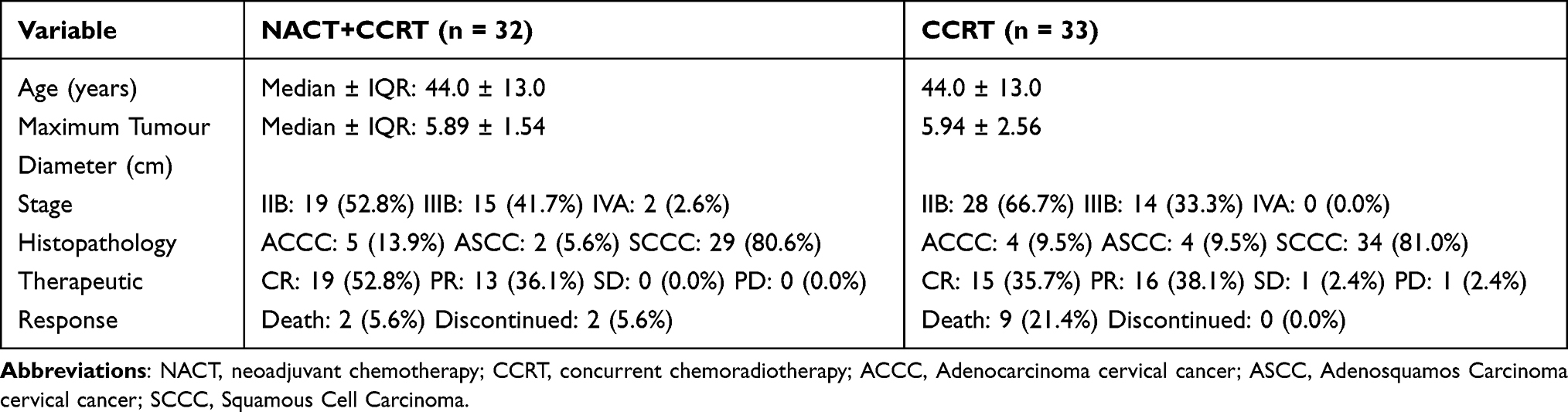 |
Table 1 Baseline Characteristics and Therapeutic Response |
Complete response (CR) was achieved in 59.4% of patients in the NACT+CCRT group compared with 45.5% in the CCRT cohort (p = 0.452). Although the difference did not reach statistical significance, the combined regimen demonstrated a clinically meaningful trend toward enhanced tumour eradication. Partial response (PR) occurred in 40.6% and 48.5% of patients in the respective groups. The NACT+CCRT arm achieved an overall response rate (ORR) of 100%, encompassing both CR and PR, whereas the CCRT group exhibited stable disease (3.0%) and progressive disease (3.0%), indicating a modestly lower ORR overall.
Table 2 presents a comparative analysis of treatment-related toxicities between patients receiving neoadjuvant chemotherapy followed by concurrent chemoradiotherapy (NACT + CCRT; n = 32) and those receiving CCRT alone (n = 33). No statistically significant differences were observed in haematological toxicities, including leukopenia, neutropenia, anaemia, and thrombocytopenia (all p > 0.05). Radiation-induced proctitis was infrequent and comparable between groups (p = 1.0000). Similarly, non-haematological toxicities such as cystitis, constipation, abdominal pain, hepatic toxicity, and renal toxicity did not differ significantly. In contrast, nausea and vomiting (p = 0.0022) and fatigue (p = 0.0000) were significantly more prevalent and of higher grade in the CCRT-only group. These findings indicate that the incorporation of neoadjuvant chemotherapy prior to concurrent chemoradiotherapy does not exacerbate overall treatment toxicity and may, in fact, mitigate certain gastrointestinal and fatigue-related adverse effects.
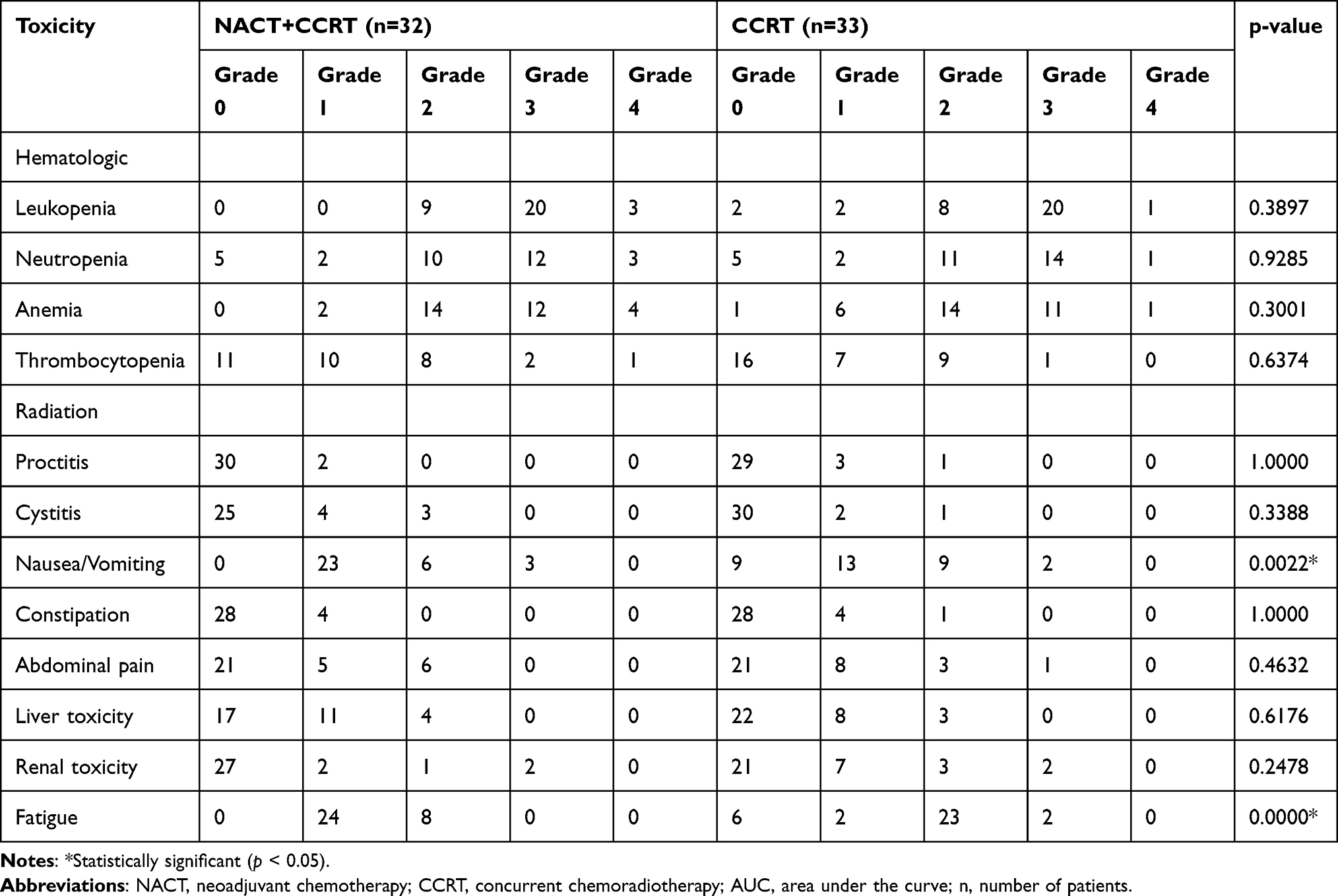 |
Table 2 Side Effect Comparison |
Mortality differed significantly between treatment modalities. Deaths occurred in 2 patients (5.6%) in the NACT+CCRT arm versus 9 patients (21.4%) in the CCRT arm (χ2(1) = 4.032; p < 0.045), suggesting a survival advantage associated with the neoadjuvant approach.
Repeated-measures ANOVA demonstrated a significant overall reduction in tumour dimensions across both treatment groups (F(1,63) = 387.539; p < 0.001). Between-group comparison revealed no significant difference (F(1,63) = 0.088; p = 0.768), and the interaction between time and treatment modality was also nonsignificant (F(1,63) = 0.016; p = 0.898). These findings indicate that both regimens were comparably effective in mediating volumetric tumour regression.
Quantitative analysis confirmed substantial tumour shrinkage exceeding 75% in both groups (p < 0.001). In the CCRT cohort, mean tumour size decreased from 5.005 ± 0.241 cm to 1.144 ± 0.238 cm, an average reduction of 3.816 ± 0.277 cm (≈ 76%). In the NACT+CCRT group, tumour dimensions declined from 4.948 ± 0.245 cm to 1.036 ± 0.242 cm, reflecting a mean reduction of 3.912 ± 0.281 cm (≈ 79%). Although intergroup differences were statistically nonsignificant, both treatment modalities yielded robust clinical efficacy, validating their therapeutic role in controlling primary tumour burden among patients with locally advanced and metastatic cervical cancer.
Discussion
The comparable baseline characteristics between the two treatment cohorts demonstrate a strong degree of internal validity, reinforcing the inferential reliability of the study outcomes. The balanced distribution of baseline parameters, including age (p = 0.968), disease stage (p = 0.366), and histopathological type (p = 1.000), confirms adequate homogeneity, ensuring that any observed clinical differences may be attributed to treatment modality rather than patient-related confounders.
The median age of 44 years in both groups corresponds with global epidemiological trends indicating that advanced-stage cervical carcinoma predominantly affects women aged 40–50 years.8–10 Similarly, the balanced stage distribution predominantly stages IIB (60.3%) and IIIB (37.2%) represents a typical profile of locally advanced disease, consistent with reports by Aziz (2009) and Bruni et al (2023), which noted that over 70% of cervical cancer cases in low- and middle-income countries are diagnosed at advanced stages due to limited screening and radiotherapy access.11
Although the Complete Response (CR) rate was higher in the NACT+CCRT group (59.4%) than in the CCRT-only group (45.5%), the difference did not reach statistical significance (p = 0.452). Nonetheless, this 13.9% improvement suggests a clinically meaningful trend consistent with global data supporting the addition of induction chemotherapy in advanced cases. Li et al (2024) reported a markedly higher CR rate with NACT+CCRT (87.7%) compared to CCRT (67.6%, p < 0.001), and the INTERLACE trial, involving over 500 participants, confirmed a significant progression-free survival advantage using a paclitaxel–carboplatin induction regimen.12,13 Despite lower absolute CR rates in the present study, the concordant trend implies that induction chemotherapy may enhance radiosensitivity and eliminate micro metastatic tumour before radiation.
Repeated Measures ANOVA indicated comparable tumour regression efficacy between NACT+CCRT and CCRT, with mean volume reduction ranging from 75–79% (p = 0.898). Both regimens demonstrated substantial cytoreductive capacity, suggesting a potential plateau in chemoradiation effectiveness. Nevertheless, the higher CR proportion in the NACT+CCRT cohort implies that induction chemotherapy may help certain tumours surpass the radiobiologic remission threshold. The synergistic rationale for combining NACT with radiotherapy is multifactorial. Cytoreduction improves oxygenation and perfusion, augmenting radio-sensitization.12 Early systemic therapy may eradicate occult micro metastases, mitigating progression risks. Moreover, chemotherapy-induced redistribution of cells into the radiosensitive G2/M phase, coupled with vascular normalization, optimizes intratumoral oxygenation and enhances radiotherapeutic efficacy.14 These mechanisms collectively validate the hypothesis that NACT not only diminishes tumour burden but also establishes a biologically favourable microenvironment for subsequent chemoradiation.15
Two adverse effects demonstrated statistically significant differences between the NACT+CCRT and CCRT groups: nausea/vomiting (p = 0.0022) and fatigue (p < 0.0001). Nausea and vomiting of grade >1 were more frequently observed in the CCRT group, indicating that the administration of neoadjuvant chemotherapy prior to chemoradiation may enhance gastrointestinal tolerance to subsequent cytotoxic and radiotherapeutic exposure. Similarly, grade >1 fatigue was reported more commonly among patients receiving CCRT alone, suggesting that NACT may mitigate systemic exhaustion typically associated with simultaneous chemoradiation stress.
Mortality differed significantly between groups, favouring NACT+CCRT (5.6%) over CCRT alone (21.4%) (χ2(1) = 4.032; p < 0.045). This indicates improved short-term survival and systemic disease control in patients receiving NACT. Several factors were identified as influencing the therapeutic response to neoadjuvant chemotherapy (NACT) in this study. Histologically, the predominance of Squamous Cell Carcinoma (SCC) exceeding 80% in both treatment arms was advantageous, as existing literature consistently demonstrates that SCC exhibits a superior response to neoadjuvant chemotherapy compared with adenocarcinoma.13 Regarding disease stage, the relatively balanced distribution with the majority of patients classified as stages IIB–IIIB represents an ideal population for NACT administration. Previous evidence indicates that patients within these stages display favourable chemotherapeutic responsiveness and higher rates of tumour regression following NACT.
When compared with landmark studies, the findings of the present investigation demonstrate concordant trends. The INTERLACE trial, which enrolled 500 patients, reported significant improvements in both progression-free survival (HR 0.65; 95% CI: 0.46–0.91; p = 0.013) and overall survival (HR 0.61; 95% CI: 0.40–0.91; p = 0.04) following induction chemotherapy.12 Although the current study was limited by smaller sample size and reduced statistical power, the observed directionality of outcomes aligns with INTERLACE results. Similarly, a series of studies by Li et al corroborate these findings, with the 2022 investigation demonstrating a 79.2% overall response rate including 10.4% complete responses, and the 2024 study reporting markedly higher CR rates in the NACT+CCRT group (87.7%) compared to controls (67.6%).12 Collectively, these parallels reinforce the consistency and clinical plausibility of NACT as a beneficial adjunct to concurrent chemoradiation in advanced-stage cervical cancer.16
The findings affirm that while CCRT remains the standard treatment for advanced cervical carcinoma, NACT+CCRT represents a promising adjunctive strategy for patients with optimal performance status (ECOG 0–1), SCC histology, and tumour size exceeding 4 cm. In regions such as Indonesia, where delayed presentation and radiotherapy access barriers persist, NACT may serve as a pragmatic bridging therapy for disease control prior to definitive local treatment. Internationally, these results align with the INTERLACE trial and emerging meta-analytic evidence supporting NACT integration into multimodal management of cervical cancer. The enhanced early response and reduced mortality observed warrant longitudinal assessment of its impact on progression-free and overall survival.
Limitations and Future Directions
Key limitations include a single-centred observational design and a limited follow-up duration, all of which constrain generalizability, and patients who discontinued treatment or died before completion of therapy did not have evaluable response data and were therefore not included in the response analysis. This approach may introduce potential selection bias and could lead to an overestimation of treatment response rates. Future investigations should adopt multi-centre randomized controlled designs with standardized chemotherapy protocols and extended follow-up to evaluate long-term efficacy and quality-of-life outcomes. Furthermore, biomarker-driven stratification studies are essential to delineate subgroups deriving maximal benefit from NACT. Economic and cost-effectiveness analyses should also be prioritized to facilitate sustainable integration of NACT into clinical practice, particularly in low-resource healthcare systems.
Conclusion
This study demonstrates that both concurrent chemoradiotherapy (CCRT) and neoadjuvant chemotherapy followed by chemoradiotherapy (NACT+CCRT) are effective treatment strategies for locally advanced and metastatic cervical cancer. The NACT+CCRT group exhibited higher complete and overall response rates, superior disease control, and lower treatment-period mortality compared with CCRT alone. Although the difference in tumour size reduction between the two groups was not statistically significant, both achieved substantial mass regression (>75%) with an acceptable safety profile. These results support the hypothesis that neoadjuvant chemotherapy prior to chemoradiation enhances radiosensitivity and early micro metastatic eradication, potentially improving short-term clinical outcomes. Overall, CCRT remains the standard of care for advanced cervical cancer, while NACT+CCRT may be considered a viable alternative in clinically optimal patients. Large-scale randomized controlled trials are warranted to verify long-term benefits on progression-free and overall survival and to support the development of evidence-based therapeutic guidelines in Indonesia.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. Institutional approval was granted by the Institutional Review Board of Hasan Sadikin Hospital, Bandung, Indonesia. Institutional approval was also required and obtained for the publication of the case details.
Data Sharing Statement
The data supporting the reported results are not publicly available due to privacy and ethical restrictions. However, they can be provided by the corresponding author upon reasonable request. Informed Consent Statements Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper based on Declaration of Helsinki.
Acknowledgments
The authors express their gratitude to the medical and administrative personnel of Hasan Sadikin Hospital for their invaluable support throughout the study. We also acknowledge the technical assistance of the team and the insightful contributions from colleagues who aided in the discussion and enhancement of this research.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kementerian Kesehatan Republik Indonesia. Profil kesehatan Indonesia 2022. Jakarta; 2022.
2. Li J, Li Y, Wang H, et al. Neoadjuvant chemotherapy with weekly cisplatin and paclitaxel followed by chemoradiation for locally advanced cervical cancer. BMC Cancer. 2023;23(1).
3. Zhou Y, Rassy E, Coutte A, et al. Current standards in the management of early and locally advanced cervical cancer: update on the benefit of neoadjuvant/adjuvant strategies. Cancers. 2022;14(10).
4. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2021 update. Int J Gynecol Obstet. 2021;155(S1):28–8. doi:10.1002/ijgo.13865
5. Danil N, Arifuddin S, Hartono E, et al. Perbandingan Respon Terapi dan Toksisitas Regimen Kemoterapi Kombinasi antara Paclitaxel, Carboplatin, dan Ifosfamide (TIP) dengan Paclitaxel dan Carboplatin (TP) pada Kanker Serviks Stadium IIb. Indonesian J Obstet Gynecol Sci. 2023;6(1):82. doi:10.24198/obgyniav6i1.451
6. Fowler J, Maani E, Dunton CJ. Cervical cancer [Internet]. 2023 [cited March 27, 2024]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431093/.
7. Zhang S, Xu H, Zhang L, Qiao Y. Cervical cancer: epidemiology, risk factors and screening. Chin J Cancer Res. 2020;32(6):720–728. doi:10.21147/j.issn.1000-9604.2020.06.05
8. Steel GG. Basic Clinical Radiobiology.
9. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. doi:10.3322/caac.21551
10. Aziz MF. Gynecological cancer in Indonesia. J Gynecol Oncol. 2009;20:8–10. doi:10.3802/jgo.2009.20.1.8
11. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022. CA Cancer J Clin. 2024;74:229–263. doi:10.3322/caac.21834
12. McCormack M, Gallardo Rincón D, Eminowicz G, et al. LBA8 A randomised Phase III trial of induction chemotherapy followed by chemoradiation compared with chemoradiation alone in locally advanced cervical cancer: the GCIG INTERLACE trial. Ann Oncol. 2024;34(Suppl 12):S1276. doi:10.1016/j.annonc.2023.10.028
13. Sibarani C, Salima S, Suardi D, Adrianto N, Mangkuliguna G. Efficacy and Safety of Neoadjuvant Chemotherapy Plus Concurrent Chemoradiotherapy Compared to Concurrent Chemoradiotherapy Alone in Locally Advanced Cervical Cancer: A Systematic Review and Meta-Analysis. Asian Pac J Cancer Prev. 2025;26:2793–2802. doi:10.31557/APJCP.2025.26.8.2793
14. Vale C, Tierney JF, Stewart LA, et al. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: a systematic review and meta-analysis of individual patient data from 18 randomized trials. J Clin Oncol. 2008;26:5802–5812. doi:10.1200/JCO.2008.16.4368
15. McCormack M, Eminowicz G, Gallardo D, et al. Induction chemotherapy followed by standard chemoradiotherapy versus standard chemoradiotherapy alone. Lancet. 2024;404:1525–1535. doi:10.1016/S0140-6736(24)01438-7
16. Schwab CL, English DP, Roque DM, Santin AD. Taxanes: their impact on gynecologic malignancy. Anticancer Drugs. 2014;25(5):522–38a. doi:10.1097/CAD.0000000000000057
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical and Management Dilemmas Concerning Early-Stage Cervical Cancer in Pregnancy – A Case Report
Kurniadi A, Setiawan D, Kireina J, Suardi D, Salima S, Erfiandi F, Andarini MY
International Journal of Women's Health 2023, 15:1213-1218
Published Date: 27 July 2023
Correlation of Histopathological and Radiological Response Patterns and Their Prognostic Implications in Breast Cancer After Neoadjuvant Chemotherapy
Bozer A, Yilmaz C, Çetin Tunçez H, Kocatepe Çavdar D, Adıbelli ZH
Breast Cancer: Targets and Therapy 2024, 16:1005-1017
Published Date: 31 December 2024