Back to Journals » Infection and Drug Resistance » Volume 19
Neglected Trichilemmal Carcinoma with Severe Opportunistic Cutaneous Wound Myiasis: A First Case Report and Implications for Elderly Rural Populations
Authors Cheng S, Zhang R, Li Y, Tian Z, Yang X, Xia Y
Received 11 December 2025
Accepted for publication 23 April 2026
Published 3 June 2026 Volume 2026:19 587439
DOI https://doi.org/10.2147/IDR.S587439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Arif Siddiqui
Sai Cheng,1,2 Ruzhi Zhang,1 Yajuan Li,2 Zhongwei Tian,2 Xiaoyu Yang,3 Yonghua Xia2
1Department of Dermatology, The Second Affiliated Hospital of Wannan Medical University, Wuhu, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Henan Medical University, Xinxiang, People’s Republic of China; 3Department of Pathology,The First Affiliated Hospital of Henan Medical University, Xinxiang, People’s Republic of China
Correspondence: Ruzhi Zhang, Email [email protected] Yonghua Xia, Email [email protected]
Abstract: This report describes the first documented case of trichilemmal carcinoma (TLC) complicated by opportunistic cutaneous wound myiasis in an elderly rural female patient with a long-standing ulcerated scalp tumour and heavy maggot infestation. Histopathological examination confirmed the diagnosis of TLC. A two-stage management strategy was implemented for the patient: initial eradication of myiasis and control of bacterial superinfection, followed by wide local excision of the tumour with split-thickness skin grafting. The patient achieved a good therapeutic outcome with no tumour recurrence at the 5-month follow-up. This case emphasizes the importance of considering parasitic infestation in the differential diagnosis of neglected ulcerative cutaneous malignancies, especially among vulnerable rural elderly populations with limited healthcare access. It also underscores the necessity of a stepwise therapeutic approach prioritizing infection control prior to definitive surgery, and provides a practical management reference for complex infected cutaneous malignancies.
Keywords: trichilemmal carcinoma, wound myiasis, elderly rural population, neglected neoplasm, bacterial superinfection, stepwise treatment
Introduction
Trichilemmal carcinoma (TLC) is a rare, low-grade malignant tumour of the hair follicle, which is thought to originate from the outer root sheath. It predominantly affects sun-exposed areas in elderly individuals.1,2 Clinically, it typically presents as a solitary, slow-growing nodule or plaque that may eventually ulcerate. Histopathological hallmarks include lobulated growth, glycogen-rich clear cells, abrupt trichilemmal-type keratinisation and an infiltrative margin.3
Cutaneous myiasis is a parasitic infestation caused by the larvae (maggots) of certain dipterous flies. It is clinically classified as furuncular, migratory or wound myiasis. Wound myiasis occurs when flies deposit eggs in existing skin lesions such as ulcers, traumatic wounds or neglected tumours. The developing larvae cause local tissue damage, pain and a significant risk of secondary bacterial infection.4
Although ulceration is a known potential complication of TLC and such wounds are susceptible to myiasis, the development of myiasis as a complication of a pre-existing TLC has not previously been reported. A systematic search of PubMed, Embase and Web of Science using the keywords “trichilemmal carcinoma”, “myiasis” and “maggot infestation” conducted prior to submission yielded no prior cases. This paper presents the first reported case of cutaneous myiasis as an opportunistic infestation following TLC, and discusses the associated diagnostic and therapeutic challenges as well as the probable pathogenic sequence.
Case Report
Clinical History
A 78-year-old woman attended our dermatology department with a scalp mass that had been present for over seven years and had recently ulcerated. The lesion initially presented as an asymptomatic, bean-sized papule which gradually enlarged. One month prior to her visit, the surface eroded and produced mild exudate. Three days prior to admission, the tumour underwent spontaneous full-thickness ulceration, accompanied by severe pain and the emergence of numerous maggots, which prompted her to seek medical attention. The patient had lived in a rural area all her life. Her past medical history included cerebral infarction, hypertension and hypothyroidism. She denied any history of diabetes mellitus or local trauma to the scalp. Six months prior to admission, a non-contrast cranial MRI scan performed for acute cerebral infarction incidentally identified a localised cauliflower-like scalp lesion (Figure 1). This incidental finding was not investigated further at that time due to the severity of her neurological condition.
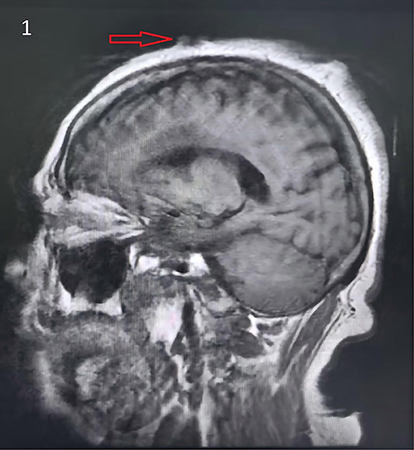 |
Figure 1 Incidental MRI finding (sagittal view, T1-weighted). An oval, cauliflower-like lesion measuring approximately 15 mm × 8 mm with a central depression can be seen on the scalp (red arrow). Infiltration into the subcutaneous fat layer is evident at the base of the lesion. |
Clinical Findings
On dermatological examination at admission, the following clinical features were observed: a dermatological examination revealed an irregular, exophytic tumour measuring 4 cm on the vertex of the scalp. The centre was ulcerated and contained necrotic tissue, haemorrhagic and serous exudate, as well as 30–40 actively moving white maggots (see Figures 2A and B). The surrounding skin was markedly erythematous and oedematous.
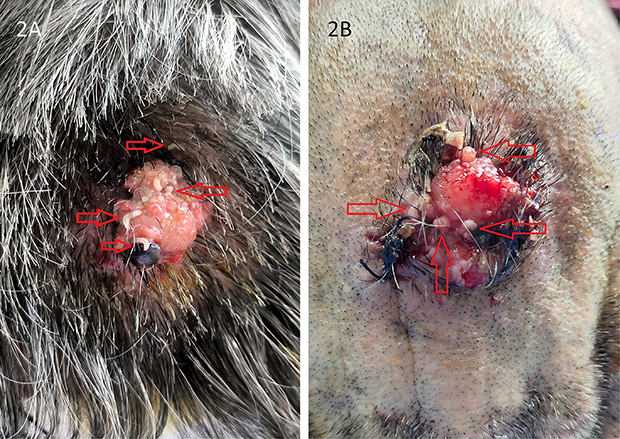 |
Figure 2 Clinical presentation at admission. (A) An irregular, exophytic tumour measuring 4 cm on the vertex of the scalp. (B) A close-up view of the ulcerated centre showing necrotic tissue, haemorrhagic exudate and numerous white maggots (red hollow arrows indicate visible larvae). |
Diagnostic Assessment
Laboratory tests: Routine blood tests revealed a mildly elevated white blood cell count of 10.67×109/L(normal range:4–10×109/L). Liver and renal function, electrolyte levels and clotting profiles were all within normal limits.
Bacterial Smear: Wound exudate was collected via sterile swab, Gram-stained using the standard Hucker’s modification method in accordance with the Clinical and Laboratory Standards Institute (CLSI) Microscopy Procedures for the Examination of Clinical Specimens (M15-A4), and examined under light microscopy at ×100 and ×1000 magnification. A bacterial smear of the wound exudate revealed numerous Gram-positive cocci and bacilli.
The maggots were removed for clinical management. Species identification to the species level could not be performed due to logistical constraints; however, morphological examination of the posterior spiracles was conducted to differentiate the family, which revealed three distinct slit-like openings with an intact peritreme—a hallmark feature of the Calliphoridae family—and the maggots were most likely a traumatic myiasis-causing species within the family Calliphoridae, consistent with the clinical presentation of wound myiasis.
Histopathology: Excised tissue was fixed in 10% neutral-buffered formalin, paraffin-embedded, sectioned at 4 μm, and stained with hematoxylin and eosin in compliance with the College of American Pathologists (CAP) Laboratory Accreditation Program standards for surgical pathology. Microscopic examination of the excised tumour revealed a lobulated, infiltrative dermal tumour with pushing borders. The tumour nodules were composed of atypical epithelial cells with abundant clear cytoplasm, prominent nucleoli and frequent mitotic figures. A diagnostic hallmark was the presence of abrupt trichilemmal-type keratinisation at the centre of tumour lobules (Figure 3A–C), in line with the classic histopathological diagnostic criteria for TLC outlined in the WHO Classification of Skin Tumours (5th Edition, 2020) and the foundational characterisation of TLC pathological features4.
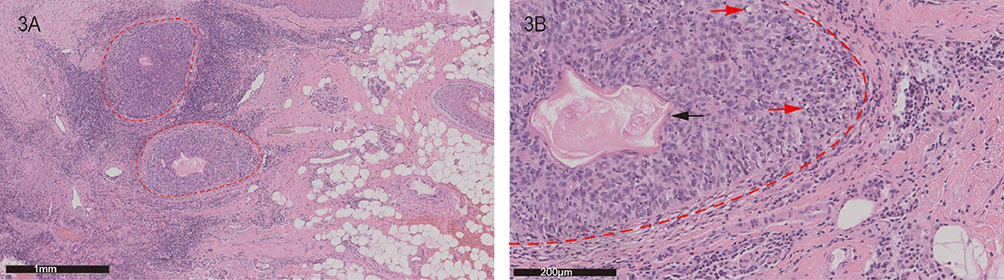 |
Figure 3 Histopathological features of the tumour (haematoxylin and eosin stain). (A) ×40: Low-power view showing a lobulated tumour mass with an infiltrative border (indicated by red dashed lines). (B) ×200: The tumour consists of cellular nests with peripheral palisading and central cells with clear cytoplasm (red arrowhead), accompanied by abundant abrupt trichilemmal-type keratinization (black arrowhead); atypical cells with large hyperchromatic nuclei, prominent nucleoli and frequent mitotic figures are also evident. |
Immunohistochemistry: Performed on formalin-fixed, paraffin-embedded sections using the standard avidin-biotin-peroxidase complex (ABC) technique in accordance with CAP immunohistochemistry (IHC) testing guidelines, with primary antibodies against P53 (clone DO7), P40 (clone ZR8), Ki67 (clone MIB1), and BerEP4 (clone BerEP4) used per manufacturer’s optimized protocols, the antibody panel was selected based on established IHC diagnostic criteria for TLC and differential diagnosis from other cutaneous epithelial tumours.5 The tumour cells showed diffuse positivity for P40, indicating squamous differentiation. The Ki-67 proliferation index was approximately 20%. P53 showed an aberrant overexpression pattern. Ber-EP4 was negative, which served as a key marker for differentiating TLC from basal cell carcinoma (Figure 4A–D). These findings are consistent with the characteristic IHC profile for TLC identified by systematic global clinical analysis. Final diagnosis: TLC; cutaneous myiasis (wound type), opportunistic, complicating TLC; bacterial superinfection secondary to cutaneous myiasis/ulcer.
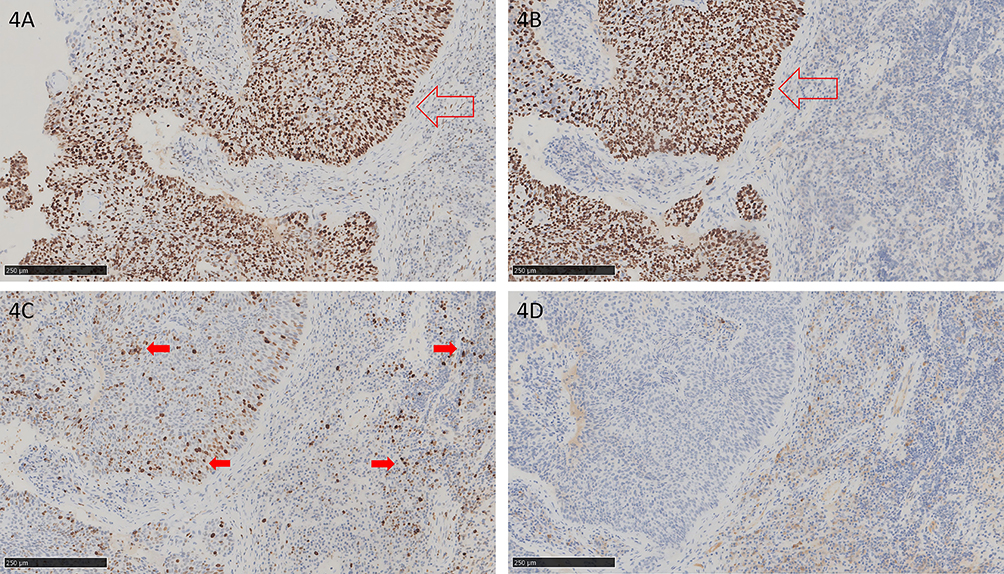 |
Figure 4 Immunohistochemical profile (all ×100 magnification). (A) P53 shows an aberrant, strong nuclear overexpression pattern (indicated by the red hollow arrow). (B) Tumour cells are diffusely positive for P40 (indicated by the red hollow arrow). (C) Ki-67 shows a mildly elevated proliferative index of approximately 20% (solid red arrows indicate positively stained cells). (D) Ber-EP4 is negative in tumour cells (positive internal control in adjacent sebaceous glands). |
Therapeutic Intervention and Follow-Up
Management was conducted in two sequential stages. In Stage 1, the parasitic infestation and local infection were addressed. The wound was thoroughly irrigated with hydrogen peroxide to stimulate the migration of any remaining larvae to the surface, which were then meticulously extracted with forceps. Necrotic tissue was surgically debrided. Topical 2% w/w mupirocin ointment was applied thinly to the wound bed twice daily and oral amoxicillin-clavulanate (400 mg amoxicillin/57 mg clavulanate per tablet), one tablet twice daily based on smear test results, in accordance with the Infectious Diseases Society of America (Infectious Diseases Society of America, IDSA) clinical practice guidelines for skin and soft tissue infections (skin and soft tissue infections, SSTIs). After seven days, with no further emergence of larvae and a clean, granulating wound bed, Stage 2 began. The tumour was completely excised with 1 cm clinical margins. The defect was covered with a split-thickness skin graft. The postoperative course was uneventful. Histopathological examination of the resection specimen confirmed clear lateral and deep margins. Excellent healing and graft take were observed at the 2-week follow-up (Figure 5). No signs of recurrence were observed at the 5-month follow-up. The patient provided written informed consent for the publication of this case report and all accompanying images.
 |
Figure 5 Postoperative outcome. The grafted wound site at 2-week follow-up, showing satisfactory healing and complete graft take. |
Discussion
We present a unique and previously unreported case of TLC that was subsequently complicated by wound myiasis. The pathogenic sequence of this case is initiated by TLC: tumour ulceration compromises the skin barrier, leading to bacterial overgrowth, and the malodorous exudate serves as an attractant for fly oviposition, ultimately resulting in myiasis.
The slow-growing yet locally infiltrative nature of TLC ultimately leads to full-thickness ulceration, which breaches the skin’s critical barrier function.4 The resulting necrotic tissue and protein-rich exudate create an ideal environment for bacterial proliferation, which was confirmed microbiologically in our case. The myiasis in this case is an opportunistic infestation arising as a complication of primary TLC. This completes the epidemiological pathway for infestation. Our patient’s lifelong residence in a rural area provided the necessary environmental exposure to these Diptera. It is worth noting that while larval infestation in this case was clearly pathogenic and detrimental, sterile larvae of certain species (eg, Lucilia sericata) are intentionally used in maggot debridement therapy (MDT) for chronic, non-healing ulcers. MDT takes advantage of larvae’s ability to debride necrotic tissue, reduce bacterial burden (including MRSA), and promote granulation.6 However, in our patient, the infestation was uncontrolled, involving an undiagnosed malignancy, and caused significant pain and tissue destruction—highlighting the critical distinction between therapeutic application and pathological infestation.
TLC was firmly diagnosed through its classic histopathological triad of lobulated architecture, clear glycogen-rich cells and abrupt trichilemmal keratinisation,7,8 supported by an immunohistochemical profile positive for P40 and negative for Ber-EP4. The myiasis diagnosis was unequivocally clinical, based on direct visualisation of motile maggots.
The cornerstone of successful management was resolving the acute parasitic and infectious complications prior to definitive oncological surgery. Eradicating the larvae and controlling the infection reduced tissue inflammation, improved wound bed quality and minimised the risk of systemic sepsis, thereby establishing safer conditions for wide excision. Wide local excision with clear margins remains the gold standard therapeutic approach for primary TLC to prevent local recurrence.9
Clinical Implications and Public Health Perspectives
This case provides several important insights: First, High index of suspicion: Clinicians should consider secondary myiasis when making a differential diagnosis for elderly patients from rural or resource-limited settings who present with long-standing, ulcerated tumours of the head and neck. Second, Primacy of Staged Management: A structured, sequential approach — beginning with aggressive parasite removal and infection control, followed by definitive tumour excision is paramount for achieving optimal outcomes in such complex cases. Third, Highlighting a Vulnerable Population: This case starkly illustrates the severe consequences of neglected skin cancers in ageing populations with potentially limited access to healthcare or awareness of it. It highlights the urgent need for enhanced community health education and improved access to dermatological care for the elderly in rural regions. Fourth, Vigilance Regarding Incidental Findings: The prior incidental MRI finding, which was not initially investigated, highlights the importance of examining and following up on suspicious cutaneous lesions identified during imaging for other reasons.
Specific environmental factors directly elevate the risk of cutaneous wound myiasis, particularly in patients with neglected ulcerated skin tumours,10 and their synergistic effects are evident in this case. A warm temperate climate (eg, hot summers in rural Henan Province) accelerates the breeding cycle of myiasis-causing flies (eg, Calliphoridae) and promotes larval development, increasing local fly density; rural agricultural settings increase close exposure to livestock—natural reservoir hosts for these flies—further raising the likelihood of fly-human contact; inadequate on-site sanitation (presence of organic waste) serves as an additional attractant for flies; and limited access to primary healthcare in rural areas delays the management of early-stage skin tumours, leading to progressive ulceration, necrotic tissue and malodorous exudate—these wound characteristics are the primary triggers for fly oviposition, the key step in myiasis development.11 Collectively, these interrelated environmental factors created a high-risk epidemiological context for myiasis in our patient, a lifelong rural resident with long-neglected TLC.
In addition, the patient’s personal perspective on this clinical course—when asked about her experience, she stated (translated from the local dialect):
I didn’t think much of the lump at first—it was just there. But when it started to hurt and I saw the worms, I was terrified. I never imagined a skin problem could become like this. If I had known earlier, I would have come to the hospital sooner.
—further underscores the fear and regret commonly experienced by patients with neglected skin lesions, and reinforces the critical need for targeted community health education for rural elderly populations at high risk of such complications.
Study Limitations
This case highlights several practical considerations for clinicians encountering similar presentations. First, to facilitate the detection of myiasis in ulcerated tumours during clinical examinations, deliberate and thorough inspection is essential, as superficial observation may be insufficient given larvae often retract into deep wound crevices. Gentle irrigation of the wound with normal saline is recommended to provoke larval movement, which effectively aids in the visualization and identification of maggots.12 Second, to confirm the success of the initial anti-parasitic and anti-infective management and determine the patient’s readiness for tumour excision, clinicians should verify the achievement of four key indicators: (1) no visible larvae identified on serial wound examinations over 48–72 hours; (2) complete resolution of the patient-reported characteristic “moving sensation” in the wound; (3) a marked reduction in malodorous wound exudate; and (4) the emergence of healthy, vascularized granulation tissue in the wound bed.13 Third, to increase awareness among health professionals, we propose that myiasis be routinely included in the differential diagnosis of any malodorous, necrotic ulcer—particularly in elderly, rural, or institutionalized patients, and especially for lesions located on the scalp or other poorly visualized areas. To increase patients’ awareness of myiasis as a potential complication of neglected skin lesions, health professionals should implement targeted educational initiatives: at the clinical level, provide one-on-one counseling for elderly rural patients with chronic skin tumours on the risks of myiasis from unmanaged ulceration; at the community level, launch public health education campaigns to emphasize the importance of seeking prompt medical attention for persistent or ulcerated skin lesions, and highlight the early signs of myiasis to facilitate timely patient reporting. Additionally, these educational efforts should be tailored to rural populations with limited access to healthcare, the primary high-risk group for this complication.
It is important to acknowledge the limitations of this report. Firstly, it describes a single case, which precludes broader generalisations and necessitates further independent case validation to confirm the novelty of TLC complicated by wound myiasis. Secondly, long-term oncological follow-up data beyond five months is not yet available. Additionally, as molecular identification was not performed, the exact fly species remains undetermined, which limits the specificity of the parasitological diagnosis. To further validate this first report and elucidate the clinical characteristics of this rare comorbidity, future literature expansion should include: systematic integration of TLC case data from regional dermatological registries and multicentre tumour databases; targeted reviews of cutaneous myiasis studies in patients with neglected skin malignancies; meta-analysis of risk factors for parasitic infestation in ulcerated adnexal tumours, with a focus on rural elderly populations with limited healthcare access. These expanded literature analyses, combined with additional case reports, will be critical to confirming the association between TLC and opportunistic wound myiasis and defining its clinical significance in high-risk populations.
Conclusion
This is the first reported case of neglected TLC complicated by severe cutaneous wound myiasis. It highlights the importance of a comprehensive diagnostic approach and stepwise therapeutic strategy for complex infected cutaneous malignancies, and also emphasizes the urgent need for enhanced dermatological care and health education for elderly rural populations with limited healthcare access.
Ethics Statement
This case report was conducted in accordance with the Declaration of Helsinki. Ethical review and approval, including for publication, were waived by the Institutional Review Board of The First Affiliated Hospital of Henan Medical University because this is a single retrospective case report that does not involve any interventional procedures or patient identification beyond anonymized clinical images. Written informed consent was obtained from the patient for publication of this report and any accompanying images.
Acknowledgments
We would like to thank the patient for her support and assistance in this study.
Funding
This study was supported by the Project Fund for Excellent Research and Innovation Teams in Universities of Anhui Province (Grant No. 2024AH010032). Additional support was provided by the Doctoral Research Start-up Fund of Henan Medical University (Grant No. xyyfy2019BS-001) and the Joint Construction Project of the Health Commission of Henan Province (Grant No. LHGJ20220597).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Headington JT. Tumours of the hair follicle. A review. Am J Pathol. 1976;85(2):479–8.
2. Sun J, Zhang L, Xiao M, et al. Systematic analysis and case series of the diagnosis and management of trichilemmal carcinoma. Front Oncol. 2023;12:1078272. doi:10.3389/fonc.2022.1078272
3. Xie Y, Wang L, Wang T. Huge trichilemmal carcinoma with metastasis presenting with two distinct histological morphologies: a case report. Front Oncol. 2021;11:681197. doi:10.3389/fonc.2021.681197
4. Zobairy H, Modaresi P, Cabada MM, Sofi-Mahmudi A. Nasopharyngeal myiasis in intensive care unit (ICU) patients: report of two cases. Iran J Parasitol. 2023;18(1):113–118. doi:10.18502/ijpa.v18i1.12388
5. Azarmi S, Akbarzadeh K, Ekrami A, Sheikh Z, Dehghan O. Scalp myiasis associated with soft tissue sarcoma lesion: a case report and review of relevant literature. BMC Infect Dis. 2024;24(1):51. doi:10.1186/s12879-023-08957-8
6. Simonetti O, Zerbato V, Bellinato F, et al. Eat and heal. Past, present and future of maggot debridement therapy: a narrative review. Infez Med. 2025;33(2):239–246. doi:10.53854/liim-3302-11
7. Wang Y, Sun Y, Kong W, Wang Y. Aural myiasis: a case report and literature review. Ear Nose Throat J. 2022;101(7):430–432. doi:10.1177/0145561320966072
8. Jadhav K, Venkateswaran R, Waghmare R, Bakhshi G, Jaiswal Y. Trichoblastic carcinoma of the right clavicular region: a case report with a review of the literature. Cureus. 2025;17(4):e82797. doi:10.7759/cureus.82797
9. Ahmed RS, Ali RM, Siddiq SO, et al. Cutaneous myiasis complicating squamous cell carcinoma: a case report with literature review. Dermatol Rep. 2025;17(4):10167. doi:10.4081/dr.2025.10167
10. Keskin K. Oral and paranasal myiasis: two case reports. SN Compr Clin Med. 2025;7:209. doi:10.1007/s42399-025-01984-3
11. Monawwer SA, Ali S, Ali SL, Malikzai A. Oral myiasis: a known case of scar epilepsy in a 45-year-old. Clin Case Rep. 2023;11(6):e7546. doi:10.1002/ccr3.7546
12. Güllüev M, Ata N, Öztürk K, Özbüğday Y, Koç E, Görgülü MH. Aural and nasal myiasis. J Ear Nose Throat Head Neck Surg. 2024;32(1):45–50. doi:10.24179/kbbbbc.2023-99793
13. Khan HZ, Shahid SA, Bakht N, Zaidi SSN. Myiasis encountered in squamous cell carcinoma of the oral cavity: a case report. Cureus. 2024;16(6):e62414. doi:10.7759/cureus.62414
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.