Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Negative and positive self-thoughts predict subjective quality of life in people with schizophrenia
Authors Takeda T ![]() , Nakataki M
, Nakataki M ![]() , Ohta M
, Ohta M ![]() , Hamatani S
, Hamatani S ![]() , Matsuura K, Yoshida R, Kameoka N, Tominaga T, Umehara H
, Matsuura K, Yoshida R, Kameoka N, Tominaga T, Umehara H ![]() , Kinoshita M, Watanabe S, Numata S, Sumitani S
, Kinoshita M, Watanabe S, Numata S, Sumitani S ![]() , Ohmori T
, Ohmori T ![]()
Received 15 October 2018
Accepted for publication 19 December 2018
Published 21 January 2019 Volume 2019:15 Pages 293—301
DOI https://doi.org/10.2147/NDT.S190381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Tomoya Takeda,1 Masahito Nakataki,2 Masashi Ohta,2 Sayo Hamatani,3 Kanae Matsuura,2 Reona Yoshida,2 Naomi Kameoka,2 Takeo Tominaga,4 Hidehiro Umehara,2 Makoto Kinoshita,2 Shinya Watanabe,4 Shusuke Numata,4 Satsuki Sumitani,5 Tetsuro Ohmori4
1Graduate School of Medical Science, Tokushima University, Tokushima, Japan; 2Department of Psychiatry, Tokushima University Hospital, Tokushima, Japan; 3Research Center for Child Mental Development, Chiba University, Chiba, Japan; 4Department of Psychiatry, Graduate School of Biomedical Sciences, Tokushima University, Tokushima, Japan; 5Academic Support Office for Students with Special Needs, Tokushima University, Tokushima, Japan
Purpose: Recently, cognitive variables such as negative and positive self-belief and thoughts have attracted much attention because they are associated with functional outcomes and quality of life (QOL). However, it is unclear how cognitive variables affect subjective and objective QOL. This study aimed to investigate the relationship of negative and positive self-belief and thoughts with subjective and objective QOL.
Participants and methods: Thirty-six people with schizophrenia participated in this study. Subjective and objective QOL were assessed with the Schizophrenia Quality of Life Scale (SQLS) and Quality of Life Scale (QLS), respectively. Neurocognitive function was assessed with the Brief Assessment of Cognition in Schizophrenia (BACS). Clinical symptoms were assessed with the Positive and Negative Syndrome Scale and Calgary Depression Scale for Schizophrenia. Side effects were assessed with the Drug-induced Extrapyramidal Symptoms Scale (DIEPSS). Negative and positive self-belief and thoughts were assessed with the Defeatist Performance Belief Scale and Automatic Thoughts Questionnaire-Revised. A generalized linear model was tested, with subjective and objective QOL as the response variable and symptoms, neurocognitive function, and cognitive variables that were significantly correlated with subjective and objective QOL as explanatory variables.
Results: In the schizophrenia group, the common objects score on the QLS was predicted by the composite BACS score, and the total QLS score was predicted by the DIEPSS score. Motivation and Energy, Psychosocial, and Symptoms and Side effects scores on the SQLS were predicted by depression and by negative automatic thought (NAT) and positive automatic thought (PAT).
Conclusion: Our results indicated that key targets for improving objective and subjective QOL in people with schizophrenia are side effects, neurocognitive function, depression, and NAT and PAT.
Keywords: defeatist performance belief, negative and positive automatic thoughts, subjective quality of life, objective quality of life, schizophrenia
Introduction
The goal of schizophrenia treatment has moved from “remission of symptoms” to “recovery in life.” In order to achieve recovery, it is necessary to identify the factors of functioning that lead to a good quality of life (QOL). QOL has been measured from two viewpoints. One is subjective QOL, which is rated by themselves, and the other is objective QOL, which is rated by observers.1 The concept of subjective QOL comprises well-being and satisfaction with life and that of objective QOL comprises daily life functioning and external resources.2,3 Furthermore, the correlation between objective and subjective QOL is reported to be weak to moderate.4,5 To achieve “recovery in life,” we must consider both subjective and objective viewpoints to understand the target and effect of treatment.
Previous studies have shown that several clinical factors such as positive symptoms, negative symptoms, depressive symptoms, dose of antipsychotics, and lower daily activity are associated with low subjective QOL.4–7 In addition, clinical factors such as neurocognitive function, positive symptoms, negative symptoms, depressive symptoms, side effects, dose of antipsychotics, and duration of illness have been found to be associated with low objective QOL.1,4,5,8,9 Together, these studies show that symptoms and neurocognitive function affect both subjective and objective QOL.
Recently, cognitive variables such as defeatist performance belief (DPB) have received much attention because they have been found to be associated with negative symptoms, functional outcomes, and QOL.10–13 DPB is a maladaptive belief (eg, “If you cannot do something well, there is little point in doing it at all”) that guides overgeneralized conclusion about one’s ability to perform a task.10 Grant and Beck10 suggested that neurocognitive deficits could contribute to failure experiences and difficulties in daily life, which may lead to the development of DPB and negative appraisals. Furthermore, Rector et al14 suggested that these cognitive variables might contribute to the avoidance of activities of daily living. Chung et al15 showed that not only negative beliefs but also positive beliefs about oneself are necessary for recovery. Negative and positive appraisals related to beliefs are negative automatic thought (NAT) and positive automatic thought (PAT) regarding oneself, the future, and the world.16,17 NAT and PAT increase automatically when people encounter negative and positive life events.17,18 Previous studies suggested that PAT (positive self-statement) might contribute to social adaptation and QOL.19,20
Previous studies have studied how symptoms and neurocognitive function influence subjective and objective QOL; however, it is still unclear how negative and positive self-belief and thoughts affect them. In this study, we investigated the relationship of negative and positive self-thought with both subjective and objective QOL.
Methods
Participants
Thirty-six people with schizophrenia participated in this study, including 16 men and 20 women with a mean age (±SD) of 42.86±9.40 years. All of them were diagnosed with schizophrenia based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria. At the time of study admission, they were clinically stable, as judged by a therapeutic psychiatrist after drug adjustment was completed. There was no remarkable change in their psychopathology during this study. The exclusion criteria were as follows: 1) past history or presence of any serious medical and neurological disorders that affect the brain or cognitive functioning, such as epilepsy, serious head injury, or brain tumor; 2) drug or alcohol abuse; and 3) active drug use in the past year.
Moreover, 37 demographically matched healthy controls were selected, including 17 men and 20 women. They were college students, hospital employees, or hospital employee’s acquaintances, with a mean age of 43.32±9.77 years. All participants provided written informed consent, and the study was approved by the institutional ethics committee of Tokushima University. This study was conducted in accordance with the Declaration of Helsinki.
Measures
Japanese Adult Reading Test (JART)
We used the 25-item short version of the JART,21,22 which was validated to estimate the premorbid intellectual ability by assessing the ability of reading Chinese characters.22
Wechsler Adult Intelligence Scale-III (WAIS-III)
To estimate the present intellectual ability, we used the short version of the WAIS-III,23,24 which comprises Information and Matrix Reasoning25 and has good reliability and validity compared to the standard version of WAIS-III.26
Positive and negative symptoms
To assess positive and negative symptoms, we used the Positive and Negative Syndrome Scale (PANSS).27,28 Higher scores indicate a greater level of symptom severity.
Depression
To assess depression, we used the Calgary Depression Scale for Schizophrenia (CDSS).29,30 The CDSS was specifically developed to distinguish depressive symptoms from positive and negative symptoms or antipsychotic-induced adverse effects in people with schizophrenia.30 Higher scores indicate a greater level of depression.
Side effects
To assess drug-induced extrapyramidal symptoms, we used the Drug-induced Extrapyramidal Symptoms Scale (DIEPSS).31 Higher scores indicate a greater level of extrapyramidal adverse effects.
Neurocognitive function
To assess neurocognitive function, we used the Brief Assessment of Cognition in Schizophrenia (BACS).32,33 The domains of neurocognitive function evaluated by the BACS include verbal memory, working memory, motor speed, verbal fluency, attention and speed of information processing, and executive function. A composite score is calculated by averaging the scores on these six standardized primary measures.32
DPB
To assess DPB, we used the Defeatist Performance Belief Scale (DPS), which is a subscale of the Dysfunctional Attitudes Scale (DAS).17,34 The DPS contains 15 items assessing an individual’s tendency to overgeneralize past failures to expected future failure.10 Higher scores indicate a greater level of DPB. In this study, the DPS showed good internal consistency in people with schizophrenia and controls (α=0.79 and 0.86, respectively).
Automatic thoughts
To assess automatic thoughts, we used the Automatic Thoughts Questionnaire-Revised (ATQ-R).17,35 This 40-item self-report instrument is designed to measure the frequency of occurrence of NATs (negative self-statements) and PATs (positive self-statements). Higher scores indicate a greater frequency of occurrence of NAT and PAT. The ATQ-R has a good reliability in Japanese people (α of NAT =0.95, α of PAT =0.82).36 Its construct validity was supported by its significant relationship with measures of depressive symptoms, eg, higher NAT was related to higher depression (Pearson’s r=0.72, P<0.01) and higher PAT was related to lower depression (Pearson’s r=−0.58, P<0.01).36
QOL
To assess subjective QOL, we used the Schizophrenia Quality of Life Scale (SQLS).37,38 It is a 30-item self-report questionnaire specific to people with schizophrenia. It comprises the following three scales: Psychosocial (PS), Motivation and Energy (ME), and Symptoms and Side effects (SS). Lower scores indicate better level of subjective QOL. PS addresses various emotional problems, for example, feeling lonely, depressed, or hopeless. ME address various problems of motivation and activity, such as lacking the will to do things. SS address issues such as sleep disturbance and blurred vision, which can be caused by medication.
To assess objective QOL, we used the Quality of Life Scale (QLS).39,40 It is a 21-item tool comprising the following five scales: Interpersonal relationships, Instrumental roles, Intrapsychic foundations, Common objects and activities, and total score. Higher scores indicate better objective QOL. Interpersonal relationships address various aspects of interpersonal and social experiences. Instrumental roles address the subjects’ roles of a worker, students, or housekeepers. Intrapsychic foundations address subjects’ sense of purpose and motivation. Common objects and activities address the possession of common objects and engagement in a range of regular activities.
Statistical analyses
Data analysis was conducted using SPSS Statistics for Windows, Version 22.0, R version 3.3.3 (2017-03-06), and R-studio.41–43 The demographic indices were compared between people with schizophrenia and controls using unpaired Chi-squared test, independent t-test, and the Mann–Whitney U test. For correlation analysis, Pearson’s correlation coefficients and Spearman’s rank correlation coefficients were calculated to evaluate the relationship of symptoms and neurocognitive function with cognitive variables and QOL in people with schizophrenia, according to the normality of the distribution of the dependent variables. Here, we used the false discovery rate (FDR) correction to adjust for multiple testing and set the significant threshold as an FDR-adjusted P-value of 0.05. Finally, a generalized linear model (GLM) was tested with subjective and objective QOL as the response variable and symptoms, neurocognitive function, and cognitive variables that had significant correlations with subjective and objective QOL as explanatory variables. The GLM is a flexible generalization of an ordinary linear regression that allows for response variables that have error distribution models other than a normal distribution. GLM is determined by two components (the distribution of the dependent variable and the link function). We used Gaussian and gamma distributions according to the normality of the dependent variables. For the GLM analysis, we used the MASS, qcc, AER, and pscl package in R-studio.44–47
Results
The demographic indices and cognitive performances of people with schizophrenia and controls are summarized in Table 1. People with schizophrenia were shown to have lower education year, premorbid intelligence quotient, present intelligence quotient, verbal memory, working memory, motor speed, attention and speed of information processing, verbal fluency, executive function, interpersonal relationships, instrumental role, intrapsychic foundation, common objects and activities, and total QLS score than controls. On the other hand, people with schizophrenia were shown to have higher NAT, DPB, ME score, and PS score than controls. The composite BACS score of the schizophrenia group was −1.20±0.76.
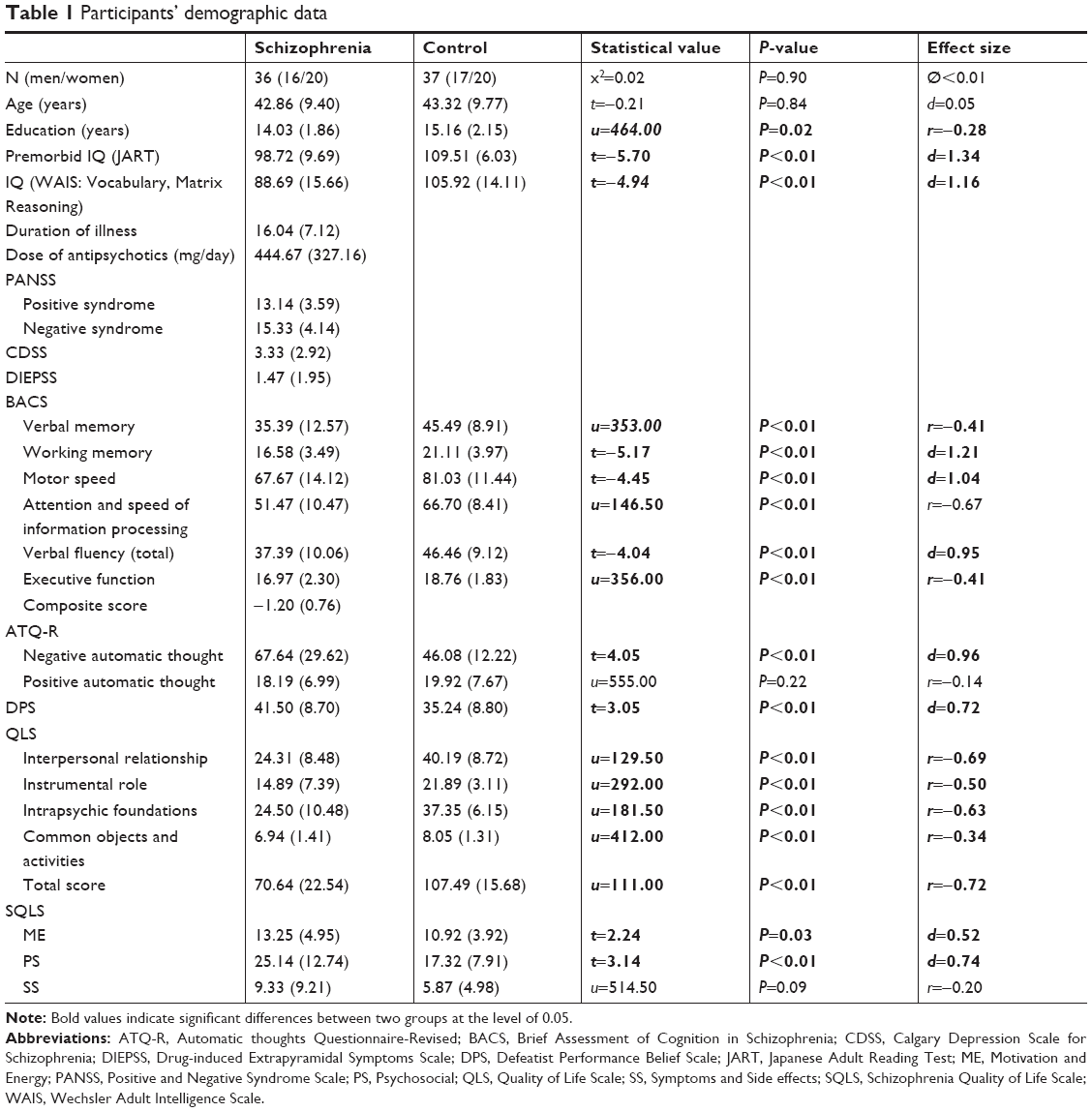 | Table 1 Participants’ demographic data |
Results of the Pearson’s correlation analyses and Spearman’s rank correlation coefficient analyses are shown in Tables 2 and 3. As shown in Table 2, higher verbal fluency score and the composite score of BACS were significantly related to higher common objects and activities score of QLS in the schizophrenia group. Fewer side effect and higher motor speed score and the composite BACS score and PAT score were significantly related to higher total QLS score. Furthermore, higher PAT score was significantly related to fewer ME score on the SQLS (Table 3). Higher depression and NAT were significantly related to higher PS score on the SQLS, and higher DPB and NAT were significantly related to the SS score (Table 3). On the other hand, in the control group (data not shown in Tables 2 and 3), there was no significant correlation between self-thought and objective QOL. However, there were significant correlations between self-thought and subjective QOL. DPB had a significant correlation with the PS score and the ME score (Pearson’s r=0.54, 0.43, P<0.01, respectively). NAT had a significant correlation with the PS score and the ME score (Pearson’s r=0.76, 0.61, P<0.01, respectively). PAT had a significant correlation with the ME score (Spearman’s rho r=−0.61, P<0.01). As with people with schizophrenia, self-thought was associated with subjective QOL in the control group.
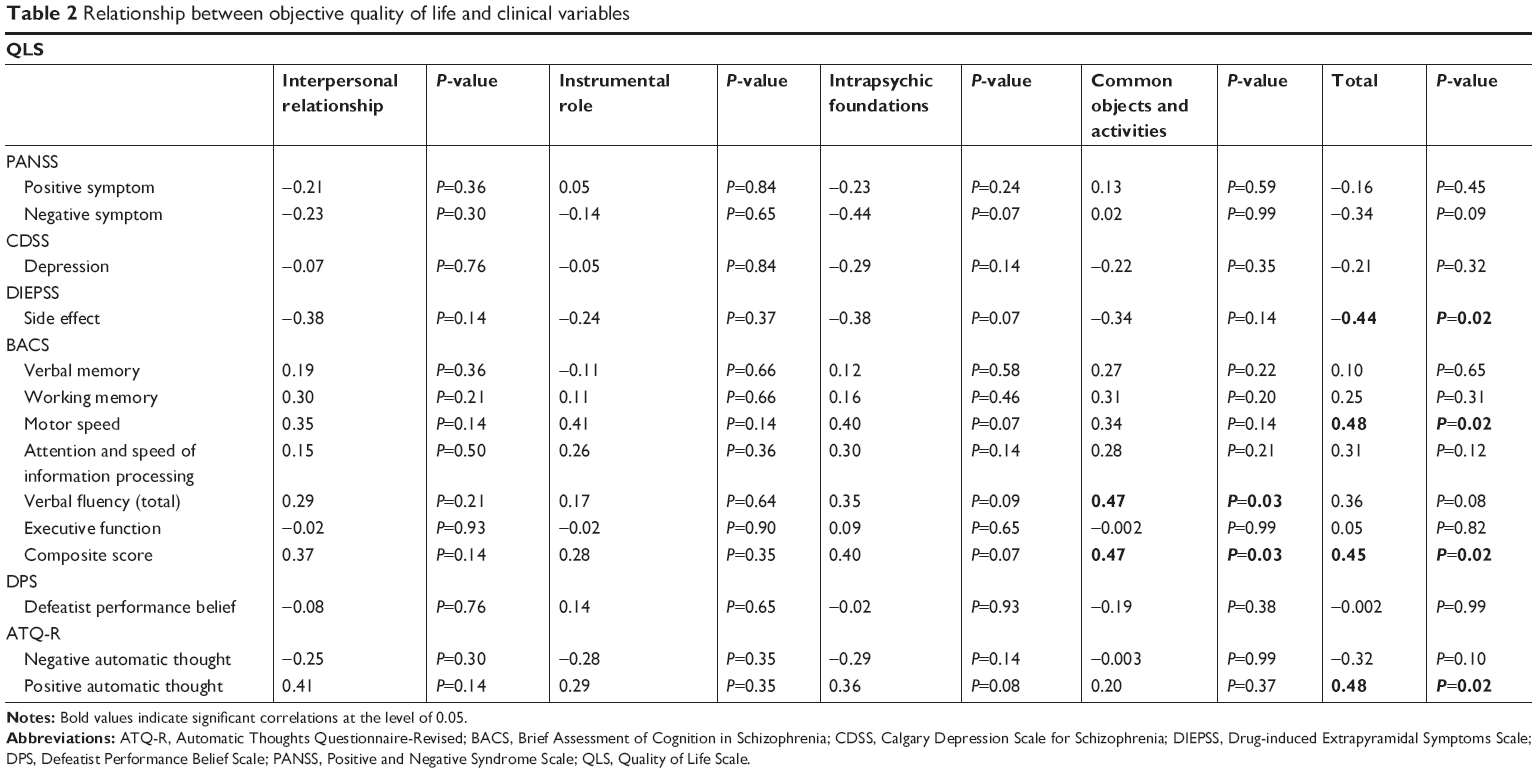 | Table 2 Relationship between objective quality of life and clinical variables |
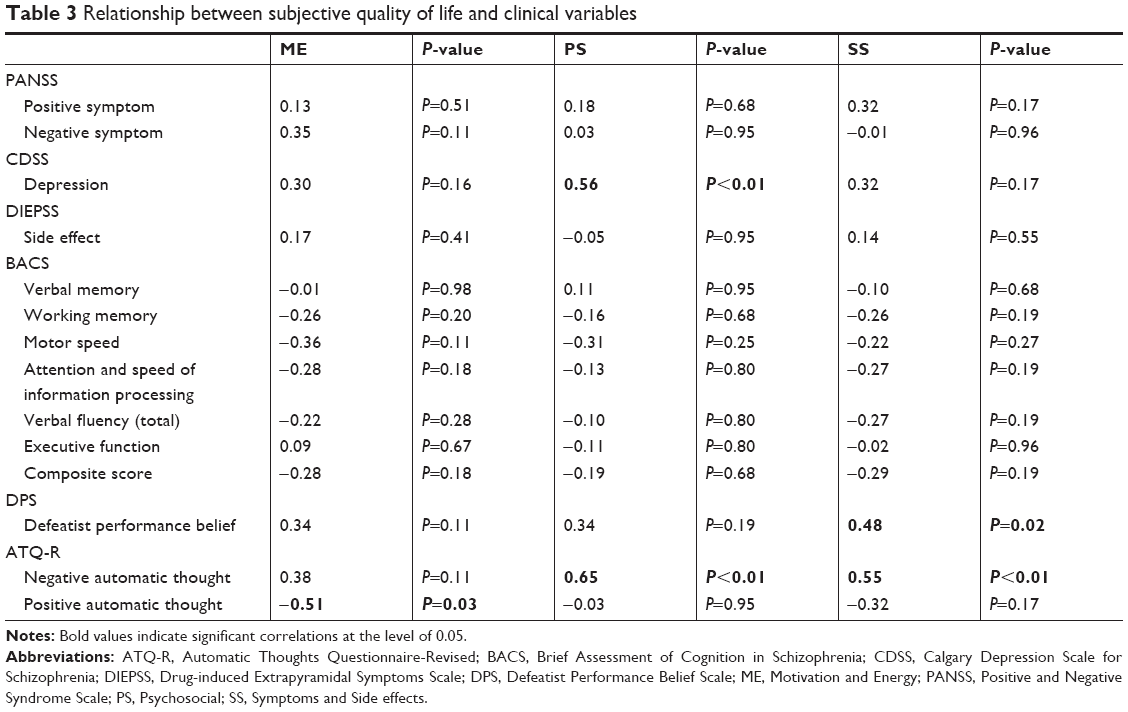 | Table 3 Relationship between subjective quality of life and clinical variables |
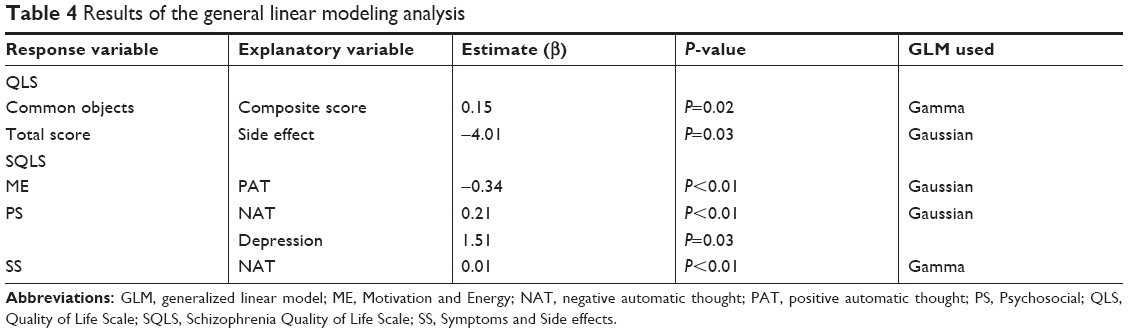
Table 4 shows the results of the GLM analysis in the schizophrenia group. The common objects and activities score on the QLS was predicted by the composite BACS score (β=0.15, P=0.02). Total QLS score was predicted by side effects (β=−4.01, P=0.03). Furthermore, the ME score on the SQLS was predicted by PAT (β=−0.34, P<0.01); the PS score was predicted by NAT (β=0.21, P<0.01) and depression (β=1.51, P=0.03); and the SS score was predicted by NAT (β=0.01, P<0.01).
 | Table 4 Results of the general linear modeling analysis |
Discussion
We showed that people with schizophrenia have higher negative belief and thoughts than controls. Furthermore, the results of this study indicated that objective QOL was predicted by side effects and neurocognitive function, whereas subjective QOL was predicted by depression and PAT and NAT. Therefore, we suggested that the key targets of treatment in people with schizophrenia to improve subjective and objective QOL are side effect, depression, neurocognitive function, and negative and positive self-thoughts.
Previous studies indicated that people with schizophrenia have higher DPB than controls.10–12 In addition, Hill et al48 showed that people with schizophrenia have higher NAT than controls. We confirmed these findings in Japanese people with schizophrenia. On the other hand, PAT did not differ significantly between the people with schizophrenia and controls. As far as we know, this is the first study to compare PATs between people with schizophrenia and controls. However, some previous studies have compared positive self-cognition between people with schizophrenia and controls, and they reported no differences between the two groups.49,50 In addition, Trémeau et al51 indicated that affective and cognitive processes involved in the anticipation and experience for positive affective events showed no deficit in people with schizophrenia. Our results are in line with previous studies and suggest that it is possible for stable people with schizophrenia to retain positive self-thought while having strong negative self-belief and thoughts.
As for the relationship of objective QOL and clinical variables with neurocognitive function and self-thought, the results of this study were consistent with those of previous studies that showed that neurocognitive function and side effects affect objective QOL.1,8,9 This result suggested that improvement of neurocognitive function and reduction of side effects might help improve objective QOL in people with schizophrenia. Previous studies showed a small correlation between DPB and objective QOL.11,12 However, this study did not find the significant relationship between DPB and objective QOL. This inconsistency might be caused by a difference in the measurement of QOL and the low statistical power due to the small number of participants. As for automatic thought, this study showed that automatic thought did not predict objective QOL. As far as we know, this is the first study that investigated the relationship between automatic thought and objective QOL in people with schizophrenia; however, further studies are needed to confirm these findings.
As for the relationship of subjective QOL and clinical variables with neurocognitive function and self-thought, the results of this study were consistent with those of previous studies that reported that depression affects subjective QOL.4–7 In addition, this study showed that NAT predicts higher feelings of loneliness. On the other hand, PAT predicted higher motivation and activities. Previous studies indicated that lower NAT and higher PAT have a significant relationship with subjective life satisfaction, social adaptation, and QOL in healthy subjects19,52 and people with depression.20 This study suggested that both PAT and NAT might be important for improving subjective QOL for people with schizophrenia as well. However, contrary to the expectation, DPB did not predict objective and subjective QOL in this study. Grant and Beck10 indicated that DPB was significantly correlated with objective QOL (Pearson’s r=-0.45, P<0.01). In addition, Campellone et al13 conducted a meta-analytic review and found a small effect size for the relationship of DPB and functional outcomes such as QOL and life skills. This inconsistency might be caused by a difference in the measurement of QOL and statistical methods. Furthermore, previous studies indicated that automatic thought strongly predicts depression than belief.48,53 Above all, automatic thought may affect the current state of mood and motivation rather than long-lasting beliefs. Therefore, automatic thought, rather than beliefs, might have more effect on subjective QOL, including motivation and emotional problems. However, few studies have examined the relationship among DPB, automatic thought, and QOL in people with schizophrenia. Thus, future studies need to further consider the relationship among these variables.
Conclusion
This study indicated that improving self-thought is an important target of treatment, in order to achieve recovery and improve the QOL of people with schizophrenia. Therefore, our findings may provide further evidence for the importance of PS treatment (eg, cognitive remediation therapy and cognitive behavior therapy) combined with pharmacotherapy.
This study has some limitations. First, the sample size was relatively small. Second, the participants showed relatively mild symptoms. Therefore, our results may not reflect the characteristics of all people with schizophrenia. Third, medications may have had an influence on our findings. Some of our people with schizophrenia might have depressed mood due to the side effects of antipsychotics. However, it is difficult to separate general depression from that caused by the side effects of antipsychotics. Fourth, we did not use structural interview for assessing control subjects. However, controls were evaluated with brief interviews to confirm the absence of schizophrenia and had no history of neurological or psychiatric disorders or any first-degree relatives with psychotic episodes. Future studies need to employ more detailed assessments of the mental status of healthy controls. Fifth, DPS that we used in this study has no significant correlation with negative symptoms (Pearson’s r=0.14, P=0.41). Meta-analysis indicated that the effect size is 0.25 between DPB and negative symptoms. This inconsistency might be caused by a difference in the measurement of negative symptoms and the low statistical power due to the small number of participants. Future study needs to clarify the relationship between DPB and negative symptoms in a larger sample of Japanese people with schizophrenia.
Abbreviations
ATQ-R, Automatic Thoughts Questionnaire-Revised; BACS, Brief Assessment of Cognition in Schizophrenia; CDSS, Calgary Depression Scale for Schizophrenia; DAS, Dysfunctional Attitudes Scale; DIEPSS, Drug-induced Extrapyramidal Symptoms Scale; DPB, defeatist performance belief; DPS, Defeatist Performance Belief Scale; FDR, false discovery rate; GLM, generalized linear model; JART, Japanese Adult Reading Test; ME, Motivation and Energy; SS, Symptoms and Side effect; NAT, negative automatic thought; PANSS, Positive and Negative Syndrome Scale; PAT, positive automatic thought; PS, Psychosocial; QLS, Quality of Life Scale; QOL, quality of life; SQLS, Schizophrenia Quality of Life Scale; WAIS-III, Wechsler Adult Intelligence Scale-III.
Acknowledgment
The authors would like to thank all subjects for participating in this study.
Author contributions
TTa carried out this study and drafted the manuscript. MO, SH, KM, RY, NK, TTo, HU, MK, SW, SN, and SS acquired the data. MN conceptualized the study, coordinated its implementation, and helped with drafting the manuscript. TO helped with the conception and design of the study. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Yamauchi K, Aki H, Tomotake M, et al. Predictors of subjective and objective quality of life in outpatients with schizophrenia. Psychiatry Clin Neurosci. 2008;62(4):404–411. | ||
Katschnig H. Schizophrenia and quality of life. Acta Psychiatr Scand. 2000;102(s407):33–37. | ||
Priebe S. Social outcomes in schizophrenia. Br J Psychiatry. 2007;191(S50):s15–s20. | ||
Tomotake M, Kaneda Y, Iga J, et al. Subjective and objective measures of quality of life have different predictors for people with schizophrenia. Psychol Rep. 2006;99(2):477–487. | ||
Aki H, Tomotake M, Kaneda Y, et al. Subjective and objective quality of life, levels of life skills, and their clinical determinants in outpatients with schizophrenia. Psychiatry Res. 2008;158(1):19–25. | ||
Gardsjord ES, Romm KL, Friis S, et al. Subjective quality of life in first-episode psychosis. A ten year follow-up study. Schizophr Res. 2016;172(1–3):23–28. | ||
Savill M, Orfanos S, Reininghaus U, Wykes T, Bentall R, Priebe S. The relationship between experiential deficits of negative symptoms and subjective quality of life in schizophrenia. Schizophr Res. 2016;176(2–3):387–391. | ||
Tolman AW, Kurtz MM. Neurocognitive predictors of objective and subjective quality of life in individuals with schizophrenia: a meta-analytic investigation. Schizophr Bull. 2012;38(2):304–315. | ||
Ueoka Y, Tomotake M, Tanaka T, et al. Quality of life and cognitive dysfunction in people with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):53–59. | ||
Grant PM, Beck AT. Defeatist beliefs as a mediator of cognitive impairment, negative symptoms, and functioning in schizophrenia. Schizophr Bull. 2009;35(4):798–806. | ||
Horan WP, Rassovsky Y, Kern RS, Lee J, Wynn JK, Green MF. Further support for the role of dysfunctional attitudes in models of real-world functioning in schizophrenia. J Psychiatr Res. 2010;44(8):499–505. | ||
Kiwanuka JN, Strauss GP, Mcmahon RP, Gold JM. Psychological predictors of functional outcome in people with schizophrenia. Schizophr Res. 2014;157(1–3):299–304. | ||
Campellone TR, Sanchez AH, Kring AM. Defeatist performance beliefs, negative symptoms, and functional outcome in schizophrenia: a meta-analytic review. SCHBUL. 2016;42(6):1343–1352. | ||
Rector NA, Beck AT, Stolar N. The negative symptoms of schizophrenia: a cognitive perspective. Can J Psychiatry. 2005;50(5):247–257. | ||
Chung YC, Kim HM, Lee KH, et al. Clinical characteristics of patients who have recovered from schizophrenia: the role of empathy and positive-self schema. Early Interv Psychiatry. 2013;7(2):138–145. | ||
Sm K, Tps O. Differential causal roles of dysfunctional attitudes and automatic thoughts in depression. Cogn Ther Res. 1992;16(3):309–328. | ||
Sakamoto S, Tanaka E, Tanno Y. Testing Beck’s model of depression: Using the DAS and the ATQ. Psychological Research Nihon University. 2004;25:14–23. | ||
Burgess E, Haaga DAF. The positive automatic thoughts questionnaire (ATQ-P) and the automatic thoughts questionnaire – Revised (ATQ-RP): equivalent measures of positive thinking? Cogn Ther Res. 1994;18(1):15–23. | ||
Ingram RE, Kendall PC, Siegle G, Guarino J, Mclaughlin SC, et al. Psychometric properties of the positive automatic thoughts questionnaire. Psychol Assess. 1995;7(4):495–507. | ||
Tanoue A, Ito D, Ohno M. Factors correlating depression and social adaptation for depression: using the ATQ-R, Tac, kiss. Japanese J Behavior Therapy. 2010;36(2):95–106. | ||
Nelson H, Willison J. National Adult Reading Test (NART). Windsor: NFER-Nelson; 1991. | ||
Matsuoka K, Uno M, Kasai K, Koyama K, Kim Y. Estimation of premorbid IQ in individuals with Alzheimer’s disease using Japanese ideographic script (kanji) compound words: Japanese version of national adult reading test. Psychiatry Clin Neurosci. 2006;60(3):332–339. | ||
Wechsler D. WAIS-III: Wechsler Adult Intelligence Scale, Administration and Scoring Manual. 3rd ed. San Antonio: Psychological Corporation/Harcourt BraceTexas; 1997. | ||
Japanese WAIS-III Publication Committee. Nihonban WAIS-III Chinou Kensa Japanese Wechsler Adult Intelligence Scale. 3rd ed. Nihon bunka kagakusha, Tokyo; 2006 (in Japanese). | ||
Fujita K, Maekawa H, Dairoku K, Yamanaka K. WAIS-III no kaisyaku jirei to rinshou kenkyu. Nihon bunka kagakusha. Tokyo; 2011. | ||
Dairoku K, Yamanaka K, Fujita K, Maekawa H. Short forms of Japanese WAIS-III for estimating FSIQ. Proceedings of the 73rd Annual Convention of the Japanese Psychological Association; 2009:433. | ||
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. | ||
Kay SR, Opler LA, Fiszbein A. [Positive and Negative Syndrome Scale (PANSS) Rating Manual]. Seiwa, Tokyo; 1991. Japanese. | ||
Addington D, Addington J, Maticka-Tyndale E. Assessing depression in schizophrenia: the Calgary depression scale. Br J Psychiatry. 1993;163(S22):39–44. | ||
Kaneda Y, Fujii A, Ohmori T. Psychometric properties of the Japanese version of the Calgary depression scale for schizophrenics. J Nerv Ment Dis. 2000;188(4):237–239. | ||
Inada T. Evaluation and Diagnosis of Drug-Induced Extrapyramidal Symptoms: Commentary on the DIEPSS and Guide to Its Usage. Seiwa, Tokyo; 1996 (in Japanese). | ||
Keefe RS, Goldberg TE, Harvey PD, Gold JM, Poe MP, Coughenour L. The brief assessment of cognition in schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res. 2004;68(2–3):283–297. | ||
Kaneda Y, Sumiyoshi T, Keefe R, Ishimoto Y, Numata S, Ohmori T. Brief assessment of cognition in schizophrenia: validation of the Japanese version. Psychiatry Clin Neurosci. 2007;61(6):602–609. | ||
Weissman AN, Beck AT. Development and validation of the dysfunctional attitudes scale: a preliminary investigation. Paper presented at the Annual Meeting of the American Educational Research Association. 1978. | ||
Hollon SD, Kendall PC. Cognitive self-statements in depression: development of an automatic thoughts questionnaire. Cogn Ther Res. 1980;4(4):383–395. | ||
Nishikawa D, Matsunaga M, Furutani K. [The effects of rumination on automatic thoughts and depressive symptoms]. Shinrigaku Kenkyu. 2013;84(5):451–457. Japanese. | ||
Wilkinson G, Hesdon B, Wild D, et al. Self-report quality of life measure for people with schizophrenia: the SQLS. Br J Psychiatry. 2000;177(01):42–46. | ||
Kaneda Y, Imakura A, Fujii A, Ohmori T. Schizophrenia quality of life scale: validation of the Japanese version. Psychiatry Res. 2002;113(1–2):107–113. | ||
Heinrichs DW, Hanlon TE, Carpenter WT. The quality of life scale: an instrument for rating the schizophrenic deficit syndrome. Schizophr Bull. 1984;10(3):388–398. | ||
Heinrichs DW, Halton TE, Carpenter WT. The Quality of Life Scale. Seiwa, Tokyo; 2001 (in Japanese). | ||
IBM Corporation. IBM SPSS Statistics for Windows, Version 22.0. IBM Corp 2012; Armonk, NY. | ||
R studio team. RStudio: Integrated Development for R. Rstudio, Inc 2015; Boston, MA. | ||
R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing 2004; Vienna, Austria. Available from http://www.R-project.org. Accessed date January 2, 2019. | ||
Venables WN, Ripley BD. Modern Applied Statistics with S. 4th ed. New York: Springer; 2002. | ||
Scrucca L. qcc: an R package for quality control charting and statistical process control. R News/1. 2004:11–17. | ||
Kleiber C, Zeileis A. Applied Econometrics with R. New York: Springer-Verlag, 2008; ISBN978-0-387-77316-2. URL https://CRAN.R-project.org/package=AER | ||
Jackman S. pscl: Classes and Methods for R Developed in The Political Science Computational Laboratory. Sydney, New South Wales, Australia; United States Studies Centre, University of Sydney; 2017. | ||
Hill CV, Oei TPS, Hill MA. An empirical investigation of the specificity and sensitivity of the automatic thoughts Questionnaire and dysfunctional attitudes scale. J Psychopathol Behav Assess. 1989;11(4):291–311. | ||
Barrowclough C, Tarrier N, Humphreys L, Ward J, Gregg L, Andrews B. Self-esteem in schizophrenia: relationships between self-evaluation, family attitudes, and symptomatology. J Abnorm Psychol. 2003;112(1):92–99. | ||
Fowler D, Freeman D, Smith B, et al. The brief core schema scales (BCSS): psychometric properties and associations with paranoia and grandiosity in non-clinical and psychosis samples. Psychol Med. 2006;36(6):749–759. | ||
Trémeau F, Antonius D, Cacioppo JT, et al. Anticipated, on-line and remembered positive experience in schizophrenia. Schizophr Res. 2010;122(1–3):199–205. | ||
Arimitsu K, Hofmann SG. Cognitions as mediators in the relationship between self-compassion and affect. Pers Individ Dif. 2015;74:41–48. | ||
Hollon SD, Kendall PC, Lumry A. Specificity of depressotypic cognitions in clinical depression. J Abnorm Psychol. 1986;95(1):52–59. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.